ORIGINAL ARTICLE
Five-year potency preservation after iodine-125 prostatebrachytherapy
Shuichi Nishimura • Atsunori Yorozu • Toshio Ohashi • Masanori Sakayori •
Yasuto Yagi • Toru Nishiyama • Shiro Saito • Yutaka Shiraishi • Kayo Yoshida •
Kazuhito Toya • Naoyuki Shigematsu
Received: 13 July 2013 / Accepted: 11 October 2013
� Japan Society of Clinical Oncology 2013
Abstract
Background We aimed to evaluate long-term erectile
function following prostate brachytherapy, based on patient
characteristics and treatment factors.
Methods Between 2003 and 2006, 665 men with local-
ized prostate cancer were treated with 125I permanent seed
implantation. None was given adjuvant hormone therapy.
Erectile function was assessed before treatment, and at
6 months, 1, 2, 3, 4 and 5 years after implantation using the
Mount Sinai Erectile Function Score (MSEFS) of 0–3
(0 = no erections, 1 = erections insufficient for inter-
course, 2 = suboptimal erections but sufficient for inter-
course, 3 = normal erectile function). Potency was defined
as score 2 or 3, and 382 men were potent before treatment.
Univariate and multivariate analyses were performed on
the data from these 382 patients to identify variables
associated with potency preservation.
Results In patients who were potent before treatment, the
actuarial potency preservation rate fell to 46.2 % at
6 months after brachytherapy, and then slowly recovered
reaching 52.0 % at 5 years after brachytherapy. In multi-
variate logistic regression analysis, patient age (p = 0.04)
and pre-treatment MSEFS (p \ 0.001) were predictors of
5-year potency preservation. Neoadjuvant hormone therapy
affected potency preservation only at 6 months after
brachytherapy.
Conclusions Patient age at implantation and pre-treatment
erectile function are predictive factors for the development
of erectile dysfunction following prostate brachytherapy.
Keywords Prostate cancer � Brachytherapy �Potency � Preservation
Introduction
Definitive therapies for patients with localized prostate
cancer include radical prostatectomy, conformal or exter-
nal beam radiation therapy (EBRT), and permanent pros-
tate brachytherapy. For patients with low-risk prostate
cancer, brachytherapy is as effective for disease control as
radical prostatectomy or EBRT [1, 2]. Penile erectile
function is an important consideration for many patients
when deciding on the therapy modality for their prostate
cancer. Compared to patients receiving prostatectomy or
EBRT, those given brachytherapy tend to have higher rates
of potency preservation [3–5]. Nevertheless, many patients
receiving brachytherapy experience varying degrees of
decreased erectile function after treatment. Identifying
factors affecting erectile function after brachytherapy is
important for patients trying to decide between the cur-
rently available therapies.
The rate of potency preservation after prostate brachy-
therapy depends on various clinical factors. According to a
recent study, racial differences may affect erectile function
after brachytherapy [6]. Though a few reports have focused
on brachytherapy-related erectile dysfunction (ED) [7–9],
S. Nishimura � A. Yorozu � M. Sakayori � K. Yoshida � K. Toya
Department of Radiology, National Hospital Organization
Tokyo Medical Center, 2-5-1 Higashigaoka, Meguro-ku,
Tokyo 152-8902, Japan
T. Ohashi (&) � Y. Shiraishi � N. Shigematsu
Department of Radiology, Keio University School of Medicine,
35 Shinanomachi, Shinjuku-ku, Tokyo 160-8582, Japan
e-mail: [email protected]
Y. Yagi � T. Nishiyama � S. Saito
Department of Urology, National Hospital Organization Tokyo
Medical Center, 2-5-1 Higashigaoka, Meguro-ku,
Tokyo 152-8902, Japan
123
Int J Clin Oncol
DOI 10.1007/s10147-013-0632-8

there have been no large-scale studies on this subject in
Asian countries.
In Japan, use of the iodine-125 (125I) seed source was
permitted in July 2003, and the first administration of I-125
prostate brachytherapy took place at our institution in
September of the same year. In this study, we evaluated the
5-year potency preservation rate in 665 consecutive
patients and analyzed factors predicting ED development.
Patients and methods
During the period from September 2003 through November
2006, we treated 665 consecutive patients with localized
prostate cancer at the National Hospital Organization
Tokyo Medical Center using 125I permanent seed implan-
tation. The following risk factors were assessed: prostate-
specific antigen (PSA) level, Gleason score and T-category
(according to the 1997 American Joint Commission on
Cancer). The subjects were divided into a low risk (T1–
T2a, PSA \10 ng/mL and Gleason score B6), an inter-
mediate risk (T2b–T2c, PSA = 10–20 or Gleason
score = 7) and a high risk (T3a, PSA [20 ng/mL or
Gleason score C8) group. For the low risk group, seed
implantation alone (monotherapy) was performed, whereas
for the intermediate and high risk groups a combination of125I seed implantation at a reduced radiation dose and
EBRT was preferred (combined therapy). The intermediate
risk group patients with PSA \10 ng/mL, Gleason
score = 7 and positive core needle biopsy rates \33 %
received monotherapy.
Neoadjuvant hormone therapy (HT) was administered to
538 patients (80.9 %) and consisted of a luteinizing hor-
mone-releasing hormone (LH-RH) agonist in 183 patients
(27.5 %), an antiandrogen in 209 (31.4 %) and both in 146
(22.0 %). The median duration of HT was 8 months (range
2–72). The proportion of subjects receiving HT was higher
in this than in past studies. There are three main reasons for
this difference. First, many of our patients had been waiting
to receive brachytherapy for a long time, in some cases for
more than a year; therefore, neoadjuvant HT was started
even in low risk patients. The second reason involves the
legal issue of discharge criteria in Japan: total seed activity
at the time of discharge must be lower than 1,300 MBq,
such that patients with pre-treatment prostate volumes
[40 mL have to undergo HT to achieve the cytoreduction
necessary to prevent prolonged hospitalization. Third, and
this is particularly true in Japan, HT is often started in both
early and advanced stages of prostate cancer. In the sur-
veillance study reported by the Japanese Urological
Association, 72.6 % of clinically-confirmed T1c–T3 cases
received HT [10]. On the other hand, none of our present
patients received adjuvant HT after implantation.
Of the 665 patients, the first 227 consecutive men were
treated by a preplanning technique, followed by 438 men
treated by an intraoperative technique. The prescribed dose
was 145 Gy in the monotherapy group and 100 Gy in the
combined therapy group. Our planning techniques have
previously been described in detail [11, 12], and there were
no significant differences in post-implant dosimetric results
between the two methods [13].
For post-implant dosimetric analysis, a computerized
tomography (CT) scan was obtained 1 month after
implantation. The calculated parameters used were the
percentage volume of the prostate receiving 150 % of the
prescribed dose (prostate V150) and the values of the
minimal dose received by 90 % of the prostate volume
(prostate D90). In the combined therapy group, supple-
mental EBRT was started 1 month after brachytherapy.
The prescribed EBRT doses were 45 Gy in 25 fractions of
1.8 Gy per fraction using 6 MV photons delivered by the
3D-conformal technique in the supine position, including
the prostate and seminal vesicles plus a 0.8-cm rectal-side
margin and a 1.5-cm margin on the other sides. The bio-
logically effective doses (BEDs) were calculated from the
prostate D90 and the EBRT dose using an a/b ratio of 2
(Gy2), applying the formulas described previously by
Stock et al. [14]. The total BED for the combination
therapy was the sum of the BED from the implant and that
from the EBRT.
Patients were reviewed clinically prior to treatment, at
6 months, and then yearly thereafter until 5 years post-
implantation. Six hundred and fifty-nine patients under-
went pre-implant and post-implant erectile function
assessments. Of them, 550 patients were assessed until
5 years after implantation. Erectile function was assessed
by medical interview or mailed questionnaire using the
Mount Sinai Erectile Function Score (MSEFS): 0, unable
to have erections; 1, erections insufficient for intercourse;
2, suboptimal erections but sufficient for intercourse; 3,
normal erectile function [15]. Potent was defined as an
MSEFS C2 with or without the use of a PDE-5 inhibitor,
and 382 men were potent before treatment. Patients who
had received neoadjuvant HT in other hospitals were
evaluated retrospectively by medical interview.
In this study, analyses were designed for patients who
were potent before treatment. The clinical and treatment-
related factors included patient age, pre-treatment MSEFS,
diabetes, pre-implant prostate volume, supplemental
EBRT, the utilization of neoadjuvant HT, prostate V150,
prostate D90 and total BED. Univariate analysis was per-
formed using an independent samples t test. Multivariate
analysis was performed using logistic regression analysis.
Analyses were carried out using SPSS 20.0 (SPSS Inc.,
Chicago, IL, USA). Differences were regarded as statisti-
cally significant at a p-value \0.05.
Int J Clin Oncol
123

Results
The clinical characteristics of patients are shown in
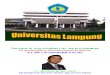
Table 1. In patients who were potent before treatment, the
rates of 6-month, 1-, 2-, 3-, 4- and 5-year potency preser-
vation were 46.2, 49.0, 51.0, 47.9, 49.3 and 52.0 %,
respectively (Fig. 1). The potency rate had fallen at
6 months, after which a gradual recovery trend was
observed. Of the patients who became impotent during the
course of follow-up, 109 were prescribed PDE-5 inhibitors,
in response to which 79 patients regained potency. None of
our patients received penile prostheses.
In logistic regression analysis, pre-treatment MSEFS
and utilization of neoadjuvant HT were associated with
potency preservation at 6 months (Table 2). Age, pre-
treatment MSEFS and diabetes mellitus were significant
factors at 1 year. Only age and pre-treatment MSEFS
remained significantly associated with potency preser-
vation at 5 years (Table 3), the same results as at
2–4 years.
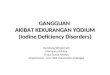
Neoadjuvant HT was considered to have played a role in
the potency rate decrease at 6 months. Compared to hor-
mone-naı̈ve patients, patients with antiandrogen therapy
alone showed no significant differences in potency pres-
ervation at 6 months (64.1 vs. 61.3 %, p = 0.718),
whereas those receiving LH-RH agonist, with or without
antiandrogen therapy, had a significantly lower rate of
potency preservation (30.9 %, p \ 0.001) (Fig. 2). There
were no significant differences among the hormone-naı̈ve
(59.3 %), antiandrogen therapy alone (55.0 %) and LH-RH
Table 1 Patient characteristics (n = 665)
Potent
(n = 382)
Impotent
(n = 277)
Age (years)
Mean (range) 65 (49–84) 70 (53–85)
Initial PSA (ng/mL)
Mean (range) 7.7 (1.1–43.3) 7.6 (3.5–38.9)
Pre-implant prostate volume (ml)
Mean (range) 20.5 (6.2–49.6) 20.6 (7.0–46.3)
MSEFS
0 0 147
1 0 130
2 190 0
3 192 0
Clinical stage
T1c–2a 311 (81.3 %) 227 (81.9 %)
T2b–2c 70 (18.4 %) 47 (17.0 %)
T3a 1 (0.3 %) 3 (1.1 %)
Gleason score
\7 222 (58.1 %) 117 (42.2 %)
=7 151 (39.5 %) 142 (51.3 %)
[7 9 (2.4 %) 18 (6.5 %)
Neoadjuvant hormone therapy 315 (82.5 %) 220 (79.4 %)
Diabetes mellitus 36 (9.4 %) 30 (10.8 %)
Supplemental EBRT 181 (47.4 %) 160 (57.8 %)
PSA prostate-specific antigen, MSEFS Mount Sinai Erectile Function
Score, EBRT external beam radiation therapy
Fig. 1 Rate of potency preservation after brachytherapy for patients
who were not impotent prior to treatment
Table 2 Univariate and multivariate analyses of factors affecting
6-month potency preservation rate
Factors Univariate
analysis
Multivariate analysis
p value Odds
ratio
95 % CIp value
Clinical
Age 0.001 0.195
Diabetes mellitus 0.571 0.672
Pre-treatment MSEFS
(2 vs 3)
0.001 0.001 4.017 2.548–6.335
Treatment-related
Pre-implant prostate
volume
0.669 0.328
Neoadjuvant hormone
therapy
0.001 0.001 3.635 2.187–6.041
EBRT 0.456 0.845
Dosimetric
Prostate V150 0.300 0.151
Prostate D90 0.980 0.834
Total BED 0.995 0.753
Age, pre-implant prostate volume, prostate V150, prostate D90 and total
BED were analyzed as continuous variables. Remaining covariates were
analyzed as categorical variables
95 % CI 95 % confidence interval, MSEFS Mount Sinai Erectile Function
Score, EBRT external beam radiation therapy, prostate V150 the percent
volume of the post-implant prostate receiving 150 % of the prescribed
dose, prostate D90 the minimum dose received by 90 % of the prostate
volume, BED biologically effective dose
Int J Clin Oncol
123

agonist with or without antiandrogen therapy (47.6 %)
cohorts at 5 years.
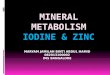
By age groups, patients B60 years old showed a good
potency preservation rate at 5 years (71.4 %), as compared
to those 61–70 and C71 years old (p \ 0.001). On the
other hand, there was no marked difference between the
61–70 and C71 year age groups (50.8 vs. 39.2 %,
p = 0.085) (Fig. 3).
Pre-treatment MSEFS correlated strongly with post-
treatment potency over the entire follow-up period. Patients
with an initial MSEFS = 3 and MSEFS = 2 had actuarial
5-year potency preservation rates of 74.7 and 27.7 %,
respectively (p \ 0.001) (Fig. 4).
Discussion
There are several scales for evaluating ED. In this study,
we used the MSEFS. This 4-point scoring system is con-
sidered to be reliable and is simple to apply. The
Table 3 Univariate and multivariate analyses of factors affecting
5-year potency preservation rate
Factors Univariate
analysis
Multivariate analysis
p value p value Odds
ratio
95 % CI
Clinical
Age 0.001 0.040 1.045 1.002–1.089
Diabetes mellitus 0.827 0.995
Pre-treatment
MSEFS (2 vs 3)
0.001 0.001 6.620 3.986–10.996
Treatment-related
Pre-implant
prostate volume
0.124 0.084
Neoadjuvant
hormone therapy
0.097 0.835
EBRT 0.007 0.077
Dosimetric
Prostate V150 0.100 0.536
Prostate D90 0.257 0.192
Total BED 0.061 0.267
Age, pre-implant prostate volume, prostate V150, prostate D90 and
total BED were analyzed as continuous variables. Remaining covar-
iates were analyzed as categorical variables
95 % CI 95 % confidence interval, MSEFS Mount Sinai Erectile
Function Score, EBRT external beam radiation therapy, prostate V150
the percent volume of the post-implant prostate receiving 150 % of
the prescribed dose, prostate D90 the minimum dose received by
90 % of the prostate volume, BED biologically effective dose
Fig. 2 Rate of potency preservation stratified by neoadjuvant
hormone therapies. Open circles indicate hormone-naı̈ve patients.
Plus symbols correspond to patients receiving an antiandrogen
prescription. Triangles correspond to patients receiving LH-RH
agonist with or without an antiandrogen. Vertical bars represent
95 % confidence interval
Fig. 3 Rate of potency preservation stratified by patient age at the
time of implantation. Open circles indicate patients B60 years old.
Plus symbols represent patients 61–70 years old. Triangles represent
patients C71 years old. Vertical bars represent 95 % confidence
interval
Fig. 4 Rate of potency preservation stratified by pre-implant Mount
Sinai Erectile Function Scores (MSEFS). Open circles indicate
patients with MSEFS = 3. Plus symbols represent patients with
MSEFS = 2. Vertical bars represent 95 % confidence interval
Int J Clin Oncol
123

International Index of Erectile Function (IIEF) is also
widely used for evaluating ED, and Zagar et al. [16]
showed MSEFS results to correlate strongly with those of
the IIEF.
Various studies have assessed sexual function after
prostate brachytherapy. Five-year potency preservation
rates in patients who were potent before treatment were
reportedly 50–60 % [17, 18], similar to our result (52.0 %).
Snyder et al. [19] reported a higher 5-year potency pres-
ervation rate of 68.0 %. One reason for this difference
might be the use of PDE-5 inhibitors (740 of 1063 patients
at Mount Sinai vs. 109 of 659 at our institution).
Age had a strong impact on erectile function, with a
32.2 % lower 5-year potency preservation rate for patients
older than 70, compared with patients who were\61 years
old. Taira et al. [17] reported 7-year potency preservation
rates of 73.5, 48.1 and 33.3 % for men \60, 60–70 and
[70 years old, respectively. Our results showed the same
tendency for age groups. Furthermore, Kollmeier et al. [20]
reported post-brachytherapy erectile function in men
B60 years old to be favorable and that the majority did not
require medications.
Patients with an initial MSEFS = 3 had a 47.0 % higher
5-year potency preservation rate than those with
MSEFS = 2. This tendency was previously demonstrated
by Stock, Stone and colleagues [8, 15]. Snyder et al.
reported that patients with an initial MSEFS = 3 had a
22.5 % higher rate of potency preservation than those with
MSEFS = 2. This dependence on pre-treatment potency
status was also demonstrated by Merrick et al. [9]. They
reported 3-year potency preservation rates for patients with
pre-implant IIEF scores of 24–30, 18–23 and 13–17 to be
57.6, 48.0 and 22.1 %, respectively.
Previous studies have shown that neoadjuvant HT with
EBRT or brachytherapy was associated with long-lasting
sexual symptoms [3]. We recommend that patients, espe-
cially young men, waiting for brachytherapy receive neo-
adjuvant antiandrogen therapy in terms of potency
preservation, because no actuarial difference was seen in
our study between the hormone-naı̈ve cohort and that
receiving only antiandrogen therapy. We also found that
erectile function of patients with neoadjuvant LH-RH
agonist therapy decreased at 6 months, but improved at
1–5 years after brachytherapy. To our knowledge, this
outcome has not previously been reported.
A correlation between additional EBRT and potency
preservation has been suggested [18, 19]. On the other
hand, there are also data suggesting that no actuarial cor-
relation exists between additional EBRT and potency
preservation [9, 17]. In our univariate analysis, patients
receiving monotherapy had a higher actuarial 5-year
potency preservation rate than those given the combination
of EBRT and brachytherapy (59.2 vs. 44.4 %, p = 0.007).
In our multivariate analysis, however, we found no sig-
nificant difference in potency rate with the addition of
EBRT (p = 0.077). This might be explained by con-
founding factors such as hormone therapy, as numerous
patients given the combination therapy also received neo-
adjuvant HT.
In our study, 109 patients were prescribed PDE-5
inhibitors. This prescription rate was lower than that in the
study at Mount Sinai Hospital [19], possibly reflecting a
difference in attitudes towards sexual issues among nations
or races. Zelefsky et al. [21] reported that sildenafil was
associated with a 74 % response rate, a significant increase
compared to no treatment, in patients with ED after
radiotherapy for localized prostate cancer, and that patients
with less severe ED after radiotherapy were more likely to
respond than those with complete absence of erectile
function. Early use of PDE-5 inhibitors after prostatectomy
or brachytherapy reportedly improves IIEF scores, and
contributes to rapid recovery of erectile function [22, 23].
These data also suggested that patients might be more
likely to benefit from earlier (i.e., before their potency
scores decrease) and more aggressive use of PDE-5
inhibitors.
The limitations of this study include medical interview
bias. The initial assessments might have been unreliable
when the patients were asked to recall erectile function
prior to treatment, especially if they had received hormone
therapy at other hospitals. Accordingly, appropriate pre-
treatment evaluations are needed employing a detailed
questionnaire about the sexual functions of individual
patients.
Conclusion
Over a 5-year follow-up period, 52.0 % of patients with
prostate brachytherapy maintained their potency. On mul-
tivariate analysis, patient age at implantation and pre-
treatment erectile function score were associated with
5-year potency preservation. Although neoadjuvant LH-RH
agonist therapy affected the 6-month actuarial potency
preservation rate, no definite impact on this rate was seen at
5 years after implantation. In addition, over the entire study
period, no significant differences were seen between
patients receiving no hormone therapy and those given
antiandrogen treatment alone.
Acknowledgments The authors are grateful to Ms. Kazuko Ogawa
at Keio University School of Medicine for her support and assistance.
Conflict of interest The authors declare that they have no conflict
of interest.
Int J Clin Oncol
123

References
1. Kupelian PA, Potters L, Khuntia D et al (2004) Radical prosta-
tectomy, external beam radiotherapy \ 72 Gy, external beam
radiotherapy C72 Gy, permanent seed implantation, or combined
seeds/external beam radiotherapy for stage T1–T2 prostate can-
cer. Int J Radiat Oncol Biol Phys 58:25–33
2. Peschel RE, Colberg JW (2003) Surgery, brachytherapy, and
external-beam radiotherapy for early prostate cancer. Lancet
Oncol 4:233–241
3. Sanda MG, Dunn RL, Michalski J et al (2008) Quality of life and
satisfaction with outcome among prostate-cancer survivors.
N Engl J Med 358:1250–1261
4. Robinson JW, Moritz S, Fung T (2002) Meta-analysis of rates of
erectile function after treatment of localized prostate carcinoma.
Int J Radiat Oncol Biol Phys 54:1063–1068
5. Crook JM, Gomez-Iturriaga A, Wallace K et al (2011) Compar-
ison of health-related quality of life 5 years after SPIRIT: sur-
gical prostatectomy versus interstitial radiation intervention trial.
J Clin Oncol 29:362–368
6. Alemozaffar M, Regan MM, Cooperberg MR et al (2011) Pre-
diction of erectile function following treatment for prostate can-
cer. JAMA 306:1205–1214
7. Zelefsky MJ, Hollister T, Raben A et al (2000) Five-year bio-
chemical outcome and toxicity with transperineal CT-planned
permanent I-125 prostate implantation for patients with localized
prostate cancer. Int J Radiat Oncol Biol Phys 47:1261–1266
8. Stone NN, Stock RG (2007) Long-term urinary, sexual, and rectal
morbidity in patients treated with iodine-125 prostate brachy-
therapy followed up for a minimum of 5 years. Urology
69:338–342
9. Merrick GS, Butler WM, Wallner KE et al (2005) Erectile
function after prostate brachytherapy. Int J Radiat Oncol Biol
Phys 62:437–447
10. Cancer Registration Committee of the Japanese Urological A
(2005) Clinicopathological statistics on registered prostate cancer
patients in Japan: 2000 report from the Japanese Urological
Association. Int J Urol 12:46–61
11. Ohashi T, Yorozu A, Toya K et al (2005) Acute urinary morbidity
following I-125 prostate brachytherapy. Int J Clin Oncol
10:262–268
12. Ohashi T, Yorozu A, Toya K et al (2007) Rectal morbidity fol-
lowing I-125 prostate brachytherapy in relation to dosimetry. Jpn
J Clin Oncol 37:121–126
13. Yoshida K, Ohashi T, Yorozu A et al (2013) Comparison of
preplanning and intraoperative planning for I-125 prostate
brachytherapy. Jpn J Clin Oncol 43:383–389
14. Stock RG, Stone NN, Cesaretti JA et al (2006) Biologically
effective dose values for prostate brachytherapy: effects on PSA
failure and posttreatment biopsy results. Int J Radiat Oncol Biol
Phys 64:527–533
15. Stock RG, Kao J, Stone NN (2001) Penile erectile function after
permanent radioactive seed implantation for treatment of prostate
cancer. J Urol 165:436–439
16. Zagar TM, Stock RG, Cesaretti JA et al (2007) Assessment of
postbrachytherapy sexual function: a comparison of the IIEF-5
and the MSEFS. Brachytherapy 6:26–33
17. Taira AV, Merrick GS, Galbreath RW et al (2009) Erectile
function durability following permanent prostate brachytherapy.
Int J Radiat Oncol Biol Phys 75:639–648
18. Potters L, Torre T, Fearn PA et al (2001) Potency after permanent
prostate brachytherapy for localized prostate cancer. Int J Radiat
Oncol Biol Phys 50:1235–1242
19. Snyder KM, Stock RG, Buckstein M et al (2012) Long-term
potency preservation following brachytherapy for prostate cancer.
BJU Int 110:221–225
20. Kollmeier MA, Fidaleo A, Pei X et al (2013) Favourable long-
term outcomes with brachytherapy-based regimens in men
B60 years with clinically localized prostate cancer. BJU Int
111:1231–1236
21. Zelefsky MJ, McKee AB, Lee H et al (1999) Efficacy of oral
sildenafil in patients with erectile dysfunction after radiotherapy
for carcinoma of the prostate. Urology 53:775–778
22. Bannowsky A, Schulze H, van der Horst C et al (2008) Recovery
of erectile function after nerve-sparing radical prostatectomy:
improvement with nightly low-dose sildenafil. BJU Int
101:1279–1283
23. Pahlajani G, Raina R, Jones JS et al (2010) Early intervention
with phosphodiesterase-5 inhibitors after prostate brachytherapy
improves subsequent erectile function. BJU Int 106:1524–1527
Int J Clin Oncol
123
Recommended