Embed Size (px)
Citation preview
Toxicity of Local Anesthetics 2005 Donald H. Lambert
TOXCITY OF LOCAL ANESTHETICS�CENTRAL NERVOUS SYSTEM
� SIGN AND SYMPTOMS� EFFECT OF POTENCY� RATE OF INJECTION� ACID BASE STATUS
� CARDIOVASCULAR SYSTEM� INOTROPY� PERIPHERAL VASCULAR SYSTEM� CC/CNS RATIO� VENTRICULAR ARRHYTHMIAS� PREGNANCY� RESUSCITATION
� MISCELLANEOUS� METHEMOGLOBINEMIA� ALLERGY� LOCAL TISSUE TOXICITY
This is the outline for this session.
The objectives of this session are:1. Understand the circumstances that cause systemic and cardiovascular
toxicity in the daily clinical practice of regional anesthesia.2. Understand the management of systemic and cardiovascular toxicity
of local anesthetics.3. Cite methods for avoiding local anesthetic neural toxicity.
When properly given, local anesthetics are generally free of side effects.However, systemic or localized toxicity occurs with accidental intravascularinjection or by injecting excessive doses (especially intrathecally). Additionally,other adverse effects occur with certain agents, e.g., allergic reactions to theamino-esters, and methemoglobinemia with benzocaine and with high doses ofprilocaine.
Systemic toxicity affects the central nervous and the cardiovascular systems.The central nervous system (CNS) is more susceptible to local anesthetic toxicitythan is the cardiovascular system. The dose and blood level of local anestheticthat produce CNS toxicity is lower than the dose that causes circulatory collapse.Although local anesthetic cardiovascular toxicity occurs less frequently thanCNS toxicity, it is more serious and more difficult to treat.
Toxicity of Local Anesthetics
● Central Nervous System� Earliest signs and symptoms are those of
excitation owing to depression of inhibitorycells allowing excitatory cell preponderance
● Tinnitus● Light headedness● Confusion● Circum-oral numbness● Tonic-clonic convulsions
The initial symptoms of CNS toxicity include feelings of lightheadedness anddizziness followed by visual and auditory disturbances such as difficulty infocusing and tinnitus. Other subjective CNS symptoms are disorientation andfeelings of drowsiness. Objective signs of CNS toxicity are excitatory in nature.They include shivering, muscular twitching and tremors initially involvingmuscles of the face and distal parts of the extremities. Later, tonic-clonicconvulsions occur.
Toxicity of Local Anesthetics
● Central Nervous System� Excitation is followed by depression
● Drowsiness● Unconsciousness
� Respiratory Arrest
If a sufficiently large dose or a rapid intravenous injection of local anesthetic isgiven, the initial signs of CNS excitation are followed rapidly by CNSdepression. Ultimately, seizure activity ceases and respiratory depression isfollowed by respiratory arrest. In some patients, CNS depression occurs withoutthe preceding excitatory phase, particularly if other CNS depressant drugs weregiven.
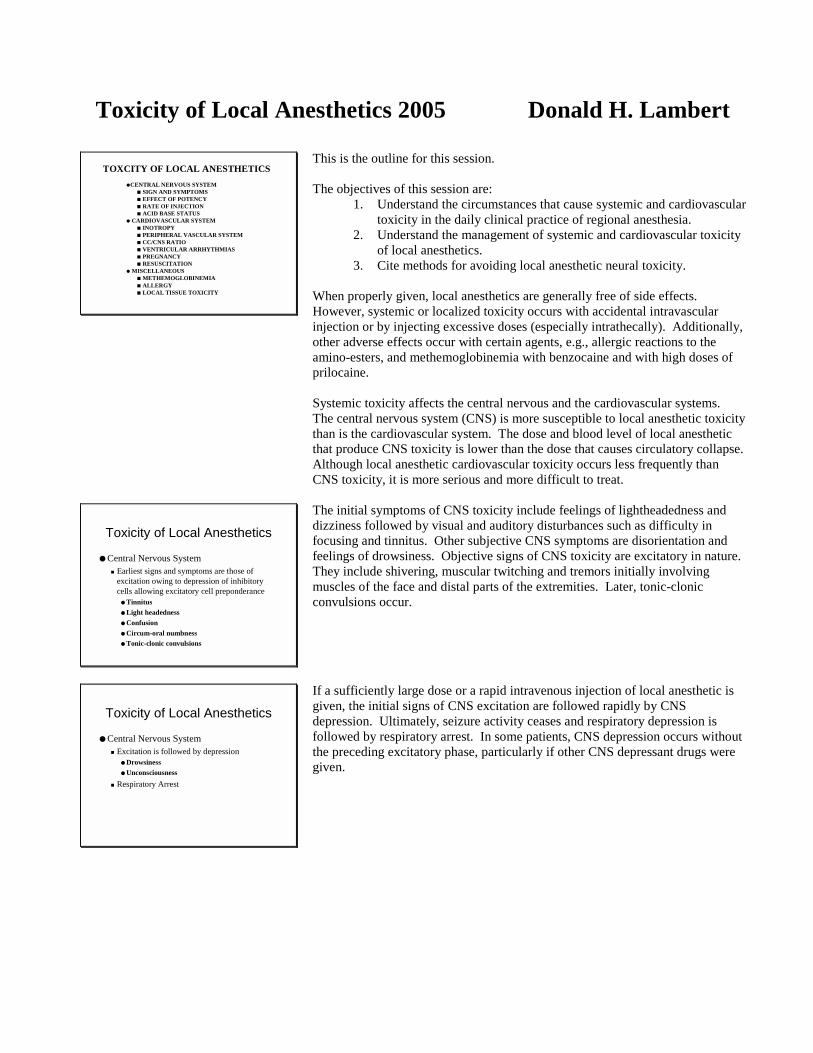
Classically, CNS excitation is believed to be due to local anesthetic blockade ofinhibitory pathways in the cerebral cortex. The blockade of inhibitory pathwaysdis-inhibits facilitator neurons, resulting in convulsions, owing to unopposedexcitatory nerve activity. Further increases in the dose of local anesthetic causesinhibition of both inhibitory and facilitator pathways resulting in CNSdepression. This graphic shows what I have observed clinically. With lidocaine,there is more excitation (upper left) before the seizure (upper right) than with themore potent agents like etidocaine, where there is little excitation (lower left) andthe seizure occurs abruptly (lower right).1
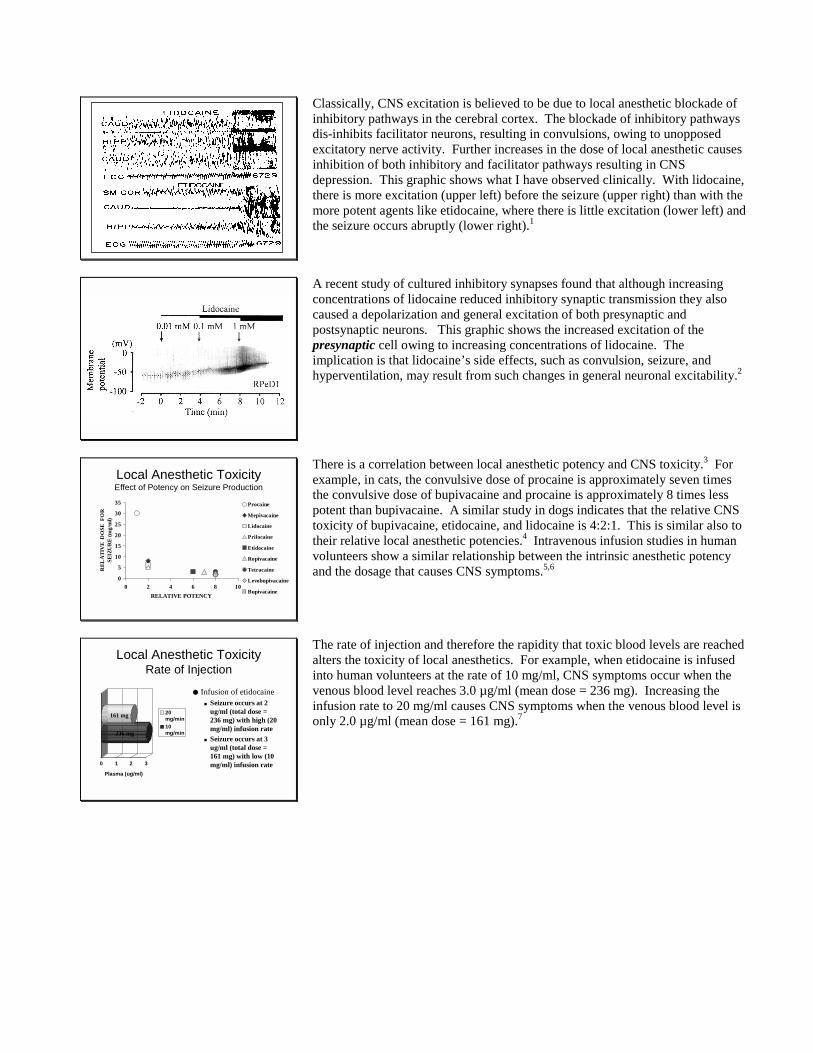
A recent study of cultured inhibitory synapses found that although increasingconcentrations of lidocaine reduced inhibitory synaptic transmission they alsocaused a depolarization and general excitation of both presynaptic andpostsynaptic neurons. This graphic shows the increased excitation of thepresynaptic cell owing to increasing concentrations of lidocaine. Theimplication is that lidocaine’s side effects, such as convulsion, seizure, andhyperventilation, may result from such changes in general neuronal excitability.2
Local Anesthetic ToxicityEffect of Potency on Seizure Production
0
5
10
15
20
25
30
35
0 2 4 6 8 10RELATIVE POTENCY
REL
ATI
VE
DO
SE F
OR
SE
IZU
RE
(mg/
ml)
Procaine
Mepivacaine
Lidocaine
Prilocaine
Etidocaine
Ropivacaine
Tetracaine
Levobupivacaine
Bupivacaine
There is a correlation between local anesthetic potency and CNS toxicity.3 Forexample, in cats, the convulsive dose of procaine is approximately seven timesthe convulsive dose of bupivacaine and procaine is approximately 8 times lesspotent than bupivacaine. A similar study in dogs indicates that the relative CNStoxicity of bupivacaine, etidocaine, and lidocaine is 4:2:1. This is similar also totheir relative local anesthetic potencies.4 Intravenous infusion studies in humanvolunteers show a similar relationship between the intrinsic anesthetic potencyand the dosage that causes CNS symptoms.5,6
Local Anesthetic ToxicityRate of Injection
0 1 2 3
Plasma (ug/ml)
20mg/min10mg/min
● Infusion of etidocaine� Seizure occurs at 2
ug/ml (total dose =236 mg) with high (20mg/ml) infusion rate
� Seizure occurs at 3ug/ml (total dose =161 mg) with low (10mg/ml) infusion rate
161 mg
236 mg
The rate of injection and therefore the rapidity that toxic blood levels are reachedalters the toxicity of local anesthetics. For example, when etidocaine is infusedinto human volunteers at the rate of 10 mg/ml, CNS symptoms occur when thevenous blood level reaches 3.0 µg/ml (mean dose = 236 mg). Increasing theinfusion rate to 20 mg/ml causes CNS symptoms when the venous blood level isonly 2.0 µg/ml (mean dose = 161 mg).7
Local Anesthetic ToxicityRate of Injection
● Slow rates of injection are less likely toresult in systemic toxicity
● Intermittent injections, at slow rates willlessen further the likelihood of systemictoxicity
● These two steps, in my opinion, are betterthan a test dose of local anesthetic withepinephrine as tracer
Because rapid rates of injection result in CNS excitation more quickly thanslower injections, we should use slow rates of injection when large doses of localanesthetics are administered. Intermittent and slow injections are preferred, asthey are associated with less toxicity.
Much has been said about what constitutes the ideal “test dose” for epidural localanesthetics injections, and epinephrine (5 ug/ml) is widely employed as a“tracer” to increase the heart rate if intravascular injection occurs. However thesafest approach might be to use slow and intermittent injections while monitoringthe patient for signs of CNS toxicity.
Local Anesthetic ToxicityAcid Base Status
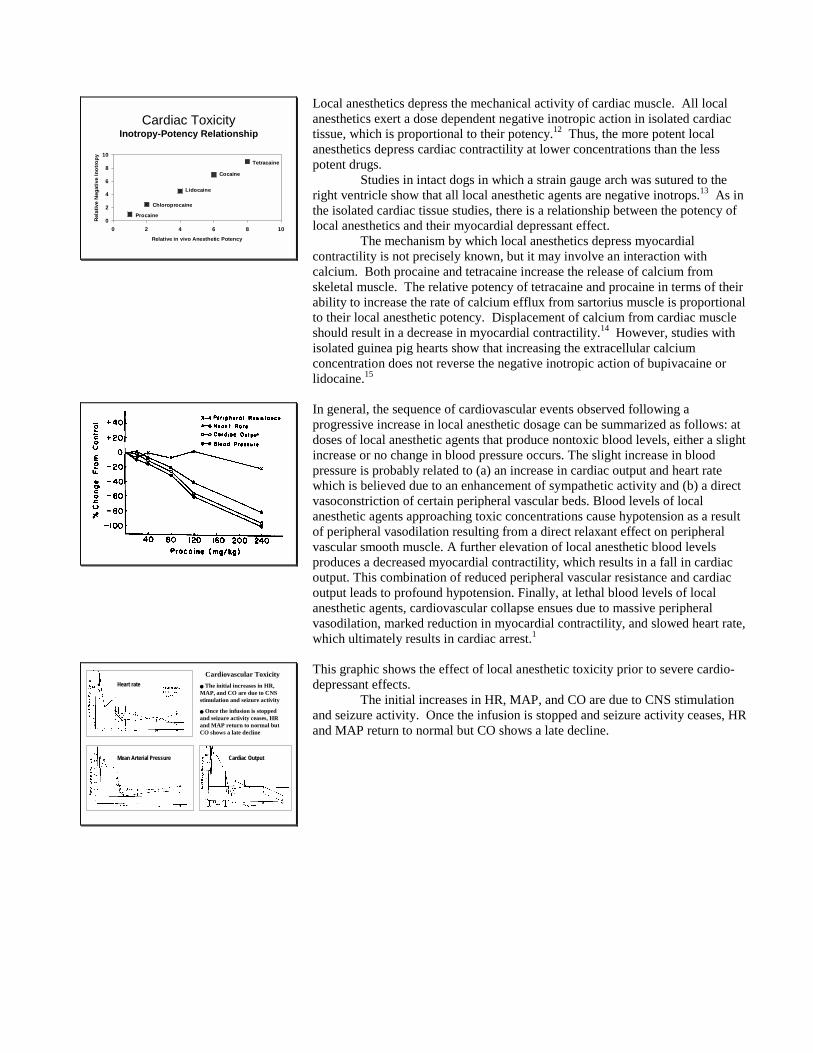
● The seizure thresholdis lowered byincreased pCO2and/or decreased pH� This is likely to occur
when local anestheticscause respiratorydepression or duringseizure activity itself
05
101520253035
SZ T
hres
hold
Proc
aine
Lido
cain
e
Bup
ivac
aine
pCO225-40pCO265-81
The acid base status effects the CNS toxicity of local anesthetic. In cats, theconvulsive threshold of various local anesthetics is related to the arterial pCO2.3For example, increasing the pCO2 from 25 - 40 torr to 65 - 81 torr decreases theconvulsive threshold of procaine, mepivacaine, prilocaine, lidocaine, andbupivacaine by approximately 50%.3 Decreasing the arterial pH also decreasesthe convulsive threshold of these agents. In fact, the pH is probably moreimportant than the pCO2 in terms of the CNS toxicity of local anesthetics.8Respiratory acidosis (increased pCO2, decreased pH) decreases the convulsivethreshold of local anesthetics. However, compensated metabolic alkalosis(increased pCO2, increased pH) does not decrease the convulsive threshold asmuch as the increased pCO2 owing to respiratory acidosis.
Local Anesthetic ToxicityAcid Base Status
● Hypercarbia� Increases cerebral
blood flow● More local anesthetic
is delivered to thebrain
� CO2 penetrates cells● Decrease intracellular
pH� Causes cation
trapping
● Hypercarbia (acidosis)� Decreases protein
binding● Brain is exposed to
more free localanesthetic
� Increases cationconcentration
● Less enters the nerves
This potentiation effect of acidosis and/or hypercarbia may be due to severalfactors. Hypercarbia increases cerebral blood flow. Therefore, more localanesthetic is delivered to the brain.9 Additionally, hypercarbia may increase thediffusion of CO2 across the nerve membrane, causing intracellular pH to fall.Intracellular acidosis promotes the conversion of the base form of the localanesthetic to the cationic (active) form. Since the cation does not diffuse acrossthe nerve membrane, ionic trapping occurs, increasing CNS toxicity of the localanesthetic.
Hypercarbia and/or acidosis also decrease the binding of localanesthetics by plasma protein.10,11 Therefore, elevating the pCO2 or decreasingthe pH increases the proportion of free drug available for diffusion into the brain.On the other hand, acidosis increases the cationic form of the local anesthetic andthis should decrease diffusion into the nerve.
Cardiac ToxicityInotropy-Potency Relationship
0
2
4
6
8
10
0 2 4 6 8 10
Relative in vivo Anesthetic Potency
Rela
tive
Neg
ativ
e In
otro
py
Procaine
Chloroprocaine
Lidocaine
Cocaine
Tetracaine
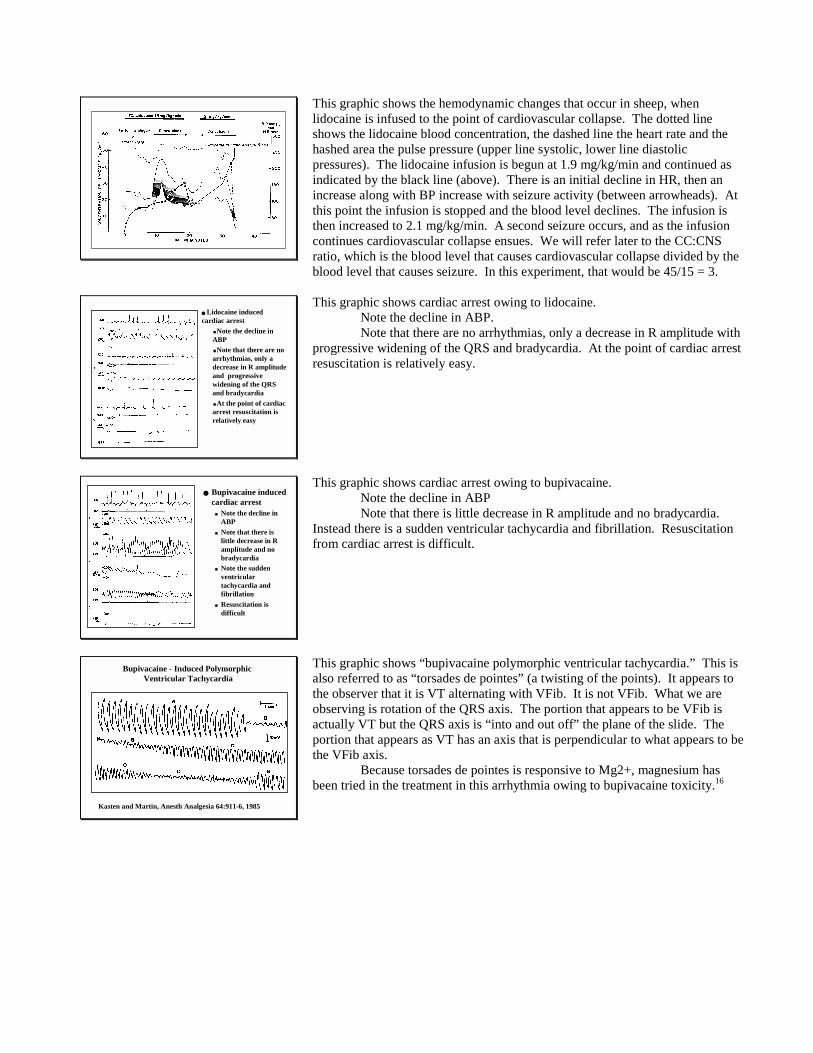
Local anesthetics depress the mechanical activity of cardiac muscle. All localanesthetics exert a dose dependent negative inotropic action in isolated cardiactissue, which is proportional to their potency.12 Thus, the more potent localanesthetics depress cardiac contractility at lower concentrations than the lesspotent drugs.
Studies in intact dogs in which a strain gauge arch was sutured to theright ventricle show that all local anesthetic agents are negative inotrops.13 As inthe isolated cardiac tissue studies, there is a relationship between the potency oflocal anesthetics and their myocardial depressant effect.
The mechanism by which local anesthetics depress myocardialcontractility is not precisely known, but it may involve an interaction withcalcium. Both procaine and tetracaine increase the release of calcium fromskeletal muscle. The relative potency of tetracaine and procaine in terms of theirability to increase the rate of calcium efflux from sartorius muscle is proportionalto their local anesthetic potency. Displacement of calcium from cardiac muscleshould result in a decrease in myocardial contractility.14 However, studies withisolated guinea pig hearts show that increasing the extracellular calciumconcentration does not reverse the negative inotropic action of bupivacaine orlidocaine.15
In general, the sequence of cardiovascular events observed following aprogressive increase in local anesthetic dosage can be summarized as follows: atdoses of local anesthetic agents that produce nontoxic blood levels, either a slightincrease or no change in blood pressure occurs. The slight increase in bloodpressure is probably related to (a) an increase in cardiac output and heart ratewhich is believed due to an enhancement of sympathetic activity and (b) a directvasoconstriction of certain peripheral vascular beds. Blood levels of localanesthetic agents approaching toxic concentrations cause hypotension as a resultof peripheral vasodilation resulting from a direct relaxant effect on peripheralvascular smooth muscle. A further elevation of local anesthetic blood levelsproduces a decreased myocardial contractility, which results in a fall in cardiacoutput. This combination of reduced peripheral vascular resistance and cardiacoutput leads to profound hypotension. Finally, at lethal blood levels of localanesthetic agents, cardiovascular collapse ensues due to massive peripheralvasodilation, marked reduction in myocardial contractility, and slowed heart rate,which ultimately results in cardiac arrest.1
Heart rate
Mean Arterial Pressure Cardiac Output
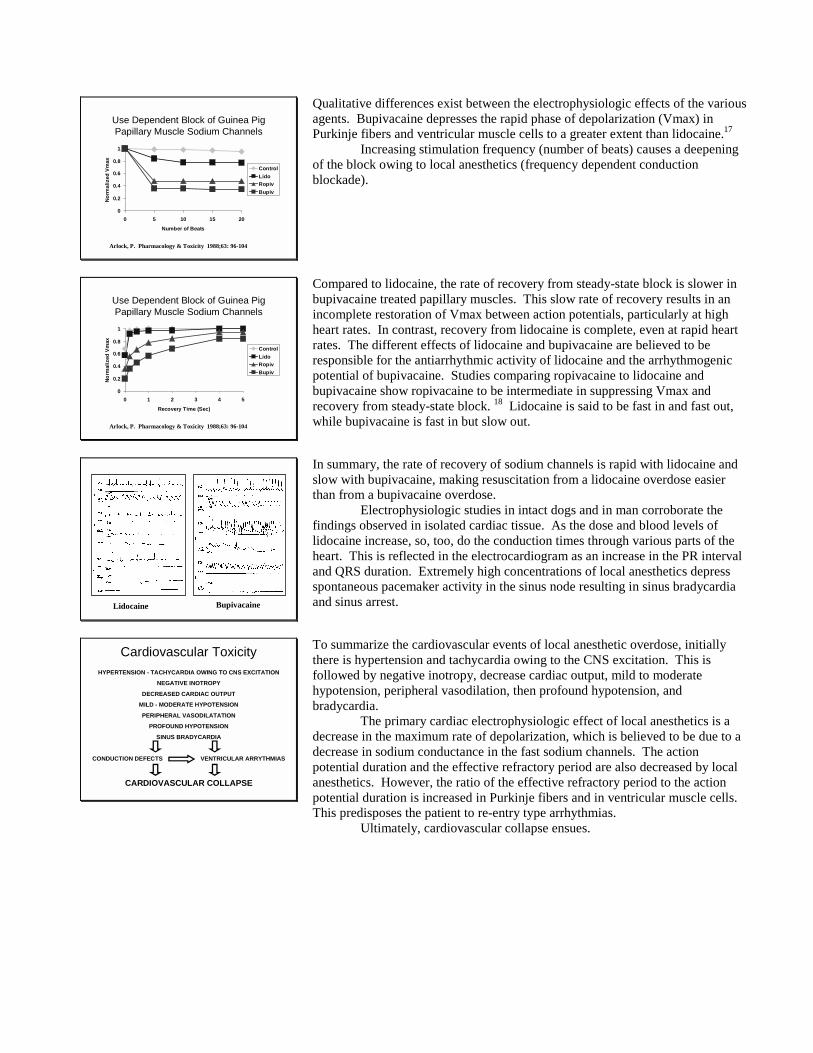
Cardiovascular Toxicity� The initial increases in HR,MAP, and CO are due to CNSstimulation and seizure activity
� Once the infusion is stoppedand seizure activity ceases, HRand MAP return to normal butCO shows a late decline
This graphic shows the effect of local anesthetic toxicity prior to severe cardio-depressant effects.
The initial increases in HR, MAP, and CO are due to CNS stimulationand seizure activity. Once the infusion is stopped and seizure activity ceases, HRand MAP return to normal but CO shows a late decline.
This graphic shows the hemodynamic changes that occur in sheep, whenlidocaine is infused to the point of cardiovascular collapse. The dotted lineshows the lidocaine blood concentration, the dashed line the heart rate and thehashed area the pulse pressure (upper line systolic, lower line diastolicpressures). The lidocaine infusion is begun at 1.9 mg/kg/min and continued asindicated by the black line (above). There is an initial decline in HR, then anincrease along with BP increase with seizure activity (between arrowheads). Atthis point the infusion is stopped and the blood level declines. The infusion isthen increased to 2.1 mg/kg/min. A second seizure occurs, and as the infusioncontinues cardiovascular collapse ensues. We will refer later to the CC:CNSratio, which is the blood level that causes cardiovascular collapse divided by theblood level that causes seizure. In this experiment, that would be 45/15 = 3.
� Lidocaine inducedcardiac arrest
�Note the decline inABP�Note that there are noarrhythmias, only adecrease in R amplitudeand progressivewidening of the QRSand bradycardia�At the point of cardiacarrest resuscitation isrelatively easy
This graphic shows cardiac arrest owing to lidocaine.Note the decline in ABP.Note that there are no arrhythmias, only a decrease in R amplitude with
progressive widening of the QRS and bradycardia. At the point of cardiac arrestresuscitation is relatively easy.
� Bupivacaine inducedcardiac arrest� Note the decline in
ABP� Note that there is
little decrease in Ramplitude and nobradycardia
� Note the suddenventriculartachycardia andfibrillation
� Resuscitation isdifficult
This graphic shows cardiac arrest owing to bupivacaine.Note the decline in ABPNote that there is little decrease in R amplitude and no bradycardia.
Instead there is a sudden ventricular tachycardia and fibrillation. Resuscitationfrom cardiac arrest is difficult.
Bupivacaine - Induced Polymorphic Ventricular Tachycardia
Kasten and Martin, Anesth Analgesia 64:911-6, 1985
This graphic shows “bupivacaine polymorphic ventricular tachycardia.” This isalso referred to as “torsades de pointes” (a twisting of the points). It appears tothe observer that it is VT alternating with VFib. It is not VFib. What we areobserving is rotation of the QRS axis. The portion that appears to be VFib isactually VT but the QRS axis is “into and out off” the plane of the slide. Theportion that appears as VT has an axis that is perpendicular to what appears to bethe VFib axis.
Because torsades de pointes is responsive to Mg2+, magnesium hasbeen tried in the treatment in this arrhythmia owing to bupivacaine toxicity.16
Use Dependent Block of Guinea PigPapillary Muscle Sodium Channels
0
0.2
0.4
0.6
0.8
1
0 5 10 15 20
Number of Beats
Norm
aliz
ed V
max
ControlLidoRopivBupiv
Arlock, P. Pharmacology & Toxicity 1988;63: 96-104
Qualitative differences exist between the electrophysiologic effects of the variousagents. Bupivacaine depresses the rapid phase of depolarization (Vmax) inPurkinje fibers and ventricular muscle cells to a greater extent than lidocaine.17
Increasing stimulation frequency (number of beats) causes a deepeningof the block owing to local anesthetics (frequency dependent conductionblockade).
Use Dependent Block of Guinea PigPapillary Muscle Sodium Channels
0
0.2
0.4
0.6
0.8
1
0 1 2 3 4 5
Recovery Time (Sec)
Norm
aliz
ed V
max
ControlLidoRopivBupiv
Arlock, P. Pharmacology & Toxicity 1988;63: 96-104
Compared to lidocaine, the rate of recovery from steady-state block is slower inbupivacaine treated papillary muscles. This slow rate of recovery results in anincomplete restoration of Vmax between action potentials, particularly at highheart rates. In contrast, recovery from lidocaine is complete, even at rapid heartrates. The different effects of lidocaine and bupivacaine are believed to beresponsible for the antiarrhythmic activity of lidocaine and the arrhythmogenicpotential of bupivacaine. Studies comparing ropivacaine to lidocaine andbupivacaine show ropivacaine to be intermediate in suppressing Vmax andrecovery from steady-state block. 18 Lidocaine is said to be fast in and fast out,while bupivacaine is fast in but slow out.
Lidocaine Bupivacaine
In summary, the rate of recovery of sodium channels is rapid with lidocaine andslow with bupivacaine, making resuscitation from a lidocaine overdose easierthan from a bupivacaine overdose.
Electrophysiologic studies in intact dogs and in man corroborate thefindings observed in isolated cardiac tissue. As the dose and blood levels oflidocaine increase, so, too, do the conduction times through various parts of theheart. This is reflected in the electrocardiogram as an increase in the PR intervaland QRS duration. Extremely high concentrations of local anesthetics depressspontaneous pacemaker activity in the sinus node resulting in sinus bradycardiaand sinus arrest.
Cardiovascular ToxicityHYPERTENSION - TACHYCARDIA OWING TO CNS EXCITATION
NEGATIVE INOTROPY
DECREASED CARDIAC OUTPUT
MILD - MODERATE HYPOTENSION
PERIPHERAL VASODILATATION
PROFOUND HYPOTENSION
SINUS BRADYCARDIA
CONDUCTION DEFECTS VENTRICULAR ARRYTHMIAS
CARDIOVASCULAR COLLAPSE
To summarize the cardiovascular events of local anesthetic overdose, initiallythere is hypertension and tachycardia owing to the CNS excitation. This isfollowed by negative inotropy, decrease cardiac output, mild to moderatehypotension, peripheral vasodilation, then profound hypotension, andbradycardia.
The primary cardiac electrophysiologic effect of local anesthetics is adecrease in the maximum rate of depolarization, which is believed to be due to adecrease in sodium conductance in the fast sodium channels. The actionpotential duration and the effective refractory period are also decreased by localanesthetics. However, the ratio of the effective refractory period to the actionpotential duration is increased in Purkinje fibers and in ventricular muscle cells.This predisposes the patient to re-entry type arrhythmias.
Ultimately, cardiovascular collapse ensues.
Cardiovascular Toxicity
In 1979, Albright reported a number of the cardiotoxic reactions owing tobupivacaine in pregnant patients.19
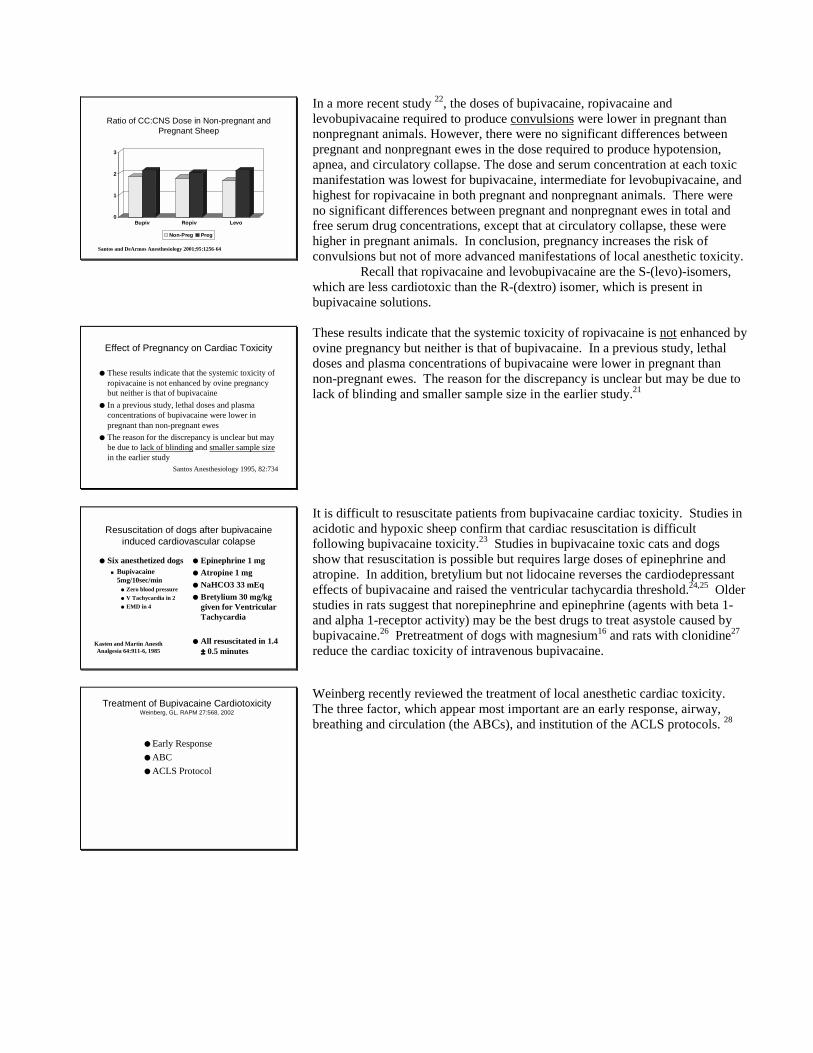
Cardiac Reactions with BupivacaineFDA Meeting - October 1983
(1973-1983)
No. Cases Dose (mg) DeathsNon OBS 14 50-360 5Obstetric0.5% 8 75-135 60.75% 27 50-180 10Subtotal 35 16Grand total 49 21
As a consequence of these reports, the FDA convened a panel of experts toreview these bupivacaine toxicity cases. There were a total of 14 non-obstetricand 35 obstetric cases (grand total of 49). Nearly half of these patients diedindicating the difficulty associated with resuscitating the patients. While somepatients received excessive doses, some patients were affected by as little as 50mg of bupivacaine. A majority of the obstetric patients received 0.75%bupivacaine. The panel was concerned that the pregnant patient may be moresusceptible to bupivacaine than non-pregnant patients. As a result, the 0.75%bupivacaine solution is not recommended for obstetric anesthesia in the U.S.A.Fortunately bupivacaine was not removed from the market.
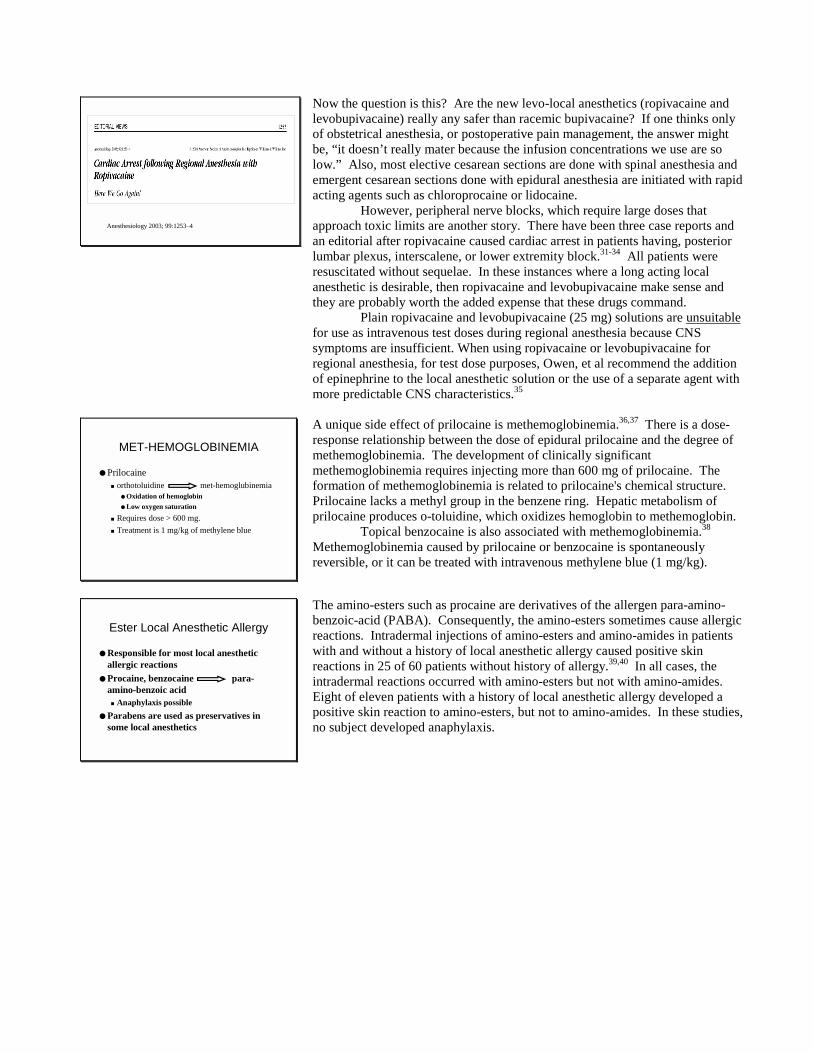
Ratio of CC:CNS Dose in Non-pregnant andPregnant Sheep
0
2
4
6
8
10
Lido Mepiv Bupiv Ropiv
Non-Preg Preg
Studies in pregnant and non-pregnant sheep show that the CC/CNS dosage ratio(see above) for bupivacaine decreases from 3.7 ± 0.5 in non-pregnant sheep to2.7 ± 0.4 in pregnant animals.20 Nevertheless, there was little difference in theCC/CNS blood level ratio, which varied from 1.6 ± 0.1 in non-pregnant animalsto 1.4 ± 0.1 in pregnant ewes. However, the blood level of bupivacaine whencirculatory collapse occurred was lower in pregnant animals.
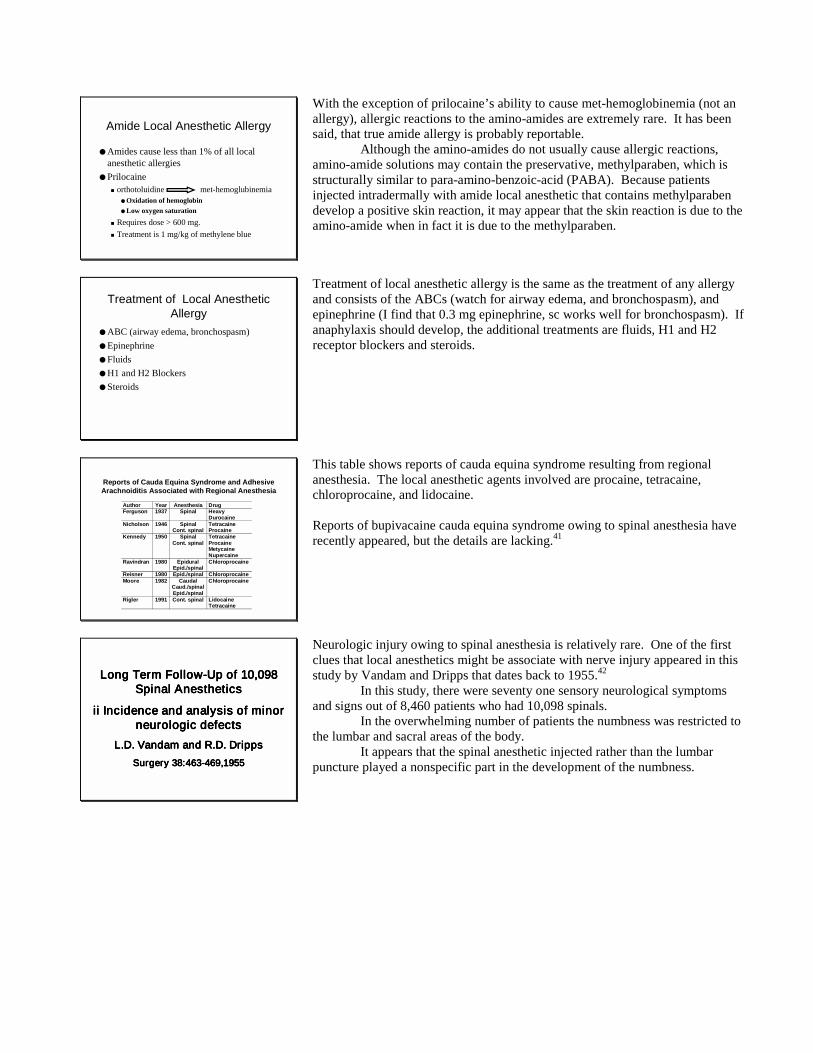
Ratio of CC:CNS Dose in Non-pregnant andPregnant Sheep
0
2
4
6
8
10
Lido Mepiv Bupiv Ropiv Bupiv ii Ropiv ii
Non-Preg Preg
When the study in the previous slide was repeated, the same group found thatpregnancy did not enhance bupivacaine's or ropivacaine's cardiotoxicity (bupiv iiand ropiv ii).21 Also, there was no difference in the myocardial uptake ofbupivacaine in pregnant and non-pregnant sheep at the time of cardiovascularcollapse. Thus, if the pregnant sheep is more susceptible to the cardiotoxiceffects of bupivacaine, it apparently is not due to myocardial uptake of drug.
Ratio of CC:CNS Dose in Non-pregnant andPregnant Sheep
0
1
2
3
Bupiv Ropiv Levo
Non-Preg Preg
Santos and DeArmos Anesthesiology 2001;95:1256-64
In a more recent study 22, the doses of bupivacaine, ropivacaine andlevobupivacaine required to produce convulsions were lower in pregnant thannonpregnant animals. However, there were no significant differences betweenpregnant and nonpregnant ewes in the dose required to produce hypotension,apnea, and circulatory collapse. The dose and serum concentration at each toxicmanifestation was lowest for bupivacaine, intermediate for levobupivacaine, andhighest for ropivacaine in both pregnant and nonpregnant animals. There wereno significant differences between pregnant and nonpregnant ewes in total andfree serum drug concentrations, except that at circulatory collapse, these werehigher in pregnant animals. In conclusion, pregnancy increases the risk ofconvulsions but not of more advanced manifestations of local anesthetic toxicity.
Recall that ropivacaine and levobupivacaine are the S-(levo)-isomers,which are less cardiotoxic than the R-(dextro) isomer, which is present inbupivacaine solutions.
Effect of Pregnancy on Cardiac Toxicity
● These results indicate that the systemic toxicity ofropivacaine is not enhanced by ovine pregnancybut neither is that of bupivacaine
● In a previous study, lethal doses and plasmaconcentrations of bupivacaine were lower inpregnant than non-pregnant ewes
● The reason for the discrepancy is unclear but maybe due to lack of blinding and smaller sample sizein the earlier study
Santos Anesthesiology 1995, 82:734
These results indicate that the systemic toxicity of ropivacaine is not enhanced byovine pregnancy but neither is that of bupivacaine. In a previous study, lethaldoses and plasma concentrations of bupivacaine were lower in pregnant thannon-pregnant ewes. The reason for the discrepancy is unclear but may be due tolack of blinding and smaller sample size in the earlier study.21
Resuscitation of dogs after bupivacaineinduced cardiovascular colapse
● Six anesthetized dogs� Bupivacaine
5mg/10sec/min● Zero blood pressure● V Tachycardia in 2● EMD in 4
● Epinephrine 1 mg● Atropine 1 mg● NaHCO3 33 mEq● Bretylium 30 mg/kg
given for VentricularTachycardia
● All resuscitated in 1.4±±±± 0.5 minutes
Kasten and Martin AnesthAnalgesia 64:911-6, 1985
It is difficult to resuscitate patients from bupivacaine cardiac toxicity. Studies inacidotic and hypoxic sheep confirm that cardiac resuscitation is difficultfollowing bupivacaine toxicity.23 Studies in bupivacaine toxic cats and dogsshow that resuscitation is possible but requires large doses of epinephrine andatropine. In addition, bretylium but not lidocaine reverses the cardiodepressanteffects of bupivacaine and raised the ventricular tachycardia threshold.24,25 Olderstudies in rats suggest that norepinephrine and epinephrine (agents with beta 1-and alpha 1-receptor activity) may be the best drugs to treat asystole caused bybupivacaine.26 Pretreatment of dogs with magnesium16 and rats with clonidine27
reduce the cardiac toxicity of intravenous bupivacaine.
Treatment of Bupivacaine CardiotoxicityWeinberg, GL. RAPM 27:568, 2002
● Early Response● ABC● ACLS Protocol
Weinberg recently reviewed the treatment of local anesthetic cardiac toxicity.The three factor, which appear most important are an early response, airway,breathing and circulation (the ABCs), and institution of the ACLS protocols. 28

Treatment of Bupivacaine Cardiotoxicity ii
● Antiarrhytmic therapy� Benzodiazepines or propofol for seizures and
CNS induced arrhythmias� Epinephrine may promote arrhythmias� Amiodarone [now first line ACLS
antiarrhythmic] may be useful� Lidocaine may compete with bupivacaine or
could be additive (data are mixed)
In his review, Weinberg suggests using amiodarone, instead of bretylium (whichis no longer supported as an effective ACLS agent), and he points out thatepinephrine may itself be arrhythmogenic. 28
It seems logical (watch out for backfiring logic) and some havesuggested that lidocaine (by competition for the sodium channel) might beeffective in the treatment of bupivacaine arrhythmias. On the other hand,lidocaine could be additive to the toxic effects of bupivacaine. The data aremixed on this use of lidocaine.
Treatment of Bupivacaine Cardiotoxicity iii
● Vasopressor support� Epinephrine� Vasopressin 40 U now in ACLS protocol
● May be less arrhythmogenic than epinephrine
● Contraindications� Calcium channel blockers� Phenytoin� Bretyllium no longer supported
For vasopressor support, vasopressin 40 U, which is now in the ACLS protocolmay be preferable to epinephrine because epinephrine itself can causearrhythmias.
Drugs which are contraindicated include:Calcium channel blockersPhenytoinBretylium
Treatment of Bupivacaine Cardiotoxicity iv
● Novel therapies� Lipid infusion (soybean oil)
● Bupivacaine inhibits transport of fatty acids intomitochondria
● Provides substrate● Improves survival and increase dose required for
toxicity in rats● Sequesters lipid soluble bupivacaine in blood
� Insulin/Glucose/Potassium● May restore K+ gradients for repolarization● May promote ATP source
Other methods for resuscitation include lipid infusions (including propofol) orinsulin/glucose/potassium (I/G/K) infusion and these are currently underinvestigation.29,30
Lipid infusion provides mitochondrial substrate, improves survival andincrease the dose required for toxicity in rats. The lipids may sequester thehighly lipid soluble bupivacaine in blood, making less bupivacaine available toinhibit the cardiovascular system.
I/G/K may restore K+ gradients for repolarization and help restore ATPstores.
Anesthesiology 2003; 99:1253–4
Now the question is this? Are the new levo-local anesthetics (ropivacaine andlevobupivacaine) really any safer than racemic bupivacaine? If one thinks onlyof obstetrical anesthesia, or postoperative pain management, the answer mightbe, “it doesn’t really mater because the infusion concentrations we use are solow.” Also, most elective cesarean sections are done with spinal anesthesia andemergent cesarean sections done with epidural anesthesia are initiated with rapidacting agents such as chloroprocaine or lidocaine.
However, peripheral nerve blocks, which require large doses thatapproach toxic limits are another story. There have been three case reports andan editorial after ropivacaine caused cardiac arrest in patients having, posteriorlumbar plexus, interscalene, or lower extremity block.31-34 All patients wereresuscitated without sequelae. In these instances where a long acting localanesthetic is desirable, then ropivacaine and levobupivacaine make sense andthey are probably worth the added expense that these drugs command.
Plain ropivacaine and levobupivacaine (25 mg) solutions are unsuitablefor use as intravenous test doses during regional anesthesia because CNSsymptoms are insufficient. When using ropivacaine or levobupivacaine forregional anesthesia, for test dose purposes, Owen, et al recommend the additionof epinephrine to the local anesthetic solution or the use of a separate agent withmore predictable CNS characteristics.35
MET-HEMOGLOBINEMIA
● Prilocaine� orthotoluidine met-hemoglubinemia
● Oxidation of hemoglobin● Low oxygen saturation
� Requires dose > 600 mg.� Treatment is 1 mg/kg of methylene blue
A unique side effect of prilocaine is methemoglobinemia.36,37 There is a dose-response relationship between the dose of epidural prilocaine and the degree ofmethemoglobinemia. The development of clinically significantmethemoglobinemia requires injecting more than 600 mg of prilocaine. Theformation of methemoglobinemia is related to prilocaine's chemical structure.Prilocaine lacks a methyl group in the benzene ring. Hepatic metabolism ofprilocaine produces o-toluidine, which oxidizes hemoglobin to methemoglobin.
Topical benzocaine is also associated with methemoglobinemia.38
Methemoglobinemia caused by prilocaine or benzocaine is spontaneouslyreversible, or it can be treated with intravenous methylene blue (1 mg/kg).
Ester Local Anesthetic Allergy
● Responsible for most local anestheticallergic reactions
● Procaine, benzocaine para-amino-benzoic acid� Anaphylaxis possible
● Parabens are used as preservatives insome local anesthetics
The amino-esters such as procaine are derivatives of the allergen para-amino-benzoic-acid (PABA). Consequently, the amino-esters sometimes cause allergicreactions. Intradermal injections of amino-esters and amino-amides in patientswith and without a history of local anesthetic allergy caused positive skinreactions in 25 of 60 patients without history of allergy.39,40 In all cases, theintradermal reactions occurred with amino-esters but not with amino-amides.Eight of eleven patients with a history of local anesthetic allergy developed apositive skin reaction to amino-esters, but not to amino-amides. In these studies,no subject developed anaphylaxis.
Amide Local Anesthetic Allergy
● Amides cause less than 1% of all localanesthetic allergies
● Prilocaine� orthotoluidine met-hemoglubinemia
● Oxidation of hemoglobin● Low oxygen saturation
� Requires dose > 600 mg.� Treatment is 1 mg/kg of methylene blue
With the exception of prilocaine’s ability to cause met-hemoglobinemia (not anallergy), allergic reactions to the amino-amides are extremely rare. It has beensaid, that true amide allergy is probably reportable.
Although the amino-amides do not usually cause allergic reactions,amino-amide solutions may contain the preservative, methylparaben, which isstructurally similar to para-amino-benzoic-acid (PABA). Because patientsinjected intradermally with amide local anesthetic that contains methylparabendevelop a positive skin reaction, it may appear that the skin reaction is due to theamino-amide when in fact it is due to the methylparaben.
Treatment of Local AnestheticAllergy
● ABC (airway edema, bronchospasm)● Epinephrine● Fluids● H1 and H2 Blockers● Steroids
Treatment of local anesthetic allergy is the same as the treatment of any allergyand consists of the ABCs (watch for airway edema, and bronchospasm), andepinephrine (I find that 0.3 mg epinephrine, sc works well for bronchospasm). Ifanaphylaxis should develop, the additional treatments are fluids, H1 and H2receptor blockers and steroids.
Reports of Cauda Equina Syndrome and AdhesiveArachnoiditis Associated with Regional Anesthesia
Author Year Anesthesia DrugFerguson 1937 Spinal Heavy
DurocaineNicholson 1946 Spinal
Cont. spinalTetracaineProcaine
Kennedy 1950 SpinalCont. spinal
TetracaineProcaineMetycaineNupercaine
Ravindran 1980 EpiduralEpid./spinal
Chloroprocaine
Reisner 1980 Epid./spinal ChloroprocaineMoore 1982 Caudal
Caud./spinalEpid./spinal
Chloroprocaine
Rigler 1991 Cont. spinal LidocaineTetracaine
This table shows reports of cauda equina syndrome resulting from regionalanesthesia. The local anesthetic agents involved are procaine, tetracaine,chloroprocaine, and lidocaine.
Reports of bupivacaine cauda equina syndrome owing to spinal anesthesia haverecently appeared, but the details are lacking.41
Lo ng Term Fo llo w -Up o f 10,098Lo ng Term Fo llo w -Up o f 10,098Lo ng Term Fo llo w -Up o f 10,098Lo ng Term Fo llo w -Up o f 10,098Spinal Ane s the tic sSpinal Ane s the tic sSpinal Ane s the tic sSpinal Ane s the tic s
ii Incidence and analy s is o f m ino rii Incidence and analy s is o f m ino rii Incidence and analy s is o f m ino rii Incidence and analy s is o f m ino rneuro lo g icneuro lo g icneuro lo g icneuro lo g ic de fects de fects de fects de fects
L.D. L.D. L.D. L.D. Vandam Vandam Vandam Vandam and R.D. and R.D. and R.D. and R.D. DrippsDrippsDrippsDrippsSurg ery 38:463-469,1955Surg ery 38:463-469,1955Surg ery 38:463-469,1955Surg ery 38:463-469,1955
Neurologic injury owing to spinal anesthesia is relatively rare. One of the firstclues that local anesthetics might be associate with nerve injury appeared in thisstudy by Vandam and Dripps that dates back to 1955.42
In this study, there were seventy one sensory neurological symptomsand signs out of 8,460 patients who had 10,098 spinals.
In the overwhelming number of patients the numbness was restricted tothe lumbar and sacral areas of the body.
It appears that the spinal anesthetic injected rather than the lumbarpuncture played a nonspecific part in the development of the numbness.
Reis nerReis nerReis nerReis ner, e t al, e t al, e t al, e t al
Pers is tent Pers is tent Pers is tent Pers is tent Neuro lo g ic Neuro lo g ic Neuro lo g ic Neuro lo g ic Deficit andDeficit andDeficit andDeficit andAdhes iv e Adhes iv e Adhes iv e Adhes iv e Arachno iditis Arachno iditis Arachno iditis Arachno iditis Fo llo w ingFo llo w ingFo llo w ingFo llo w ing
Intrathecal Intrathecal Intrathecal Intrathecal 2-C h lo ro pro caine Injectio n2-C h lo ro pro caine Injectio n2-C h lo ro pro caine Injectio n2-C h lo ro pro caine Injectio n
Rav indranRav indranRav indranRav indran , e t al, e t al, e t al, e t al
Pro lo ng ed Neural Blo ckade fo llo w ingPro lo ng ed Neural Blo ckade fo llo w ingPro lo ng ed Neural Blo ckade fo llo w ingPro lo ng ed Neural Blo ckade fo llo w ingReg io nal Analg e s ia w ith 2-Reg io nal Analg e s ia w ith 2-Reg io nal Analg e s ia w ith 2-Reg io nal Analg e s ia w ith 2-
C h lo ro pro caineC h lo ro pro caineC h lo ro pro caineC h lo ro pro caine
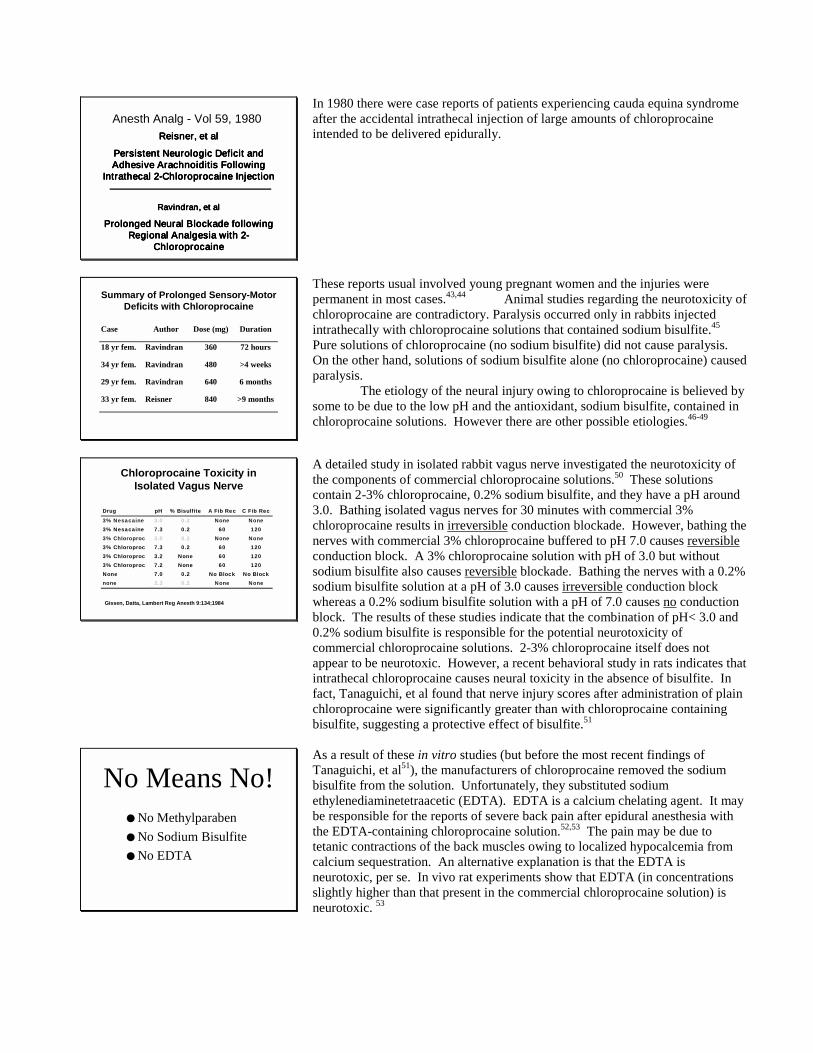
Anesth Analg - Vol 59, 1980In 1980 there were case reports of patients experiencing cauda equina syndromeafter the accidental intrathecal injection of large amounts of chloroprocaineintended to be delivered epidurally.
Summary of Prolonged Sensory-MotorDeficits with Chloroprocaine
Case Author Dose (mg) Duration
18 yr fem. Ravindran 360 72 hours
34 yr fem. Ravindran 480 >4 weeks
29 yr fem. Ravindran 640 6 months
33 yr fem. Reisner 840 >9 months
These reports usual involved young pregnant women and the injuries werepermanent in most cases.43,44 Animal studies regarding the neurotoxicity ofchloroprocaine are contradictory. Paralysis occurred only in rabbits injectedintrathecally with chloroprocaine solutions that contained sodium bisulfite.45
Pure solutions of chloroprocaine (no sodium bisulfite) did not cause paralysis.On the other hand, solutions of sodium bisulfite alone (no chloroprocaine) causedparalysis.
The etiology of the neural injury owing to chloroprocaine is believed bysome to be due to the low pH and the antioxidant, sodium bisulfite, contained inchloroprocaine solutions. However there are other possible etiologies.46-49
Chloroprocaine Toxicity inIsolated Vagus Nerve
Drug pH % Bisulfite A Fib Rec C Fib Rec
3% Nesacaine 3.0 0.2 None None3% Nesacaine 7.3 0.2 60 1203% Chloroproc 3.0 0.2 None None3% Chloroproc 7.3 0.2 60 1203% Chloroproc 3.2 None 60 1203% Chloroproc 7.2 None 60 120None 7.0 0.2 No Block No Blocknone 3.3 0.2 None None
Gissen, Datta, Lambert Reg Anesth 9:134;1984
A detailed study in isolated rabbit vagus nerve investigated the neurotoxicity ofthe components of commercial chloroprocaine solutions.50 These solutionscontain 2-3% chloroprocaine, 0.2% sodium bisulfite, and they have a pH around3.0. Bathing isolated vagus nerves for 30 minutes with commercial 3%chloroprocaine results in irreversible conduction blockade. However, bathing thenerves with commercial 3% chloroprocaine buffered to pH 7.0 causes reversibleconduction block. A 3% chloroprocaine solution with pH of 3.0 but withoutsodium bisulfite also causes reversible blockade. Bathing the nerves with a 0.2%sodium bisulfite solution at a pH of 3.0 causes irreversible conduction blockwhereas a 0.2% sodium bisulfite solution with a pH of 7.0 causes no conductionblock. The results of these studies indicate that the combination of pH< 3.0 and0.2% sodium bisulfite is responsible for the potential neurotoxicity ofcommercial chloroprocaine solutions. 2-3% chloroprocaine itself does notappear to be neurotoxic. However, a recent behavioral study in rats indicates thatintrathecal chloroprocaine causes neural toxicity in the absence of bisulfite. Infact, Tanaguichi, et al found that nerve injury scores after administration of plainchloroprocaine were significantly greater than with chloroprocaine containingbisulfite, suggesting a protective effect of bisulfite.51
No Means No!● No Methylparaben● No Sodium Bisulfite● No EDTA
As a result of these in vitro studies (but before the most recent findings ofTanaguichi, et al51), the manufacturers of chloroprocaine removed the sodiumbisulfite from the solution. Unfortunately, they substituted sodiumethylenediaminetetraacetic (EDTA). EDTA is a calcium chelating agent. It maybe responsible for the reports of severe back pain after epidural anesthesia withthe EDTA-containing chloroprocaine solution.52,53 The pain may be due totetanic contractions of the back muscles owing to localized hypocalcemia fromcalcium sequestration. An alternative explanation is that the EDTA isneurotoxic, per se. In vivo rat experiments show that EDTA (in concentrationsslightly higher than that present in the commercial chloroprocaine solution) isneurotoxic. 53
Tissue ToxicityCauda Equina Syndrome afterContinuous Spinal Anesthesia
Rigler ML, Drasner K, Krejcie TC, et alAnesthesia Analgesia 72:275-281;1991
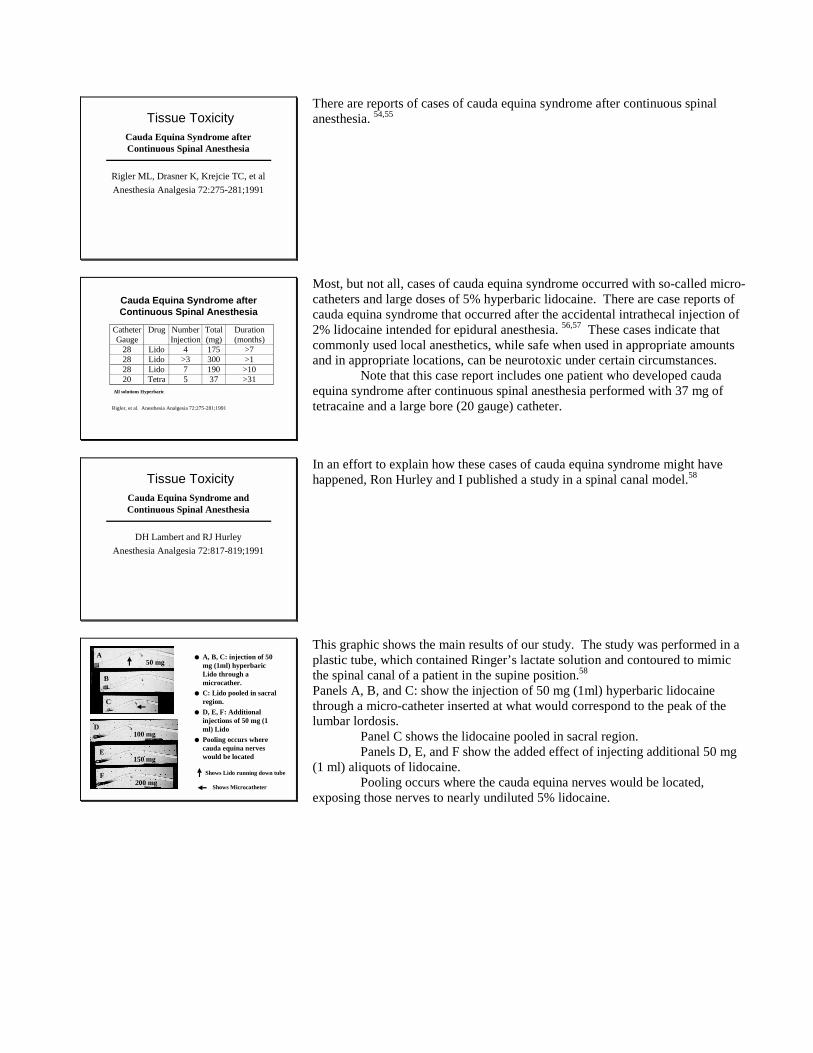
There are reports of cases of cauda equina syndrome after continuous spinalanesthesia. 54,55
Cauda Equina Syndrome afterContinuous Spinal Anesthesia
CatheterGauge
Drug NumberInjection
Total(mg)
Duration(months)
28 Lido 4 175 >728 Lido >3 300 >128 Lido 7 190 >1020 Tetra 5 37 >31
All solutions Hyperbaric
Rigler, et al. Anesthesia Analgesia 72:275-281;1991
Most, but not all, cases of cauda equina syndrome occurred with so-called micro-catheters and large doses of 5% hyperbaric lidocaine. There are case reports ofcauda equina syndrome that occurred after the accidental intrathecal injection of2% lidocaine intended for epidural anesthesia. 56,57 These cases indicate thatcommonly used local anesthetics, while safe when used in appropriate amountsand in appropriate locations, can be neurotoxic under certain circumstances.
Note that this case report includes one patient who developed caudaequina syndrome after continuous spinal anesthesia performed with 37 mg oftetracaine and a large bore (20 gauge) catheter.
Tissue ToxicityCauda Equina Syndrome andContinuous Spinal Anesthesia
DH Lambert and RJ HurleyAnesthesia Analgesia 72:817-819;1991
In an effort to explain how these cases of cauda equina syndrome might havehappened, Ron Hurley and I published a study in a spinal canal model.58
● A, B, C: injection of 50mg (1ml) hyperbaricLido through amicrocather.
● C: Lido pooled in sacralregion.
● D, E, F: Additionalinjections of 50 mg (1ml) Lido
● Pooling occurs wherecauda equina nerveswould be located
50 mgA
B
C
D100 mg
150 mg
200 mgF
E
Shows Lido running down tube
Shows Microcatheter
This graphic shows the main results of our study. The study was performed in aplastic tube, which contained Ringer’s lactate solution and contoured to mimicthe spinal canal of a patient in the supine position.58
Panels A, B, and C: show the injection of 50 mg (1ml) hyperbaric lidocainethrough a micro-catheter inserted at what would correspond to the peak of thelumbar lordosis.
Panel C shows the lidocaine pooled in sacral region.Panels D, E, and F show the added effect of injecting additional 50 mg
(1 ml) aliquots of lidocaine.Pooling occurs where the cauda equina nerves would be located,
exposing those nerves to nearly undiluted 5% lidocaine.
Cauda Equina Syndrome andContinuous Spinal Anesthesia
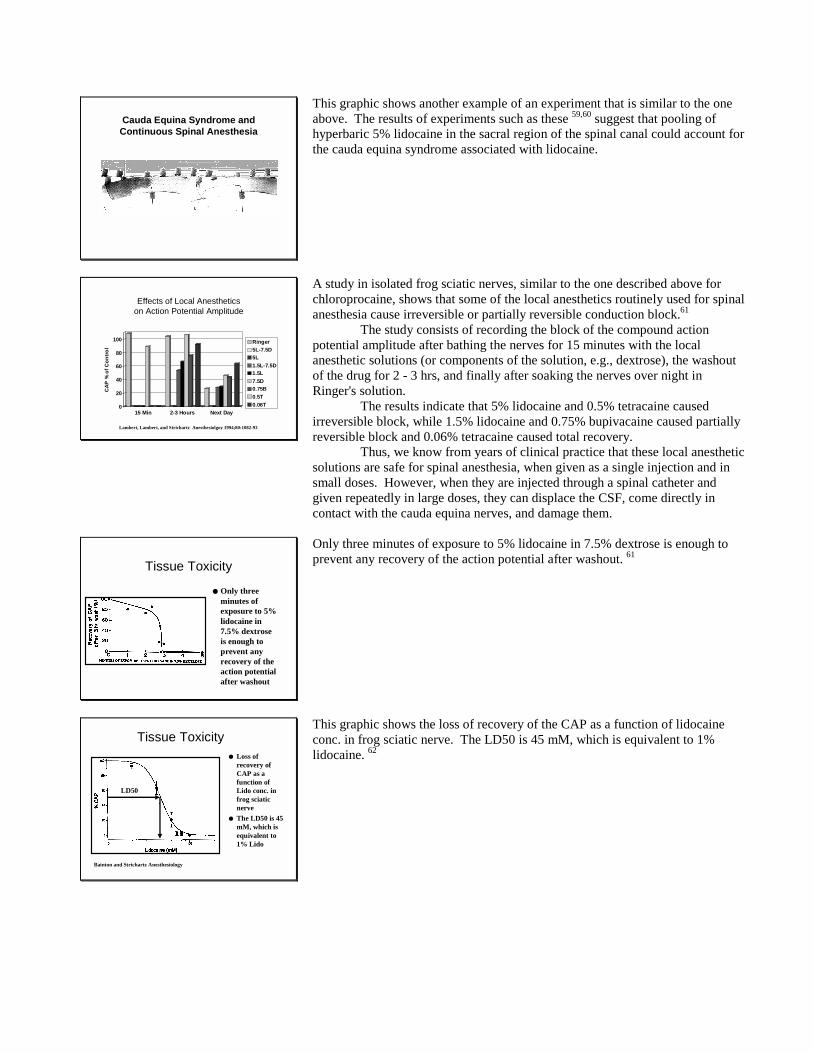
This graphic shows another example of an experiment that is similar to the oneabove. The results of experiments such as these 59,60 suggest that pooling ofhyperbaric 5% lidocaine in the sacral region of the spinal canal could account forthe cauda equina syndrome associated with lidocaine.
Effects of Local Anestheticson Action Potential Amplitude
0
20
40
60
80
100
CAP
% o
f Con
trol
15 Min 2-3 Hours Next Day
Ringer5L-7.5D5L1.5L-7.5D1.5L7.5D0.75B0.5T0.06T
Lambert, Lambert, and Strichartz Anesthesiolgoy 1994;80:1082-93
A study in isolated frog sciatic nerves, similar to the one described above forchloroprocaine, shows that some of the local anesthetics routinely used for spinalanesthesia cause irreversible or partially reversible conduction block.61
The study consists of recording the block of the compound actionpotential amplitude after bathing the nerves for 15 minutes with the localanesthetic solutions (or components of the solution, e.g., dextrose), the washoutof the drug for 2 - 3 hrs, and finally after soaking the nerves over night inRinger's solution.
The results indicate that 5% lidocaine and 0.5% tetracaine causedirreversible block, while 1.5% lidocaine and 0.75% bupivacaine caused partiallyreversible block and 0.06% tetracaine caused total recovery.
Thus, we know from years of clinical practice that these local anestheticsolutions are safe for spinal anesthesia, when given as a single injection and insmall doses. However, when they are injected through a spinal catheter andgiven repeatedly in large doses, they can displace the CSF, come directly incontact with the cauda equina nerves, and damage them.
Tissue Toxicity
● Only threeminutes ofexposure to 5%lidocaine in7.5% dextroseis enough toprevent anyrecovery of theaction potentialafter washout
Only three minutes of exposure to 5% lidocaine in 7.5% dextrose is enough toprevent any recovery of the action potential after washout. 61
Tissue Toxicity● Loss of
recovery ofCAP as afunction ofLido conc. infrog sciaticnerve
● The LD50 is 45mM, which isequivalent to1% Lido
LD50
Bainton and Strichartz Anesthesiology
This graphic shows the loss of recovery of the CAP as a function of lidocaineconc. in frog sciatic nerve. The LD50 is 45 mM, which is equivalent to 1%lidocaine. 62
Irreversible Conduction Block in MammalianNerve by 2% and 5% Lidocaine
0
20
40
60
80
100
CAP
- %
of C
ontr
ol
Rem
aini
ng
Day 2 Day 3
A-Control2% A Fibers5% A FibersC-Control2% C Fibers5% C Fibers
Strichartz, et al RAPM 1994;19S;21
The results obtained in frog sciatic nerve have been criticized because they wereobtained in a non-mammalian preparation. However, similar results wereobtained in mammalian (rabbit) vagus nerves.63
Sakura, et al using a rat intrathecal infusion behavioral model also obtainedresults similar to those gained in frog nerve.
Do Local Anesthetics Currently Used for SpinalAnesthesia Differ in Nerotoxic Potential?
-20
0
20
40
60
80
100
Perc
ent M
axim
um
Poss
ible
Effe
ct
1 2 3Infusion
LIDOBUPIVTETRASALINE
Sakura et al ASA Abstract 1993;79:A880
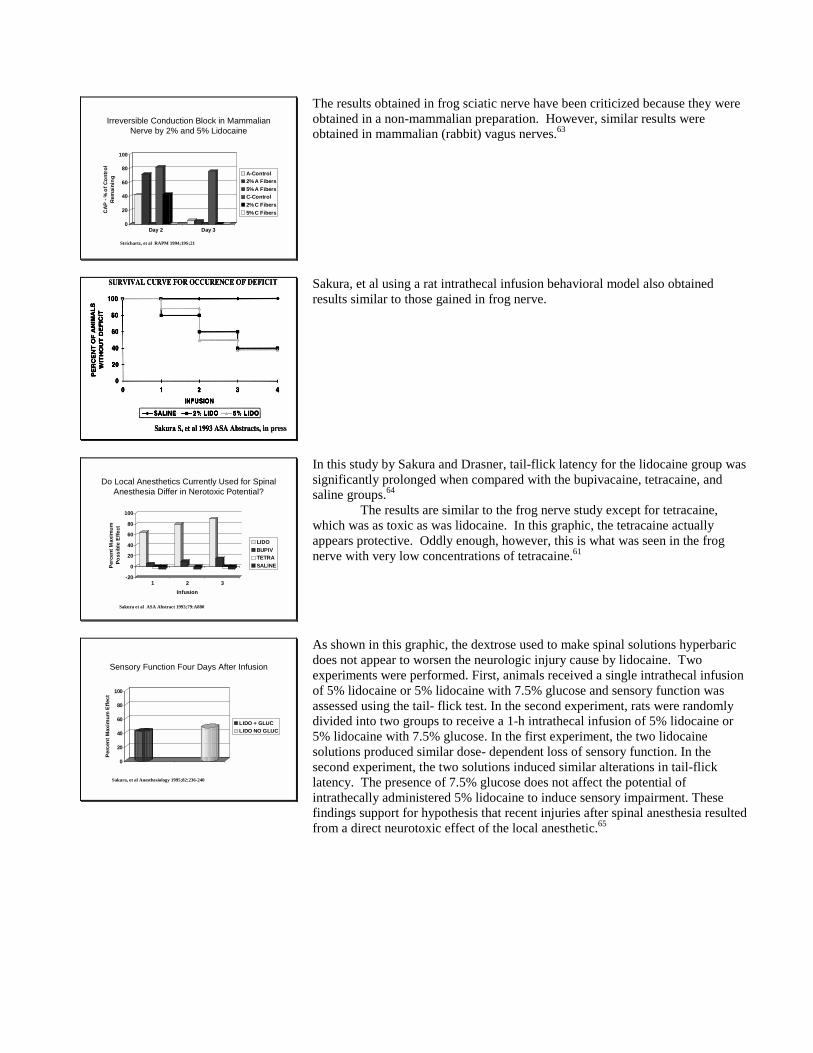
In this study by Sakura and Drasner, tail-flick latency for the lidocaine group wassignificantly prolonged when compared with the bupivacaine, tetracaine, andsaline groups.64
The results are similar to the frog nerve study except for tetracaine,which was as toxic as was lidocaine. In this graphic, the tetracaine actuallyappears protective. Oddly enough, however, this is what was seen in the frognerve with very low concentrations of tetracaine.61
Sensory Function Four Days After Infusion
0
20
40
60
80
100
Perc
ent M
axim
um E
ffect
LIDO + GLUCLIDO NO GLUC
Sakura, et al Anesthesiology 1995;82:236-240
As shown in this graphic, the dextrose used to make spinal solutions hyperbaricdoes not appear to worsen the neurologic injury cause by lidocaine. Twoexperiments were performed. First, animals received a single intrathecal infusionof 5% lidocaine or 5% lidocaine with 7.5% glucose and sensory function wasassessed using the tail- flick test. In the second experiment, rats were randomlydivided into two groups to receive a 1-h intrathecal infusion of 5% lidocaine or5% lidocaine with 7.5% glucose. In the first experiment, the two lidocainesolutions produced similar dose- dependent loss of sensory function. In thesecond experiment, the two solutions induced similar alterations in tail-flicklatency. The presence of 7.5% glucose does not affect the potential ofintrathecally administered 5% lidocaine to induce sensory impairment. Thesefindings support for hypothesis that recent injuries after spinal anesthesia resultedfrom a direct neurotoxic effect of the local anesthetic.65
References
1. Covino BG, Vassallo H: Local anesthetics: mechanisms of action and clinical use. NewYork, Grune and Stratton, 1976
2. Onizuka S, Kasaba T, Hamakawa T, Takasaki M: Lidocaine excites both pre- andpostsynaptic neurons of reconstructed respiratory pattern generator in Lymnaea stagnalis. Anesth Analg2005; 100: 175-82
3. Englesson S: The influence of acid-base changes on central nervous system toxicity oflocal anaesthetic agents. I. An experimental study in cats. Acta Anaesthesiol Scand 1974; 18: 79-87
4. Liu PL, Feldman HS, Giasi R, Patterson MK, Covino BG: Comparative CNS toxicity oflidocaine, etidocaine, bupivacaine, and tetracaine in awake dogs following rapid intravenousadministration. Anesth Analg 1983; 62: 375-9
5. Scott DB: Evaluation of the toxicity of local anaesthetic agents in man. Br J Anaesth1975; 47: 56-61
6. Scott DB, Lee A, Fagan D, Bowler GM, Bloomfield P, Lundh R: Acute toxicity ofropivacaine compared with that of bupivacaine. Anesth Analg 1989; 69: 563-9
7. Scott DB: Toxicity caused by local anaesthetic drugs [editorial]. Br J Anaesth 1981; 53:553-4
8. Jong RHd, Wagman IH, Prince DA: Effect of carbon dioxide on the cortical seizurethreshold to lidocaine. Exp Neurol 1967; 17: 221-32
9. Sakabe T, Maekawa T, Ishikawa T, Takeshita H: The effects of lidocaine on caninecerebral metabolism and circulation related to the electroencephalogram. Anesthesiology 1974; 40: 433-41
10. Burney RG, DiFazio CA, Foster JA: Effects of pH on protein binding of lidocaine.Anesth Analg 1978; 57: 478-80
11. Apfelbaum JL, Shaw LM, Gross JB, Caldwell CB, Spaulding BC: Modification oflidocaine protein binding with CO2. Can Anaesth Soc J 1985; 32: 468-71
12. Block A, Covino BG: Effect of local anesthetic agents on cardiac conduction andcontractility. Regional Anesthesia 1982; 6: 55-61
13. Stewart DM, Rogers WP, Mahaffrey JE, Witherspoon S, Woods EF: Effect of localanesthetics on the cardiovascular system in the dog. Anesthesiology 1963; 24: 620-624
14. Kuperman AS, Altura BT, Chezar JA: Action of procaine on calcium efflux from frognerve and muscle. Nature 1968; 217: 673-5
15. Tanz RD, Heskett T, Loehning RW, Fairfax CA: Comparative cardiotoxicity ofbupivacaine and lidocaine in the isolated perfused mammalian heart. Anesth Analg 1984; 63: 549-56
16. Solomon D, Bunegin L, Albin M: The effect of magnesium sulfate administration oncerebral and cardiac toxicity of bupivacaine in dogs. Anesthesiology 1990; 72: 341-6
17. Clarkson CW, Hondeghem LM: Mechanism for bupivacaine depression of cardiacconduction: fast block of sodium channels during the action potential with slow recovery from block duringdiastole. Anesthesiology 1985; 62: 396-405
18. Arlock P: Actions of three local anaesthetics: lidocaine, bupivacaine and ropivacaine onguinea pig papillary muscle sodium channels (Vmax). Pharmacol Toxicol 1988; 63: 96-104
19. Albright G: Cardiac arrest following regional anesthesia with etidocaine or bupivacaine.Anesthesiology 1979; 51: 285-286
20. Morishima HO, Pedersen H, Finster M, Hiraoka H, Tsuji A, Feldman HS, Arthur GR,Covino BG: Bupivacaine toxicity in pregnant and nonpregnant ewes. Anesthesiology 1985; 63: 134-9
21. Santos AC, Arthur GR, Wlody D, De Armas P, Morishima HO, Finster M: Comparativesystemic toxicity of ropivacaine and bupivacaine in nonpregnant and pregnant ewes. Anesthesiology 1995;82: 734-40; discussion 27A
22. Santos AC, DeArmas PI: Systemic toxicity of levobupivacaine, bupivacaine, andropivacaine during continuous intravenous infusion to nonpregnant and pregnant ewes. Anesthesiology2001; 95: 1256-64
23. Covino B: Toxicity of local anesthetics. Adv Anesth 1986; 3: 3724. Kasten GW, Martin ST: Bupivacaine cardiovascular toxicity: comparison of treatment
with bretylium and lidocaine. Anesth Analg 1985; 64: 911-6
25. Chadwick HS: Toxicity and resuscitation in lidocaine- or bupivacaine-infused cats.Anesthesiology 1985; 63: 385-90
26. Heavner JE, Pitkanen MT, Shi B, Rosenberg PH: Resuscitation from bupivacaine-induced asystole in rats: comparison of different cardioactive drugs. Anesth Analg 1995; 80: 1134-9
27. De Kock M, Le Polain B, Henin D, Vandewalle F, Scholtes JL: Clonidine pretreatmentreduces the systemic toxicity of intravenous bupivacaine in rats. Anesthesiology 1993; 79: 282-9;discussion 22A
28. Weinberg GL: Current concepts in resuscitation of patients with local anesthetic cardiactoxicity. Reg Anesth Pain Med 2002; 27: 568-75
29. Weinberg G, Ripper R, Feinstein DL, Hoffman W: Lipid emulsion infusion rescues dogsfrom bupivacaine-induced cardiac toxicity. Reg Anesth Pain Med 2003; 28: 198-202
30. Weinberg G, VadeBoncouer T: Improved energetics may explain the favorable effect ofinsulin infusion on bupivacaine cardiotoxicity. Anesth Analg 2001; 92: 1075-6
31. Chazalon P, Tourtier JP, Villevielle T, Giraud D, Saissy JM, Mion G, Benhamou D:Ropivacaine-induced cardiac arrest after peripheral nerve block: successful resuscitation. Anesthesiology2003; 99: 1449-51
32. Huet O, Eyrolle LJ, Mazoit JX, Ozier YM: Cardiac arrest after injection of ropivacainefor posterior lumbar plexus blockade. Anesthesiology 2003; 99: 1451-3
33. Polley LS, Santos AC: Cardiac arrest following regional anesthesia with ropivacaine:here we go again! Anesthesiology 2003; 99: 1253-4
34. Reinikainen M, Hedman A, Pelkonen O, Ruokonen E: Cardiac arrest after interscalenebrachial plexus block with ropivacaine and lidocaine. Acta Anaesthesiol Scand 2003; 47: 904-6
35. Owen MD, Gautier P, Hood DD: Can ropivacaine and levobupivacaine be used as testdoses during regional anesthesia? Anesthesiology 2004; 100: 922-5
36. Lund PC, Cwik JC: Propitocaine (Citanest) and methemoglobinemia. Anesthesiology1965; 26: 569-571
37. Scott DB, Owen JA, Richmond J: Methemoglobinemia due to prilocaine. Lancet 1964; 2:7728-729
38. Aepfelbacher FC, Breen P, Manning WJ: Methemoglobinemia and topical pharyngealanesthesia. N Engl J Med 2003; 348: 85-6
39. Aldrete JA, Johnson DA: Evaluation of intracutaneous testing for investigation of allergyto local anesthetic agents. Anesth Analg 1970; 49: 173-83
40. Aldrete JA, O'Higgins JW: Evaluation of patients with history of allergy to localanesthetic drugs. South Med J 1971; 64: 1118-21
41. Moen V, Dahlgren N, Irestedt L: Severe neurological complications after centralneuraxial blockades in Sweden 1990-1999. Anesthesiology 2004; 101: 950-9
42. Vandam LD, Dripps RD: A long-term follow-up of 10,098 spinal anesthetics II.Incidence and analysis of minor neurologic defects. Surg 1955; 38: 463-469
43. Ravindran RS, Bond VK, Tasch MD, Gupta CD, Luerssen TG: Prolonged neuralblockade following regional analgesia with 2-chloroprocaine. Anesth Analg 1980; 59: 447-451
44. Reisner LS, Hochman BN, Plumer MH: Persistent neurologic deficit and adhesivearachnoiditis following intrathecal 2-chloroprocaine injection. Anesth Analg 1980; 59: 452-454
45. Wang BC, Hillman DE, Spielholz NI, Turndorf H: Chronic neurological deficits andNesacaine-CE--an effect of the anesthetic, 2-chloroprocaine, or the antioxidant, sodium bisulfite? AnesthAnalg 1984; 63: 445-7
46. Kalichman MW: Physiologic mechanisms by which local anesthetics may cause injury tonerve and spinal cord. Reg Anesth 1993; 18: 448-52
47. Kalichman MW, Powell HC, Myers RR: Pathology of local anesthetic-induced nerveinjury. Acta Neuropathol (Berl) 1988; 75: 583-9
48. Kalichman MW, Powell HC, Myers RR: Quantitative histologic analysis of localanesthetic-induced injury to rat sciatic nerve. J Pharmacol Exp Ther 1989; 250: 406-13
49. Kalichman MW, Powell HC, Reisner LS, Myers RR: The role of 2-chloroprocaine andsodium bisulfite in rat sciatic nerve edema. J Neuropathol Exp Neurol 1986; 45: 566-75
50. Gissen AJ, Datta S, Lambert D: The chloroprocaine controversy. II. Is chloroprocaineneurotoxic? Reg Anesth 1984; 9: 135-145
51. Taniguchi M, Bollen AW, Drasner K: Sodium bisulfite: scapegoat for chloroprocaineneurotoxicity? Anesthesiology 2004; 100: 85-91
52. Fibuch EE, Opper SE: Back pain following epidurally administered Nesacaine-MPF [seecomments]. Anesth Analg 1989; 69: 113-5
53. Wang BC, Li D, Hiller JM, Simon EJ, Budzilovich G, Hillman DE: Lumbarsubarachnoid ethylenediaminetetraacetate induces hindlimb tetanic contractions in rats: prevention byCaCl2 pretreatment; observation of spinal nerve root degeneration. Anesth Analg 1992; 75: 895-9
54. Rigler ML, Drasner K, Krejcie TC, Yelich SJ, Scholnick FT, DeFontes J, Bohner D:Cauda equina syndrome after continuous spinal anesthesia. Anesth Analg 1991; 72: 275-81
55. Schell RM, Brauer FS, Cole DJ, Applegate RL, II: Persistent sacral nerve root deficitsafter continuous spinal anaesthesia. Can J Anaesth 1991; 38: 908-11
56. Drasner K, Rigler ML, Sessler DI, Stoller ML: Cauda equina syndrome followingintended epidural anesthesia. Anesthesiology 1992; 77: 582-5
57. Cheng AC: Intended epidural anesthesia as possible cause of cauda equina syndrome.Anesth Analg 1994; 78: 157-9
58. Lambert DH, Hurley RJ: Cauda equina syndrome and continuous spinal anesthesia.Anesth Analg 1991; 72: 817-819
59. Rigler ML, Drasner K: Distribution of catheter-injected local anesthetic in a model of thesubarachnoid space. Anesthesiology 1991; 75: 684-692
60. Ross BK, Coda B, Heath CH: Local anesthetic distribution in a spinal model: a possiblemechanism of neurologic injury after continuous spinal anesthesia. Reg Anesth 1992; 17: 69-77
61. Lambert LA, Lambert DH, Strichartz GR: Irreversible conduction block in isolated nerveby high concentrations of local anesthetics. Anesthesiology 1994; 80: 1082-93
62. Bainton CR, Strichartz GR: Concentration dependence of lidocaine-induced irreversibleconduction loss in frog nerve. Anesthesiology 1994; 81: 657-67
63. Strichartz GR, Manning T, Datta S: Irreversible conduction block in mammalian nervesby direct application of 2% and 5% lidocaine. [Abstract]. Regional Anesthesia 1994; 19 [Supplement]: 21
64. Drasner K, Sakura S, Chan VW, Bollen AW, Ciriales R: Persistent sacral sensory deficitinduced by intrathecal local anesthetic infusion in the rat. Anesthesiology 1994; 80: 847-52
65. Sakura S, Chan VW, Ciriales R, Drasner K: The addition of 7.5% glucose does not alterthe neurotoxicity of 5% lidocaine administered intrathecally in the rat. Anesthesiology 1995; 82: 236-40