-
7/29/2019 Signos neurolgicos adolescentes con y sin psicosis
1/8
266 http://neuro.psychiatryonline.org J Neuropsychiatry Clin
Neurosci 19:3, Summer 2007
REGULAR ARTICLES
Neurological Signs andCognitive PerformanceDistinguish
BetweenAdolescents With andWithout PsychosisDavid B. Arciniegas,
M.D.Donald C. Rojas, Ph.D.
Michelle Ramos Kleman, M.S.W.Ryan Asherin, B.A.Martin L. Reite,
M.D.
Received February 1, 2006; revised May 13, 2006; accepted
August21, 2006. From the University of Colorado School of Medicine,
Den-ver, Colorado. Address correspondence to Dr. Arciniegas,
Neuro-psychiatry Service, University of Colorado School of
Medicine, Cam-pus Box C268-25, 4200 East Ninth Avenue, Denver, CO
80262; [email protected] (e-mail)
Copyright 2007 American Psychiatric Publishing, Inc.
Neurological and cognitive aspects of adolescentpsychotic
disorders are understudied. The authorsassessed 19 adolescents with
psychosis and 16healthy comparison subjects using the Neurologi-cal
Evaluation Scale (NES) and age-appropriateWechsler intelligence
quotient (IQ) scales. NESscores were highest and IQ scores were
lowest
among subjects with psychosis. Subjects with psy-chosis did not
demonstrate age-related decreasesin NES score. The combination of
NES and IQscores predicted both the presence of psychosis
andpsychiatric diagnosis. There were no relationshipsbetween
medication status and either NES or IQscores. These results support
a broadly conceivedneurodevelopmental formulation of
adolescentpsychotic disorders.
(The Journal of Neuropsychiatry and ClinicalNeurosciences 2007;
19:266273)
Schizophrenia and related psychotic disorders are in-creasingly
regarded as neurodevelopmental disor-ders in which the structure
and/or function of large-
scale distributed networks serving cognition, emotion,
behavior, and motor function are disturbed.1 These dis-
turbances manifest in adults not only as psychosis but
also as impairments in sensory integration, complexmo-
tor sequencing, coordination, primitive reflexes,2,3 eye
movements,4
visual and auditory information process-ing, sustained
attention, working memory, verbal epi-
sodic memory, and executive function.5
Several studies suggest that subtle signs of neurolog-
ical dysfunction (soft signs) are relatively common
among children and adolescents with schizophrenia and
related psychotic disorders.68 Additionally, Karp et al.8
demonstrated a failure of age-expected reductions in the
number and severity of these signs among adolescents
with schizophrenia, suggesting that psychosis devel-
oping in this age range, and perhaps in older individ-
uals as well, is associated with other signs of aberrant
neurodevelopment.Studies pairing neurological assessment with
either
symptom severity or cognitive performance among ad-
olescents with schizophrenia and related psychotic dis-
-
7/29/2019 Signos neurolgicos adolescentes con y sin psicosis
2/8
J Neuropsychiatry Clin Neurosci 19:3, Summer 2007
http://neuro.psychiatryonline.org 267
ARCINIEGAS et al.
orders have not been published. Additionally, studies of
this population have not employed standardized neu-
rological assessment scales, thereby limiting the com-
parability of their findings to those of adults with these
conditions. The Neurological Examination Scale (NES)2
is a standardized clinical assessment of subtle (soft)
neurological signs with excellent construct validity and
interrater reliability,2,3 and is the most widely used neu-
rological assessment tool in studies of adults with psy-
chotic disorders. The NES may therefore be well suited
to the study of adolescents with these conditions.
We undertook the present study to investigate ado-
lescent psychotic disorders from a neurodevelopmental
perspective using structured psychiatric diagnostic in-
terviews, the NES, and standardized measures of cog-
nition. The overarching hypothesis of this study is that
psychosis is only one of several manifestations of aber-
rant neurodevelopment among adolescents with schizo-
phrenia, schizoaffective disorder, and bipolar disorder
with psychotic features. Specific study hypotheses in-
cluded: 1) adolescents with psychosis demonstrate a
greater frequency and severity of neurological signs on
the NES than healthy comparison subjects of a similar
age; 2) adolescents with psychosis perform more poorly
on standardized cognitive tests (full-scale, verbal, and
performance IQ) than healthy comparison subjects of a
similar age; 3) the severity of neurological dysfunction
on the NES is independent of the severity of
cognitiveimpairment; 4) adolescents with psychosis will dem-
onstrate a failure of age-expected neurological matu-
ration on the NES; and 5) group membership (psy-
chotic versus nonpsychotic) is predicted by NES score
and full-scale IQ.
METHOD
After complete description of the study to the subjects
and their legal guardians, we obtained written informed
consent for study participation from the legal guardianand
assent from the subjects in accordance with the pol-
icies and procedures of the Colorado Multiple Institu-
tional Review Board.
Subjects
Nineteen subjects with psychosis ages 9 to 17 years (six
female) with schizophrenia, schizoaffective disorder, or
bipolar disorder with psychotic features were recruited
via referrals from child psychiatrists, mental health
agencies, and mental health advocacy organizations in
the Denver, Colo., metropolitan area, and through ad-
vertisements in this locale. Sixteen adolescents of similar
age (five female) with no personal or family history of
mental illness or neurological disease were similarly re-cruited
and served as comparison subjects.
General Clinical AssessmentTwo of the investigators (D.B.A. and
M.L.R.) performed
general clinical assessments inclusive of developmental,
medical, surgical, neurological, psychiatric, and sub-
stance histories, and also assessment of pubertal status
using the Pubertal Development Scale.9 Psychotropic
medication use was recorded and categorized as: anti-
psychotics; lithium in any formulation; anticonvulsant
mood-stabilizers; antidepressants (all classes); stimu-
lants; and benzodiazepines.
Psychiatric Diagnoses
We administered the Schedule for Affective Disorders
and Schizophrenia for School-Age ChildrenPresent
and Lifetime version (K-SADS-PL)10 under the super-
vision of one investigator (M.L.R.). A DSM-based clini-
cal interview was performed by a second investigator
(D.B.A.). These assessments were used to arrive at a con-
sensus-based study diagnosis by the lead investigators
(M.L.R., D.B.A., D.C.R.) which were completed without
consideration of neurological and cognitive assessment
findings.
Neurological Assessment
Physical examinations, elemental neurological exami-
nations, and examinations for subtle neurological signs
using the NES2 were performed by a single investigator
(D.B.A.). This investigator remained blind to K-SADS-
PL diagnoses (and hence consensus-based study diag-
noses) until the neurological assessments were com-
pleted and scored. NES findings were categorized into
eight domains of neurological function (Table 1).
Cognitive AssessmentA trained professional research assistant
blinded to
study diagnosis performed cognitive assessments. As-
sessment of cognition was performed using the WAIS,
3rd edition (WAIS-III)11 or WISC, 3rd edition (WISC-
III)12 as appropriate for age. Some participants (three
subjects with psychosis, two comparison subjects) were
administered the 4-subtest version of the Wechsler Ab-
breviated Scale of Intelligence (WASI).13 Dependent
variables derived from the Wechsler scales included full
-
7/29/2019 Signos neurolgicos adolescentes con y sin psicosis
3/8
268 http://neuro.psychiatryonline.org J Neuropsychiatry Clin
Neurosci 19:3, Summer 2007
NEUROLOGICAL SIGNS AND COGNITIVE PERFORMANCE IN ADOLESCENTS
TABLE 1. Mean (SD) Scores on Neurological Examination Scale
(NES) and Intelligence Quotient (IQ), and Puberty Development
Scale(PDS) Assessments Among Adolescents With Psychosis,
Schizophrenia (Schz) or Schizoaffective Disorder (SchzA),
BipolarDisorder with Psychosis (BD-P), and Adolescents Without
Psychosis (Comparators)
Psychosis (N 19) Schz/SchzA (N 11) BD-P (N 8) Comparators (N
16)
Age at NES assessment in years 14.6 (2.3) 14.9 (2.5) 14.1 (2.1)
14.4 (1.9)NES Total 20.1 (5.7) 21.6 (5.1) 18.0 (6.1) 9.2 (3.9)
Primitive reflexes 2.5 (1.3) 2.7 (1.1) 2.3 (1.5) 0.4 (0.5)
Complex motor sequencing 6.4 (2.1) 7.2 (1.4) 5.4 (2.6) 2.9
(1.9)Motor coordination 4.0 (1.8) 2.3 (1.4) 2.8 (2.4) 0.6
(0.5)Short-term memory 1.5 (1.2) 1.5 (1.1) 1.4 (1.3) 0.4
(1.1)Cerebral dominance 1.2 (0.2) 1.2 (0.3) 1.2 (0.2) 1.0
(0.1)Integrative sensory function 2.9 (2.2) 3.4 (2.6) 2.1 (1.4) 1.6
(1.7)Eye movements 1.2 (1.4) 1.2 (1.5) 1.3 (1.2) 0.4 (0.8)Motor
inhibition 3.2 (1.4) 3.4 (2.6) 2.9 (1.0) 2.6 (1.3)
Age at IQ assessment in years 14.1 (2.2) 14.2 (2.3) 13.8 (2.0)
14.1 (2.2)Full Scale IQ 92.5 (9.9) 87.2 (7.2) 99.8 (8.6) 111.4
(11.2)Verbal IQ 100.1 (11.6) 95.5 (10.3) 106.3 (11.0) 114.8
(13.6)Performance IQ 86.1 (11.4) 81.0 (11.8) 93.1 (6.4) 105.9
(9.7)Verbal IQ-Performance IQ 13.9 (14.1) 14.5 (17.6) 13.1 (8.2)
8.9 (12.5)PDS Score 2.5 (0.6) 2.5 (0.9) 2.5 (0.9) 2.8 (0.6)
scale (FS) IQ, verbal (V) IQ, and performance (P) IQ,
which were available from all of these assessments.
Inclusion Criteria
Subjects with a diagnosis of schizophrenia, schizoaffec-tive
disorder, or bipolar disorder with psychosis and no
current or past diagnoses of alcohol or substance abuse/
dependence, no history or examination findings sugges-
tive of neurological (including traumatic brain injury or
epilepsy) or developmental disorders, and no current
major medical illness were included. Comparison sub-
jects were included if their evaluations revealed no per-
sonal or family history of mental illness or neurological
disease.
Statistical Analyses
All statistical analyses were performed using Statistica6.1
(StatSoft, Inc., Tulsa, Okla.). Students t tests were
used to test the hypothesis that NES scores are higher
and IQ scores are lower among adolescents with psy-
chosis than among comparison subjects. A one-sided
test for differences between proportions was used to test
the hypothesis that subjects with psychosis demonstrate
a higher frequency of neurological subtle signs than
healthy comparison subjects. Separate one-way analysis
of variance (ANOVA) tests were employed to test for
differences in NES and IQ scores between diagnostic
groups (schizophrenia/schizoaffective disorder versus
bipolar disorder with psychotic features versus never
mentally ill). We employed within-group Pearsons
product-moment correlations to test the hypothesis that
adolescents with psychosis demonstrate a failure of age-
expected neurological maturation on the NES, and to
investigate the relationship between NES scores and
VIQ, PIQ, and FSIQ scores. We performed binomial lo-
gistic regression analysis to examine whether group
membership (psychotic versus nonpsychotic) is pre-dicted by
total NES and FSIQ. Multinomial logistic re-
gression analysis was used to determine whether diag-
nosis (schizophrenia/schizoaffective disorder versus
bipolar disorder with psychotic features versus never
mentally ill) is predicted by total NES and FSIQ. Fishers
exact test was used to examine differences in the pro-
portion of subjects treated with each of the classes of
psychotropic medications described above. Addition-
ally, an exploratory analysis using simple linear regres-
sion was employed to investigate whether total NES,
FSIQ, VIQ, and PIQ scores predicted psychotropic med-
ication treatment status (i.e., treatment versus no treat-
ment) among subjects with psychosis.
RESULTS
The psychotic group (N 19) consisted of seven subjects
with schizophrenia (one female), four subjects with schi-
zoaffective disorder (one female), and eight subjects
with bipolar disorder with psychotic features (four fe-
males). All subjects with bipolar disorder with psychotic
features were euthymic (i.e., not in a manic, hypomanic,
manic, or mixed episode and also not psychotic) at the
time of study assessments. The mean age of onset for
first psychiatric diagnosis in the psychotic group was
6.9 (SD 2.5) years (range 4 to 11 years) and included
-
7/29/2019 Signos neurolgicos adolescentes con y sin psicosis
4/8
J Neuropsychiatry Clin Neurosci 19:3, Summer 2007
http://neuro.psychiatryonline.org 269
ARCINIEGAS et al.
attention-deficit hyperactivity disorder (42.1%), schizo-
phrenia (10.5%), bipolar disorder (type unspecified or
not otherwise specified, 31.6%), aggressiveness
(5.3%), and no formal diagnosis (10.5%). The mean age
of onset for study diagnosis was 9.7 (SD 2.8) years(range 4 to
13 years).
Among the psychotic subjects, 31.6% had a history of
maternal drug use during pregnancy, including expo-
sure to stimulants (21.1%), alcohol (21.1%), and nicotine
(5.3%), alone or in combination, and 16 of 19 subjects
(84.2%) had a history of treatment with stimulant med-
ications prior to or since the onset of study diagnosis.
At the time of NES assessment, medications used among
subjects with psychosis included antipsychotics (84.2%),
lithium in any formulation (36.8%), anticonvulsant
mood-stabilizers (42.1%), antidepressants (36.8%), stim-
ulants (31.6%), and benzodiazepines (21.1%). At the
time of IQ assessment, medications used among subjects
with psychosis included antipsychotics (78.9%), lithium
in any formulation (42.1%), anticonvulsant mood-sta-
bilizers (47.4%), antidepressants (42.1%), stimulants
(36.8%), and benzodiazepines (15.8%). Subjects with bi-
polar disorder with psychotic features differed from
those with schizophrenia/schizoaffective disorder with
respect to the frequency of treatment with lithium (75%
versus 18%, Fishers exact p0.03) and anticonvulsant
mood-stabilizers (88% versus 18%, Fishers exact p
0.005).There was no effect of diagnosis on Pubertal Devel-
opment Scale (PDS) scores (F 0.6, df 2.32, p 0.57).
Post-hoc comparison using Tukeys Honest Significant
Difference (HSD) test for unequal sample sizes demon-
strated no differences in PDS scores between diagnostic
subgroups.
Comparison of NES Scores Between Groups
Total NES scores were significantly higher among sub-
jects with psychosis than among comparison subjects
(t 6.5, p0.001). There also was a significant effect of
diagnosis on total NES score (F 23.2, df 2,32, p0.001),
primitive reflexes (F 19.5, df 2,32, p0.001),
complex motor sequencing (F 15.7, df 2,32, p0.001),
motor coordination (F 8.2, df 2,32, p0.002), and
short-term memory (F 3.5, df 2,32, p0.04) scores.
Post-hoc comparison using Tukeys HSD test for un-
equal sample sizes demonstrated a significant difference
in total NES scores between both subject groups and the
comparison subjects (p0.001 and p0.003, respec-
tively), but no difference between subjects with schizo-
phrenia/schizoaffective disorder and subjects with bi-
polar disorder with psychotic features. A similar pattern
was observed in post-hoc comparisons of primitive re-
flex, complex motor sequencing, and motor coordina-
tion scores: subjects with schizophrenia/schizoaffectivedisorder
did not differ from subjects with bipolar dis-
order with psychotic features, but both groups differed
significantly from the comparison subjects (all p0.05).
Mean total and subscale NES scores among subjects
with schizophrenia/schizoaffective disorder, bipolar
disorder with psychotic features, and the never mentally
ill comparison subjects are presented in Table 2. Item-
level data on the NES for the psychosis and healthy
comparison groups as well as differences using a one-
sided test for difference in proportions are described in
Table 1.
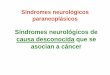
Comparison of Neurological Maturation Between Groups
There was an inverse relationship between age at time
of NES assessment and total NES among the healthy
comparison subjects (r 0.68, p0.004), but not among
subjects with psychosis, collectively (Figure 1) or by
diagnostic group (schizophrenia/schizoaffective disor-
der and bipolar disorder with psychotic features).
Comparison of Cognitive Assessments Between Groups
FSIQ, VIQ, and PIQ scores were significantly loweramong subjects
with psychosis than among compari-
son subjects (Table 1). There was a significant effect of
diagnosis on FSIQ (F 21.0, df 2,32, p0.001), VIQ
(F 8.3, df 2,32, p0.002), and PIQ (F 21.2, df 2,32,
p0.001). Post-hoc comparison using Tukeys HSD for
unequal sample sizes demonstrated a significant dif-
ference between subjects with schizophrenia/schizoaf-
fective disorder and subjects with bipolar disorder
with psychotic features (p0.04), as well as a signifi-
cant difference between subjects with schizophrenia/
schizoaffective disorder and the comparison subjects
(p0.001). We also observed a trend towards a similardifference
between subjects with bipolar disorder with
psychotic features and the comparison subjects
(p 0.05). Post-hoc comparison of VIQ scores demon-
strated significant differences between subjects with
schizophrenia/schizoaffective disorder and the com-
parison subjects (p0.003), but not the subjects with
bipolar disorder with psychotic features. VIQ scores
among subjects with bipolar disorder with psychotic
features did not differ from those of the comparison
-
7/29/2019 Signos neurolgicos adolescentes con y sin psicosis
5/8
270 http://neuro.psychiatryonline.org J Neuropsychiatry Clin
Neurosci 19:3, Summer 2007
NEUROLOGICAL SIGNS AND COGNITIVE PERFORMANCE IN ADOLESCENTS
TABLE 2. Percentage of Adolescents With and Without Psychosis
Demonstrating Abnormalities (Score0) on all NES
AssessmentItems*
% of Subjectswith Psychosis (N 19)
% of ComparisonSubjects (N 16) p Value
Primitive ReflexesGlabellar response 78.9 25.0 0.002Snout
response 52.6 0.0 0.001Grasp reflex 31.6 18.8 0.20Suck reflex 5.3
0.0 0.18
Complex Motor SequencingFist-Ring Test 73.7 50.0
0.08Fist-Edge-Palm Test 63.2 31.3 0.04Ozeretski Test 73.7 37.5
0.02
Rhythm Tapping Part A 89.5 43.8 0.004Rhythm Tapping Part B 89.5
50.0 0.007
Motor CoordinationTandem Gait 31.6 12.5 0.09Romberg Sign 10.5
0.0 0.10Rapid Alternating Movements (dominant) 31.6 0.0 0.01Rapid
Alternating Movements (nondominant) 47.4 6.3 0.006Finger-Thumb
Opposition 42.1 18.8 0.07Finger-to-Nose Test 21.1 18.8 0.43
Motor InhibitionAdventitious movements 78.9 87.5 0.25Tremor 15.8
0.0 0.05Mirror movements 84.2 56.3 0.04Synkinesis 36.8 37.5
0.48
Eye MovementsConvergent gaze 10.5 0.0 0.10Gaze impersistence
(right visual field) 42.1 25.0 0.15
Gaze impersistence (left visual field) 26.3 6.3 0.06Short-Term
Memory
Short-term memory 5 minutes 73.7 18.8 0.002Short-term memory 10
minutes 52.6 12.5 0.01
Integrative Sensory FunctionAudio-visual integration 15.8 12.5
0.39Stereognosis 10.5 6.3 0.33Graphesthesia 80.0 56.3
0.07Extinction (Face-Hand Test) 26.3 6.3 0.06Right-left confusion
42.1 25.0 0.15
*Excluding cerebral dominance items (hand, foot, eye). Listed p
values reflect the results of one-sided tests for differences
betweenproportions.
subjects. However, PIQ scores were lower among sub-
jects with schizophrenia/schizoaffective disorder than
among subjects with bipolar disorder with psychotic
features (p0.05) and the comparison subjects (p
0.0002), and PIQ scores were lower among subjectswith bipolar
disorder with psychotic features than
among comparison subjects (p0.04).
Relationships Between Neurological and CognitiveFunction
Total NES scores did not correlate significantly with
FSIQ, VIQ, or PIQ scores among the subjects with psy-
chosis, either collectively or by psychiatric diagnosis
(schizophrenia/schizoaffective disorder and bipolar dis-
order with psychotic features), or among the compari-
son subjects.
Prediction of Psychiatric Diagnosis Using Neurologicaland
Cognitive AssessmentsBinomial logistic regression demonstrated that
the com-
bination of total NES score (Wald statistic 6.9,
p0.009) and FSIQ (Wald statistic 4.2, p0.04) cor-rectly
predicted membership in the psychotic group in
18 of 19 subjects (94.7%) and in the comparison group
in 15 of 16 subjects (93.8%), yielding a log odds ratio of
5.6. Multinomial logistic regression indicated that the
combination of total NES (Wald statistic 7.0, p0.04)
and FSIQ (Wald statistic 7.8, p0.03) modeled psychi-
atric diagnosis well. The model correctly identified
schizophrenia/schizoaffective disorder in 10 of 11 cases
(91.0%), with one case classified as bipolar disorder with
psychotic features. The model also correctly classified
five out of eight subjects with bipolar disorder with psy-
-
7/29/2019 Signos neurolgicos adolescentes con y sin psicosis
6/8
J Neuropsychiatry Clin Neurosci 19:3, Summer 2007
http://neuro.psychiatryonline.org 271
ARCINIEGAS et al.
FIGURE 1. Total NES Score by Age Among Adolescents Withand
Without Psychosis
0
4
8
12
16
20
24
28
32
TotalN
ESScore
Subjects withpsychosis
Comparisonsubjects
9 10 11 12 13 14 15 16 17 18 19
Age (years)
chotic features (63.0%), with two cases misclassified as
schizophrenia/schizoaffective disorder and one case
misclassified as never mentally ill. Finally, the model
correctly classified 15 of 16 never mentally ill subjects
(93.8%), with one case misclassified as bipolar disorderwith
psychotic features.
Relationships Between NES Scores, IQ Scores, andTreatment With
Psychotropic Medications
We utilized simple linear regression to investigate
whether total NES, FSIQ, PIQ, or VIQ predicted treat-
ment status (treatment versus no treatment) with each
of the classes of psychotropic medication described
above. Total NES scores did not predict treatment status
with any class of medication (all p0.26). Initial analy-
ses suggested that FSIQ predicts antipsychotic medica-
tion treatment status (adjusted R2
0.23, p0.03) andthat VIQ predicts antipsychotic and
antidepressant
medication treatment status (adjusted R2 0.23, p0.03,
and adjusted R2 0.17, p0.05, respectively). However,
these findings failed to remain significant after Bonfer-
roni correction for multiple comparisons.
DISCUSSION
Subtle neurological signs were significantly more com-
mon and more severe among adolescents withpsychosis
than among similarly aged healthy comparison subjects.
The neurological domains demonstrating the widest di-
vergence between the subjects with and without psy-
chosis included primitive reflexes, complex motor se-
quencing, motor coordination, and short-term memory.Total NES
scores did not distinguish between subjects
with schizophrenia/schizoaffective disorder and bipolar
disorder with psychotic features, but NES scores in both
groups differed significantly from those of the compar-
ison subjects. Additionally, adolescents with psychosis
failed to demonstrate age-expected reductions of NES
scores.
These findings suggest that neurological dysfunction
as assessed by the NES is strongly associated with the
presence of psychosis, regardless of whether that psy-
chosis is persistent or mood episode-related. Although
the possibility of medication effect on neurological signs
in this population may be of immediate concern, the
regression analyses performed here suggest that this is
an unlikely explanation for this finding. This suggestion
is supported by the lack of association between NES
scores and antipsychotic medication use reported else-
where.2,1416
Similarly, IQ scores were lower among subjects with
psychosis than among the comparison subjects. Al-
though the mean full scale IQ for the psychosis group
was within the normal ranges described for these mea-
sures, population-based studies demonstrate highermean IQ levels
( 1 SD) in the Denver metropolitan
region than in the Wechsler scale standardization sam-
ple.17 The IQ scores of the psychotic adolescents in this
study therefore reflect a greater departure from expected
performance than might otherwise be apparent by these
scores. Since deterioration of IQ in childhood-onset
schizophrenia may begin up to 2 years prior to psycho-
sis onset and stabilize within 2 years thereafter,18 it is
also possible that among the subjects with psychosis
studied here, and particularly those with schizophre-
nia/schizoaffective disorder, IQ may not yet have
reached its final (and possibly even lower) level.In contrast to
neurological signs, and similar to IQ
findings among adults with these conditions,19,20 there
was a significant effect of diagnosis on IQ: scores were
lowest among subjects with schizophrenia/schizoaffec-
tive disorder, highest among the healthy comparison
subjects, and intermediate among subjects with bipolar
disorder with psychotic features. Simple logistic regres-
sion did not identify a predictive relationship of FSIQ,
VIQ, or PIQ on psychotropic medication treatment
-
7/29/2019 Signos neurolgicos adolescentes con y sin psicosis
7/8
272 http://neuro.psychiatryonline.org J Neuropsychiatry Clin
Neurosci 19:3, Summer 2007
NEUROLOGICAL SIGNS AND COGNITIVE PERFORMANCE IN ADOLESCENTS
status. Although it is possible that treatment history
may have influenced the IQ differences between adoles-
cents with schizophrenia/schizoaffective disorder and
bipolar disorder with psychotic features observed here,
data adequate to the task of examining this issue statis-tically
were not available for analyses. However, Zam-
mit et al.,21 in a population-based sample of more than
50,000 male subjects, identified lower IQ as a risk factor
for schizophrenia but not bipolar disorder. This suggests
that cognitive differences between these conditions an-
tedate both their onset and treatment with psychotropic
medications. This finding supports framing IQ differ-
ences between schizophrenia/schizoaffective disorder
and bipolar disorder with psychotic features subjects ob-
served in the present study as reflective of differences
in neurodevelopment between these disorders rather
than as a consequence of them or their treatments.
Collectively, the present findings suggest that NES
and IQ reflect dependent domains in which aberrant
neurodevelopment occurs among adolescents with psy-
chosis. The utility of including neurological and cogni-
tive assessments in the evaluation of adolescents with
these conditions is evidenced by the robust prediction
of group membership (psychotic versus nonpsychotic)
using the combination of total NES and FSIQ scores: the
discrimination between schizophrenia/schizoaffective
disorder and never mentally ill subjects was excellent,
with no member of either group misclassified as a mem-ber of the
other.
The present findings also suggest that diagnosis (i.e.,
disorders with persistent psychosis versus disorders
with mood episode-related psychosis) may differen-
tially influence development in these domains of neu-
ropsychiatric function. If similar findings are observed
in a larger sample of adolescent subjects with schizo-
phrenia/schizoaffective disorder and bipolar disorder
with psychotic features, inclusion of neurological and
cognitive examinations in the clinical assessment of
adolescents with psychotic disorders might improve
diagnostic accuracy. However, this suggestion is neces-sarily
speculative, as the present data indicate that NES
and IQ alone are not sufficient to the task of discrimi-
nating fully between bipolar disorder with psychotic
features and the other diagnostic groups included
herein. The single subject in each of those two groups
that was diagnostically misclassified by the model was
predicted to be a member of the bipolar disorder with
psychotic features group. Additionally, three of the eight
subjects in the bipolar disorder with psychotic features
group were diagnostically misclassified, with two iden-
tified as members of the schizophrenia/schizoaffective
disorder group and one identified as never mentally ill.
These observations suggest that inclusion of additional
factors in the model is needed to separate the bipolardisorder
with psychotic features subjects from those
with schizophrenia/schizoaffective disorder and
healthy comparison subjects. Alternatively, if NES and
IQ assessments are more strongly related to the neuro-
biology of these conditions than are phenomenological
psychiatric diagnostic assessments, then cross-sectional
K-SADS-PL and clinical interview-based diagnoses may
not be the optimal method by which to discriminate be-
tween adolescents with these diagnoses.2224
Several limitations of the present study require con-
sideration. It is possible that examiner knowledge of
subject diagnosis may contribute to NES scores, and that
examiner-subject interactions may influence the perfor-
mance of subjects on both neurological and cognitive
assessment measures. To the latter point, the blinded
cognitive assessment by a trained technician is consis-
tent with the methodology of other studies of this popu-
lation and should minimize the potential effect of cli-
nician bias on subject performance. The structured
administration and anchored scoring methods of the
NES limit the likelihood of clinician influence on subject
performance, although this concern cannot be assuaged
entirely. However, the magnitude of the NES differencesbetween
adolescents with and without psychosis ob-
served here, as well as the comparability of total NES
scores among subjects with and without psychosis to
those reported in previous studies,2,3 argue against eval-
uator bias as an explanation for the present findings.
The present findings also argue against psychotropic
medication administration as an explanation for differ-
ences in NES and IQ scores between subjects with and
without psychosis, as well as for differences in IQ scores
between the psychotic subgroups. However, the absence
of treatment-nave subjects precludes a more definitive
assessment of this issue.The subject groups were not identical
with respect to
gender, particularly for diagnostic subgroup compari-
sons. Though there is no a priori rationale for suggesting
an effect of gender on NES score,2,14,25 careful matching
of subjects is needed in future studies in order to more
fully evaluate the effect, if any, of gender in this
context.
The size of the present sample precludes evaluation
of a larger number of predictor variables, including
medications (individually or by class), gender, and so-
-
7/29/2019 Signos neurolgicos adolescentes con y sin psicosis
8/8
J Neuropsychiatry Clin Neurosci 19:3, Summer 2007
http://neuro.psychiatryonline.org 273
ARCINIEGAS et al.
cioeconomic status, and also reduces the power neededto
investigate significant predictor variables with
smaller effect sizes. Similarly, the nature of the cognitive
assessments employed in the present study precludes
evaluation of the relationships, if any, between specificdomains
of cognition and neurological dysfunction.Further studies of a
larger sample of adolescents with
psychotic disorders inclusive of these variables, includ-ing
longitudinal studies with periodic diagnostic reas-sessment,
symptom severity assessments, and structural
or functional neuroimaging using magnetic resonance
imaging, neurophysiological assessments (e.g., electro-
encephalography, evoked or event-related potentials,
and/or magnetoencephalography) are needed to ad-
dress these issues.
This work was supported by a grant from NIMH (R01MH63442) and a
grant from the Developmental Psychobiol-ogy Research Group (DPRG)
of the University of Colorado
Health Sciences Center, Denver, Colorado.
References
1. Andreasen NC, Paradiso S, OLeary DS: Cognitive dysmetriaas an
integrative theory of schizophrenia: a dysfunction in
cor-tical-subcortical-cerebellar circuitry? Schizophr Bull
1998;24:203218
2. Buchanan RW, Heinrichs DW: The neurological evaluation
scale(NES): a structured instrument for the assessment of
neurolog-ical signs in schizophrenia. Psychiatry Res 1989;
27:335350
3. Heinrichs DW, Buchanan RW: Significance and meaning of
neu-rological signs in schizophrenia. Am J Psychiatry 1988;
145:1118
4. Ross DE, Thaker GK, Buchanan RW, et al: Eye tracking
disorderin schizophrenia is characterized by specific
ocularmotordefectsand is associated with the deficit syndrome. Biol
Psychiatry1997; 42:781796
5. Keri S, Janka Z: Critical evaluation of cognitive
dysfunctions asendophenotypes of schizophrenia. Acta Psychiatr
Scand 2004;110:8391
6. Bender L: Childhood schizophrenia: clinical study of 100
schizo-phrenic children. Am J Orthopsychiatry 1947; 1740
7. Pollack M, Goldfarb W: The face-hand test in schizophrenic
chil-dren. Arch Neurol Psychiatry 1957; 77635776428. Karp BI,
Garvey M, Jacobsen LK, et al: Abnormal neurologic
maturation in adolescents with early-onset schizophrenia. Am
JPsychiatry 2001; 158:118122
9. Kaiser J, Gruzelier JH: The Adolescence Scale (AS-ICSM): a
toolfor the retrospective assessmentof puberty milestones.
ActaPae-diatrica 1999; Suppl:88648868
10. Kaufman J, Birmaher B, Brent D, et al: Schedule for
AffectiveDisorders and Schizophrenia for School-Age
Children-Presentand Lifetime Version (K-SADS-PL): initial
reliability and validitydata. J Am Acad Child Adolesc Psychiatry
1999; 38:10651069
11. Wechsler D: Wechsler Adult Intelligence Scale, III, manual.
SanAntonio, Tex, Psychological Corp, 1997
12. Wechsler D: Wechsler Intelligence Scale for children, III,
manual.San Antonio, Tex, Psychological Corp, 1991
13. The Psychological Corporation: The Wechsler Abbreviated
Scaleof Intelligence. San Antonio, Tex, Harcourt Brace
Jovanovich,1999
14. Arango C, Kirkpatrick B, Buchanan RW: Neurological signs
and
the heterogeneity of schizophrenia. Am J Psychiatry
2000;157:560565
15. Lawrie SM, Byrne M, Miller P, et al: Neurodevelopmental
indi-ces and the development of psychotic symptoms in subjects
at
high risk of schizophrenia. Br J Psychiatry 2001; 178:52453016.
Flyckt L, Sydow O, Bjerkenstedt L, et al: Neurological signs
and
psychomotor performance in patients with schizophrenia,
theirrelatives and healthy controls. Psychiatry Res 1999;
86:113129
17. Willcutt EG, Pennington BF, Olson RK, et al:
Neuropsychologicalanalyses of comorbidity between reading
disability and atten-tion deficit hyperactivity disorder: in search
of the common def-icit. Dev Neuropsychol 2005; 27:3578
18. Gochman PA, Greenstein D, Sporn A, et al: IQ stabilization
inchildhood-onset schizophrenia. Schizophr Res 2005; 77:271277
19. Seidman LJ, Kremen WS, Koren D, et al: A comparative
profileanalysis of neuropsychological functioning in patients
withschizophrenia and bipolar psychoses. Schizophr Res2002;
53:3144
20. Hobart MP, Goldberg R, Bartko JJ, et al: Repeatable battery
for
the assessment of neuropsychological status as a screening
testin schizophrenia, II: convergent/discriminant validity and
di-agnostic group comparisons. Am J Psychiatry 1999;
156:19511957
21. Zammit S, Allebeck P, David AS, et al: A longitudinal study
ofpremorbid IQ score and risk of developing schizophrenia, bi-polar
disorder, severe depression, and other nonaffective psy-choses.
Arch Gen Psychiatry 2004; 61:354360
22. McKenna K, Gordon CT, Lenane M, et al: Lookingfor
childhood-onset schizophrenia: the first 71 cases screened. J Am
AcadChildAdolesc Psychiatry 1994; 33:636644
23. Nicolson R, Lenane M, Brookner F, et al: Children and
adoles-cents with psychotic disorder not otherwise specified: a 2-
to 8-year follow-up study. Compr Psychiatry 2001; 42:319325
24. Stayer C, Sporn A, Gogtay N, et al: Looking for
childhoodschizophrenia: case series of false positives. J Am Acad
Child
Adolesc Psychiatry 2004; 43:1026102925. Arango C, Bartko JJ,
Gold JM, et al: Prediction of neuropsycho-
logical performance by neurological signs in schizophrenia. AmJ
Psychiatry 1999; 156:13491357