CORSO PER GIOVANI INFETTIVOLOGI SULLA TUBERCOLOSI BRESCIA 16-18 GIUGNO
LA DIAGNOSI DI TUBERCOLOSI
D Cirillo
San Raffaele Scientific Institute
Milan Italy

Outline
• Urgent need for an improved diagnosis
• Microscopy
• Culture and DST needs for standards and EQAs
• Molecular diagnosis is a reality
• What can be achieved with current molecular tools
• What cannot be achieved with the current molecular tools
• Diagnosis of infection: current tests and open issues

Urgent need for new diagnostics
• TB case detection gaps:
– cases undiagnosed
• Inaccessible facilities
• Not self reporting, not returning
• Wrong diagnosis
– Cases diagnosed in private care and not reported
• Infection control (Stop TB/MDR-TB transmission)
• Guide treatment
• Monitoring treatment

TB epidemiology in a low burden country
72%
*
* Provisional data

An accurate diagnosis starts from
– Good selection and quality of the diagnostic specimen
– Appropriate transport
– QA laboratory
– Clear reporting and understanding of the limitations of laboratory data

Rapid test
Inexpensive
Specificity for Mycobacterium spp:
>95%
Sensitivity: 25-65% (90 % of higly
infectious cases)
Positive Predictive Value for TB
depends on epidemiological situation 1st AFB smear 80-82 %
2nd AFB smear 10-14 %
3rd AFB smear 5-8 %
Fluorescence Ziehl-Neelsen staining
Does not allow species identification
Not applicable to all samples
Microscopy : a century old procedure
LED microscopy recommended over light and fluorescent microscopy

Advantages
• Definitive diagnosis of TB
• Increases case finding of 30-50%
• Early detection of cases
• Provide strains for DST and epidemiological studies
Disadvantages
• Complex and expensive compared to microscopy
• Requires complex handling of specimens
• Skilled technicians
• Appropriate infrastructure and biosafety levels
LIMITATIONS: need for decontamination and identification
*coverage 500.000/1000000
TB Culture

solid • Low cost for reagents, not
automated
• Culture level infrastructure
• Low contamination rate
• Long time to positivity
• Colony morphology
• ID required
• DST only for selected drugs
liquid
• Complex and expensive can be automated (MGIT)
• Highest infrastructure and biosafety levels
• Case finding increased 10% over solid
• Diagnostic delay reduced to days
• ID required
• DST only for selected drugs
Strip speciation tests for fast ID of Tbcomplex
Molecular test for speciation of most common mycobacteria
Culture: solid/ liquid

Morphology/Biochemical
tests
Molecular tests
LPAs
Probes on liquid phase
Sequencing
Spoligotyping
Enzyme restriction
Immuno- cromatographic
test
9
M. tuberculosis identification
EQA and standardization

• Definitive diagnosis of DRTB
3 main methods
Absolute concentration
method
Proportion methods Resistant Ratio
method
DST

Current DST reliable for:
• Rifampicin
• Isoniazide
• FQs
• AGs
• Injectables
• Other drugs: results suboptimal

Advantages compared to solid media: • more rapid • high quality of media • fully automated system • testing of 1st, 2nd , and new drugs (Linezolid) • safety: plastic tubes • pyrazinamide sensitivity test Disadvantages: • expensive • higher contamination rate • dependency on a company • no DST for Cycloserine
Liquid media compared to solid media
Break points for 2nd line drugs recently revised Still poor correlation with clinical outcome, some testing not fully reliable
DST: Liquid/solid media comparison


SENSITIVITY OF CURRENT DIAGNOSTICS
0 1 2 3 4 6
Log cfu/ml
5
Automated NAAT 100-
150/ml
Solid Culture
100-1000/ml
Liquid Culture 10-100/ml
LAMP-TB 100-1000/ml
Fluorescent/LEDmicroscopy 5,000-
10,000/ml Immunochrom.f
or speciation 1,000,000/ml
Line-Probe Assay 1000-10,000/ml

Is new real-time technology improving the sensitivity of
molecular tests?

Other molecular tests
Tortoli et al 2012 JCM
Taqman vs Amplicor on 15000 samples Improvement in specificity Decrease in invalid results Improvement in post test probability
Methods based on on NAs detection have intrinsic limitations: • Absence of target: suboptimal specimen selection, quantity,
quality,.. • Suboptimal sample preparation

Are molecular tests tools for difficult to diagnose cases?
• TB in Children
• Extrapulmonary Tuberculosis

Diagnosis in difficult cases
• Children diagnosis is not microbiologically confirmed in 40-60% of cases, current molecular tools still suboptimal. A host/pathogens biomarkers approach is probably needed
• Extrapulmonary TB: the performance of molecular tools varies and should be considered separately for each specific specimen type.
• Suboptimal sensitivity/specificity versus a gold standard:
– Compared to culture in liquid media
– Compared to a combined standard based on the “intention to treat”/ response to treatment
Unsolved Problems of Molecular Tests for Direct Diagnosis of
Tuberculosis
Decreased confidence in the test

• Adequate infrastructures and biosefety levels
• MGIT DST: the gold standard
• MDRTB : 3-6 weeks; XDRTB : 6-9 weeks
• Reproducibility and accuracy of results are drugs dependent: – Rifampicin, isoniazid : good results
– Second-line: fluoroquinolones and injectables
Van Deun A. et al 2011. IJTLD 15(1):116-124
Correlation of sensitivity test results and clinical outcome is difficult to evaluate and we have very limited or no evidence for Pyr,E, and 2nd line drugs other than INJ and FQs on MDR cases
Conventional DST: technical challenges
In addition: Capital cost of facilities Cost of maintenance Cost of staff

Zhang Y and Yew W, Int J Tuberc Lung Dis 2009
MECHANISMS OF DRUG RESISTANCE IN M. tuberculosis

WHO Global plan (2006-2015):development and roll out of new technologies to be adopted in
resources-limited settings
GenoType MTBDRplus, InnoLiPA Rif.TB
•Reverse hybridization, colorimetric reaction
•Results in 6-7 h
• some flexibility (n probes/strip: 30-40)
• Technical expertise: some
•Biosafety lev 2 Xpert MTB/RIF
•Integrated/automated qPCR
•Results in 2h
•Closed system (limited number of probes: <10)
• Technical expertise: none
Commercial Molecular tests for TB/MDR TB detection endorsed by
WHO

Morgan M et al 2005. BMC Infect Dis 5:62 Ling DI et al 2008. Eur Respir J 32:1165-1174 Ling DI et al 2008. Eur Respir J 32:1165-1174
Hot-spot rpoB gene cod. 315 katG gene nt -8,-15,-16 inhA gene
Inno-LiPA Rif.TB GenoType MTBDRplus GenoType MTBDRplus*
LPAs: performances (*based on 2° generation)
Rifampicin Isoniazid
Sensitivity 95-98% Specificity 98-100%
Sensitivity 95-99% Specificity 97-100%
Sensitivity 82-93% Specificity 95-100%
Dec. clin. spec. (AFB-pos) Sensitivity 72-92% Specificity 96-99%
Decontaminated clinical specimens (AFB-positive) Sensitivity 95-99% Specificity 97-99%
LPA performance in isolates and clinical samples

Boehme CC et al 2011. Lancet 377(9776):1495-505
RIF-R detection Time to report to treatment center
Xpert MTB/RIF: 0-1 d
LPA: 10-26 d*
Culture DST: 30-124 d**
Xpert MTB/RIF: 0-1 d (Microscopy: 1-2 d)
LPA: 27-53 d*
Culture DST: 38-102 d** (culture: 42-62 d)
Some results not reported/lost
* test on AFB-pos clinical specimen + test on clinical isolate for AFB-neg cases ** DST performed by MGIT + DST performed on LJ
TAT to Rif –R detection and reporting

What can be achieved or partially achieve with the current molecular tools
• Diagnosis of TB, rifampicin resistant TB, MDR-TB in smear positive/negative samples
• Identification of up to 80% fluoroquinolones and up to 40-80% of injectable resistant cases among MDR-TB cases
• Improvement of diagnosis of TB in extrapulmonary samples
• Support to diagnosis of TB in children
• Diagnosis of NTMs infection

Bactericidal antibiotic that inhibits the bacterial DNA-dependent RNA polymerase. Target: β-subunit of the RNA polymerase (encoded by rpoB), blocking elongation of the RNA chain.
Mutations in a “hot-spot” region of 81 bp of rpoB gene (Rifampin resistance-determining region) → RIF resistance (> 95%)
codon 526/ 531 high level resistance to rifampicin, rifabutin e rifapentin 516 e 522 high PPV for rifabutin res
DR testing: Rifampicin

Mutations in KatG gene prevent INH activation (cod. 315, 60-90%) Mutations in the direct target inhA (inhA belongs to the family of short-chain dehydrogenases/reductases. It is essential in MTB)
Mutations in the promoter of inhA gene leading to drug tritration (direct target over-production)
INH: targeting mycolic acid biosysthesis
Ratan A et al. EID 1998
ISONIAZID ISONIAZID
Only Kat G 315 and inhA are included in LPA
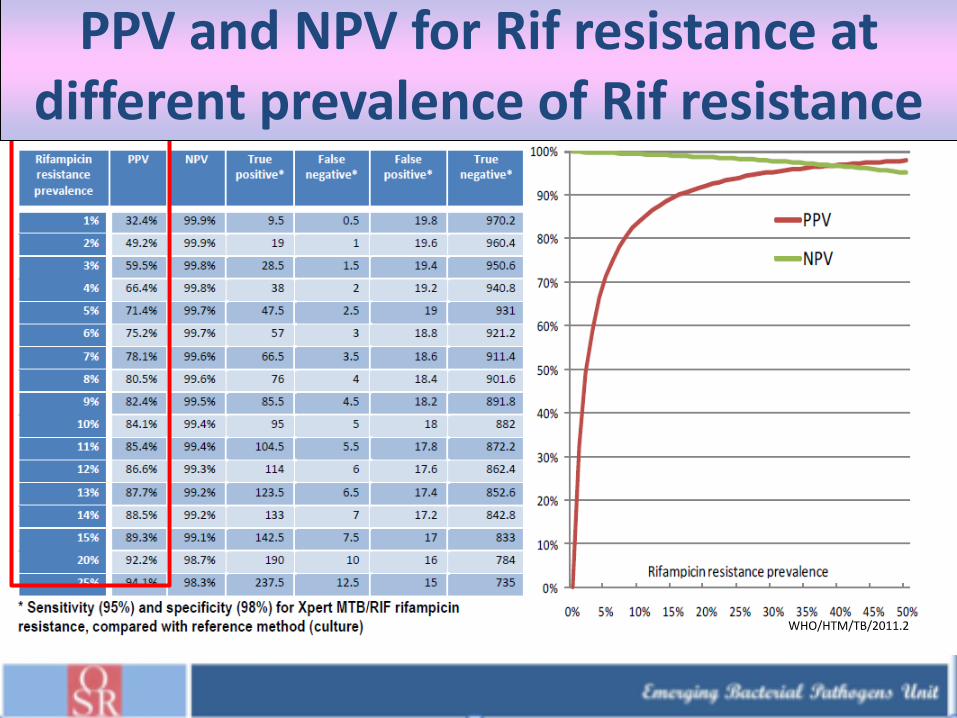
WHO/HTM/TB/2011.2
PPV and NPV for Rif resistance at different prevalence of Rif resistance

Discrepancies with MGIT DST • In vitro growth of Rif sensitive strains from
samples identified as Rif res or MDR by LPA
• Few cases from strains tested by LPA
• rpoB absence of WT8 (codo530-533) and absence of
rpoB MUT3
• Strains bearing the mutations grow slowly in liquid
culture and are identified as Rif sensitive
• inhA mut strains sensitive to INH by MGIT DST
Discordant reports are confusing for patients Management if not appropriately explained

Real heteroresistance
• Co-presence of mutated and wild type population
• Two different strains
False heteroresistance
• Laboratory cross contamination due to insufficient control of amplicons
Heteroresistance
LPAs can detect heteroresistance from clinical strains: clinical role?

• Low sensitivity of embB306 locus for predicting E Res and MDR-TB (35.5%), High specificity for identifying MDR-TB (92.6%; 87/94). The positive predictive value (77.4%; 24/31) and the negative predictive value (66.4%; 87/131) of this locus are moderate.
• Plinke et al AAC 2006, Miotto et al ERJ 2012: higher PPV for E resistance
Role of point mutations in predicting clinical outcome: embB Codon 306
Xin Shen, AAC2007

Commercial tests for Fluoroquinolones and injectables
• Commercial LPA tests for detection of resistance to second line drugs show a high PPV and a low NPV due to the limited number of mutations included in the tests
• PPV and NPV may vary with the genotypic background of the strains and/or with the prevalence of specific genotypes in the target population
Miotto et al. ERJ 2012

• PPV and NPV may vary in different genotypic backgrounds
• High prevalence of specific clones bearing selected mutations not included in current diagnostic assays may modify PPV and NPV
Molecular test performances should be evaluated in the epidemiological contests

• To identify epidemiological links between TB patients to detect and control outbreaks early and rapidly
• Rule out suspected outbreaks and confirm transmission has NOT occurred
• To identify incorrect TB diagnosis based on false-positive cultures and thus avoid unnecessary investigation and treatment
• To distinguish exogenous re-infection from endogenous reactivation in patients with a past history of TB
• Discover unusual transmission settings and transmission between different regions
• Monitor the size of clusters and thus monitor progress towards TB elimination
• Vaccine and DR detection implications
Role of Molecular typing

Needs for better tools
Among 3037 patients with new cases of tuberculosis and 892 with previously treated cases, 5.7% (95% confidence interval [CI], 4.5 to 7.0) and 25.6% (95% CI, 21.5 to 29.8), had multidrug-resistant (MDR) tuberculosis. Among all patients with tuberculosis, approximately 1 of 4 had disease that was resistant to isoniazid, rifampin, or both, and 1 of 10 had MDR tuberculosis. Approximately 8% of the patients with MDR tuberculosis had extensively drug-resistant (XDR) tuberculosis

Tools in different algorithms

• How to monitor the response to therapy? – Sputum smear is still guiding decisions on admission and discharge
– Sputum culture is still the only reliable monitoring tool for MDR patients
• Patients with H monoresistance may go undetected, in R res H should be left until proven R?
• Contact treatment in absence of H sensitivity data
• Discrepancy between phenotypic and genotypic results
• Are all the mutations in rpoB equally contributing to resistance?
• Mutations to key second line drugs and cross resistance
• How to report molecular data in order to provide clinical guidance?
Open Issues

• Needs to be performed on good diagnostic specimens
• Needs to follow an appropriate algorithm integrating molecular tests, culture and DST
• Needs to be performed in qualified laboratories following international guidelines
• Current tools are based on detection of MTB and are suboptimal in Children, HIV coinfected and EPTB
Take home message: Diagnosis of TB
IGRAs should not be used in the diagnosis of active TB

(N°31/39)
Xpert29%
Xpert+LPA42%
LPA4%
N°labs
80
40% of laboratory testing
MDR by 2nd line LPA all
MDR tested by DST
9337
5625
New molecular tools for routine diagnosis and drug resistance testing adapted and used in Italy
Other
molecular
tests for ID

Response to TB infection is a continuum
Where is the turning point between latent TB and asymptomatic TB?

Diagnosis of LTBI: Tuberculin Skin Test
100 y old test, a lot of data
But:
• Mix of antigens, cross reacting with BCG
• Low specificity
• Low sensitivity in selected populations
• Operational challenges
• Tuberculin skin test and IGRAs
• measure cellular immune response to mycobacterial (TB ) antigens
• Re-sensitization in-vivo in TST and ex-vivo in IGRAs
• Surrogate markers of MTB infection
• Don’t distinguish TB infection from active TB disease
• Do not predict risk of progression of infection
• No direct evidence of presence of a viable bacilli
• No suitable for monitoring response to therapy
Diagnosis of LTBI: no gold standard

Interferon Gamma Release Assay
• THEORY: T-cells previously
sensitized to TB antigen produce
high levels of IFN-gamma when
re-exposed to the same
mycobacterial antigen.
• Based on the immunological
response of the infected person,
not on detection of any bacterial
antigens
IGRAs

3x1mL blood collection Incubation at 37ºC
for 16-24 hours
Centrifuge tubes for 5
min
IFN- stable
refrigerated for at
least 8 weeks.
Stage One – Blood collection and harvesting
Nil TB Mitogen
QuantiFERON®-Gold In Tube
Option 1: Shipment of the blood collection tubes within 16 hours to a laboratory prior to incubation.
Option 2: Shipment of the blood collection within 3 days after incubation to the laboratory.
Possibility to batch samples.

Software
calculates and
prints results
Add stop-
solution and
read
absorbance
Wash and add
substrate
Incubate for
120min at room
temperature
Add plasma
and conjugate
Stage 2 – Interferon-γ ELISA
QuantiFERON®-Gold In Tube
No need for new equipment.
User-friendly software supplied free-of-charge from Cellestis.
Easy “Standard”-ELISA.

QF-TB Gold: peptides used
7 peptides
ESAT-6
6 peptides
CFP-10
1 peptide
TB 7.7

T-Spot TB
• Blood collected into Vacutainer CPT™ tube
• Tube centrifuged
• Lymphocyte band removed
• Cells washed & counted
• Cells added to 96-well plate
• Antigens added to wells
• Incubate overnight

Step 2 – Detection of spots
• Plate washed
• Add detection reagent for 60
minutes
• Plate washed
• Add substrate; spots in 7 minutes
• Plate washed and dried
• Count spots by “eye” using a
magnifying glass or dissecting
microscope or by automated Elispot
reader
neg
Pos

Quick summary of evidences
• TST specificity is high in BCG non vaccinated, low and variable in BCG vaccinated
• IGRA (QFT>Tspot) have very high sensitivity
• IGRA specificity is higher than TST
• IGRA non affected by BCG vaccination and serial tests
• In low incidence Countries correlate well with markers of exposure
• Sensitivity higher than TST in immunosuppressed patients
• In children correlates better than TST with level of exposure
• In high incidence Countries correlate less than TST with level of exposure
• Low sensitivity in active TB (no rule out, no rule in)
• HIV: Both IGRAs more sensitive than TST but sensitivity

Tests IGRA per LTBI
• Pletora di dati pubblicati non sempre da casistiche controllate
• Specificità in soggetti a basso rischio : 98/100%, progression rate sensibilmente piu alto rispetto al TST su pz seguiti per 2 anni. NPV 88-100%
• Dati considerevolmente diversi in soggetti ad alto rischio. NPV T-Spot 0.94;QTF 0.88
• BCG ininfluente su IGRA

IGRA e HIV
(Stephan et al AIDS 2008)
Comparison of performance of the 2 IGRAs tests in LIS in
IHV positive
286 patients enrolled
Both IGRAs more sensitive than TST but sensitivity lower
than in non HIV
Low concordance between tests
Tspot independent from total CD4

IGRA in children (> 5ys)
• Correlate better that TST to exposure
• The amount of mitogen response correlate
with age

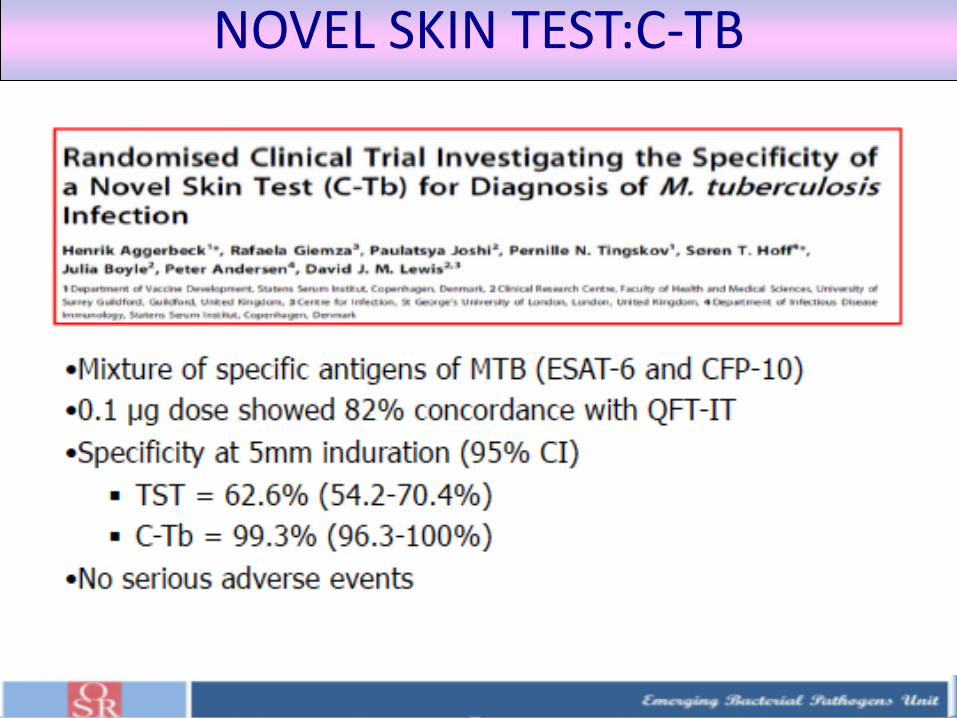
NOVEL SKIN TEST:C-TB

56
Nuovi Biomarkers: dal sito
dell’infezione al sangue periferico
• Citochine
• Metaboliti derivati dal metabolismo micobatterico
• Metaboliti derivanti dalle cellule infettate
• Acidi nucleici ( ospite/ micobatterio)
• T cell activation markers on Mycobacterium
tuberculosis (MTB)-specific T cells C27 by
flow cytometric analysis (expressed differentially
during latent and active Tuberculosis).

Domande a cui rispondere in
futuro • IGRA come “ predittori” di progressione a malattia ( alti
valori di gamma IFN) (cut-off)
• Significato delle conversioni e “retroversioni” e loro
frequenza
• Effetto boosting del TST
• IGRA come “ surrogate markers “ per risposta a terapia
LTBI
• Necessita’ di nuovi biomarkers su piattaforme integrate
da utilizzare come “surrogate end-points per la diagnosi
e valutazione della risposta a nuovi farmaci e nuovi
vaccini

Take home message:LTBI
• IGRA do not distinguish between latent and active
disease
• Do not cross-react with BCG and a large number of
other Mycobacteria
• No sufficient data on small children
• More specific than TST, less sensitive
• TSPOT TB more sensitive in immunocompromised?
• Recommended according to different algorithms in
different guidelines
• Monitoring of health care workers

Conclusions
• Laboratory diagnosis of TB is still
suboptimal due to the absence of ideal
tools
• Being technically demanding and
expensive should:
– Follow National guidelines
– Performed only in designated centers with
high quality standards

New diagnostics?
Nanopore USB sequencing Biomarkers

Riccardo Alagna Emanuele Borroni Andrea M. Cabibbe Irene Festoso Lucinda Furci Paola Mantegani Paolo Miotto Luca Norbis Elisa Schena Enrico Tortoli Elisa Tagliani Ilaria Valente Diego Zallocco
Emerging Bacterial Pathogens Unit WHO Supranational Reference Laboratory for TB Control San Raffaele Scientific Institute Milano, ITALY
Fulvio Salvo and Delek Hospital Staff AISPO
Alberto Matteelli Alberto Roggi and SRL/ NTP Burkina faso
Institute of Infectious and Tropical Diseases University of Brescia Brescia, ITALY
Lanfranco Fattorini Istituto Superiore di Sanità Roma, ITALY
Acknowledgments
GB Migliori FSM,Tradate
Recommended