CLICK TO ADD TITLEPricing and Patient Access Framework to Support Better Access to Medicines
March 22nd 2017
Organised by Thematic Working Group on Medicines in Health Systems
Contact for questions
Raja Shankar – [email protected]
Maya Malarski – [email protected]

Presenters:
Suthira TaychakhoonavudhChulalongkorn University
Rungpetch SakulbumrungsilChulalongkorn University
Raja ShankarQuintilesIMS
Maya MalarskiImperial College London
Panelists:
Surachat NgorsurachesSouth Dakota State University
Meet & Greet

Housekeeping Rules
To keep the technical process simple, we will not be using webcams for this session
Please keep your microphones “Muted” while listening to a presenter to avoid background noise during the session
Please submit your questions and comments through the Questions Box at the bottom of the GoToWebinarcontrol panel. You can submit questions at any point during the webinar
You can also ask questions verbally, to do so, please press Hand Rise Icon on the left side of the GoToWebinar control panel. This will allow us to keep track on sequence
Panelists/presenters will collect all questions submitted by you during the session
In case you did not get answer on your question during the live session, panelists will get back to you later via email
In case of technical problems, please write to [email protected]
Please complete the post-webinar survey

• Introduction - 5 mins
• Presentation – 20 mins
o Raja Shankar
o Maya Malarski
• Panel Response to Main Questions – 10 min
o Moderated by Raja Shankar
o Rungpetch Sakulbumrungsil
o Suthira Taychakhoonavudh
o Surachat Ngorsuraches
• Open Q&A with Panel – 23 minutes
o Moderated by Raja Shankar
o Rungpetch Sakulbumrungsil
o Suthira Taychakhoonavudh
o Surachat Ngorsuraches
• Close – 2 mins
o Maya Malarski
Agenda

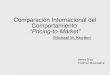
Global penetration 5 years from launch (population on drug as % of total global
prevalent patient population)*
Sources: World Bank, IMS MIDAS, World Cancer Research Fund, “Epidemiology of atrial fibrillation: European perspective” by Zoni-Berisso, Lercari,
Carazza, Domenicucci, Centers for Disease Control and Prevention
700,000anti-TNF patients
out of all RA
patients
40,000patients out of
400,000
HER2+
trastuzumab10%
1.5mNOAC patients out of
all SPAF and VTE
patients
NOACs
Anti-TNFs
<5%
<5%
*Assumes 100% compliance and incidence rates similar across all countries
Globally, innovative medicines reach
<10% of patients five years after launch

In developing countries, they reach less
than 1%
Developing country penetration 5 years from launch (population on drug as % of
total global prevalent patient population)*
Herceptin,
NOACs,
anti-TNFs
average
<1%
Sources: World Bank, IMS MIDAS, World Cancer Research Fund, “Epidemiology of atrial fibrillation: European perspective” by Zoni-Berisso, Lercari,
Carazza, Domenicucci, Centers for Disease Control and Prevention
*Assumes 100% compliance and incidence rates similar across all countries
While this is due to many causes; a structured Pricing and Patient Access [PPA]
System can improve access to medicine, especially with Universal Coverage

There are three major considerations
when reforming PPA systems
Three main elements of the framework:
Objective Setting
Price & Access
System (Technical)
Reform Process

A PPA system helps health systems
prioritize competing access to medicine
objectives within their budgets
Ob
jec
tive
Se
ttin
g
Even the richest systems cannot achieve all objectives perfectly; each system must decide the right balance between its priorities
Provide access to all medicines
Incentivise continuing innovation in unmet need areas
Achieve equal access for all patients
Ensure quality standards
Assure reliable supply of medicines
0
2
4
6
8
10
12
14
16
18
20
Equity
Quality
Supply
security
Sustaining
innovation
Maximising
access
Rational
use of
medicines
US Germany UK Brazil India Thailand
Ensure appropriate medicine choice
and utilisation
*Size of line indicates relative budget amount

Pric
e &
Ac
ce
ss S
yst
em
(Te
ch
nic
al)
PPA systems must evaluate and prioritize
two different product types
Patented
(innovative or therapeutically
equivalent)
Generic
(low competition, low/high volume)
• New patented product, typically represents unique and/or high clinical value; e.g., Sovaldi and Herceptin at time of launch
• No easily comparable price benchmark exists
• New patented product, 2nd or later to market with similar MoA or therapeutic benefit, e.g. anti-TNFs, DPP4s or ACEi/ARBs
• Comparable price benchmark exists if previous one reimbursed; limited price competition also possible
• However, not completely substitutable due to possible minor differences in outcomes overall or in different patient types
• Off-patent product, but not completely substitutable between brands due to delivery mechanisms, e.g., asthma inhalers
• Price benchmarks available and limited price competition possible
• Generics with low volume use; market can only sustain 1-2 manufacturers, e.g., injectable antibiotics for MRSA
• Price benchmark exists; but price competition infeasible as manufacturers need sustainable return on investment in supply
• Generic with high volume use and can sustain multiple competitors, e.g., metformin, enalapril
• Price benchmarks available and price competition possible

Pric
e &
Ac
ce
ss S
yst
em
(Te
ch
nic
al)
Payers predominantly take one of three
approaches to set price and access for
these products
Clinical EffectivenessSet price and access based on extent of incremental clinical
benefit over SoC
Cost EffectivenessConsider both
incremental value and incremental cost to set
price and access
Budget OptimisationSet price and access to
minimise (incremental*) budget impact
Clinical value Cost
Driver of Pricing and Patient Access Decision
DE FR IT (N)
USA
IT (R) CA AUS
SK UK
IT (R) CA (P) UK (CCG)
SA IN BR
ID MEX
N = National, R = Regional, P = Provincial, CCG = Clinical Commissioning Group, SoC = Standard of Care
While one approach predominates, countries may use others as secondary
1 2 3
BR NZ
MAL
* For new products only
MAL
All others for generics

Pric
e &
Ac
ce
ss S
yst
em
(Te
ch
nic
al)
The suitable PPA approaches depend on
product type...
Clinical Effectiveness Cost Effectiveness Budget Optimisation
Clinical value Cost
1 2 3
Generic (low competition, low/high volume)
Patented (innovative/ therapeutically equivalent)
Most payers use health technology assessment (HTA) to understand the value new patented products bring
Some payers primarily focus on minimising budget impact even for new products; however, they still indirectly
consider the outcomes of HTA done by others (either national payers in their countries, or even the assessments
done by HTA bodies such as NICE in other countries)
Generics have already undergone HTA; therefore most payers use them to
free up resources to invest
in new products
Driver of Pricing and Patient Access Decision

...and are executed with an array of
different pricing tools
Pric
e &
Ac
ce
ss S
yst
em
(Te
ch
nic
al)
Patented
Generic
Clinical HTA Cost per QALY/DALY
Price volume / financial risk share agreements
Pricing based on value added services beyond drug
Therapeutic referencing
Market driven pricing
Performance based / outcome risk share
International reference pricing
Negotiated confidential discounts/rebates/free goods
Tenders
Mandated price cuts
Cost Effectiveness
Clinical value Cost
1 2 3Clinical Effectiveness Budget Optimisation
Driver of Pricing and Patient Access Decision

In Thailand, we recommended 3 steps to
set price and access for medicines
Pric
e &
Ac
ce
ss S
yst
em
(Te
ch
nic
al)
Determine Product Type
Apply HTA/ Pricing Tools
• Determine if product is patented or generic• For generics, determine if existing generic or if product
losing exclusivity
• Determine if/what type of HTA to perform based on product type
• Apply pricing and access tools based on outcome of HTA
Innovative Solutions• If a reasonable price cannot be achieved in step 2, use
innovative pricing and access techniques to achieve desired outcome
1
2
3

Recommended PPA Framework for
Thailand
Pric
e &
Ac
ce
ss S
yst
em
(Te
ch
nic
al)
IRP: International Reference PricingLoE: Loss of ExclusivitySoC: Standard of CareTRG: Therapeutic Reference Group
Central / Regional Tender or Negotiation
Product Type
Patented
Generic
Existing Generic
New Generic
≥3 CompetitorsHigh Volume
<3 CompetitorsLow Volume/ Complex
≥3 CompetitorsHigh Volume
<3 CompetitorsLow Volume/ Complex
Level 1
Level 2
Level 3
Level 4
Level 5
≤3 in TRG
>3 in TRG
High unmet Need
Low unmet Need
Inpatient: Current procurement system in the short term
+IR
P+
Inte
rna
tio
na
l Re
fere
nc
e P
ric
ing
+R
atio
na
l Use
Gu
ide
line
s b
ase
d o
n c
linic
al a
nd
e
co
no
mic
co
nsi
de
ratio
ns+Ti
me
in M
ark
et
Dis
co
un
t2
-5%
pe
r ye
ar
aft
er 2
ye
ars
Max. Procurement Price Reimbursement Price
Reimbursement Price
SH
OR
T TE
RM
LON
G T
ER
M
Set the procurement reference price based on median price of products with ≥10% market share or of the 4-5 top products by volume
Central / Regional Tender
Central / Regional Tender
40% discount from brand price (based on max. procurement price)at LoE, next two entrants priced at further 10% discounts
Cost Effectiveness-based negotiation
Alternative Funding Solutions
+
Cost Effectiveness-based negotiation
Negotiate with manufacturer or wait for more data
Not recommended for listing until clinical benefit can be demonstrated
Reimbursement Price: Price that central procurer pays for product including taxes and margins
Max. Procurement Price: Maximum price at which hospitals can currently procure products excluding hospital margins
10% discount from previous entrant for the 2nd and 3rd
entrants If high budget impact renegotiate after 2 years
Central / Regional Tender

PPA for generics largely driven by
harnessing competitive forces
Pric
e &
Ac
ce
ss S
yst
em
(Te
ch
nic
al)
Generic
Existing Generic
New Generic
Central / Regional Tender or Negotiation
≥3 CompetitorsHigh Volume
<3 CompetitorsLow Volume/
Complex
≥3 CompetitorsHigh Volume
<3 CompetitorsLow Volume/
Complex
Inpatient: Current procurement system in the short term
+IR
P
Max. Procurement Price Reimbursement Price
SH
OR
T TE
RM
LON
G T
ER
M
Set the procurement reference price based on median price of products with ≥10% market share or of the 4-5 top products by volume
Central / Regional Tender
Central / Regional Tender
40% discount from brand price (based on max. procurement price)at LoE, next two entrants priced at further 10% discounts
+IR
P
Generic
Existing Generic
New Generic
Central / Regional Tender or Negotiation
≥3 CompetitorsHigh Volume
<3 CompetitorsLow Volume/
Complex
≥3 CompetitorsHigh Volume
<3 CompetitorsLow Volume/
Complex
Inpatient: Current procurement system in the short term
+IR
P
Max. Procurement Price Reimbursement Price
SH
OR
T TE
RM
LON
G T
ER
M
Set the procurement reference price based on median price of products with ≥10% market share or of the 4-5 top products by volume
Central / Regional Tender
Central / Regional Tender
40% discount from brand price (based on max. procurement price)at LoE, next two entrants priced at further 10% discounts
+IR
P
IRP: International Reference PricingLoE: Loss of ExclusivitySoC: Standard of CareTRG: Therapeutic Reference Group
Reimbursement Price: Price that central procurer pays for product including taxes and margins
Max. Procurement Price: Maximum price at which hospitals can currently procure products excluding hospital margins

Pric
e &
Ac
ce
ss S
yst
em
(Te
ch
nic
al)
Incremental Benefit over SoC Level of unmet need Public health importance
• Extent of additional clinical
benefit over standard of care
Influencing elements:
− Extent of benefit -efficacy, safety, QoL
− Strength of evidence –trial design (head to head vs. placebo vs. single arm trials), size of trials, duration of trials,
patient inclusion criteria
• Extent of patient and
caregiver unmet need
Influencing elements:
− Mortality
− Morbidity
− Quality of Life (QoL)
− Patient economic and social impact
− Caregiver burden
− Number and quality of available alternative treatments
• Extent of benefit to the
broader population and health system
Influencing elements:
− Number of people directly and indirectly affected by the condition
− Total health system resources consumed
− Economic burden to
society
− Preventive effect
1 32
Description of each factor
For patented medicines, we must first
assess incremental benefit based on
three factors

Pric
e &
Ac
ce
ss S
yst
em
(Te
ch
nic
al)
The level of benefit should be determined
through an integrated assessment of
these factors
Level 1
Level 2
Level 3
Level 4
Level 5
Lev
el o
f b
en
efit
Incremental Benefit over SoC
Level of unmet need
Public health importance
Example
VerySubstantial
High - Very High High – Very High Prevenar
Substantial –Very
SubstantialHigh - Very High High Sovaldi
Substantial Moderate - High Moderate - High Zytiga
Slight or Same N/A N/A Tradjenta
Unquantifiable High or Low High or Low Bosulif/Glybera
1 32
Level of benefit recommended to be determined by an expert committee from the NLEM and/or
NHSO with clinical experts appointed for each appropriate therapy area

Pric
e &
Ac
ce
ss S
yst
em
(Te
ch
nic
al)
IRP: International Reference PricingLoE: Loss of ExclusivitySoC: Standard of CareTRG: Therapeutic Reference Group
Reimbursement Price: Price that central procurer pays for product including taxes and margins
Max. Procurement Price: Maximum price at which hospitals can currently procure products excluding hospital margins
+IR
P
Patented
Level 1
Level 2
+R
atio
na
l Use
G
uid
elin
es
ba
sed
on
clin
ica
l an
d e
co
no
mic
co
nsi
de
ratio
ns
+Ti
me
in M
ark
et
Dis
co
un
t2
-5%
pe
r ye
ar
aft
er
2
ye
ars
Reimbursement Price
Cost Effectiveness-based negotiation
Alternative Funding Solutions
+
Negotiation strategies:• Confidential price-volume
agreements• Risk-sharing• Discounts/ rebates
Alternative strategies:• Restrict to sub-populations • Innovative funding solutions:− High value, high cost drugs fund− Additional funding sources− Co-payments− Added services
• Increase cost effectiveness threshold
Products with high clinical benefit can
undergo cost effectiveness analyses to
help negotiate price and access

Pric
e &
Ac
ce
ss S
yst
em
(Te
ch
nic
al)
Negotiation strategies:• Confidential price-volume
agreements• Risk-sharing• Discounts/ rebates
Patented Level 3 Cost Effectiveness-based negotiation +IR
P
+R
atio
na
l Use
G
uid
elin
es
ba
sed
on
clin
ica
l an
d e
co
no
mic
co
nsi
de
ratio
ns
+Ti
me
in M
ark
et
Dis
co
un
t2
-5%
pe
r ye
ar
aft
er
2
ye
ars
IRP: International Reference PricingLoE: Loss of ExclusivitySoC: Standard of CareTRG: Therapeutic Reference Group
Reimbursement Price: Price that central procurer pays for product including taxes and margins
Max. Procurement Price: Maximum price at which hospitals can currently procure products excluding hospital margins
For products with substantial clinical
benefit CE analyses and negotiation can
help to set price levels

Pric
e &
Ac
ce
ss S
yst
em
(Te
ch
nic
al)
+IR
P
Patented Level 4
≤3 in TRG
>3 in TRG
Reimbursement Price
10% discount from previous entrant for the 2nd and 3rd entrants If high budget impact renegotiate after 2 years
Central / Regional Tender
+R
atio
na
l Use
Gu
ide
line
s b
ase
d o
n c
linic
al a
nd
ec
on
om
ic c
on
sid
era
tio
ns
IRP: International Reference PricingLoE: Loss of ExclusivitySoC: Standard of CareTRG: Therapeutic Reference Group
Reimbursement Price: Price that central procurer pays for product including taxes and margins
Max. Procurement Price: Maximum price at which hospitals can currently procure products excluding hospital margins
Therapeutic reference pricing can be
used for products with comparable
clinical benefit to SoC

Patented Level 5
High unmet Need
Low unmet Need
Reimbursement Price
Negotiate with manufacturer or wait for more data
Not recommended for listing until clinical benefit can be demonstrated
Access Strategies:• Negotiate with manufacturer for
an interim price• Conditional access agreement for
prioritized products
+IR
P
+R
atio
na
l Use
Gu
ide
line
s b
ase
d o
n c
linic
al a
nd
ec
on
om
ic c
on
sid
era
tio
ns
IRP: International Reference PricingLoE: Loss of ExclusivitySoC: Standard of CareTRG: Therapeutic Reference Group
Reimbursement Price: Price that central procurer pays for product including taxes and margins
Max. Procurement Price: Maximum price at which hospitals can currently procure products excluding hospital margins
Products with an unquantifiable clinical
benefit can be listed if high unmet need,
otherwise wait to grant access
Pric
e &
Ac
ce
ss S
yst
em
(Te
ch
nic
al)

IRP should be applied to:
Patented Products and...
...Low Volume Generics
Competitive forces are sufficient to address pricing for high volume generics
Through a 3 Step Process:
1. Select reference basket
2. Select price to reference
3. Set price ceiling depending on product type:a. Marketed Patented Medicines
and Low Volume Genericsb. New Patented Medicines
IRP is only one tool to set ceiling price; further discounts can be negotiated based on the overall PPA framework and tools discussed above
International Reference Pricing (IRP) can
be used as an additional safeguard to
achieve a fair price
Pric
e &
Ac
ce
ss S
yst
em
(Te
ch
nic
al)

PPA system implementation needs to
address four areas to ensure a successful
transition
Re
form
Pro
ce
ss
1 2
3 4
Awareness Building Institutional Change
Stakeholder Buy-in Capability Building

Discussion & Questions
Panelists
• Rungpetch C. Sakulbumrungsil - Chulalongkorn University, Thailand
• Suthira Taychakhoonavudh - Chulalongkorn University, Thailand
• Surachat Ngorsuraches - South Dakota State University, USA
Questions
1. What challenges in medicine access as part of universal coverage, led NHSO
to seek advice on pricing and patient access reform?
2. What were the major lessons from the project process that could be relevant
for other countries undertaking similar efforts?
3. What are some of the implementation challenges going forward?

Thank you
Acknowledgements

www.healthsystemsglobal.org
Recommended