1
OrganizationalStructures
forClinicalTransformationBy:MaryStaley‐Sirois,PT,MBA&ColinKonschak,MBA,FHIMSS,FACHEThe healthcare industry is in the process of transforming itself using technology. These
transformationeffortsfocusonmovingfrommanualprocesses,oftenbasedonhistoricalpractices,
to technology‐enabled or even automated processes. The overall effort involved in such a
transformation creates a tremendous amount of disruption to all aspects of the organization,
creatingtheabsoluteneedforacommitmenttomanagingchange.
Thispaperexplores, throughcase studies, theclinicalandcultural considerations in implementing
andmanagingworkflowchangesatthreelargehealthcaresystems.
Introduction
Thescopeofclinicalandculturaltransformationinhealthcaretodayisprofoundandall‐inclusive.It
requirescollaborationbetweenallclinicalandtechnicalareasofahealthcareorganization,
necessitatingnewgovernanceandorganizationalstructures.
Thetransformationismulti‐dimensional,takingonmedical,clinicalandculturalimplications.Onthe
medicalandclinicalsides,effortsfocusondeterminingandimplementingbest‐practice,evidence‐
basedprocessesthatsupporttheadoptionofclinicaltechnologies.Ontheculturalside,theclinical
transformationeffortsrequirehealthcareorganizationstoworkcollaboratively,bringingtogether
groupsofphysicians,nurses,pharmacists,ancillarycareproviders,andinformationsystempersonnel
tochallengethewaythingsaredonetoday.Theresultsofsuchcollaborationarenewcareprocesses
andpractices,aswellasdatastandardsandintegritythatbettersupportapatient‐centricapproachto
care.Thesedevelopmentswillensurepatientsafety,qualityofcare,workflowefficiencies,care
timelinessandeffectiveness,andoverallcaregiverproductivity.
Theoveralleffortcreatesatremendousamountofdisruptiontoallaspectsoftheorganization,
creatingtheabsoluteneedforacommitmenttomanagingchangeateverypointalongtheway.
Becausethescopeofthisclinicalandculturaltransformationissoprofoundandall‐inclusive,
organizationsmustcreatenewgovernanceandorganizationalstructuresthatensurecollaboration
acrossclinicalandtechnicalareas.Tosucceed,organizationalchangestructures,committeesand
teamsshouldensure:
• Leadershipalignmentattheseniorexecutivelevel,includingboard‐levelsupport
• Participationofmulti‐disciplinaryend‐userworkteams
• Sponsorshipbyclinical,operationalandphysicianleaders
2
Essentially,thoughthegoalforeachorganizationappearstobethe
implementationofatechnology,the
organizationsfocustheirgoalsonstepsthataffectuseofthetechnology.Thus,theirendgoalsare
actuallytheadoptionofthetechnology.
• FacilitationfromITpersonnel
Recurringtheme
Thecasestudiesthatfollowexplorethreelargehealthcare
systemsthataretransformingclinicalcarethroughthe
implementationofworkflowchangessupportedbytechnologies.
Therecurringthemeinalloftheorganizationalstructuresisthe
presenceofphysicianandnursingchampionshipalongwith
carefulalignmentoftheorganization’soperationalentities.
Essentially,thoughthegoalappearstobetheimplementationofa
technology,theorganizationsdefinegoalsthatalignwiththe
utilizationofthetechnology.Thus,theirendgoalsarethe
adoptionofthetechnologyintheprovisionofhighqualitypatient
care.
Finally,inadditiontoaddressingorganizationalclinicaltransformationmodels,effortsweremadeto
provideexamplesofclinicaltransformationdepartmentreportingwithintheoverallorganizational
leadershipstructure.Today,trendsrevealreportingoftransformationdepartmentsthroughtheChief
InformationOfficer(CIO);however,commentsfrommanagementindicatespecificchallengeswiththis
structure,namely,alackofclinical/medicalprocesschangeimpactingleadership,understandingand
appreciation.
Alignmentmustprovideclearandhighlysupportedlinesofcommunicationbetweentransformational
leadersandclinical/medicalstaffoperationalleadersatalllevelsoftheorganization.Sowhile
healthcareorganizationscontinuetolookfororganizationalalignmentbestpracticeforpositiveclinical
transformation,theleadershipofclinicaltransformationalignedwiththeCIOcouldputthetechnology
implementationgoalsatrisk.Itisimperativethatclinicalinformationsystemimplementationsare
championedbyseniormedicalandclinicalleadersworkingincompletealignmentwiththeCIO.
CaseStudyOne:ReorganizationAroundaNewClinicalApplication
HealthcareOrganizationOne(HO1)isa12‐hospitalhealthsystemthatisimplementingaclinical
centerpieceapplicationthatwilladdressscheduling,access,emergencydepartment(ED),orderentry,
andclinicaldocumentation.HO1begantheirclinicaltransformationeffortsbycreatingadepartment
ofclinicaltransformation(CT).TheCTdepartmentreportedtotheChiefOperatingOfficer(COO),who
inturnpartnerswiththeinformationsystemsdepartment(IS).Atthestartoftheirclinical
transformationjourney,HO1hadnoseniormedicalornursingofficer;andthelackofalignmentofthe
CTdepartmentandIScreatedsignificantissues.
3
Eventually,aChiefMedicalOfficer(CMO)andChiefNursingOfficer(CNO)joinedwiththeChief
MedicalInformationOfficer(CMIO)toreorganizetheCTdepartment.Thegoalsincluded:
• TobetteralignwiththeworkofIS;and,
• Becomeabridgebetweentechnologyandclinicaloperations.
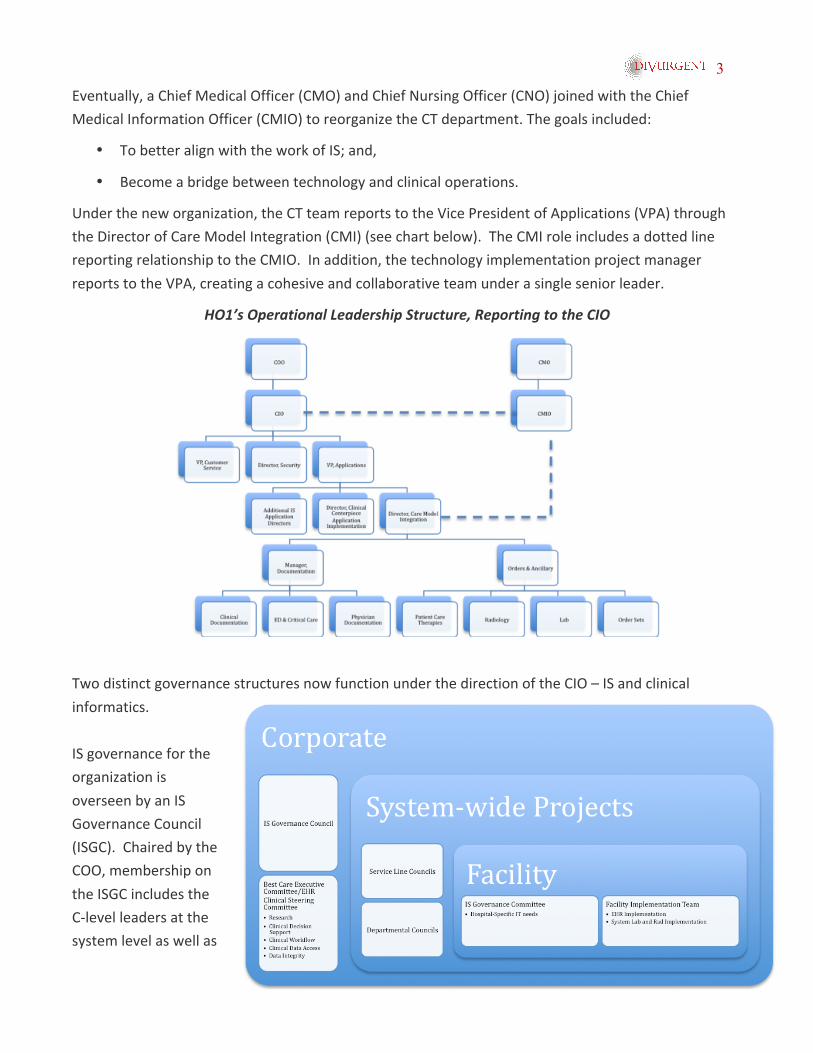
Undertheneworganization,theCTteamreportstotheVicePresidentofApplications(VPA)through
theDirectorofCareModelIntegration(CMI)(seechartbelow).TheCMIroleincludesadottedline
reportingrelationshiptotheCMIO.Inaddition,thetechnologyimplementationprojectmanager
reportstotheVPA,creatingacohesiveandcollaborativeteamunderasingleseniorleader.
HO1’sOperationalLeadershipStructure,ReportingtotheCIO
TwodistinctgovernancestructuresnowfunctionunderthedirectionoftheCIO–ISandclinical
informatics.
ISgovernanceforthe
organizationis
overseenbyanIS
GovernanceCouncil
(ISGC).Chairedbythe
COO,membershipon
theISGCincludesthe
C‐levelleadersatthe
systemlevelaswellas
4
theCIOandhisseniorleadershipteam.
TheExecutiveCommittee(EC)overseesclinicalinformaticsgovernancefortheorganization.This
includesthedataandworkflowthatwillbeimpactedduringimplementationoftheelectronichealth
record(EHR).TheCMOchairsthiscommitteeofseniorclinicalleaders,includingphysicians,nursing,
quality,patientsafetyandIS.Inputtodiscipline‐specificdataandworkflowcomesthroughthe
system‐level,interdisciplinaryand/ordepartmentalclinicalcouncils,witheachcouncilco‐chairedbya
physicianandanoperationalleader.
Hospital‐levelgovernanceforIS(aswellasclinicaldataandprocessstandardizationthatisaresultof
theEHR)occursthroughFacilityImplementationTeams(FIT).TheFITisco‐sponsoredby:asenior
hospitalexecutive,aphysicianleaderandrepresentativesfromvarioushospitaldepartmentsandthe
medicalstaff.
CaseStudyTwo:Enterprise‐buildLocalizedat22Hospitals
HealthcareOrganizationTwo(HO2)isa22‐hospitalhealthcaresystemimplementingaclinical
centerpieceapplicationthatwilladdressscheduling,access,ED,orderentry,medicationmanagement,
andclinicaldocumentation.
Inaddition,theyareimplementingasystemstandardRIS.LikeHO1,theyarecreatinganenterprise
buildwithlocalizationattheaffiliateorhospitallevel.Theoverallprojecttimelineissixyears.
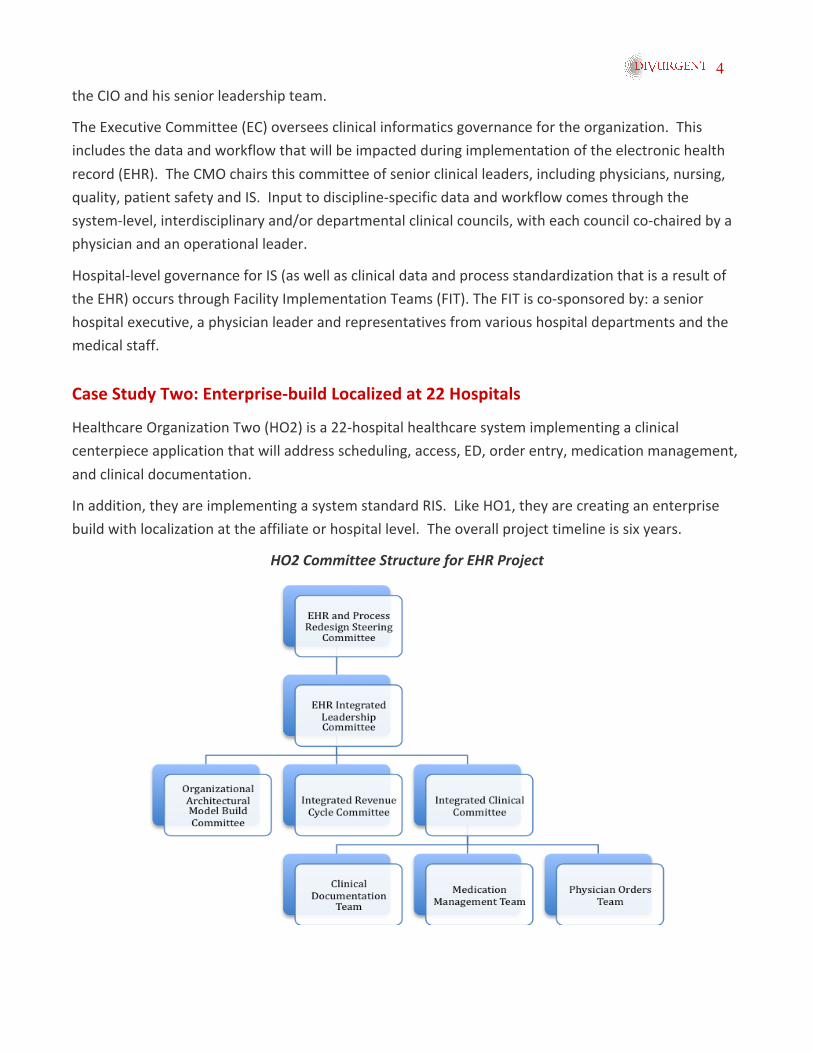
HO2CommitteeStructureforEHRProject
5
TheCEOchairsthesystem‐levelEHRandProcessTransformationSteeringCommittee,with
membershipincludingtheC‐suiteleaders.ReportingtothiscommitteeistheEHRIntegrated
LeadershipCommittee,whichismadeupofoperationalleadershipfromthefouraffiliatesthatare
targetedforgo‐livefirst.Reportingtothiscommitteearetwolinesofwork‐thetechnicalbuildand
operationalstandardization.
Thetechnicalbuildisconsideredtheorganization’sArchitecturalModel.Duringbuildsessions,
operational/clinicalfrontlineleadersandstaffaddresstechnicalconsiderationssuchasnavigation
tools,headersandtheoverallapplicationlookandfeel.
AnIntegratedRevenueCycleCommitteeandtheIntegratedClinicalCommitteeoverseeoperational
andclinicalstandardization,includingdatacontentanddefinition,documentationflowsheetsand
workflow.
Thesearechairedbykeyoperationalleadersandalthoughintegrated,arefocusedonspecific
functionalareas.
SimilartoHO1,HO2hasaCTdepartmentreportingthroughtheCIO.Itisthroughtheprojectstructure
abovethattransformationalprojectactivitiesoccur.
CaseStudyThree:TwoClinicalInformationSystems,OneImplementationTeam
HealthcareOrganizationThree(HO3)isa43‐siteorganizationfocusedonimplementingtwomajor
clinicalinformationsystemvendors.Whiletheyareusingdifferentvendors,chosenbasedoncurrent
businessneedsandpractices,asingleprojectteamleadsthetransformation.Inspiteofthedifferent
clinicalapplications,theorganizationiscommittedtoassimilaraspossiblecareprocesses,practices
anddatastructures.
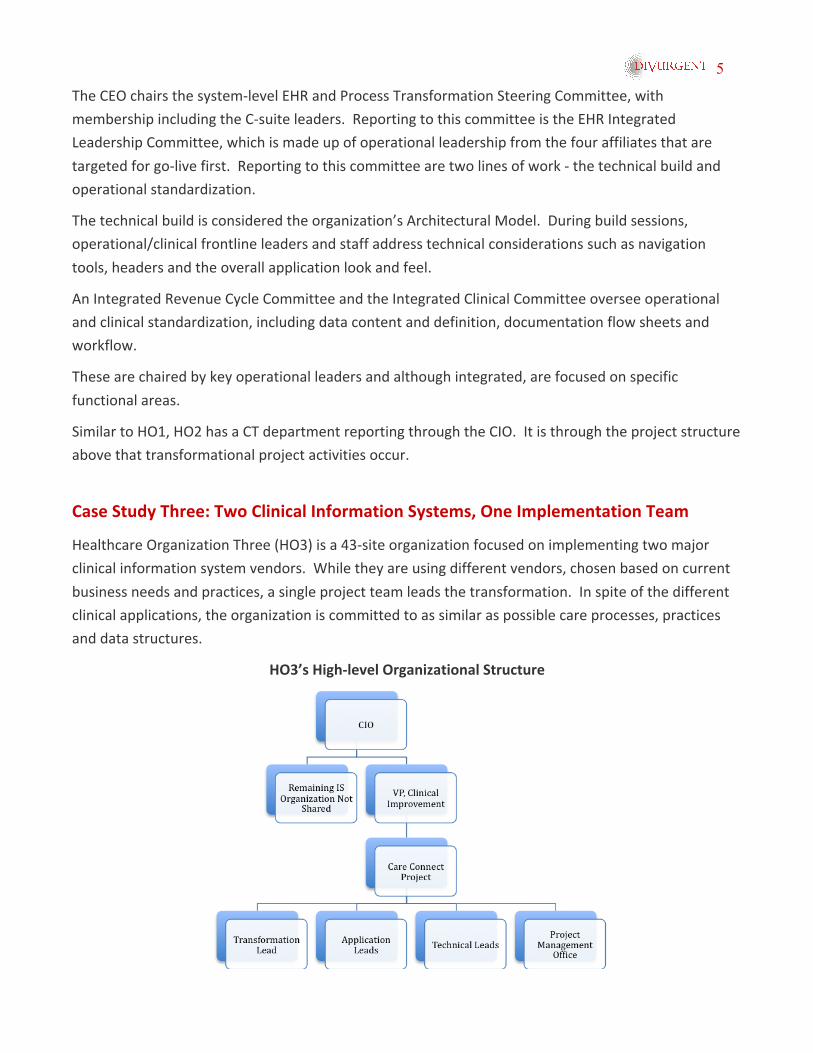
HO3’sHigh‐levelOrganizationalStructure
6
TheprojectreportsthroughtheCIOviaaVicePresidentofClinicalImprovement,whoisresponsible
forthetransformationaswellastheapplicationimplementationareas.Theseteamsworkwith
hospital‐basedprocessandapplicationdesignteams.
TheTransformationLeadisresponsibleforoverallprojectgovernance,changemanagement,process
redesignandstandardizationanduserreadiness.Theseeffortsareparamounttothesuccessofan
EHRimplementation.ItissignificanttonotethattheTransformationLeadthatinitiallyreported
throughtheCMOwasrepositionedwiththearrivalofanewCIO.
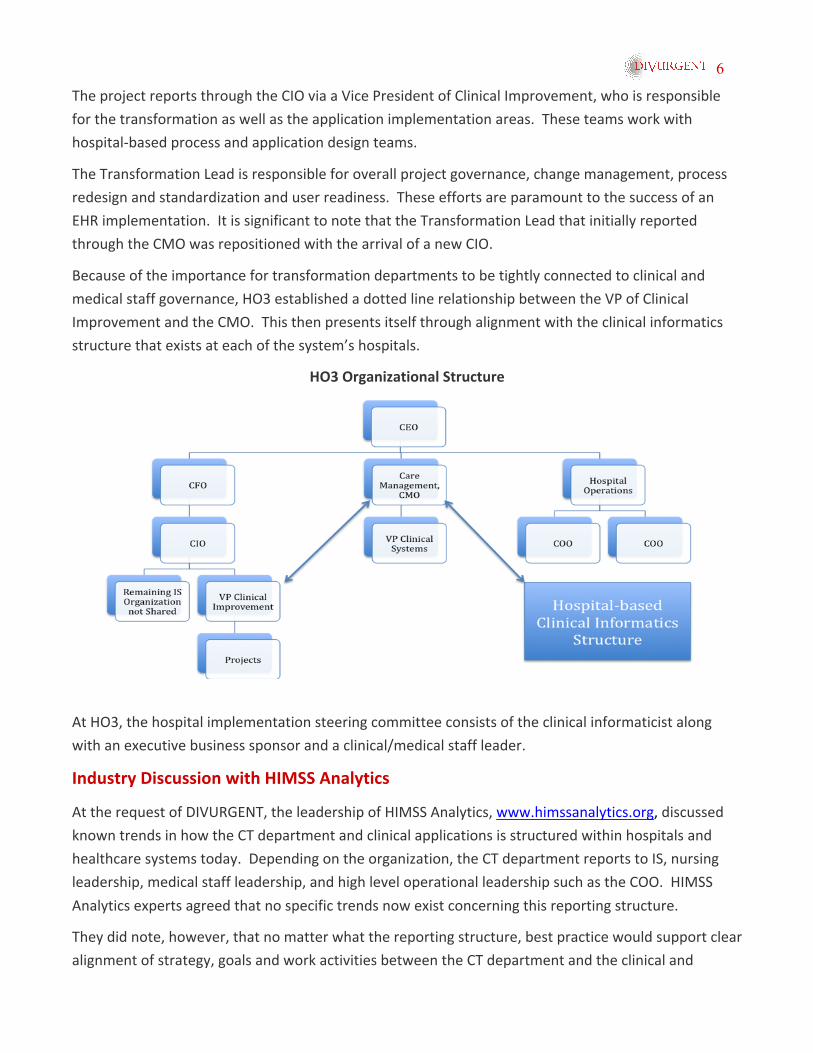
Becauseoftheimportancefortransformationdepartmentstobetightlyconnectedtoclinicaland
medicalstaffgovernance,HO3establishedadottedlinerelationshipbetweentheVPofClinical
ImprovementandtheCMO.Thisthenpresentsitselfthroughalignmentwiththeclinicalinformatics
structurethatexistsateachofthesystem’shospitals.
HO3OrganizationalStructure
AtHO3,thehospitalimplementationsteeringcommitteeconsistsoftheclinicalinformaticistalong
withanexecutivebusinesssponsorandaclinical/medicalstaffleader.
IndustryDiscussionwithHIMSSAnalytics
AttherequestofDIVURGENT,theleadershipofHIMSSAnalytics,www.himssanalytics.org,discussed
knowntrendsinhowtheCTdepartmentandclinicalapplicationsisstructuredwithinhospitalsand
healthcaresystemstoday.Dependingontheorganization,theCTdepartmentreportstoIS,nursing
leadership,medicalstaffleadership,andhighleveloperationalleadershipsuchastheCOO.HIMSS
Analyticsexpertsagreedthatnospecifictrendsnowexistconcerningthisreportingstructure.
Theydidnote,however,thatnomatterwhatthereportingstructure,bestpracticewouldsupportclear
alignmentofstrategy,goalsandworkactivitiesbetweentheCTdepartmentandtheclinicaland
7
medicalstaffleadership(CNOandCMO).InfurtherdiscussingthefutureoftheCTdepartment,they
indicatedthatitcouldevolveintoonedepartmentwithoverallresponsibilityforaformalinformatics
strategy.
Thisgroupaswellasleadersofthethreehealthcareorganizationsfeaturedhereforcasestudies,
expressedsomefrustrationoverallwithhospitalleadershipteams.Theyexpressedthathospital
leadership,includingtheCIO,didnotfullyappreciatetheneedtoconsidertransformationalprocess
andpracticeactivitieswellinadvanceofthetechnologyimplementation.
Finally,weassumethatthegoalofatechnologyimplementationisnottheimplementationitself,but
theadoptionofthetechnologyintoclinicalandmedicalstaffpracticeandworkflowprocesses.
Therefore,thehealthsystemsdiscussedheremaintainedsignificantfocusontheimportanceofawell‐
definedandwell‐supportedchangemanagementstrategyandplan.ThisissomethingforwhichaCT
departmentisuniquelyqualified.
Conclusions
Whilehealthcareorganizationscontinuetolookfororganizationalalignmentbestpracticeforpositive
clinicaltransformationoutcomes,themovetoplacementundertheCIOputstheappreciationfor,and
supportof,theimpactonclinical/medicalprocessesandpracticeatrisk.Alignment,ifreportingtothe
CIO,mustprovideclearandhighlysupportedlinesofcommunicationbetweentransformational
leadersandclinical/medicalstaffoperationalleadersatalllevelsoftheorganizationinordertobe
successful.
AboutTheAuthors:
MaryLawrenceStaley‐Sirois,PT,MBAisPresidentofResurgenceConsulting.Ms.Siroishasnearly20yearsofhealthcareoperationalandstrategicplanningexperienceacrossawidespectrumofproviderandacademicenvironments.Asaphysicaltherapistbyclinicalbackground,shehasworkedwithlargeandsmallhealthcaresystemsontheplanningnecessaryforclinicaltransformationasaresultofanEHRdeployment,organizationgovernanceandchangemanagement,medicalandclinicalstaffcollaborationonbestpracticeandevidence‐basedprocesses,regulatorycompliancereadinessandissueresolution,organizationalbudgetdevelopmentandrelatedbenefitsrealizationprojection,anddetailedprojectplanning.
Ms.Sirois’workisfocusedonleveragingtheskillsandteamofthehealthcareorganizationinthedeploymentofstrategicinitiatives‐fromproductdevelopment,tooperationalmanagement,totransformationofclinicalprocessandpractice,toEHRadoption.Ms.Siroisiswell‐publishedonHIPAAcomplianceandisapublicspeakerinhealthcareoperationsandregulatorycompliance.Inadditiontoherworkinthehealthcareprovidermarket,Ms.Siroisworkscloselywithinternationalorganizationsforthedevelopmentofoperationalandeducationalprogramstoimprovehealthcareindevelopingcountries.

8
ColinB.Konschak,MBA,FHIMSS,FACHEisaManagingPartnerwithDIVURGENTandleadstheAdvisoryServicesPractice.Heisahighlyaccomplishedexecutivewithover17yearsofexperienceandrecognizedachievementinqualityservicedeliveryandprojectmanagement.Mr.Konschakhasextensiveexperienceinhealthcareoperations,P&Lmanagement,accountmanagement,strategicplanningandalliancemanagement.Hisbroadhealthcareexperienceencompassespharmaceutical,provider,payer,informationtechnologyandconsulting.Mr.KonschakisaregisteredPharmacist,possessesanMBAinhealthservicesadministration,isboardcertifiedinhealthcaremanagement,andisasixsigmablackbelt.HeisanAdjunctProfessorwithOldDominionUniversityleadingclassesintheirMBAprogramonPerformanceImprovement,NegotiationandBusinessEthics.Mr.Konschak’scommitmenttothehealthcareindustryisevidentinhisparticipationinsomeoftoday’sleadinghealthcaretradeorganizationsincludingservingastheimmediatePastPresidentoftheVirginiaHIMSSChapter,andachievingandmaintainingFellowstatusinboththeHealthcareInformationManagementandSystemsSociety(HIMSS)andtheAmericanCollegeofHealthcareExecutives(ACHE).
AboutDIVURGENT:
Foundedbyateamofconsultingveterans,DIVURGENTisanationalhealthcareconsultingfirmfocusedsolelyonthebusinessofhospitalsandotherhealthcareproviders.DIVURGENTprovidesadvisory,interimmanagement,revenuecyclemanagement,projectmanagement,andmodelingandsimulationservicestohelpimprovepatients’lives.
Wearecommittedto:
ProvidingThoughtLeadership
ProvidingExceptionalValueforourServices
FacilitatingKnowledgeTransfer
EnsuringClientSatisfaction
5919GreenvilleAvenueSuite144Dallas,TX75216‐1906
1340GreatNeckRoadSuite1272VirginiaBeach,VA23454
(877)254‐9794 [email protected] www.DIVURGENT.com
Recommended

















