Inhibidores de la tisosinquinasa de Bruton en el tratamiento de los linfomas Andrés López Servici d’Hematología Vall d’Hebron Institut de Reçerca (VHIR) Universitat Autónoma de Barcelona (UAB)
Hematology Department

Outline 1. History 2. BTK function 3. Ibrutinib
a. Mechanisms of action b. Phase I c. Phase II d. Safety e. Expansion
• First line CLL • Mutated p53 in CLL • Other LPS’s
f. Approval g. Mechanisms of resistance h. Optimization (Association) i. Possible new synergistic drugs j. Thoughts

History

Ogden Bruton Carr (1908-2033) pediatrician and chief of pediatrics at Walter Reed Army Hospital. He discovered "Bruton-type agammaglobulinemia"
PEDIATRICS Vol. 9 No. 6 June 1, 1952 pp. 722 -8
History

History

Other names: AT, ATK, BPK, IMD1, MGC126261, MGC126262, PSCTK1, XLA
Localización cromosómica: Xq22.1 The BTK protein is a 77 kDa protein of 659 amino acids The gene spans over 36 kb and is composed of 19 exons
BTK

Mechanisms of Action

Its exact Mechanism of action remains unknown, but it plays a crucial role in B-cell maturation. BTK binds PIP3. PIP3 binding induces BTK to phosphorylate phospholipase C (PLC), which in turn hydrolyzes PIP2 into two second messengers: IP3 and DAG, which then go on to modulate the activity of downstream proteins during B-cell signalling.
BTK

BTK in BCR and TLR downstream

Molecule Developer Stage of developement PCI-32765 Pharmacyclics / Janssen Approved ONO-405* ONO/Gelead Phase I CC-292 Celgene Phase I BGB-31111 Bei Gene/Merck Serono Phase I ACP-1961 Acerta Pharma BV Phase I CNX-774 Avila Therapeutics Lab. CGI-1746 Genentech Lab. RN-486 Hoffman-La Roche Animal GDC-0834 Genentech Animal LFM-A132 Lab. Hematol. Rotterdam Lab.
*. Reversible binding 1. Have a lower binding to ITK 2. Dual BTK and Jak2 inhibitor
BTK inhibitors

Ibrutinib

Celera Genomics
Ibrutinib (PCI-32765) is currently under development and delivery by Pharmacyclics, Inc, and Johnson & Johnson’ Janssen Pharmaceutical
Ibrutinib. A First in Class BTK inhibitor

Ibrutinib inhibits BTK function by irreversible binding to Cys481 region
Ibrutinib binding

Ibrutinib deregulates CXCR4 surface membrane expression by preventing its phosphorilation
Ibrutinib

Ibrutinib diminishes cellular response to tissue homing chemokines: CXCL12, CXCL13 and CCL19
Ibrutinib

BTK and ITK have similar domain organization
Ibrutinib

Dubovsky et al Blood 2013; 122: 2539-49
Ibrutinib

Ibrutinib inhibits ITK in T-cells
Ibrutinib

ITK function in T helper cell differentiation.
Andreotti et al. Cold Spring Harb Perspect Biol 2010;2:a002287
Ibrutinib

Ibrutinib
April 7th, 2015
PubMed: 286 articles ClinicalTrials.org: 92 CT

Ibrutinib. Phase I

Activity of Ibrutinib on different lymphomas Phase I: 2 doses: 560 and 420
56 pts
Advani et al. J Clin Oncol 2012; 31:88-94
Ibrutinib

Ibrutinib. Phases II

Targeting BTK with Ibrutinib in Relapsed Chronic Lymphocytic Leukemia
Byrd et al. N Engl J Med. 2013; 369:32-42
N Engl J Med, 2013

ALC: absolute lymphocyte count. SPD: sume of the products of lymph node diameters Byrd et al N Engl J Med 2013; 369: 32-42
Ibrutinib in Relapsed CLL/SLL. Phase Ib-II
Ibrutinib in CLL/SLL

Byrd et al N Engl J Med 2013; 369: 32-42
Curves for cumulative best response
Ibrutinib in Relapsed CLL/SLL. Phase Ib-II
Ibrutinib in CLL/SLL

Byrd et al N Engl J Med 2013; 369: 32-42
Ibrutinib in Relapsed CLL/SLL. Phase Ib-II
Ibrutinib in CLL/SLL

Byrd et al N Engl J Med 2013; 369: 32-42
Ibrutinib in Relapsed CLL/SLL. Phase Ib-II
Ibrutinib in CLL/SLL

Byrd et al. ASH 2014
Ibrutinib in Relapsed CLL/SLL. Phase II
Prolonging therapy, additional 20% with 420 mg dose and 15% with 840 mg dose achieved a PR with lymphocytosis
These results leaded to an expansion cohort of 117 patients. After a mFU of 20.5 months, the ORR was 88.3% (with an additional 5.4% of PR with lymphocytosis)
Ibrutinib in CLL/SLL

Targeting BTK with Ibrutinib in Relapsed or Refractory
Mantle Cell Lymphoma
ML Wang, S Rule, P Martin, A Goy, R Auer, BS Kahl, W Jurczak, RH Advani, JE Romaguera, ME Williams, JC Barrientos, E Chmielowska,
J Radford, S Stilgenbauer, M Dreyling, WW Jedrzejczak, P Johnson, SE Spurgeon, L Li, L Zhang, K Newberry, Z Ou, N Cheng, B Fang, J McGreivy,
F Clow, JJ Buggy, BY Chang, DM Beaupre, LA Kunkel, KA Blum
N Engl J Med. 2013.
Wang M, et al. N Engl J Med. 2013; 369:507-516

Study Design
Cohort 1 560 mg/d ibrutinib
No prior treatment with* (n = 65)
* Or less than 2 complete cycles
Cohort 2 560 mg/d ibrutinib
Prior treatment with bortezomib†
(n = 50) † at least 2 previous complete cycles
Recruiting: Feb. 2011Mar. 2012
• Phase 2, open, international multicenter (18 centers).
• Patients with relapsed or refractory MCL
• (n = 115)
• Patients received a daily dose of ibrutinib until disease progression or unacceptable toxicity (SAEs)
Wang M, et al. N Engl J Med. 2013; 369:507-516
Ibrutinib in MCL

Patient characteristics (I) No prior therapy with Bortezomib
(n = 63)
Prior therapy with Bortezomib
(n = 48)
All patients (N = 111)*
Age, years Median (range)
66 (46-83)
69 (40-84)
68 (40-84)
Sex, n (%) Male Female
46 (73) 17 (27)
39 (81) 9 (19)
85 (77) 26 (23)
ECOG performance status, n (%) 0-1 2 >2
53 (84) 9 (14) 1 (2)
46 (96)
2 (4) 0
99 (89) 11 (10)
1 (1)
Prior regimens Median (range) ≥ 3 regimens, n (%)
2 (1-5) 31 (49)
3 (1-5) 30 (62)
3 (1-5) 61 (55)
Refractory disease, n (%)† 27 (43) 23 (48) 50 (45)
*Four patients were excluded by investigator decition and did not receive Ibrutinib. †Refractory disease defined as lack of at least a PR to prior therapy of entering in the study
Wang M, et al. N Engl J Med. 2013; 369:507-516
Ibrutinib in MCL

Patient characteristics (II) No prior therapy with Bortezomib
(n = 63)
Prior therapy with Bortezomib
(n = 48)
All patients (N = 111)*
Type of prior therapy, n (%) Hyper-CVAD SCT Lenalidomide Rituximab†
18 (29) 8 (13) 9 (14)
56 (89)
15 (31)
4 (8) 18 (38) 43 (90)
33 (30) 12 (11) 27 (24) 99 (89)
Simplified MIPI, n (%) Low Risk Intermediate Risk High Risk
9 (14)
24 (38) 30 (48)
6 (12)
18 (38) 24 (50)
15 (14) 42 (38) 54 (49)
Bulky disease (diameter ≥ 10 cm), n (%) 6 (10) 3 (6) 9 (8)
At least 1 lymph node ≥ 5 cm, n (%) 26 (41) 17 (35) 43 (39)
Advanced disease, n (%)‡ 49 (78) 31 (65) 80 (72)
*Four patients were excluded by investigator decition and did not receive Ibrutinib. † Rituximab as single agent or in combination are included. ‡Advanced disease defined as bone marrow, or extranodal involvement or both
Ibrutinib in MCL
Wang M, et al. N Engl J Med. 2013; 369:507-516

Distribution of patients All patients (N = 111)
Follow-up Median (range), months
15.3 (1.9-22.3)
Patients still on treatment, n (%) 46 (41)
Patients who discontinued, n (%) 65 (59)
For progression, n (%) Other causes, n (%) AE’s Patient/Investigator ‘s decisión
50 (45)*
15 (14) 8 (7)†
7 (6)‡
*Two patients discontinuing before 30 days form the first dose and 1 unconfirmed disease progression are included. †2 subdural hematomas and 1 pneumonia, bilirubin elevated, sepsis, matastatic adenocarcinoma, respiratory failure and cardiac arrest. ‡1 patient undergone to a SCT is included
Ibrutinib in MCL
Wang M, et al. N Engl J Med. 2013; 369:507-516

n (%) All Pacients (N = 111)
SAE’s emerging from treatment 62 (56)
Infections Pneumonia UTI
22 (20) 6 (5) 4 (4)
General disorders Peripheral edema Pyrexia
11 (10) 3 (3) 3 (3)
Neoplasia MCL
10 (9) 8 (7)
*Events at least in 2% of patients. UTI: urinary tract infection
Safety: SAEs*
Wang M, et al. N Engl J Med. 2013; 369:507-516
Ibrutinib in MCL

n (%) All Pacients (N = 111)
Blood/lymphatic Febrile neutropenia
9 (8) 3 (3)
Cardiac Atrial fibrillation
8 (7) 5 (5)
Gastrointestinal Abdominal pain
8 (7) 3 (3)
Renal/urinary Acute renal failure
6 (5) 3 (3)
Injury/Poisoning/Procedural Subdural hematoma
5 (5) 3 (3)
*Events at least in 2% of patients. UTI: urinary tract infection
Safety: SAEs*
Wang M, et al. N Engl J Med. 2013; 369:507-516
Ibrutinib in MCL

0
10
20
30
40
50
60
70
80
90
100
No tratamiento previo conBortezomib
(n = 63)
Tratamiento previo conBortezomib
(n = 48)
Todos los pacientes(N = 111)
No prior treatment with Bortezomib (n=63)
Prior treatment with Bortezomib (n=48)
All patients (n=111)
Patie
nts
(%)
68% 67% 68%
Partial response (PR)
Complete response (CR)
19%
49%
23%
44%
21%
47%
Efficacy: RR
Wang M, et al. N Engl J Med. 2013; 369:507-516
Ibrutinib in MCL

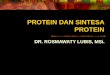
Efficacy: Subgroup analysis
The response to ibrutinib did not vary with baseline characteristics or risk factors associated with failure of chemotherapy.
Wang M, et al. N Engl J Med. 2013; 369:507-516
Ibrutinib in MCL

All patients (n= 111)
Time to Response, median in months (range)
1.9 (1.4-13.7)
Time to Complete Response, median in months (range)
5.5 (1.7-11.5)
Efficacy: Time to Response
Ibrutinib in MCL
Wang M, et al. N Engl J Med. 2013; 369:507-516

Efficacy: Duration of Response
Ibrutinib in MCL
Wang M, et al. N Engl J Med. 2013; 369:507-516
Duration of Response. Median in months (95% IC)
No prior Bortezomib
Prior Bortezomib All patients
15.8 (5.6-NR)
NR (NR-NR)
17.5 (15.8-NR)
NR, not reached

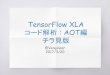
Efficacy: PFS
PFS Median in months (95% CI)
No Exposición a Bortezomib
Exposición a Bortezomib
Todos los pacientes
7.4 (5.3-19.2)
16.6 (8.3-NR)
13.9 (7.0-NR)
Among subjects who achieved a PR the median PFS was 17.5
months
The median PFS among patients achieving CR has not been
reached yet
NR, not reached
Ibrutinib in MCL
Wang M, et al. N Engl J Med. 2013; 369:507-516

Efficacy: OS
Median OS in months (95% CI)
No exposure to Bortezomib
Exposure to Bortezomib All patients
NR (10.0-NR)
NR (11.9-NR)
NR (13.2-NR)
NR: not reached
The median OS for this study has not
been reached (OS estimated at 18
months is 58%)
Ibrutinib in MCL
Wang M, et al. N Engl J Med. 2013; 369:507-516

• The efficacy data were evaluated by an IRC
− OR = 69%
− 21% in CR, and 48% in RP
− Duration of Response (median) = 19.6 months
Efficacy: Evaluation of IRC (Independent Review Committee)
Ibrutinib in MCL
Wang M, et al. N Engl J Med. 2013; 369:507-516

Lymphocyte count
Wang M, et al. N Engl J Med. 2013; 369:507-516
Ibrutinib in MCL

ASH 2014: follow-up at 27 months
• Median PFS = 13 mo
• PFS at 24 mo = 31%
• Median OS = 22.5 months
• OS at 24 mo = 47%
PFS
OS
• Long-term follow-up demonstrated durable responses.
• ∼1/3 of patients without progression and ∼50% alive at 2 years
Wang ML et al. ASH 2014; Poster/Abstract 4453
Ibrutinib in MCL

Ibrutinib in previous treated Waldenström´s Macroglobulinaemia (NCT01614821)
Ibrutinib in WM
N Engl J Med 2015; 372:1430-1440
Steven P. Treon, M.D., Ph.D, Christina K. Tripsas, M.A., Kirsten Meid, M.P.H., Diane Warren, B.S., Gaurav Varma, M.S.P.H., Rebecca Green, B.S., Kimon V. Argyropoulos, M.D., Guang Yang, Ph.D., Yang Cao, M.D., Lian Xu, M.S., Christopher J. Patterson, M.S., Scott Rodig, M.D., Ph.D., James L. Zehnder, M.D., Jon C. Aster, M.D., Ph.D., Nancy Lee Harris, M.D., Sandra Kanan, M.S., Irene Ghobrial, M.D., Jorge J. Castillo, M.D., Jacob P. Laubach, M.D., Zachary R. Hunter, Ph.D., Zeena Salman, B.A., Jianling Li, M.S., Mei Cheng, Ph.D., Fong Clow, Sc.D., Thorsten Graef, M.D., M. Lia Palomba, M.D., and Ranjana H. Advani, M.D.

The rationale
BTK signalling is increased in WM due to a mutation in the MYD88 molecule.
The MYD88 mutation is found in over 90% of WM patients and is absent or rarely expressed in patients with similar B-cell malignancies, including multiple myeloma.(1)
*This study began as an investigator-initiated study but the results were subsequently used by the company to support registration filings in the U.S. and EMEA.
1. Treon, S.P., Xu, L., et al. (2012). MYD88 L265P somatic mutation in Waldenstrom's macroglobulinemia. N Engl J Med. 367(9): 826-33.
Ibrutinib in WM
Treon et al. N Engl J Med 2015; 372:1430-1440

Study Design • Prospective, multi-centre, Phase 2 trial of single agent ibrutinib in 63
patients with relapsed or refractory WM.
• Patients are treated with ibrutinib 420mg orally once a day. • Treatment continues until progressive disease or unacceptable toxicity. • Patients in this study will receive up to 26 cycles of treatment.
Ibrutinib in WM
Treon et al. N Engl J Med 2015; 372:1430-1440

Primary outcome The primary outcome measures are: • overall response rate (> 25% reduction in disease burden), • major response rates (> 50% reduction in disease burden), and • very good partial response (VGPR)/complete response (CR) rate
(90-100% reduction in disease burden).
Secondary outcome Includes: • safety and tolerability of ibrutinib, and • progression-free survival (PFS).
Ibrutinib in WM
Treon et al. N Engl J Med 2015; 372:1430-1440

Patient Characteristics
Ibrutinib in WM
Treon et al. N Engl J Med 2015; 372:1430-1440

Results 35 evaluable patients overall response rate was 83% major response rate was 66%.
The only non-responder was shown to have an unmutated MYD88, suggesting that the mutation drives BTK activation and so provides the target for ibrutinib.
The median duration of response has not been reached (2.8+, 18.8+ months). The median time to response was 1.2 months (range, 0.7-13.4 months).
Ibrutinib in WM
Treon et al. N Engl J Med 2015; 372:1430-1440

Markers of disease burden
Median IgM level fell from 3,190 to 1,232 mg/dL (P=5.1 x 10-9).
Ibrutinib in WM
Treon et al. N Engl J Med 2015; 372:1430-1440

Markers of disease burden
The median hematocrit in these patients improved from 30.8% to 39.7%; (P=1.1 x 10-11).
Ibrutinib in WM
Treon et al. N Engl J Med 2015; 372:1430-1440

Safety profile Ibrutinib was well tolerated. After six or more treatment cycles, over 90% of participants in the WM study remain on ibrutinib therapy. Only three patients discontinued treatment.
Ibrutinib in WM
Treon et al. N Engl J Med 2015; 372:1430-1440

Conclusion Ibrutinib in R/R WM is associated with:
1. Rapid reduction of serum IgM,
2. Improvements in hematocrit and
3. An overall response rate of 83% in heavily pre-treated patients.
The responses are durable, and treatment with Ibrutinib is well
tolerated Ibrutinib offers a new treatment option in this patient group.
Ibrutinib in WM
Treon et al. N Engl J Med 2015; 372:1430-1440

Ibrutinib. Safety

Adverse events %
Diarrhea 49
Fatigue 37
Cough 31
URT infection 27
Dyspnea 27
Arthralgia 27
Rash 27
Adverse events %
Pyrexia 27
Nausea 25
Peripheral edema 25
Anorexia 21
Constipation 20
Vomiting 20
Muscle spasms 20
Ibrutinib safety

Bleedings and infectious events (≥ Grado 3)* n (%) Grado 3 Grado 4 Grado 5 Total
Bleeding event Subdural hematoma†
Hematuria
5 (5) 2 (2) 2 (2)
0 (0) 0 (0) 0 (0)
0 (0) 0 (0) 0 (0)
5 (5) 2 (2) 2 (2)
Infectious event Pneumonia Cellulitis UTI Bronchitis Costridium difficile colitis LRTI Sepsis
24 (22) 6 (5) 3 (3) 3 (3) 2 (2) 2 (2) 2 (2) 0 (0)
1 (1) 0 (0) 0 (0) 0 (0) 0 (0) 0 (0) 0 (0) 1 (1)
3 (3) 1 (1) 0 (0) 0 (0) 0 (0) 0 (0) 0 (0) 1 (1)
28 (25) 7 (6) 3 (3) 3 (3) 2 (2) 2 (2) 2 (2) 2 (2)
*At least in 2% of patients. †4 patients had subdural hematomas: 1 grade 1, 1 grade 2, and 2 grade 3 and. All were associated with falls, head trauma, or both; 4 patients taking aspirin or warfarin in two previous days or at the date of the event. UTI, urinary tract infection; LRTI, infection of the lower respiratory tract.
Ibrutinib safety

Jones, et al. Blood 2014 (ASH)
Patients recruited in 2 clinical trials of R/R CLL/SLL n = 327 Most of severe hemorrhagic events occurred in patients taking 2 anticoagulant drugs
Ibrutinib safety

Ibrutinib. Expansion

O’Brian et al. ASH 2014
Ibrutinib in R/R CLL/SLL with 17p-. Phase II
• N=144 pts • At dose of 420 mg/day • ORR: 82.6% • CR: 17.4% • mFU: 13.0 m • mDoR: NR • PFS (@ 12 m.): 79.3% • PFS (@ 12 m.) of responders: 88.3%
Warning
7.6% of Richter transformation
Ibrutinib in CLL/SLL

Three-year follow-up in treatment-naïve and previously treated patients with CLL and SLL receiving single-agent Ibrutinib
Byrd et al. Blood 2015 (Feb 23, online)
Ibrutinib in CLL/SLL

Byrd et al. Blood 2015 (Feb 23, online)
Ibrutinib in CLL/SLL
Three-year follow-up in treatment-naïve and previously treated patients with CLL and SLL receiving single-agent Ibrutinib

Byrd et al. Blood 2015 (Feb 23, online)
Ibrutinib in CLL/SLL
Three-year follow-up in treatment-naïve and previously treated patients with CLL and SLL receiving single-agent Ibrutinib

Byrd et al. Blood 2015 (Feb 23, online)
Ibrutinib in CLL/SLL
Three-year follow-up in treatment-naïve and previously treated patients with CLL and SLL receiving single-agent Ibrutinib

Byrd et al. Blood 2015 (Feb 23, online)
Ibrutinib in CLL/SLL
Three-year follow-up in treatment-naïve and previously treated patients with CLL and SLL receiving single-agent Ibrutinib

Farrooqui et al. Lancet Oncol 2015; 16: 169-76
Ibrutinib in CLL/SLL

Farrooqui et al. Lancet Oncol 2015; 16: 169-76
Ibrutinib in CLL/SLL

Farrooqui et al. Lancet Oncol 2015; 16: 169-76
Ibrutinib in CLL/SLL

Farrooqui et al. Lancet Oncol 2015; 16: 169-76
Ibrutinib in CLL/SLL

Byrd et al N Engl J Med 2014; 371: 213-23
Relapsed CLL at risk for poor outcome. Phase III: Ibrutinib vs Ofatumumab
Ibrutinib in CLL/SLL

Byrd et al N Engl J Med 2014; 371: 213-23
Relapsed CLL at risk for poor outcome. Phase III: Ibrutinib vs Ofatumumab
Ibrutinib in CLL/SLL
No significant difference in 12-month PFS was observed in Ibrutinib-treated patients: - with or without del (17p) or - who developed lymphocytosis compared with those without lymphocytosis

Byrd et al N Engl J Med 2014; 371: 213-23
Relapsed CLL at risk for poor outcome. Phase III: Ibrutinib vs Ofatumumab
Ibrutinib in CLL/SLL

Ibrutinib in R/R DLBCL
Multicenter Phase II Study: Preliminary results
N=70 • Median prior therapies: 3 (1-7) • Median age (years): 63 (28-92) • CS IV: 63% • Refractory: 54% • Prior SCT: 23%
Wilson et al. Blood 2012 (ASH)
Patients with CARD11 or MYD88 mutated did not responded That suggests dominance of CD79b driven BCR signaling in these patients
Ibrutinib in other LPS’s
GCB ABC
ORR 5.3% 40%
CR 0 8%

Ibrutinib in First line B-cell NHL
N=33
Younes et al. Blood 2013 (ASH)
• Neutropenia: 67% • Nausea: 67% • Thrombosis: 61% • Diarrhea: 30% • Headache: 27% • Constipation: 27% • Alopecia: 27%
Ibrutinib in other LPS’s
NHL DLBCL
ORR 100% 100%
CR 73% 64%

Ibrutinib after allogeneic SCT
N = 16 Collected from 4 phase II/III clinical trials
•Median prior therapies: 5 •17p-: 63%
Miklos et al. In 2015 BMT Tandem Meeting. San Diego, 2015
ORR: 88% CR: 12% Median DoR, PFS and OS not reached with a median FU of 23 months
• PFS (@24 m): 77% • Median time on Ibrutinib: 18 m(0.4-39) • Ibrutinib discontinuation: 5 . Disease progression: 2 . Pneumonia: 2 . Voluntary withdrawal: 1 One patient achieved a complete resolution of chronic GVHD
Ibrutinib: other indications

Conclusions • BTK blocking in B-cell neoplasms by Ibrutinib
induces apoptosis of B cells and inhibition of adhesion of B cells in lymph nodes
• The clinical development of Ibrutinib comprising multiple B-cell neoplasms, including MCL, CLL, and WM in monotherapy, induces high response rates and maintenance over time of the response
• Adverse effects grade 3 or 4 are rare, and favorable toxicity profile allows an opportunity for less intensive treatment and more effective than currently available regimens for patients with MCL
Ibrutinib in CLL/SLL and MCL

Ibrutinib. Approval

November 2013: FDA approved Ibrutinib for patients with MCL in R/R February 2014: FDA approved Ibrutinib for CLL in R/R July 2014: FDA approved the drug for CLL with 17p delection January 2015: FDA expands approved use of Ibrutinib for WM. First drug approved to treat WM July 2014: EMA approved Ibrutinib for CLL and MCL in R/R Ibrutinib is currently under development by Pharmacyclics, Inc and Johnson & Johnson's Janssen Pharmaceutical division for additional B-cell malignancies including diffuse large B-cell lymphoma and multiple myeloma.
Ibrutinib approval

Ibrutinib. Mechanisms of resistance

1. BTK alternative pathways (detected if ERK and AKT remain actives) is one of mechanisms of primary resistance to Ibrutinib. Such that Ibrutinib resistant cells retain high levels of pAKT and show increased levels of bcl-2
2. C481S mutation at the BTK binding side confers acquired resistance to Ibrutinib in CLL and MCL
3. R665W and L845F mutations of PLCγ2 cause acquired resistance to Ibrutinib
4. Ibrutinib inhibits only IgM-induced STAT3 activation but not IL6-induced (autocrine) STAT3 activation
Resistance to Ibrutinib

6. In patients with WM, mutated CXCR4 decrease ORR to 30%
7. wtMYD88 in WM diminishes response to Ibrutinib
8. MYD88 mutated confers resistance to Ibrutinib in CLL (and DLBCL)
9. S338X mutation of CXCR4 in WM or CLL showed acquired resistance to Ibrutinib and can confer resistance to other molecules as Bendamustine, Fludarabine, Bortezomib and Idelalisib
10.Activation of bcl2 pathway is involved in Ibrutinib resistance in WM
Resistance to Ibrutinib

Ibrutinib. Optimization (Association)

Patients with MCL failing to Ibrutinib are unlikely to respond to salvage chemotherapy and have poor outcomes
Cheah et al. Ann Oncol 2015
mFU: 10.7 months
After Ibrutinib, what?

Patients with MCL failing to Ibrutinib are unlikely to respond to salvage chemotherapy and have poor outcomes
Martin et al. Blood 2014 (ASH)
N: 32
Received or undergone: • Rituximab: 11 • Lenalidomide: 6 • Alkilator agent: 6 • Bendamustine: 3 • Anthracyclin: 2 • Bortezomib: 1 • Purine analog: 1 • SCT: 2
Median OS (months: 4)
After Ibrutinib, what?

Ibrutinib + Rituximab in R/R CLL/SLL Phase II N=40
• Unmutated IGHV: 80% • TP53 mutated: 50% • ATM mutated: 32%
mFU: 14 mo. • 80% continue on therapy • PFS (18 mo.) : 78% • PFS (18 mo.) mp53: 72%
Burger et al. Lancet Oncol 2014
Trying to optimize Ibrutinib
All 17p-
ORR 95% 80%
CR 8% 10%

Ibrutinib + Ofatumumab in R/R CLL/SLL Phase Ib/II
• Prior therapies: 3 (2-10) • Unmutated: 91% • 17p-: 37%
mFU: 9.8 m. • 89% remain on the study
Jaglowski et al. 2012
Trying to optimize Ibrutinib
All
ORR 100%
CR 4%

Ibrutinib + Lenalidomide in R/R CLL/SLL
Phase I N: 9
Pollyea et al. Blood 2014 (ASH)
• Ibrutinib: 420 mg • Lenalidomide: 2.5 to 10 mg
Trying to optimize Ibrutinib
All
ORR 100%
CR 0

Ibrutinib + Rituximab + Bendamustine in R/R CLL/SLL
Phase II N=30 Doses: • Ibrutinib (420 mg/d) • Rituximab (375 mg/m2) • Bendamustine (70 mg/m2)
Brown et al. Blood 2013 (ASH)
Trying to optimize Ibrutinib
All
ORR 93%
CR 17%

Phase III studies in R/R MCL
R
Ibrutinib
Temsirolimus
R
Bendamustine + Rituximab + Ibrutinib
Bendamustine + Rituximab + Placebo
( In patients > 65 y.)

I: Ibrutinib 560 mg oral
ASCT: THAM or BEAM (stratified per site before start of trial)
Observation: up to 4.5 yrs after maintenance (9.5 yrs in arm A)
Arm A: Standard of care Experimental Arm A + I Experimental Arm I
TRIAL DESIGN
N= 870 patients

Ibrutinib. Possible new combinations

Possible futures combinations with Ibrutinib in B-cell malignancies
1. AKT inhibitors (MK2206) to overcome alternative pathways
2. Bcl2 inhibitors (ABT199) to induced synergistic cytotoxicity due to increased bcl2 expression induced by Ibrutinib and sensitizes to ant-bcl2 drugs a. Acts synergistically in MCL b. Has a modest synergy in CLL
3. Proteasome inhibitor (Carfilzomib): acts synergistically by
inducing BAX and bcl2 cleavage and activating p53

Possible futures combinations with Ibrutinib in B-cell malignancies
4. Syk inhibitors overcomes C481Smut of BTK and R665Wmut of PLCγ2
5. IRAK4 inhibitors (ND-2110 and ND-2158) overcome resistance of CLL to Ibrutinib
6. SINE (KPT330-Selinexor) has synergy in MCL
7. Anti-PD1 reinforces antitumor activity of Ibrutinib

Thoughts

Thoughts
1. BTK inhibitors are a new therapeutic approach for B-cell NHL, specially CLL, MCL and WM, being Ibrutinib the first in class BTK inhibitor
2. Responses to Ibrutinib in these pathologies are equal or superior to conventional chemotherapy
3. Clinical trials to elucidate the role of this compound on DLBCL (mainly non-GCB), and other B-cell neoplasms are ongoing

Thoughts
4. We are knowing the emerging mechanisms of resistance to Ibrutinib in different B-cell neoplasias
5. Clinical trials optimizing Ibrutinib are underway
6. Combinations with other emerging drugs to overcome potential mechanisms of resistance are currently under investigation

Hematology Department
Acknowledgements
Dr. F. Bosch Dra. A. Marín Dr. P. Abrisqueta Dra. M. Gironella Dra. S. Bobillo Dra. C. Carpio Dr. B. Merchán
Dr. J. Castellví (A. Patológica) Dr. M. Simó (M. Nuclear) Dra. M. Barios (M. Nuclear) Dra. R. Boyer (Radiología)

Hematology Department
Thank...
...YOU ALL FOR YOUR PATIENCE AND ATTENTION!
Recommended