Dott. ssa Pamela Guglielmini Dott.ssa Elena Traverso
SC Oncologia Medica
Azienda Ospedaliera Nazionale “SS. Antonio e Biagio e C. Arrigo” Alessandria
Eventi metabolici:
un caso clinico

- Ipertensione arteriosa in terapia medica (amlodipina 5 mg/die)
- Obesità (BMI =32) - Ex fumatrice (10 sigarette/die) - PS = ECOG 0
ANAMNESI
Donna, 76 anni, A.A.
Caso Clinico
Esordio 4/2016:
Tru cut della mammella sinistra Diagnosi istopatologica: CDI G3
TNM: cT4 cN1 Mx
Fattori Prognostici: ER 99% PgR neg Ki67 41% HER 2 2+ FISH non amplificata
Stadiazione
TC-TB con m.d.c.: lesioni secondarie polmonari bilaterali e linfonodali mediastiniche.
Caso Clinico
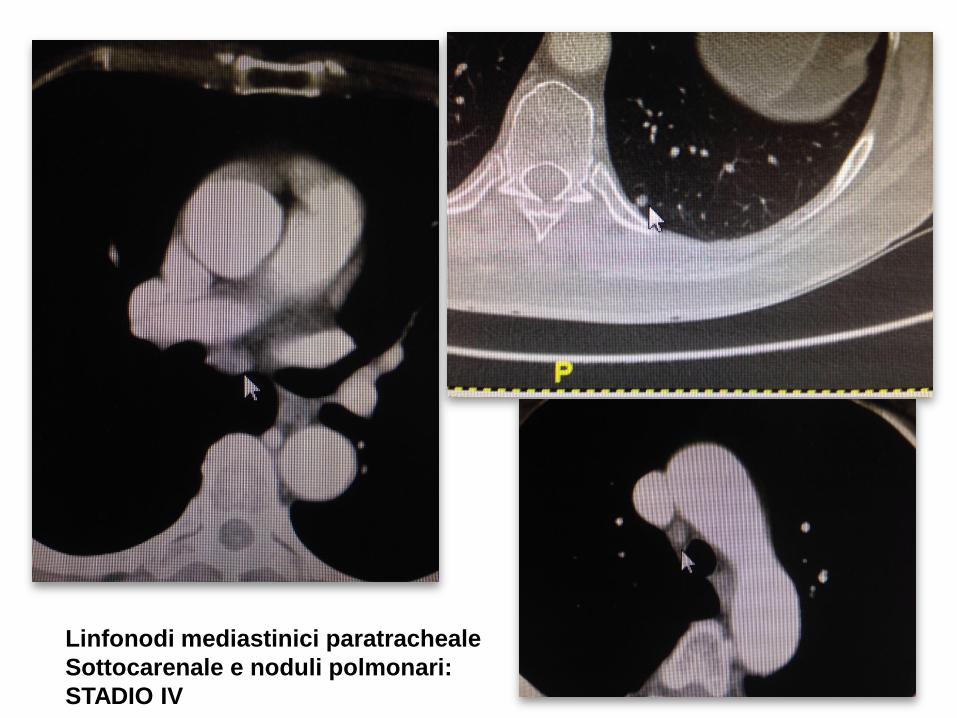
Linfonodi mediastinici paratracheale
Sottocarenale e noduli polmonari:
STADIO IV
Dal Maggio al Luglio 2016: 1° LINEA TAXOLO (1-8-15 q28) x 12 cicli ben tollerata
Agosto 2016 - Giugno 2017 Mantenimento: LETROZOLO 2,5 mg/die continuativamente
Giugno 2017: TAC rivalutazione: PD EPATICA e PLEURICA
Comparsa di nodulazioni secondarie pleuriche dx e 2 localizzazioni secondarie epatiche.
Luglio 2017: 2° LINEA: EVEROLIMUS 10 MG/DIE + EXEMESTANE 25
MG/DIE
Caso Clinico
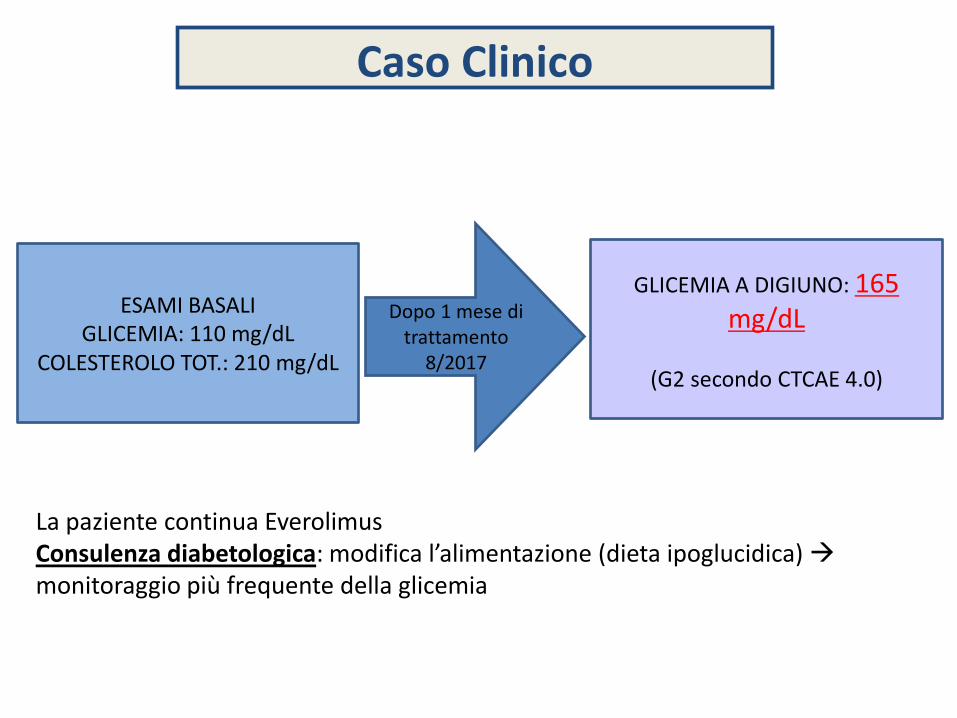
ESAMI BASALI GLICEMIA: 110 mg/dL
COLESTEROLO TOT.: 210 mg/dL
Dopo 1 mese di
trattamento
8/2017
GLICEMIA A DIGIUNO: 165 mg/dL
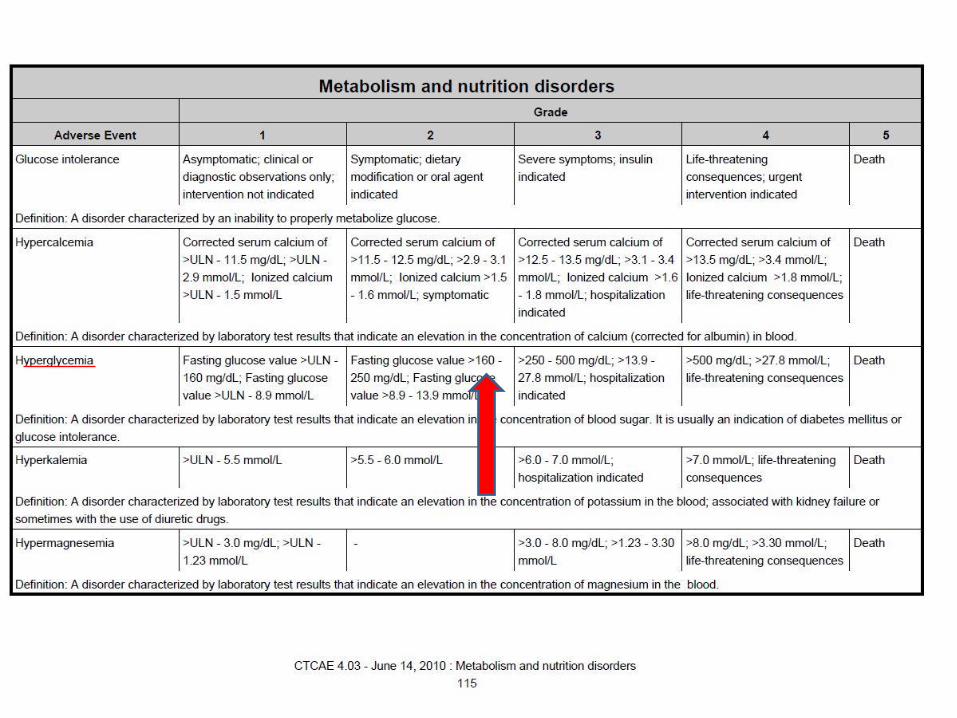
(G2 secondo CTCAE 4.0)
La paziente continua Everolimus Consulenza diabetologica: modifica l’alimentazione (dieta ipoglucidica) monitoraggio più frequente della glicemia
Caso Clinico
Dopo 2 settimane
GLICEMIA A DIGIUNO: 260 mg/dL
HBA1C: 6% (G3 secondo CTCAE 4.0)
!!!
Caso Clinico
La paziente ha temporaneamente sospeso Everolimus Consulenza diabetologica: iniziare terapia antidiabetica orale (Metformina 500 mg x 3/die) e proseguire dieta ipoglucidica.
GLICEMIA A DIGIUNO: 130 mg/dL
Dopo 1 mese GLICEMIA A DIGIUNO: 105 mg/dL
HBA1C: 4.5%
La paziente riprende Everolimus a dosi ridotte ( 5 mg/die)
Dopo 2 settimane
Caso Clinico
EVE 10 mg + EXE
PBO + EXE
Number of patients still at risk
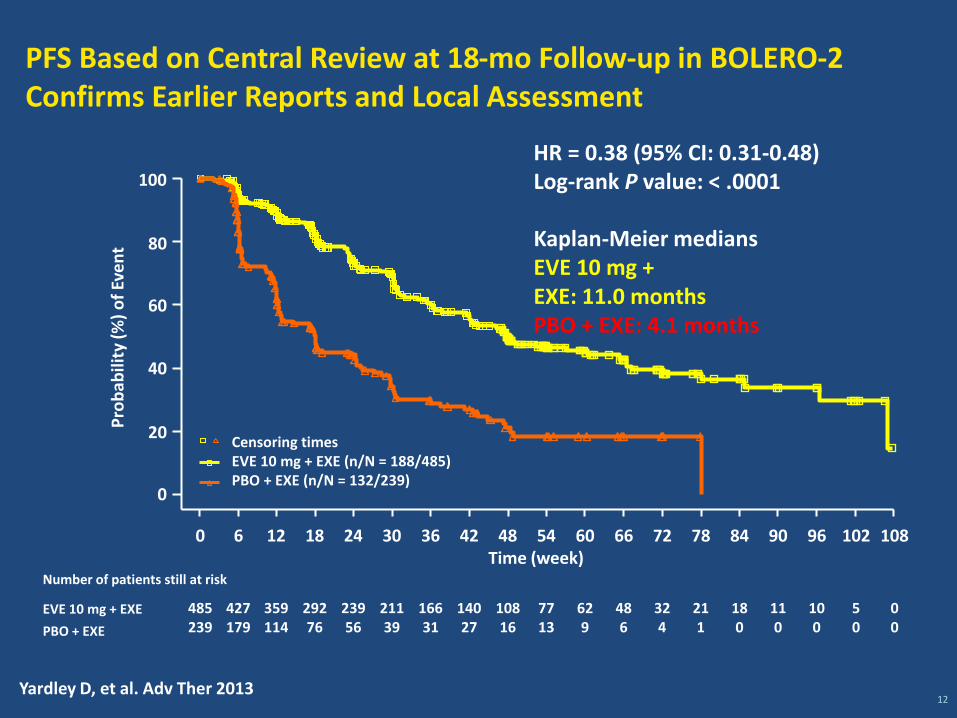
HR = 0.38 (95% CI: 0.31-0.48) Log-rank P value: < .0001
Kaplan-Meier medians EVE 10 mg + EXE: 11.0 months PBO + EXE: 4.1 months
0 6 12 18 24 30 36 42 48 54 60 66 72 78 84 90 96 102 108
485
239
427
179
359
114
292
76
239
56
211
39
166
31
140
27
108
16
77
13
62
9
48
6
32
4
21
1
18
0
11
0
10
0
5
0
0
0
Censoring times
EVE 10 mg + EXE (n/N = 188/485) PBO + EXE (n/N = 132/239)
0
20
40
60
80
100
Pro
bab
ility
(%
) o
f Ev
en
t
Time (week)
PFS Based on Central Review at 18-mo Follow-up in BOLERO-2 Confirms Earlier Reports and Local Assessment
12
Yardley D, et al. Adv Ther 2013
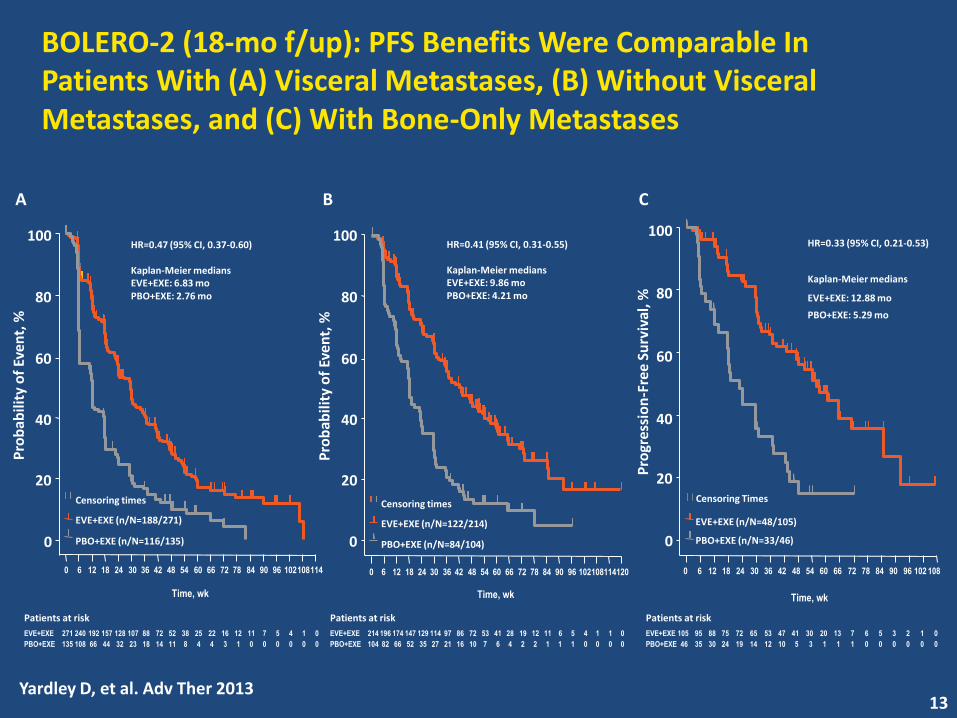
BOLERO-2 (18-mo f/up): PFS Benefits Were Comparable In Patients With (A) Visceral Metastases, (B) Without Visceral Metastases, and (C) With Bone-Only Metastases
0
20
40
60
Pro
bab
ility
of
Even
t, %
Pro
bab
ility
of
Even
t, %
80
100
Time, wk Time, wk
0 6 12 18 24 30 36 42 48 54 60 66 72 78 84 90 96 102 108 114
EVE+EXE
PBO+EXE
Patients at risk
271 240 192 157 128 107 88 72 52 38 25 22 16 12 11 7 5 4 1 0
135 108 66 44 32 23 18 14 11 8 4 4 3 1 0 0 0 0 0 0
0
20
40
60
80
100
0 6 12 18 24 30 36 42 48 54 60 66 72 78 84 90 96 102 108 114 120
EVE+EXE
PBO+EXE
Patients at risk
214 196 174 147 129 114 97 86 72 53 41 28 19 12 11 6 5 4 1 1 0
104 82 66 52 35 27 21 16 10 7 6 4 2 2 1 1 1 0 0 0 0
A B C
HR=0.47 (95% CI, 0.37-0.60)
Kaplan-Meier medians
EVE+EXE: 6.83 mo
PBO+EXE: 2.76 mo
HR=0.41 (95% CI, 0.31-0.55)
Kaplan-Meier medians
EVE+EXE: 9.86 mo
PBO+EXE: 4.21 mo
Censoring times
EVE+EXE (n/N=122/214)
PBO+EXE (n/N=84/104)
Censoring times
EVE+EXE (n/N=188/271)
PBO+EXE (n/N=116/135) 0
20
40
60
80
100
Time, wk
0 6 12 18 24 30 36 42 48 54 60 66 72 78 84 90 96 102 108
EVE+EXE
PBO+EXE
Patients at risk
105 95 88 75 72 65 53 47 41 30 20 13 7 6 5 3 2 1 0
46 35 30 24 19 14 12 10 5 3 1 1 1 0 0 0 0 0 0
EVE+EXE (n/N=48/105)
PBO+EXE (n/N=33/46)
Censoring Times
EVE+EXE: 12.88 mo
Kaplan-Meier medians
PBO+EXE: 5.29 mo
HR=0.33 (95% CI, 0.21-0.53)
Pro
gres
sio
n-F
ree
Surv
ival
, %
13
Yardley D, et al. Adv Ther 2013
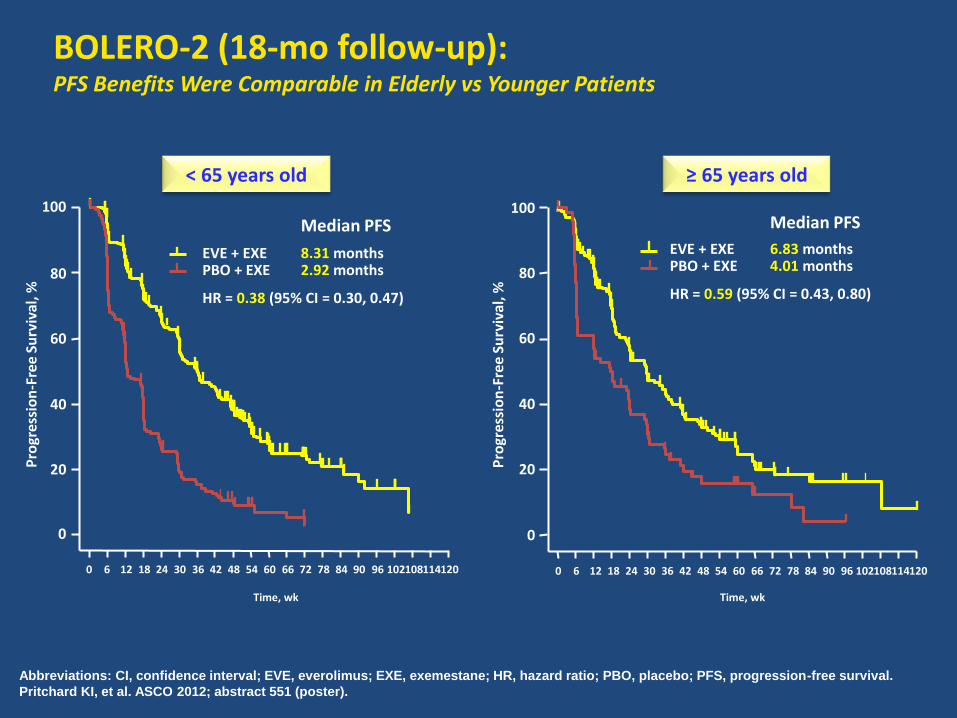
BOLERO-2 (18-mo follow-up): PFS Benefits Were Comparable in Elderly vs Younger Patients
Abbreviations: CI, confidence interval; EVE, everolimus; EXE, exemestane; HR, hazard ratio; PBO, placebo; PFS, progression-free survival.
Pritchard KI, et al. ASCO 2012; abstract 551 (poster).
0
20
40
60
80
Pro
gres
sio
n-F
ree
Surv
ival
, %
100
Time, wk
0 6 12 18 24 30 36 42 48 54 60 66 72 78 84 90 96 102 108 114 120
Pro
gres
sio
n-F
ree
Surv
ival
, %
0
20
40
60
80
100
Time, wk
0 6 12 18 24 30 36 42 48 54 60 66 72 78 84 90 96 102 108 114 120
< 65 years old ≥ 65 years old
EVE + EXE PBO + EXE
8.31 months
Median PFS
2.92 months
EVE + EXE PBO + EXE
HR = 0.38 (95% CI = 0.30, 0.47) HR = 0.59 (95% CI = 0.43, 0.80)
6.83 months
Median PFS
4.01 months
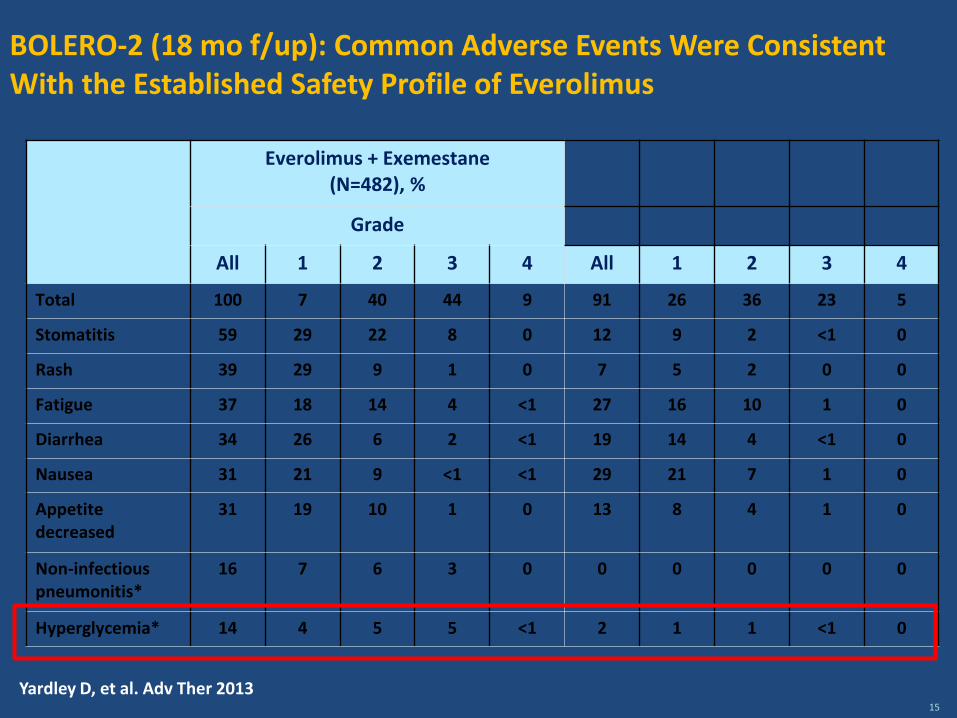
BOLERO-2 (18 mo f/up): Common Adverse Events Were Consistent With the Established Safety Profile of Everolimus
Everolimus + Exemestane (N=482), %
Grade
All 1 2 3 4 All 1 2 3 4
Total 100 7 40 44 9 91 26 36 23 5
Stomatitis 59 29 22 8 0 12 9 2 <1 0
Rash 39 29 9 1 0 7 5 2 0 0
Fatigue 37 18 14 4 <1 27 16 10 1 0
Diarrhea 34 26 6 2 <1 19 14 4 <1 0
Nausea 31 21 9 <1 <1 29 21 7 1 0
Appetite decreased
31 19 10 1 0 13 8 4 1 0
Non-infectious pneumonitis*
16 7 6 3 0 0 0 0 0 0
Hyperglycemia* 14 4 5 5 <1 2 1 1 <1 0
15
Yardley D, et al. Adv Ther 2013
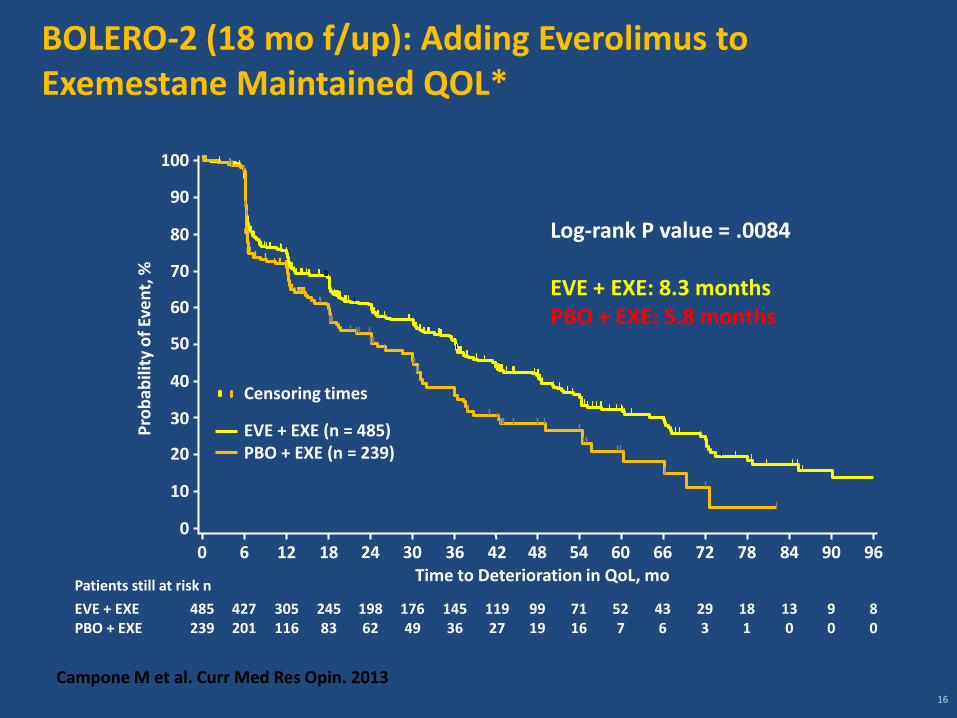
BOLERO-2 (18 mo f/up): Adding Everolimus to Exemestane Maintained QOL*
16
Log-rank P value = .0084
EVE + EXE: 8.3 months PBO + EXE: 5.8 months
100
90
80
70
60
50
40
30
20
10
0
0 6 12 18 24 30 36 42 48 54 60 66 72 78 84 90 96
485
239
EVE + EXE
PBO + EXE
427
201
305
116
245
83
198
62
176
49
145
36
119
27
99
19
71
16
52
7
43
6
29
3
18
1
13
0
9
0
8
0
Patients still at risk n
Pro
bab
ility
of
Eve
nt,
%
Censoring times
EVE + EXE (n = 485) PBO + EXE (n = 239)
Time to Deterioration in QoL, mo
Campone M et al. Curr Med Res Opin. 2013
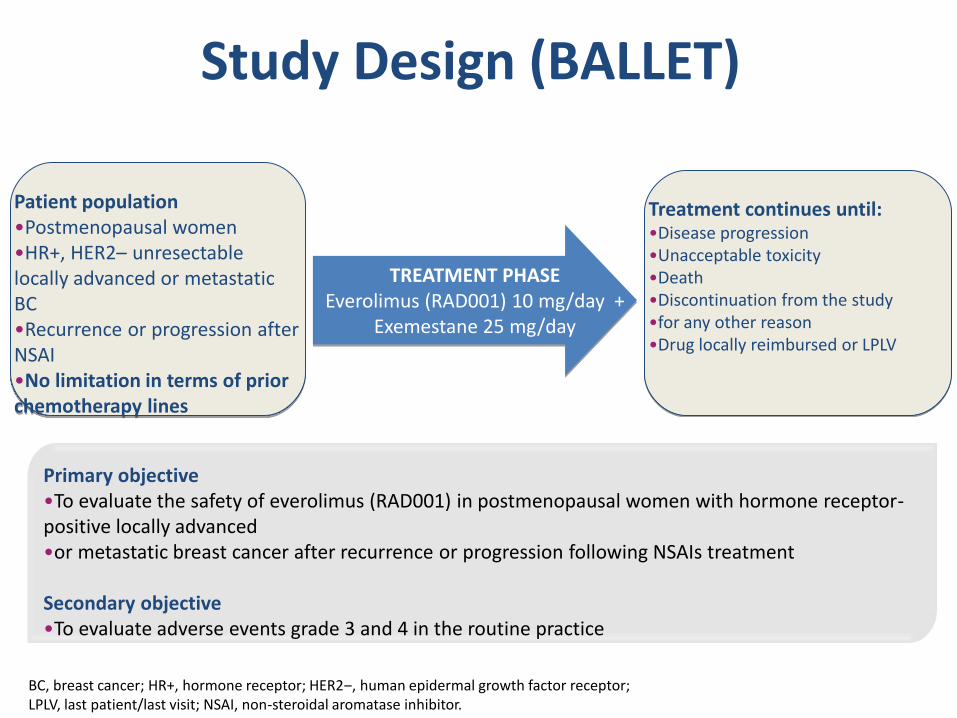
Study Design (BALLET)
Patient population •Postmenopausal women •HR+, HER2– unresectable locally advanced or metastatic BC •Recurrence or progression after NSAI •No limitation in terms of prior chemotherapy lines
TREATMENT PHASE Everolimus (RAD001) 10 mg/day +
Exemestane 25 mg/day
Treatment continues until: •Disease progression •Unacceptable toxicity •Death •Discontinuation from the study •for any other reason •Drug locally reimbursed or LPLV
Primary objective •To evaluate the safety of everolimus (RAD001) in postmenopausal women with hormone receptor-positive locally advanced •or metastatic breast cancer after recurrence or progression following NSAIs treatment Secondary objective •To evaluate adverse events grade 3 and 4 in the routine practice
BC, breast cancer; HR+, hormone receptor; HER2‒, human epidermal growth factor receptor; LPLV, last patient/last visit; NSAI, non-steroidal aromatase inhibitor.
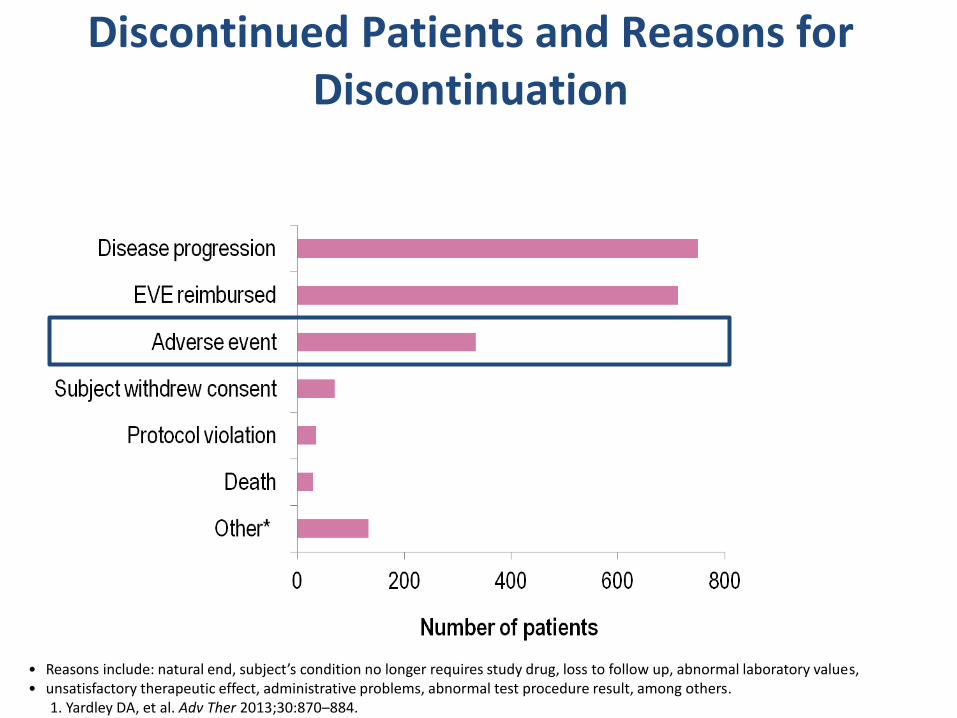
Discontinued Patients and Reasons for Discontinuation
• Reasons include: natural end, subject’s condition no longer requires study drug, loss to follow up, abnormal laboratory values, • unsatisfactory therapeutic effect, administrative problems, abnormal test procedure result, among others. 1. Yardley DA, et al. Adv Ther 2013;30:870–884.
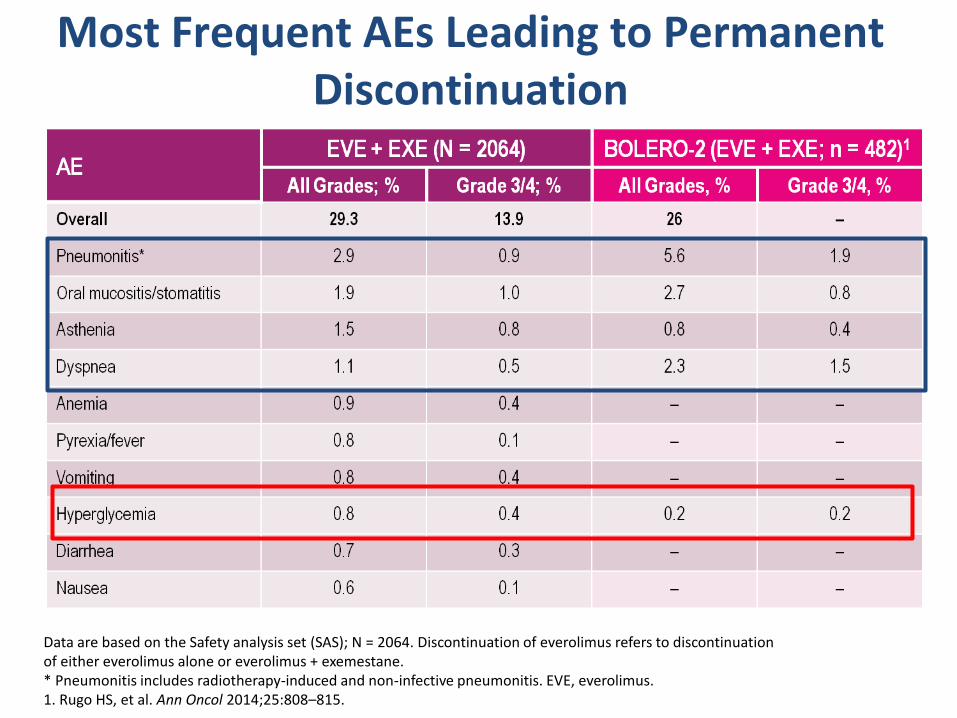
Most Frequent AEs Leading to Permanent Discontinuation
Data are based on the Safety analysis set (SAS); N = 2064. Discontinuation of everolimus refers to discontinuation of either everolimus alone or everolimus + exemestane. * Pneumonitis includes radiotherapy-induced and non-infective pneumonitis. EVE, everolimus. 1. Rugo HS, et al. Ann Oncol 2014;25:808–815.
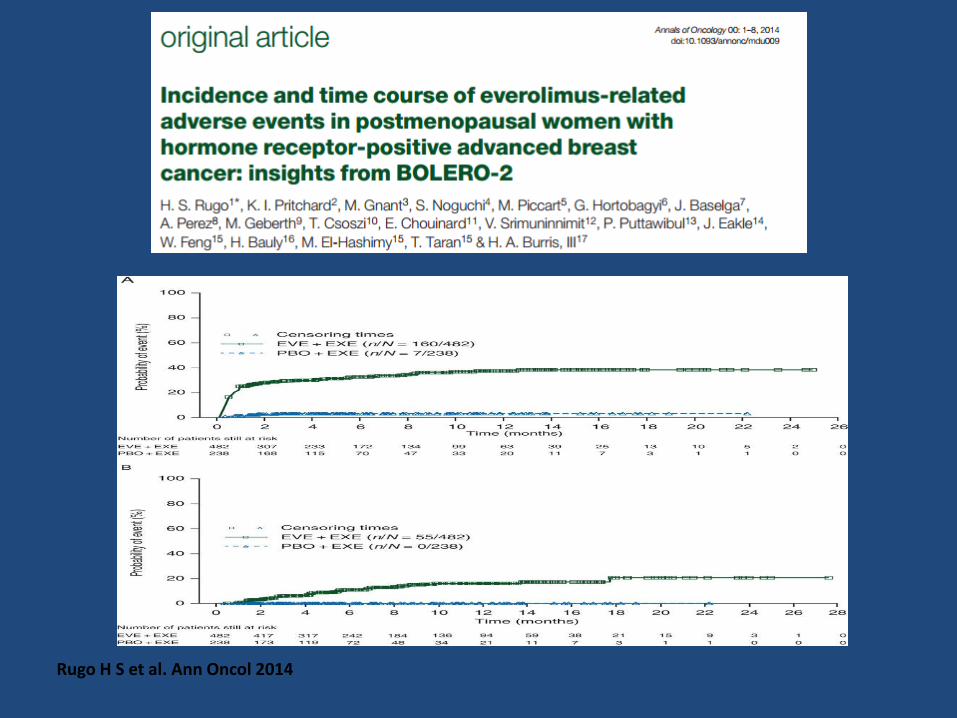
Rugo H S et al. Ann Oncol 2014

Hyperglycemia Management
• Monitorare i livelli di glucosio a digiuno prima di iniziare la terapia con everolimus e • periodicamente durante il trattamento
• Consigliare ai pazienti di segnalare sete eccessiva o aumento della minzione
• Evitare zuccheri a rapido assorbimento
Gestione dell’ Iperglicemia in riferimento alle linee guida: • Registrare e mantenere un valore glicemico nella norma (HbA1c <7%) • In caso di Iperglicemia modificare lo stile di vita e/o somministrare Metformina
• Intervenire subito farmacologicamente o cambiare classe di farmaci nel caso in cui il trattamento • non risulti efficace. • Somministrare Insulina in quei pazienti che non raggiungono il beneficio sperato con altre
terapie; • utilizzare Insulina a rapida azione solo nel caso in cui si somministrano STEROIDI
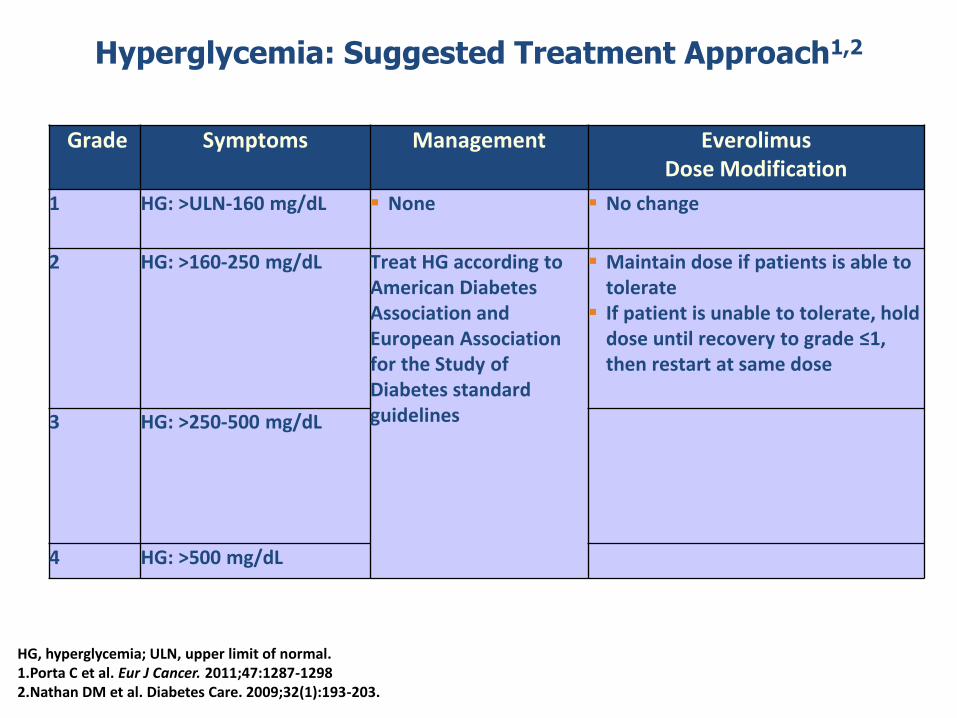
Hyperglycemia: Suggested Treatment Approach1,2
Grade Symptoms Management Everolimus Dose Modification
1 HG: >ULN-160 mg/dL None No change
2 HG: >160-250 mg/dL Treat HG according to American Diabetes Association and European Association for the Study of Diabetes standard guidelines
Maintain dose if patients is able to tolerate
If patient is unable to tolerate, hold dose until recovery to grade ≤1, then restart at same dose
3 HG: >250-500 mg/dL
4 HG: >500 mg/dL
HG, hyperglycemia; ULN, upper limit of normal. 1.Porta C et al. Eur J Cancer. 2011;47:1287-1298 2.Nathan DM et al. Diabetes Care. 2009;32(1):193-203.
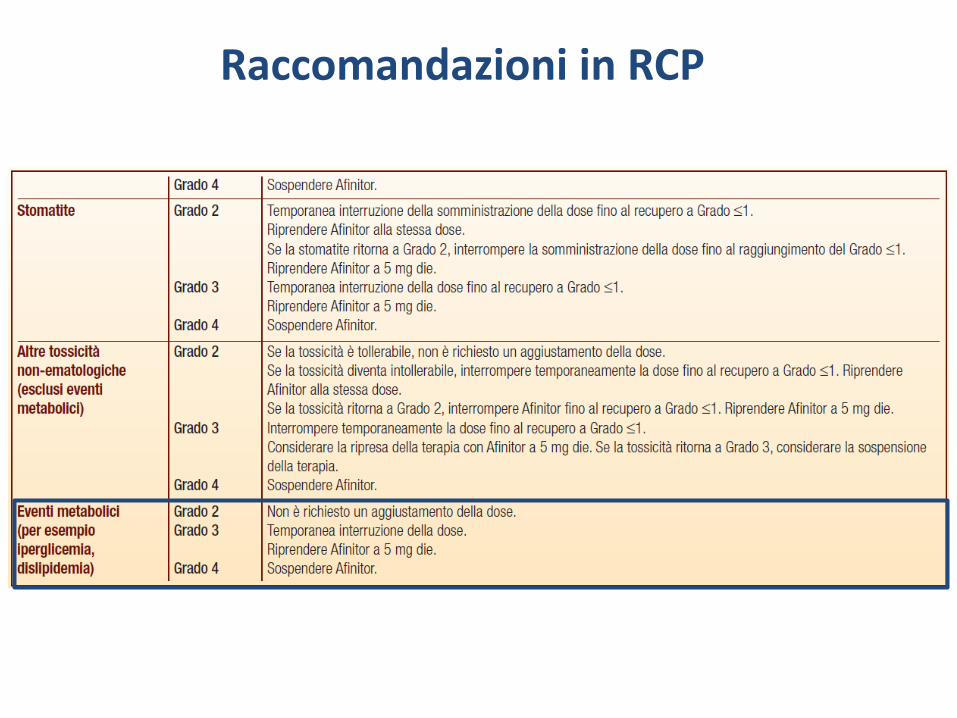
Raccomandazioni in RCP

Il provvedimento terapeutico adottato per la gestione dell’evento metabolico è corretto o potrebbero esserci ulteriori accorgimenti specifici da prendere in considerazione?
Ogni quanto sarebbe consigliabile effettuare un follow-up per il monitoraggio corretto di questo tipo di AE e con quali esami?
Discussione
È possibile stilare delle linee guida ideali da seguire (follow up, esami, ecc ecc) per poter ottimizzare il trattamento? O un PDTA ottimale? Prevenzione?
Discussione
Recommended