Embed Size (px)
Citation preview

ORIGINAL ARTICLE
Urinary transforming growth factor-b1, collagen IV and the effect ofinsulin in children at diagnosis of diabetes mellitus
PETER HOLMQUIST1 & OLE TORFFVIT2
1Department of Paediatrics and 2Institute of Clinical Sciences, Department of Renal Medicine, University Hospital Lund,
Sweden
AbstractObjective. This study investigated whether metabolic derangement at diagnosis of diabetes mellitus affects the function ofthe basement membrane and the excretion of several components and whether insulin treatment can normalize this. It wasdesigned to evaluate urinary excretion rates of transforming growth factor-b1 (TGF-b1), the carboxy-terminal domain ofcollagen IV (NC1) and albumin in children during the first 20 days of treatment after diagnosis of type 1 diabetes. Materialand methods. Thirty-four newly diagnosed diabetic children between 4 and 16 years of age and 26 healthy children ofmatching age were studied with timed overnight urine collections. Urine was collected during the first 20 days of treatment.Results. Urinary excretion of albumin and TGF-b1 in diabetic children were significantly increased at entry but normalizedduring 20 days of treatment with insulin compared with control children. In contrast, the non-significant high NC1excretion at diagnosis did not change but became significantly increased after 20 days of insulin treatment. Overall, thekidney size was within normal limits and unaffected by treatment. The largest kidneys had less NC1 excretion (R��0.67,pB0.05, n�13) and a lower glomerular filtration rate (R��0.77, pB0.01, n�10) than the smallest kidneys. After20 days of treatment TGF-b1 excretion had decreased in children with kidney size�8.5 cm. Conclusion. Correction of themetabolic derangement with insulin decreased excretion of albumin and TGF-b1, but had no effect on kidney size and urineNC1 excretion, presumably because the observation period was too short.
Key Words: Albuminuria, children, collagen IV, type 1 diabetes, transforming growth factor-b
Introduction
Urine cytokines and growth factors are involved in
the development of glomerular and tubular hyper-
trophy and basement membrane thickening, char-
acteristics of diabetic nephropathy [1�4]. An
important cytokine in this context is transforming
growth factor-b1 (TGF-b1) [5]. This is up-regulated
by hyperglycaemia within 24 h of onset of diabetes in
the rat model and attenuated by insulin [6]. TGF-b1
is implicated in the pathogenesis of diabetic glomer-
ulosclerosis and tubulointerstitial fibrosis [7,8]. Dia-
betic patients with an increased urinary TGF-b1
excretion rate are prone to developing nephropathy
[8�10]. TGF-b1 stimulates collagen formation in the
extracellular matrix [1,7,9,11] and proteoglycan
synthesis [12]. One of the end-products is collagen
IV [1]. A high urine collagen IV excretion rate in
diabetic patients has been described as being asso-
ciated with renal function and size [7,13,14].
High blood glucose stimulates and angiotensin-
converting enzyme (ACE) inhibition decreases
TGF-b1 levels [9,11,15]. A direct effect of insulin
on the TGF-b1 excretion rate has been suggested
[14,16]. Few studies on urinary TGF-b1 excretion
are available in newly diagnosed diabetic patients
[17], especially in children [16,18,19]. In rat models
ACE inhibition [20] and monoclonal anti-TGF-bantibodies [21] affect TGF-b1 and collagen IV. The
combination fully arrests the renal injury of diabetic
nephropathy [22].
The hypothesis in this study was that correction of
the metabolic derangement with insulin affects the
function of the basement membrane and several of
its components and that insulin treatment may
normalize this. In humans studies of the kidney
Correspondence: P. Holmquist, Department of Paediatrics, University Hospital, SE-221 85 Lund, Sweden. Tel: �46 46 171000. Fax: �46 46 145459.
E-mail: [email protected]
Scandinavian Journal of Urology and Nephrology, 2009; 43: 142�147
(Received 13 February 2008; accepted 23 September 2008)
ISSN 0036-5599 print/ISSN 1651-2065 online # 2009 Informa UK Ltd. (Informa Healthcare, Taylor & Francis AS)
DOI: 10.1080/00365590802502111
Scan
d J
Uro
l Nep
hrol
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
SUN
Y S
tate
Uni
vers
ity o
f N
ew Y
ork
at S
tony
Bro
ok o
n 10
/26/
14Fo
r pe
rson
al u
se o
nly.

have to be done indirectly. Thus, the study was
designed to evaluate urinary excretion rates of TGF-
b1, the carboxy-terminal domain of collagen IV
(NC1), glycosaminoglycans (GAG), Tamm-Horsfall
protein (THP) and albumin in children during the
first 20 days of treatment after diagnosis of type 1
diabetes.
Material and methods
Subjects
The recruiting area of the Department of Paedia-
trics, University Hospital in Lund, has approxi-
mately 250 000 inhabitants, of whom 50 000 are
under the age of 15 years. Included in this study
were children with initial diagnosis and subsequent
treatment at this department. Thirty-four children
were between 4 and 16 years of age. As control
subjects, 26 healthy school children of similar age
participated. All participants were of Caucasian
origin. Children and parents gave their informed
consent, and the local ethics committee approved
the study.
Metabolic treatment
The study started at diagnosis of diabetes and ended
after 20 days of treatment at the hospital. During
this time metabolic derangement was corrected and
the blood glucose normalized. After admission, all
children were treated with intravenous insulin at
0.05�0.20 U/kg/h together with saline solution
(130 mmol Na, 4 mmol K, 2 mmol Ca, 1 mmol
Mg, 30 mmol Ac, 110 mmol Cl) at 4�10 ml/kg/h.
Treatment during the first 12 h aimed at blood
glucose 10 mmol/l. When blood glucose was stable
(B10 mmol/l) the saline solution was changed to
5% glucose and 40 mmol/l of sodium and potassium
added. Within 36 h the intravenous was changed to
subcutaneous insulin injections. Fast-acting insulin
was given as four divided doses during the subse-
quent 3�5 days. Thereafter, medium-acting insulin
was started with an overnight dose. At discharge
after 3 weeks most children had combined doses of
fast- and medium-acting insulin in the morning and
afternoon, and medium-acting insulin was given at
night. Older children were treated with rapid-acting
insulin at lunchtime.
Methods
On days 1 and 20 venous blood tests were taken in a
resting position and fasting between 07.00 and
09.00 h. Timed overnight urine collections were
analysed. Albumin [23], THP [24] and NC1 [13]
were analysed with an enzyme-linked immunosor-
bent assay (ELISA) technique as described pre-
viously. GAG was analysed as described previously
[25]. Biologically active TGF-b1 was analysed with a
commercially available solid-phase sandwich ELISA
(Emax Immunoassay System; Promega Corp., Ma-
dison, WI, USA). Serum and urinary concentrations
of creatinine were analysed by an enzymic method
(creatinine-hydrolase; EKTA Chem-analyser Instru-
ment, Kodak, New York, USA). Serum creatinine
reference values for childrenB5 years�35�70 mol/l,
5�10 years�40�85 mol/l and 10�15 years of age�50�90 mol/l. Ketonuria was measured on the day of
diagnosis (day 0) with urine Ketodiabur Dipsticks
(Boehringer Mannheim, Mannheim, Germany).
Glycosylated haemoglobin (HbA1c) was measured
on the day of diagnosis with high-speed equipment
(DCA 2000; Bayer, Germany) or cation-exchange
chromatography on high-performance liquid chro-
matography (HPLC) (Auto-A; Kyoto-Diaiichi, Ka-
gaku Co., Kyoto, Japan), both with a normal value of
4�6%. The methods were adjusted to give similar
results. Hemocue (Angelholm, Sweden) and Gluc-
ometer Elite (Bayer Diagnostica, Zurich, Switzer-
land) were used to measure blood glucose. Blood
glucose on days 1 and 20 was calculated as the mean
of a minimum of five measurements a day.
A trained paediatric radiologist measured kidney
size with ultrasonography (Toshiba SSA-270A). The
kidney size was taken as the mean from three
measurements of the length in both kidneys. They
were judged according to renal ultrasound measure-
ments described in control children aged 9�10
years�9.2 cm (SD 0.9) and 10�11 years�9.2 cm
(SD 0.8) [26]. According to these results kidney size
is between 8 and 10 cm for children between 4 and
16 years of age. Glomerular filtration rate (GFR)
was measured as the clearance of an intravenous
injection of 5 ml of iohexol (Omnipaque 300 mg I/
ml non-ionic contrast medium) on days 1 and 20 in
a non-fasting state [27]. Age-related reference values
using capillary measurements at 3 and 4 h ranged
from 75 to 125 ml/min/1.73 m2.
Statistics
Results are given as the median and range. Spear-
man’s correlation coefficient and Mann�Whitney U
test were used. For differences between and within
groups on different days chi-square with Fisher’s
exact test was used. Differences between different
days were tested with Wilcoxon’s paired test. Sig-
nificance was taken as pB0.05 (two-tailed). The
data were analysed using the Statistical Package for
Social Sciences (SPSS, Chicago, IL, USA).
TGF-b1, collagen and insulin in diabetes 143
Scan
d J
Uro
l Nep
hrol
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
SUN
Y S
tate
Uni
vers
ity o
f N
ew Y
ork
at S
tony
Bro
ok o
n 10
/26/
14Fo
r pe
rson
al u
se o
nly.

Calculations
Body mass index (BMI) was calculated as kg/m2.
Excretion rates were calculated in relation to
1.73 m2 body surface area (�weight0.425�height0.725�71.84/100) to adjust for size and gender
or as the ratio between the substances measured and
urine creatinine.
Results
At diagnosis base deficit was �0.2 (�26 to 5)
mmol/l, pH 7.37 (7.06�7.44) and blood glucose
21.9 (9.1�49) mmol/l. Twenty-one out of 34 chil-
dren had ketonuria at entry. Urinary excretion rates
of albumin, TGF-b1, THP, GAG and NC1 were
similar in children with and without ketonuria and
not affected by gender (data not shown). Table I
shows the baseline and day 20 data for all diabetic
and control children. At entry urinary TGF-b1 and
albumin were significantly higher in diabetic than in
control children. On day 20 albumin and TGF-b1
had normalized. There was no significant difference
between NC1 excretion at entry and day 20, and on
day 20 the excretion was significant higher than in
control children. After 20 days BMI was increased,
insulin dose decreased from 1.4 (0.0�3.5) to 0.6
(0.2�1.0) units/kg (p�0.000) and the median of the
daily mean blood glucose decreased. THP and GAG
excretion were unchanged during the treatment
period.
Kidney size was measured in 14 patients at entry
and repeated in five patients on day 20. In addition,
two patients not measured at entry were tested on
day 20. Thus, in total seven patients were measured
on day 20. The kidney size was normal in compar-
ison with a normal reference material with a kidney
size of 8�10 cm for children between 4 and 16 years
of age [26]. In the present study, the children had a
median age of 10 years and a median kidney size of
9 cm. No correlation was found between kidney size
on day 1 (0.509, n�14) and day 20 (0.382, n�7)
and age. There was no change in renal size or GFR
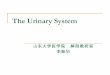
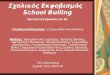
during the 20 days. At entry patients with largest
kidneys had a low NC1 excretion rate (R��0.77,
p�0.002, n�13) (Figure 1) and decreased GFR
(R��0.77, p�0.009, n�10) (Figure 2). In con-
trast, on day 20 patients with large kidneys had a
high excretion of albumin (R�0.86, p�0.014) and
Figure 1. At diagnosis, diabetes patients with the largest kidneys
had low urinary excretion of the C-terminal domain of collagen IV
(NC1)/min/1.73 m2 (R��0.77, p�0.002, n�13).
Table I. Data on diabetic children on days 1 and 20, and control children.
Diabetic day 1 Diabetic day 20 Control
(n�34) (n�31) (n�26)
Age (years) 10 (4�16) 10 (7�12)
Gender (M/F) 17/17 15/16 8/13
BMI 16 (13�23) 17 (13�23)** 17 (14�27)
HbA1c (%) 10.0 (5.6�15.3)
Mean blood glucose (mmol/L) 11.0 (6.8�16.7) 5.7 (4.4�8.9)***
S-Creatinine (mmol/l) 44 (29�75) 45 (32�73)
GFR (ml/min/1.73 m2) 132 (93�223) 130 (87�187)
Kidney size (cm) 9.0 (7.3�10.5) (n�14) 8.7 (7.7�10.3) (n�7)
Albumin/creatinine (mg/mmol) 1.1 (0.05�14.6)$$ 0.45 (0.04�4.9)** 0.55 (0.03�26.6)
TGF-b/creatinine (ng/mmol) 0.08 (0.01�73.1)$ 0.03 (0.01�32.0) 0.02 (0.01�3.1)
NC1/creatinine (ng/mmol) 1.5 (0.2�6.3) 2.0 (0.4�25.6)$ 0.8 (0.5�3.4)
THP/creatinine (mg/mmol) 5.54 (0.09�23.7) 3.21 (0.18�65.3) 9.24 (0.5�22.1)
GAG/creatinine (mg/mmol) 6.5 (0.3�17.7) 5.8 (1.2�69.5) 8.2 (4.5�13.4)
Data are given as median (range).
BMI�body mass index; HbA1c; glycosylated haemoglobin; GFR�glomerular filtration rate of iohexol; TGF�transforming growth factor;
NC1�C-terminal domain of collagen IV; THP�Tamm-Horsfall protein; GAG�glycosaminoglycans.
***pB0.001, **pB0.01 vs day 1; $$pB0.01, $pB0.05, vs control.
144 P. Holmquist & O. Torffvit
Scan
d J
Uro
l Nep
hrol
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
SUN
Y S
tate
Uni
vers
ity o
f N
ew Y
ork
at S
tony
Bro
ok o
n 10
/26/
14Fo
r pe
rson
al u
se o
nly.

a larger insulin dose (R�0.81, p�0.027) than
patients with smallest kidneys.
At entry, no association was found between NC1
excretion and GFR or TGF-b1, nor between TGF-
b1 and kidney size and GFR. However, if urine data
from controls were included, a correlation was
revealed between urine NC1 and TGF-b1 excretions
on day 1 (R�0.39, p�0.006, n�49) but not on
day 20 (R�0.27, p�0.072, n�46). No associations
were found between GFR, albumin, GAG, THP,
NC1 or TGF-b1 excretions and HbA1c, or mean
blood glucose. Urine NC1 was associated with GAG
(R�0.39, p�0.026, n�33), which was associated
with THP (R�0.49, p�0.004, n�34), which was
associated with NC1 (R�0.52, p�0.002, n�33).
On day 20, a high insulin dose per kilogram body
weight was associated with increased urinary excre-
tion of TGF-b1 (R�0.36, p�0.046). On day 20,
TGF-b1 was associated with renal size (R��0.76,
p�0.049, n�7). Five out of seven patients with
kidney size above 8.5 cm had no excretion of
TGF-b1.
Discussion
At diagnosis of diabetes mellitus, increased urinary
excretion rates of albumin, TGF-b1 and NC1 were
found compared with control children. Treatment
for 20 days normalized albumin and TGF-b1 but not
NC1 excretion rates. A high blood glucose stimu-
lates hypertrophy of tubular cells [4,11], and in-
creased urinary TGF-b1 excretion [3,9,11] and
collagen IV production [4,9]. Metabolic control,
measured as HbA1c, may [17,28] or may not
[16,18,19] correlate with urinary TGF-b1 excretion.
In this study, no association was found between
HbA1c, blood glucose and TGF-b1 excretion at
entry. Sustained high urinary TGF-b1 excretion
has been found in children at the onset of diabetes
[16] and in prepubertal and postpubertal children
[19]. However, the excretion of TGF-b1 may also be
low [18]. An elevated TGF-b1 excretion may be the
result of an inflammatory reaction or an immunolo-
gical response mediated by TGF-b1 itself [17]. In
the kidneys TGF-b1 is filtered across the glomerular
capillaries or secreted from epithelial cells in the
tubular system [7].
Insulin increases TGF-b1 production [14,16] but
may decrease urinary excretion [11,28]. Treatment
with insulin decreased urinary excretion of albumin
and TGF-b1, but did not significantly affect NC1
excretion and kidney size. Whether this is due to
insulin itself or to normalization of glycaemia or any
other effect of insulin is unclear. The normalization
of high TGF-b1 excretion in the present study may
reflect an effect of insulin treatment [11,28] and an
improved metabolic control [17]. An association
between insulin dose and TGF-b1 excretion was
actually found on day 20. Insulin affects both renal
size and GFR [29]. Renal size decreases with
achievement of good metabolic control [30] and
persistent large kidneys are predictive of the devel-
opment of renal insufficiency [31]. In the present
study the median renal size for children between 4
and 16 years of age was within normal limits of 8�10 cm [26] and did not change during treatment.
Those children with the largest kidneys on day 1 had
reduced GFR and excreted less NC1. A low GFR
due to poor metabolic control may be compensated
by an increase in renal size (tubular mass). Since
kidney size was measured twice in only five patients
and in another two patients only on day 20 these are
uncertain data regarding changes in or related to this
parameter. The association between NC1 and GAG
and THP found in the present study indicates that
NC1 production may be increased not only in the
glomerular basement membrane but even in the
tubular membranes. However, those with the largest
kidneys at entry had a decreased NC1 excretion.
This is in contrast to a positive correlation between
NC1, GFR and kidney size previously found in an
adult population of patients with a long duration of
diabetes [32]. As the adult population was in a stable
metabolic status the negative association in the
present study must be caused by a deranged meta-
bolic status at entry characterized by glucosuria and
insulin deficiency [17]. A decreased excretion of
THP is in keeping with an experimental study in the
diabetic rat showing decreased production in large
kidneys [33]. Similarly, the synthesis of NC1 and
Figure 2. At entry patients with largest kidneys had decreased
glomerular filtration rate (GFR) (R��0.77, p�0.009, n�10).
TGF-b1, collagen and insulin in diabetes 145
Scan
d J
Uro
l Nep
hrol
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
SUN
Y S
tate
Uni
vers
ity o
f N
ew Y
ork
at S
tony
Bro
ok o
n 10
/26/
14Fo
r pe
rson
al u
se o
nly.

GAG may be expected to decrease, as decreased
excretion of TGF-b1 was seen in large kidneys.
Diabetic patients without microalbuminuria have
increased collagen production associated with TGF-
b1 excretion [14]. In contrast, adult patients without
microalbuminuria using the present assay for NC1
have a normal excretion rate of NC1 that increases
with microalbuminuria and then decreases with
overt nephropathy [13]. Results in previous studies
on collagen IV depend on the assay and the antigen
used. In one study u-collagen IV increased as renal
function decreased, but no difference was found in
normoalbuminuric and microalbuminuric patients
[34]. The study by Watanabe et al., using the
collagen 7S domain, found high u-collagen IV in
patients with micro�macroalbuminuria [35]. In the
present study no association was found between
TGF-b1 and NC1 urinary excretion in the diabetic
patients, but with the control group included an
association was found on day 1. The results indicate
that other factors than TGF-b1 re responsible for the
persistently high NC1 excretion.
Over time the relationship between synthesis and
breakdown of collagens may alter and adjust the
thickness of the basement membranes [4]. At
diagnosis the large filtrating capillary area seen in
prepubertal children may compensate for a mesan-
gial expansion [8,29] and explain the capacity to
excrete more NC1 and increase GFR even in
patients with small but still normal sized kidneys.
Furthermore, neutralization of TGF-b1 production
in a mouse model reverses mesangial expansion,
inhibits further decrease in GFR, but does not affect
albuminuria [9]. In the present study, albumin
excretion normalized during treatment, but those
with the largest kidneys continued to excrete more
albumin. These children also needed more insulin
and could represent a group of patients with more
deranged metabolic control at entry. In line with
many studies, this investigation found no association
between GFR and albumin, NC1 or TGF-b1 excre-
tion [2,3,8,17,19]. Serum creatinine and GFR were
unchanged during treatment.
Hyperfiltration has long been suggested to predict
the development of diabetic nephropathy [36�39].
Kidney hyperfiltration [18] and hypertrophy [19]
stimulate TGF-b1 production, which promotes
growth [11]. Angiotensin II blockade reduces renal
TGF-b1 production, which may be of significance as
TGF-b1 adjusts homeostasis and renal hyperfiltra-
tion through vasoconstriction properties [11,15].
After 20 days of treatment TGF-b1 was associated
with renal size in the present study. This finding is,
however, of limited value since there were few
patients and only five out of seven patients had no
excretion of TGF-b1.
In conclusion, insulin treatment at diagnosis of
diabetes normalized increased excretion of both
albumin and TGF-b1. Thus, increased albumin
and TGF-b1 was probably caused by deranged
metabolic control. In contrast, insulin had no effect
on NC1. Longitudinal studies should be carried out
to clarify whether sustained high urinary excretion of
NC1 could be a marker of later nephropathy.
Acknowledgements
The help from Asa Pettersson, Renal Research
Laboratory, and the staff of the Paediatric Depart-
ment in Lund is highly appreciated.
References
[1] Lehmann R, Schleicher E. Molecular mechanism of diabetic
nephropathy. Clin Chim Acta 2000;/297:/135�44.
[2] Drummond K, Mauer SM. The early natural history of
nephropathy in type 1 diabetes: II. Early renal structural
changes in type 1 diabetes. Diabetes 2002;/51:/1580�7.
[3] Sato H, Iwano M, Akai Y. Increased excretion of urinary
transforming growth factor beta1 in patients with diabetic
nephropathy. Am J Nephrol 1998;/18:/490�4.
[4] Ziyadeh FN. Renal tubular basement membrane and
collagen type IV in diabetes mellitus. Kidney Int 1993;/43:/
114�20.
[5] Nicholas SB. Advances in pathogenetic mechanisms of
diabetic nephropathy. Cell Mol Biol 2003;/49:/1319�25.
[6] Shankland SJ, Scholeya JW. Expression of transforming
growth factor b1 during diabetic renal hypertrophy. Kidney
Int 1994;/46:/430�42.
[7] Hoffman BB, Sharma K, Ziyadeh FN. Potential role of
TGF-b in diabetic nephropathy. Miner Electrolyte Metab
1998;/24:/190�6.
[8] Fagerudd J, Groop P-H, Honkanen E, Teppo A-M, Gron-
hagen-Riska C. Urinary excretion of TGF-b1, PDGF-BB
and fibronectin in insulin-dependent diabetes mellitus pa-
tients. Kidney Int 1997;/52(Suppl 63):/195�7.
[9] Ziyadeh FN. Mediators of diabetic renal disease: the case for
TGF-b as the major mediator. J Am Soc Nephrol 2004;/15:/
55�7.
[10] Chen S, Jim B, Ziyadeh FN. Diabetic nephropathy and
transforming growth factor-beta: transforming our view of
glomerulosclerosis and fibrosis build-up. Semin Nephrol
2003;/23:/532�43.
[11] Border WA, Noble NA. Evidence that TGF-b should be a
therapeutic target in diabetic nephropathy. Kidney Int 1998;/
54:/1390�1.
[12] de Dios ST, Frontanilla KV, Nigro J, Ballinger ML, Ivey
ME, Cawson EA, et al. Regulation of the atherogenic
properties of vascular smooth muscle proteoglycans by oral
anti-hyperglycemic agents. J Diabetes Complications 2007;/
21:/108�17.
[13] Torffvit O, Agardh C-D, Cederholm B, Wieslander J. A new
enzyme linked immunosorbent assay for urine and serum
concentrations of the carboxyterminal domain (NC1) of
collagen IV. Application in type 1 (insulin-dependent)
diabetes. Scand J Clin Lab Invest 1989;/49:/431�9.
[14] Ellis D, Forrest KY, Erbey J, Orchard TJ. Urinary measure-
ment of transforming growth factor-b and type IV collagen
as new markers of renal injury: application in diabetic
nephropathy. Clin Chem 1998;/44:/950�6.
146 P. Holmquist & O. Torffvit
Scan
d J
Uro
l Nep
hrol
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
SUN
Y S
tate
Uni
vers
ity o
f N
ew Y
ork
at S
tony
Bro
ok o
n 10
/26/
14Fo
r pe
rson
al u
se o
nly.

[15] Sochett EB, Cherney DZ, Curtis JR, Dekker MG, Scholey
JW, Miller JA. Impact of renin angiotensin system modula-
tion on the hyperfiltration state in type 1 diabetes. J Am
Nephrol 2006;/17:/1703�9.
[16] Flores L, Naf S, Hernaez R, Conget I, Gomis R, Esmatjes E.
Transforming growth factor beta at clinical onset of type 1
diabetes mellitus. A pilot study. Diabet Med 2004;/21:/
818�22.
[17] De Muro P, Faedda R, Fresu P, Masala A, Cigni A, Concas
G, et al. Urinary transforming growth factor-b1 in various
types of nephropathy. Pharmacol Res 2004;/49:/293�8.
[18] Korpinen E, Teppo AM, Hukkanen L, .Akerblom HK,
Gronhagen-Riska C, Vaarala O. Urinary transforming
growth factor-b and a1-microglobulin in children and
adolescents with type 1 diabetes. Diabetes Care 2000;/23:/
664�8.
[19] Cummings EA, Cameron FJ, Sochett EB. Urinary TGF-b is
associated with kidney size but not albumin excretion rate in
children and adolescents with type 1 diabetes. Diabetes
1999;/48(Suppl 1):/140.
[20] Gilbert RE. Expression of transforming growth factor-b1 and
type IV collagen in the renal tubulointerstitium in experi-
mental diabetes. Diabetes 1998;/47:/414�22.
[21] Ziyadeh FN, Hoffman BB, Han DC, Iglesias-De La Cruz
MC, Hong SW, Isono M. Long-term prevention of renal
insufficiency, excess matrix gene expression and glomerular
mesangial matrix expansion by treatment with monoclonal
antitransforming growth factor-b antibody in db/db diabetic
mice. Proc Natl Acad Sci USA 2000;97:8015�20.
[22] Benigni A, Zoja C, Corna D, Zatelli C, Conti S, Campana
M, et al. Add-on anti-TGF-b antibody to ACE inhibitor
arrests progressive diabetic nephropathy in the rat. J Am Soc
Nephrol 2003;/14:/1816�24.
[23] Torffvit O, Wieslander J. A simplified enzyme-linked im-
munosorbent assay for urinary albumin. Scand J Clin Lab
Invest 1986;/46:/545�8.
[24] Torffvit O, Agardh C-D, Kjellsson B, Wieslander J. Tubular
secretion of Tamm-Horsfall protein in type 1 (insulin-
dependent) diabetes mellitus using a simplified enzyme
linked immunoassay. Clin Chim Acta 1992;/205:/31�41.
[25] Tencer J, Torffvit O, Thysell H, Grubb A, Rippe B.
Decreased excretion of urine glycosaminoglycans as marker
in renal amyloidosis. Nephrol Dial Transpl 1997;/12:/1161�6.
[26] Frutos TB. Normal Anatomy and Variants. In: Carty H,
Brunelle F, Stringer DA, Kan SCS, editors., editors.
Imaging children. 2nd ed. New York: Elsevier Churchill
Livingstone; 2005. p 567�71.
[27] Krutzen E, Back SE, Nilsson-Ehle P. Plasma clearance of a
new contrast agent, iohexol: a method for the assessment of
glomerular filtration rate. J Lab Clin Med 1984;/104:/955�61.
[28] Chaturvedi N, Schalkwijk CG, Abrahamian H, Fuller JH,
Stehouwer CDA, EURODIAB Prospective Complication
Study Group. Circulating and urinary transforming growth
factor b1, amadori albumin, and complications of type 1
diabetes. Diabetes Care 2002;25:2320�7.
[29] Drummond K. Young kidneys respond differently than adult
kidneys to insulin dependent diabetes mellitus. Diabetic
Nephropathy Study Group. J Am Soc Nephrol 1990;/1:/307.
[30] Feldt-Rasmussen B, Hegedus L, Mathiesen ER, Deckert T.
Kidney volume in type 1 (insulin-dependent) diabetic
patients with normal or increased urinary albumin excretion:
effect of long-term improved metabolic control. Scand J Clin
Lab Invest 1991;/51:/31�6.
[31] Baumgartl H-J, Sigl G, Banholzer P, Haslbeck M, Standl E.
On the prognosis of IDDM patients with large kidneys.
Nephrol Dial Transplant 1998;/13:/630�4.
[32] Torffvit O, Wieslander J, Forsberg L, Hederstrom E, Agardh
CD. Urinary excretion of the carboxy terminal domain of
type IV collagen is associated with kidney size and function
in IDDM. J Diabetes Complications 1990;/4:/166�9.
[33] Rasch R, Torffvit O, Bachmann S, Jensen PK, Jacobsen NO.
Tamm-Horsfall glycoprotein in streptozotocin diabetic rats:
a study of kidney in situ hybridization, immunohistochem-
istry, and urinary excretion. Diabetologia 1995;/38:/525�35.
[34] Cohen MP, Lautenslager GT, Shearman CW. Increased
collagen IV excretion in diabetes. A marker of compromised
filtration function. Diabetes Care 2001;/24:/914�8.
[35] Watanabe H, Sanada H, Shigetomi S, Katoh T, Watanabe T.
Urinary excretion of type IV collagen as a specific indicator
of the progression of diabetic nephropathy. Nephron 2000;/
86:/27�35.
[36] Chiarelli F, Verrotti A, Morgese G. Glomerular hyperfiltra-
tion increases the risk of developing albuminuria in diabetic
children. Pediatr Nephrol 1995;/9:/154�8.
[37] Levy-Marchal C, Laborde K, Kindermans C, Dechaux M,
Czernichow P. Persisting glomerular hyperfiltration in short-
term diabetic children without microalbuminuria. Acta
Paediatr Scand 1989;/78:/712�6.
[38] Rudberg S, Persson B, Dahlquist G. Increased glomerular
filtration as a predictor of diabetic nephrology, an 8 year
prospective study. Kidney Int 1992;/41:/822�8.
[39] Mogensen CE, Christensen CK, Pedersen MM, Alberti
KGMM, Boye N, Christensen T, et al. Renal and glycemic
determinants of glomerular hyperfiltration in normoalbumi-
nuric diabetics. J Diabetes Complications 1990;/4:/159�65.
TGF-b1, collagen and insulin in diabetes 147
Scan
d J
Uro
l Nep
hrol
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
SUN
Y S
tate
Uni
vers
ity o
f N
ew Y
ork
at S
tony
Bro
ok o
n 10
/26/
14Fo
r pe
rson
al u
se o
nly.