MR2 OSCAR MALPARTIDA TABUCHIENFERMEDADES INFECCIOSAS Y
TROPICALESHNGAI-UPCH
11 DE JULIO 2015
Servicio de nefrologia HNGAIUnidad Investigación y docencia
Nefropatía asociada al HIV


Introducción
35 millones infectados con HIV en el mundo24.7 millones en SAA12.9 (37% en TARV)

Definición: HIVAN (clásico)
Es una forma de glomerulopatía colapsante (glomeruloscerosis FS)
Relacionada HIV-1Más común en raza negra, estadios
avanzados
Otras enfermedades HIVICK, microangiopatía y alteraciones/toxicidad por ARV.

Perla clínica HIVAN
“Paciente joven, ascendencia africana, CV-HIV elevada, enfermedad renal de rápida progresión a ESRD, riñones grandes”

Efecto de TARV
HIVAN asociado a inmunosupresión severaEEUU: 60% disminución de ERC-V en era
post TARVTARV/envejecimiento produce nuevo patrón
de CKD (inflamación crónica)Nefrotoxicidad asociada a TARV: Tenofovir y
cristaluria/litiasis asociada a IP

Histopatología
HIVAN clásico: glomerulopatía colapsanteEnfermedades renales asociadas a HIV tienen
un amplio espectro histológico Alteraciones glomerulares, tubulointersticiales Asociado a TARV Comorbilidades asociadas (HCV, CV, DM, CMV)

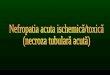
Histopatología HIVAN
Colapso de capilares glomerularesEpiteliosis visceral glomerularHipertrofia y proliferación podocitosHipercelularidad y prominencia
mesangialInclusiones tubuloreticulares endoteliales TRI

Histopatología
HIVAN clásico puede verse en cualquier grupo etáreo y estadio
Más común en estadios avanzados y descendientes África Occidental (2º Hispano)
HIVICK y formas no colapsantes luego de TARV
HIVICK en poblaciones europeas

Background. Treatment and co-morbidities of human immunodeficiency virus (HIV)-infected individuals have changed dramatically in the last 20 years with a potential impact on renal complications. Our objective was to assess the change in distribution of the glomerular diseases in HIV patients. Methods. We retrospectively analysed demographic, clinical, laboratory and renal
histopathological data of 88 HIV-infected patients presenting with a biopsy-proven glomerular disease between 1995 and 2007.
Results. In our study including 66% Black patients, HIV-associated nephropathy (HIVAN) was observed in 26 cases, classic focal segmental glomerulosclerosis (FSGS) in 23 cases, immune complex glomerulonephritis in 20 cases and other glomerulopathies in 19 patients. HIVAN decreased over time, while FSGS emerged as the most common cause of glomerular diseases (46.9%) in HIV-infected individuals undergoing kidney biopsy in the last 2004–07 period. Patients with HIVAN were usually Black (97%), with CD4 <200/mL (P = 0.01) and glomerular filtration rate <30 mL/min/1.73m2 (P < 0.01). Compared to HIVAN, patients with classic FSGS were less often Black (P < 0.01), have been infected for longer (P = 0.03), were more often co-infected with hepatitis C virus (P = 0.05), showed more often cardiovascular (CV) risk factors (P < 0.01), had less often CD4 <200/mL (P = 0.01), lower HIV viral load (P = 0.01) and tended to be older (P = 0.06).
Conclusions. Classic FSGS associated with metabolic and CV risk factors has overcome HIVAN in HIV-infected patients. Compared with other glomerulopathies, HIVAN remains strongly associated with severe renal failure, Black origin and CD4 lower than 200/mL at presentation.

Histopatología

Etiopatogenia
HIVAN: cDNA-HIV y proteínas virales en células renales
Inducen muerte celular y apoptosisHIVICK (?)APOL1 en ascendencia africana.Entrada?
CD209 podocitos/células dendríticas Ag linfocitario 75 (DEC205), c. tubulares

Etiopatogenia

Screening y detección temprana
Clinical Practice Guideline for the Management of Chronic Kidney Disease in Patients Infected With HIV: 2014 Update by the HIV Medicine Association of the Infectious Diseases Society of America
HIV asociado a mayor riesgo de ERCPA, SrCr (eGFR y albuminuria en TDF) Proteinuria/creatinuria +
albuminuria/creatinuriaSe debe tamizar para e. renal incipiente:
HIVAN, y otras glomerulo-tubulopatíasCuándo?
Al diagnóstico Antes de iniciar TARV Dos veces al año en pacientes estables o que modifican
TARV


Utilidad Biopsia renal
Berliner A.R. · Fine D.M. · Lucas G.M. · Rahman M.H. · Racusen L.C. · Scheel P.J. · Atta M.G. Observations on a Cohort of HIV-Infected Patients Undergoing Native Renal Biopsy Am J Nephrol 2008;28:478–486
No toda ERC con proteinuria y disminución en función renal es HIVAN
Hallazgos (eco, proteinuria, CD4) no predicen de forma confiable su presencia
Decisión terapéutica es guiada por histopatología (TARV probado en HIVAN, en otras?)
Dependerá de posibilidad de diagnósticos alternativos, que puedan cambiar terapia y de riesgo/beneficio

AIMS: This study aims to explore the spectrum of renal disease in HIV-infected patients, identify clinical predictors of
HIV-associated nephropathy (HIVAN), and investigate the performance of renal biopsy in HIV-infected patients. METHOD: Of 263 HIV-infected patients with renal disease evaluated between 1995 and 2004, 152 had a renal biopsy,
while 111 had not. A group comparison was performed. RESULTS: The leading biopsy diagnoses were HIVAN (35%), noncollapsing focal segmental glomerulosclerosis (22%), and
acute interstitial nephritis (7.9%), amongst over a dozen others. There was a trend of decreasing yearly incidence of HIVAN diagnoses, paralleling the use of antiretroviral therapy. By multivariate logistic regression, CD4 counts >200 cells/mm(3) and higher estimated glomerular filtration rate were strong negative predictors of HIVAN. HIVAN patients were more likely to require dialysis (p < 0.0001) and had worse overall survival (p = 0.02). Younger age and lower estimated glomerular filtration rate were significant predictors of renal biopsy in multivariate regression analysis. More biopsied patients progressed to dialysis (51 vs. 25%, p = 0.001) and death (15 vs. 5.4%, p = 0.001), despite more frequent corticosteroid treatment (29 vs. 3.6%, p = 0.001).
CONCLUSION: These findings may reflect more severe acute and/or chronic disease at the time of biopsy and
suggests that earlier renal biopsy may be warranted in HIV-infected patients, especially in light of the changing spectrum of renal disease in this group.

Tratamiento
ARVManejo de enfermedades renales asociadasTerapia de reemplazo renalTransplante

TARV
Antes de era TARV, HIVAN progresaba inexorablemente a ESRD
HIVAN es una indicación de TARV (CD4)Beneficio en HIVICK, microangiopatía
trombóticaSe ha observado mejora de eGFR en
pacientes en TARV y ERC



Manejo adicional1. Corticoides
En los primeros años de la epidemia se utilizaron corticoides con resultados modestos
Información con alto poder estadístico escasa
PDN 1mg/kg/díaIO vs necrosis avascularEscasa información era TARV (beneficio
añadido?)

Cohort study of the treatment of severe HIV-associated nephropathy with corticosteroids. Background Human immunodeficiency virus-associated nephropathy (HIVAN) results in rapidly progressive
azotemia. The effectiveness and safety of corticosteroids in the treatment of HIVAN, however, remains controversial.
Methods We conducted a retrospective cohort study of patients with biopsy-proven HIVAN and progressive
azotemia who were eligible for corticosteroid treatment and who had no clinical or histologic evidence of an alternative cause of acute renal failure. Selected patients were treated with 60 mg of prednisone for one month, followed by a several-month taper.
Results Twenty-one eligible patients were identified. Thirteen subjects had received corticosteroid treatment,
whereas eight had not. The mean serum creatinine was 6.2 and 6.8 mg/dL, respectively (P > 0.05). The relative risk (95% CI) for progressive azotemia with corticosteroid treatment at three months was 0.20 (0.05, 0.76, P < 0.05). This association remained significant despite adjustment in separate logistical regression analyses for baseline creatinine, 24-hour proteinuria, CD4 count, history of intravenous drug use, hepatitis B, and hepatitis C. In an additional logistic regression model, using backward stepwise selection of the previously mentioned covariates, only corticosteroid treatment (P = 0.02) and baseline serum creatinine (P = 0.10) were retained within the model. In the corticosteroid-treated group, the mean level of proteinuria decreased by 5.5 g/24 hour (P= 0.01). On long-term follow-up, there was no significant difference in the incidence of hospitalizations (1 per 2.1 vs. 1 per 2.3 patient months) or of serious infections (1 per 2.6 vs. 1 per 2.3 patient months), but there was a significantly longer duration of hospitalization in the corticosteroid-treated group (3.2 vs. 2 days per patient month). At six months, only one of the non–corticosteroid-treated patients but seven of the corticosteroid-treated group continued to have independent renal function (P = 0.06). Three of the corticosteroid-treated group continued to have independent function at two years of follow-up.

Regimen recomendado
Clinical Practice Guideline for the Management of Chronic Kidney Disease in Patients Infected With HIV: 2014 Update by the HIV Medicine Association of the Infectious Diseases Society of America
PDN 1mg/kg/día por 1-4 semanas y si responden se prolonga hasta 11 semanas y luego retirados en 2-26 semanas

Manejo adicional2. IECA/ARB
Clinical Practice Guideline for the Management of Chronic Kidney Disease in Patients Infected With HIV: 2014 Update by the HIV Medicine Association of the Infectious Diseases Society of America
ATI- ATII tienen un rol patogénico directo in vivo en modelos animales

Manejo adicional3. Medidas generales
Clinical Practice Guideline for the Management of Chronic Kidney Disease in Patients Infected With HIV: 2014 Update by the HIV Medicine Association of the Infectious Diseases Society of America
Control de PA<140/90Evitar nefrotóxicosPérdida de peso en obesosNo fumar

Terapia de reemplazo renal
Recommendations for Preventing Transmission of Infections Among Chronic Hemodialysis Patients CDC 2001
Pacientes con TARV en TRR (HD-PD) tienen tasas de supervivencia similares a controles
HD vs PD no hay diferencia en morbi-mortalidad
Infecciones CAPD ? No parece haber mayor riesgo…
Precauciones universales para prevención de infecciones en HD

Abstract Background Controversy continues concerning the morbidity and mortality of HIV-infected ESRD patients on the two
dialysis options. This article presents our experience with complications and survival rate among our HIV-infected ESRD patients on peritoneal dialysis and hemodialysis. We reviewed the literature on this subject.
Methods The charts of seven and eight HIV-infected ESRD patients on peritoneal dialysis and hemodialysis
respectively, between January 1989 and November 2004, were reviewed retrospectively for specific clinical and demographic data. Their survival was calculated using the Kaplan-Meier method.
Results Total follow-up of HIV-infected PD and HD patients was 248.3 and 207 patient months, respectively. There
was no significant difference in hospitalization rate between HIV-infected PD and HD patients (1.01 and 1.39 admission/year, respectively, P = NS). Survival of HIV-infected patients on PD at one, two and three years was 100, 83, and 50%, and for HD patients was 75, 33, and 33%, respectively. HIV-infected patients on HD had more prevalent advanced HIV disease. Two out of seven PD patients were on PD for more than five years and one of the HD patients was on that form of dialysis for more than nine years. Median survival of patients with advanced (Stage IV) AIDS (both HD and PD) was 15.1 months (range 1.6–17.3) while this value for non-advanced (Stage II, III) patients was 61.2 months (range 6.8–116.6).
Conclusion Type of renal replacement therapy does not have a significant effect on the morbidity and mortality of
HIV-infected ESRD patients. Survival is worse in patients with advanced HIV disease. Both dialysis options provide similar results in HIV patients; hence, the choice of dialysis modality should be based on patient’s preference and social conditions.

Transplante renal
Outcomes of kidney transplantation in HIV-infected recipients. NEJM 2010
Se puede realizar en HIV150 casos en EEUUMayores tasas de rechazo agudo (31%)Supervivencia del injerto a los 2 y 3 años de
88.2-73.7% respectivamente



GRACIAS
Recommended