135
(g3Tio,k)yg,)iY,oNm,,gf,ed(,8,o,il)
DURAL SINUS THROMBOSIS: REPORT OF TWO CASES Mitsunobu IDE, Minoru JIMBO, Masaaki YAMAMOTO, Yutaka UMEBARA and Shinji HAGIWARADepartment of Neurosurgery (Director: Prof. MinoruJIMBO), Tokyo Women's Medical College Daini Hospital
(Received July 2, 1993)
Diagnosis of dural sinus thrombosis is frequently difficult and may be delayed due to
lack of specific neurological signs. The initial diagnostic clues are usually present on
computed tomographic (CT> seans. We report two cases of dural sinus thrombosis, in
which routine precontrast CT scans visualized thrombi as increased attenuation within
the sinuses. We stress that recognition of this specific CT finding of dural sinus
thrombosis on routine precontrast study can lead to early diagnosis and prompt
appropriate therapy.
Introduction
Dural sinus thrombosis may occur more fre-
quently than is suspected. Towbin found dural
sinus thrombosis in 9% of 182 consecutive au-
topsies of adult casesi}. Dural sinus thrombosis
can be asymptomatic or present with only mild
neurological deficits, but it may also have an
acute, rapidly fatal course. Diagnosis of dural
sinus thrombosis is frequently difficult and may
be delayed due to lack of specific neurological
signs. Early diagnosis and prompt appropriate
treatment can lead to decreased risk of mortality
and morbidity. The initial diagnostic clues are
usually present on computed tomographic (CT)
scans. We report two cases of acute dural sinus
thrombosis and discuss the CT findings of this
condition; hyperdense intraluminal thrombi de-
tected on precontrast CT scans.
Case Report
Patient 1.
A six-year-old boy began to vomit frequently
and complained of continuous headache, and was
admitted to a local hospital. Four days later, he
was transferred to our facility immediately after a
generalized seizure. On arrival, he was stuporous
and exhibited left hemiparesis and nuchal stif-
-1429
fness. Platelet count, bleeding time and coagula-
tion time were within normal limits. Coagulation
studies demonstrated normal prothrombin and
partial thromboplastin times. Low fibrinogen (120
mg/100 ml) and high fibrin degradation product
concentrations (O.45 mg/1) were considered to
have resulted from aggravated intravascular
coagulation and fibrinolysis, respectively. Precon-
trast CT scans on admission revealed a hyper-
dense hematoma in the right temporal lobe, as-
sociated with hypodense edema in the right hem-
isphere. The precontrast CT scans also demon-
strated areas of increased attenuation in the
regions of the superior sagittal, straight and right
transverse sinuses and the Galenic and internal
cerebral veins (Fig. 1). The attenuation value in
these intraluminal regions was 75-90 Hounsfield
units (HU). Based on these CT findings, a diagno-
sis of dural sinus thrombosis was made and ther-
apy with fructose added glycerol (GLYCEOL@)
and low molecular weight dextran was initiated.
Cerebral angiography could not be performed.
Despite aggressive medical treatment, his neuro-
logical condition deteriorated rapidly and he be-
came comatose on the second hospital day. Repeat
CT scans demonstrated a new hematoMa in the
right thalamus and widespread hypodense areas
in the midbrain and the bilateral basal ganglia. He

136
-.
i
-k
'sit''
e,
+
tz#. /
=
r-e
th ;]
fteqhiv.r'" '
l' ".'"` va"'hua "t
Fig. 1 Patient 1. Precontrast computed tomographic scans demonstrating areas of increased attenuation
in the region of the superior sagittal, straight, and right transverse sinuses and the Galenic and internal
cerebral veins. The attenuation value in these regions is 75-90 Hounsfield units. Hemorrhagic venous
infarcts are also present in the right temporal lobe.
a.?"di
gs
sexe Egggmekgg
if ig i ?f' x ig'
,c s?gigs
・ ee
ee,
ev
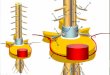
Fig. 2 Patient 1. View of the posterior fossa at autopsy.
The right transverse and sigmoid sinuses, which have
been peeled from the skull with forceps, are occluded by
fresh thrombus.
enaes.(ISii glsl. s e
pt paubes "tws
sgl
es
ts
vaknv ・ge' 'Z'; g
.,,.,li'g#magelasr llha".S'tlltlit/i'{eeffg'//$S,sTe}g:;s
ixiag
x
tsee
Fig. 3 Patient 1. Transectional view of the superior
sagittal sinus, demonstrating an anternortem thrombus.
(hematoxylin and eosin ×40)
died on the third hospital day.
At autopsy, the brain was edematous andweighed 1,350 g. The cerebral surface was enti-
rely covered with severe subarachnoid hemor-
rhage. The superior sagittal, straight, bilateral
transverse and sigmoid sinuses were occluded by
fresh antemortem thrombi (Figs. 2 and 3). The left
transverse and sigmoid sinuses were hypoplastic.
The internal cerebral and Galenic veins were also
thrombosed. On brain section there were exten- '
sive hemorrhagic infarcts of the midbrain, both
thalami and the basal ganglia.
Patient 2.
A 38-year-old woman was admitted to our faci-
lity with a 24-hour history of worsening headache
and frequent vomiting. On admission, her con-
sciousness was clear. There was neither neuro-
logical deficit nor papilledema. She had no definite
past history of otic disease. She had been taking
oral contraceptives for 10 months. Routine coagu-
- 1430 -

137
g'・
#・ ・
E#lybs'
iilill
'k.S ,i
'Ss
$
geec
mu""6e・
,estw
・kgxts
ikll
・A
pt
,".k., .A ss deig:pt・
sik.
S',
tw・
"'sa er, sW tl '
tsW''
gE
ff ?g f, S'
Fig. 4 Patient 2. Precontrast computed tomographic scans demonstrating areas of increased attenuation
in the region of the left transverse and superior sagittal sinuses. The attenuation value of these regions is
80-90 Hounsfield units.
Fig. 5 Patient 2. Anteroposterior (A) and lateral (B) views of digital subtraction angiQgram demonstrating
occlusion of the superior sagittal and left transverse sinuses.
lation studies showed normal findings. Precon-
trast CT scans revealed areas of increased at-
tenuation within the superior sagittal and left
transverse sinuses, but neither parenchymal
lesions nor subarachnoid hemorrhage (Fig. 4).
Digital subtraction angiography (DSA) demon-
strated obstruction of the superior sagittal and
left transverse sinuses (Fig. 5). Magnetic reson-
ance (MR) imaging demonstrated hyperintense
areas in the superior sagittal and left transverse
sinuses on both Tl- and T2-weighted images with
concurrent mastoiditis on the left side (Fig. 6). A
diagnosis of dural sinus thrombosis was made and
therapy with low molecular weight dextran and
systemic fibrinolytic agent was initiated. Uro-
kinase was administered through continuous
venous infusion (2 X 105 units/day) fpr five days.
In addition, an otologist was consulted for man-
agement of the mastoiditis. Headache and vomit-
ing subsided within a week. She was discharged a
month later and had no neurological deficits.
Follow-up MR imaging demonstrated recanaliza-
-1431-

138
Fig. 6 Patient 2. Axial Tl- (A) and T2-weighted (B) and coronal Tl-weighted (C) magnetic resonance
images demonstrating hyperintense areas in the superior sagittal and left transverse sinuses (arrows)
with concurrent mastoidotis on the left side.
Fig. 7 Patient 2. Coronal Tl-weighted magnetic reson-
ance image two months after the onset demonstrating
recovery of flow void sign in the superior sagittal and left
transverse sinuses <arrows).
tion of
(Fig. 7).
the left transverse and sagittal slnuses
Discussion
Dural sinus thrombosis has various etiologies.
Septic dural sinus thrombosis may be a serious
complication of meningitis or encephalitis2}. It can
also occur as a result of middle ear or paranasal
sinus infections. Aseptic dural sinus thrombosis is
seen during pregnancy and the puerperium3). It
has been reported in several young women given
oral contraceptives4)5). Dehydration and cachexia,
as well as a number of hematological and vascular
diseases, have been reported to be associated with
aseptic dural sinus thrombosis6)nyiO). In patient 1,
neither antemortem nor postmortem examination
revealed the etiology of the disease. The clinical
course of patient 1 was fulminant because in-
volvement of the deep venous system caused
hemorrhagic infarcts in the midbrain and thal-
amus. Factors contributing to increased mortality
include rapid thrombus evolution and involve-
ment of the deep venous system. The internal
cerebral vein is often affected in childrenii). We
speculate that oral contraceptives and mastoiditis
were the major causes of dural sinus thrombosis
in patient 2.
- 1432 -

139
DSA, MR imaging and MR angiography areexcellent tools for the diagnosis of dural sinus
thrombosisi2}i3). However, the initial diagnostic
clues are usually present on CT scans, and their
recognition can lead to early diagnosis and prompt
appropriate therapy. The use' of CT scanning for
diagnosing dural sinus thrombosis has been re-
ported by a number of authors2)ii)i4}i5}. Buonanno
et al. have advocated the "empty triangle" sign as
a CT finding specific to superior sagittal sinus
thrombosisi4). Infusion of contrast medium and a
narrow CT display window, and a high window
level, may be necessary to demonstrate this sign.
However, these special window settings are not
likely to be implemented unless dural sinus
thrombosis is suspected. Less specific signs in-
clude cerebral edema, small ventricles, hemor-
rhage within the cerebral parenchyma, and gyral
enhancementi4)i6}i7).
We wish to cali attention to other CT signs of
dural sinus thrombosis. In our two patients,
routine precontrast CT scans visualized thrombi
as increased attenuation within the sinuses be-
cause of the high hemoglobin concentration of
fresh thrombi. Direct visualization of a thrombus
as increased attenuation within the sinuses and
veins on precontrast CT scans has been reported
previously2}ii)i5)i8}. In fact, the attenuation value of
the superior sagittal sinus ranges from 50 to 68
HU. This could be misleading if the diagnosis
were made without measuring the actual attenua-
tion value of the lesioni5). In our two patients, the
attenuation value of the affected sinuses and
veins was 75--90 HU, which is in good agreement
with that of fresh thrombus'9>. These areas of'
increased attenuation corresponded closely with
the extent of thrombosis revealed by the autopsy
or DSA.
We could not treat patient 1 with fibrinolytic or
anticoagulant therapy because the hemorrhagic
infarction was far advanced on admission. In
contrast, we successfully treated patient 2 with
systemic fibrinolytic therapy following early
diagnosis. According to Kalbag and Woolf, seizure
onset signals the development of hemorrhagic
infarction and systemic use of anticoagulants is
contraindicated thereafter20). From this view-.
point, early diagnosis and prompt appropriate
therapy are crucial. Di Rocco et al. reported
successful systemic use of anticoagulant and
fibrinolytic agents2i}. Successful treatment by
local infusion of fibrinolytic agents has recently
been reported22>N24). These reports encourage clini-
cians to attempt these innovative therapies in
otherwise hopeless cases of dural sinus throm-
bosis.
Referecnes
1) Towbin A: The syndrome of latent cerebral venous
thrombosis: Its frequency and relation to age and
congestive heart failure. Stroke 4: 419-430, 1973.
2) Wendling LR: Intracranial venous sinus thrombosis:
Diagnosis suggested by computed tomography. AJR 130: 978-980, 1978.
3) Cross JN, Castro PO, Jennett WB: Cerebral strokes
associated with pregnancy and the puerperium. Br Med
J 3: 214, 19684) Atkinson EA, Fa' irburn B, Heathfield KWG: In- tracranial venous thrombosis as a complication of oral
contraceptives. Lancet 1: 914-918, r970
5) Shende MC, Lourie H: Sagittal sinus thrombosis related to oral contraceptives. Case report.J Neurosurg
33: 714-717, 1970
6) Bousser MG: Cerebral vein thrombosis in Behcet's syndrome: Arch Neurol 39: 322, 1982
7) David RB, Hadfield MG, Vines FS et al: Dural sinus occlusion in leukemia. Pediatrics 56: 793-796,
19758) Donhowe SP, Lazaro RP: Dural sinus thrombosis in paroxysmal nocturnal hemoglobinuria. Clin Neurol
Neurosurg 86: 149-152, 1984
9) Dunsker SB, Torres-Reyes E, Peden JC Jr: Pseu- dotumor cerebri associated with idiopathic cryofi-
brinogeneMia: Report of a case. Arch Neurol 23: 120-127, 1970
10) Iijima S, Nakamura S, Shio H et al: A case of superior sagittal sinus thrombosis with primary thrombocythemia. Rjnsho Shinkeigaku 20: 333-338,
198011) Justich E, Lammer J, Fritsch G et al: CT diagnosis
of thrombosis of dural sinuses in childhood. EurJ Radiol
4: 294-295, 1984
l2) McMurdo SK Jr, Brant-Zawadzki M, Bradley WG et al: Dural sinus thrombosis: Study using intermediate field strength MR imaging. Radiology
161: 83-86, 1986
13) Padayachee,TS, Bingham JB, Graves wo et al: Dural sinus thrombosis: Diagnosis and follow-up by
- 1433 -

140
magnetic resonance angiography and imaging. Neuro・
rad童010gy 33:165467,1991
14)Buonanno FS, Moody DM, Ball MR et al:Com-
puted cranial tomographic findings in cerebral sino・
venous occlusion. J Comput Assist Tomogr 2:281-290,
197815)Patrona6 NJ, Duda EEg, Mirfa㎞raee M et a1:
Superior sagittal sinus thrombosis diagnosed by com-
puted tomography. Surg Neurol 15:11-14,1981
16)Virapongse C, Cazenave C, Quis董ing R et a1:The
empty triangie sign:Frequency and signi丘cance in 76
.cases of dural s査nus thrombosis. Radiol.ogy 162:
779-785,1987
17)Zil㎞a A, Daiz AS:Computed tomography in the
diagnosis of superior sagittal sinus thrombosis.JCom-
put. Assist Tomogr 4:124-126,1980
18>Crimmins TJ, Rockswold GL, Wock DH:Progres-
sive posttraumatic. superior sagittal sinus thrombosis
complicated by puimonary embolism. J Neurosurg 60:
179-182,1984
19)Norman D, Price D, Douglas B et a1:Quantitative
aspects of computed tomography of the blood and
cerebrospipal fluid. Radiology 123:335-338,1977
20)Kalba霧RM, Woolf AL:Cerebral Venous Thrombosis,
pp247-248,0xford University Press, London(1967)
21)Di Rocco C, Iannelli A, Leone G et a1:Heparin-
urokinase.treatrnent in aseptic dural sinus thrombosis.
Arch Neurol 38:431-435,1981
22)Barnwe11 SL, Higashida RT, Halbach W et al:
Direct endovascular thrombolytic therapy for dural
sinus thrombosis. Neurosurgery 28:135-142,199工
23)Persson L,.Li1,a A:Extensive dural sinus山ronlbosis
treated by surgical removai and蓋ocal streptokinase
infusion, Neurosurgery 26:117-121,1990
24)Scott JA, Pascuzzi RM, Hall PV et a1:Treatment of.
dural sinus thrombosis with locai urokipase infusion.J
Neurosurg 68:284-287,1988.
静脈洞血栓症の2例
東京女子医科大学 附属第二病院脳神経外科.
イデ ミツノブジン.ボ井出 光信・神保ウメバラ ユタカ ハギワラ
梅原 裕・萩原
ミノル ヤマモト マサァキ
実・山本 昌昭シン ジ
信司
頭痛,嘔吐などを主訴に来院し,初期には特異的な症候を呈さない静脈洞血栓症の診断は,しばし
ぽ困難で,診断が遅れることが多い.
静脈洞血栓症は早期に診断し,速やかに適切な治療を開始せねぽ,症例1のように致命的となるこ
と.が少なくない. ・
本症の確定診断は脳血管撮影によってなされることが多いが,本.症を疑わなけれぽ実施されること.
は少ない.本症を疑うきっかけは,やはりCT scanであると考えられる.これまで,静脈洞血栓症に
特異的なCT所見としては㌔mpty triangle sign”が知られているが,これは,慢性期の所見であり,
造影剤の投与および特殊なwindow settingを要する..やはり,本症を疑ってかからなければ見落とさ
れる可能性が高い.
我々の2症例ではplain CT scanで静脈洞内の新鮮血栓がhigh density areaとして描出されてお
り,その範.囲は,剖検所見あるいは脳血管撮影所見と一致していた.この所見は静脈洞血栓症の早期
の診断,治療の上で重要なものと考え報告する.
一. P434一
Recommended