Embed Size (px)
Citation preview

1
WHY MEDICAL RECORD DOCUMENTATION
IS IMPORTANT
นพ. มนตรี แสงภัทราชัย ผู้ช่วยผู้อ านวยการใหญ่ฝ่ายการแพทย์ ประธานคณะกรรมการเวชระเบียน
ประธานคณะท างานความปลอดภัยผู้ป่วย (IPSG2)
รองประธานคณะกรรมการบริหารคุณภาพ ศูนย์การแพทย์โรงพยาบาลกรุงเทพ
BDMS Risk Management Network; 16 June 2014, Bangkok Hospital, Thailand
Outline
Who is JCI ?
Medical Documentation related JCI Standards

2
Who is
Founded in 1994 by The Joint Commission
The oldest and largest standards-setting and accrediting body, nonprofit organization, in health care in the United States, it evaluates more than 20,000 organizations and inspires them to excel in providing safe and effective care.
Joint Commission International (JCI)
The mission of Joint Commission International is to improve the safety and quality of care in the international community through the provision of education, publications, consultation, and evaluation services.

3
JCI-Accredited Organizations (440+ Hospitals worldwide)
Thailand: 32 Accredited Hospitals (Update June 2014)
12 from BDMS Hospitals
Section: Patient-Centered Standards
International Patient Safety Goals (IPSG)
Access to Care and Continuity of Care (ACC)
Patient and Family Rights (PFR)
Assessment of Patients (AOP)
Care of Patients (COP)
Anesthesia and Surgical Care (ASC)
Medication Management and Use (MMU)
Patient and Family Education (PFE)
Section: Health Care Organization Management Standards
Quality Improvement and Patient Safety (QPS)
Prevention and Control of Infections (PCI)
Governance, Leadership, and Direction (GLD)
Facility Management and Safety (FMS)
Staff Qualifications and Education (SQE)
Management of Information (MOI)

4
Patient and Family Rights (PFR)
General Consent (PFR 5)
Standard PFR. 5
General consent for treatment, if obtained when a patient is admitted as an inpatient or is registered for the first time as an outpatient, is clear in its scope and limits.

5
Informed Consent (PFR 5.1 – 5.4)
Standard PFR. 5.1
Patient informed consent is obtained through a process defined by the hospital and carried out by trained staff in a manner and language the patient can understand.
Standard PFR. 5.2
Informed consent is obtained before surgery, anesthesia, procedural sedation, use of
blood and blood products, and other high-risk treatments and procedures.
Standard PFR. 5.3
Patients and families receive adequate information about the illness, proposed
treatment(s), and health care practitioners so that they can make care decisions.
Standard PFR. 5.4
The hospital establishes a process, within the context of existing law and culture, for
when others can grant consent.
General Consent Form

6
Generic Consent Form

7
Medication Management and Use
(MMU)
Organization and Management (MMU 1)
Selection and Procurement (MMU 2)
Ordering and Transcribing (MMU 4)
Storage (MMU 3)
Preparing and Dispensing (MMU 5)
Administration (MMU 6)
Monitoring (MMU 7)

8
Safety Prescribing Policy
UNSAFE PRESCRIBING

9
Safety Prescribing
HIGH ALERT DRUGs
UNSAFE PRESCRIBING

10
Safety Prescribing

11
Preprint Order

12
UNSAFE PRESCRIBING
Safety Prescribing

13
Management of Information
(MOI)
14
Management of Information (MOI)
These standards have been focused to address how well the hospital obtains, manages, and uses information to provide, coordinate, and integrate services.
The principles of good information management apply to all methods, whether paper-based or electronic, and JCI standards are equally compatible with either method.
Information Management (MOI 1 – 8)
Management and Implement of Documents (MOI 9)
Patient Clinical Record (MOI 10 - 12)

15
Standard MOI.10
The hospital initiates and maintains a standardized clinical record for every patient assessed or treated and determines the
record’s content, format, and location of entries.
Patient Clinical Record (MOI 10 - 12)
P
Measurable Elements of MOI.10.1
1. Patient clinical records contain adequate information to identify the patient.
2. Patient clinical records contain adequate information to support the diagnosis.
3. Patient clinical records contain adequate information to justify the care and treatment.
4. Patient clinical records contain adequate information to document the course and results of treatment.
Standard MOI.10.1
The clinical record contains sufficient information to identify the patient, to support the diagnosis, to justify the treatment, and
to document the course and results of treatment.

16
GOOD Medical Record
Documentation
POOR Medical Record
Documentation
Standard MOI.10.1.1
The clinical records of patients receiving emergency care include the time of arrival and departure, the conclusions at
termination of treatment, the patient’s condition at discharge, and follow-up care instructions.
Measurable Elements of MOI.10.1.1
1. The clinical records of all emergency patients include arrival and departure times.
2. The clinical records of discharged emergency patients include conclusions at the termination of treatment.
3. The clinical records of discharged emergency patients include the patient’s condition at discharge.
4. The clinical records of discharged emergency patients include any follow-up care instructions.

17
Standard MOI.11
The hospital identifies those authorized to make entries in the patient clinical record.
P
Measurable Elements of MOI.11
1. Those authorized to make entries in the patient clinical record are identified in hospital policy.
2. There is a process to ensure that only authorized individuals make entries in patient clinical records.
3. There is a process that addresses how entries in the patient record are corrected or overwritten.
4. Those authorized to have access to the patient clinical record are identified in hospital policy.
5. There is a process to ensure that only authorized individuals have access to the patient clinical record.

18
19
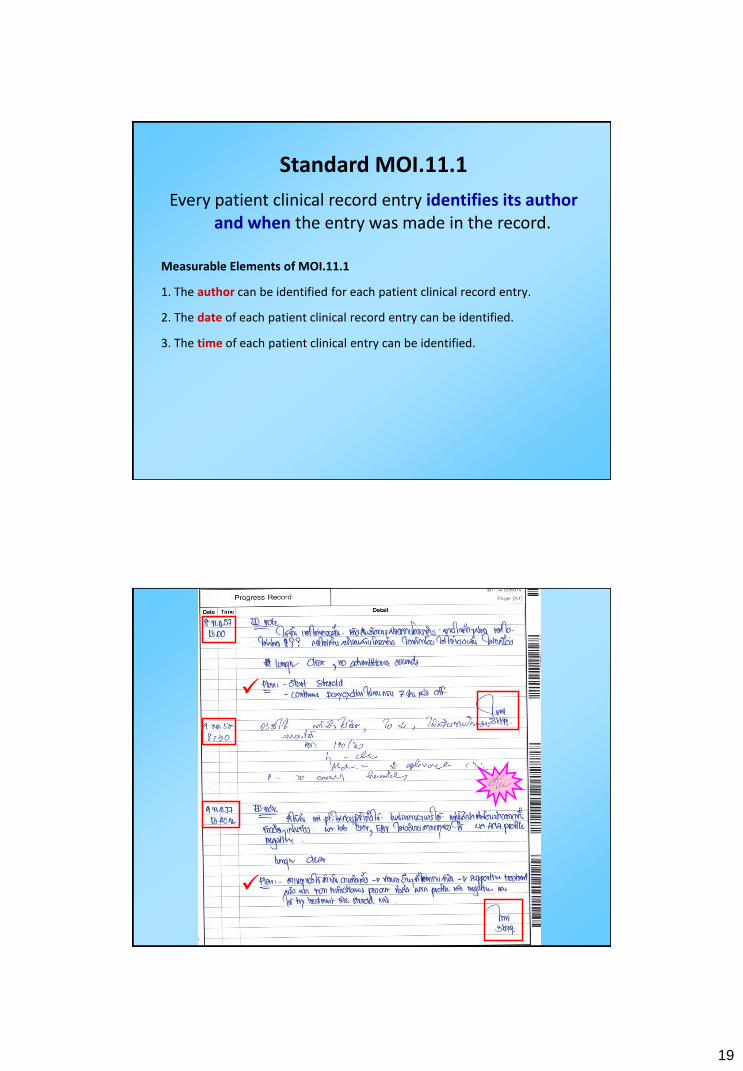
Measurable Elements of MOI.11.1
1. The author can be identified for each patient clinical record entry.
2. The date of each patient clinical record entry can be identified.
3. The time of each patient clinical entry can be identified.
Standard MOI.11.1
Every patient clinical record entry identifies its author and when the entry was made in the record.

20
Standard MOI.12
As part of its monitoring and performance improvement activities, the hospital regularly assesses patient clinical record
content and the completeness of patient clinical records.
Measurable Elements of MOI.12
1. A representative sample of active and discharged patient clinical records is reviewed at least quarterly or more frequently as determined by laws and regulations.
2. The review is conducted by physicians, nurses, and others authorized to make entries in patient records or to manage patient records.
3. The review focuses on the timeliness, legibility, and completeness of the clinical record.
4. Record contents required by laws or regulations are included in the review process.
5. The results of the review process are incorporated into the hospital’s quality oversight mechanism.
(Cause of Death: Sloppy Doctors. Time. 2007.)
21
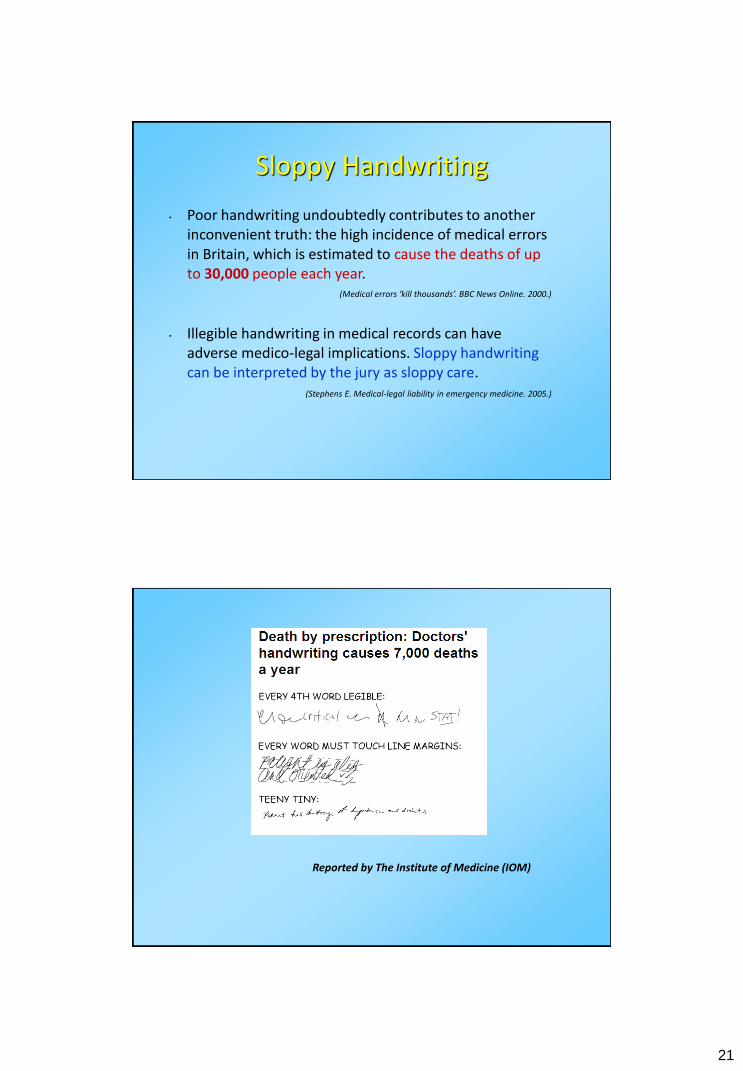
Sloppy Handwriting
• Poor handwriting undoubtedly contributes to another inconvenient truth: the high incidence of medical errors in Britain, which is estimated to cause the deaths of up to 30,000 people each year.
(Medical errors ‘kill thousands’. BBC News Online. 2000.)
• Illegible handwriting in medical records can have adverse medico-legal implications. Sloppy handwriting can be interpreted by the jury as sloppy care.
(Stephens E. Medical-legal liability in emergency medicine. 2005.)
Reported by The Institute of Medicine (IOM)

22
Illegible Handwriting
Legible Handwriting

23
WHY MEDICAL RECORD DOCUMENTATION
IS IMPORTANT
นพ. มนตรี แสงภัทราชัย ผู้ช่วยผู้อ านวยการใหญ่ฝ่ายการแพทย์ ประธานคณะกรรมการเวชระเบียน
ประธานคณะท างานความปลอดภัยผู้ป่วย (IPSG2)
รองประธานคณะกรรมการบริหารคุณภาพ ศูนย์การแพทย์โรงพยาบาลกรุงเทพ
BDMS Risk Management Network; 16 June 2014, Bangkok Hospital, Thailand
Have a Nice Day





























