1
Adjuvant chemotherapy in resectable liver-limited metastasis colorectal cancer
R4 陳三奇指導 VS: 鄧豪偉

2
Reference• Clinicopathological features and prognosis in resectable synchronous and metachronous colorectal liver
metastasis Ann Surg Oncol 2007
• Multicenter Randomized Trial of Adjuvant Fluorouracil and Folinic Acid Compared With Surgery Alone After Resection of Colorectal Liver metastases: FFCD ACHBTH AURC 9002 Trial 2006 JCO
• Outcome After Hepatectomy for Multiple (Four or More) Colorectal Metastases in the Era of E ective ffChemotherapy 2007 Annals of Surgical Oncology
• Adjuvant Chemotherapy After Potentially Curative Resection of Metastases From Colorectal Cancer: A Pooled Analysis of Two Randomized Trials 2007 Annals of Surgical Oncology 2008 JCO.
• Perioperative chemotherapy with FOLFOX4 and surgery versus surgery alone for resectable liver metastases from colorectal cancer (EORTC Intergroup trial 40983): a randomised controlled trial 2008 Lancet
• A randomized phase III study comparing adjuvant 5-fluorouracil/folinic acid with FOLFIRI in patients following complete resection of liver metastases from colorectal cancer2009 Annals of oncology
• Adjuvant oxaliplatin- or irinotecan-containing chemotherapy improves overall survival following resection of metachronous colorectal liver metastases 2010 Int J Colorectal Dis
• NCCN guidline 2012 version 3.

3
Introduction
• Colorectal cancer when diagnosis– 50%-60%: metastases– 20%-34% synchronous liver metastases– Frequent metachronously following treatment.

4
• Prognosis of liver metastasis :– no treatment : 5-year survival- 0.4%-4%.– Palliative CT( fluorouracil ): 3-year survival -5-10%.
• Surgery in selected patients:– remove colorectal liver metastases– cure is possible in this population– 5-y-s : 25-40%.

5
• Poor prognostic factor: – >3 metastases, bilobar distribution, an advanced stage of the primary tumor.
• The synchronous group :– indicate a more disseminated disease status – a shorter disease-free survival than metachronous metastasis.
• Most treatment failures are due to :– local hepatic recurrences– lung metastases
• occur within the first 2 years => may need more aggressive chemotherapy ?!
Clinicopathological features and prognosis in resectable synchronous and metachronous colorectal liver metastasis Ann Surg Oncol. 2007 Feb;14(2):786-94

6
Neoadjuvant or adjuvant chemotherpay
• Potential advantages of preoperative CT:– Earlier treatment of micrometastatic disease– Determination of responsiveness to chemotherapy
(as a prognostic factor and postoperation treatment) • Disadvantages : – liver steatohepatitis and sinusoidal liver injury (irinotecan-
and oxaliplatin-based chemotherapeutic regimens)– missing the “window of opportunity” for resection – achievement of a complete response, thereby making it
difficult to identify areas for resection.

7
• Method: – Patients: eligible for complete resection of liver
metastasis. (n=171) – Randomised sugery alone or combine with
adjuvant chemotherapy. – Follow up time: 87m.
• Chemo-regiment: – Leucovorin 200 mg/m2 bolus then – 5-FU 400mg/m2, QD x 5days, monthly, 6 cycles.
Multicenter Randomized Trial of Adjuvant Fluorouracil and Folinic Acid Compared With Surgery Alone After Resection of Colorectal Liver metastases: FFCD ACHBTH AURC 9002 Trial 2006 JCO

8
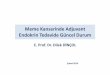
• DFS: 5-y-s: 33.5% vs 26.7% (P=0.028 )• OS : 5-y-s: 51% vs 41% , (P=0.13)
Multicenter Randomized Trial of Adjuvant Fluorouracil and Folinic Acid Compared With Surgery Alone After Resection of Colorectal Liver metastases: FFCD ACHBTH AURC 9002 Trial 2006 JCO
P=0.028P=0.13
Disease free survival Overall survival

9
• Conclusion: – Adjuvant intravenous systemic chemotherapy (5-
FU+ LV) provided a significant disease-free survival.
Multicenter Randomized Trial of Adjuvant Fluorouracil and Folinic Acid Compared With Surgery Alone After Resection of Colorectal Liver metastases: FFCD ACHBTH AURC 9002 Trial 2006 JCO

10
• Method: – 98 patients with four or more colorectal hepatic
metastases were resected. – Neoadjuvant C/T: 57%. 5-FU+ LV, (irinotecan 48% ,
oxaliplatin 12%) – Adjuvant: 92%.
Outcome After Hepatectomy for Multiple (Four or More)Colorectal Metastases in the Era of E ective Chemotherapy ff2007 Annals of Surgical Oncology

11
• Actuarial 5-year survival was 33%.
• Long-term survival can be achieved after resection of multiple colorectal metastases; however, because most patients will experience recurrence of disease, effective adjuvant therapy and close follow-up is necessary.Outcome After Hepatectomy for Multiple (Four or More)
Colorectal Metastases in the Era of E ective Chemotherapy ff2007 Annals of Surgical Oncology

12
• 278 patients(CT:138, S:140), complete resection of liver or lung metastasis. – FFCD- Leucovorin 200 mg/m2 bolus then 5-FU 400mg/m2, QD x 5days, monthly, 6 cycles– ENG trial: Leucovorin 100mg/m2, then 5-FU 370mg/m2, QD x 5days, monthly, 6 cycles
Adjuvant Chemotherapy After Potentially Curative Resection of Metastases From Colorectal Cancer: A Pooled Analysis of Two Randomized Trials 2007 Annals of Surgical Oncology 2008 JCO.

13
Adjuvant Chemotherapy After Potentially Curative Resection of Metastases From Colorectal Cancer: A Pooled Analysis of Two Randomized Trials 2007 Annals of Surgical Oncology 2008 JCO.
Conclusion: marginal statistical significance in favor of adjuvant chemotherapy with an FU bolus–based regimen after complete resection of colorectal cancer metastases

14
• 364 patients with resectable liver metastases from colorectal cancer.– Randomised 182 patients in perioperative
chemotherapy group, 182 in surgery group.– Regimen: FOLFOX4 6cycles before and after
surgery.
Perioperative chemotherapy with FOLFOX4 and surgery versus surgery alone for resectable liver metastases from colorectal cancer (EORTC Intergroup trial 40983): a randomised controlled trial 2008 Lancet

15
• Perioperative chemotherapy with FOLFOX4 is compatible with major liver surgery and reduces the risk of events of progression-free survival in eligible and resected patients.
Perioperative chemotherapy with FOLFOX4 and surgery versus surgery alone for resectable liver metastases from colorectal cancer (EORTC Intergroup trial 40983): a randomised controlled trial 2008 Lancet

16
• 306 patients, completely resectable liver-limited metastases colorectal cancer. – FA, 400 mg/m2 infused over 2h– 5-FU as a 400 mg/m2 i.v. bolus– 5-FU continuous infusion, 2400 mg/m2 over 46 h. • with or without irinotecan: 180 mg/m2 infusion
(FOLFIRI)
A randomized phase III study comparing adjuvant 5-fluorouracil/folinic acid with FOLFIRI in patients following complete resection of liver metastases from colorectal cancer2009 Annals of oncology

17
• Conclusion: FOLFIRI in the adjuvant treatment of LMCRC showed no significant improvement in DFS compared with LV5FUs.
A randomized phase III study comparing adjuvant 5-fluorouracil/folinic acid with FOLFIRI in patients following complete resection of liver metastases from colorectal cancer2009 Annals of oncology

18
• Between 2000 and 2007, in Taipei Veterans General Hospital hospitalization.
• 52 patients having undertaken resection of metachronous colorectal liver disease with curative intent.– 31 patients: FOLFOX or FOLFIRI x 6-12 cycles– 19 patients: 5-FU/leucovorin (LV)-based
chemotherapy.
Adjuvant oxaliplatin- or irinotecan-containing chemotherapy improves overall survival following resection of metachronous colorectal liver metastases 2010 Int J Colorectal Dis

19
• Conclusions: Adjuvant FOLFOX/FOLFIRI chemotherapy following resection of metachronous CLMs is demonstrated to have better DFS and OS than 5-FU/LV chemotherapy.
Adjuvant oxaliplatin- or irinotecan-containing chemotherapy improves overall survival following resection of metachronous colorectal liver metastases 2010 Int J Colorectal Dis

20
Ongoing trial
• HEPATICA study– two-arm, multicenter, randomized, comparative
efficacy and safety study.– Randomized after resection or resection combined
with RFA– CT: CAPOX + Bevacizumab or CAPOX alone– Follow up 5yrs– The primary endpoint : disease free survival. – Secondary endpoints are overall survival, safety and
quality of life

21
• Arm A (CAPOX+Bevacizumab) consists of – 8 cycles of CAPOX (either all cycles postoperatively
or 3 cycles preoperatively followed by 5 cycles postoperatively)• Oxaliplatin: 130 mg/m2, day 1, every 3 weeks• Capecitabine: orally ,1000 mg/m2 twice-daily. Day1-14,
every 3 weeks.• bevacizumab at 7.5 mg/kg, maximum of 48 weeks.
• Arm B : CAPOX only.

22

23

24
Thanks for your attention~
Recommended