Embed Size (px)
DESCRIPTION
Undergraduate Medical Education Review 2005‐2010 ay Rosenfield, ViceDean Undergraduate Medical EducationJ ViceDean, Undergraduate Medical Education – Professor Jay Rosenfield
Citation preview
Undergraduate Medical Education Review 2005‐2010
ay Rosenfield, ViceDean Undergraduate Medical Education J
“Our medical school attracts the
most remarkable, highly
motivated young adults from
across Canada – students who
demonstrate outstanding
leadership skills, civic engagement
and social responsibility,
and who take full advantage of
all our offerings, including our
tremendous variety of clinical
and related research experiences.
We are also very proud of the vast
cadre of teaching faculty and
staff who educate, mentor and
support our students, who, by all
indicators, are extremely satisfied
with their program.”
– Professor Jay Rosenfield
ViceDean, Undergraduate Medical Education
TABLE OF CONTENTS
INTRODUCTION ............................................................................................................. 1
1. CURRICULUM ........................................................................................................ 3
2. CURRICULAR ENRICHMENT OPPORTUNITIES FOR STUDENTS ........................ 18
3. PARTNERSHIPS WITH HOSPITALS IN THE STUDENT EXPERIENCE ................... 23
4. TECHNOLOGY AND THE STUDENT EXPERIENCE ............................................... 31
5. STUDENT SUPPORT – REGISTRARIAL AFFAIRS ................................................. 38
6. STUDENT SUPPORT – FINANCIAL AID AND AWARDS ...................................... 41
7. STUDENT SUPPORT – COUNSELLING AND COMMUNITY BUILDING .............. 42
8. ATTRACTING STUDENTS – ADMISSIONS ........................................................... 45
9. EVALUATION AND IMPROVEMENT IN UME TO SUPPORT THE STUDENT EXPERIENCE ........................................................................................................ 48
10. LIAISON AND PROMOTION OF UME OUTSIDE THE UNIVERSITY .................... 50
11. CONCLUSION ...................................................................................................... 52
APPENDICES ................................................................................................................ 56

Undergraduate Medical Education Review 2005‐2010
Undergraduate Medical Education Review 2005‐2010
JAY ROSENFIELD, VICE‐DEA
NTRODUCTION
N, UNDERGRADUATE MEDICAL EDUCATION
I
The Vice‐Dean, Undergraduate Medical Education has overall responsibility for all aspects of the MD program. This includes the portfolios of Admissions, Student Awards and Finances, the Faculty Registrar, Student Affairs and Curriculum centrally, as well as the critical partnerships with our
1
affiliated institutions and academies.
Since the summer of 2005, when I became what was then the Associate Dean of Undergraduate Medical Education (UME), we have seen considerable changes in the UME portfolio. It has been a period of tremendous growth and development as we have embarked on enrolment expansion that will amount to a 30% increase in entering class size by 2011, a greater shift to community learning environments, major capital projects, curriculum renewal, and full integration of technology into the student experience. Our accomplishments will enable us to move forward on equally significant projects in the years to come in a manner that is student‐centred and responsive to the strategic
research and medical education. directions of the Faculty and the latest innovations in pedagogical
These accomplishments could not have been realized without the dedication and constant efforts of countless individuals in UME. First, I must acknowledge my senior management team, in particular the UME Executive Committee (the Associate Deans, Academy Directors, Preclerkship and Clerkship Directors, Registrar, and Administrative and Special Projects Managers) and all the Course Directors. Their tireless interest in the mindful evolution of medical education at the University of Toronto for the benefit of students and society at large is an inspiration to everyone around them, and also a testament to the culture of leadership that we strive to cultivate in UME. As noted in later sections of this report, it is with sadness that we have parted with several such leaders in recent months. As they leave their previous roles for new directions, I give my personal thanks to long‐time course directors Ian Taylor and Bill Chapman, Associate Deans Maureen Shandling and Anna Jarvis, and Academy Directors Leslie Nickell and Vince
These accomplishments could not have been realized without the dedication and constant efforts of countless individuals in UME.
Chien for their remarkable contributions over many years.
With its emphasis on small‐group and hands‐on learning, our MD program could not function without the involvement of many hundreds of teachers spread across our fully and community affiliated teaching hospitals, offices, and agencies. Many of them serving as volunteers, these preceptors, tutors, lecturers, seminar leaders, and others are one of the principal reasons for our students’ successes and enrichment. Each year, we honour a select few outstanding teachers through the Aikins and Medical Alumni Association teaching awards (see Appendices 1.1 and 1.2), but we owe

Undergraduate Medical Education Review 2005‐2010
a debt of gratitude to all those who welcome our students into their clinics and busy schedules. On a university scale, Dr. Martin Schreiber was one of three recipients awarded the 2009 Presidents Teaching Award, in recognition of for his excellence in undergraduate medicine teaching. I personally wish to thank all of our teachers/faculty, their departments, and our Department Chairs, who whole‐
a debt of gratitude to all those who welcome our students into their clinics and busy schedules. On a university scale, Dr. Martin Schreiber was one of three recipients awarded the 2009 Presidents Teaching Award, in recognition of for his excellence in undergraduate medicine teaching. I personally wish to thank all of our teachers/faculty, their departments, and our Department Chairs, who whole‐heartedly support our UME education endeavours.
The presence of hundreds of students and teachers necessitates a strong administrative force to keep our program running smoothly, and UME is fortunate to have the support of amazing and talented administrative staff in the Medical Sciences Building, in the clinical departments, and at every affiliated clinical site. During my term, I have expanded our administrative staff such that approximately 70 individuals in core administrative positions now support the program and attend our annual staff retreat. There they are updated on recent developments, meet new members of our
heartedly support our UME education endeavours.
The presence of hundreds of students and teachers necessitates a strong administrative force to keep our program running smoothly, and UME is fortunate to have the support of amazing and talented administrative staff in the Medical Sciences Building, in the clinical departments, and at every affiliated clinical site. During my term, I have expanded our administrative staff such that approximately 70 individuals in core administrative positions now support the program and attend our annual staff retreat. There they are updated on recent developments, meet new members of our team, and take the opportunity to renew professional liaisons face‐to‐face.
More generally, I have also ensured that staff support has increased in many areas to meet the needs of an evolving UME portfolio. In particular, two key additions have been made in my office. Shortly after my term began, I created a new position for an overall Administrative Manager; Dr. Riet van
Lieshout has been responsible for administrative oversight of every aspect of UME since 2005, ensuring the efficient day‐to‐day operations of our central offices and providing guidance on matters relating to finance, staffing, etc. Furthermore, in view of the larger projects upon which UME is embarking, in 2008, we created another high‐level administrative position reporting directly to me. The Special Projects Manager, Neil Neebar, assists with analysis, reporting, and the organization of other endeavours in which I am involved. Other new positions are described in the appropriate sections below. In both old and new roles, our staff have kept pace with the changing demands and challenges that have accompanied the growth of UME; indeed, in the course of my term, four of our UME staff employees have been the recipients of the prestigious University of Toronto Stepping Up Merit Awards (2005/2006 – Faculty Registrar Ms. Judy Irvine and the Co‐ordinator of Registrarial Affairs Ms. Stella Miller, and 2006/2007 – Dr. Riet van Lieshout and Ms. Jennifer Anderson, Co‐ordinator Enrolment
Expansion) for demonstrating leadership on major new projects. These awards serve as an indicator dards we maintain in UME.
team, and take the opportunity to renew professional liaisons face‐to‐face.
More generally, I have also ensured that staff support has increased in many areas to meet the needs of an evolving UME portfolio. In particular, two key additions have been made in my office. Shortly after my term began, I created a new position for an overall Administrative Manager; Dr. Riet van
Lieshout has been responsible for administrative oversight of every aspect of UME since 2005, ensuring the efficient day‐to‐day operations of our central offices and providing guidance on matters relating to finance, staffing, etc. Furthermore, in view of the larger projects upon which UME is embarking, in 2008, we created another high‐level administrative position reporting directly to me. The Special Projects Manager, Neil Neebar, assists with analysis, reporting, and the organization of other endeavours in which I am involved. Other new positions are described in the appropriate sections below. In both old and new roles, our staff have kept pace with the changing demands and challenges that have accompanied the growth of UME; indeed, in the course of my term, four of our UME staff employees have been the recipients of the prestigious University of Toronto Stepping Up Merit Awards (2005/2006 – Faculty Registrar Ms. Judy Irvine and the Co‐ordinator of Registrarial Affairs Ms. Stella Miller, and 2006/2007 – Dr. Riet van Lieshout and Ms. Jennifer Anderson, Co‐ordinator Enrolment
Expansion) for demonstrating leadership on major new projects. These awards serve as an indicator dards we maintain in UME.
Our students astonish all of us with their zeal for learning, their passion for the future of medical practice, and their diverse ambitions.
2
of quality and external recognition for the high stan
Finally, I would like to make special mention of our remarkably talented, devoted, enthusiastic and visionary students, for whom the medical school exists. From the moment that they arrive in Year 1, our students astonish all of us with their zest for learning, their passion for the future of medical practice, and their diverse ambitions. More than anyone, it is the students who challenge us to achieve success and to identify and resolve problems, and it is they who will continue to push us forward as true partners. In UME, we refer to our “student colleagues” in recognition of the central role they play in defining the medical education that we deliver. The richness of the experience we can offer them throughout the course of their training is the fundamental measure and benchmark of our program.
of quality and external recognition for the high stan
Finally, I would like to make special mention of our remarkably talented, devoted, enthusiastic and visionary students, for whom the medical school exists. From the moment that they arrive in Year 1, our students astonish all of us with their zest for learning, their passion for the future of medical practice, and their diverse ambitions. More than anyone, it is the students who challenge us to achieve success and to identify and resolve problems, and it is they who will continue to push us forward as true partners. In UME, we refer to our “student colleagues” in recognition of the central role they play in defining the medical education that we deliver. The richness of the experience we can offer them throughout the course of their training is the fundamental measure and benchmark of our program.

Undergraduate Medical Education Review 2005‐2010
CURRICULUM CURRICULUM UME is a vast network, incorporating over 900 students, a similar number of teachers at fully‐affiliated and community‐affiliated hospitals, and hundreds of staff members. At the centre of UME is the curriculum, or education, program, which incorporates the majority of our constituents. Our curriculum is governed by a set of overall goals and objectives (see Appendix 2.1) that were developed under my leadership in 2003. They represent one of the first competency‐based approaches to undergraduate medical education objectives ever adopted in Canada. Our curriculum objectives are constantly scrutinized and are revised as warranted to reflect the evolution of medical education. As is necessary in any large enterprise, I have introduced change carefully in the MD curriculum, always ensuring buy‐in from the key stakeholders as we have moved forward. In the first few years of my term, I worked with the Preclerkship and Clerkship Directors to make important but comparatively straightforward improvements. At the same time, my strategy has been to lay the roundwork for the more sweeping reorganization of our curriculum that is now underway. g
a. Improvements to date
Crucial to the student experience is a balance between structured educational activities and self‐directed personal time. Working together with the Preclerkship Director, we have therefore strived to build more generous allowances for the latter into what can otherwise be an overwhelming curriculum. In Years 1 and 2, students now have self‐study blocks in most weeks, and the creation of “Academy Days” in 2008/09 has reduced the amount of time spent on travel between hospitals and the University campus. The resulting change to the schedules of most of our courses required considerable effort on the part of our Academy Directors and Course Directors (most importantly, to recruit new small‐group teachers whose clinical schedule would match the revised teaching timeslots), but the positive impact on our students is already evident. As well, several years ago, the Preclerkship Committee endeavoured to provide a meaningful reprieve from the intensity of both Year 1 and Year 2 by endorsing a policy to observe a March Break every year, a move that was and continues to be strongly supported by students.
In the Clerkship, students no longer juggle the academic requirements of their February rotation in Year 4 while having to attend residency program interviews across the country. In 2006/07, we introduced a two‐week CaRMS break for all students in their final year to alleviate this difficulty; the break was increased to three weeks in 2007/08, and we intend to maintain it at that length henceforth.
Crucial to the student
experience is a balance
between structured
educational activities
and self-directed
personal time.
3
Undergraduate Medical Education Review 2005‐2010
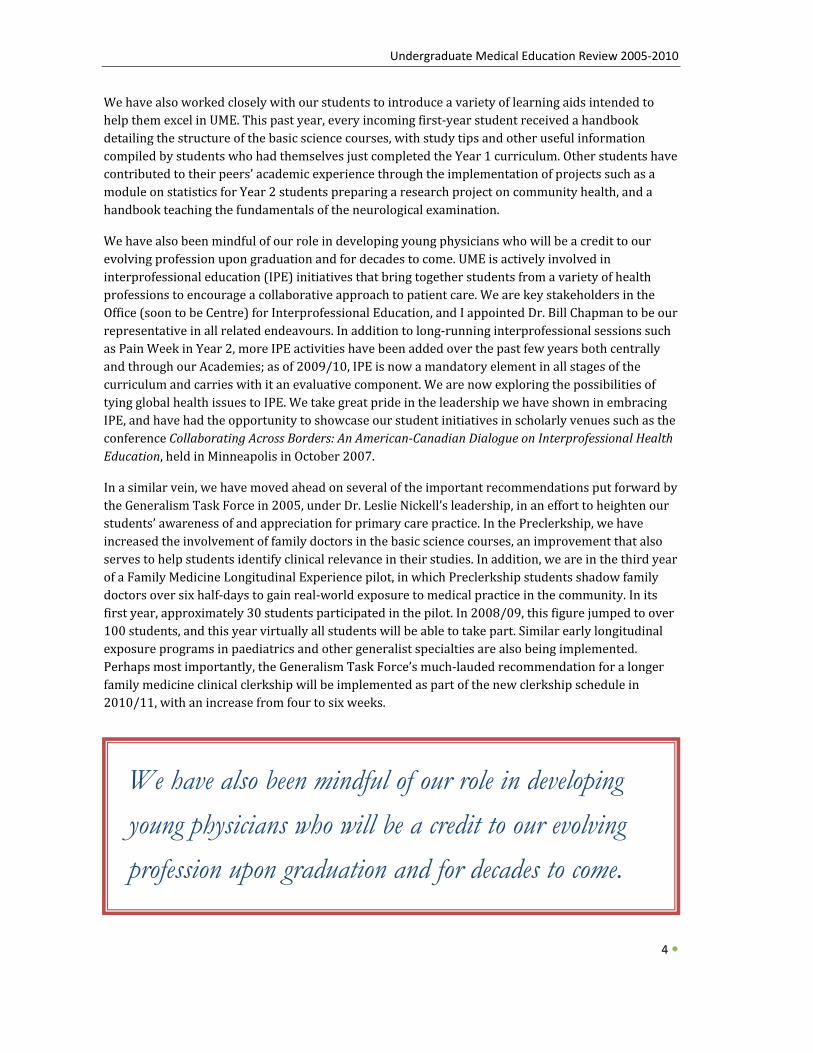
We have also worked closely with our students to introduce a variety of learning aids intended to help them excel in UME. This past year, every incoming first‐year student received a handbook detailing the structure of the basic science courses, with study tips and other useful information compiled by students who had themselves just completed the Year 1 curriculum. Other students have contributed to their peers’ academic experience through the implementation of projects such as a module on statistics for Year 2 students preparing a research project on community health, and a handbook teaching the fundamentals of the neurological examination.
We have also been mindful of our role in developing young physicians who will be a credit to our evolving profession upon graduation and for decades to come. UME is actively involved in interprofessional education (IPE) initiatives that bring together students from a variety of health professions to encourage a collaborative approach to patient care. We are key stakeholders in the Office (soon to be Centre) for Interprofessional Education, and I appointed Dr. Bill Chapman to be our representative in all related endeavours. In addition to long‐running interprofessional sessions such as Pain Week in Year 2, more IPE activities have been added over the past few years both centrally and through our Academies; as of 2009/10, IPE is now a mandatory element in all stages of the curriculum and carries with it an evaluative component. We are now exploring the possibilities of tying global health issues to IPE. We take great pride in the leadership we have shown in embracing IPE, and have had the opportunity to showcase our student initiatives in scholarly venues such as the conference Collaborating Across Borders: An AmericanCanadian Dialogue on Interprofessional Health
4
Education, held in Minneapolis in October 2007.
In a similar vein, we have moved ahead on several of the important recommendations put forward by the Generalism Task Force in 2005, under Dr. Leslie Nickell’s leadership, in an effort to heighten our students’ awareness of and appreciation for primary care practice. In the Preclerkship, we have increased the involvement of family doctors in the basic science courses, an improvement that also serves to help students identify clinical relevance in their studies. In addition, we are in the third year of a Family Medicine Longitudinal Experience pilot, in which Preclerkship students shadow family doctors over six half‐days to gain real‐world exposure to medical practice in the community. In its first year, approximately 30 students participated in the pilot. In 2008/09, this figure jumped to over 100 students, and this year virtually all students will be able to take part. Similar early longitudinal exposure programs in paediatrics and other generalist specialties are also being implemented. Perhaps most importantly, the Generalism Task Force’s much‐lauded recommendation for a longer family medicine clinical clerkship will be implemented as part of the new clerkship schedule in 2010/11, with an increase from four to six weeks.
We have also been mindful of our role in developing young physicians who will be a credit to our evolving profession upon graduation and for decades to come.
Undergraduate Medical Education Review 2005‐2010
b. Strategy for change
External Review In recognition that insight from experts outside our UME core could serve as a catalyst for innovation, I made the decision to organize an external review of the Clerkship at the conclusion of Dr. Anita Rachlis’s first term as Clerkship Director in 2007. As expected, the reviewers, Dr. Allan Jones and Dr. Brian Hodges, made a number of important recommendations (see Appendix 2.2) regarding not just the Clerkship but the program as a whole (paraphrased here for brevity):
• That curriculum management be restructured to enable greater efficiency but also
• . sufficiently diverse representation. That the Faculty’s strategic planning exercise be completed to provide direction for UME
• the That a curriculum map be completed and maintained as a matter of priority to formbasis for consideration of changes to curricular content.
• to That greater flexibility be built into the curriculum to allow it to better respondchanges.
• That significant clinical experiences be introduced from the early stages of the curriculum.
• hey That the knowledge competencies expected of our students be fully defined so that tcan be coordinated and integrated across courses and years of the program.
• munity‐based That e‐learning opportunities be increased, especially to support com
• clerkship experiences. That the Electives Director role be filled as a matter of priority.
• That the Liaison Committee on Medical Education (LCME) standards be kept in mind in preparation for the next accreditation.
SelfStudy Student and Faculty, midaccreditation cycle
I accepted these recommendations (see Appendix 2.3) and followed up with a comprehensive curriculum review and renewal project later that year as part of the Faculty’s strategic planning exercise. I struck a Curriculum Review Steering Group consisting of leaders and educational innovators from around the Faculty as well as current and former students (see Appendix 2.4); our initial discussions raised a number of important themes and concepts around medical education. Placing high value on the student perspective, the Curriculum Review Steering Group requested that the student members conduct an independent, focus‐group‐based review of the undergraduate curriculum to highlight curriculum improvement opportunities. The resulting Student Curriculum Review Report highlighted six key themes
The resulting
Student Curriculum
Review Report
highlighted six key
themes and three
principles for UME
curriculum reform. and three principles for UME curricular reform (see Appendix 2.5).
In the meantime, I moved forward with the first recommendation of Drs. Hodges and Jones: our curriculum management structure was in
5
Undergraduate Medical Education Review 2005‐2010
6
need of revision. In December 2007, under the authority of Faculty Council and delegated responsibility to the Vice‐Dean, Undergraduate Medical Education, a renewed Undergraduate Medical Education Curriculum committee (UMECC) was formed to oversee the design, implementation, management, and evaluation of the undergraduate MD education program (see Appendix 2.6 for Terms of Reference). In an effort to strengthen undergraduate ties to public health issues, the Director of the Dalla Lana School of Public Health was invited to serve on this committee; similarly, the Chairs of several clinical departments and a basic science department were invited to participate to ensure ongoing close collaboration. Ties to the Wilson Centre, and medical education research were also strengthened with the addition of the Director of the Wilson Centre to the Curriculum Committee.
Midway through the current eight‐year accreditation period, a one‐day retreat was held in May 2008 with close to 100 participants representing all UME constituencies and external stakeholders; the retreat included panel discussions and consideration of the students’ own curriculum review report results. The extensive recommendations had some overlap with the recommendations put forward in the Clerkship Review but delved much deeper into the ways we could improve. I initiated the entire process of review in recognition that an eight‐year period between accreditations is far too long to forgo self‐study and continuous quality improvement. In fact, the introduction of an internal mid‐cycle review at all medical schools, much like the standard practice in post‐graduate medicine, is now on the national undergraduate deans’ agenda this fall, in part because of the successful process I have ndertaken at the University of Toronto. u
c. Upcoming changes
Planning Principles Using the recommendations arising not only from the Clerkship Review, the Curriculum Review, and the Student Review, but also from the results of the 2008 retreat, the Graduation Questionnaire,1 and the Medical Council of Canada Qualifying Examinations (MCCQE) results, and ongoing reports from students in the program, we have identified important principles to guide us in a significant renewal of the curriculum over the next few years, focussed primarily on the layout of courses, the integration of themes, and the time devoted to certain key topics.
1 The Graduate Questionnaire is an anonymous survey of students in the final year of the MD program, administered by the Association of American Medical Colleges (AAMC).
Undergraduate Medical Education Review 2005‐2010
In June 2008, the UMECC passed a set of governing principles to guide UME curriculum renewal activities. The resulting measures, a selection of which are outlined below, have all arisen in direct response to the themes identified by students, faculty, and the reviews noted above.
Theme 1: Clinical relevance – Students indicated a greater need for understanding the clinical relevance of what they are being taught. They want teaching to be coordinated with hands‐on opportunities so they can apply the detail they learn to the real world, within the appropriate context and with a focus on common conditions. They also feel applied learning is the best way to learn (e.g. the longstanding ASCM I “Day of the Doctor” session).
Curriculum Committee Response 1:
Clinical Relevance Principle: “All teaching events in the Undergraduate Medicine program (lectures, seminars, PBL, and other tutorials, laboratory sessions, bedside teaching, etc.) will have some component that explicitly links the teaching to current medical practice.”
Joint contributions from clinicians and basic scientists: “Where possible and appropriate, concurrent input in teaching sessions from both clinicians and basic scientists will be encouraged.”
In June 2008, the UMECC passed a set of governing principles to guide UME curriculum renewal activities.
Theme 2: Clinical exposure –Students indicated a desire for more opportunities for early career exploration to instantiate the knowledge and skills acquired in class. They also wish for more clinical exposure to help them make informed CaRMS choices.
Curriculum Committee Response 2: Halfday off per week in the Preclerkship: “In the preclerkship, students will have, at a minimum, a clearly identified half‐day per week that is free of scheduled activities. This time is to be used for activities that include clinical observational experiences, course work utside of medicine, research activities, or other approved co‐curricular experiences, chosen y the individual student. This time is sepob arate from “free” time for self‐study.” ongitudinal Preclerkship experiences: “A longitudinal clinical experience spanning more han one year will be developed in tLt
7
he preclerkship.” Integrated Clerkship experiences: “The clerkship will consist of both discipline‐specific and integrated experiences, with the learning environment both in the community and at the Academic Health Sciences Centres.”
Undergraduate Medical Education Review 2005‐2010
8
Theme 3: Evaluation – Students are seeking greater input on their progress towards becoming physicians and less focus on their knowledge of what they consider to be minutiae. Ideally, they would receive immediate, individualized, specific oral feedback based on direct observation. This requires changes to the current Clerkship evaluation.
Curriculum Committee Response 3:
Tracking clinical experiences: “Students will be required to track their own clinical experiences via a portfolio system. This will apply not only to core courses (ASCM) but also to additional longitudinal and elective experiences they pursue, in addition to the logging of encounters in clerkship. Encouragement of more direct observation and increased utilization of mid‐rotation feedback will be in place.”
Theme 4: Overspecialization – Students want contextualized teaching in varied learning settings. They would like greater balance between generalist and specialist perspectives, and feel this could be achieved through overviews of complex topics conducted by clinical teachers and through more rural placements.
Curriculum Committee Response 4:
Individual course committees: “All courses in the Curriculum will have a functioning course committee, which meets regularly and keeps minutes. Such committees will have input, at a minimum, from a primary/generalist, specialist, and student perspective. Input from the relevant individuals knowledgeable about the basic or foundational science for the particular area of study will also be included.”
See also the descriptions of the longitudinal Preclerkship experiences and integrated Clerkship experiences above (Curriculum Committee Response 2).
Theme 5: Course delivery – Students would like to have more peer‐to‐peer interaction, better modelling of best practices, lectures coordinated with the practical, enhanced IT learning, and more responsibility overall. For the Preclerkship, they would like an increase in small‐group learning, more experiential content and clinician‐led seminars, and a curriculum augmented by technology. For the Clerkship, they want more learning in the clinical context, near‐peer learning, and real case‐based learning.
Curriculum Committee Response 5: UME Course Curriculum Review Committee: “A new sub‐committee of the UMECC will be struck, to oversee courses as a whole, reviewing on a regular basis course structure, content, governance, and integration with the curriculum as a whole. This committee will complement the activities of ESAC and UMEPEC. This committee will have the opportunity to seek input from various stakeholders to ensure that the different aspects of the curriculum overall are receiving appropriate attention. This would include the following two strategies: (1) a “systems‐based” approach to curricular review, to ensure that the content of the curriculum as it pertains to body systems (cardiovascular, neurologic, musculoskeletal, etc.)
Undergraduate Medical Education Review 2005‐2010
icics appropriate; and (2) theme‐based, to ensure the major competencies (professional, ollaborator, advos appropriate; and (2) theme‐based, to ensure the major competencies (professional, ollaborator, advocate, manager, etc.) are being adequately addressed.” Curriculum map: Curriculum mapping of the MD program will be complete by the end of 2008. (see Section 4.d. IT contribu
cate, manager, etc.) are being adequately addressed.” Curriculum map: Curriculum mapping of the MD program will be complete by the end of 2008. (see tions to curricular improvementtions to curricular improvementSection 4.d. IT contribu ). Digital capture of large events: All large‐group events (lectures) will be captured in some type of permanent digital media. This could be audio or video capture, depending on the instructors’ preference, along with all slides, overheads, etc. Such capture will take into account relevant copyright laws and intellectual property considerations.
See also the description of tracking clinical experiences above (Curriculum Committee Response 3).
Theme 6: Full range of competencies covered, in addition to medical expert – Our students expect high‐quality teaching with practical content. They want teaching around all the CanMEDS competencies and the four principles of family medicine, including small‐group ethics teaching, community visits, and independent projects.
Curriculum Committee Response 6: Addressing the curricular competencies: “The seven curriculum competencies expected of graduates will be an integral part of all courses, as appropriate and relevant. Evidence of successful completion of these competencies, will be a requirement for graduation, in addition to passing all regular course work.” See also the descriptions of the UME Course Curriculum Review Committee (Curriculum Committee Response 5), tracking clinical experiences (Curriculum Committee Response 3), and integrated Clerkship experiences (Curriculum Committee Response 2).
9
Preclerkship Curriculum Under the skilled leadership of Dr. Schreiber, major changes have been launched in the Preclerkship beginning this academic year 2009/10. The first course in Year 1, Structure & Function (STF), has been condensed and topics including biochemistry and genetics have been deferred to later courses to focus the content on anatomy and histology with structure/systems integration. Long considered by students to be the most challenging Preclerkship course with respect to workload, STF now incorporates more self‐study time every week. The second block course of Year 1, Metabolism & Nutrition (MNU), has taken on the biochemistry and genetics components, but has also gained two weeks to ensure that students do not become overloaded in that course. Brain & Behaviour (BRB) follows more or less unchanged, except that it now commences two weeks earlier than before. Most significantly, for the first time, Year 1 will now
… the first-year students applauded these curriculum changes, and noted that their experience to date was excellent…
Undergraduate Medical Education Review 2005‐2010
end with a new pharmacology block designed to reinforce and build on pharmacology content integrated into the previous courses. At the Class Presidents’ Lunch in October 2009, the first‐year students applauded these curriculum changes, and noted that their experience to date was excellent, with well‐integrated and relevant lectures, seminars, and labs.
In Year 2, changes will be introduced in 2010/11 to better coordinate the two block courses, Pathobiology of Disease (PBD) and Foundations of Medical Practice (FMP). Full integration of these courses to create a single, full‐year course is being contemplated as a means to reduce redundancy between the two and ensure that all important systems and areas of medicine can be covered ffectively. e
Clerkship Curriculum Under the innovative leadership of Dr. Rachlis, a major redesign of the Clerkship is underway to move away from a calendar‐based Year 3/Year 4 distinction in favour of a PreCaRMS and PostCaRMS schedule.2 In contrast to the inequitable system currently in place, all students will be guaranteed to experience all the core Clerkships prior to the CaRMS application deadline in late fall, and to conclude all their elective time by December. Overall elective time will be reduced from 17 weeks to 13 weeks, but students will gain “selective” time in the post‐CaRMS period, which will be renamed the Transition to Residency rotation. This new curricular organization acts upon the recommendations of the Generalism Task Force and the 2006/07 external review of the Clerkship to increase the family medicine Clerkship to six weeks and to provide more community experiences throughout the Clerkship as a whole. It will also provide students with a valuable review period at the end of Clerkship prior to the Medical Council examinations, as well as the opportunity to onsolidate their learning over the past four years through a “fusion” experience. c
This new curricular organization acts upon the recommendations of the Generalism Task Force and the 2006/07 external review of the Clerkship…
2 This refers to the point in Year 4 by which students must submit their program rankings for residency, CaRMS being the Canadian Residency Matching Service. (generally early December)
10
Undergraduate Medical Education Review 2005‐2010
11
The improved curriculum will include more explicit teaching and evaluation in non‐medical expert competencies and will afford students the opportunity to engage in innovative learning strategies such as integrated Clerkships, selectives, and the use of portfolios for self‐directed learning, reflection, and assessment. It will also add much‐needed flexibility to the curriculum, enabling it to adopt and adapt to recommendations of the “Future of Medical Education in Canada” project, as well as ensuring greater emphasis on generalist and integrated community experiences in several of the other Clerkships. Moreover, the new Clerkship will further develop community‐based sites for student education to improve access to teaching resources, provide diversity in educational experiences, and expose students more widely to generalism and community‐based faculty role models.
Our clinical departments are playing a major role in the design of the Transition to Residency program. For example, under the creative leadership of Richard Reznick and his education team, the Department of Surgery has developed multiple tracks for students with varied interests, including “Surgery for the Family Physician.” The Department of Medicine is also currently developing new odels of Clerkship teaching. m
d. New leaders
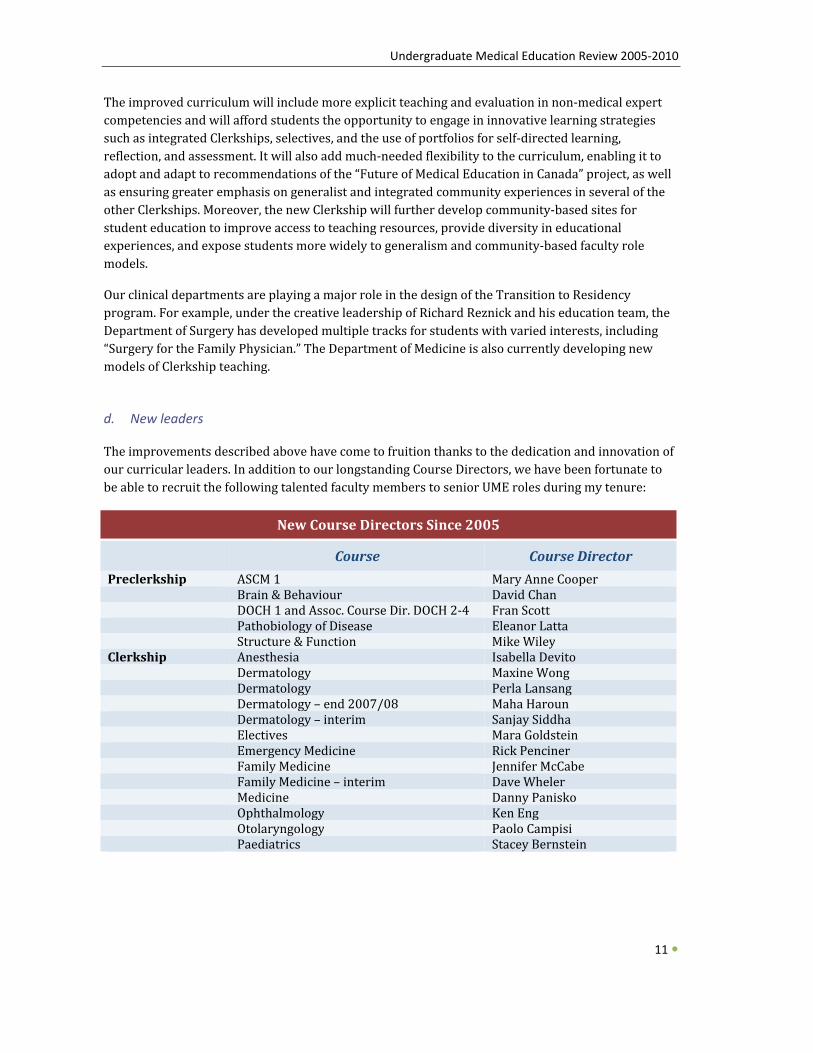
The improvements described above have come to fruition thanks to the dedication and innovation of our curricular leaders. In addition to our longstanding Course Directors, we have been fortunate to be able to recruit the following talented faculty members to senior UME roles during my tenure:
New Course Directors Since 2005
Course Course Director Preclerkship ASCM 1 Mary Anne Cooper Brain & Behaviour David Chan DOCH 1 and Assoc. Course Dir. DOCH 2‐4 Fran Scott Pathobiology of Disease Eleanor Latta Structure & Function Mike WileyClerkship Anesthesia Isabella Devito Dermatology Maxine Wong Dermatology Perla Lansang Dermatology – end 2007/08 Maha Haroun Dermatology – interim Sanjay Siddha Electives Mara Goldstein Emergency Medicine Rick Penciner Family Medicine Jennifer McCabe Family Medicine – interim Dave Wheler Medicine Danny Panisko Ophthalmology Ken Eng Otolaryngology Paolo Campisi Paediatrics Stacey Bernstein
Undergraduate Medical Education Review 2005‐2010
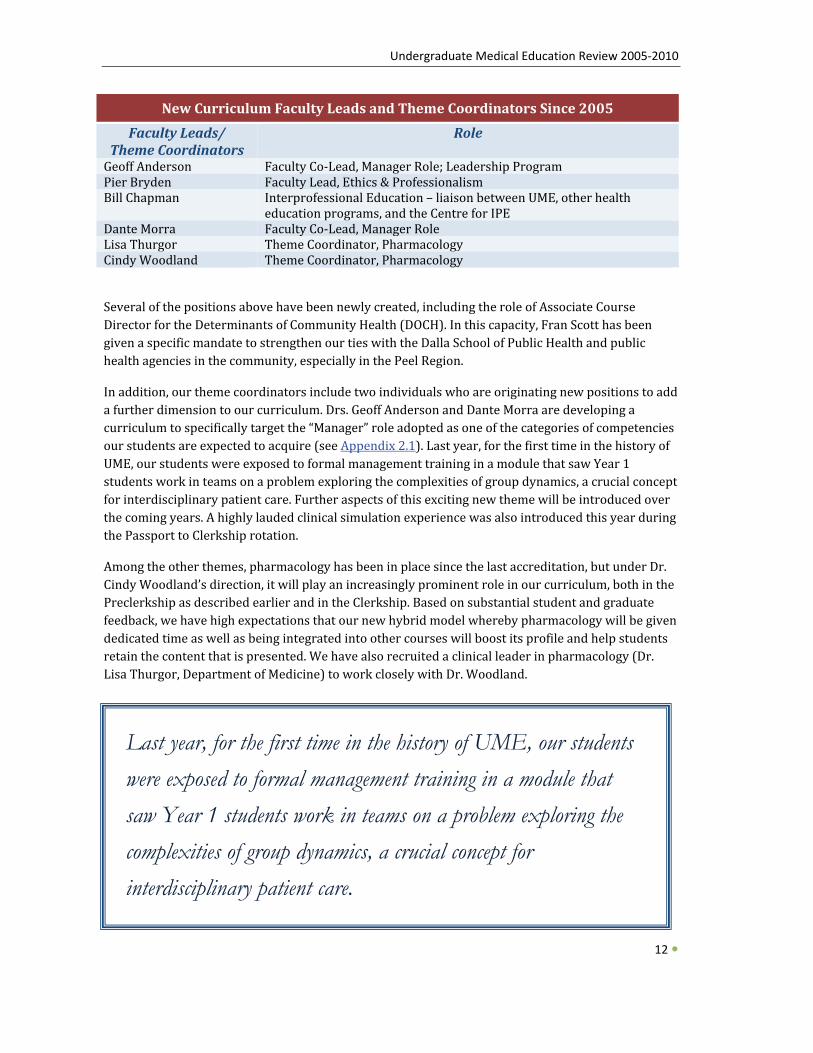
New Curriculum Faculty Leads and Theme Coordinators Since 2005
Faculty Leads/ Theme Coordinators
Role
Geoff Anderson Faculty Co‐Lead, Manager Role; Leadership ProgramPier Bryden Faculty Lead, Ethics & ProfessionalismBill Chapman Interprofessional Education – liaison between UME, other health
education programs, and the Centre for IPE Dante Morra Faculty Co‐Lead, Manager RoleLisa Thurgor Theme Coordinator, PharmacologyCindy Woodland Theme Coordinator, Pharmacology
Several of the positions above have been newly created, including the role of Associate Course Director for the Determinants of Community Health (DOCH). In this capacity, Fran Scott has been given a specific mandate to strengthen our ties with the Dalla School of Public Health and public health agencies in the community, especially in the Peel Region.
In addition, our theme coordinators include two individuals who are originating new positions to add a further dimension to our curriculum. Drs. Geoff Anderson and Dante Morra are developing a curriculum to specifically target the “Manager” role adopted as one of the categories of competencies our students are expected to acquire (see Appendix 2.1). Last year, for the first time in the history of UME, our students were exposed to formal management training in a module that saw Year 1 students work in teams on a problem exploring the complexities of group dynamics, a crucial concept for interdisciplinary patient care. Further aspects of this exciting new theme will be introduced over the coming years. A highly lauded clinical simulation experience was also introduced this year during the Passport to Clerkship rotation.
Among the other themes, pharmacology has been in place since the last accreditation, but under Dr. Cindy Woodland’s direction, it will play an increasingly prominent role in our curriculum, both in the Preclerkship as described earlier and in the Clerkship. Based on substantial student and graduate feedback, we have high expectations that our new hybrid model whereby pharmacology will be given dedicated time as well as being integrated into other courses will boost its profile and help students retain the content that is presented. We have also recruited a clinical leader in pharmacology (Dr. Lisa Thurgor, Department of Medicine) to work closely with Dr. Woodland.
12
Last year, for the first time in the history of UME, our students were exposed to formal management training in a module that saw Year 1 students work in teams on a problem exploring the complexities of group dynamics, a crucial concept for interdisciplinary patient care.

Undergraduate Medical Education Review 2005‐2010
Our Ethics & Professionalism theme, led by Dr. Pier Bryden, is also evolving, with a greater emphasis on student reflection and integration with the curricular objectives via longitudinal learning opportunities using a portfolio model. A pilot of the portfolio approach is underway this year using Year 1 and Year 3 students at each Academy. The level of student interest and support has been extraordinary; students are involved in all aspects of the pilot project and their expressions of interest to this point have far outstripped our initial expectations. We have a strong Portfolio Committee with representation from all Academies, the Department of Family Medicine, Post‐Graduate Medical Education, the UME student body, and the UME administrative staff. Through other changes in the ethics and professionalism curriculum, our students will also gain stronger awareness f the history of medicine and study in the humanities.
Our Ethics & Professionalism theme, led by Dr. Pier Bryden, is also evolving, with a greater emphasis on student reflection and integration with the curricular objectives via longitudinal learning opportunities using a portfolio model. A pilot of the portfolio approach is underway this year using Year 1 and Year 3 students at each Academy. The level of student interest and support has been extraordinary; students are involved in all aspects of the pilot project and their expressions of interest to this point have far outstripped our initial expectations. We have a strong Portfolio Committee with representation from all Academies, the Department of Family Medicine, Post‐Graduate Medical Education, the UME student body, and the UME administrative staff. Through other changes in the ethics and professionalism curriculum, our students will also gain stronger awareness f the history of medicine and study in the humanities. o
o
e. Accreditation e. Accreditation
I had the privilege to act as the Senior Academic Coordinator for the 2004 accreditation. The UME MD program received an excellent accreditation review by the Liaison Committee on Medical Education (LCME) and Committee on Accreditation of Canadian Medical Schools (CACMS) resulting in an eight‐year
I had the privilege to act as the Senior Academic Coordinator for the 2004 accreditation. The UME MD program received an excellent accreditation review by the Liaison Committee on Medical Education (LCME) and Committee on Accreditation of Canadian Medical Schools (CACMS) resulting in an eight‐year accreditation until May 2012.
A number of significant program strengths were noted, as well as a small number of areas of noncompliance with standards, and several areas of transition that required follow‐up. I am pleased to report that we are now in full compliance with all accreditation standards, although we must still report to the CACMS and LCME in May 2010 regarding one issue “in transition,” namely how we are evaluating some of our new program competency objectives. I have outlined below our original 2004 responses to the areas of non‐compliance identified at that time in the accreditation survey:
accreditation until May 2012.
A number of significant program strengths were noted, as well as a small number of areas of noncompliance with standards, and several areas of transition that required follow‐up. I am pleased to report that we are now in full compliance with all accreditation standards, although we must still report to the CACMS and LCME in May 2010 regarding one issue “in transition,” namely how we are evaluating some of our new program competency objectives. I have outlined below our original 2004 responses to the areas of non‐compliance identified at that time in the accreditation survey:
I am pleased to report that
we are now in full
compliance with all
accreditation standards…
Issue 1. Issue 1. Student research opportunities – A narrative description of research opportunities available to students during the preclerkship years, including funding available for such activities, the numbers of students participating, and the degree to which available opportunities meet student demand. (IS14)
Student research opportunities – A narrative description of research opportunities available to students during the preclerkship years, including funding available for such activities, the numbers of students participating, and the degree to which available opportunities meet student demand. (IS14)
13
Response 1. In response to this concern, the Faculty of Medicine was successful in obtaining significant funding from the Academic Initiatives Fund of the Provost’s office to improve the student experience by (i) providing for increased stipendiary support for students engaged in research, and (ii) base funding for administrative support of the research program, including the hiring of an Academic Director. Our students now have the opportunity to participate in unique research activities through the creation of the Comprehensive Research Experience for Medical Students (CREMS) Program under the leadership of Dr. Don Branch.
Response 1. In response to this concern, the Faculty of Medicine was successful in obtaining significant funding from the Academic Initiatives Fund of the Provost’s office to improve the student experience by (i) providing for increased stipendiary support for students engaged in research, and (ii) base funding for administrative support of the research program, including the hiring of an Academic Director. Our students now have the opportunity to participate in unique research activities through the creation of the Comprehensive Research Experience for Medical Students (CREMS) Program under the leadership of Dr. Don Branch.
Undergraduate Medical Education Review 2005‐2010
14
Issue 2. Formative feedback in clerkships – For each required clerkship, a brief description (table) of the strategies employed to give students formative assessment, when such assessment takes place, and at whose initiation. (ED 30)
Response 2. In response to this area of non‐compliance, Clerkship Course Directors reviewed the issue of mid‐rotation feedback with their course committees identifying areas that could benefit from a more structured review of student performance. As a result, mid‐rotation feedback forms were developed and instituted in all the Clerkship. In an effort to track this new practice, tudents were required to confirm via signature on their final clinical performance evaluation sform that they did receive a mid‐rotation review. The implementation of the Medical Student Information System (MedSIS) has since allowed or the electronic completion of evaluation forms, resulting in improved monitoring and ompliance control. fc
Issue 3. Faculty responsibility for admissions decisions – A description of changes in the respective roles of the Admissions Committee and Director of Admissions to ensure that the final responsibility for admissions decisions res s with the duly constituted faculty committee. (MS4) t
Response 3. In response to this area of non‐compliance, the terms and reference of the Admissions Committee were amended in October 2004 to include the responsibility to review and approve selection of applicants to the MD program.
Issue 4. Career counselling – (a) A description of how the Faculty assures that all students have appropriate career counselling, including guidance in the selection of fourth year electives; and (b) a summary of student evaluation of career counselling activities for the 2004 and 2005 graduating classes (Graduate Questionnaire or internal assessment). (MS19)
Response 4. At the time of the accreditation visit, the Office of Student Affairs (OSA) was in the process of ddressing this issue in follow‐up to the 2003/2004 OSA Annual Report through the mpleai
mentation of the following activities:
• The Director and Coordinator of the Office of Student Affairs were trained to administer the Association of American Medical Colleges (AAMC) Careers in Medicine Program
• Financial support and mentorship was provided for production of the third edition of Canadian Medical Residency Guide: Taking Control of your Future Medical Career (2005),
Undergraduate Medical Education Review 2005‐2010
15
a publication distributed to incoming University of Toronto (U of T) Doctor oStudents free of charge.
•
f Medicine
Discussions were held with current and past student leaders to obtain their perspective on how best to provide more individual career counselling.
• Recognizing that students were experiencing significant stress adjusting to the MD program in addition to financial difficulties, the three half time counsellor positions for the Office of Student Affairs were created in the areas of career counselling, psychotherapy, and learning skills to improve student well‐being and enhance the student experience in our program (see Section 7.a. Student support – counselling and community building: Counselling).
Issue 5. A description of changes made in curriculum to identify specific curriculum content deficiencies identified in the selfstudy (pharmacology, nutrition, genetic counselling, palliative and endoflife care). (ED11 & ED13)
Response 5. • Pharmacology: The curriculum has been significantly updated to ensure that
pharmacology teaching is being appropriately identified and delivered including the development of on‐line resources to enhance self‐directed learning as well as
continuing and professional education. • ods to Nutrition: Course Directors continue to modify course content and delivery meth
include identified gaps in the curriculum. For example: Metabolism & Nutrition (MNU) – A new nutrition seminar has been introduced. Pathobiology of Disease (PBD) – The role of diet in cancer prevention is now discusin the context of neoplasia pathology.
sed
Surgery Clerkships – Deficiencies in nutrition curriculum have been highlighted to teachers during faculty development sessions.
• Genetic Counselling: Students now acquire an understanding of genetic counselling through several Preclerkship courses, most notably Structure & Function (STF), Metabolism & Nutrition (MNU) and Pathobiology of Disease (PBD).
• End‐of‐Life and Palliative Care: In the Preclerkship, this topic is mainly addressed during the two second‐year block courses, PBD and Foundations of Medical Practice (FMP). Palliative and end‐of‐life care concepts have been heavily revised and reinforced in these courses and those in Year 1 to ensure that students develop a comprehensive basis for future learning. In addition, seminars on these topics have been introduced in the Clerkship.
Issue 6. An outline or table showing the general competencies expected of graduates, the institutional earning objectives related to each competency, and any outcome measures implemented to ssess achievement of each listed objective. la
Undergraduate Medical Education Review 2005‐2010
16
Response 6. In response to this issue and after considerable deliberation, a comprehensive table was created, outlining the ways in which the new faculty goals and objectives are taught and how we measure the degree to which students have achieved them. Overall outcomes for the curriculum and the competencies expected of medical students at the time of graduation have been identified and documented, with the measures of evaluation noted for each.
Issue 7. (a) A table showing, for each of the last five years, the average cost of attendance (financial aid budget) per student, the total amount of financial aid funded by educational loans for all enrolled students, the total amount of financial aid funded by institutional grants and scholarships for all enrolled students, the total amount funded by self help (such as work study programs) for all enrolled students, and the percentage of enrolled students receiving institutional grants and scholarships; and (b) a narrative summary of any outcomes for students from institutional efforts to freeze tuition and increase studen financial aid. t
Response 7. (a)The relevant statistics regarding financial aid over the past five years have been identified and documented. The figures show that while the total financial aid determined as necessary continues to increase, the amount of aid provided has also increased significantly. (b) In response to a 4.5% average increase in university tuition fees, a recommendation was accepted by the University of Toronto Governing Council that medical school tuition increases be limited to 2%, reflecting inflation only (see Section 6. Student support – financial aid and awards).
Issue 8. A summary of any changes made to strengthen financial aid counselling, including an update on staffing in Office of Faculty Admissions and Awards.
Response 8. New positions in the Office of Student Financial Services, including the new full‐time position of Associate Registrar, Student Financial Services, were created. Financial counselling is now available to all students through both the Associate Registrar and the Financial Counsellor. Incoming students are mandated to meet with our financial counselling staff upon acceptance of an offer of admission to UME. Students are represented on a newly expanded Student Finance Committee, and have provided positive comments regarding the enhanced counselling and financial aid made available in the last three years.
Undergraduate Medical Education Review 2005‐2010
17
Issue 9. An update on the availability of an adequate pool of faculty tutors for small group learning, including tutors for the ASCM, DOCH (Year 1) and FMP (Year 2). Describe any adjustments in the size or frequency of small group learning experiences related to availability of faculty tutors.
Response 9. Several recent interventions have facilitated and improved the recruitment and training of tutors: First, the Hospital University Education Committee sponsored an agreement outlining xpectations for each of the clinical departments with respect to the number of teachers each edepartment would provide. Secondly, the Centre for Faculty Development was established at St. Michael’s Hospital, roviding a range of opportunities for faculty development. We continue to provide course‐pecific faculty development for tutors in problem‐based learning. ps
IU
ssue 10. pdated affiliation agreements for the primary and partial clinical affiliates.
Response 10. Existing affiliation agreements were reviewed in close consultation with the senior leaders and legal counsel of both the fully‐affiliated and community‐affiliated partner institutions. The language in the agreements has been revised and refined to meet the needs of both the University of Toronto and our partner constituencies. The sections on teaching responsibilities and obligations have been strengthened.
With the announcement of an additional 35 undergraduate medical spaces at the University of Toronto, the development of the Mississauga Academy has gained further momentum. The LCME and CACMS will hold a consultation visit to review the expansion plans and preparations in February 2010. Looking forward, the current accreditation status enjoyed by the undergraduate MD program will last until 2012, but we will not rest on our laurels. Self‐study planning activities will begin shortly to prepare for the next full accreditation survey to take place that year, and I will be appointing a Senior Academic Coordinator to oversee that process shortly. As an overall index of satisfaction with our medical education program, the following table shows the five‐year trend on the Canadian Graduation Questionnaire of our students’ responses to the question Please rate the quality of your medical education” compared to national averages: “

Undergraduate Medical Education Review 2005‐2010
20052009 Canadian Medical School Graduation Questionnaire
Results: Question 18a. Please rate the quality of your medical education: University of Toronto All Schools 2 005 2 006 2 007 2 008 2 009 2 009Excellent 3 5.4 62.3 40.0 33.0 43.8 24.6 Very Good 5 2.4 31.9 42.9 54.3 47.5 50.7 Good 9.8 5.8 14.3 12.8 6.3 19.4 Fair 2.4 0.0 2.9 0.0 2.5 4.8 Poor 0.0 0.0 0.0 0.0 0.0 0.4 Total 100.0 100.0 100.0 100.0 100.0 100.0 Number of Responses
82 69 70 94 80 1222
URRICULAR ENRICHMENT OPPORTUNITIES FOR STUDENTS C
18
a. Redevelopment of electives and selectives
Electives represent a significant tool for career sampling available for our students, and as such, their structure, placement, and support within the curriculum are of considerable importance. At the Preclerkship level, our new Electives Director, Dr. Mara Goldstein, has moved to formalize student shadowing opportunities as Enriching Educational Experiences (EEEs). While these placements will not be mandatory, nor will they be transcripted, this structure will help boost equity of shadowing opportunities among students (by providing them with a roster of potential preceptors instead of making them dependant on personal contacts), ensure appropriate oversight and understanding of student capabilities by the faculty and community doctors whom they shadow, and enable tracking of students’ experiences for legal, insurance, and potentially research purposes. The Student Career Exploration Program, a new student‐driven initiative, is participating actively in the creation of the EEE program to facilitate placements.
A GH [global health] student representative
position has been created on the Electives Committee to
foster increased appreciation of the opportunities we
already offer and those we have yet to explore.
Undergraduate Medical Education Review 2005‐2010
19
UME is also mindful of its global health (GH) role with regard to electives. A GH student representative position has been created on the Electives Committee to foster increased appreciation of the opportunities we already offer and those we have yet to explore. As but one example, we have fostered elective options that combine clinical exposure with social responsibility on topics such as HIV. When the new Clerkship structure is implemented, including the introduction of a menu of selectives, we anticipate the possibility of further enhancing the possibilities for mandating socially responsible clinical experiences.
With respect to the visiting elective program, which is also part of our role in the global health care network, we are continuously weighing our hospital affiliates’ capacity to accommodate our own students for core rotations and electives, while affording as many Canadian and international students as feasible the chance to benefit from the unique learning experiences in Toronto. International students are now accepted in the last two years of their programs, only between January and June; these changes are designed to maximize the elective opportunities available to our students in the all‐important Pre‐CaRMS period, and they also help ensure that our preceptors
ill levels. encounter international students with appropriate sk
(For changes to the electives application process, see Section 4. f. Technological solutions for electives management.)
b. Longitudinal clinical experiences – FMLE and Paediatrics LE pilots
As described previously, we are now in the third year of a pilot for the Family Medicine Longitudinal Experience (FMLE), which grew out of the recommendations of the Generalism Task Force. I am strongly supportive of this initiative, as it meets the needs of our Preclerkship students seeking greater clinical exposure while also ensuring the centrality of generalism in our curriculum. Moving forward, the FMLE will become an integral part of the UME program and we have laid the foundation for it to grow through the establishment of both faculty and administrative positions to support the project.
In addition to the Department of Family Medicine, the Department of Paediatrics is also piloting a longitudinal preclinical experience. Other departments have introduced activities for Preclerkship students as well, and we are exploring the possibility of moving towards a menu of selectives that students in Years 1 and 2 will choose from, in parallel to what is planned in the Clerkship.
c. Leadership program
As part of the new Manager curriculum described above, all of our students will be exposed to leadership principles. For those students with a particular interest and aptitude for leadership, we have launching a new longitudinal “LEAD” program this fall, spearheaded by Dr. Geoff Anderson. Each year, sixteen students will be recruited to participate in the program, which will consist of courses, networking opportunities, and experience working on real projects as part of summer
ive collaboration between UME, placements and electives. The LEAD program represents an innovat

Undergraduate Medical Education Review 2005‐2010
the Department of Health Policy, Management, and Evaluation, the School for Public Policy and Governance, and the Rotman School of Business, and is aimed at developing physicians who have the skills and knowledge to take up academic and public service leadership positions over the course of their careers.
the Department of Health Policy, Management, and Evaluation, the School for Public Policy and Governance, and the Rotman School of Business, and is aimed at developing physicians who have the skills and knowledge to take up academic and public service leadership positions over the course of their careers.
The LEAD program represents an innovative collaboration between UME, the Department of Health Policy, Management, and Evaluation, the School for Public
Policy and Governance, and the Rotman School of Business…
d. Expansion of research opportunities and the creation of CREMS
Prior to 2006, UME students were limited to a summer research program lasting twelve weeks – a period that for some was sufficient to get a taste for research, but that in many cases proved too short to accomplish their goals. Consequently, beginning in the summer of 2006, we folded the existing summer research program into a broader initiative with different streams depending on a student’s interest: the Comprehensive Research Experience for Medical Students (CREMS), led by the newly‐appointed director, Dr. Don Branch. Under this program (see Appendix 3.1
d. Expansion of research opportunities and the creation of CREMS
Prior to 2006, UME students were limited to a summer research program lasting twelve weeks – a period that for some was sufficient to get a taste for research, but that in many cases proved too short to accomplish their goals. Consequently, beginning in the summer of 2006, we folded the existing summer research program into a broader initiative with different streams depending on a student’s interest: the Comprehensive Research Experience for Medical Students (CREMS), led by the newly‐appointed director, Dr. Don Branch. Under this program (see Appendix 3.1) program Preclerkship students engage in quality, funded research with faculty members in the basic sciences, clinical sciences, or public health for lengths of time ranging from the original twelve weeks (the summer between first and second year) to a full year (bridging first and second year), with a possible
continuation into the summer before third year for students whose research shows exceptional promise. CREMS has proven highly successful and is viewed by students as a way to gain new skills and differentiate themselves from other applicants for residency. Hundreds of students have participated already, and we expect the numbers to remain constant in future. Identifying stable sources of funding does remain an ongoing challenge. This year, in partnership with the Ontario Medical Student’s Association (OMSA) and the Faculty of Medicine at the University of Toronto, I supported an expansion of the annual Medical Student Research Day to include all six Ontario medical schools (see Appendix 3.2). With the involvement of over 40 faculty members and over 160 medical students, the inaugural Ontario Medical Student Research Day was
20
considered a great success.
To further bolster our research partnerships, we have created another senior faculty position, Director of Physician Scientist Training Programs. This position is held by Dr. Norman Rosenblum, who is also the Director of our MD/PhD program and the Royal College Clinician Investigator (CIP) program. Dr. Rosenblum is working to expand the availability of longitudinal, in‐depth research programs for our students that will bridge their undergraduate and post‐graduate medical training.
With the involvement of
over 40 faculty members
and over 160 medical
students, the inaugural
Ontario Medical Student
Research Day was
considered a great
success.

Undergraduate Medical Education Review 2005‐2010
21
e. Joint degrees and partnerships with other Faculties
For students with a more focussed interest in research, we are proud to offer a variety of what I term “MD Plus” opportunities, whereby students can pursue another degree or enrichment opportunity concurrent with the MD. UME has run a comparatively small but prestigious MD/PhD program for close to 25 years. This program is specifically intended for students who wish to engage in biomedical research, but I am increasingly approached by students and prospective applicants who would like to pair their interests in medicine with less traditional fields. We recognize the value to UME in attracting students whose talents exceed one narrow domain, and the value to society in training these individuals to contribute to medicine in their own ways. To appeal to the diversity of student interests and backgrounds our new Director of Physician Scientist Training Programs is organizing exciting initiatives with the Faculty of Engineering and the Rotman School of Business to establish joint degrees between these fields at the Masters and PhD levels. In addition, Dr. Ian Johnson, Course Director of Determinants of Community Health 1‐4, is actively engaged in the development of a new MD/MPH degree in partnership with the Dalla Lana School of Public Health. We expect that these new opportunities will prove popular with our students and will help cement our reputation as the best medical school in Canada for academically‐oriented candidates wishing a variety of enrichment and individualized curriculum opportunities..
f. Curriculum Renewal Fund
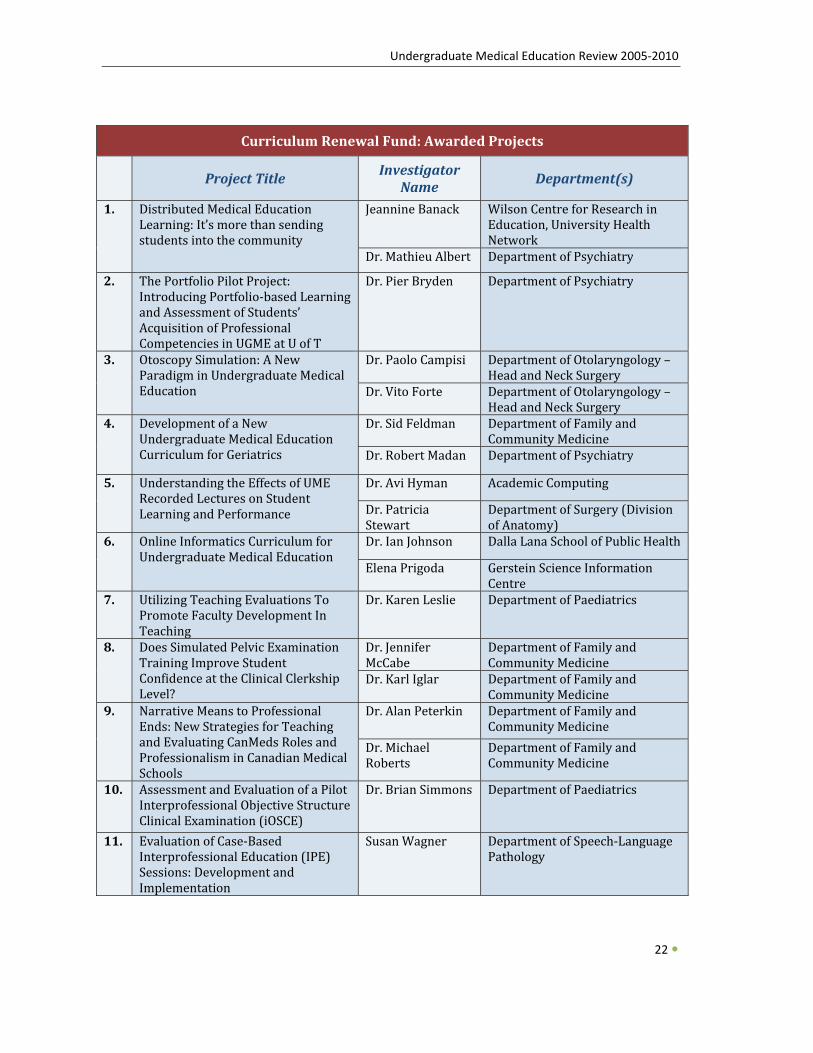
The Ministry of Health and Long‐Term Care (MOHLTC) provided the Council of Ontario Faculties of Medicine (COFM) with $1.8m in funding to establish a curriculum renewal fund to promote innovation in medical education in Ontario. From this amount, the Undergraduate Medical Education program at the University of Toronto was allocated $163,443.10. I chose to utilize this generous allocation by conducting a grant competition, through which funding was awarded to 11 projects in the following key areas:
• Distributed medical education; and/or flexible delivery of curriculum;
• pment for community preceptors; and • Collaborative
Faculty develo• Primary care.
The approved projects were scheduled to commence in May 2009 with a duration of 12 months. The project results are expected to be presented at the Faculty’s 2010 Educational Achievement Event.
Undergraduate Medical Education Review 2005‐2010
22
Curriculum Renewal Fund: Awarded Projects
Project Title
Investigator Name
Department(s)
1. Distributed Medical Education Learning: It’s more than sending students into the community
Jeannine Banack Wilson Centre for Research in Education, University Health Network
Dr. Mathieu Albert Department of Psychiatry
2. The Portfolio Pilot Project: Introducing Portfolio‐based Learning and Assessment of Students’ Acquisition of Professional Competencies in UGME at U of T
Dr. Pier Bryden Department of Psychiatry
3. Otoscopy Simulation: A New Paradigm in Undergraduate Medical Education
Dr. Paolo Campisi Department of Otolaryngology –Head and Neck Surgery
Dr. Vito Forte Department of Otolaryngology –Head and Neck Surgery
4. Development of a New Undergraduate Medical Education Curriculum for Geriatrics
Dr. Sid Feldman Department of Family and Community Medicine
Dr. Robert Madan Department of Psychiatry
5. Understanding the Effects of UMERecorded Lectures on Student Learning and Performance
Dr. Avi Hyman Academic Computing
Dr. Patricia Stewart
Department of Surgery (Division of Anatomy)
6. Online Informatics Curriculum for Undergraduate Medical Education
Dr. Ian Johnson Dalla Lana School of Public Health
Elena Prigoda Gerstein Science Information Centre
7. Utilizing Teaching Evaluations To Promote Faculty Development In Teaching
Dr. Karen Leslie Department of Paediatrics
8. Does Simulated Pelvic Examination Training Improve Student Confidence at the Clinical Clerkship Level?
Dr. Jennifer McCabe
Department of Family and Community Medicine
Dr. Karl Iglar Department of Family and Community Medicine
9. Narrative Means to Professional Ends: New Strategies for Teaching and Evaluating CanMeds Roles and Professionalism in Canadian Medical Schools
Dr. Alan Peterkin Department of Family and Community Medicine
Dr. Michael Roberts
Department of Family and Community Medicine
10. Assessment and Evaluation of a Pilot Interprofessional Objective Structure Clinical Examination (iOSCE)
Dr. Brian Simmons Department of Paediatrics
11. Evaluation of Case‐Based Interprofessional Education (IPE) Sessions: Development and Implementation
Susan Wagner Department of Speech‐Language Pathology

Undergraduate Medical Education Review 2005‐2010
PARTNERSHIPS WITH HOSPITALS IN THE STUDENT XPERIENCE PARTNERSHIPS WITH HOSPITALS IN THE STUDENT XPERIENCE EE
a. Academies
The Academies are our students’ clinical bases in all four years of the program. Over the past five years, they have all grown and developed new initiatives to meet the needs of their students and their hospital communities.
Peters‐Boyd The Peters‐Boyd Academy, under the direction of Dr. Leslie Nickell, has successfully navigated the de‐merger of its two hospitals, Sunnybrook Health Sciences Centre and Women’s College Hospital, while maintaining its educational partnerships with these two core sites as well as with North York General. It has accommodated an additional 12 students per year (66, up from 54 in 2005), in part through productive partnerships with community hospitals; at the Preclerkship level, the Scarborough Hospital and Markham FHT have both hosted ASCM 1 students from Peters‐Boyd in ambulatory care settings since 2005, while North York General Hospital has taken students for ASCM 1, ASCM 2, and DOCH 1. Such relationships with community affiliates serve to introduce more students to primary care settings from the earliest stages of their training, while also helping to ensure that students are not overcrowded in clinical settings.
In addition, the Peters‐Boyd Academy has worked to improve the students’ learning and study environment through a renovation to the dedicated lounge space and AV enhancements in all teaching rooms. P‐B has also increased the social activities on offer, and the introduction of “Academy Days” in the Preclerkship means that students at our furthest core site (Sunnybrook) are able to spend more time at the Academy and less time in transit to get there.
23
http://www.md.utoronto.ca/partners/academies/Peters‐boyd
Undergraduate Medical Education Review 2005‐2010
P‐B has also developed an innovative solution to a problem that has plagued all of the core teaching sites: the lack of suitable patients for basic clinical skills practice. In view of the high proportion of tertiary and quaternary‐care patients whose conditions make them inappropriate for student practice in Years 1 and 2, Peters‐Boyd launched the patient volunteer program, whereby patients in the family practice unit are recruited to attend ASCM sessions outside of their regular appointments. This model has proved highly successful and has now been adopted at other hospitals, including the
P‐B has also developed an innovative solution to a problem that has plagued all of the core teaching sites: the lack of suitable patients for basic clinical skills practice. In view of the high proportion of tertiary and quaternary‐care patients whose conditions make them inappropriate for student practice in Years 1 and 2, Peters‐Boyd launched the patient volunteer program, whereby patients in the family practice unit are recruited to attend ASCM sessions outside of their regular appointments. This model has proved highly successful and has now been adopted at other hospitals, including the Wightman‐Berris sites.
With Dr. Nickell taking on the role of Associate Dean, Health Professions Student Affairs, as of July 2009, the search will now commence to identify her successor. We are grateful to Dr. Nickell for her tremendous efforts at Peters‐Boyd, and recognize the high standards she has set for the next Academy Director. Dr. Catherine Kelly is graciously serving as Interim Academy Director in the meantime.
Wightman‐Berris sites.
With Dr. Nickell taking on the role of Associate Dean, Health Professions Student Affairs, as of July 2009, the search will now commence to identify her successor. We are grateful to Dr. Nickell for her tremendous efforts at Peters‐Boyd, and recognize the high standards she has set for the next Academy Director. Dr. Catherine Kelly is graciously serving as Interim Academy Director in the meantime.
Wightman‐Berris At the Wightman‐Berris Academy, a change in leadership was necessitated by the sudden loss of our dear friend, Dr. John Bradley, in 2006. Dr. Jacqueline James stepped into the breach as W‐B Academy Director, in addition to maintaining her role as ASCM 2 Course Director, and has proved to be as successful at steering our largest Academy as John was. Over the past few years, the W‐B has seen the opening of the Sydney and Florence Cooper Family Education Centre at Mount Sinai Hospital (MSH), a state‐of‐the art teaching area featuring videoconferencing, new computer labs, and smart boards in seminar rooms. IT upgrades and other improvements were also applied to the medical education acilities at Toronto Western Hospital (TWH) and Toronto General Hospital (TGH).
Wightman‐Berris At the Wightman‐Berris Academy, a change in leadership was necessitated by the sudden loss of our dear friend, Dr. John Bradley, in 2006. Dr. Jacqueline James stepped into the breach as W‐B Academy Director, in addition to maintaining her role as ASCM 2 Course Director, and has proved to be as successful at steering our largest Academy as John was. Over the past few years, the W‐B has seen the opening of the Sydney and Florence Cooper Family Education Centre at Mount Sinai Hospital (MSH), a state‐of‐the art teaching area featuring videoconferencing, new computer labs, and smart boards in seminar rooms. IT upgrades and other improvements were also applied to the medical education acilities at Toronto Western Hospital (TWH) and Toronto General Hospital (TGH). f
f
http://www.md.utoronto.ca/partners/academies/Wightman‐Berris.htm
24
Undergraduate Medical Education Review 2005‐2010
The W‐B has also moved forward with regard to interprofessional education, piloting two IPE sessions for clerks at MSH and TGH. In addition, the Academy‐based Passport to Clerkship sessions have been modified to highlight the roles of teams and allied health professionals. To further this trend towards integration, rehabilitation students are now welcome to make use of the Helliwell
The W‐B has also moved forward with regard to interprofessional education, piloting two IPE sessions for clerks at MSH and TGH. In addition, the Academy‐based Passport to Clerkship sessions have been modified to highlight the roles of teams and allied health professionals. To further this trend towards integration, rehabilitation students are now welcome to make use of the Helliwell Centre at TGH, as are MD students from the other Academies.
On the community side, Wightman‐Berris has developed relationships with Toronto East General Hospital (TEGH) and Credit Valley Hospital (CVH). Students now attend TEGH for ASCM 1, 2, and DOCH 2 research, and CVH for ASCM 1 and 2. Just as for P‐B students at NYGH and the Scarborough hospitals, W‐B students benefit from the far lower student‐patient ratio at the community sites and the exposure to patient encounters that are not always available in the tertiary and quaternary care
Centre at TGH, as are MD students from the other Academies.
On the community side, Wightman‐Berris has developed relationships with Toronto East General Hospital (TEGH) and Credit Valley Hospital (CVH). Students now attend TEGH for ASCM 1, 2, and DOCH 2 research, and CVH for ASCM 1 and 2. Just as for P‐B students at NYGH and the Scarborough hospitals, W‐B students benefit from the far lower student‐patient ratio at the community sites and the exposure to patient encounters that are not always available in the tertiary and quaternary care environments of TGH, TWH, and MSH.
The W‐B has also expanded its profile internationally by piloting an exchange program, now in its second year, to welcome a small number of clerks from Shanghai Medical School to undertake core rotations in Medicine and Surgery.
environments of TGH, TWH, and MSH.
The W‐B has also expanded its profile internationally by piloting an exchange program, now in its second year, to welcome a small number of clerks from Shanghai Medical School to undertake core rotations in Medicine and Surgery.
Looking ahead, Wightman‐Berris has plans to pilot optional lunch‐time sessions on Academy Days on topics such as career counselling and mentorship with staff or postgraduate trainees. They are also working to create a small simulation centre for students to practise IV placement and other minor procedures.
Looking ahead, Wightman‐Berris has plans to pilot optional lunch‐time sessions on Academy Days on topics such as career counselling and mentorship with staff or postgraduate trainees. They are also working to create a small simulation centre for students to practise IV placement and other minor procedures.
The Academies are our students’ clinical bases in all four years of the program. Over
the past five years, they have all grown and developed new initiatives to meet the needs
of their students and their hospital communities.
FitzGerald At the FitzGerald Academy, Dr. Vince Chien has prioritized the role of technology in the student experience. Antiquated computer labs with unusable internet service were overhauled in 2005. This was followed two years later with renovation of the classrooms to incorporate smart boards and other learning technology. The “Fitz” also served as an early beta site for the roll‐out of MedSIS (see Section 4.e. Student information system and electronic evaluations
FitzGerald At the FitzGerald Academy, Dr. Vince Chien has prioritized the role of technology in the student experience. Antiquated computer labs with unusable internet service were overhauled in 2005. This was followed two years later with renovation of the classrooms to incorporate smart boards and other learning technology. The “Fitz” also served as an early beta site for the roll‐out of MedSIS (see Section 4.e. Student information system and electronic evaluations) in an effort to streamline its administrative activities, and it has also championed LinkHealthPro. This online application, the brainchild of Dr. Chien and Knowledge4You Corporation, facilitates mentorship opportunities within and across health care professions, and is open to individuals at all stages in their career, including students. Dr. Chien has also been instrumental in the creation and uptake of video‐based learning modules to support curricular activities.
25
Undergraduate Medical Education Review 2005‐2010
26
Even greater changes are eagerly anticipated by the FitzGerald Academy as its new home in the Li Ka Shing Knowledge Institute at St. Michael’s Hospital is scheduled to open in 2010. The Li Ka Shing Knowledge Institute is designed to bring together the worlds of research, education, and patient care to emphasize rapid knowledge translation of best practices in health care. Our students will benefit from close encounters with teachers and scientists, and also from improved infrastructure. The new space will feature modern teaching and social spaces for students, including the latest advances in
Even greater changes are eagerly anticipated by the FitzGerald Academy as its new home in the Li Ka Shing Knowledge Institute at St. Michael’s Hospital is scheduled to open in 2010. The Li Ka Shing Knowledge Institute is designed to bring together the worlds of research, education, and patient care to emphasize rapid knowledge translation of best practices in health care. Our students will benefit from close encounters with teachers and scientists, and also from improved infrastructure. The new space will feature modern teaching and social spaces for students, including the latest advances in
http://www.md.utoronto.ca/partners/academies/FitzGerald.htm
information technology.
Like the other Academies, the FitzGerald Academy has also embarked on increasing partnerships with community sites in recent years, including Bridgepoint Health, St. Joseph’s Health Centre, and Trillium Health Centre for the delivery of Preclerkship and Clerkship instruction. The Fitz has also created ties with George Brown College, a collaboration that has produced unique interprofessional community health research experiences in the DOCH 2 course for our students. This innovative partnership marks the first core curricular collaboration between a Faculty of Medicine and a college in Canada. As Vince Chien steps down now, I thank him for his stellar work at the Fitz and his edication to students.
information technology.
Like the other Academies, the FitzGerald Academy has also embarked on increasing partnerships with community sites in recent years, including Bridgepoint Health, St. Joseph’s Health Centre, and Trillium Health Centre for the delivery of Preclerkship and Clerkship instruction. The Fitz has also created ties with George Brown College, a collaboration that has produced unique interprofessional community health research experiences in the DOCH 2 course for our students. This innovative partnership marks the first core curricular collaboration between a Faculty of Medicine and a college in Canada. As Vince Chien steps down now, I thank him for his stellar work at the Fitz and his edication to students. d
d
b. Community hospitals
As noted above, our Academies have all embraced community ties over the past few years at the Preclerkship level. At the Clerkship level, we have a longstanding relationship with many community hospitals both within and separate from the Academy model, and our students’ presence at these sites continues to grow in a trend of distributed medical education (DME) that has been adopted all over the world. In Years 3 and 4, students particularly benefit from the chance to become more involved in patient care without “competition” from their peers and residents; exposure to community practice also encourages our students to give serious consideration to careers outside
b. Community hospitals
As noted above, our Academies have all embraced community ties over the past few years at the Preclerkship level. At the Clerkship level, we have a longstanding relationship with many community hospitals both within and separate from the Academy model, and our students’ presence at these sites continues to grow in a trend of distributed medical education (DME) that has been adopted all over the world. In Years 3 and 4, students particularly benefit from the chance to become more involved in patient care without “competition” from their peers and residents; exposure to community practice also encourages our students to give serious consideration to careers outside

Undergraduate Medical Education Review 2005‐2010
urban centres and the medical science institutions. In addition, the students encounter different patient profiles at each site, thereby better preparing them for the profession. Community experience also allows students to see first‐hand the importance and rewards of generalist practice in the pectrum of medical care.
urban centres and the medical science institutions. In addition, the students encounter different patient profiles at each site, thereby better preparing them for the profession. Community experience also allows students to see first‐hand the importance and rewards of generalist practice in the pectrum of medical care. s
s
In view of the central role that our community affiliates play in the training of our students, we recognized the need for senior faculty leadership to have insight into the unique issues these sites face. A new position, Director of Distributed Medical Education, was created in 2006 and Dr. Adrian Brown from North York General Hospital was appointed. Furthermore, we are moving towards more formal linkages between the Academies and community‐affiliated hospitals beyond the somewhat ad hoc partnerships currently in place. The Academy Directors are now working with me on a policy document entitled Academy Roles and Governance to help advance us in this direction. This will ensure a greater oversight and flow of ideas around medical education than currently exists. In addition, we have recently signed a new agreement with the Rural Ontario Medical Program (ROMP) to facilitate even more placements for our students in communities outside of our immediate network. All of these initiatives are informed by the recommendations of the recently completed external review of DME by Carol Herbert and Joanna Bates, which set new directions for an
In view of the central role that our community affiliates play in the training of our students, we recognized the need for senior faculty leadership to have insight into the unique issues these sites face. A new position, Director of Distributed Medical Education, was created in 2006 and Dr. Adrian Brown from North York General Hospital was appointed. Furthermore, we are moving towards more formal linkages between the Academies and community‐affiliated hospitals beyond the somewhat ad hoc partnerships currently in place. The Academy Directors are now working with me on a policy document entitled Academy Roles and Governance to help advance us in this direction. This will ensure a greater oversight and flow of ideas around medical education than currently exists. In addition, we have recently signed a new agreement with the Rural Ontario Medical Program (ROMP) to facilitate even more placements for our students in communities outside of our immediate network. All of these initiatives are informed by the recommendations of the recently completed external review of DME by Carol Herbert and Joanna Bates, which set new directions for an
Community experience also allows students to see first-hand the importance and rewards of generalist practice in the spectrum of medical care.
integrated network system (see Appendix 4.1integrated network system (see Appendix 4.1).
27
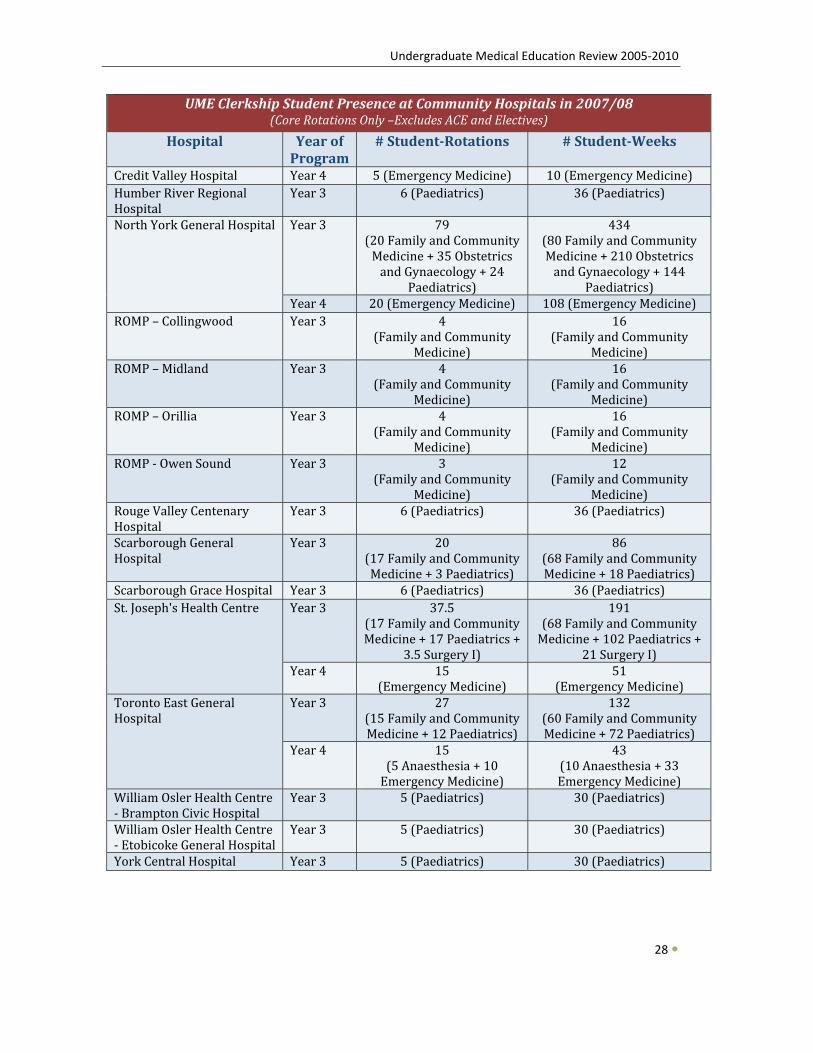
Undergraduate Medical Education Review 2005‐2010
28
UME Clerkship Student Presence at Community Hospitals in 2007/08 (Core Rotations Only –Excludes ACE and Electives)
Hospital Year of Program
# StudentRotations # StudentWeeks
Credit Valley Hospital Year 4 5 (Em cine)ergency Medi 10 (E ine)mergency MedicHumber River Regional Hospital
Year 3 6 (Pae trics)dia 36 (Pa trics)edia
North York General Hospital
Year 3 79(20 Family and Community Medicine + 35 Obstetrics and Gynaecology + 24
Paedi trics) a
434 (80 Family and Community Medicine + 210 Obstetrics and Gynaecology + 144
Paed ics) iatrYear 4 20 (Emergency Medicine) 1 )08 (Emergency Medicine
ROMP – Collingwood Year 3 4(Family and Community
Medicine)
16 (Family an ommunity d C
Medicine) ROMP – Midland Year 3 4
(Family and Community Medicine)
16 (Family an ommunity d C
Medicine) ROMP – Orillia Year 3 4
(Family and Community Medicine)
16 (Family an ommunity d C
Medicine) ROMP ‐ Owen Sound Year 3 3
(Fam nity ily and CommuMedicine)
12 (Fam nity ily and Commu
Medicine) Rouge Valley Centenary Hospital
Year 3 6 (Pae trics)dia 36 (Pa cs)ediatri
Scarborough General Hospital
Year 3 20(17 Fa unity mily and CommMedi trics) cine + dia 3 Pae
86 (68 Fa unity mily and CommMedi rics) cine + aediat18 P
Scarborough Grace Hospital Year 3 6 (Paediatrics) 36 (Paediatrics)St. Joseph's Health Centre
Year 3 37.5(17 Family and Community Medicine + 17 Paediatrics +
3.5 Surgery I)
191 (68 Family and Community Medicine + 102 Paediatrics +
21 Surgery I) Year 4 15
(Emergency Medicine) 51
(Emergency Medicine) Toronto East General Hospital
Year 3 27(15 Family a Community ndMed cs) icine + 12 Paediatri
132 (60 Family a Community nd Me s) dicine + 72 Paediatric
Year 4 15(5 10 Anaesthesia + Em ne) ergency Medici
43 (1 3 0 Anaesthesia + 3Em e) ergency Medicin
William Osler Health Centre ‐ Brampton Civic Hospital
Year 3 5 (Paediatrics) 30 (Paediatrics)
William Osler Health Centre ‐ Etobicoke General Hospital
Year 3 5 (Paediatrics) 30 (Paediatrics)
York Central Hospital Year 3 5 (Paediatrics) 30 (Paediatrics)
Undergraduate Medical Education Review 2005‐2010
c. Creation of the Mississauga Academy
Undoubtedly the largest project undertaken in UME since 2005 is the expansion of the medical school and the creation of a fourth Academy based at the UTM campus, Credit Valley Hospital (CVH), and Trillium Health Centre (THC). Dr. Pamela Coates was appointed as Mississauga Academy Director in 2006, and her strong background in hospital leadership at CVH has greatly assisted us in building a positive relationship with our partners. Dr. Coates is assisted in this endeavour by UME’s Special
c. Creation of the Mississauga Academy
Undoubtedly the largest project undertaken in UME since 2005 is the expansion of the medical school and the creation of a fourth Academy based at the UTM campus, Credit Valley Hospital (CVH), and Trillium Health Centre (THC). Dr. Pamela Coates was appointed as Mississauga Academy Director in 2006, and her strong background in hospital leadership at CVH has greatly assisted us in building a positive relationship with our partners. Dr. Coates is assisted in this endeavour by UME’s Special Projects Manager, Neil Neebar.
Although this project has met with a series of unforeseen delays over the past few years, it is with great excitement that we and our partners look forward to the opening of the new Academy in September 2011, as formally announced by the provincial government in May 2009. The slower‐than‐anticipated development has yielded a number of positive aspects, as it has allowed us to devote more time to carefully assessing our infrastructure requirements at each site and to building up a core of well‐trained teaching faculty in Mississauga without the pressures of significant student volume from the start. We have gradually introduced students to the Mississauga hospitals at both the Preclerkship level in ASCM 1, ASCM 2, and MNU, and in the Clerkship for courses such as Emergency Medicine and Family Medicine; importantly, our students’ enthusiasm for the project is growing and their initial concerns are subsiding as more and more of them experience training at CVH and THC first‐hand. The delays also provided us with the opportunity to think beyond the original small scope of the expansion, and so we were able to work with the government and our partner hospitals to develop a larger, more robust Academy of 54 students per year instead of just 36. With the greater number of students also comes a commitment of significant financial support from the government. Furthermore, whereas the UME students would previously have held a limited space on the UTM campus, they will now be part of a larger community occupying an impressive new Health Sciences Building. We have also begun laying the foundation for a full Academy human resources infrastructure, including faculty development exercises and the creation of a standardized patient
Projects Manager, Neil Neebar.
Although this project has met with a series of unforeseen delays over the past few years, it is with great excitement that we and our partners look forward to the opening of the new Academy in September 2011, as formally announced by the provincial government in May 2009. The slower‐than‐anticipated development has yielded a number of positive aspects, as it has allowed us to devote more time to carefully assessing our infrastructure requirements at each site and to building up a core of well‐trained teaching faculty in Mississauga without the pressures of significant student volume from the start. We have gradually introduced students to the Mississauga hospitals at both the Preclerkship level in ASCM 1, ASCM 2, and MNU, and in the Clerkship for courses such as Emergency Medicine and Family Medicine; importantly, our students’ enthusiasm for the project is growing and their initial concerns are subsiding as more and more of them experience training at CVH and THC first‐hand. The delays also provided us with the opportunity to think beyond the original small scope of the expansion, and so we were able to work with the government and our partner hospitals to develop a larger, more robust Academy of 54 students per year instead of just 36. With the greater number of students also comes a commitment of significant financial support from the government. Furthermore, whereas the UME students would previously have held a limited space on the UTM campus, they will now be part of a larger community occupying an impressive new Health Sciences Building. We have also begun laying the foundation for a full Academy human resources infrastructure, including faculty development exercises and the creation of a standardized patient program in Mississauga for clinical skills instruction and testing.
The recent announcement from the provincial government represents the realization of a long‐cherished goal in which our senior management team and our partners in Mississauga have invested considerable effort. We are naturally aware of the challenges we will face in the next two years as we ramp up to the official opening. Nevertheless, the increasing support from within the various facets of the UME community is very encouraging, and a constant reminder of the importance of this project.
program in Mississauga for clinical skills instruction and testing.
The recent announcement from the provincial government represents the realization of a long‐cherished goal in which our senior management team and our partners in Mississauga have invested considerable effort. We are naturally aware of the challenges we will face in the next two years as we ramp up to the official opening. Nevertheless, the increasing support from within the various facets of the UME community is very encouraging, and a constant reminder of the importance of this project.
29
… it is with great excitement that we and our partners look forward to the opening of the new Academy in September 2011…
Undergraduate Medical Education Review 2005‐2010
d. Hospital University Education Committee and Council of Education Deans
Over the past five years, both the Council of Education Deans (“Edudeans”) and the Hospital University Education Committee (HUEC) have made an impact in various ways on the Undergraduate Medical Education portfolio; in turn, my portfolio has influenced the policies and agenda items of
30
these two bodies.
The Council of Education Deans, formerly chaired by me, and consisting of the four Vice‐Deans of Education in the Faculty of Medicine, continues to evolve and grow as a unit advisory to the Dean of Medicine. Likewise, HUEC, which I now chair, is also in a state of change, revision, and reaffirmation nder my new leadership. u
The consultative nature of HUEC in particular allows the Undergraduate Medical Education portfolio to connect with all of our teaching hospitals.
The Council of Education Deans and HUEC are both forums for discussion and the development of education practices. In some cases, policies, guidelines, and recommendations are developed directly by these consultative groups, and in others they are brought to these two bodies from individual education portfolios, including UME. Guidelines for Appropriate Use of the Internet, Electronic Networking and other Media, is one such document developed within HUEC and now in place for our MD students; another example is the Standards of Professional Practice Behaviour. Also discussed at HUEC as part of the review and approval process was the proposed Credit/No‐Credit grading practice that has since received approval and been implemented for MD students beginning this academic year. There are at present a number of other proposals under review within various governance and advisory bodies, including the Policy on Protection of Digital Personal Health Information and a single, unifying mask‐fitting policy that would be applicable to all health professional learners.
The consultative nature of HUEC in particular allows the Undergraduate Medical Education portfolio to connect with all of our teaching hospitals, oftentimes filling the gap of knowledge about the full continuum of education offered in the Faculty of Medicine. To ensure student representation, the President of the Medical Society serves as a full member of HUEC, which has afforded him the opportunity to introduce the student governance structure to the other members and to highlight undergraduate issues to the Vice‐Presidents of Hospital Education who also sit on the Committee. Issues such as distributed medical education, the expansion to Mississauga, the capacity of our affiliated hospitals for education, insurance, student safety, criminal record checks, the future of medical education, remuneration, and clinical placements in the H1N1 pandemic have all been tabled for discussion at HUEC in recent months.
Looking forward, I will be spearheading a review of HUEC’s terms of reference, a process that we expect will serve to renew this committee and its relation to the new education committee struck by the Toronto Academic Health Sciences Network (TAHSN), and to refocus it on those items most crucial to the educational mission of the Faculty of Medicine MD students and residents.
Undergraduate Medical Education Review 2005‐2010
TTECHNOLOGY AND THE STUDENT EXPERIENCE ECHNOLOGY AND THE STUDENT EXPERIENCE
a. Partnership with the Discovery Commons
One of the most significant areas of change in UME falls under the umbrella of technology. We recognize that this generation of students is highly skilled in computing and expects access to state‐of‐the art technology to match these skills throughout their medical training. Building on our longstanding relationship with the Division of Academic Computing, we seized the opportunity to contribute significantly to the AV/IT future of the Faculty and our students. Through partnership in the establishment of the Discovery Commons (DC), the creation of a new UME‐funded positions in the DC to support videoconferencing and lecture video‐capture, and the transitioning of two UME staff members specializing in online course presence and evaluation analysis to join the DC, we have forged even stronger ties and opened up new opportunities for our students to reap the benefits of the latest technological advances. In all of the projects below, the DC and its leadership have played an instrumental role and we look forward to continued development with them. I have allocated ignificant resources from the UME budget for these critical IT initiatives. s
31
b. IT infrastructure in our learning spaces
One of our most tangible endeavours, which occurred concurrently with the building of the Discovery Commons in the Medical Sciences Building, was the much‐needed 2007 renovation of the two large lecture theatres used for all Year 1 and 2 large‐group sessions. This was the first time the theatres had undergone major improvements since the MSB was built in the 1960s, and we used the opportunity to outfit them with wireless hotspots, videoconference‐ready projection screens, high‐definition projectors, a new sound system, and power outlets at the desks; this was also the first
Undergraduate Medical Education Review 2005‐2010
project to adopt the new standard teaching podiums designed by the Office of Space Management for use across the campus. As part of the same project, we also built a new dissection lab and classroom in the Division of Anatomy; subsequently, we installed state of the art computers and screens this year at each dissection table, allowing students access to the latest digital anatomy resources alongside their gross dissections. We intend to seek funds in 2010 to bring video‐capture and projection to all the dissection labs as well. This technology has been implemented at other medical schools such as the Island Medical School in Victoria, and has proved to be an asset for students and nstructors alike. i
c. Digital capture of course materials and online presence
Our courses have also embraced new technological possibilities to the benefit of students. In the Preclerkship, most lectures are now screen‐ and audio‐captured and then posted online as streaming videos, so that students can review the slides while listening to the lecturer’s voice and seeing his or her on‐screen annotations. From its inception in the fall of 2008, this project has been exceptionally
successful, with each lecture typically being viewed hundreds of times. In addition, a pilot in our DOCH 2 course in 2008 featured pre‐recorded lecture material to facilitate team‐based learning, and it too was well received by students. As mentioned earlier, the UME Curriculum Committee has adopted a policy requiring all large‐group sessions to be captured in permanent digital media going forward.
32

Undergraduate Medical Education Review 2005‐2010
Videoconferencing has also been used for several years to connect students at community affiliated hospitals with the fully‐affiliated hospitals; our use of videoconferencing will continue to grow, especially in 2011/12 when the Mississauga Academy opens its doors to its first class. Videoconferencing reduces the need for travel and hence wasted time, it reinforces our students’
33
sense of cohesion with their classmates, and it promotes standardization across sites.
Students are also benefitting from the improved web presence of our courses. Since 2006/07, our courses have transitioned from individually‐maintained web pages on the library’s server and others to exclusive use of the University of Toronto Portal. Hence, students now experience the convenience of a single logon to access all their course materials, and course directors can communicate directly with the class through the notification feature in Blackboard instead of relying on academic listserv messages. In addition, through a tremendous coordinated effort involving the Discovery Commons and UME staff, access to the Portal has been obtained for hundreds of teachers so that they can be apprised of what the students are learning and coordinate their own contributions to each course accordingly.
One of the most significant areas of change in UME falls under the umbrella of technology.
d. IT contributions to curricular improvement
Other tools are enabling our students to take an active role in their learning. In the Clerkship, where learning becomes more self‐directed and also dependent on the vagaries of clinical practice, a PDA‐ and web‐based tool named My Practice Portfolio (previously “eLog”) enables students and faculty to monitor exposure to different types of cases and fulfillment of curricular objectives. The tool serves as a basis for formative feedback from faculty, and by comparing individual student‐patient encounters to the average, the students and their preceptors can take steps to fill any gaps. Course directors can also use My Practice Portfolio to identify important variations between sites with respect to patient profiles. We are now working with the Discovery Commons to develop cross‐course functionality in My Practice Portfolio with respect to both procedures and objectives; this will enable us to identify patterns of weakness in individual students and areas for improvement in the curriculum as a whole. In addition, we are exploring the possibility of introducing My Practice
ier. Portfolio in the Preclerkship for student clinical placements via the FMLE and EEEs described earl
In the Preclerkship, we are also conducting a pilot project with “clickers,” a technology popular in large‐group teaching such as lectures that allows students to interact with instructors through electronic voting. Teachers can ask students to indicate whether they have understood a concept or quiz the class with multiple‐choice‐type questions, thereby ascertaining whether the lecture content has been absorbed. We are currently considering full support for our students to access this technology in future without any out‐of‐pocket costs.
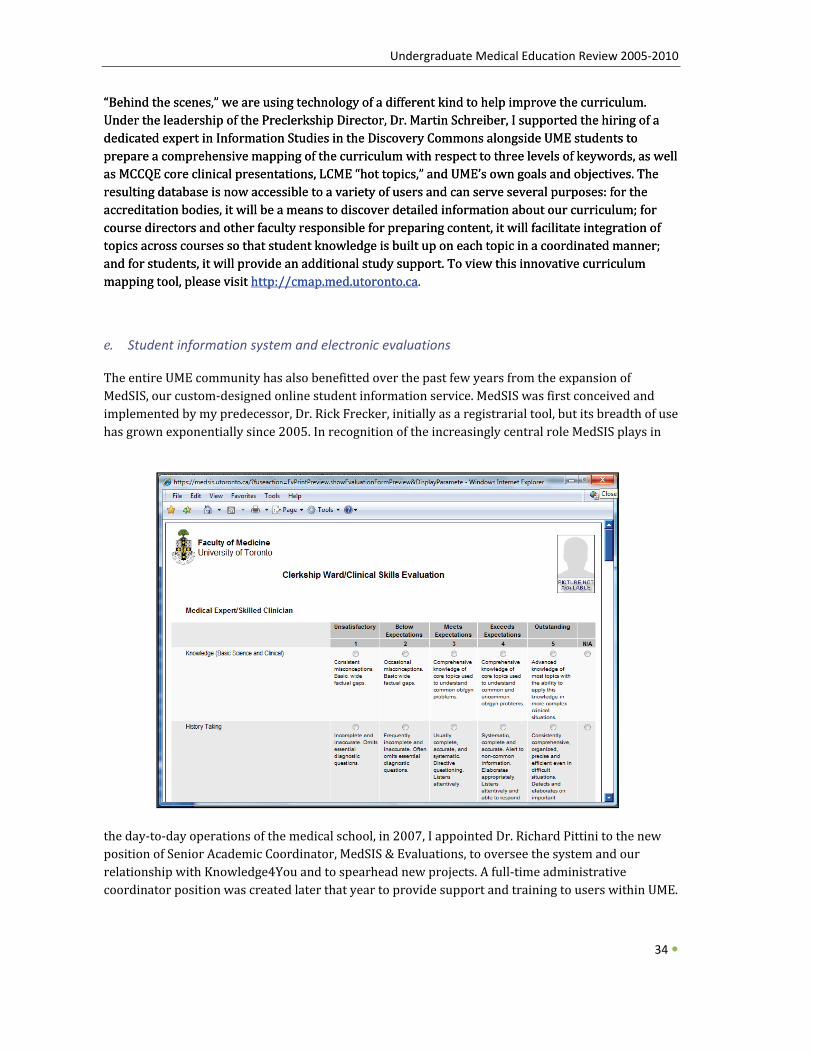
Undergraduate Medical Education Review 2005‐2010
“Behind the scenes,” we are using technology of a different kind to help improve the curriculum. Under the leadership of the Preclerkship Director, Dr. Martin Schreiber, I supported the hiring of a dedicated expert in Information Studies in the Discovery Commons alongside UME students to prepare a comprehensive mapping of the curriculum with respect to three levels of keywords, as well as MCCQE core clinical presentations, LCME “hot topics,” and UME’s own goals and objectives. The resulting database is now accessible to a variety of users and can serve several purposes: for the accreditation bodies, it will be a means to discover detailed information about our curriculum; for course directors and other faculty responsible for preparing content, it will facilitate integration of topics across courses so that student knowledge is built up on each topic in a coordinated manner; and for students, it will provide an additional study support. To view this innovative curriculum apping tool, please visit mm http://cmap.med.utoronto.ca
“Behind the scenes,” we are using technology of a different kind to help improve the curriculum. Under the leadership of the Preclerkship Director, Dr. Martin Schreiber, I supported the hiring of a dedicated expert in Information Studies in the Discovery Commons alongside UME students to prepare a comprehensive mapping of the curriculum with respect to three levels of keywords, as well as MCCQE core clinical presentations, LCME “hot topics,” and UME’s own goals and objectives. The resulting database is now accessible to a variety of users and can serve several purposes: for the accreditation bodies, it will be a means to discover detailed information about our curriculum; for course directors and other faculty responsible for preparing content, it will facilitate integration of topics across courses so that student knowledge is built up on each topic in a coordinated manner; and for students, it will provide an additional study support. To view this innovative curriculum apping tool, please visit http://cmap.med.utoronto.ca.
e. Student information system and electronic evaluations
The entire UME community has also benefitted over the past few years from the expansion of MedSIS, our custom‐designed online student information service. MedSIS was first conceived and implemented by my predecessor, Dr. Rick Frecker, initially as a registrarial tool, but its breadth of use has grown exponentially since 2005. In recognition of the increasingly central role MedSIS plays in
the day‐to‐day operations of the medical school, in 2007, I appointed Dr. Richard Pittini to the new position of Senior Academic Coordinator, MedSIS & Evaluations, to oversee the system and our relationship with Knowledge4You and to spearhead new projects. A full‐time administrative coordinator position was created later that year to provide support and training to users within UME.
34
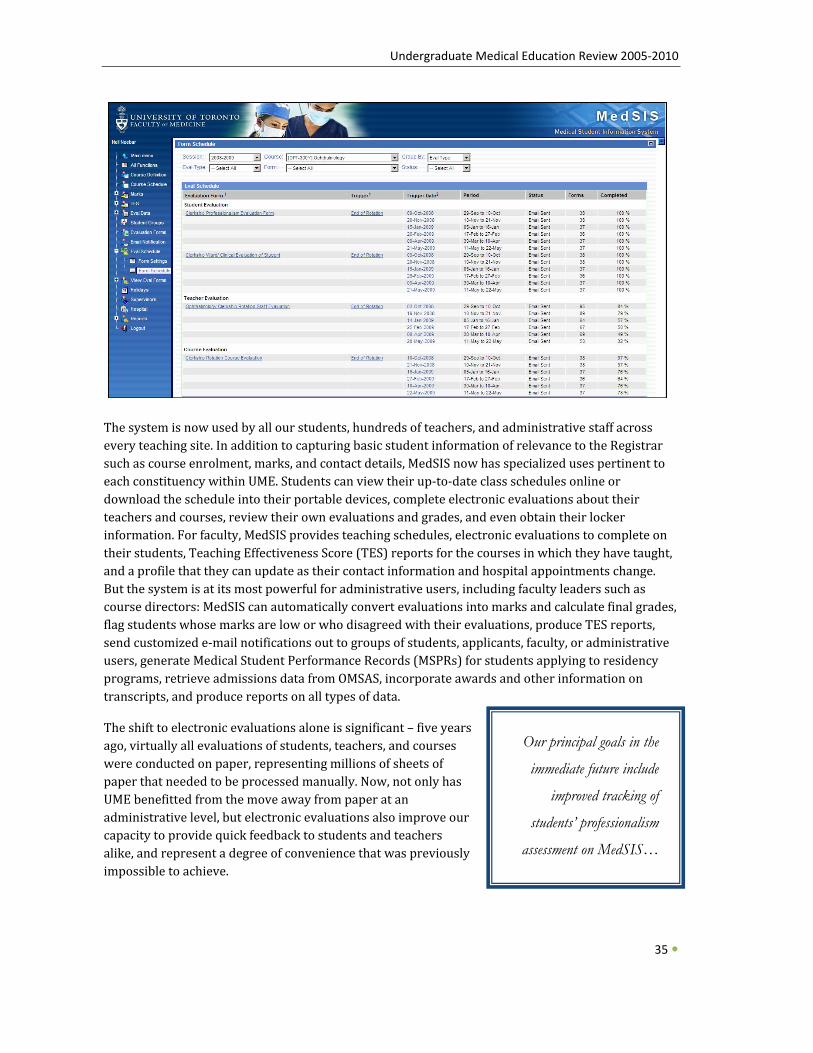
Undergraduate Medical Education Review 2005‐2010
The system is now used by all our students, hundreds of teachers, and administrative staff across every teaching site. In addition to capturing basic student information of relevance to the Registrar such as course enrolment, marks, and contact details, MedSIS now has specialized uses pertinent to each constituency within UME. Students can view their up‐to‐date class schedules online or download the schedule into their portable devices, complete electronic evaluations about their teachers and courses, review their own evaluations and grades, and even obtain their locker information. For faculty, MedSIS provides teaching schedules, electronic evaluations to complete on their students, Teaching Effectiveness Score (TES) reports for the courses in which they have taught, and a profile that they can update as their contact information and hospital appointments change. But the system is at its most powerful for administrative users, including faculty leaders such as course directors: MedSIS can automatically convert evaluations into marks and calculate final grades, flag students whose marks are low or who disagreed with their evaluations, produce TES reports, send customized e‐mail notifications out to groups of students, applicants, faculty, or administrative users, generate Medical Student Performance Records (MSPRs) for students applying to residency programs, retrieve admissions data from OMSAS, incorporate awards and other information on
Our principal goals in the
immediate future include
improved tracking of
students’ professionalism
assessment on MedSIS…
transcripts, and produce reports on all types of data.
The shift to electronic evaluations alone is significant – five years ago, virtually all evaluations of students, teachers, and courses were conducted on paper, representing millions of sheets of paper that needed to be processed manually. Now, not only has UME benefitted from the move away from paper at an administrative level, but electronic evaluations also improve our capacity to provide quick feedback to students and teachers alike, and represent a degree of convenience that was previously impossible to achieve.
35
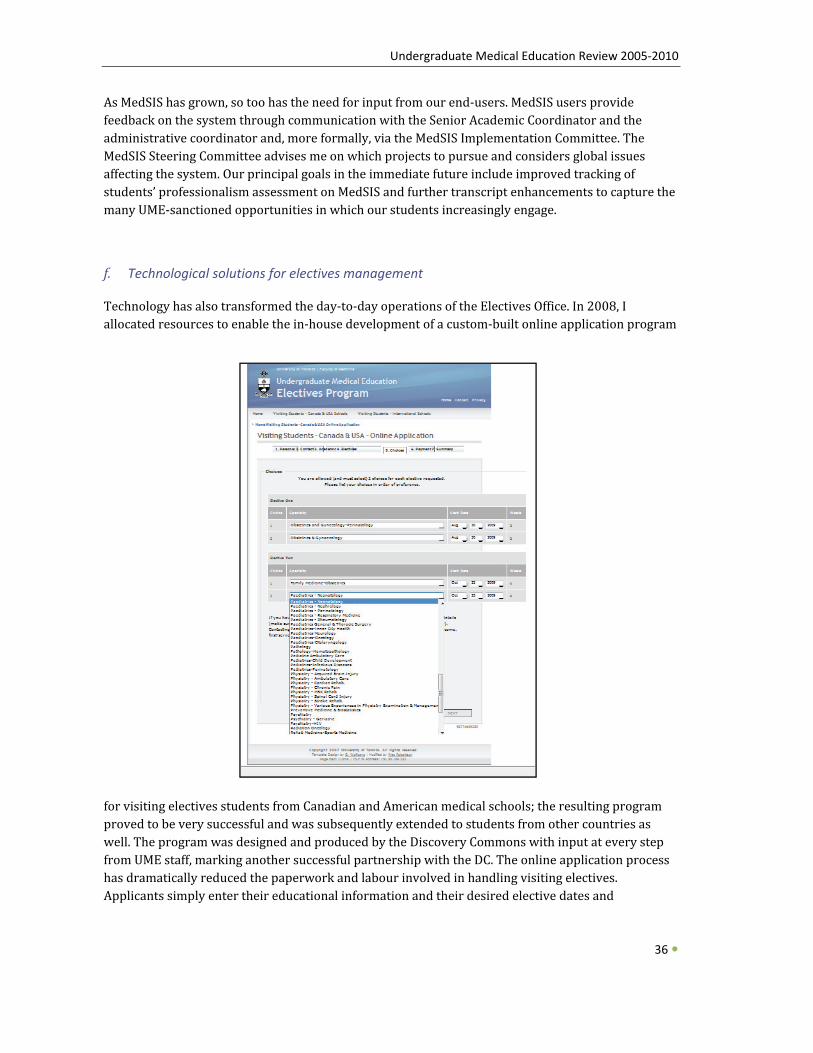
Undergraduate Medical Education Review 2005‐2010
As MedSIS has grown, so too has the need for input from our end‐users. MedSIS users provide feedback on the system through communication with the Senior Academic Coordinator and the administrative coordinator and, more formally, via the MedSIS Implementation Committee. The MedSIS Steering Committee advises me on which projects to pursue and considers global issues affecting the system. Our principal goals in the immediate future include improved tracking of students’ professionalism assessment on MedSIS and further transcript enhancements to capture the any UME‐sanctioned opportunities in which our students increasingly engage. m
36
f. Technological solutions for electives management
Technology has also transformed the day‐to‐day operations of the Electives Office. In 2008, I allocated resources to enable the in‐house development of a custom‐built online application program
for visiting electives students from Canadian and American medical schools; the resulting program proved to be very successful and was subsequently extended to students from other countries as well. The program was designed and produced by the Discovery Commons with input at every step from UME staff, marking another successful partnership with the DC. The online application process has dramatically reduced the paperwork and labour involved in handling visiting electives. Applicants simply enter their educational information and their desired elective dates and
Undergraduate Medical Education Review 2005‐2010
specialties; payment is submitted online at the point of application. The applicants subsequently upload their supporting documentation and photograph, and receive e‐mail alerts as their application status changes. In addition to streamlining the applications themselves, the program also facilitates analysis of visiting elective trends. We are now in the development phase of a similar online tool for University of Toronto students to submit proposal forms for electives taking place here and at other schools, and we anticipate similar success, as well as the adoption of many of our rograms by other Canadian Faculties of Medicine. p
g. UME website
Last but not least in the area of technology, we are keenly aware of the importance of the public face of the medical school on the web. In an effort to create a professional, student‐friendly, and welcoming website for the MD program, our Special Projects Manager, Neil Neebar conducted extensive consultation with each of the constituencies in UME and recently completed the development of an entirely redesigned website. The new site, http://www.md.utoronto.ca, was launched in July 2009 and boasts a fresh look with wider useable space for information, more intuitive enus, and inviting images. m
37

Undergraduate Medical Education Review 2005‐2010
STUDENT SUPPORT – REGISTRARIAL AFFAIRS
a. Staffing
As UME has grown and evolved over the past few years, the Office of the Registrar has kept pace. In 2005, Faculty Registrar Judy Irvine and her staff moved out of the Dean’s Corridor into a larger office suite also accommodating the Associate Registrar (Student Financial Services), Administrative Manager, and Business Officer. Since 2007, this office has become the hub for all academic‐related contact with students, replacing the congested reception area of the Curriculum Office. Students now go the Office of the Registrar for everything from picking up course syllabi and handing in assignments and elective proposals, to obtaining transcripts and signatures, submitting petitions for consideration, and seeking academic and financial counselling. This one‐stop approach to services has been greatly appreciated by students, and has increased the efficiency of administrative staff.
b. Services
New services have also been added to the registrarial responsibilities. Since the 2005/06 academic year, the Registrar herself has acted as the official signing agent for student elective applications at other schools, for confirmation of registration and documentation completion for visiting electives students, and for proof of registration for all students seeking career sampling placements outside of their regular curricular activities. The chart below captures all of the activities of the Registrar’s Office. I must personally thank Ms. Irvine and her team for the tremendous initiative they have all exhibited over the past few years to improve our students’ experience, with academic‐related services more efficient and friendly.
Through the efforts of this office, important new initiatives projects have been launched including the creation in 2006/07 of the Medical Student Performance Record (MSPR), a standardized report depicting in tabular form each student’s performance on the clinical competencies of every Clerkship course and elective in Years 3 and 4; I worked closely with the Registrar to ensure that the format of this new report would prove informative and efficient for residency application committees. In the same year, the Office of the Registrar also successfully developed and implemented a project whereby Clerkship students can access the Occupational Health Units at their academy sites to ensure compliance with their annual immunization requirements.
This one-stop approach to services has been greatly
appreciated by students, and has increased the
efficiency of administrative staff.
38
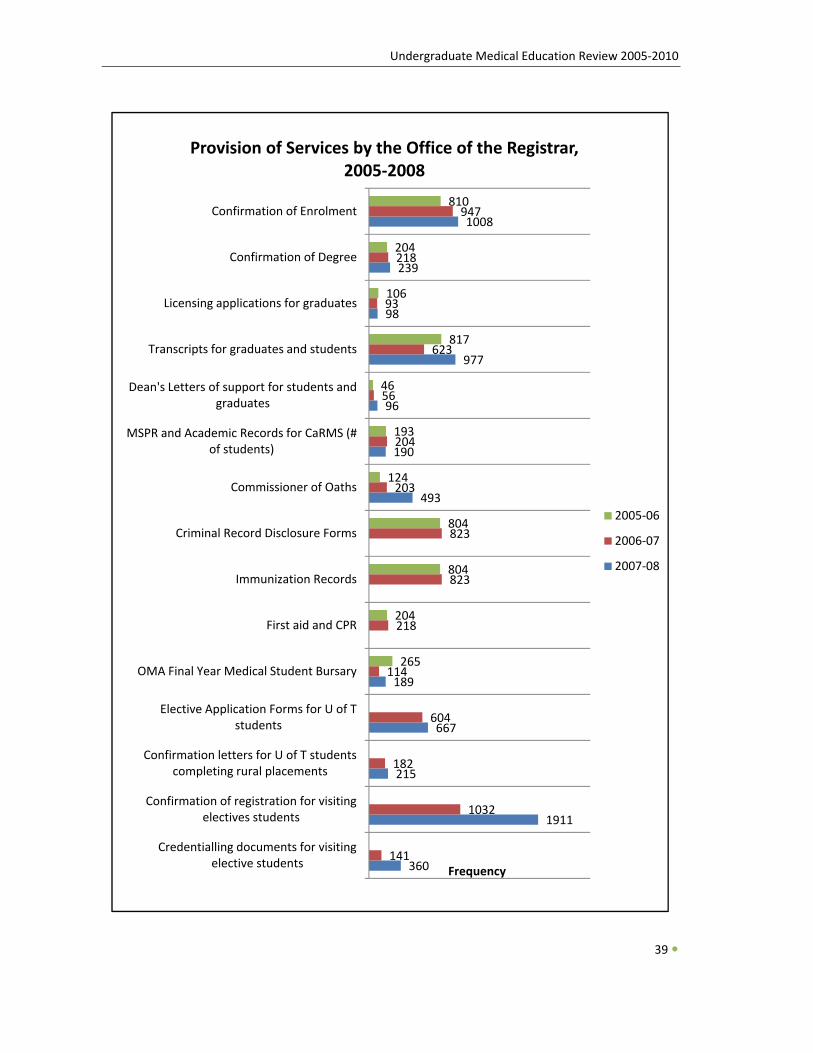
Undergraduate Medical Education Review 2005‐2010
39
360
1911
215
667
189
493
190
96
977
98
239
1008
141
1032
182
604
114
218
823
823
203
204
56
623
93
218
947
265
204
804
804
124
193
46
817
106
204
810
Credentialling documents for visiting elective students
Confirmation of registration for visiting electives students
Confirmation letters for U of T students completing rural placements
Elective Application Forms for U of T students
OMA Final Year Medical Student Bursary
First aid and CPR
Immunization Records
Criminal Record Disclosure Forms
Commissioner of Oaths
MSPR and Academic Records for CaRMS (# of students)
Dean's Letters of support for students and graduates
Transcripts for graduates and students
Licensing applications for graduates
Confirmation of Degree
Confirmation of Enrolment
Frequency
Provision of Services by the Office of the Registrar, 2005‐2008
2005‐06
2006‐07
2007‐08

Undergraduate Medical Education Review 2005‐2010
c. Transcription of Grades
The next major registrarial challenge will centre on the new grading policy (Credit/No Credit (Pass/Fail) notation on official transcripts). With the support of faculty on the Examination and Student Assessment Committee (ESAC), the Preclerkship Committee, and the Clerkship Committee, our students researched the issues around grading practices and the policies in use at other medical schools relating to the transcription of grades (specifically a three‐way Honours/Pass/Fail
c. Transcription of Grades
The next major registrarial challenge will centre on the new grading policy (Credit/No Credit (Pass/Fail) notation on official transcripts). With the support of faculty on the Examination and Student Assessment Committee (ESAC), the Preclerkship Committee, and the Clerkship Committee, our students researched the issues around grading practices and the policies in use at other medical schools relating to the transcription of grades (specifically a three‐way Honours/Pass/Fail distinction versus a binary Credit/No‐Credit distinction).
Under the skilful leadership of Andrew Brown (1T1), Senior VP, Education, and Chair of the Student Curriculum Evaluation Committee, a public debate was held to discuss the merits of the H/P/F system and other options; to this end, we facilitated several student townhall meetings, position papers, podcasts, and other strategies. Ultimately, a referendum sponsored by the Faculty and the Medical Society was held, producing an astonishing student turnout of 84%, of which 77% voted in favour of a change to a Credit/No Credit transcription system for the entire MD program. The UMECC unanimously agreed with the outcome of the students’ referendum. With full faculty support, I took this motion through each subsequent stage of governance as part of the approval process. In March 2009, our students’ and faculty’s efforts were rewarded when final approval was granted by Faculty
distinction versus a binary Credit/No‐Credit distinction).
Under the skilful leadership of Andrew Brown (1T1), Senior VP, Education, and Chair of the Student Curriculum Evaluation Committee, a public debate was held to discuss the merits of the H/P/F system and other options; to this end, we facilitated several student townhall meetings, position papers, podcasts, and other strategies. Ultimately, a referendum sponsored by the Faculty and the Medical Society was held, producing an astonishing student turnout of 84%, of which 77% voted in favour of a change to a Credit/No Credit transcription system for the entire MD program. The UMECC unanimously agreed with the outcome of the students’ referendum. With full faculty support, I took this motion through each subsequent stage of governance as part of the approval process. In March 2009, our students’ and faculty’s efforts were rewarded when final approval was granted by Faculty Council.
The Office of the Registrar will work closely with curricular leaders to ensure that the new grading policy is applied appropriately across all courses in Years 1 through 3 beginning this year, with Year 4 to come on board in 2010/11. We feel strongly that the new grading policy is in concert with our shift to a more competency‐based model of medical education, and I am gratified at the effort that ur students and faculty have expended in partnership to make this vision a reality.
Council.
The Office of the Registrar will work closely with curricular leaders to ensure that the new grading policy is applied appropriately across all courses in Years 1 through 3 beginning this year, with Year 4 to come on board in 2010/11. We feel strongly that the new grading policy is in concert with our shift to a more competency‐based model of medical education, and I am gratified at the effort that ur students and faculty have expended in partnership to make this vision a reality. o
o
… a referendum sponsored by the Faculty and the Medical Society was held, producing an
astonishing student turnout of 84%, of which 77% voted in favour of a change to Credit/No Credit transcription system for the entire MD
program.
40
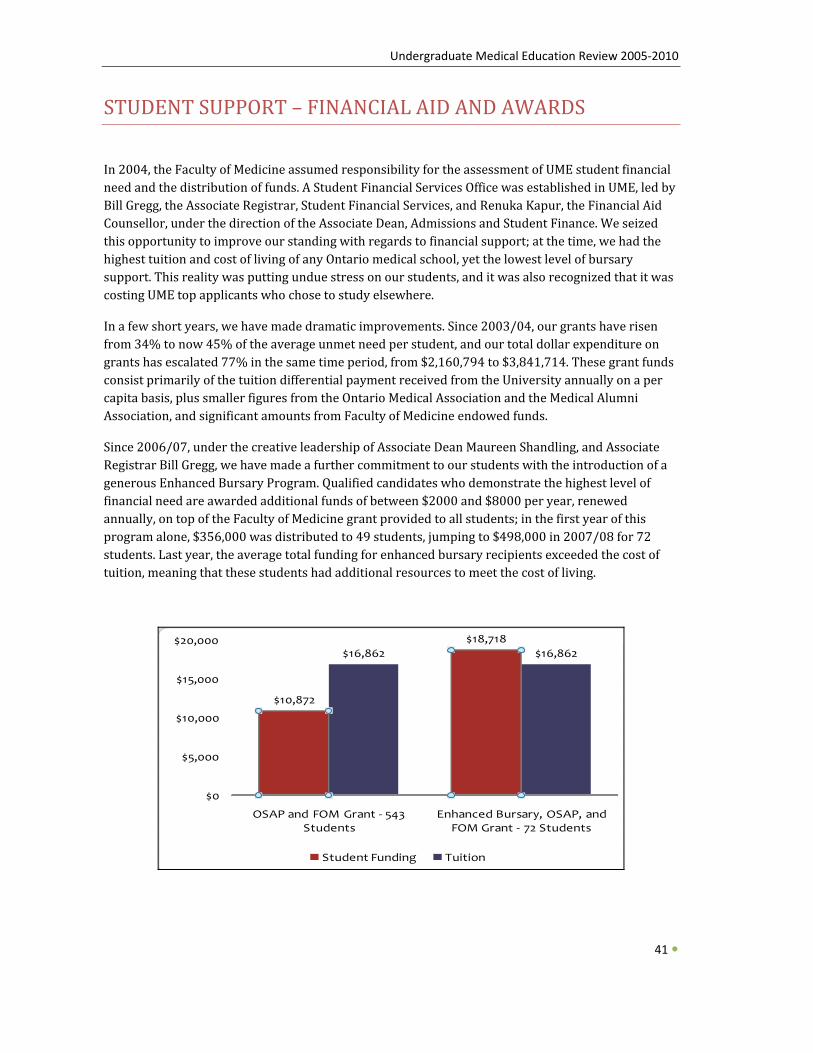
Undergraduate Medical Education Review 2005‐2010
STUDENT SUPPORT – FINANCIAL AID AND AWARDS
In 2004, the Faculty of Medicine assumed responsibility for the assessment of UME student financial need and the distribution of funds. A Student Financial Services Office was established in UME, led by Bill Gregg, the Associate Registrar, Student Financial Services, and Renuka Kapur, the Financial Aid Counsellor, under the direction of the Associate Dean, Admissions and Student Finance. We seized this opportunity to improve our standing with regards to financial support; at the time, we had the highest tuition and cost of living of any Ontario medical school, yet the lowest level of bursary support. This reality was putting undue stress on our students, and it was also recognized that it was costing UME top applicants who chose to study elsewhere.
In a few short years, we have made dramatic improvements. Since 2003/04, our grants have risen from 34% to now 45% of the average unmet need per student, and our total dollar expenditure on grants has escalated 77% in the same time period, from $2,160,794 to $3,841,714. These grant funds consist primarily of the tuition differential payment received from the University annually on a per capita basis, plus smaller figures from the Ontario Medical Association and the Medical Alumni Association, and significant amounts from Faculty of Medicine endowed funds.
Since 2006/07, under the creative leadership of Associate Dean Maureen Shandling, and Associate Registrar Bill Gregg, we have made a further commitment to our students with the introduction of a generous Enhanced Bursary Program. Qualified candidates who demonstrate the highest level of financial need are awarded additional funds of between $2000 and $8000 per year, renewed annually, on top of the Faculty of Medicine grant provided to all students; in the first year of this program alone, $356,000 was distributed to 49 students, jumping to $498,000 in 2007/08 for 72 students. Last year, the average total funding for enhanced bursary recipients exceeded the cost of uition, meaning that these students had additional resources to meet the cost of living. t
OSAP and Enhanced Bursary, OSAP, and FOM Grant ‐ 72 StudenStudent Fu $10,872 $18,718Tuition $16,862 $16,862
$10,872
$18,718$16,862 $16,862
$0
$5,000
$10,000
$15,000
$20,000
OSAP and FOM Grant ‐ 543 Students
Enhanced Bursary, OSAP, and FOM Grant ‐ 72 Students
Student Funding Tuition
41
Undergraduate Medical Education Review 2005‐2010
However, distribution of funds is only one aspect of our financial responsibility to students. Counselling, guidance, and education on financial topics all play a role in preparing them for the important decisions that arise during four years of medical school, residency, and beyond. In this area in particular, we have made great strides since 2005 to meet the expectations of our students. Presentations are offered by Financial Services staff throughout the year, particularly in the fall when students return to campus and a new year of tuition payments. In response to feedback from student surveys, beginning in 2006/07, our Financial Services staff have also undertaken to meet personally with every incoming Year 1 student to discuss the costs of medical education, budgeting and funding strategies, and any questions or concerns the student might have. Also in 2006/07, we provided support for an exciting initiative by medical student Kari Visscher to run workshops for Preclerkship students on the topic of How Money Works. The workshops proved very successful, and led to the creation of an online series available to all medical students across Canada. In addition to organized outreach efforts to students, our staff also provide counselling and information on an as‐needed basis as students seek assistance at critical junctures.
We are very pleased with the progress that we have made with respect to financial services over the past few years, and while the uncertain economy may well present new challenges in this area, we ook forward to the new ideas our students bring forward to meet their needs. l
42
In UME, there is
strong recognition
that a student’s
success cannot be
measured by
grades alone, nor
can their well-
being be reduced to
academic
performance.
STUDENT SUPPORT – COUNSELLING AND COMMUNITY BUILDING
In UME, there is strong recognition that a student’s success cannot be measured by grades alone, nor can their well‐being be reduced to academic performance. The Office of Student Affairs (now open to students across the professional programs in the Faculty of Medicine under the name Office of Health Professions Student Affairs) therefore plays a prominent role in the support we provide to our students, to enable them to successfully complete the MD egree. d
a. Counselling
The overarching aim of the OSA is to help students actualize their goal of completing the MD program, and to this end, we have grown the Office more in the past five years than any other area of UME. As part of the University of Toronto, our students have access to the central Counselling and Learning Skills Services in the Koffler
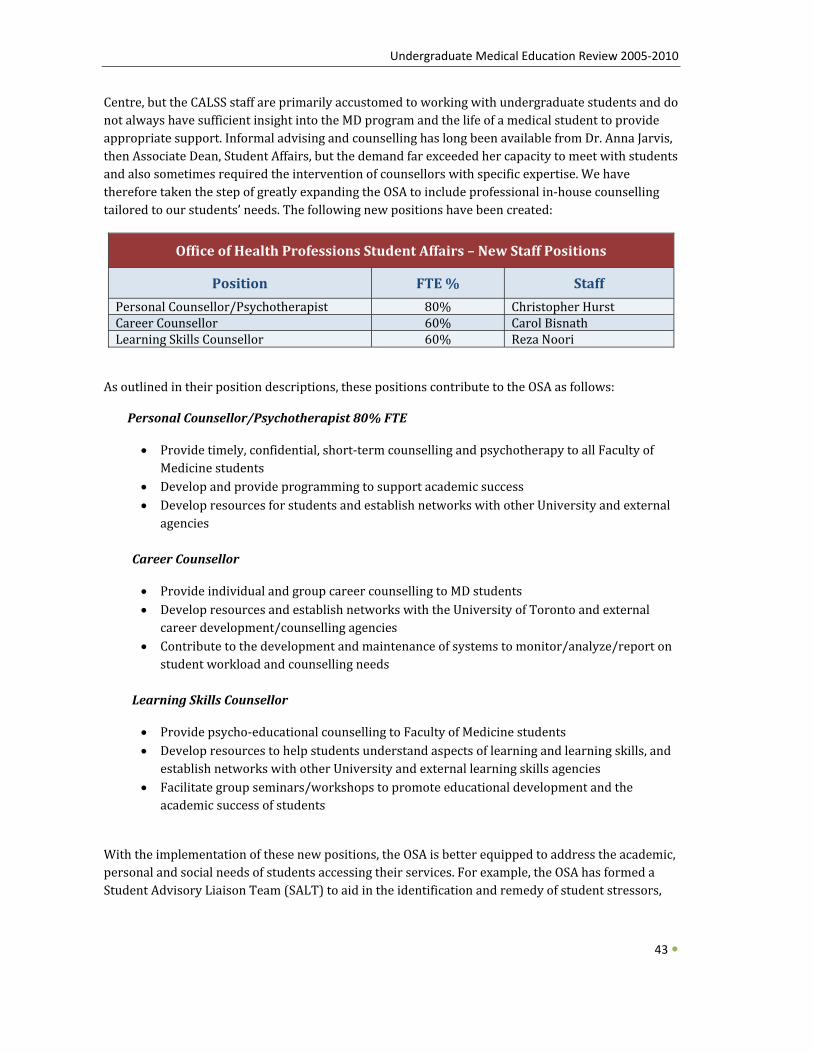
Undergraduate Medical Education Review 2005‐2010
43
Centre, but the CALSS staff are primarily accustomed to working with undergraduate students and do not always have sufficient insight into the MD program and the life of a medical student to provide appropriate support. Informal advising and counselling has long been available from Dr. Anna Jarvis, then Associate Dean, Student Affairs, but the demand far exceeded her capacity to meet with students and also sometimes required the intervention of counsellors with specific expertise. We have therefore taken the step of greatly expanding the OSA to include professional in‐house counselling tailored to our students’ needs. The following new positions have been created:
Office of Health Professions Student Affairs – New Staff Positions
Position F TE % Staff
Personal Counsellor/Psychotherapist 80% Christopher Hurst Career Counsellor 60% Carol Bisnath Learning Skills Counsellor 60% Reza Noori
As outlined in their position descriptions, these positions contribute to the OSA as follows:
Personal Counsellor/Psychotherapist 80% FTE
• erapy to all Faculty of Provide timely, confidential, short‐term counselling and psychoth
• Medicine students Develop and provide programming to support academic success
• Develop resources for students and establish networks with other University and external agencies
Career Counsellor
• Provide individual and group career counselling to MD students • Develop resources and establish networks with the University of Toronto and external
career development/counselling agencies • Contribute to the development and maintenance of systems to monitor/analyze/report on
student workload and counselling needs
Learning Skills Counsellor
• Provide psycho‐educational counselling to Faculty of Medicine students • s, and Develop resources to help students understand aspects of learning and learning skill
establish networks with other University and external learning skills agencies • Facilitate group seminars/workshops to promote educational development and the
academic success of students
With the implementation of these new positions, the OSA is better equipped to address the academic, personal and social needs of students accessing their services. For example, the OSA has formed a Student Advisory Liaison Team (SALT) to aid in the identification and remedy of student stressors,

Undergraduate Medical Education Review 2005‐2010
concerns and issues. Under the leadership of the Personal Counsellor/ Psychotherapist, this Team is comprised of approximately 17 members including student volunteers from the core UME program and also the MD/PhD program. SALT members work in collaboration with the OSA to offer activities relating to student wellness, career development and learning skills strategies. All of our counsellors devote most of their time to private appointments with individual students, but also offer group seminars and workshops throughout the year to address various themes of pertinence to our student population. Our counselling services have proved to be very successful, and we intend to provide imilar support at the Mississauga Academy when it opens in 2011. s
b. Student life and community outreach
While developing the counselling aspect of the OSA’s mandate, we have not neglected its equally important role in supporting student life and outreach into the community. Working with the University of Toronto Medical Society (MedSOC), the OSA offers social activities for our students and also supports a number of innovative volunteer programs that build links between our students and the Toronto community. In 2007/08 alone, seven new community programs were launched, bringing the total to 23. The new programs include hearing screening for Grade 1 students from disadvantaged areas, blood pressure testing in populations susceptible to hypertension, mentoring of teenagers from alternative high schools, and outreach with St. Christopher House serving Toronto’s downtown west‐end neighbourhoods. Work is also underway on IMAGINE, an exciting initiative to create a free holistic health clinic run by students with supervision from faculty from all the allied health professional programs to meet the needs of the homeless and disadvantaged communities of Toronto. UME has been very supportive of this ambitious project and will continue to provide assistance and advice to the student leaders as they move forward towards implementation.
Work is also underway on IMAGINE, an exciting initiative to create a free holistic health clinic run by students with supervision from faculty from all the allied health professional programs to meet the needs of the homeless and disadvantaged communities of Toronto.
44
c. Service learning
We are now building on the foundation of community programs we support via the OSA in order to ensure compliance with a new accreditation standard on which we will be judged at our next review in 2011/12: opportunities for service learning, defined by the LCME as “a structured learning experience that combines community service with preparation and reflection.” I have allocated resources to create a new full‐time position in the OSA for a Senior Officer, Service Learning Opportunities & Community Partnerships/Student Life Enrichment, to strengthen and augment our outreach and service learning programs, encourage student development as leaders and
Undergraduate Medical Education Review 2005‐2010
45
professionals, and liaise with other University groups, community partners, and funding sources. With the GTA’s rich diversity and sheer size, all our students will be able to identify ways in which they can serve the community while tapping into their own interests, broadening their horizons, and eveloping their professional competencies. d
d. New leadership
Given the significant changes that have occurred in the Office of Student Affairs, we determined that greater administrative oversight was warranted. A new full‐time Operations Manager position was created to develop and coordinate the infrastructure of the OSA, lead technical projects, manage the finances of the office, and provide direction to the administrative staff. After an interim hire, we welcomed Nisha Panchal earlier this year to this new role. Two of the top‐priority, student‐related challenges this position will address are (1) the creation of confidential counselling space that meets the LCME accreditation standards, and (2) development of plans to provide effective student support in light of the enrolment expansion, distributed medical education, and the launch of the Mississauga Academy.
Finally, it is with a mixture of regret and excitement that I must note one other important change in the OSA. After two incredibly productive terms, Dr. Anna Jarvis stepped down this past spring as Associate Dean, Health Professions Student Affairs. After a comprehensive search encompassing internal and external candidates, we were pleased to welcome to the role Dr. Leslie Nickell, Peters‐Boyd Academy Director for the last five years. We look forward to the new directions in which Dr. Nickell will take the OSA, including an even greater emphasis on outreach, particularly in raditionally marginalized sectors of the population. t
TTRACTING STUDENTS – ADMISSIONS A
The goal of the admissions process is to select individuals who will become superb and compassionate medical practitioners, scientists, and scholars – in effect, the future leaders of medicine in Canada. While our admissions practices have not changed dramatically in the past few years, admissions has been at the forefront of a number of demographic changes facing UME. Since 2003, applications to the University of Toronto have almost doubled, after remaining steady since the mid‐1990s – we are second only to UBC across the country in this regard, which is a testament to the increasingly strong reputation of our program. Each year, we attract almost ten times the number of applicants as we have seats. Of particular importance as a sign of excellence, we are succeeding at enticing top students not only to apply but moreover to accept our offers of admission. Our rate of acceptance has grown, and has been higher every year since 2005 than in any of the previous five
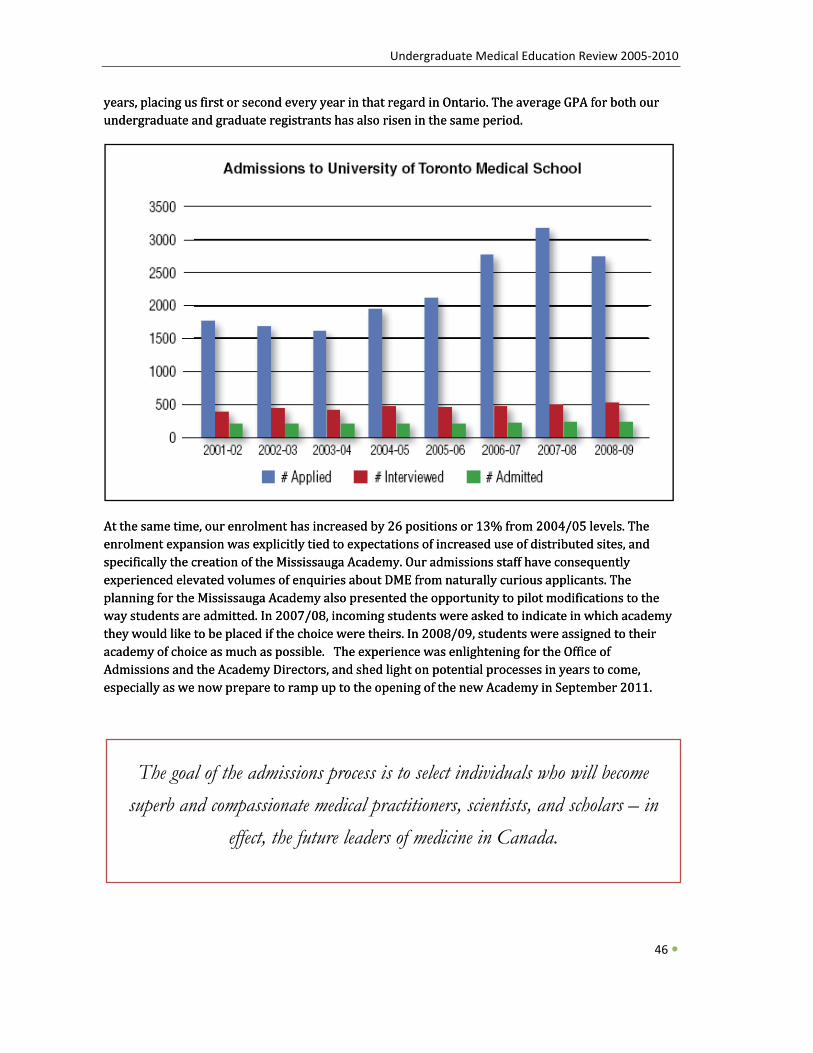
Undergraduate Medical Education Review 2005‐2010
years, placing us first or second every year in that regard in Ontario. The average GPA for both our undergraduate and graduate registrants has also risen in the same period. years, placing us first or second every year in that regard in Ontario. The average GPA for both our undergraduate and graduate registrants has also risen in the same period.
46
At the same time, our enrolment has increased by 26 positions or 13% from 2004/05 levels. The enrolment expansion was explicitly tied to expectations of increased use of distributed sites, and specifically the creation of the Mississauga Academy. Our admissions staff have consequently experienced elevated volumes of enquiries about DME from naturally curious applicants. The planning for the Mississauga Academy also presented the opportunity to pilot modifications to the way students are admitted. In 2007/08, incoming students were asked to indicate in which academy they would like to be placed if the choice were theirs. In 2008/09, students were assigned to their academy of choice as much as possible. The experience was enlightening for the Office of Admissions and the Academy Directors, and shed light on potential processes in years to come, especially as we now prepare to ramp up to the opening of the new Academy in September 2011.
At the same time, our enrolment has increased by 26 positions or 13% from 2004/05 levels. The enrolment expansion was explicitly tied to expectations of increased use of distributed sites, and specifically the creation of the Mississauga Academy. Our admissions staff have consequently experienced elevated volumes of enquiries about DME from naturally curious applicants. The planning for the Mississauga Academy also presented the opportunity to pilot modifications to the way students are admitted. In 2007/08, incoming students were asked to indicate in which academy they would like to be placed if the choice were theirs. In 2008/09, students were assigned to their academy of choice as much as possible. The experience was enlightening for the Office of Admissions and the Academy Directors, and shed light on potential processes in years to come, especially as we now prepare to ramp up to the opening of the new Academy in September 2011.
The goal of the admissions process is to select individuals who will become superb and compassionate medical practitioners, scientists, and scholars – in
effect, the future leaders of medicine in Canada.
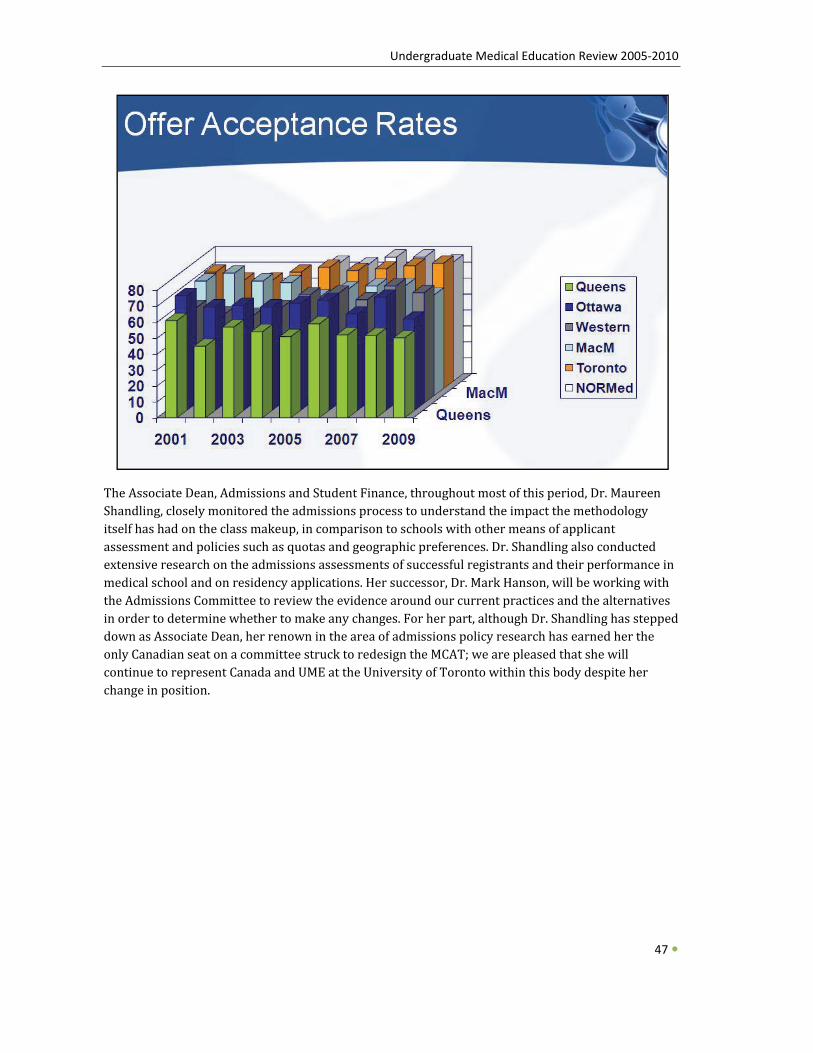
Undergraduate Medical Education Review 2005‐2010
The Associate Dean, Admissions and Student Finance, throughout most of this period, Dr. Maureen Shandling, closely monitored the admissions process to understand the impact the methodology itself has had on the class makeup, in comparison to schools with other means of applicant assessment and policies such as quotas and geographic preferences. Dr. Shandling also conducted extensive research on the admissions assessments of successful registrants and their performance in medical school and on residency applications. Her successor, Dr. Mark Hanson, will be working with the Admissions Committee to review the evidence around our current practices and the alternatives in order to determine whether to make any changes. For her part, although Dr. Shandling has stepped down as Associate Dean, her renown in the area of admissions policy research has earned her the only Canadian seat on a committee struck to redesign the MCAT; we are pleased that she will continue to represent Canada and UME at the University of Toronto within this body despite her change in position.
47
Undergraduate Medical Education Review 2005‐2010
EVALUATION AND IMPROVEMENT IN UME TO SUPPORT THE TUDENT EXPERIENCE
EVALUATION AND IMPROVEMENT IN UME TO SUPPORT THE TUDENT EXPERIENCE SS
The improvements we have made in all areas of the program are closely tied to pedagogical research, trends in student performance, quantitative and qualitative feedback, and ongoing evaluation. We have a strong relationship with both the Wilson Centre for Research in Education and the Centre for Faculty Development (CFD),and our instructors participate in a vast number of workshops and other initiatives developed collaboratively with both organizations on wide‐ranging topics including effective presentation skills, mentoring, the role of education in cultural awareness and diversity, teaching around professionalism, and development of the instructors themselves as scholars in medical education research; approximately 1000 faculty members have taken part in these activities to date. Hence, through our ties to both the CFD and the Wilson Centre, we are the beneficiaries of highly trained teachers and innovative approaches to medical education.
To ensure that UME is meeting its objectives, we rely on the Program Evaluation Committee (UMEPEC) and our Director of Program Evaluation, Dr. Bart Harvey, a position I created towards the start of my term. UMEPEC has been instrumental in mapping our courses’ content to our curricular objectives, and is now working with all our Course Directors to identify ways in which the objectives are evaluated. Already, UMEPEC’s findings have revealed a gap in the area of the “Manager” competencies, which has led us to develop a curriculum around this role. As the UME curriculum heads into a period of dramatic change, UMEPEC’s input on how well we are adhering to our stated objectives will become more vital than ever.
UMEPEC also concerns itself with external markers of our program’s performance, reporting annually on our graduates’ results on the Medical Council of Canada Qualifying Examinations and their impressions of the program as captured on the AAMC’s Canadian Medical School Graduation
Questionnaire. Since 2004, performance targets have been in place in UME for the MCCQE‐1 (which is taken immediately after completion of the MD program), and I subsequently extended the targets to apply to th
The improvements we have made in all areas of the program are closely tied to pedagogical research, trends in student performance, quantitative and qualitative feedback, and ongoing evaluation.
e MCCQE‐2 (taken during the second year of residency) as well. The targets are as follows:
• That the mean standardized scores for University of Toronto medical graduates exceed the Canadian national average (which also includes Toronto’s graduates) on all aspects of the MCCQE.
48
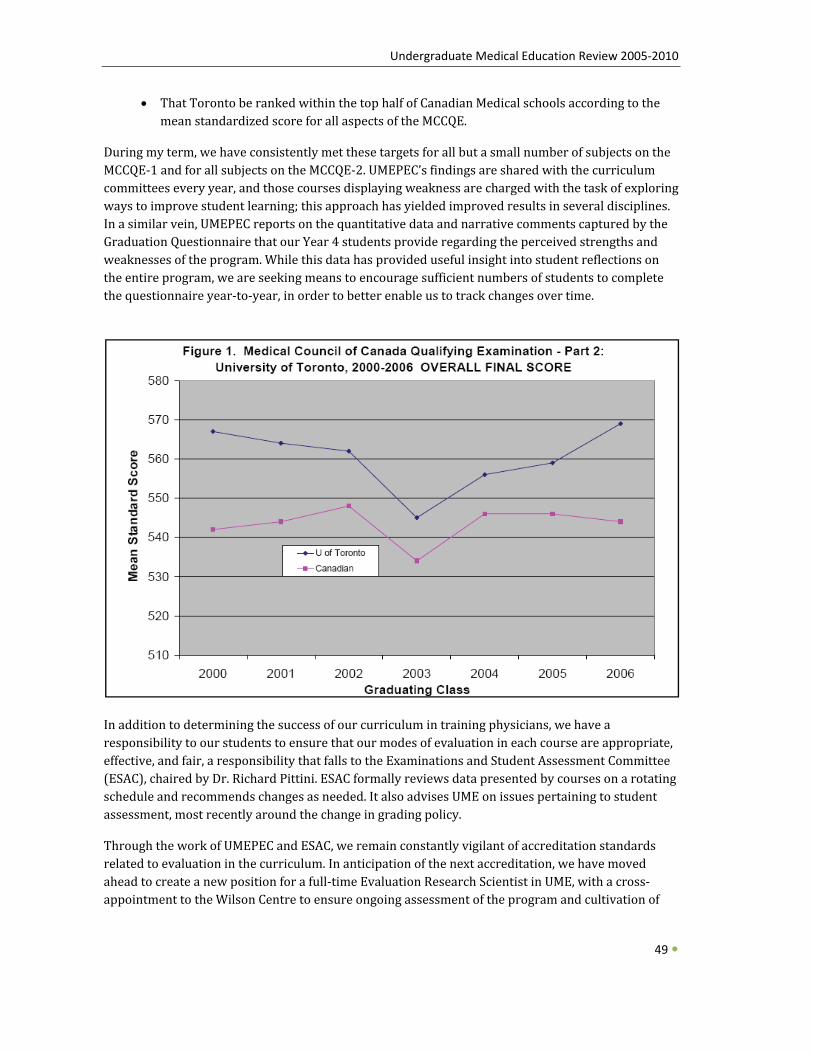
Undergraduate Medical Education Review 2005‐2010
• That Toronto be ranked within the top half of Canadian Medical schools according to the mean standardized score for all aspects of the MCCQE.
During my term, we have consistently met these targets for all but a small number of subjects on the MCCQE‐1 and for all subjects on the MCCQE‐2. UMEPEC’s findings are shared with the curriculum committees every year, and those courses displaying weakness are charged with the task of exploring ways to improve student learning; this approach has yielded improved results in several disciplines. In a similar vein, UMEPEC reports on the quantitative data and narrative comments captured by the Graduation Questionnaire that our Year 4 students provide regarding the perceived strengths and weaknesses of the program. While this data has provided useful insight into student reflections on the entire program, we are seeking means to encourage sufficient numbers of students to complete the questionnaire year‐to‐year, in order to better enable us to track changes over time.
In addition to determining the success of our curriculum in training physicians, we have a responsibility to our students to ensure that our modes of evaluation in each course are appropriate, effective, and fair, a responsibility that falls to the Examinations and Student Assessment Committee (ESAC), chaired by Dr. Richard Pittini. ESAC formally reviews data presented by courses on a rotating schedule and recommends changes as needed. It also advises UME on issues pertaining to student
49
assessment, most recently around the change in grading policy.
Through the work of UMEPEC and ESAC, we remain constantly vigilant of accreditation standards related to evaluation in the curriculum. In anticipation of the next accreditation, we have moved ahead to create a new position for a full‐time Evaluation Research Scientist in UME, with a cross‐appointment to the Wilson Centre to ensure ongoing assessment of the program and cultivation of

Undergraduate Medical Education Review 2005‐2010
the tools necessary to enable it to remain of foremost consideration for all members of the undergraduate medical education community. Dr. Jodi Herold, an outstanding evaluation scientist, the tools necessary to enable it to remain of foremost consideration for all members of the undergraduate medical education community. Dr. Jodi Herold, an outstanding evaluation scientist, was hired earlier this year to serve in this unique joint position.
Looking ahead, I am pleased that, following a submission led by Dr. Pittini with my support, the University of Toronto has been chosen as the only Canadian site for the National Board of Medical Examiners’ Clinical Progress Test pilot study. This project is in alignment with our desire to move forward as innovators in evaluation, and I anticipate that participation in this study will assist in the development of additional evaluation methods for UME students as we continue to evolve our curriculum towards a longitudinal competency‐based format.
was hired earlier this year to serve in this unique joint position.
Looking ahead, I am pleased that, following a submission led by Dr. Pittini with my support, the University of Toronto has been chosen as the only Canadian site for the National Board of Medical Examiners’ Clinical Progress Test pilot study. This project is in alignment with our desire to move forward as innovators in evaluation, and I anticipate that participation in this study will assist in the development of additional evaluation methods for UME students as we continue to evolve our curriculum towards a longitudinal competency‐based format.
… the University of Toronto has been chosen as the only Canadian site for the National Board of Medical
Examiners’ Clinical Progress Test pilot study. This project is in alignment with our desire to move forward as innovators in
evaluation …
LIAISON AND PROMOTION OF UME OUTSIDE THE NIVERSITY
LIAISON AND PROMOTION OF UME OUTSIDE THE NIVERSITY UU
As a leader on the national and international stages, UME and the University of Toronto is in an excellent position to contribute substantively to important developments in medical education. It is my privilege to represent the University of Toronto in a number of senior roles, and to facilitate the low of ideas to and from our institution. f
50
a. Future of Medical Education in Canada Project (http:www.afmc.ca/fmec)
Most excitingly, the Association of Faculties of Medicine of Canada (AFMC) has launched a major national project entitled the Future of Medical Education in Canada (FMEC), in which I have been intimately involved as a member of the Steering Committee. With Angela Towle, my counterpart at
Undergraduate Medical Education Review 2005‐2010
51
UBC, I travelled extensively in the US and Europe in 2008 and 2009 to conduct an international consultation on best medical education practices elsewhere. Our reports to the AFMC served to inform the review process, and on a more personal note, this experience has also given me important insight into ways that we can continue to improve UME here at the University of Toronto in the future. I have subsequently been appointed to serve as Co‐Chair, along with Jim Rourke and Nick Busing, of the Implementation Committee of FMEC, and look forward to continued collaboration with my colleagues from across Canada with the shared goal of improved medical education for all future physicians in this country. I have had the honour of being invited to present the final recommendations of the Project at several national fora this year, including the AFMC/CCME annual meeting, the Medical Council of Canada annual meeting, and the International Colloquium on Longitudinal Integrated Clerkships. I will be presenting the recommendations to the AFMC board in ovember, and to a Harvard Medical School Symposium in the spring. N
b. Medical Council of Canada
Outside of AFMC, I am involved with other national bodies as well. I am proud to act as the University of Toronto representative to the Medical Council of Canada. Related to this position, I serve with a select group of individuals on the Research & Development Committee and the Appeals Committee. Furthermore, I have been named the MCC representative on the board working on implementation of the Medical Information Number of Canada (MINC) project, a system of universal identification umbers that is expected to one day be used for all medical professionals in Canada. n
c. Royal College of Physicians and Surgeons of Canada (RCPSC), government, and international projects
As Chair of the RCPSC’s Annual Conference Advisory Committee from 2006 to 2008, I have played a role in establishing the trends and issues that the College chooses to examine. Internationally, I have served as a Visiting Professor at the University of Copenhagen, where I highlighted our innovative curricular objectives; I was also invited to address the Association for Medical Education in Europe on generalism.
Finally, as part of my role as Vice‐Dean, I also maintain a productive, positive relationship with leaders in the Ministry of Health and Long‐Term Care and the Ministry of Training, Colleges, and Universities, particularly in view of such projects as the enrolment expansion and creation of the new Academy in Mississauga. Formally, I served a six‐year term on the Minister of Education’s Advisory Committee on Special Education, allowing me to develop broader ties to legislators, educators, and senior civil servants across the province. Although it can admittedly be challenging at times to maintain the operations of the medical school and move forward on important projects when political considerations have dictated different timelines, I am confident that we have developed an understanding with the government about our needs as the largest producer of new doctors in the province.

Undergraduate Medical Education Review 2005‐2010
52
CONCLUSION
It has been a great honour for me to serve as the head of the Undergraduate Medical Education program since 2005. As described above, we have made enormous strides in many areas with plans to move further forward in the coming years. The changes we institute are informed by student needs, the aims of the Faculty, and the good of society.
Five years ago, the Faculty of Medicine put forth a set of twelve recommendations in its Academic Plan 20042010. UME has moved ahead on all the recommendations pertaining to the MD program:
• Recom or the 21st centur
mendation 1: “Advance our scientific and professional training platform fy.”
o As much as physician training is necessarily a hands‐on activity, we have nevertheless incorporated innovative technology into the classroom and at the bedside to accommodate our students’ diverse learning styles, and have also
• Recomsignificantly strengthened our research offerings. mendation 4: “Significantly augment student aid for professional students…..”
o As noted earlier, our funding to students has increased from 34% to 45% of unmet financial need on average, not including the substantial impact that the Enhanced Bursary Fund has had on those students with the greatest budgetary pressures.
• Recom other commu ise.”
mendation 7: “Better integrate the community affiliated teaching hospitals andnity‐based teaching and practice sites into the education and research enterpr
o We have been able to achieve greater communication and integration with the community hospitals, and their involvement in all years of our program at the current Academies has grown increasingly significant. The establishment of an entirely community‐based Academy in Mississauga will serve to cement our strong relationship with and regard for community teaching sites. In addition, our policy document Academy Roles and Governance and the recent distributed medical education external review will clarify some of the uncertainty that remains around oversight in community‐based education.
• Recomthe Facul
mendation 10: “Enhance information technology and communications capability of ty.”
o We were major stakeholders in the creation of the Discovery Commons and continue to partner extensively with them on staffing and projects. We are firm believers in the value of in‐house expertise when we are seeking to craft technological solutions to meet our needs.
We have also made continual progress on the strategic directions laid out by me for UME in the aculty’s December 2007 Strategic Plan White Paper. To recap: F
Undergraduate Medical Education Review 2005‐2010
53
• ReviewMedica
the Admissions process, to ensure congruity with overall strategic goals of the l School.
o The Admissions process has undergone extensive study, and armed with the data accumulated by Dr. Shandling on our processes and those of other schools, our new
o Associate Dean, Admissions and Student Finance, Dr. Mark Hanson, is well‐placed tmake recommendations on the directions in which we should move.
• Augmean enh
nt services provided to medical students by the Office of Student Affairs, including ancement of career counselling services and service learning opportunities.
o Our career counsellor position is now a 0.6 FTE, an increase of half‐a‐day a week, to ameliorate our students’ access to this type of support. We are continuing to look at ways to further enhance this function, and expect that the new Associate Dean, Student Affairs, and the new Operations Manager will provide input on this issue.
he Our responsibility to provide service learning opportunities has been boosted by tcreation of a dedicated Senior Officer role.
• Revise the Terms of Reference of the Curriculum Committee, to ensure that all licensing accreditation standards are being met, and to facilitate more representation of key stakeholders involved in the education of medical students and the outcomes of the traininprofes
g of physicians, such as our affiliated hospitals, urban and rural teaching sites, other sional and academic partners (e.g., bioethics, humanities), and the public.
of o Our Curriculum Committee has been refashioned based on the recommendations the Clerkship Review and the Curriculum Review process.
• Convene a strategic planning retreat by early 2008 with stakeholders, both internal and externCurric
al to the Faculty of Medicine, to address the priority issues identified by the ulum Review Steering Group.
o This retreat took place in May 2008, and the discussion generated very positive ideas and insight which we are now working to implement as described throughout this report.
• Respond to the key recommendations of the Generalism Task Force, including provision of increased exposure of students to primary care and generalist role models, both early in their tr d specia
aining, and in the Clerkship, to ensure an appropriate balance of generalist anlist curriculum in the MD program.
o We have incorporated more teaching by family doctors in particular and also generalists in other fields into the core Preclerkship curriculum. In addition, we are now in the third year of a pilot for the Family Medicine Longitudinal Experience, and will be introducing the much‐anticipated six‐week Family Medicine Clerkship in 2010/11.
• Review and enhance the Electives program by the newly hired Director of Electives with the ma g electiv
ndate to enhance flexibility for and creativity of the medical students in designines.
o Changes to the Electives program include the planned introduction of Enriching Education Experiences (EEEs) in the Preclerkship and more consistent elective blocks in the Clerkship to allow all students sufficient career exploration opportunities prior to the CaRMS deadline. In addition, we are developing a menu of selective opportunities for the post‐CaRMS period, which will give students on the
Undergraduate Medical Education Review 2005‐2010
54
verge of graduation the flexibility to try new experiences that they could not accommodate in the regular curriculum.
• Review and enhance the Research programs available to medical students, including the Comprehensive Research Experience for Medical Students (CREMS), the MD/PhD program and othealth
her potential joint graduate degree opportunities in the University such as in public , management, engineering and law.
o Our new Director of Physician Scientist Training Programs, Dr. Norman Rosenblum, and our DOCH 1‐4 course director, Ian Johnson, are both working to develop
t, combined MD/Master’s or PhD degrees in the areas of public health, managemenand engineering. We are also dedicating resources to advance these initiatives.
• Enhance information technology (IT) initiatives and infrastructure in UME, to support state‐of‐the‐art pedagogy in MD education. This includes all e‐learning initiatives such as portfolios and case logs, curriculum mapping, on‐line courses and modules, on‐line schedugreate
ling and evaluation, videoconferencing, live and recorded video streaming, and r integration of simulations.
o We are constantly working to enhance the My Practice Portfolio application, which is now used in all the core Clerkships. The majority of lectures are now screen‐ and audio‐captured and posted online as streaming movie files, and the Curriculum Committee has passed a motion that will make digital capture of large‐group sessions a requirement in future. Curriculum mapping continues apace, as does the uptake and evolution of MedSIS. New technology in hands‐on anatomy instruction is now being introduced, and we are also looking forward to the build‐up of videoconferencing at all our sites.
• Initiate placement of Preclerkship and Clerkship students in Mississauga, and fully comple issauga commu
te the development of the Mississauga Academy in partnership with the Missnity‐affiliated hospitals in order to fully open in September 2010.
o Although the opening of the Mississauga Academy has been delayed until the 2011/12 academic year, we continue to ramp up our student placement in Mississauga. In 2008/09, we had eighteen year 1 students undertaking some learning at CVH and THC, six students in Y2 at CVH, and clerks taking Family Medicine and Emergency Medicine rotations in Mississauga as well.
• Initiate a program for a defined subset of medical students, for development of advanced academic leadership skills, in collaboration with the Department of HPME, and other Univer lic Policy.
sity resources such as the Rotman School of Business, and the School of Pub
o A business plan for this project was completed in the first half of 2009, and recruitment of the first group of 16 students is underway.
Despite our successes, we must acknowledge the challenges looming on the horizon. Although economic forecasts of late have tended towards positive predictions of quick recovery, the fact is that the future remains uncertain in this regard. Given UME’s rapid expansion with respect to staff and faculty positions, technology requiring constant upkeep, and community teaching based on a remuneration model, we must steer our budget carefully and be vigilant of the potential need to rein in expenditures. From the outset of my term, I recognized the importance of creating a new
Undergraduate Medical Education Review 2005‐2010
administrative manager position to help manage our financial health, and this decision has proven invaluable. A new advancement position in UME is being created at present in partnership with our Faculty advancement office, to bring in new sources of revenue to support our quality programs and new initiatives, particularly those that entail additional student stipends.
For much of my term, the future has been equally uncertain with respect to student numbers. However, with the provincial government’s announcement in May 2009 of an additional 35 students over the next three years, we can now plan with greater confidence the distribution of students among our sites and all associated resources including teachers, equipment, space, and information technology. Furthermore, we can now move forward to reap the full rewards of the strong relationships we have developed with the leadership and staff at both CVH and THC.
We are also entering a period of considerable transition, as we introduce significant changes to the structure of our curriculum and say goodbye to a number of individuals in senior positions, including Associate Deans and Course Directors. But transition brings opportunity, and I am personally eager to see and support the fresh ideas our new leaders will bring to the table. I am equally confident that our students will continue to push us to excel in delivering the best medical education in Canada.
Jay Rosenfield ARCT, MD, MEd, FRCPC te Medical Educatiersity of Toronto
Vice‐Dean, Undergraduaaculty of Medicine, Univrofessor of Paediatrics
on FP
October, 2009
Acknowledgement:
I wish to express my sincere thanks to Jennifer Anderson and Neil Neebar for their assistance in the preparation of this report.
55

Undergraduate Medical Education Review 2005‐2010
56
APPENDICES
1.1 W. T. Aikins Awards Winners 2005‐2009
1.2 Medical Alumni Association Teaching Awards
2.1 Undergraduate Medical Education Curriculum Goals and Objectives
2.2 External Review of the Clerkship Program
2.3 Administrative Response to the External Review of the Clerkship Program: Recommendations
2.4 Curriculum Review Steering Group Terms of Reference and Membership
2.5 Highlights of the Student Curriculum Review Report
2.6 Undergraduate Medical Education Curriculum Committee Terms of Reference and Membership
3.1 Comprehensive Research Experience for Medical Students Research Day 2008: Event Details and Winners
3.2 Ontario Medical Students Research Day 2009: 1st Annual Event Details and Winners
4.1 University of Toronto Faculty of Medicine Distributed Education External Review Recommendations (September 15, 2009):
Undergraduate Medical Education Review 2005‐2010
57
Appendix 1.1 W. T. AIKINS AWARDS WINNERS 2005‐2009
EXCELLENCE IN UNDERGRADUATE TEACHING
The W. T. Aikins Awards are named after Dr. W.T. Aikins, the first dean of the University of Toronto, Faculty of Medicine after it was re‐organized in 1887. These awards are the Faculty's most prestigious awards for sustained commitment to and excellence in undergraduate teaching. All Faculty of Medicine academic staff who teach undergraduate students in Medicine are eligible to receive an Aikins award. The winners are selected from nominees in a Faculty‐wide process that requires support from both faculty and students. These teaching awards are given serious consideration in the academic promotions process.
Individual Teaching Performance – Small Group • d Gynecology 2009: Adrian Brown, Department of Obstetrics an• 2009: Robert Sargeant, Department of Medicine • 2008: Stacey Bernstein, Department of Pediatrics • 2008: Christopher Wallace, Department of Surgery • gery 2007: Sender Herschorn, Division of Urology, Department of Sur• 2007: Ophyr Mourad, Department of Medicine • Gynaecology 2007: Michael Sved, Department of Obstetrics and• 2006: Wayne Gold, Department of Medicine • 2006: Robert Hilliard, Department of Paediatrics • 2005: Anne Agur, Division of Anatomy, Department of Surgery (inaugural recipient)
Individual Teaching Performance – Large Group • 2009: James Ingles, Department of Molecular Genetics • 2008: Lori Albert, Department of Medicine • 2007: Reinhart Reithmeier, Department of Biochemistry • 2006: Chris Perumalla, Department of Physiology • 2005: Steven Shumak, Department of Medicine (inaugural recipient)
Course/Program Development and Coordination • , Department of Medicine 2009: Vincent Chien• 2008: Not awarded • 2007: Not awarded • nack, Department of Medicine 2006: Jeannine Ba• 2005: Jameel Ali
Develop ethods ment and Use of Innovative Instructional M• 2009: Not Awarded • , Department of Surgery 2008: Michael Wiley• 2007: Not awarded • 2006: Not awarded • 2005: Not awarded
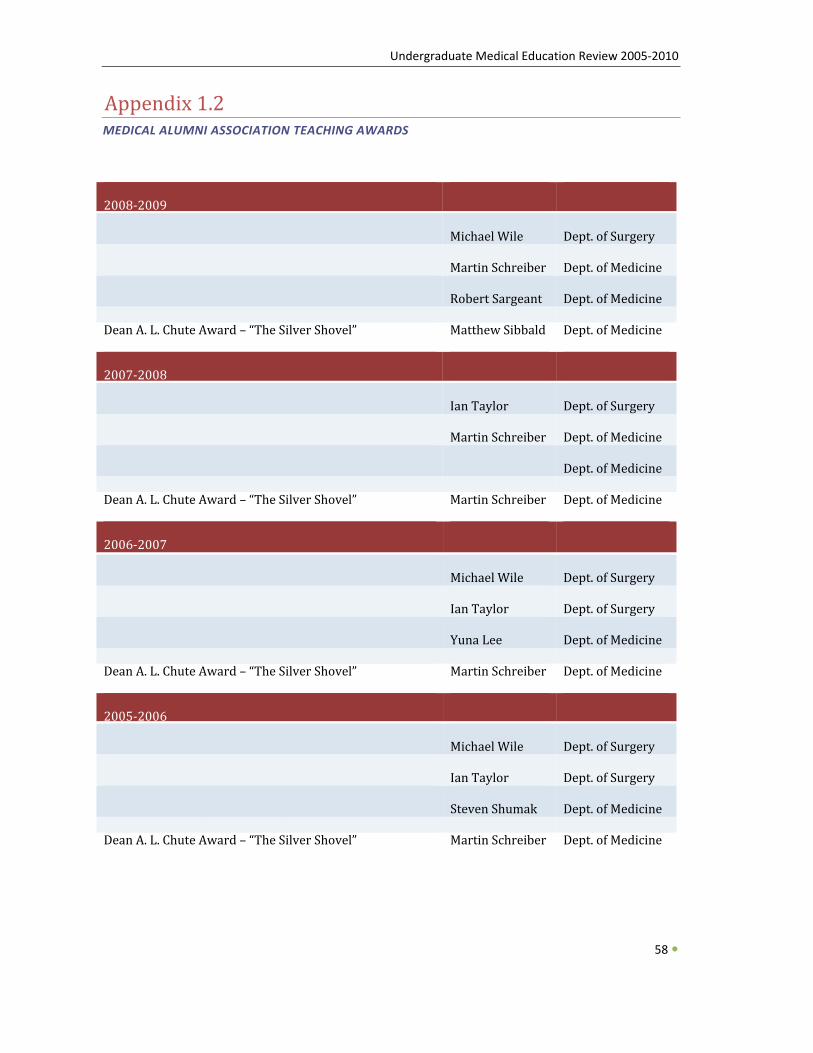
Undergraduate Medical Education Review 2005‐2010
58
Appendix 1.2 MEDICAL ALUMNI ASSOCIATION TEACHING AWARDS
2008‐2009
Dr. Harry Whittaker Memorial Teaching Award –Excellence in Teaching
Michael Wiley Dept. of Surgery
Dr. E. Mary Hollington Teaching Award – Excellence in Preclinical or Basic Science Teaching
Martin Schreiber Dept. of Medicine
Dr. E. Mary Hollington Teaching Award – Excellence in Clinical Teaching
Robert Sargeant Dept. of Medicine
Dean A. L. Chute Award – “The Silver Shovel” Matthew Sibbald Dept. of Medicine
2007‐2008
Dr. Harry Whittaker Memorial Teaching Award –Excellence in Teaching
Ian Taylor Dept. of Surgery
Dr. E. Mary Hollington Teaching Award – Excellence in Preclinical or Basic Science Teaching
Martin Schreiber Dept. of Medicine
Dr. E. Mary Hollington Teaching Award – Excellence in Clinical Teaching
Steven Shadowitz
Dept. of Medicine
Dean A. L. Chute Award – “The Silver Shovel” Martin Schreiber Dept. of Medicine
2006‐2007
Dr. Harry Whittaker Memorial Teaching Award –Excellence in Teaching
Michael Wiley Dept. of Surgery
Dr. E. Mary Hollington Teaching Award – Excellence in Preclinical or Basic Science Teaching
Ian T yloa r Dept. of Surgery
Dr. E. Mary Hollington Teaching Award – Excellence in Clinical Teaching
Yuna Lee Dept. of Medicine
Dean A. L. Chute Award – “The Silver Shovel” Martin Schreiber Dept. of Medicine
2005‐2006
Dr. Harry Whittaker Memorial Teaching Award –Excellence in Teaching
Michael Wiley Dept. of Surgery
Dr. E. Mary Hollington Teaching Award – Excellence in Preclinical or Basic Science Teaching
Ian Taylor Dept. of Surgery
Dr. E. Mary Hollington Teaching Award – Excellence in Clinical Teaching
Steven Shumak Dept. of Medicine
Dean A. L. Chute Award – “The Silver Shovel” Martin Schreiber Dept. of Medicine
Undergraduate Medical Education Review 2005‐2010
Appendix 2.1 Appendix 2.1 UNDERGRADUATE MEDICAL EDUCATION CURRICULUM GOALS AND OBJECTIVES
Approved by Faculty Council of the Faculty of Medicine, February 3, 2003 Faculty of Medicine, University of Toronto Undergraduate Medical Education Curriculum Goals and Objectives
GOALS:
Rec nog izing
g logic of linking medical student ntinuing education, and
1) the continuum of medical education, and the compellineducation to subsequent post‐graduate training and co
2) the scientific and humanistic foundations of Medicine*,
the University of Toronto, Faculty of Medicine has adopted the following goals for the undergraduate curriculum:
1. Graduates of the Undergraduate Medical Program will demonstrate the foundation of knowledge, skills and attitudes necessary to achieve the CanMeds 2000 competencies and the four principles of Family Medicine.
2. In keeping with the Faculty of Medicine’s vision of International Leadership in Health Research and Education, the Undergraduate Medical Curriculum will encourage, support and promote the development of future academic health leaders, who will contribute to our communities, and improve the health of individuals and populations through the discovery, application and communication of knowledge.
BAC
The competencies from CanMEDS 2000 and the four principles of Family Medicine have been merged for the purpose of defining the specific objectives that follow. The principle of “The Family Physician as a Skilled Clinician” is associated with the “Medical Expert/Skilled Clinical Decision Maker” CanMEDS competency. The second and third Family Medicine principles “…a resource to a defined practice population” and “community‐based” expands the CanMEDS “Health Advocate” competency. Similarly, the CanMEDS “Communicator” competency adds depth to the “Doctor‐Patient Relationship” Family Medicine principle. Based on this, curriculum objectives are organized into the followin
KGROUND:
g categories:
1. Medical Expert/Skilled Clinical Decision Maker 2. Communicator/Doctor‐Patient Relationship 3. Collaborator 4. Manager 5. Health Advocate 6. Scholar 7. Professional
59
Undergraduate Medical Education Review 2005‐2010
60
The competency descriptors are modified to acknowledge that graduates of the MD program are about to start their post‐graduate residency programs. _______________________________ * An example of this concept is contained in Dr. Edmund Pellegrino's definition of medicine as "the most humane of the sciences, the most scientific of the humanities and most empiric of the arts." pproved by Faculty Council of the Faculty of Medicine, February 3, 2003. 2 A
OBJECTIVES:
1. Medical Expert/ Skilled Clinical D
The ed
ecision Maker
m ical graduate will be able to:
and be 1. Demonstrate a knowledge of the scientific* and humanistic foundations of medicineable to apply that knowledge to the practice of medicine.
2. Demonstrate a thorough knowledge of the etiology, pathogenesis, clinical features, complications, principles of prevention and management of common and life‐threatening
nting throughout the age spectrum, including all of the core clinical illnesses presepres
3. Dementations outlined by the Medical Council of Canada. onstrate:
• The ability to obtain and document both a complete and a focused medical history, as the situation requires.
• l The ability to perform and document both a complete and focused physical and mentastatus examination, as the situation requires.
• The ability to interpret commonly‐employed laboratory tests, including tests of blood and other body fluids, various imaging modalities, and other specific tests such as electrocardiography.
• The ability to integrate the above history, physical and laboratory test findings into a meaningful diagnostic formulation. Therapeutic and on‐going management skills with respect to health and disease
4. Retrieve, analyze, and synthesize relevant and current data and literature, using information technologies and library resources, in order to help solve a clinical problem.
5. Propose clinical decisions utilizing methods which integrate the best research evidence with clinical expertise and patient values.
_______________________________
*Scientific foundations include among others, the contemporary content of those disciplines that have been traditionally titled anatomy, behavioral science, biochemistry, genetics, immunology, microbiology, pathology, pharmacology and therapeutics, physiology, and preventive medicine.
2. Communicator/DoctorPatient R
The ed
elationship
m ical graduate will be able to:
1. Communicate effectively with patients, their families and the community through verbal, fs written and other non‐verbal means of communication, respecting the differences in belie
and backgrounds among patients and students. 2. Establish professional relationships with patients, their families (when appropriate) and
community that are characterized by understanding, trust, respect, empathy and confidentiality.
3. Deliver information to the patient and family (as appropriate) in a humane manner, and in such a way that it is easily understood, encourages discussion and promotes the patient’s participation in decision‐making.
Undergraduate Medical Education Review 2005‐2010
61
4. Gather information, negotiate a common agenda, and develop and interpret a treatment plan, while considering the influence of factors such as the patient’s age, gender, ethnicity, cultural and spiritual values, socioeconomic background, medical conditions, and communication challenges.
5. Demonstrate the importance of cooperation and communication among health professionals so as to maximize the benefits to patient care and outcomes, and minimize the risk of errors.
3. Collaborator
The ed m ical graduate will be able to:
1. Describe the roles and expertise of all members of an interdisciplinary team that are required to optimally achieve a goal related to patient care, a research problem, an educational task, or an administrative responsibility.
nt and 2. Develop a care plan for a patient he/she has assessed, including investigation, treatmecontinuing care, in collaboration with the members of the interdisciplinary team.
3. Participate in interdisciplinary team discussions, demonstrating the ability to accept, consider and respect the opinions of other team members, while contributing an appropriate level of expertise to patient care.
4. Manager
The ed m ical graduate will be able to:
1. Participate effectively in health care organizations, ranging from individual clinical practices to Academic Health Sciences Centres, exerting a positive influence on clinical practice and policy‐making in one’s professional community.
2. Describe the governance, structure, financing, and operation of the health care system and its facilities and how this influences patient care, research and educational activities at a local, provincial, regional, and national level.
3. Apply a broad base of information to the care of patients in ambulatory care, hospitals and other health care settings.
4. Describe the rationale for wise stewardship of available resources, appreciating the overall ation, and the absolute and relative levels of resources in framework for resource alloc
various components of the health care system.
5. Help to build better teams. al 6. Describe how population‐based approaches to health care services can improve medic
tcome of a patient care program. practice.
7. Participate in planning, budgeting, evaluation and ou8. Participate in innovative approaches to clinical care.
Undergraduate Medical Education Review 2005‐2010
62
5. Health Advocate/Community Re
The ed
sources
m ical graduate will be able to:
1. Describe the determinants of health and principles of disease prevention and behavior , change appropriate for specific patient populations within a community and internationally
and apply these to patient care responsibilities and broader patient care initiatives. 2. Define and describe a population, its demography, cultural and socioeconomic constitution,
n circumstances of living, and health status; and understand how to gather health informatioabout this population in order to better serve its needs.
3. Respect diversity, be willing to work through systems, collaborate with other members of the health care team, and accept appropriate responsibility for the health of populations.
ce, 4. Participate in community activities directed at improving health, utilizing the best evideneffective teamwork and communication skills.
5. Describe the importance of the individual physician/patient relationship, and develop it appropriately, as a means to identify and implement individual health and disease management strategies on an individual basis.
6. Be prepared to challenge clinical orthodoxy, or identify threats to population health and advocate for their amelioration.
6. Scholar The ed ate will be able to contribute to the following scholarly activities: m ical gradu
1. Research: The medical graduate will be able to pose a research question, help develop a protocol, assist n carrying out the research, and disseminate the results. The medical graduate will
e an understanding of ethics as it relates to medical research. idemonstrat
2. Education: The ed m ical graduate will:
a) demonstrate the ability to engage in life‐long, self‐directed learning and critical inquiry.
nts and others, b) compare and contrast the diverse learning approaches of peers, patiein order to effectively interact and collaborate.
c) assist in teaching others and facilitating learning where appropriate d) nderstand the importance of being mentors to those less experienced members of u
the health care teams
3. Creative Professional Activity The medical graduate will be able to describe the importance of, and contribute to professional innovations, creative excellence, and exemplary professional practice. The graduate will also demonstrate leadership potential by participating in the development of professional practices, such as practice guidelines or health policy development, and articipation in professional organizations. p
Undergraduate Medical Education Review 2005‐2010
63
7. Professional
The ed m ical graduate will be able to:
1. Recognize and accept the need for self‐care and personal development as necessary to fulfilling one’s professional obligations and leadership role.
2. Demonstrate altruism, honesty and integrity and respect in all interactions with patients, families, colleagues, and others with whom physicians must interact in their professional lives.
nd respect for their privacy and dignity 3. Demonstrate compassionate treatment of patients a
and beliefs.
4. Be reliable and responsible in fulfilling obligations. 5. Recognize and accept the limitations in his/her knowledge and clinical skills, and
demonstrate a commitment to continuously improve his/her knowledge, ability and skills and leadership, always striving for excellence.
t 6. Describe and abide by the University/Faculty codes of professional conduct, and the relevanprofessional regulatory requirements concerning medical practice.
7. Describe the threats to medical professionalism posed by the conflicts of interest which can occur in the practice of medicine.
ing, 8. Demonstrate a sound grasp of the theories and principles governing ethical decision‐makthe major ethical dilemmas in medicine, and an approach to resolving these.
e 9. Demonstrates an understanding of the principles and practice of law as they apply to thpractice of medicine.
10. Develop the capacity to recognize common medical errors, report them to the required bodies, and discuss them appropriately with patients.
Undergraduate Medical Education Review 2005‐2010
64
Appendix 2.2 EXTERNAL REVIEW OF THE CLERKSHIP PROGRAM
EXTERNAL REVIEW of the
CLERKSHIP PROGRAM at
THE UNIVERSITY of TORONTO
Introduction and Composition of the Review Team
ril A review of the University of Toronto, Faculty of Medicine Clerkship Program was conducted on Ap24‐25, 2007 by Drs. Allan Jones and Brian Hodges. The team expresses it appreciation to Dean Catharine Whiteside and the Department Chairs, Educational Leadership, Faculty and students for their interest and candor during the review process (Appendix B). Vice Dean Jay Rosenfield and Ms. eborah Tabah deserve special thanks for the smooth coordination of the visit and timely provision f Review documents before and during the process (Appendix A). Do Reviewers
Allan Jones, MD Professor of Medicine Division of Hematology
dical Education
Former Associate DeanUndergraduate Me
University of Calgary
Brian Hodges, MD Associate Professor
ucation
Director, Wilson Centrefor Research and Ed
University of Toronto
EXECUTIVE SUMMARY A. Strengths of the Education Program . Commitment and dedication of the Clerkship Director 1There was a uniformly positive view of the clerkship leadership. 2. Commitment and dedication of the Clerkship Course Directors
to 3. Commitment of the Dean, Vice Dean Undergraduate Medical Education and Department Chairsthe success of the Undergraduate Program. Although there are differing views on clerkship content and delivery and support for innovative hanges there was general agreement that the chairs and Dean would be supportive of curricular
l education objectives. cchange if linked to the school’s mission, goals and the undergraduate medica
rgraduate mission 4. Relationship of hospitals and Academies with the unde 5. Faculty and Administration concern for the students. recent example includes the clerkship schedule change in fourth year to protect time from lerkship duties for students to attend CaRMS interviews. Ac
Undergraduate Medical Education Review 2005‐2010
65
6. Teachers and resources 7. An academic promotion system which is supportive of excellence in education and teaching. . Respected faculty development programs to help residents and faculty improve their skills in 8teaching and evaluation. . A close relationship of the Vice Dean Undergraduate and Postgraduate Education fostered by the
re endorsed strongly by both groups. 9Council of Education Deans. The Can MEDS objectives a
0. Ad by the students 1
ditional strengths reported
i) two full clerkship years, ii) excellent clinical exposure,
p, iii) clerkship organization, teaching and leadershi iv) opportunity to participate in the community, v) electives for U of T students at U of T are facilitated by the strong support from the electives
office and a excellent electives catalogue. n
. Issues of Concern B 1. Curriculum Management There is a need to create a small, effective curriculum decision making body that can hear proposals, discuss them and vote on decisions. This Curriculum Committee’s main responsibilities will include planning, implementing, and reviewing the curriculum. Currently there are too many bodies including a pre‐clerkship curriculum committee, clerkship curriculum committee and the overall curriculum committee. The latter is not functional. There is also a new curriculum advisory group (advisory only), and an Undergraduate Medical Education Executive Committee. This latter body should be expanded to included two chairs (one each from clinical and basic science), a resident who ompleted undergraduate training at University of Toronto and a student leader and be empowered s a decision making body regarding the curriculum. ca 2. Strategic Planning The directional strategic plan initiated by Dean Whiteside is vital to the success of implementing any significant undergraduate medical education curricular change or innovation. There is a need to finish the Dean’s strategic planning and the need for the strategic plan to articulate a clear five to ten year set of goals and objectives including clear statements about priorities (i.e.. generalism, social esponsibility, inter‐professional educational opportunities, education within the community etc.) rior to making major curricular changes. rp 3. Curriculum Mapping The need for a curriculum mapping process was raised repeatedly by all groups interviewed during he review process. This should be pursued in earnest and form the basis for consideration of dditions or reductions to curriculum content. ta 4. Flexibility in Planning The curriculum needs to be able to respond to changes generated internally and/or by ongoing external environment assessment (political, academic, educational, technologic). In order to achieve institutional objectives more flexibility is needed between clerkships more so than within them.
Undergraduate Medical Education Review 2005‐2010
66
5. Early Clinical Experiences There is a significant lack of clinical exposure and experiences in years one and two. The relatively ight workload of second year should include half day clinical experiences for career sampling and arly exposure to clinical settings. le 6. Learning Objectives The institutional objectives describe CanMEDS 2000 competencies and four principles of Family Medicine modified to acknowledge that the graduates of the MD program are about to start their post‐graduate residency programs. The undergraduate program has yet to completely define the requisite knowledge competencies of the graduating students (medical expert/skilled clinical ecision maker). When better defined by the curriculum committee the curriculum content can be oordinated and integrated more visibly within and across the academic periods of study. dc 7. eLearning tudents feel that it is time for the Undergraduate Medical Education Program to increase its e‐earning opportunities especially if students are encouraged to clerk at community clinical sites. SL 8. Electives The electives program which represents the largest clerkship course (18 weeks) has not had a irector for over six months. There is an opportunity for innovation to align this course more closely ith the seven categories of institutional objectives. The Director’s role should be filled as a priority.
dw 9. LCME Standards The LCME Accreditation review three years ago gave the University of Toronto Faculty of Medicine full accreditation. Currently there are several LCME Standards to keep an eye on.
Undergraduate Medical Education Review 2005‐2010
67
Appendix 2.3 AR
DMINISTRATIVE RESPONSE TO THE EXTERNAL REVIEW OF THE CLERKSHIP PROGRAM: ECOMMENDATIONS
1. Curriculum Management The Reviewers have correctly identified a major problem in the oversight and management of the UME curriculum, namely the structure and function of the Curriculum Committee. In keeping with the LCME accreditation standard ED‐33, which notes that the curriculum committee must be empowered, through bylaws or decanal mandate, to work in the best interests of the institution without regard for parochial or political influences, or departmental pressures, we are recommending that the terms of reference for the Curriculum Committee be changed, immediately. The Vice Dean, UME will Chair the Curriculum Committee and the membership of the committee will broadly represent the key stakeholder groups in the design and delivery of UME curriculum including the UME executive, Clinical, Basic Science and Community Health Sectors of the Faculty of Medicine, as well as the fully affiliated and community affiliated hospitals. Membership on the Curriculum Committee will be of the highest level academic leadership including Department Chairs, Vice Presidents Education and UME Directors. We agree that UME students, postgraduate medical education and alumni should be represented on the Curriculum Committee. Appointment to the UME Curriculum will be approved by the Dean on the recommendation of the Vice Dean UME. The pre‐clerkship and clerkship curriculum subcommittees with their own terms of reference will continue to report to the Curriculum ommittee. The Curriculum Committee will have responsibility for assigning curriculum time to Cachieve all of the institutional objectives. The terms of the Curriculum Committee and its subcommittees will focus on ensuring that the UME program meets all LCME accreditation standards and fulfills the Vision, Mission and Values of the Faculty of Medicine. The continuum of medical education among undergraduate, postgraduate and continuing education will be recognized and reflected in the curriculum design, implementation, evaluation and iterative change continually undertaken by the Curriculum Committee. As part of their mandate, the Curriculum Committee will present an annual report to the Dean via the Vice Dean UME. This report will be presented for information at Faculty Council. The collection of reports will serve as the platform for periodic reporting to LCME.
2. Strategic Planning The importance of coordinating any curriculum changes related to generalism, social responsibility, inter‐professional educational opportunities, education within the community etc, with the Faculty’s current strategic planning process is highlighted. We agree, and this is underway. A high level Curriculum Review Steering Group is in the process of meeting and making recommendations. In follow up to the clerkship review and a recent consultation from MOHLTC/MTCU Assistant Deputy Minister Joshua Tepper to the Steering Group, we are recommending that the Steering Group organize a strategic planning retreat in the Fall of 2007, with a group of stakeholders both internal and external to the Faculty of Medicine, to address the priority issues they have identified. The Dean will fund an expert consultant to manage this process. We are of the view that envisioning the future of health care and the role of physicians in 030 is necessary to guide continuous quality improvement in the content and delivery of the ME curriculum.
2U Although the Dean's Strategic Plan will be complete by mid‐Fall 2007, it will provide only general direction for physician education in our Faculty. It will articulate high level vision, mission and values. Implementation will require very specific direction within our education programs
Undergraduate Medical Education Review 2005‐2010
68
including UME, coordination across education programs, and effective integration with all of our epartments participating in the delivery of UME, with particular emphasis on our Clinical D
Departments. The Reviewers have again identified one of the most worrisome findings of the Generalism Task Force, namely the recognition by some of the Department Chairs of "disturbing and demeaning attitude" to generalists/Family Medicine. Further, the reviewers identify that our students believe that those among them who have interest in Family Medicine are marginalized. This matter will be addressed at all levels in our medical education programs, in our Clinical Departments and affiliated hospitals. The root cause of out‐dated attitudes and beliefs will be discerned and zero tolerance of inappropriate professional behaviour toward our students or other members of our cademic family will be instituted. To this end, our Associate Dean Equity and Professionalism, avid McKnight, will be fully engaged with the Dean and Vice Dean UME in next steps.
aD
3. Curriculum Mapping The importance of detailed curriculum mapping to help inform the curriculum committee in planning changes was noted. We agree, and have worked with the Discovery Commons, Academic Computing Division to hire an expert to work the Faculty on this task. It is expected that the results will be available this Academic year. This information will assist the Curriculum Committee to fulfill its mandate.
4. Flexibility in Planning
The reviewers comment that more flexibility is needed between clerkships than within them in order to achieve overall curriculum objectives. A curriculum management structure as noted above that can accomplish this is key. We are in agreement that a modern MD curriculum needs to be nimble, and appropriately responsive to new pedagogical methods and curriculum topics. Importantly, the Faculty of Medicine at the University of Toronto should be in position to take advantage of opportunities to innovate and assume the responsibility as a national leader in areas of strength, e.g., integration of research experience within the UME curriculum.
5. Early Clinical Experiences
The reviewers recommend half day clinical experiences for career sampling and early exposure to clinical settings in the preclerkship. This recommendation is in keeping with those of the Generalism Task Force. We are in agreement, and this year will pilot early student placement in family doctor’s offices. In support of this decision, we have informally listened to our students over the past two years during "fireside chats" and other venues and every student has requested more clinical experience in preclerkship. Our students are anxious to learn first hand what being a hysician is all about. We believe this is an important step in enabling our medical students to nderstand their choice about future residency training. pu
6. Learning Objectives The importance of completely defining the requisite knowledge competencies of the graduating students, particularly in the medical expert/skilled clinical decision maker role is highlighted. Ongoing curriculum mapping should assist with this critically important aspect of UME teaching nd learning. In addition, reports of the UME Program Evaluation Committee will aid in the ssessment of whether these objectives are achieved. aa
ted on 7. eLearning
enThe importance of technologies in increasing available learning opportunities is commby students to the reviewers. We are in agreement with this, and indeed the Faculty and Discovery Commons are moving forward rapidly in this area. This includes electronic curriculum on BlackBoard, evaluations on MedSIS, and videoconferencing capabilities within
Undergraduate Medical Education Review 2005‐2010
69
nsew lectures theatres and studios in the MSB, and Academies. Increased opportunities for our tudents to interact directly with the Director of Academic Computing will be sought.
8. Electives The reviewers comment that the electives program which represents the largest clerkship
ives. course (18 weeks) has not had a Director for over six months. There is an opportunity for
egories of institutional objectinnovation to align this course more closely with the seven catThe Director’s role should be filled as a priority. We are in agreement, and in fact have just recruited a talented clinician‐educator to this important role. Our Clinical Departments should embrace the elective opportunities both in preclerkship and in clerkship to promote interest of our medical students in their disciplines. The positive effect of mentorship on individual students and their decisions to enter specific disciplines of practice should be very apparent as we have many examples of outstanding postgraduate trainees and faculty members who were originally mentored as medical students during elective time in our Clinical Departments.
9. Other related issues
i. The Reviewers recommend that once the Faculty of Medicine’s strategic plan has been finalized and priorities set, the clerkship schedule will need to be addressed again. We agree that the concept of a pre‐ CaRMS period of core clerkships, and a post‐CaRMS schedule allowing for some specialization based on student interests has merit. Significant opportunities for innovation exist here.
ii. The Reviewers suggest that because the clerkship course directors’ should plan, implement and review their own Departmental clerkship goals and work in the best interest of the institution without regard for parochial interests, a dual reporting structure for the course directors is supported with assessment and accountability shared between the overall clerkship Director and the relevant Department Chair. As part of the function of the Curriculum Committee Clerkship Subcommittee function, a dual accountability can be readily
established and should prove advantageous.
iii. Several comments were made by student and graduates regarding evaluation methodology
and grading systems used in the clerkship programs. These will be studied closely.
iv. The issue of balance of Generalism/Specialty Curriculum will be highlighted in the Strategic Planning Document, with recommendations as to the increasing importance of interdisciplinary education, community and ambulatory teaching, and exposure to strong generalist role models.
v. Although seen as a strength, the students made several comments regarding pedagogical methods utilized in the clerkship including the use of lectures, seminars and labs etc. Again,
these will be studied closely, and where appropriate, changes made.
y we thank the Reviewers for such a comprehensive and helpful report. Once again, ma ay Rosenfield
uate Medical Education JVice‐Dean, Undergrad
e atharine Whitesid
cine CDean of Medi August 2007
Undergraduate Medical Education Review 2005‐2010
70
Appendix 2.4 CURRICULUM REVIEW STEERING GROUP TERMS OF REFERENCE AND MEMBERSHIP
Undergraduate Medical Education Curriculum Steering Group
TERMS OF REFERENCE
Authority Operates under the authority the Dean to the Vice‐Dean, Undergraduate Medical Education.
Purpose: To operate in the context of the Dean’s overall strategic planning process, is as follows:
1. To make high level recommendations to Faculty of Medicine Leadership and Governance regarding the overall structure of the undergraduate MD program.
2. Identify key strengths of the current program.
3. Identify areas for improvement, with recommendations for implementation.
This incl on of the following key issues:udes but is not limited to examinati
• Social Accountability of Curriculum • Pedagogical structure, including use of lectures, seminars, labs, e‐
learning, PBL, cased‐based learning, bedside teaching, and self‐directed learning
• Specialty/Generalist Balance in the Curriculum • Curriculum Management Structure, including roles of curriculum
committees, and mechanisms to respond to new curriculum needs
• Course structure • esources Distributed Medical Education/Use of Community R• Electives length and placement in curriculum • ship and Clerkship Length of total program, Preclerk• d Clerkships Length of Courses an• Grading System • Admissions Policies • Joint Programs e.g., MD/PhD, other new MD/masters programs
This group will also operate in the following context:
1) The U of T MD program is fully accredited until 2011‐2012 academic year, doing well, and the spirit of the Steering Group work will be one of continuous quality improvement as opposed to the total
Undergraduate Medical Education Review 2005‐2010
71
curriculum “renewal” which is often mandated by external accreditation bodies.
2) This review will not examine detailed curriculum content of courses, as this has been done by the accreditation process.
3) The Overall Goals and Objectives of Program, approved by Faculty Council in 2003 are assumed to be current and valid.
(See: http://www.facmed.utoronto.ca/Assets/ume/goalsobj.pdf )
Membership: 1. Adrian Brown2. Anita Rachlis 3. Anna Jarvis 4. Brian Hodges 5. Glen Bandiera 6. o Helene Polatajk7. Ian Wagg 8. Jay Rosenfield 9. Karen Leslie 10. Karl Torbicki 11. Kate Bingham 12. Kevin Imrie 13. Leslie Nickell 14. Martin Schreiber 15. Peeter Poldre 16. Rayfel Schneider 17. Richard Reznick 18. s Stephen Matthew19. Wendy Levinson
Administration: Administrative support is provided by the Curriculum Coordinator. Minutes of each meeting will be recorded and circulated to all members
Reporting: The Committee reports through its Chair to the Dean, and ultimately to the Faculty Council.
Schedule: The Undergraduate Medical Education Curriculum Steering Group will meet over the next 5‐6 months, and develop recommendations for Faculty review.
Approved: Date: 2007/04

Undergraduate Medical Education Review 2005‐2010
72
Appendix 2.5 HIGHLIGHTS OF THE STUDENT CURRICULUM REVIEW REPORT EMxcerpt taken from: University of Toronto UME Curriculum Review Planning Retreat ay 12, 2008.
Student Curriculum Leaders, Ian Wagg and Karl Torbicki reported on work that they had done with Andrew Brown and Jovana Yudin on the student UME curriculum review. Approximately one year ago the Curriculum Review Steering Group asked the students to conduct a curriculum review with the goal of improving UME. With support from the Wilson Centre, 58 students from across the four years of the medical school participated in eight focus groups, where participants were encouraged to reflect on various aspects of their experience in medical school to date. This led the student leaders to generate key themes and principles for UME curriculum reform. The following are the six major hemes that emerged from the consultation. t
1. Clinical relevance – students want science with applicability. They want teaching coordinated with hands‐on opportunities so they can apply the detail they learn to the real world within the appropriate context with a focus on common conditions. They also feel applied learning is the best way to learn (e. . g. ASCM, hearing patient experiences, Day of the Doctor type experiences) 2. Clinical exposure – students would like opportunities for career exploration to instantiate learning. They acknowledge the game that must be played to get into residencies and want more clinical exposure to help them decide. 3. Evaluation – students are seeking input on their progress towards becoming physicians and less focus on their knowledge of what they consider to be minutiae. Ideally, they would receive mmediate, individualized, specific oral feedback based on direct observation. This is nconsistent with the curii rent clerkship evaluation. 4. Overspecialization – students want contextualized teaching in varied learning settings. They would like greater balance between generalist and specialist perspectives, and feel this could be achieved through overviews of complex topics, done by clinical teachers and more rural placements. 5. Course delivery students would like to have more peer‐to‐peer interaction, better modelling of best practices, lectures coordinated with the practical, enhanced IT learning, and more responsibility. For the preclerkship, they would like smaller group learning, more experiential content and clinician‐led seminars, and a curriculum augmented by technology. For the clerkship, they want more learning in the clinical context, near‐peer learning and real case‐based learning. 6. Nonbiomedical – the students want high‐quality teaching with practical content. They want teaching around the CanMEDS competencies and the four principles of Family Medicine,
ependent projects. including small group ethics teaching, community visits and ind
ased on the identified the B
mes, three guiding principles emerged:
1. Be about medicine – student feel that the preclerkship is simply a continuation of

Undergraduate Medical Education Review 2005‐2010
73
uindergraduate studies and they really want to learn to be physicians in practice. Being involved n patient care early was said to be very motivating. 2. Create sense of growth – students want a better idea of their goals and career reality. The reclerkship and clerkship need to be better integrated and less “siloed”. Students would like lear process indicators apc nd explicit feedback regarding their development as professionals. 3. Capitalize on idealism – students would like UME to capitalize on their early enthusiasm, to create a sense of commitment to society, and to promote and take advantage of extra‐curricular pursuits.
Undergraduate Medical Education Review 2005‐2010
74
Appendix 2.6 UNDERGRADUATE MEDICAL EDUCATION CURRICULUM COMMITTEE TERMS OF REFERENCE AND MEMBERSHIP
Undergraduate Medical Education Curriculum Committee
TERMS OF REFERENCE
Authority Operates under the authority of Faculty Council with delegated responsibility from the Dean to the Vice‐Dean, Undergraduate Medical Education. Has final management authority in setting MD curriculum.
Purpose: The curriculum committee has overall responsibility for the design,
implementation, management, and evaluation of the undergraduate MD education program. The primary goal of the committee is to assure an undergraduate learning experience which allows students to develop the knowledge, skills and attitudes that will prepare them optimally for entry into postgraduate programs, and ultimately, into medical practice. The Committee achieves this goal through: oversight of the development, implementation, integration, and evaluation of the component courses of the Preclerkship and Clerkship, ensuring that the overall curriculum is both coherent and coordinated, and by providing a forum in which incremental curriculum renewal and improvement takes place on a continuous basis. Members are appointed by the Dean, on the recommendation of the Vice‐De , UME. an
Membership: 1. ucation (Chair)Vice‐Dean, Undergraduate Medical Ed
2. Preclerkship Director (Co‐Vice Chair) 3. Clerkship Director (Co‐Vice Chair) 4. rald, and Academy Directors‐Wightman‐Berris, Peters‐Boyd, Fitzge
Mississauga (4) 5. Representative, Medical Students‐ Senior VP Curriculum 6. t Affairs, and Associate Deans‐ UME, Health Professions Studen
Undergraduate Medicine Admissions and Student Finances (2) 7. al Education Representative, Postgraduate Medic8. Representative, Clinical Chairs (2) 9. Representative, Community Sector 10. Representative, Basic Science Chairs 11. Representative, resident al umni 12. Representative, Fully Affilia ted and Community Hospitals (2) 13. Representative, Educators Note: One individual may represent two constituencies
Undergraduate Medical Education Review 2005‐2010
75
Appendix 3.1 COMPREHENSIVE RESEARCH EXPERIENCE FOR MEDICAL STUDENTS RESEARCH DAY 2008
DEVENT ETAILS AND WINNERS
The 22nd annual Undergraduate Medical Student Research Day was held on January 24th, 2008. A total of 134 abstracts [~107 CREMS and 27 nonCREMS] from a broad range of research areas were resented from all years of the MD program. 40 Faculty members provided their time to read and djudicate the many posters and the Keynote address was delivered by Dr. Endel Tulving. pa
George Brown Memorial Scholarship Awards were given to MD students judged to have the best poster presentations in several different categories. This year, there was a tie in the Basic Science category. The winners were:
• Basic Science: Peter Wu 1T0 Supervisor: Carol J. Swallow (Department of Surgery, Mount Sinai Hospital)
ke kinase 4 (PLK4) deficiency causes chromosomal instability and tumourigenesis. Project: Pololi
• Basic Science: Sarah Chan 1T0 Supervisor: Michael G. Fehlings (Department of Surgical Oncology, Toronto Western Research Institute)
tion of a combined therapeutic strategy for repair of chronic spinal cord injury. Project: Examina
• Clinical Science: Marat Slessarev 1T0 Supervisor: Joseph A. Fisher (Department of Anesthesia, Toronto General Hospital)
rovascular reactivity in patients with brain arteriovenous malformations.
Project: Cereb
• Health Care: Goldie Kurtz 0T9 Supervisor: Sharon Sharir (Department of Surgery, Sunnybrook Research Institute) Project: Toward quality measures in bladder cancer surgery: A populationbased assessment of
tectomy in Ontario.
radical cys
• MD/PhD: Benjamin Steinberg 1T1 Supervisor: Sergio Grinstein (Department of Biochemistry, Hospital for Sick Children)
the counterion conductance required for lysosomal acidification. Project: The nature of
• International Health: Shail Rawal 0T9 Supervisor: Richard B. Lee (Department of Anthropology, University of Toronto) Project: The needs and experiences of informal caregivers of persons living with HIV/AIDS in
Katutura.
Overall Winners: Three projects with the highest overall marks were selected to represent the University of Toronto at the Eastern‐Atlantic Student Research Forum in Miami, Florida. The following students were selected: arah Chan, Peter Wu, and Benjamin Steinberg. S
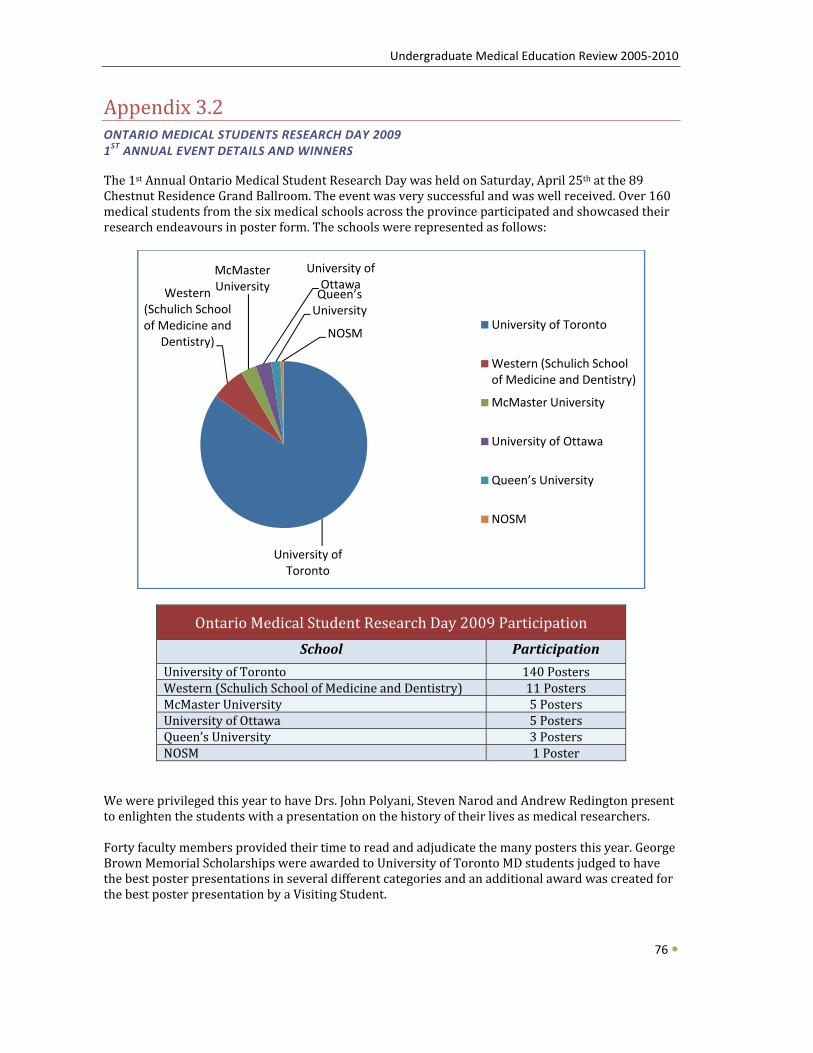
Undergraduate Medical Education Review 2005‐2010
Appendix 3.2 ONTARIO MEDICAL STUDENTS RESEARCH DAY 2009 1ST ANNUAL EVENT DETAILS AND WINNERS
The 1st Annual Ontario Medical Student Research Day was held on Saturday, April 25th at the 89 Chestnut Residence Grand Ballroom. The event was very successful and was well received. Over 160 edical students from the six medical schools across the province participated and showcased their esearch endeavours in poster form. The schools were represented as follows: mr
76
Ontario Medical Student Research Day 2009 Participation School P articipation
University of Toronto 1 40 PostersWestern (Schulich School of Medicine and Dentistry) 11 Posters McMaster University 5 Posters University of Ottawa 5 Post ersQueen’s University 3 Post ersNOSM 1 Poster
University of Toronto
Western (Schulich School of Medicine and
Dentistry)
McMaster University
University of OttawaQueen’s University
NOSMUniversity of Toronto
Western (Schulich School of Medicine and Dentistry)
McMaster University
University of Ottawa
Queen’s University
NOSM
e were privileged this year to have Drs. John Polyani, Steven Narod and Andrew Redington present W
to enlighten the students with a presentation on the history of their lives as medical researchers. Forty faculty members provided their time to read and adjudicate the many posters this year. George Brown Memorial Scholarships were awarded to University of Toronto MD students judged to have the best poster presentations in several different categories and an additional award was created for the best poster presentation by a Visiting Student.
Undergraduate Medical Education Review 2005‐2010
77
T he winners were:
• Basic Science: Mark Davis (1T1) Supervisor: Peter Backx
ptical mapping and intracardiac ecg with programmed stimulation demonstrate the nduction system
Poster: Orole of Irx3 in the cardiac co
• Clinical: Pearl Behl (1T0) Supervisor: Sandra Black
inhibitor treatment slows decline in multiple cognitive domains in ear, prospective, cohort study
Poster: CholinesteraseAlzheimer's Disease: A 1Y
• International Health: Taulee Hsieh (1T1) Supervisor: David Zakus
lthcare seeking be aviour of the most vulnerable families list participants in Kep, Poster: Hea hCambodia
• First Year: James Jung (1T2) ri Rotstein
on of macrophages is mediated by sphingosine1phosphate Supervisor: OPoster: Oxidantinduced activati
• Health Care: Yewande Akinfemiwa (1T0) r: Joyce Nyhof‐Young
uating a braguide for female breast cancer patients SupervisoPoster: Designing and eval
• MDPHD: Adam Durbin (1T1) Supervisor: David Malkin
mines the oncogeniPoster: Jnk1 deter c or tumorsuppressive activity of Ilk in rhabdomyosarcoma
• Visiting Student: Yiannis Iordanous (University of Western Ontario) (Clinical) Supervisor: Amit Garg Poster: Transplant outcomes for recipients of kidneys from medically complex living donors: Examining the gap between current evidence and practice
Undergraduate Medical Education Review 2005‐2010
78
Appendix 4.1 UNIVERSITY OF TORONTO FACULTY OF MEDICINE DISTRIBUTED EDUCATION EXTERNAL REVIEW RECOMMENDATIONS SEPTEMBER 15, 2009:
Recommendations:
1: LANGUAGE
Use language of “integrated education” rather than “distributed education”. Integrated education must be pedagogically driven.
2: VISION
Create a vision for an integrated educational continuum across the Faculty and partner institutions.
3: COORDINATION
Create a system of organized, structured coordination within the Faculty and with hospital partners.
4: ACADEMY STRUCTURE
Revisit the vision and structure of the Academy model, including opportunities to leverage the strength of the Academy structure to create a Network of Networks that could be accessed by undergraduate, postgraduate and other health sciences programs.
5: MISSISSAUGA ACADEMY
Use the Mississauga Academy as a pilot site for integration and continuity across undergraduate and postgraduate programs. Assess this model and use lessons learned in relation to recommendation #4 above.
6: FACULTY INFRASTRUCTURE
Create a senior leadership role in the Faculty with the portfolio of integrated health sciences education.
7: FUNDING
Advocate for funding resolution at a number of levels: provincial resolution of operating funding for undergraduate and postgraduate expansion; provincial resolution of community physician compensation; and response by government to the Mississauga Academy budget proposals.
8: INFORMATION TECHNOLOGY
Improve quality of information technology across the Faculty to support the vision of educational integration.
9: RESEARCH
Recognize the research opportunities brought to the table by community affiliates through their patient population base.





























