Embed Size (px)
Citation preview

8/18/2019 Wilkins Ch 12
http://slidepdf.com/reader/full/wilkins-ch-12 1/31
Chapter 12
The Ging iva
The t rue test of successful t reatment , the real evaluat ion of the ef fects of scal ing and related
inst rumentat ion, is the health of the per iodontal t issues. The obj ect ive of a l l t reatment is to br ing
the diseased per iodontal t issues to a state of heal th that can be maintained by the pat ient . To do
this , the f i rs t object ive is to learn to re cognize normal healthy t issue; to observe cer tain
character is t ics of color , texture, and form; to test for b leeding; and to apply th is knowledge to the
t reatment and superv is ion of the pat ient 's g ingiva unt i l heal th is at ta ined.
An outl ine of the c l in ical fea tu res of the per iodontal t i ss ues in heal th and d isease is incl uded in th is
chapter . Key words are def ined in Box 12-1.
Box 12-1 Key Words
Key Words : G ing iv a and Per iodon t i um
A t t ac h men t ap p ar at u s : the cementum, periodontal l igament, and the alveolar bone.
Cl in ica l a t tachmen t leve l : the probing depth measured from a f ixed point , such as the
cementoenamel junct ion.
Desmosome: cel l junct ion; consists of a dense plate near the cel l surface that relates to a
similar structure on an adjacent cel l , between which are thin layers of extracel lular
material .
Dias tema : a space between two natural adjacent teeth. Plural, diastemata. See also
Primate space, page 287.
E p i t h e l i u m
Ora l : the t issue serving as a l iner for the intraoral mucosal surfaces.
Squamous : composed of a layer of f lat , scalel ike cel ls; or may be strat i f ied.
F ib ro b la s t : f iber-producing cel l of the connect ive t issue; a f lat tened, irregularly branched
cel l with a large oval nucleus that is responsible in part for the product ion and remodeling
of the extracel lular matr ix.
F ib ro s i s : a f ibrous change of the mucous membrane, especial ly the gingiva, as a result of
chronic inf lammation; f ibrot ic gingiva may appear outwardly healthy, thus masking
underly ing disease.
Hemidesmosome: half of a desmosome that forms a si te of at tachment between junct ional
epithel ial cel ls and the tooth surface.
H y p e rk e ra t o s i s : abnormal thickening of the kerat in layer (stratum corneum) of the
epithel ium.
Hyperp las ia : abnormal increase in volume of a t issue or organ caused by format ion and
growth of new normal cel ls.
H y p e r t r o p h y : increase in size of t issue or organ caused by an increase in size of i ts
const i tuent cel ls.
K e ra t i n i z a t i o n : development of a horny layer of f lat tened epithel ial cel ls containing
kerat in.
Marke r : ident i f ier; symptoms or s igns by which a part icular condit ion can be recognized;
for example, c l inical and microbiologic markers are used to ident i fy gingival and
P.213
Page 1 of 31
11/2/2010http://pt.wkhealth.com/pt/re/9780781763226/bookContentPane_frame.htm;jsessionid=MQ...

8/18/2019 Wilkins Ch 12
http://slidepdf.com/reader/full/wilkins-ch-12 2/31
periodontal infect ions.
Ma s t i c a t i o n : act of chewing.
Nonke ra t in ized mucosa : l ining mucosa in which the strat i f ied squamous epithel ial cel ls
retain their nuclei and cytoplasm.
P e r i o d o n t i u m : t issues surrounding and support ing the teeth; in two sect ions are the
gingival unit , composed of the free and at tached gingiva and the alveolar mucosa, and the
attachment apparatus, which includes the cementum, periodontal l igament, and alveolar
process.
P ro b in g d e p t h : the distance from the gingival margin to the locat ion of the periodontal
probe t ip inserted for gent le probing at the at tachment.
Pus : a f luid product of inf lammation that contains leukocytes, degenerated t issue
elements, t issue f luids, and microorganisms.
S h arp e y ' s f i b e r s : penetrat ing connect ive t issue f ibers by which the tooth is at tached to
the adjacent alveolar bone; the f iber bundles penetrate cementum on one side and alveolar
bone on the other .
S t i p p l i n g : the pit ted, orange-peel appearance frequent ly seen on the surface of the
attached gingiva.
S u p p u ra t i o n : format ion of pus.
Tas te bud : receptor of taste on tongue and oropharynx; goblet-shaped cel ls oriented at
r ight angles to the surface of the epithel ium.
Object ives
The ul t imate object ive is to apply knowledge and sk i l l in examinat ion and assessment of the
per iodontal t issues to pat ient care so that each pat ient at ta ins and maintains opt imum oral heal th.
The dental hygienist must know when the t reatment provided by dental hygiene serv ices is def in i t ive
in restor ing health and when addit ional t reatment is needed. The pat ient can be proper ly informed so
that complete t reatment can be provided.
Speci f ic object ives are to be able to
Recognize normal per iodontal t issues.
Know the c l in ical features of the per iodontal t issues that must be examined for a compl ete
assessment .
Recognize the markers that are the basic s i gns of per iodontal infect ions and c lassi fy them by
type and degree of sever i ty .
Ident i fy the dental hygiene t reatment and in st ruct ion needed.
Out l ine the pat ient 's prevent ive program.
The Treatm ent Ar ea
The t reatment procedures are appl ied direct ly to the teeth, the gingiva, and the gingival sulcus.
Detai led knowledge and understanding of the anatomy and normal c l in ical appearance of the hard
and sof t oral t issues are prerequis i te to meaningful examinat ion and t reatment .
I. The Teeth
P.214
Page 2 of 31
11/2/2010http://pt.wkhealth.com/pt/re/9780781763226/bookContentPane_frame.htm;jsessionid=MQ...

8/18/2019 Wilkins Ch 12
http://slidepdf.com/reader/full/wilkins-ch-12 3/31
A . Cl in i cal Crown
The part of the tooth above the at tached per i odontal t issues. I t can be considered the part of the
tooth where c l in ical t reatment procedures are appl ied (Figure 12-1 ) .
B. C l in ica l Root
The part of the tooth below the ba se of the gingival sulcus or per iodontal pocket . I t is the part of the
root to which per iodontal f ibers are at tached.
C. Anatomic Crown
The part of the tooth covered by ename l.
D. Anatom ic Root
The part of the tooth covered by cementum.
I I . Oral Mucos a
The l in ing of the oral cavi ty , the oral mucosa, is a mucous membrane composed of connect ive t issue
covered with st rat i f ied squamous epi thel ium. Ther e are three div is ions or categor ies of oral mucosa.
A . Mas t i cato r y Mucosa
1 . C ov er s t he gingiva and the hard palate , the areas used most dur ing the mast icat ion of food.
2 . Except fo r the f ree marg in o f the g ing iva , the mas t ica tory mucosa is f i rm ly a ttached to
under ly ing t issues.
3 . The ep i the l ial cover ing is genera l ly kera t in ized.
FIGURE 12-1 Clinical Crown. The part of the tooth that is above the attachedperiodontal tissue. Left, When the periodontal pocket depth is increased, the clinicalcrown extends to a position at which the clinical crown length is greater than the clinicalroot length. The clinical root is that part of the tooth with attached periodontal tissues.Right, When the clinical attachment level is at the cementoenamel junction, the clinicalcrown and the anatomic crown are the same.
Page 3 of 31
11/2/2010http://pt.wkhealth.com/pt/re/9780781763226/bookContentPane_frame.htm;jsessionid=MQ...

8/18/2019 Wilkins Ch 12
http://slidepdf.com/reader/full/wilkins-ch-12 4/31
B. L in ing Mucosa
1 . C ov er s t he inner surfaces of the l ips and cheeks, the f loor of the mouth, the under s ide of the
tongue, the sof t palate, and the alveolar mucosa .
2 . These tissues are not f i rm ly a t tached to under ly ing t issue.
3 . The epi the l ia l covering is no t genera l ly kerat in ized.
C. Spec ia l ized Mucosa
1 . C ov er s t he dorsum (upper sur face) of the tongue . I t is composed of many papi l lae; some
contain taste buds.
2 . The d is tr ibu t ion o f the four t ypes o f pap i l lae is shown in F igure 12-2 .
a. Fi l i form. Threadl ike kerat in ized elevat ions that cover the dorsal sur face of the tongue;
they are the most numerous of the papi l lae.
b. Fungiform. Mushroom-shaped papi l lae interspersed among the f i l i form papi l lae on thet ip and s ides of the tongue. On c l in ical examinat ion they appear redder than the f i l i form
papi l lae and contain
var iable numbers of taste buds. The inset en largement in Figure 12-2 shows the
comparat ive shape and s ize of the f i l i form and fungiform papi l lae.
c. Circumval late (val late) . The 10 to 14 large round papi l lae arranged in a “V” between the
body of the tongue and the base. Taste b uds l ine the wal ls .
P.215
FIGURE 12-2 Papillae of the Tongue. Dorsal surface of a human tongueshows the four types of papillae. Inset enlargement shows the shape offiliform and fungiform papillae.
Page 4 of 31
11/2/2010http://pt.wkhealth.com/pt/re/9780781763226/bookContentPane_frame.htm;jsessionid=MQ...

8/18/2019 Wilkins Ch 12
http://slidepdf.com/reader/full/wilkins-ch-12 5/31
d. Fol iate. Vert ical grooves on the lateral poster ior s ides of the tongue; also contain taste
buds.
I II . The Per iodon t ium
The per iodont ium is the funct ional uni t of t issues that surrounds and supports the tooth. The four
parts are the gingiva, per iodontal l igament , cementum , and bone ; the last three make up the
at tachment apparatus.
A . Per i odon tal L i gamen t
The per iodontal l igament i s the f ibrous connect ive t issue that surrounds and at taches the
roots of teeth to the alveolar bone.
The l igament is located in the per iodontal space between the cementum and the alveolar
bone.
I t is composed of connect ive t issue cel ls a nd int racel lu lar substance.
The f ibers that are inserted into the cem entum on one s ide and the alveolar bone on the other
are cal led Sharpey's f ibers.
B. Per iodont a l L igament F iber Groups
The two general groups of f ibers are the gingival groups (around the cerv ical area with in the
gingival t issues) and the pr incipal f iber groups (surrounding the root ) .1
1. Gingival Fiber Groups (Figure 12-3 )
D en t o g i n g i v a l f i b e r s ( f ree gingival) . From the cementum in the cerv ical region into the
f ree gingiva to give support to the gingi val .
A l v eo l o g i n g i v al f i b er s (at tached gingival) . From the alveol ar crest into the f ree and
at tached gingiva to provide support .
Ci r cum f e ren t i a l f i be r s (c i rcular) . Cont inuous around the neck of the tooth to help to
maintain the tooth in posi t ion.
Den t ope r ios t ea l f i be r s (a lveolar crest ) . From the cerv ical cementum over the alveolar
crest to blend with f ibers of the per iosteum of the bone.
Transsep t a l f i be r s . From the cerv ical area of o ne tooth across to an adjacent tooth (on
the mesial or d is tal only) to provide res is tance to separat ion of teeth (Figure 12-4 ) .
2. Principal Fiber Groups (Figure 12-4)
The f ive pr inc ipal groups of col lagen f ibers are named for their locat ion on the root and for their
direct ion. They are also cal led the dentoalveolar f iber groups.
Page 5 of 31
11/2/2010http://pt.wkhealth.com/pt/re/9780781763226/bookContentPane_frame.htm;jsessionid=MQ...

8/18/2019 Wilkins Ch 12
http://slidepdf.com/reader/full/wilkins-ch-12 6/31
A p i c al f i b er s . From the root apex to adjacent surrounding bone to res is t ver t ical forces.
O b l i q u e f i b e r s . From the root above the apical f ibers obl iquely toward the occlusal to res is t
ver t ical and unexpected st rong forces.
Hor i zon t a l f i be r s . From the cementum in the mi ddle of each root to adjacent alveolar bone to
resis t t ipping of the tooth.
A l v eo l ar c r es t f i b er s . From the alveolar crest to the cementum just below the cementoenamel
junct ion to res is t int rus ive forces.
FIGURE 12-3 Gingival Fiber Groups. Cross section of the gingiva shows the relation ofthe gingival fiber groups to the gingival sulcus, the free gingiva, the cementum, and thealveolar bone.
Page 6 of 31
11/2/2010http://pt.wkhealth.com/pt/re/9780781763226/bookContentPane_frame.htm;jsessionid=MQ...

8/18/2019 Wilkins Ch 12
http://slidepdf.com/reader/full/wilkins-ch-12 7/31
I n t e r rad i cu la r f i be r s . From cementum between the roots of mult i rooted teeth to the adjacent
bone to res is t ver t ical and lateral forces.
C. Cementum
The cementum is a th in la yer of calc i f ied connect ive t issue that covers the tooth f rom the
cementoenamel junct ion to, and around, the apical foramen.
1. Funct ions
To seal the tubules of the root dent in.
To provide at tachment for the per iodontal f iber groups.
2. Character is t ics
Thickness is 50 to 200 µm ab out the apex; 30 to 60 µm about the cerv ical area.
Vascular and nerve connect ions are miss ing; therefore, cementum is insensi t ive.
Relat ionship of enamel and cementum at the cerv ical area is shown in Figure 14-2 (page 257).
D. Alveol ar Bone
The alveolar bone consists of the la mina dura, which surrounds the tooth socket , and the
support ing bone.
When teeth are lost , the alveolar bone is resorbed.
The bone funct ions to support the teeth and provide at tachment for the per iodontal l igam ent
f ibers.
E. Gingi va
The part of the mast icatory mucosa that surround s the necks of the teeth and is at tached to the
teeth and the alveolar bone.
The Gingi va and Related Struc tures
The gingiva is made up of the f ree gingiva , the at tached gingiva , and the interdental gingiva or
interdental papi l la.
I . Free Gingi va (Margin al Gingi va)
In health, the f ree gingiva is c losely adapted around each tooth. I t connects with the at tached
gingiva at the f ree gingival groove and at taches to the tooth at the coronal por t ion of the junct ional
FIGURE 12-4 Principal Fiber Groups of the Periodontium. The five principalgroups (apical, oblique, horizontal, alveolar crest, and interradicular) are shown.The transseptal fibers of the gingival fiber groups are also shown as they spanacross from the cervical area of one tooth to the neighboring tooth.
P.216
Page 7 of 31
11/2/2010http://pt.wkhealth.com/pt/re/9780781763226/bookContentPane_frame.htm;jsessionid=MQ...

8/18/2019 Wilkins Ch 12
http://slidepdf.com/reader/full/wilkins-ch-12 8/31
epithel ium (Figure 12-5 ) .
A . Fr ee Ging ival Groove
The f ree gingival groove is a shal low l inear groove that demarcates the f ree f rom the at tached
gingiva. General ly , about one-third of the teeth show a v is ib le gingival groove when the
gingiva is healthy.2
In the absence of inf lammat ion and pocket format ion, the gingival groove runs somewhat
paral le l wi th and about 0.5 to 1.5 mm f rom the gingival margin,3 and i t is approximately at the
level of the bot tom of the gingi val sulcus.
B. Oral Ep i the l ium (outer g ing iva l ep i the l ium, Figure 12-6)
Covers the f ree gingiva f rom the gingival groove over the gingival margin.
Composed of kerat in ized st rat i f ied squamous epi thel ium.
FIGURE 12-5 Parts of the Gingiva. Cross-sectional diagram shows the parts of thegingiva and adjacent tissues of a partially erupted tooth. Note that the junctionalepithelium is on the enamel.
Page 8 of 31
11/2/2010http://pt.wkhealth.com/pt/re/9780781763226/bookContentPane_frame.htm;jsessionid=MQ...

8/18/2019 Wilkins Ch 12
http://slidepdf.com/reader/full/wilkins-ch-12 9/31
C. Gingiv al Margi n (g ingi val c res t , margin of th e g ingiv a, or f reemargin, Figure 12-5)
This is the edge of the gingi va nearest the inc isal or occlusal sur face.
Marks the opening of the gingival sulcus.
I I. Gingiv al Sulcu s (Crevice)
A . Locat ion
The crevice or groove between the f ree gi ngiva and the tooth.
B. Bound ar ies (Figure 12-6)
1. Inner. Tooth sur face. May be the enamel, cem entum, or par t of each, depending on the
posi t ion of the junct ional epi thel ium.
2. Outer. Sulcular epi thel ium.
3. Base. Coronal margin of the at tached t issues. The base of the sulcus or pocket is a lso cal led
FIGURE 12-6 The Gingival Tissues. Cross-sectional diagram shows the histologicrelationships of the oral, sulcular, and junctional epithelia and the connectivetissue.
P.217
Page 9 of 31
11/2/2010http://pt.wkhealth.com/pt/re/9780781763226/bookContentPane_frame.htm;jsessionid=MQ...

8/18/2019 Wilkins Ch 12
http://slidepdf.com/reader/full/wilkins-ch-12 10/31
the “probing depth, ” the “depth of the sulcus, ” or the “bot tom of the pocket . ”
C. Sulcular Epi thel ium
The cont inuat ion of the oral epi thel ium cover ing the f ree gingiva. Sulcular epi thel ium is not
kerat in ized.
D. Depth of Sulcu s
Healthy sulc i are shal low and may be only 0.5 mm.
The average depth of the healthy sul cus is about 1.8 mm.4
E. Ging iva l Su lcus F lu id (su lcu la r f lu i d , c rev icu la r f lu id )
A serum-l ike fl u id that seeps f ro m the connect ive t issu e through the epi th e l ia l l in ing of the
sulcus or pocket .
Occurrence is s l ight to none in a n ormal sulcus; increases with inf lammat ion. I t i s par t of the
local defense mechanism and is abl e to t ransport many substances, inc luding endotoxins,enzymes, ant ibodies, and certain systemical ly administered drugs.
I II . Junc t ion al Epi th el ium (At tachment Epi thel iu m)
A . Desc r ip t i on
The junct ional epi thel ium is a cuf f - l ike band of s t rat i f ied squamous epi thel ium that is
FIGURE 12-7 Tooth Eruption and the Gingiva. (A) Before eruption, the oralepithelium covers the tooth. (B) As the tooth emerges, the reduced epithelium joins the oral epithelium as the gingival sulcus is formed. (C) Partial eruption withthe junctional epithelium along the enamel. (D) Eruption complete, with junctionalepithelium at the cementoenamel junction. (E) From disease or other cause, theattachment migrates along the root surface, exposing the cementum.
Page 10 of 31
11/2/2010http://pt.wkhealth.com/pt/re/9780781763226/bookContentPane_frame.htm;jsessionid=MQ...

8/18/2019 Wilkins Ch 12
http://slidepdf.com/reader/full/wilkins-ch-12 11/31
cont inuous with the sulcular epi thel ium and completely encirc les the tooth.
I t is t r iangular in cross sect ion, is widest at the junct ion with the sulcular epi thel ium, and
narrows down to the width of a few cel l s at the apical end.
The junct ional epi thel ium is not kerat in ized. I t has two basement membranes: one adjacent to
the connect ive t issue and one adjacent to the tooth sur face.
B. Size
The junct ional epi thel ium may be up to 15 or 20 cel ls in th ickness where i t jo ins the sulcular
epi thel ium and tapers down to 1 or 2 cel ls in th ickness at the apical end.
The length ranges f rom 0.25 to 1.35 m m.
C. Pos i t ion
As the to oth erupts, the att achment is on the enamel; dur ing erupt ion , the ep i thel ium migrates
toward the cementoenamel junct ion (Figure 12-7 ) .
At fu l l erupt ion, the at tach ment is usual ly on the ce mentum, where i t becom es f i rm ly at tach ed
(Figure 12-7D).
With wear of the tooth on the inc isal or occlusal sur face and with per iodontal in fect ions, the
at tachment migrates along the root sur face (Figure 12-7E).
D. Relat io n of Crest of Alv eolar Bone to the At t ached Gingi val T issue
The dis tance between the base of the at tachment a nd the crest of the alveolar bone is
approximately 1.0 to 1.5 mm.
This dis tance is maintained in disease when the epi thel ium moves along the root sur face and
bone loss occurs.
E. At tachment o f the Ep i the l ium t o th e Tooth Sur face
The junct ional epi thel ium or at tachment epi thel ium provides a seal at the base of the sulcus.
The at tachment , or connect ing inter face between the tooth and the t issue, is accompl ished by
hemidesmosomes and the basal lamina of the junct ional epi thel ium.
IV. Interdental Gingiva (Interdental Papi l la)
A . Locat ion
In health, the interdental g ingiva occupies the interproximal area between two adjacent teeth.
The t ip and lateral borders are cont inuous with the f ree gingiva, whereas other pa rts are
P.218
Page 11 of 31
11/2/2010http://pt.wkhealth.com/pt/re/9780781763226/bookContentPane_frame.htm;jsessionid=MQ...

8/18/2019 Wilkins Ch 12
http://slidepdf.com/reader/full/wilkins-ch-12 12/31
at tached gingiva.
An interproximal area is also cal led an embrasure. In Type 1 embrasure the gingi val t issue
f i l ls the area; in Type 2 embrasure there is s l ight to moderate recession of the interdental
gingiva; in Type 3 embrasure there is extensive recession or complete loss of the o f the
papi l la as shown in Figure 26-1 (page 431).
B. Shape
1. Varies With Spacing or Over lapping of the Teeth. The interdental g ingiva may be f lat or
saddle-shaped when wide spaces are between the teeth, or i t may be tapered and narrow
when the teeth are crowded or over lapped.
2. Between Anter ior Teeth . Pointed, pyramidal .
3. Between Poster ior Teeth
Flat ter than anter ior papi l lae because o f wider teeth, wider contact areas, and f lat tened
interdental bone.
Two papi l lae, one fac ial and one l ingual, connected by a col , are found when teeth are
in contact .
C. Col
1. A co l is the depress ion between the l ingua l o r pa la ta l and facia l pap i l lae tha t conforms to the
proximal contact area (Figure 12-8 ) .
2 . The center o f the co l a rea is no t usua l ly kera t in ized and thus is more suscept ib le to in fec t ion .
Most per iodontal infect ion begins in the col area.
FIGURE 12-8 Col. A col is the depression between the lingual or palatal and the facialpapillae under the contact area. The contact area is represented by the striped lines. (A)Mesial of mandibular molar to show wide col area. (B) Mesial of mandibular incisor toshow a narrow col. The col deepens when gingival enlargement occurs.
Page 12 of 31
11/2/2010http://pt.wkhealth.com/pt/re/9780781763226/bookContentPane_frame.htm;jsessionid=MQ...

8/18/2019 Wilkins Ch 12
http://slidepdf.com/reader/full/wilkins-ch-12 13/31
V. At tached Gingiva
A . Ex ten t
The at tached gingiva is cont inuous with the oral epi thel ium of the f ree gingiva and is covered
with kerat in ized st rat i f ied squamous epi thel ium.
Maxi l lary palatal g ingiva is cont inuous with the palatal mucosa.
The at tached gingiva of the mandibular fac ial and l ingual g ingiva and maxi l lary fac ial g ingiva
is demarcated f rom the alveolar mucosa by the mucogingival junct ion.
B. At tachment
Firmly bound to the under ly ing cementum and alveolar bone.
C. Shape
Fol lows the depressions between the emine nces of the roots of the teeth.
VI. Mucoging iva l J unct ion
A . A ppearance
The mucogingival junct ion appears as a l ine that marks the connect ion between the at tached
gingiva and the alveolar mucosa.
The anter ior l ine is scal loped, but i t is fa ir ly s t raight poster ior to the premolars.
A contrast can be seen between th e pink of the kerat in ized, st ipp led, at tached gingiva and th e
darker alveolar mucosa.
B. Locat ion
A muco gingival l ine is fo und on the faci al sur fa ce of a l l quadrants and on the l ingual su rf ace
of the mandibular arch.
There is no alveolar mucosa on the palate. The palatal t issue is f i rmly at tached to the bone of
the roof of the mouth.
The three mucogingival l ines are fac ial mandibular , l ingual mandibu lar , and fac ial maxi l lary.
In Figure 12-9, the fac ial maxi l lary and mandibular mucogingival junct ions are shown in
relat ion to the at tached gingiva and the alveolar mucosa.
VII. Alveolar Mucosa
A . Desc r ip t i on
Movable t issue loosely at tached to the under ly ing bone.
I t has a smooth, shiny sur face with nonkerat in ized, th in epi thel ium. Under ly ing vessels may be
P.219
Page 13 of 31
11/2/2010http://pt.wkhealth.com/pt/re/9780781763226/bookContentPane_frame.htm;jsessionid=MQ...

8/18/2019 Wilkins Ch 12
http://slidepdf.com/reader/full/wilkins-ch-12 14/31
seen through the epi thel ium.
B. Frena (s ingu lar : f renum o r f renu lum)
Descr ipt ion. A f renum is a narrow fold o f mucous membrane that passes f rom a m ore f ixed to
a movable part , for example, f rom the at tached gingiva at the mucogingival j unct ion to the l ip,
cheek, or undersurface of the tongue. A f renum serves to check undue movement .
Locat ions
a . Max i l lary and mandibu lar an ter io r f rena. A t m id l ines between cent ral inc isors . F igure
12-9 shows diagrammat ical ly the locat ion of the anter ior f rena.
b . L ingual f renum. From undersurface o f the tongue.
c . Buccal f rena. In the can ine–premolar areas , both max i l la ry and mandibular .
At tachme nt of Frena in Rela ti on to the At tach ed Gingiva
a . C lose ly assoc ia ted w i th the mucog ing iva l junc t ion .
b . When the a ttached g ing iva is narrow or m iss ing, the f rena may pu l l on the f ree g ing ivaand displace i t lateral ly . A “ tension test ” is used to locate f renal at tachments and check
the adequacy of the at tached gingiva (page 239).
The Recogn i t i on of Gingiv al and Per iod ontal Infect ion s
I . The Cl in ical Examinat io n
The recognit ion of normal gingiva, g ingival infect ions, and deeper per iodontal involvement depends
on a disc ipl ined, s tep-by-step examinat ion.
I t is necessary to know the extent of the disease. Gingival infect ions are conf ined to the gingiva,
whereas per iodontal infect ions inc lude al l par ts of the per iodont ium, namely, the gingiva,
per iodontal l igament , bone, and cementum.
FIGURE 12-9 Parts of the Gingiva. The mucogingival junction for each archis shown in relation to the attached gingiva, alveolar mucosa, and labialanterior frena.
Page 14 of 31
11/2/2010http://pt.wkhealth.com/pt/re/9780781763226/bookContentPane_frame.htm;jsessionid=MQ...

8/18/2019 Wilkins Ch 12
http://slidepdf.com/reader/full/wilkins-ch-12 15/31
A basi c examinat ion per fo rmed to reco gni ze the s igns and ef fe cts of inf lammat ion inc ludes
informat ion about at least the fo l lowing markers:
Gingival t issue changes (color , s ize, shape, sur face texture, posi t ion) .
Bleeding and exudates.
Mucogingival involvement (adequate width of at tached gingiva) .
Probing depths; pocket format ion (at tachment levels) .
Furcat ion involvement .
Dental b iof i lm (and calculus) present .
Mobi l i ty of teeth.
Radiographic ev idence.
I I. Signs and Symptom s
Pat ients may or may not have speci f ic symptoms to repo rt because per iodontal infect ions are
ins idious in development .
Symptoms the pat ient not ices or feels may inc lude bleeding gingiva, somet imes only whi le
brushing, somet imes with drool ing at n ight , or somet imes spontaneously.
Other possible symptoms are sensi t iv i ty to h ot and cold, tenderness or discomfort whi le eat ing
or pain af ter eat ing, food retained between the teeth, unpleasant mouth odors, chronic bad
taste, or a feel ing that the teeth are l oose. Most of these are symptoms of advanced di sease.
I II . Cl in i cal ly Normal
The terms “c l in ical ly normal” or “c l in ical ly healthy” may be used to designate gingival t issue that is
character ized by the fo l lowing:
A shade of pale or coral p ink va ri ed by complexion and pigmentat ion .
A kni fe -e dged gingival margin th at adapts c losely around the to oth.
St ippl ing; f i rmness; and minimal sulcus depth with no bleeding when probed.
Al though “norm al” va r ies wi th ana to mic, phy siologic, and other facto rs, general character is ti cs form
a basel ine for a contrast in the recognit ion of inf lammat ion.
IV. Causes of Tis sue Changes
Disease changes produce al terat ions in color , s ize, posi t ion, shape, consistency, sur face
texture, b leeding readiness, and exudate product ion.
To understand the changes that take place i n the gingival t issues dur ing the t ransi t ion f rom
health to disease, i t is necessary to have a c lear pic ture of what dental b iof i lm is , the role of
biof i lm microorganisms in the development of d isease, and the inf lammatory response by the
body.
P.220
Page 15 of 31
11/2/2010http://pt.wkhealth.com/pt/re/9780781763226/bookContentPane_frame.htm;jsessionid=MQ...

8/18/2019 Wilkins Ch 12
http://slidepdf.com/reader/full/wilkins-ch-12 16/31
When the products of the biof i lm microorganisms cause breakdown of the intercel lu lar
substances of the sulcular epi thel ium, in jur ious agents can pass into the connect ive t issue,
where an inf lammatory response is in i t iated.
An inf lammatory response means that there is increase d blood f low, incr eased perm eabi l i ty of
capi l lar ies, and increased col lect ion of defense cel ls and t issue f lu id.
The changes produce the t issue al terat ions, such a s in color , s ize, shape, and consistency,
that are descr ibed in the next sect ion.
V. Descr i pt iv e Termi nolo gy
The degree of sever i ty and dis t r ibut ion of a change should be noted when examining the gingiva.
When a deviat ion f rom normal af fects a s ingle area, i t can be designated by the number of the
adjacent tooth and the sur face of the t issue i nvolved, namely, fac ial , l ingual, mesial , or d is tal .
A . Sever i t y
Sever i ty is expressed as s l ight , moderate, or severe.
B. Dis t r ibu t ionTerms used for descr ib ing dis t r ibut ion are as fo l lows:
1. Local ized : The gingiva is involved only about a s ingle tooth or a speci f ic group of teeth.
2. General ized : The gingiva is involved a bout al l or near ly al l of the teeth throughout the mouth.
A condi t ion may also be general ized throughout a s ingle arch, the maxi l la ry or mand ibular .
3. Marginal : A change that is conf ined to the f ree or marginal g ingiva. This is speci f ied as ei ther
local ized or general ized.
4. Papi l lary : A change that involves a papi l l a but not the rest of the f ree gingiva around a tooth.
A papi l lary change may be local ize d or genera l ize d.
5. Dif fuse : Spread out , d ispersed; af fects gingival margin, at tached gi ngiva, and interdental
papi l lae; may extend into alveolar mucosa. A di f fuse condit ion is more f requent ly local ized,
rarely general ized.
VI. Ear ly Recogni t ion of T iss ue Changes
Marked changes, such as moderate to severe general ized redness, enlargement , sponginess,
deep pockets, and def in i te mobi l i ty , are relat ively easy to detect even with l imited exper ience,
provided there is good l ight and accessibi l i ty for v is ion.
In contrast , when changes are subt le, local ized about one or a few teeth, and of a le sser
degree of sever i ty , more sk i l l fu l appl icat ion of knowledge is needed.
Ear l y r ecogn i t i on and t r ea t m en t of g ingival and per iodontal infect ions prevents neglect of
condit ions that can develop into severe disea se. Treatment is less compl icated, and the
success of t reatment and recovery to healthy t issue is p redictable when ear ly recognit ion
makes ear ly t reatment possible.
The Gingival Examinat ion
The examinat ion of the gingi va inc ludes evaluat ion of color , s ize, shape, consistency, sur face
Page 16 of 31
11/2/2010http://pt.wkhealth.com/pt/re/9780781763226/bookContentPane_frame.htm;jsessionid=MQ...

8/18/2019 Wilkins Ch 12
http://slidepdf.com/reader/full/wilkins-ch-12 17/31
texture, posi t ion, mucogingival junct ions, b leeding, and exudate. These are summarized in Table 12-
1, which is a c l in ical reference chart .
I . Color
A . Signs o f Heal th
1. Pale Pink. Darker in people with darker complexions.
2. Factors Inf luencing Color
a . V as cu l ar s up pl y.
b . Th i ck nes s o f ep i the li um .
c . Degree o f k e ra t in i za t ion .
d . Phys io log ic p igmenta t ion : melan in p igmenta t ion occurs f requent ly in A f r ican Amer icans ,
As ians, Ind ians, and Cauc asians of Mediterranean cou ntr ies.
B. Changes in Disease
1. In Chronic Inf lammat ion. Dark red, b lu ish red, magenta, or deep blue.
2. In Acute Inf lammat ion. Br ight red.
3. Extent . Deep involvement can be expected when di f fuse color changes extend into the
at tached gingiva, or f rom the marginal g ingiva to the mucogingival junct ion, or through into
alveolar mucosa.
II. Size
A . Signs o f Heal th
1. Free Gingiva. Flat , not enlarged; f i ts snugly around the tooth.
2. At tached Ging iva
a . Wid th o f a ttached ging iva varies among pat ien ts and among teeth fo r an ind iv idua l , f rom
1 to 9 mm.5
Table 12-1 Examination of the Gingival Clinical Markers
APPEARANCE INHEALTH
CHANGES INDISEASECLINICAL
APPEARANCECAUSES FORCHANGES
Color Uniformly palepink or coralpink
Acute: brightred
InflammationCapillarydilationIncreasedblood flow
Page 17 of 31
11/2/2010http://pt.wkhealth.com/pt/re/9780781763226/bookContentPane_frame.htm;jsessionid=MQ...

8/18/2019 Wilkins Ch 12
http://slidepdf.com/reader/full/wilkins-ch-12 18/31
Variations inpigmentationrelated tocomplexion,race
Chronic:bluish pink,bluish red
VesselsengorgedBlood flowsluggishVenous return
impaired AnoxemiaIncreasedfibrosis
Attachedgingiva: colorchange mayextend to themucogingivalline
Deepening ofpocket,mucogingivalinvolvement
Size Not enlargedFits snuglyaround thetooth
Enlarged Edematous:inflammatoryfluid, cellularexudate,vascularengorgement,hemorrhageFibrotic: newcollagenfibers
Shape(contour)
Marginalgingiva: knife-edged, flat,follows a curvedline about thetooth
Marginalgingiva:roundedrolled
Inflammatorychanges:edematous orfibrous
Papillae:(1)normalcontact: papillais pointed andpyramidal; fillstheinterproximalarea
Papillae:bulbousflattenedbluntedcratered
Bulbous withgingivalenlargement(seeedematousand fibrotic,above)
(2)space(diastema)between teeth;gingiva is flat orsaddle shaped
Cratered innecrotizingulcerativegingivitis
Page 18 of 31
11/2/2010http://pt.wkhealth.com/pt/re/9780781763226/bookContentPane_frame.htm;jsessionid=MQ...

8/18/2019 Wilkins Ch 12
http://slidepdf.com/reader/full/wilkins-ch-12 19/31
Consistency Firm Attachedgingiva firmlybound down
Soft, spongy:dents readilywhenpressed withprobe
Associatedwith redcolor, smoothshinysurface, lossof stippling,bleeding onprobing
Edematous:fluid betweencells inconnectivetissue
Firm, hard:resists probepressure
Associatedwith pinkcolor,stippling,bleeding onlyin depth ofpocket
Fibrotic:collagenfibers
SurfaceTexture
Free gingiva:smooth
Acutecondition:smooth,shiny gingiva
Inflammatorychanges intheconnective
tissue;edema,cellularinfiltration
Attachedgingiva: stippled
Chronic:hard, firm,with stippling,sometimesheavier thannormal
Fibrosis
Position ofGingivalMargin
Fully eruptedtooth: margin is1–2 mm abovecementoenamel junction, at orslightly belowthe enamelcontour
Enlargedgingiva:margin ishigher on thetooth, abovenormal,pocketdeepenedRecession:
Edematous orfibroticJunctionalepitheliumhas migratedalong theroot; gingivalmarginfollows
Page 19 of 31
11/2/2010http://pt.wkhealth.com/pt/re/9780781763226/bookContentPane_frame.htm;jsessionid=MQ...

8/18/2019 Wilkins Ch 12
http://slidepdf.com/reader/full/wilkins-ch-12 20/31
margin ismore apical;root surfaceis exposed
Position ofJunctionalEpithelium
During eruptionalong theenamel surface(Figure 12-7)Fully eruptedtooth: the junctionalepithelium is atthecementoenamel junction
Positiondeterminedby use ofprobe, is onthe rootsurface
Apicalmigration ofthe epitheliumalong the root
MucogingivalJunctions
Make cleardemarcationbetween thepink, stippled,attachedgingiva and thedarker alveolarmucosa withsmooth shinysurface
No attachedgingiva:(1) Color
changes mayextend fullheight of thegingiva;mucogingivallineobliterated(2) Probing
reveals that
the bottom ofthe pocketextends intothe alveolarmucosa(3) Frenal
pull maydisplace thegingivalmargin fromthe tooth
Apicalmigration ofthe junctionalepithelium Attachedgingivadecreaseswith pocketdeepeningInflammationextends intoalveolar
mucosa
Bleeding Nospontaneousbleeding orupon probing
SpontaneousbleedingBleeding onprobing:bleedingnear marginin acutecondition;bleedingdeep in
Degenerationof the sulcularepitheliumwith theformation ofpocketepitheliumBlood vesselsengorgedTissue
Page 20 of 31
11/2/2010http://pt.wkhealth.com/pt/re/9780781763226/bookContentPane_frame.htm;jsessionid=MQ...

8/18/2019 Wilkins Ch 12
http://slidepdf.com/reader/full/wilkins-ch-12 21/31
b . Wider in max il la than mandib le ; b roades t zone re la ted to inc isors, nar rowes t a t the
canine and premolar regions.
B. Changes in Disease
1. Free Gingiva and Papi l lae. Become enlarged. May be local ized or l imited to speci f ic areas or
general ized throughout the gingiva. The col deepens as the papi l lae increase in s ize.
2. At tached Ging iva. Decreases in amount as the pocket deepens.
C. Enlargement From Drug Therapy
Certain drugs used for speci f ic systemic therapy cause gingival enlargement as a s ide ef fect .
Examples of such drugs are phenytoin, cyc lospor ine, and ni fedipine.
I I I. Shape (Form or Con to ur)
A . Signs o f Heal th
1. Free Gingiva
a . Fo l lows a curved l ine around each tooth ; may be s tra igh ter a long w ide molar sur faces .
b . The marg in is kni fe -edged or s l ight ly rounded on fac ia l and l ingua l g ing iva ; c lose ly
adapted to the tooth sur face.
2. Papi l lae
a . Teeth w i th contact a rea. Facia l and l ingual g ing iva are po in ted or s ligh t ly rounded
papi l lae with a col area under the contact (Figure 12-8) .
pocket inchroniccondition
edematous
Exudate No exudateexpressed onpressure
White fluid,pus, visibleon digitalpressure Amount notrelated topocket depth
Inflammationin theconnectivetissueExcessiveaccumulationof white bloodcells withserum andtissue makesup theexudate (pus)
P.221
P.222
Page 21 of 31
11/2/2010http://pt.wkhealth.com/pt/re/9780781763226/bookContentPane_frame.htm;jsessionid=MQ...

8/18/2019 Wilkins Ch 12
http://slidepdf.com/reader/full/wilkins-ch-12 22/31
b. Spaced tee th (w i th d ias temata) . In terdenta l g ing iva is f la t o r saddle shaped.
B. Changes in Disease
1. Free Gingiva. Rounded or ro l led.
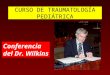
2. Papi l lae. B lunted, f lat tened, bulbous, cratered (Figure 12-10 ) .
3. Festoon (“McCal l 's festoon”) . An enlargement of the marginal g ingiva with the format ion of a
l i fesaver- l ike gingival prominence. Frequent ly , the total g ingiva is very narrow, with
associated apparent recession, as shown in Figure 12 -10D.
4. Clef ts
a . “ St i ll m an 's cl e ft ” (Figure 12-11 ) . A local ized recession may be V-shaped , apostrophe-
shaped, or form a s l i t l ike indentat ion. I t may extend several mi l l imeters toward the
mucogingival junct ion or even to or through the junct ion.
b . F loss c lef t . A c le ft c reated by incor rec t f loss pos i t ioning appears as a ver t ica l l inear or
V-shaped f issure in the marginal g i ngiva.6 I t usual ly occurs at one s ide of an i nterdentalpapi l la. The in jury can develop when dental f loss is curved repeatedly in an incomplete
“C” around the l ine angle so the f loss is pressed across the gingiva.
P.223
Page 22 of 31
11/2/2010http://pt.wkhealth.com/pt/re/9780781763226/bookContentPane_frame.htm;jsessionid=MQ...

8/18/2019 Wilkins Ch 12
http://slidepdf.com/reader/full/wilkins-ch-12 23/31
IV. Consist ency
A . Signs o f Heal th
1. F i rm when pa lpated w i th the side o f a b lun t ins t rument (probe) .
2 . A t tached g ing iva is bound down f i rm ly to the underly ing bone.
FIGURE 12-10 Gingival Shape or Contour. (A) Blunted papillae. (B) Bulbous papillae.(C) Cratered papillae. (D) Rolled, lifesaver-shaped “McCall's festoons.”
Page 23 of 31
11/2/2010http://pt.wkhealth.com/pt/re/9780781763226/bookContentPane_frame.htm;jsessionid=MQ...

8/18/2019 Wilkins Ch 12
http://slidepdf.com/reader/full/wilkins-ch-12 24/31
B. Changes in Disease
1. To Determine Consistency. Gent ly press s ide of probe on f ree gingiva. Sof t , spongy gingiva
dents readi ly ; f i rm, hard t issue res is ts .
2. Sof t , Spongy Gingiva. Related to acute stages of inf lammat ion with increased inf i l t rat ion of
f lu id and inf lammatory elements. The t issue appears red, may be smooth and shiny with loss
of s t ippl ing, has marginal enlargement , and bleeds readi ly on probing.
3. Firm, Hard Gingiva. Related to chronic inf lammat ion with increased f ibros is . The t issue may
appear pink and wel l s t ippled. Bleeding, when probed, usual ly occurs only in the deeper part
of a pocket , not near the margin.
4. Retract ion of the Margin Away From the Tooth. Normal ly , the f ree gingiva f i ts snugly about the
tooth. When the margin tends to hang s l ight ly away or is readi ly d isplaced wi th a l ight a ir
b last , the gingival f ibers that support the margi n have been dest royed (Figure 12-3) .
V. Surf ace Text ure
A . Signs o f Heal th
1. Free Gingiva. Smooth.
2. At tached Ging iva. St ippled (minutely “pebbled” or “orange peel” sur face).
3. Interdental Gingiva. The f ree gingiva is smooth; the center por t ion of each papi l la is s t ippled.
B. Changes in Disease
1. Inf lammatory Changes. May be loss of s t ippl ing, wi th smooth, shiny sur face.
Page 24 of 31
11/2/2010http://pt.wkhealth.com/pt/re/9780781763226/bookContentPane_frame.htm;jsessionid=MQ...

8/18/2019 Wilkins Ch 12
http://slidepdf.com/reader/full/wilkins-ch-12 25/31
2. Hyperkeratosis. May resul t in a leathery, hard , or nodular sur face.
3. Chronic Disease. Tissue may be hard and f ibrot ic , wi th a normal pink color and normal or
deep st ippl ing.
VI. Posi t ion
The actual posi t ion of the gingiva is the level of the at tached per iodontal t issue. I t is not d irect ly
v is ib le but can be determined by probing.
The apparent posi t ion of the gingiva is the level of the gingival margin or crest of the f ree gingiva
that is seen by direct observat ion.
A . Signs o f Heal thFor the fu l ly erupted tooth in an adult , the apparent posi t ion of the gi ngival margin is normal ly at the
level of , or s l ight ly below, the enamel contour or prominence of the cerv ical th ird of a tooth.
FIGURE 12-11 Gingival Clefts. (A) V-shaped Stillman's cleft. (B) Slit-like Stillman'sclefts of varying degrees of severity in relation to the mucogingival junction.
P.224
FIGURE 12-12 Gingival Recession. Left, Clinically visible recession of the gingivalmargin with root surface apparent to the eye. Right, The actual recession exposesthe root surface as the periodontal attachment migrates along the root surface.
Page 25 of 31
11/2/2010http://pt.wkhealth.com/pt/re/9780781763226/bookContentPane_frame.htm;jsessionid=MQ...

8/18/2019 Wilkins Ch 12
http://slidepdf.com/reader/full/wilkins-ch-12 26/31
B. Changes in Disease
1. Effect of Gingival Enlargement . When the gingiva enlarges, the gingival margin may be highon the enamel, par t ly or near ly cover ing the anatomic crown.
2. Effect of Gingival Recession
a . Def in it ion . Recess ion is the exposure o f roo t surface that resu l ts f rom the ap ica l
migrat ion of the junct ional epi thel ium (Figure 12-12 ) .
b . Ac tual recession. The ac tua l recess ion is shown by the pos i tion o f the a t tachment leve l .
The “receded area” is f rom the cementoenam el junct ion to the at tachment .
c . V is ib le recess ion. The v is ib le recession is the exposed root sur face tha t is v is ible on
cl in ical examinat ion. I t is seen f rom the gingival margin to the cementoenamel junct ion.
d . L oc al i ze d r ec es si on (Figure 12-13 ) . A local ized recession may be narrow or wide, deep
or shal low. The root sur face is denud ed, and the v is ib le recession may extend to or
through the mucogingival junct ion.
e . Measurement . Both ac tual and v is ib le recess ion can be measured w i th a probe f rom the
cementoenamel junct ion. Total recession is the actual and v is ib le posi t ions added
together.
VII. Bleeding
A . Signs o f Heal th
1 . No b leed ing s pont aneous l y o r on p rob ing .
2 . Heal t hy t i ss ue does no t b leed.
B. Changes in Disease
1. B leed ing occurs spontaneous ly or when probed.
2 . S u lc u la r ep i the l ium becom es d i s eas ed pocket epi thel ium. The ulcerated pocket wal l b leeds
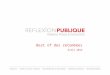
FIGURE 12-13 Localized Recession. A single tooth may show narrow or wide, deep orshallow recession. (A) Wide, shallow. (B) Wide, deep, with narrow attached gingiva. (C)Narrow, deep, with missing attached gingiva.
Page 26 of 31
11/2/2010http://pt.wkhealth.com/pt/re/9780781763226/bookContentPane_frame.htm;jsessionid=MQ...

8/18/2019 Wilkins Ch 12
http://slidepdf.com/reader/full/wilkins-ch-12 27/31
readi ly on gent le probing.
VIII. Exudate
A . Signs o f Heal th
There is no exudate except s l ight g ingival sulcus f lu id. Gingival sulcus f lu id cannot be seen by
direct observat ion.
B. Changes in Disease
1 . I ncreas ed ging iv a l su l cus f lu i d .
2 . Amount o f exudate is not an ind ica tor o f the ex tent o f d isease or the depth o f the per iodonta l
pockets.
The Gingi va of Young Chi ld ren7,
8
I . Signs of Heal th
A . Pr i mary Den t i t i on
1. Color. P ink or s l ight ly red.
2. Shape. Thick, rounded, or ro l led.
3. Consistency. Less f ibrous than adult g ingiva; not t ight ly adapted to the teeth; may be easi ly
displaced with a l ight a ir jet .
4. Surface Texture. May or may not have st ippl in g; h igh percentage of pat ients has shiny
gingiva.
5. At tached Ging iva. Width of at tached gingiva in chi ldren aged 3 to 5 years: between 1 and 6
mm.5
6. Interdental Gingiva
a . Anterio r : d ias temata are f requent ly present and the pap i l lae are f la t o r sadd le shaped.
b . Pos ter io r : col be tween fac ia l and l ingua l pap i l lae when tee th are in contac t (F igure 12-
8) .
E v ery d a y E t h i c s
Bri ta in and Nicholas were f i rs t -year dental hygi ene students just beginning to pract ice on each
other as student partners in the precl in ic program . Dur ing the oral examinat ion, Br i ta in n ot iced
that Nicholas had some areas of b le eding and changes in the contour of the marginal g ingiva. In
general , the sof t t issue seemed more sponge- l ike and loose, but Br i ta in was not sure she c lear ly
understood what is considered “normal, ” rememb er ing that the c l in ical inst ructor of ten referred
to a “ range” of normal.
Br i ta in decided to focus on and docum ent the areas that were pale pink, f i rm, and pointed in the
interproximal areas. She careful ly recorded this informat ion with great detai l and then s ignaled
for her inst ructor to ver i fy the f indings. When the i nst ructor sat down and rev iewed the
P.225
Page 27 of 31
11/2/2010http://pt.wkhealth.com/pt/re/9780781763226/bookContentPane_frame.htm;jsessionid=MQ...

8/18/2019 Wilkins Ch 12
http://slidepdf.com/reader/full/wilkins-ch-12 28/31
examinat ion she was pleased with Br i ta in 's thoroughness. The inst ructor provided posi t ive
feedback and quick ly moved on to the ne xt pair of s tudents. Br i ta in began to feel uneasy that
she hadn't pointed out the ging ival t issues that she thought were possibly inf lamed.
Q u es t i o n s f o r C o n s id e ra t i o n
1. Exp la in how the e th ica l p r inc iples o f au tonomy, benef icence, and verac i t y apply to th is
s i tuat ion.
2 . Ind icate how Nicholas is the center o f th is di lemma both f rom the perspec t ive o f Br i ta in , a
student , and the c l in ical inst ructor who f inds ou t f rom another facul ty member that he or
she thinks Nicholas has def in i te s igns of per iodontal d isease.
3 . E th ica l ly , what a l te rnat ives or ac t ions can Br i ta in take a t th is t ime to address the “uneasy”
feel ing she has about Nicholas ' g ingival s tatus?
B. Mixed Dent i t ion
Constant s tate of change related to exfol iat ion and erupt ion.
Free gingiva may appear rol led or rounded, s l ight ly reddened, shiny, and with a lack of
f i rmness.
The gingiva covers a vary ing p ort ion of the anatomic crown, depending o n the stage of
erupt ion (Figure 12-7) .
I I . Changes in Disease
Examinat ion of the per iodontal t issues of a chi ld is not d i f ferent f rom that o f an adult . A complete
examinat ion is necessary, inc luding probing around each tooth.
Gingiv i t is occurs f requent ly in chi ldren but is usual ly revers ible without leaving permanent damage.
Al though relati vely rare, per iodont i t is can occur in pr imary denti ti on.
Mucogingival problems occur in chi ldren.9 ,10 The recognit ion of def ic iencies of at tached gingiva has
part icular s igni f icance for the chi ld who wi l l need or thodont ic t reatment .
The Gingi va af ter Per iodon tal Surgery
The character is t ics of “normal healthy gingiva” take on di f ferent d imensions for the pat ient who has
completed t reatment for pockets, bone loss, and other s i gns of a per iodontal infect ion. The
juncti onal epi th el ium is apica l to the cementoenamel junct ion. Aft er he al ing, th e sulcus
depths may be with in normal range and no bleeding occurs when probed.
Depending on the exact t reatment performed, examinat ion shows changes f rom the in i t ia levaluat ion. For example, where the in i t ia l examinat ion showed a def ic iency of at tached gingiva with
f renal pul l , mucogingival surgery may have been designed and t reatment sat is factor i ly completed to
create new at tached gingiva. With each maintenance appointment , a thorough, careful examinat ion
is necessary to control factors that may permit recurrence of d isease.
Factors To Teach The Pat ient
P.226
Page 28 of 31
11/2/2010http://pt.wkhealth.com/pt/re/9780781763226/bookContentPane_frame.htm;jsessionid=MQ...

8/18/2019 Wilkins Ch 12
http://slidepdf.com/reader/full/wilkins-ch-12 29/31
Characterist ics of normal healthy gingiva.
The signif icance of bleeding; healthy t issue does not bleed.
Relat ionship of f indings during a gingival examinat ion to the personal dai ly care
procedures for infect ion control.
The special at tent ion needed for an area of gingival recession to prevent abrasion,
inf lammation, and further involvement.
How the method of brushing, st i f fness of toothbrush f i laments, abrasiveness of adent i f r ice, and pressure appl ied during brushing can be factors in gingival recession.
References
1. Av er y , J .K . and Steele, P.F. : Essent ials of Oral Histology and Embryology: A Cl in i cal
Approach. St . Louis, Mosby, 1992, pp. 131–134.
2. A i n am o , J . and Löe, H. : Anatomical Character is t ics of Gingiva: A Cl in ical and Microscopic
Study of the Free and At tached Gingiva, J. Per iodontol . , 37 , 5, January–February, 1966.
3. Orban , B . : Cl in ical and Histologic Study of the Surface C haracter is t ics of the Gingiva, Oral
Surg. Oral Med. Oral Pathol. , 1 , 827, September, 1948.
4. Bhaskar , S .N. , ed. : Orban's Oral Histology and Embryology , 11th ed. St . Louis, Mosby, 1991,
pp. 323–325.
5. Bowers , G . M. : A Study of the Width of At tached Gingiva, J. Per iodontol . , 34 , 201, May, 1963.
6. Hal lman , W.W. , Waldrop, T.C. , Houston, G.D. , and Hawkins, B.F. : Flossing Clef ts : Cl in icaland Histologic Observat ions, J. Per iodontol . , 57 , 501, August , 1986.
7. Duperon , D . and Takei, H.H. : Gingival Diseases in Chi ldhood, in Newman, M.G. , Takei, H.H. ,
Klokkevold, P.R. , and Carranza, F.A. : Carranza's Cl in ical Per iodont ics , 10th ed. St Louis,
Saunders/Elsevier , 2006, pp. 404–410.
8. Casamass imo, P .S . : Per iodontal Condit ions, in Pinkham, J.R. , ed. : Pediat r ic Dent is t ry:
Infancy Through Adolescence , 2nd ed. Phi ladelphia, W.B. Saunders Co. , 1994, pp. 35 3–357,
607–615.
9. Maynard, J .G. and Ochsenbein, C. : Mucogingival Problems, Prevalence and Therapy in
Chi ldren, J. Per iodontol . , 46 , 543, September, 1975.
10. A n d l i n -So b o c k i , A . , Marcusson, A. , and Persson, M. : 3-Year Observat ions on Gingiva l
Recession in Mandibular Inc isors in Chi ldren, J. Cl in. Per iodontol . , 18 , 155, March, 1991.
Suggested Reading s
Page 29 of 31
11/2/2010http://pt.wkhealth.com/pt/re/9780781763226/bookContentPane_frame.htm;jsessionid=MQ...

8/18/2019 Wilkins Ch 12
http://slidepdf.com/reader/full/wilkins-ch-12 30/31
A i n am o , A . , A inamo, J. , and Poikkeus, R. : Cont inuous Widenin g of the Band of At tached
Gingiva From 23 to 65 Years of Age, J. Per iodont . Res. , 16 , 595, November, 1981.
Fedi , P .F. , Vernino, A.R. , and Gray, J .L. : The Per iodont ic Syl labus , 4th ed. Balt imore,
Lippincot t Wi l l iams & Wilk ins, 2000, pp. 1–13.
Grant , D.A . , Stern, I .B. , and Lis tgarten, M.A. , eds. : Periodont ics , 6th ed. St . Louis, Mosby,
1988, pp. 3–75.
Hassel l , T .M. : Tissues and Cel ls of the Per iodont ium, Periodontol . 2000 , 3 , 9, 1993.
Hem pt on , T . J . , Wi lk ins, E. , and Lancaster , D. : Evaluat ion of At tached Tissue Aids in Treatment
of Recession, RDH , 16 , 34, June, 1996.
M ar io t t i , A . : The Extracel lu lar Matr ix of the Per iod ont ium: Dynamic and Interact ive Tissues,
Periodontol . 2000 , 3 , 39, 1993.
Mel f i , R.C. and Al ley, K.E. : Permar 's Oral Embryology and Microscopic Anatomy , 10th ed.
Phi ladelphia, L ippincot t Wi l l iams & Wilk ins, 2000, pp. 237–251.
Ser ino , G . , Wennström, J.L. , L indhe, J . , and Eneroth, L. : The Prevalence and Dist r ibut ion of
Gingival Recession in Subjects With a H igh Standard of Oral Hygiene, J. Cl in. Per iodontol . , 21 ,
57, January, 1994.
Vacek, J .S . , Gher, M.E. , Assad, D.A. , Richardson, A.C. , and Giambarresi , L. I . : The Dimensions
of the Human Dentogingival Junct ion, Int . J . Per iodont . Restorat ive Dent . , 14 , 155, Number 2,
1994.
Gingiva of Chi ld ren
A m er i c an A c ad em y o f Per i o d o n t o l o g y , Commit tee on Research, Science and Therapy:
Posi t ion Paper: Per iodontal Diseases of Chi ldren an d Adolescents, J. Per iodontol . , 67 , 57,
January, 1996.
A n d l i n -So b o c k i , A . : Changes of Facial Gingival Dimensions in Chi ldren: A 2-year Longitudinal
Study, J. Cl in. Per iodontol . , 20 , 212, March, 1993.
A n d l i n -So b o c k i , A . and Bodin, L. : Dimensional Al terat ions o f the Gingiva Related to Changes
of Facial /L ingual Tooth Posi t ion in Permanent Anter ior Teeth of Chi ldren: A 2-year Longitudinal
Study. J. Cl in. Per iodontol . , 20 , 218, March, 1993.
B im s t e in , E. and Eidelman, E. : Longitudinal Changes in the Width of At tached Gingiva in
Chi ldren, Pediat r . Dent . , 10 , 22, March, 1988.
B im s t e in , E. , Machtei , E. , and Eidelman, E. : Dimensional Di f ferences in the At tached and
Page 30 of 31
11/2/2010http://pt.wkhealth.com/pt/re/9780781763226/bookContentPane_frame.htm;jsessionid=MQ...

8/18/2019 Wilkins Ch 12
http://slidepdf.com/reader/full/wilkins-ch-12 31/31
Kerat in ized Gingiva and Gingival Sulcus in the Ear ly Permanent Dent i t ion: A Longitudinal
Study, J. Pedod. , 10 , 247, Spr ing, 1986.
B im s t e in , E. , Matsson, L. , Soskolne, A.W., and Lustman, J . : Histologic Character is t ics of the
Gingiva Associated With the Pr imary and Permanent Teeth of Chi ldren, Pediat r . Dent . , 16 , 206,
May/June, 1994.
Kesz t he ly i , G . : The Width of Plaque-Free Zo nes on Pr imary Molars With At tachment Loss, J.
Cl in. Per iodontol . , 18 , 94, February, 1991.
Saar io , M. , A inamo, A. , Mat t i la, K. , and Ainamo, J. : The Width of Radiological ly Def ined
Att ached Gingiva Over Per manent Teeth in Chi ldren, J. Cl in. Per iodontol . , 21 , 666, November,
1994.
Saar io , M. , A inamo, A. , Mat t i la, K. , Suomalainen, K. , and Ainamo, J. : Th e Width of
Radiological ly Def ined At tached Gingiva Over Deciduous Teeth, J. Cl in. Per iodontol . , 22 , 895,
December, 1995.
Tenenbaum, H. and Tenenbaum, M. : A Cl in i cal Study of the Width of the At tached Gingiva in
the Deciduous, Transi t ional and Permanent Dent i t ions, J. Cl in. Per iodontol . , 13, 270, Apr i l ,
1986.
Page 31 of 31