Effects ofResmetirom (MGL-3196)60and80mgina36-WeekStudy ofNASHPatientsStephenA.Harrison,OxfordUniversity;RebeccaTaub,MadrigalPharmaceuticals
INTRODUCTION
RESULTS
Resmetirom (MGL-3196) is a liver-directed, orally active, highly selectiveTHR-β agonist (Fig 1) in Phase 3 development for the treatment of NASHwith advanced stage 2-3 fibrosis. In a 36-week serial liver biopsy study,compared with placebo, MGL-3196 treated patients showed statisticallysignificant reduction in liver fat and NASH resolution. A per protocolpost-hoc dose evaluation was conducted in patients completing 36-weeks of treatment with resmetirom 60 or 80 mg to analyze doseresponse.
• Thedataobtainedfromthis36-weekperprotocolcompleteranalysisofpatientstreatedwithresmetirom,indicate80mgappearedmoreeffectivethan60mginreducinghepaticfatandresolvingNASH.• Lipidlowering,inparticularApoB andTGlowering,wasmorepronouncedat80ascomparedwith60mg.• Theseresultssupporttheefficacyandsafetyof80and100mgdoses,whicharebeingusedintheongoingNASHPhase3study,MAESTRO-NASH(NCT03900429).
MGL-3196-05 (NCT02912260) was a 36-week multicenter, double-blind,randomized, placebo-controlled trial in adults with biopsy-confirmedNASH (NAS≥4, F1-F3) and hepatic fat fraction ≥10% (Table 1). The studyincorporated an adaptive dosing design with all MGL-3196 patientsstarting on 80 mg (Fig 2). Patients with higher exposure had their dosereduced to 60 mg at week 4; a few had their dose increased to 100 mgat week 4 and were included in the 80 mg group. At 36 weeks 107paired liver biopsies, 73 drug-treated, 34 pbo were assessed (Fig 3). Theoverall safety and efficacy of resmetirom in patients on 60 or 80 mgdoses in NASH patients was determined.
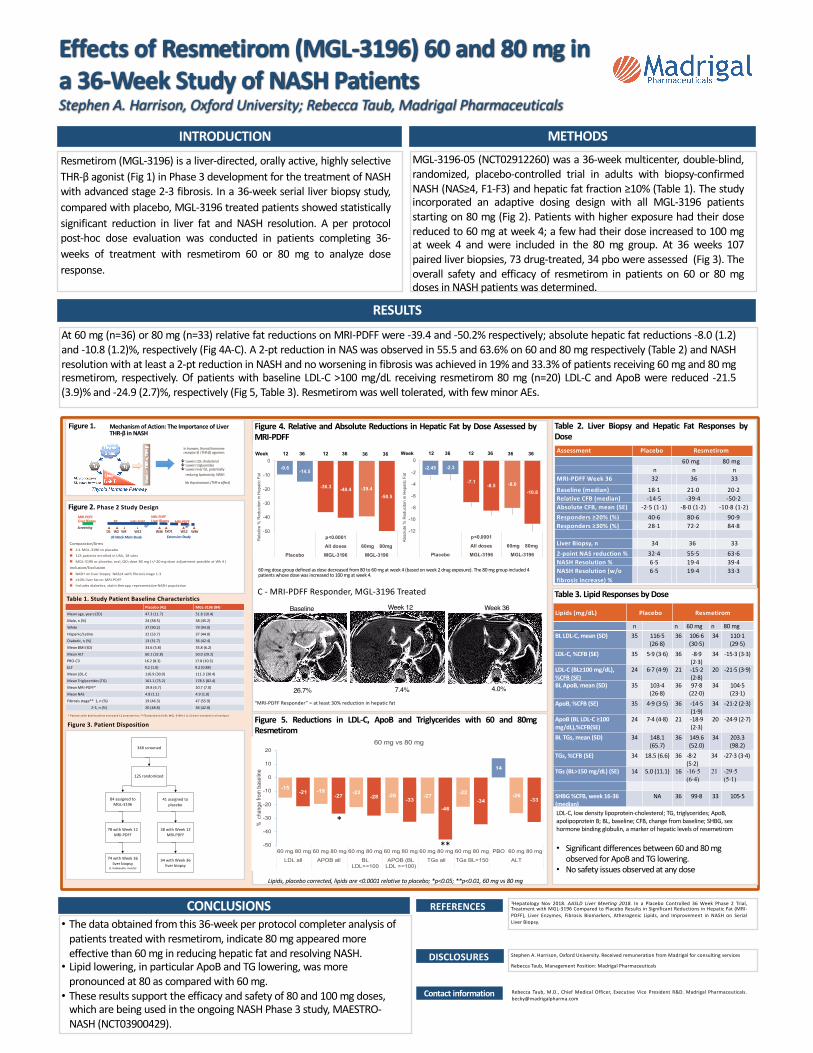
At 60 mg (n=36) or 80 mg (n=33) relative fat reductions on MRI-PDFF were -39.4 and -50.2% respectively; absolute hepatic fat reductions -8.0 (1.2)and -10.8 (1.2)%, respectively (Fig 4A-C). A 2-pt reduction in NAS was observed in 55.5 and 63.6% on 60 and 80 mg respectively (Table 2) and NASHresolution with at least a 2-pt reduction in NASH and noworsening in fibrosis was achieved in 19% and 33.3% of patients receiving 60mg and 80mgresmetirom, respectively. Of patients with baseline LDL-C >100 mg/dL receiving resmetirom 80 mg (n=20) LDL-C and ApoB were reduced -21.5(3.9)% and -24.9 (2.7)%, respectively (Fig 5, Table 3). Resmetiromwas well tolerated, with fewminor AEs.
1Hepatology Nov 2018. AASLD Liver Meeting 2018. In a Placebo Controlled 36 Week Phase 2 Trial,Treatment with MGL-3196 Compared to Placebo Results in Significant Reductions in Hepatic Fat (MRI-PDFF), Liver Enzymes, Fibrosis Biomarkers, Atherogenic Lipids, and Improvement in NASH on SerialLiver Biopsy.
CONCLUSIONS
METHODS
DISCLOSURES StephenA.Harrison,OxfordUniversity.ReceivedremunerationfromMadrigalforconsultingservices
RebeccaTaub,ManagementPosition:MadrigalPharmaceuticals
REFERENCES
Figure 3. Patient Disposition
Table 2. Liver Biopsy and Hepatic Fat Responses byDose
Figure 1. MechanismofAction:TheImportanceofLiverTHR-βinNASH
Figure 2. Phase 2 Study Design
ê LowersLDL-cholesterolê Lowerstriglyceridesê Lowersliverfat,potentially
reducinglipotoxicity,NASH
Nothyrotoxicosis(THR-αeffect)
Inhumans,thyroidhormonereceptor-β(THR-β)agonism:
ExtensionStudy
Screening
MRI-PDFFLiverBiopsy
MRI-PDFFLiverBiopsyMRI-PDFF MRI-PDFFPK
D1 W2 W4 W12 W36 W12 W36ExD136WeekMainStudy
Table 1. Study Patient Baseline Characteristics
Figure 4. Relative and Absolute Reductions in Hepatic Fat by Dose Assessed byMRI-PDFF
Comparator/Arms
n 2:1MGL-3196toplacebo
n 125patientsenrolledinUSA,18sites
n MGL-3196orplacebo,oral,QD;dose80mg(+/-20mgdoseadjustmentpossibleatWk 4)
Inclusion/Exclusion
n NASHonliverbiopsy:NAS≥4withfibrosisstage1-3
n ≥10%liverfatonMRI-PDFF
n Includesdiabetics,statintherapy,representativeNASHpopulation
Contactinformation Rebecca Taub, M.D., Chief Medical Officer, Executive Vice President R&D. Madrigal [email protected]
Baseline Week 12
“MRI-PDFFResponder”=atleast30%reductioninhepaticfat
Figure 5. Reductions in LDL-C, ApoB and Triglycerides with 60 and 80mgResmetirom
Table 3. Lipid Responses byDoseWeek 36
26.7% 7.4% 4.0%
Placebo(41) MGL-3196(84)Meanage,years(SD) 47.3(11.7) 51.8(10.4)
Male,n(%) 24(58.5) 38(45.2)
White 37(90.2) 79(94.0)
Hispanic/Latino 22(53.7) 37(44.0)
Diabetic,n(%) 13(31.7) 36(42.4)
MeanBMI(SD) 33.6(5.8) 35.8(6.2)
MeanALT 60.1(32.8) 50.0(29.2)
PRO-C3 16.2(8.3) 17.8(10.3)
ELF 9.2(1.0) 9.2(0.88)
MeanLDL-C 116.9(30.0) 111.3(30.4)
MeanTriglycerides(TG) 161.1(75.2) 178.5(82.4)
MeanMRI-PDFF* 19.8(6.7) 20.7(7.0)
MeanNAS 4.8(1.1) 4.9(1.0)
Fibrosisstage**1,n(%) 19(46.3) 47(55.9)
2-3,n(%) 20(48.8) 36(42.8)
*Patientsw ith bothbaselineandweek12assessments;**F0p lacebo=2(4.9);MGL-3196=1(1.2)wereincludedin allanalyses
84assignedtoMGL-3196
41assignedtoplacebo
78withWeek12MRI-PDFF
38withWeek12MRI-PDFF
348screened
125randomized
74withWeek36liverbiopsy
(1inadequate,muscle)
34withWeek36liverbiopsy
C- MRI-PDFFResponder,MGL-3196Treated
60mgdosegroupdefinedasdosedecreasedfrom80to60mgatweek4(basedonweek2drugexposure).The80mggroupincluded4patientswhosedosewasincreasedto100mgatweek4.
A B Assessment Placebo Resmetirom
60mg 80mgn n n
MRI-PDFFWeek36 32 36 33
Baseline(median) 18·1 21·0 20·2RelativeCFB(median) -14·5 -39·4 -50·2AbsoluteCFB,mean(SE) -2·5(1·1) -8·0(1·2) -10·8(1·2)Responders≥20%(%) 40·6 80·6 90·9Responders≥30%(%) 28·1 72·2 84·8
LiverBiopsy,n 34 36 332-pointNASreduction% 32·4 55·5 63·6NASHResolution% 6·5 19·4 39·4NASHResolution(w/ofibrosisincrease)%
6·5 19·4 33·3
Lipids(mg/dL) Placebo Resmetirom
n n 60mg n 80mgBLLDL-C,mean(SD) 35 116·5
(26·8)36 106·6
(30·5)34 110·1
(29·5)LDL-C,%CFB(SE) 35 5·9(3·6) 36 -8·9
(2·3)34 -15·3(3·3)
LDL-C(BL≥100mg/dL),%CFB(SE)
24 6·7(4·9) 21 -15·2(2·8)
20 -21·5(3·9)
BLApoB,mean(SD) 35 103·4(26·8)
36 97·8(22·0)
34 104·5(23·1)
ApoB,%CFB(SE) 35 4·9(3·5) 36 -14·5(1·9)
34 -21·2(2·3)
ApoB(BLLDL-C≥100mg/dL),%CFB(SE)
24 7·4(4·8) 21 -18·9(2·3)
20 -24·9(2·7)
BLTGs,mean(SD) 34 148.1(65.7)
36 149.6(52.0)
34 203.3(98.2)
TGs,%CFB(SE) 34 18.5(6.6) 36 -8·2(5·2)
34 -27·3(3·4)
TGs(BL>150mg/dL)(SE) 14 5.0(11.1) 16 -16·5 (6·4)
21 -29·5 (5·1)
SHBG%CFB,week16-36(median)
NA 36 99·8 33 105·5
LDL-C,lowdensitylipoprotein-cholesterol;TG,triglycerides;ApoB,apolipoproteinB;BL,baseline;CFB,changefrombaseline;SHBG,sexhormonebindingglobulin,amarkerofhepaticlevelsofresemetirom
• Significantdifferencesbetween60and80mgobservedforApoBandTGlowering.
• NosafetyissuesobservedatanydoseLipids,placebocorrected,lipidsare<0.0001relativetoplacebo;*p<0.05;**p<0.01,60mgvs80mg
-9.6
-36.3 -39.4
-14.5
-40.4-50.5
-50
-40
-30
-20
-10
0
p<0.0001All doses 60mg 80mg
Placebo MGL-3196 MGL-3196
Rel
ativ
e %
Red
ucito
n in
Hep
atic
Fat
Relative Change MRI-PDFF (% )Week 12 36 12 36 36 36
-2.45
-7.1 -8.0
-2.3
-8.5-10.8
-12
-10
-8
-6
-4
-2
0
p<0.0001All doses 60mg 80mg
Placebo MGL-3196 MGL-3196
Abso
lute
% R
educ
iton
in H
epat
ic F
at
Relative Change MRI-PDFF (% )Week 12 36 12 36 36 36
-15-21 -19
-27 -22-28 -26
-33-27
-46
-22-34
14
-26-33
-50
-40
-30
-20
-10
0
10
20
60 mg 80 mg 60 mg 80 mg 60 mg 80 mg 60 mg 80 mg 60 mg 80 mg 60 mg 80 mg PBO 60 mg 80 mg
LDL all APOB all BLLDL>=100
APOB (BLLDL >=100)
TGs all TGs BL>150 ALT
% c
hang
e fro
m b
asel
ine
60 mg vs 80 mg
*
**
Recommended

















