Priv.-Doz. Dr. med. Michael Kindermann
CaritasKlinikum Saarbrücken, St. Theresia Interventionelle Kardiologie und Angiologie
Echo assessment of
Aortic Regurgitation
and its mechanisms
Homburg, Wednesday, May 14th, 2014
Workshop: Reconstruction of the
Aortic Valve and Root
cts CaritasKlinikum Saarbrücken St. Theresia
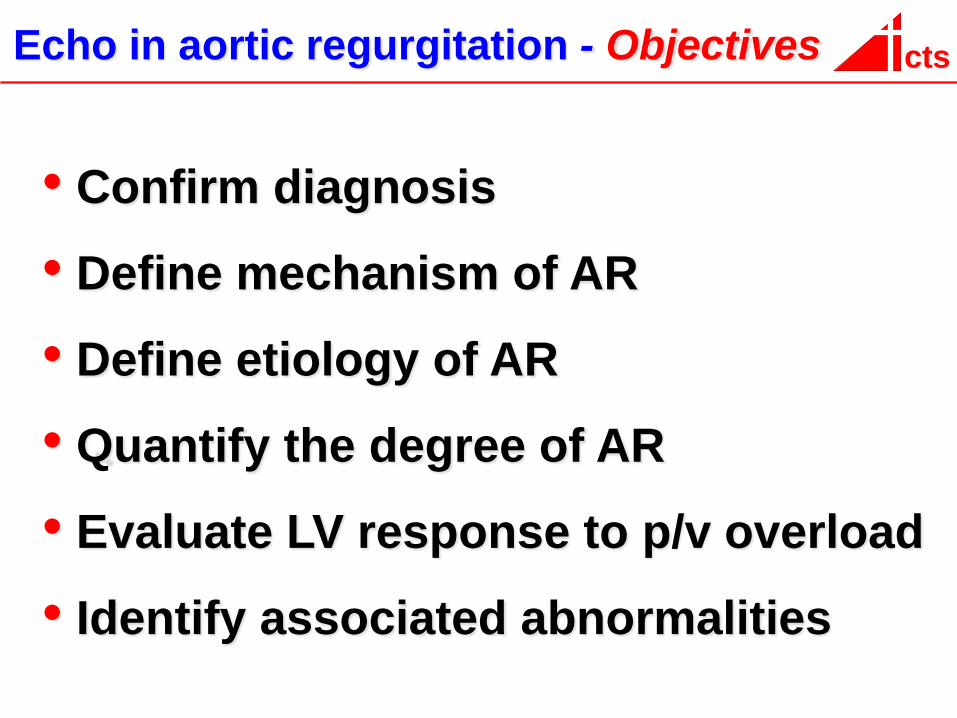
cts Echo in aortic regurgitation - Objectives
• Confirm diagnosis
• Define mechanism of AR
• Define etiology of AR
• Quantify the degree of AR
• Evaluate LV response to p/v overload
• Identify associated abnormalities

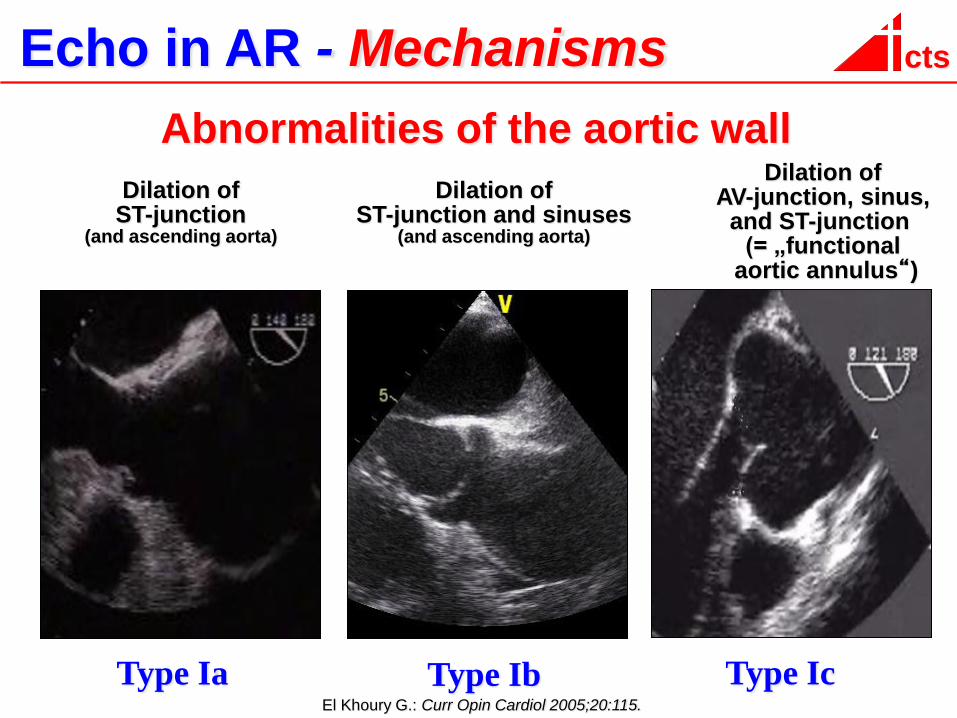
cts Echo in AR - Mechanisms
Type Ia El Khoury G.: Curr Opin Cardiol 2005;20:115.
Type Ib Type Ic
Abnormalities of the aortic wall
Dilation of ST-junction
(and ascending aorta)
Dilation of AV-junction, sinus,
and ST-junction (= „functional
aortic annulus“)
Dilation of ST-junction and sinuses
(and ascending aorta)
cts Echo in AR - Mechanisms
Type Ia El Khoury G.: Curr Opin Cardiol 2005;20:115.
Type Ib Type Ic
Abnormalities of the aortic wall
Dilation of ST-junction
(and ascending aorta)
Dilation of ST-junction and sinuses
(and ascending aorta)
Dilation of AV-junction, sinus,
and ST-junction (= „functional
aortic annulus“)
cts Echo in AR - Mechanisms
Type Ia El Khoury G.: Curr Opin Cardiol 2005;20:115.
Type Ib Type Ic
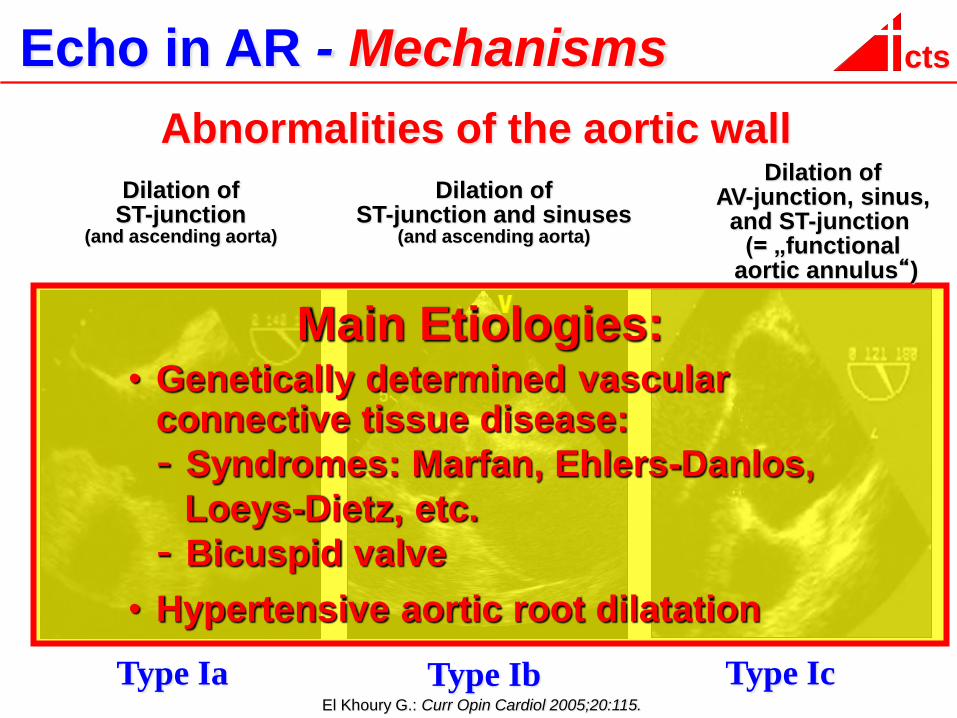
Abnormalities of the aortic wall
Main Etiologies: • Genetically determined vascular connective tissue disease:
- Syndromes: Marfan, Ehlers-Danlos,
Loeys-Dietz, etc.
- Bicuspid valve
• Hypertensive aortic root dilatation
Dilation of ST-junction
(and ascending aorta)
Dilation of ST-junction and sinuses
(and ascending aorta)
Dilation of AV-junction, sinus,
and ST-junction (= „functional
aortic annulus“)
cts Echo in AR - Mechanisms
Dilation of ST-junction and ascending aorta
Dilation of AV-junction, sinus,
ST-junction and ascending aorta
Dilation of AV-junction, sinus,
and ST-junction (= „functional
aortic annulus“)
Type Ia El Khoury G.: Curr Opin Cardiol 2005;20:115.
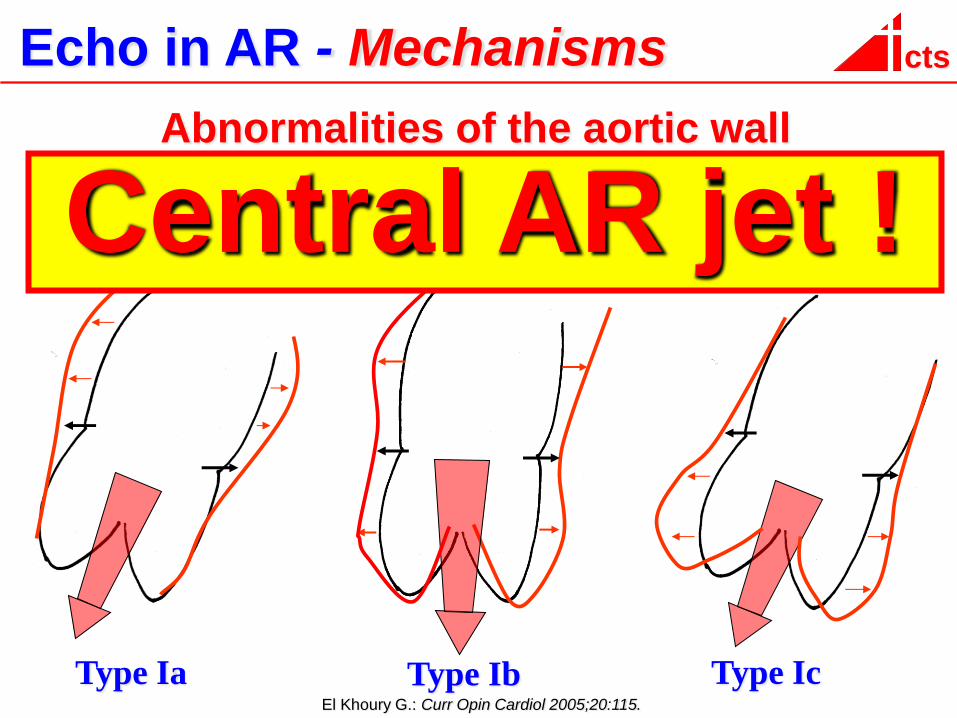
Type Ib Type Ic
Abnormalities of the aortic wall
Central AR jet !

cts Echo in AR - Mechanisms
Abnormalities of the aortic valve cusps
Perforation Prolapse Restrictive cusp motion
Type Id Type II Type III
cts Echo in AR - Mechanisms
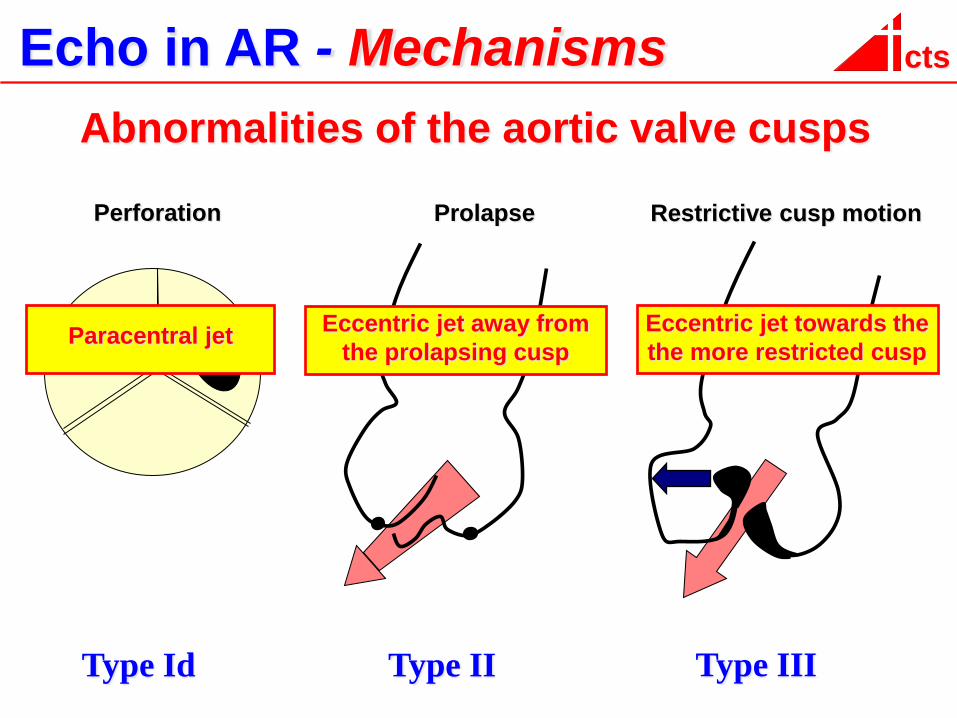
Abnormalities of the aortic valve cusps
Perforation Prolapse Restrictive cusp motion
Eccentric jet away from
the prolapsing cusp
Eccentric jet towards the
the more restricted cusp Paracentral jet
Type Id Type II Type III
cts Echo in AR - Mechanisms
Abnormalities of the aortic valve cusps
Perforation Prolaps Restrictive cusp motion
Type Id Type II Type III
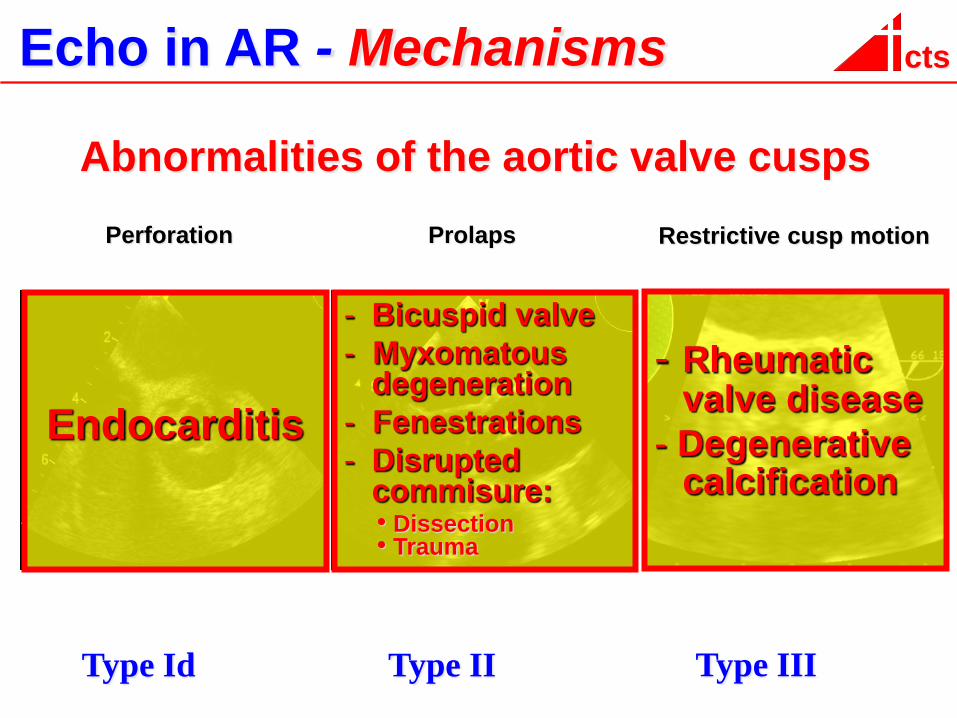
cts Echo in AR - Mechanisms
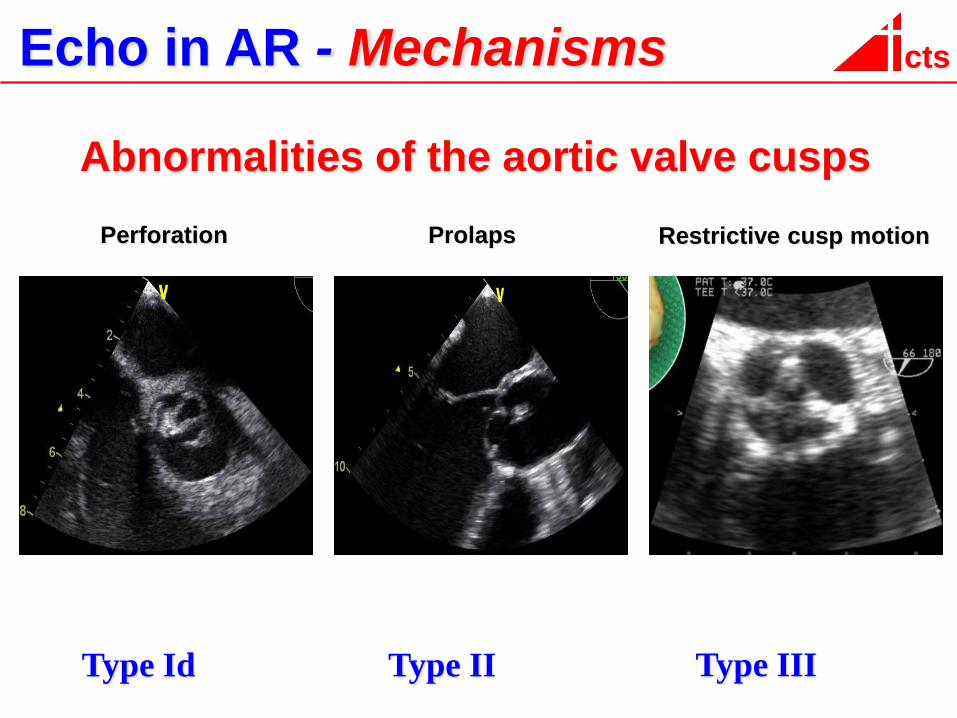
Abnormalities of the aortic valve cusps
Perforation Prolaps Restrictive cusp motion
Endocarditis
- Bicuspid valve
- Myxomatous degeneration
- Fenestrations
- Disrupted commisure:
• Dissection • Trauma
- Rheumatic valve disease
- Degenerative calcification
Type Id Type II Type III
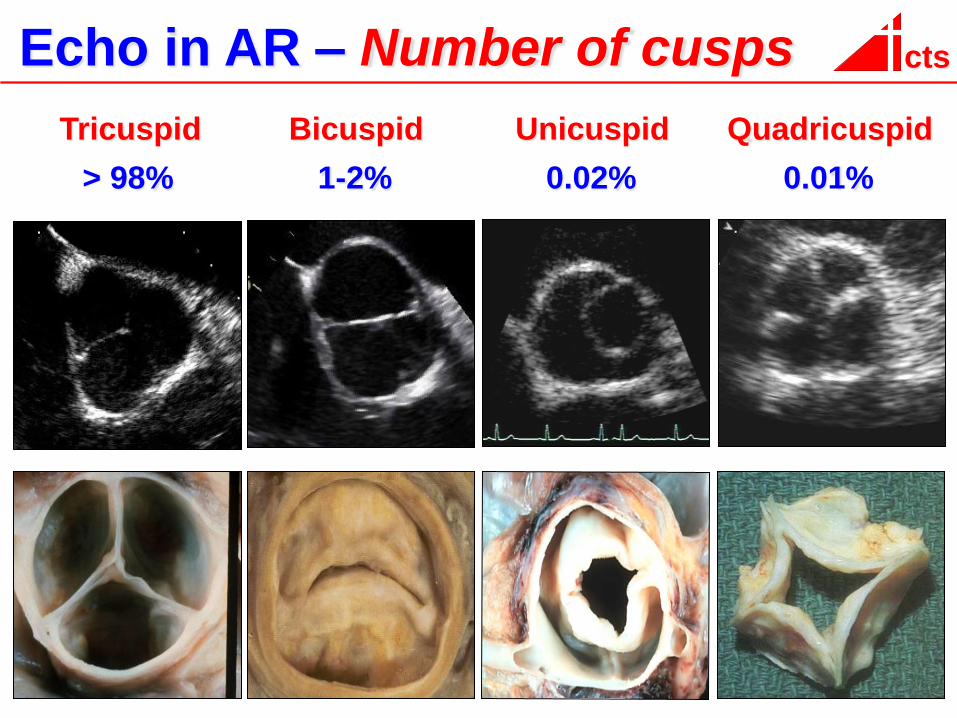
cts Echo in AR – Number of cusps
Tricuspid Bicuspid Unicuspid Quadricuspid
1-2% 0.02% 0.01% > 98%
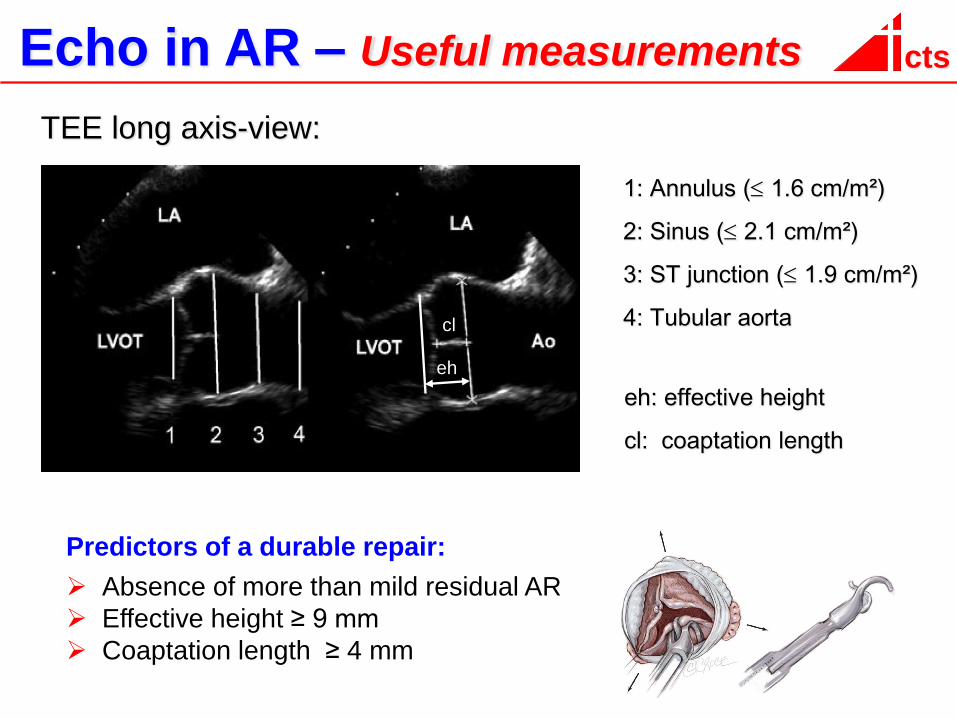
cts Echo in AR – Useful measurements
1: Annulus ( 1.6 cm/m²)
2: Sinus ( 2.1 cm/m²)
3: ST junction ( 1.9 cm/m²)
4: Tubular aorta
eh: effective height
cl: coaptation length
eh
cl
TEE long axis-view:
Predictors of a durable repair:
Absence of more than mild residual AR
Effective height ≥ 9 mm
Coaptation length ≥ 4 mm
cts
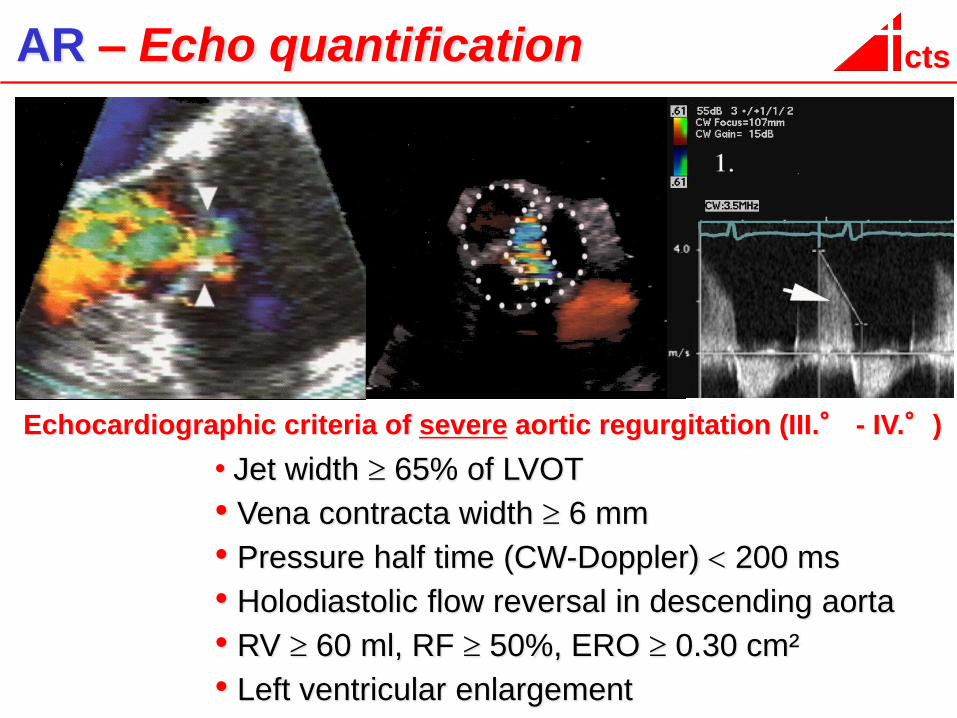
Echocardiographic criteria of severe aortic regurgitation (III.° - IV.°)
• Jet width 65% of LVOT
• Vena contracta width 6 mm
• Pressure half time (CW-Doppler) 200 ms
• Holodiastolic flow reversal in descending aorta
• RV 60 ml, RF 50%, ERO 0.30 cm²
• Left ventricular enlargement
AR – Echo quantification
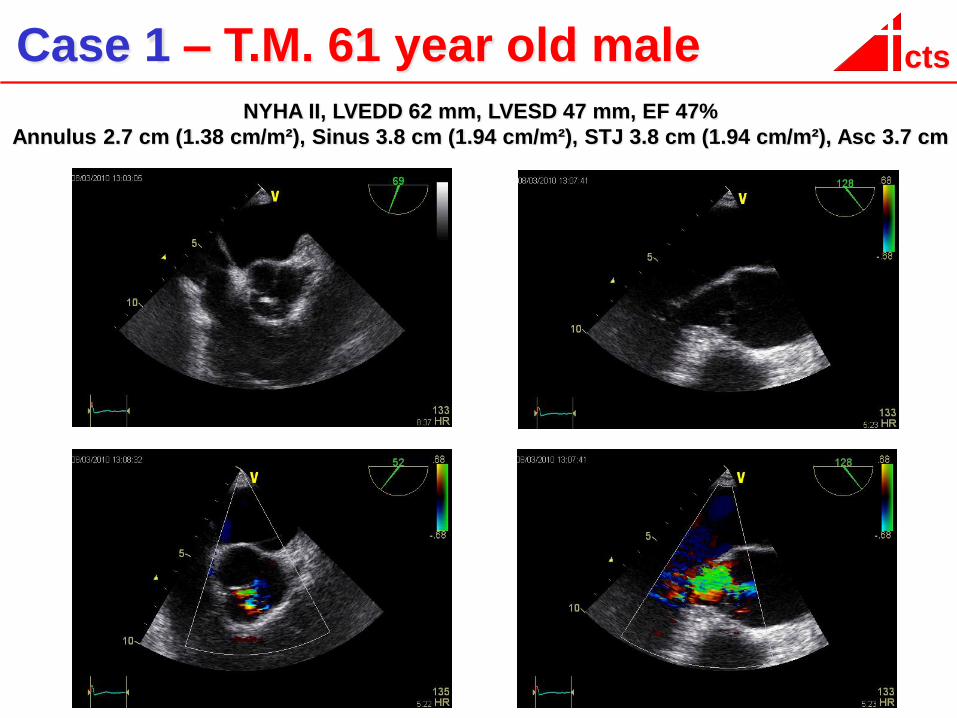
cts Case 1 – T.M. 61 year old male
NYHA II, LVEDD 62 mm, LVESD 47 mm, EF 47%
Annulus 2.7 cm (1.38 cm/m²), Sinus 3.8 cm (1.94 cm/m²), STJ 3.8 cm (1.94 cm/m²), Asc 3.7 cm
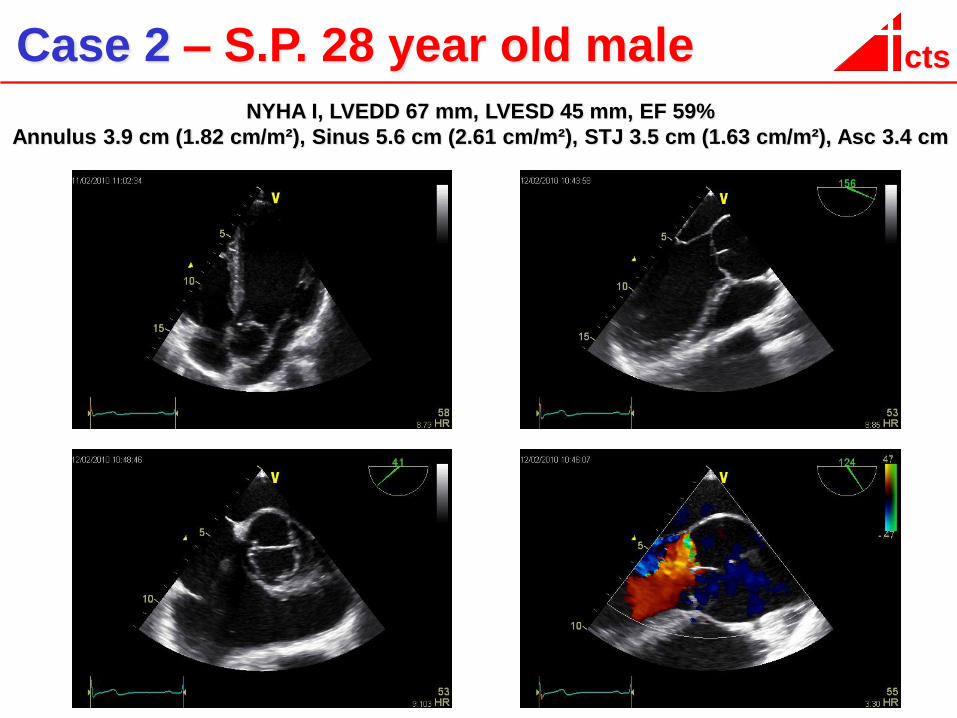
cts Case 2 – S.P. 28 year old male
NYHA I, LVEDD 67 mm, LVESD 45 mm, EF 59%
Annulus 3.9 cm (1.82 cm/m²), Sinus 5.6 cm (2.61 cm/m²), STJ 3.5 cm (1.63 cm/m²), Asc 3.4 cm
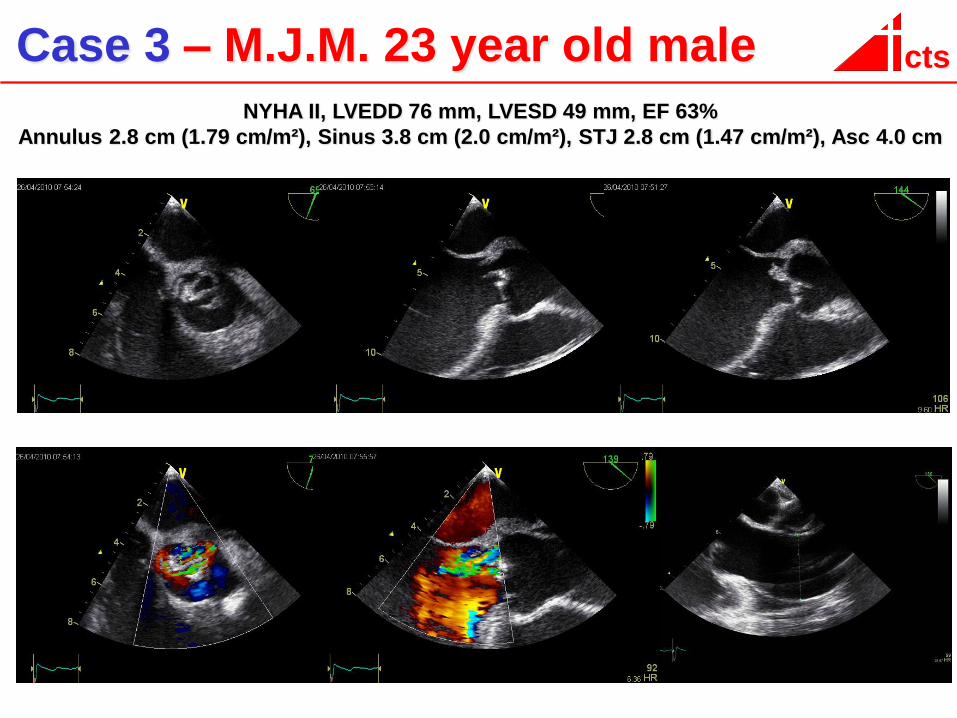
cts Case 3 – M.J.M. 23 year old male
NYHA II, LVEDD 76 mm, LVESD 49 mm, EF 63%
Annulus 2.8 cm (1.79 cm/m²), Sinus 3.8 cm (2.0 cm/m²), STJ 2.8 cm (1.47 cm/m²), Asc 4.0 cm
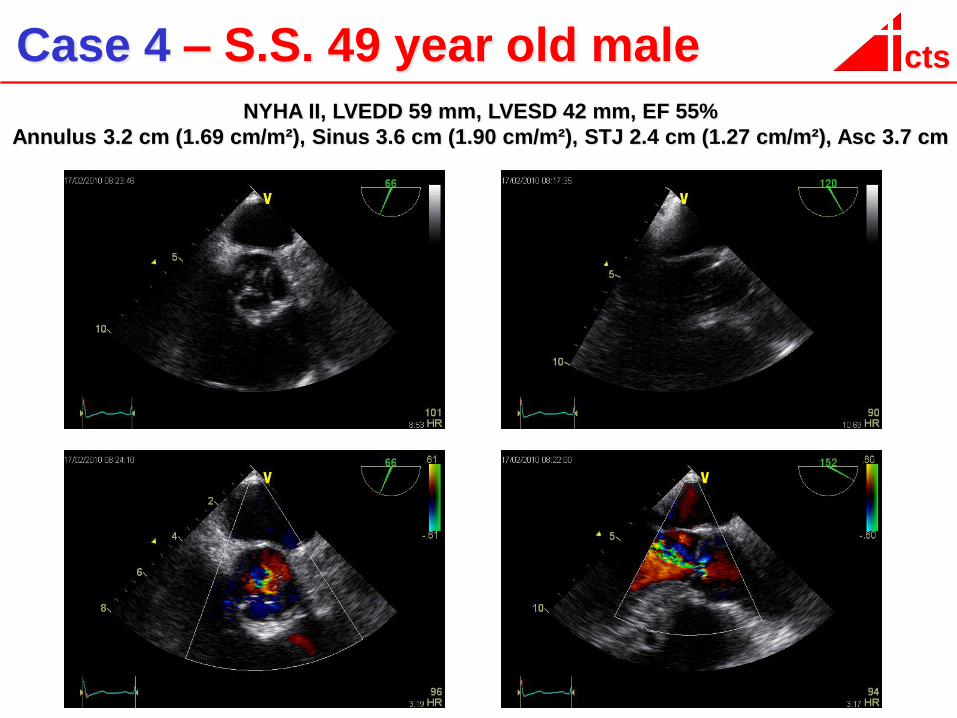
cts Case 4 – S.S. 49 year old male
NYHA II, LVEDD 59 mm, LVESD 42 mm, EF 55%
Annulus 3.2 cm (1.69 cm/m²), Sinus 3.6 cm (1.90 cm/m²), STJ 2.4 cm (1.27 cm/m²), Asc 3.7 cm

Thank you
for your
attention!
Akademisches Lehrkrankenhaus der Universität des Saarlandes
cts CaritasKlinikum Saarbrücken St. Theresia
cts
Additional
Slides
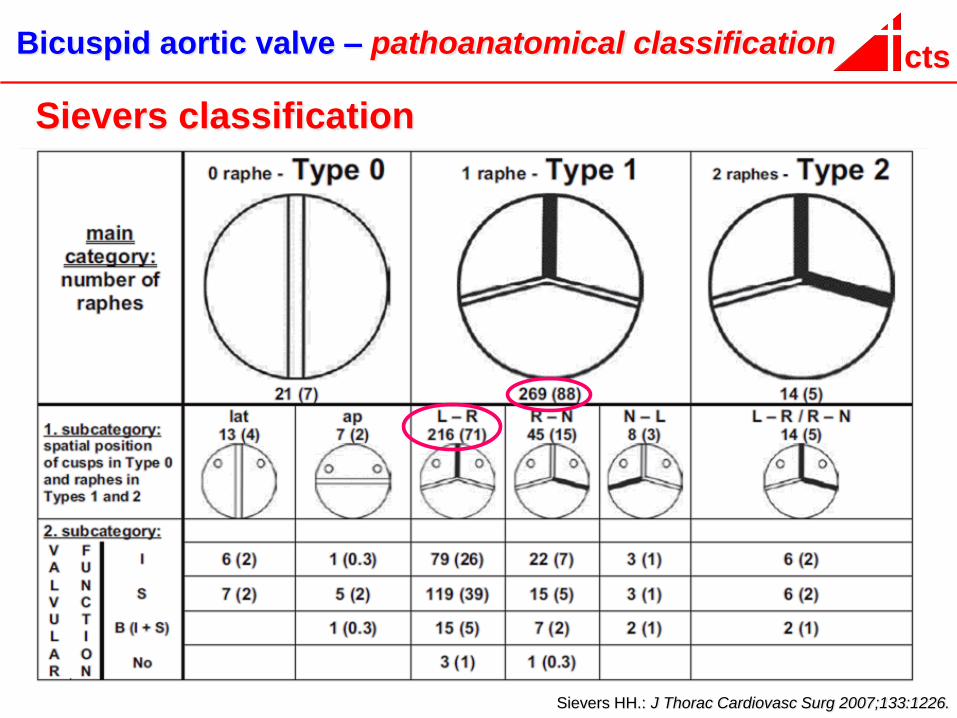
cts Bicuspid aortic valve – pathoanatomical classification
Sievers HH.: J Thorac Cardiovasc Surg 2007;133:1226.
Sievers classification
cts
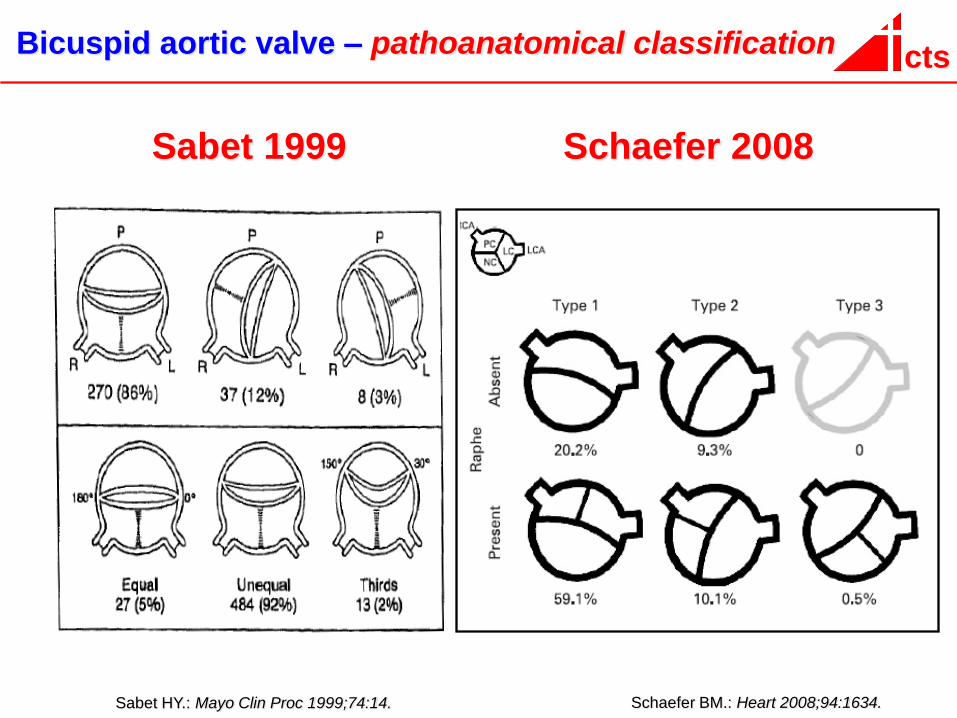
Sabet HY.: Mayo Clin Proc 1999;74:14.
Bicuspid aortic valve – pathoanatomical classification
Schaefer BM.: Heart 2008;94:1634.
Sabet 1999 Schaefer 2008
Recommended