Supraventriculaire Ritmestoornissen
Prof. Dr. Hein Heidbüchel
KU Leuven
KU Leuven
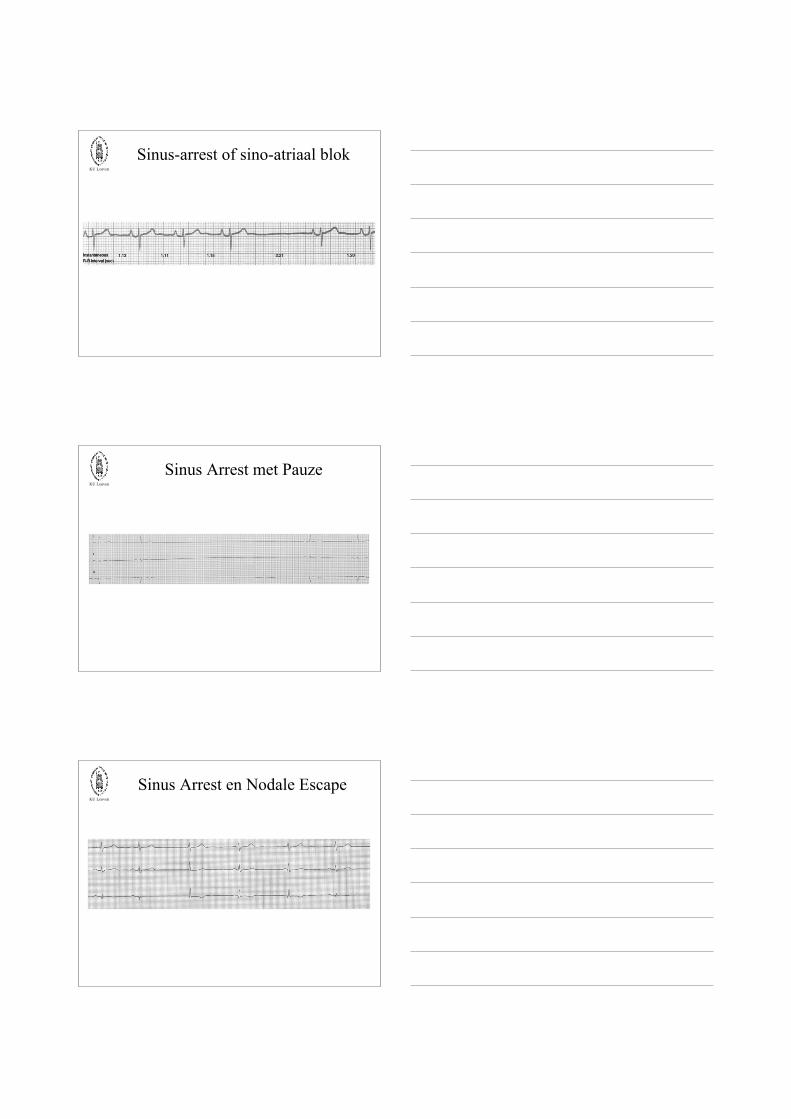
Respiratoire Sinusaritmie
KU Leuven
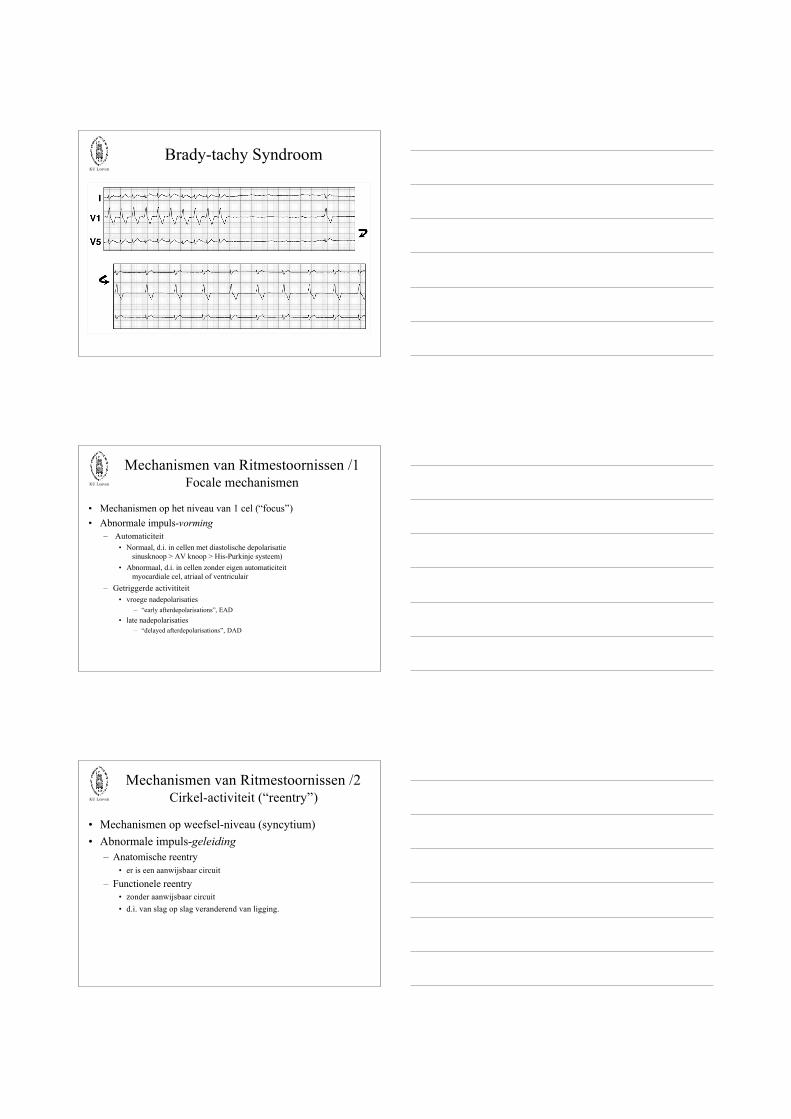
Wandering Pacemaker

KU Leuven
Laag-atriaal ritmeSinus Coronarius Ritme
KU Leuven
Nodaal Ritme
KU Leuven
Snel nodaal ritme…
KU Leuven
Sinus-arrest of sino-atriaal blok
KU Leuven
Sinus Arrest met Pauze
KU Leuven
Sinus Arrest en Nodale Escape
KU Leuven
Brady-tachy Syndroom
KU Leuven
Mechanismen van Ritmestoornissen /1Focale mechanismen
• Mechanismen op het niveau van 1 cel (“focus”)• Abnormale impuls-vorming
– Automaticiteit• Normaal, d.i. in cellen met diastolische depolarisatie
sinusknoop > AV knoop > His-Purkinje systeem)• Abnormaal, d.i. in cellen zonder eigen automaticiteit
myocardiale cel, atriaal of ventriculair– Getriggerde activititeit
• vroege nadepolarisaties– “early afterdepolarisations”, EAD
• late nadepolarisaties– “delayed afterdepolarisations”, DAD
KU Leuven
Mechanismen van Ritmestoornissen /2Cirkel-activiteit (“reentry”)
• Mechanismen op weefsel-niveau (syncytium)• Abnormale impuls-geleiding
– Anatomische reentry• er is een aanwijsbaar circuit
– Functionele reentry• zonder aanwijsbaar circuit• d.i. van slag op slag veranderend van ligging.

KU Leuven
Vroege Nadepolarisaties(“early afterdepolarisations”, EAD)
Oscillaties van de membraanpotentiaal op een (te lang) plateau
bvb. hypokaliëmie, bradycardie, medicatie met QT-verlenging
KU Leuven
Late Nadepolarisaties(“delayed afterdepolarisations”, DAD)
Oscillaties van de membraanpotentiaal na volledige repolarisatie, door cyclische vrijzettingvan Ca2+ door het sarcoplasmatisch reticulum in een met calcium overladen cel.
De Ca2+-vrijzetting induceert een depolariserende stroom.
bvb. ischemie met reperfusie, digitalis-intoxicatie, ...
KU Leuven
Cirkel-aritmieënOntstaan wanneer er unidirectioneel blok optreedt,
met geleiding rondom het blok:
bvb. ventrikel tachycardie na een oud infarct,cirkel-tachycardie bij WPW, ...
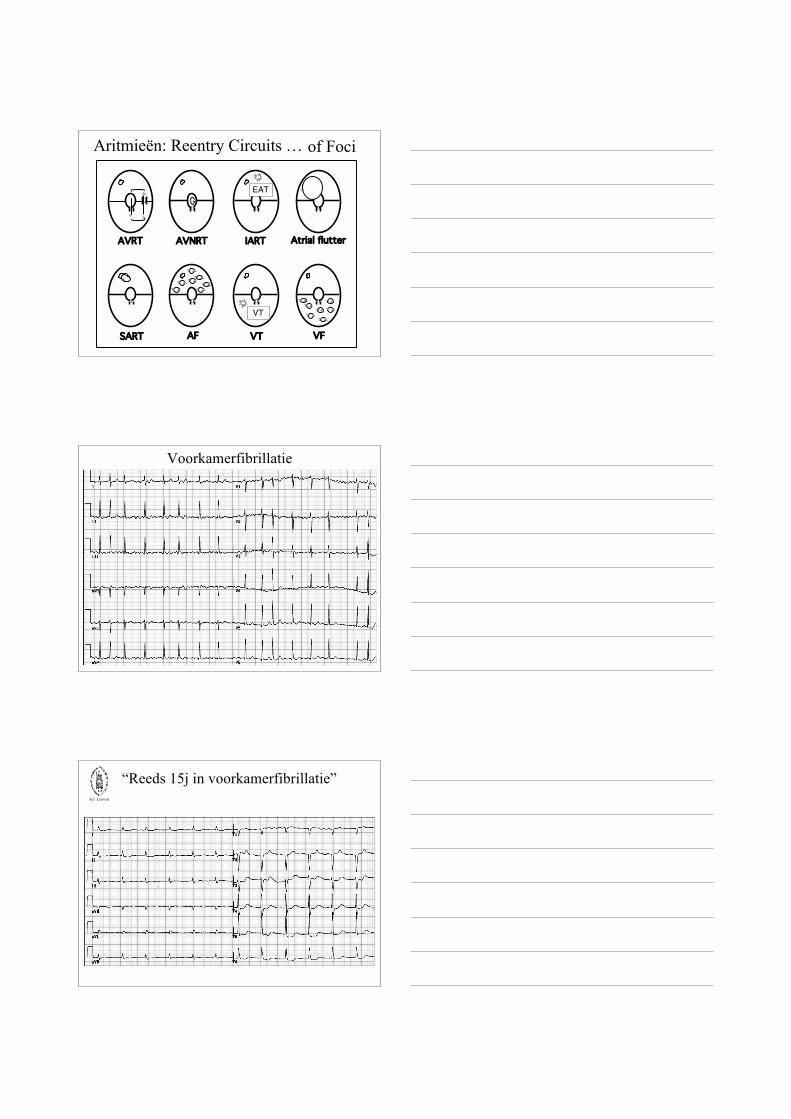
Aritmieën: Reentry Circuits …
AVRT AVNRT IART Atrial flutter
SART AF VT VF
of Foci
EAT
VT
Voorkamerfibrillatie
KU Leuven
“Reeds 15j in voorkamerfibrillatie”

KU Leuven
VoorkamerflutterTypisch, Type 1
KU Leuven
Flutter: Definitie & Classificatie
• Definitie: regelmatige atriale activatie (>250/min)• Indeling gebaseerd op frequentie:
– Type I: 250 tot 340/min– Type II: 340 tot 430/min
• Indeling gebaseerd op morfologie van de flutter-golven:– Typische (“common”) flutter: zaagtand in II, III en aVF– Atypische (“uncommon”) flutter: positieve (dikwijls discrete) P-toppen in
de inferior afleidingen
• In het kader van congenitaal hartlijden en/of na hartchirurgie:– “intra-atriale reentry tachycardie”, IART (Mustard; ASD; ...)
KU Leuven
Flutter: Type 1 (typisch) en 2 (atypisch)
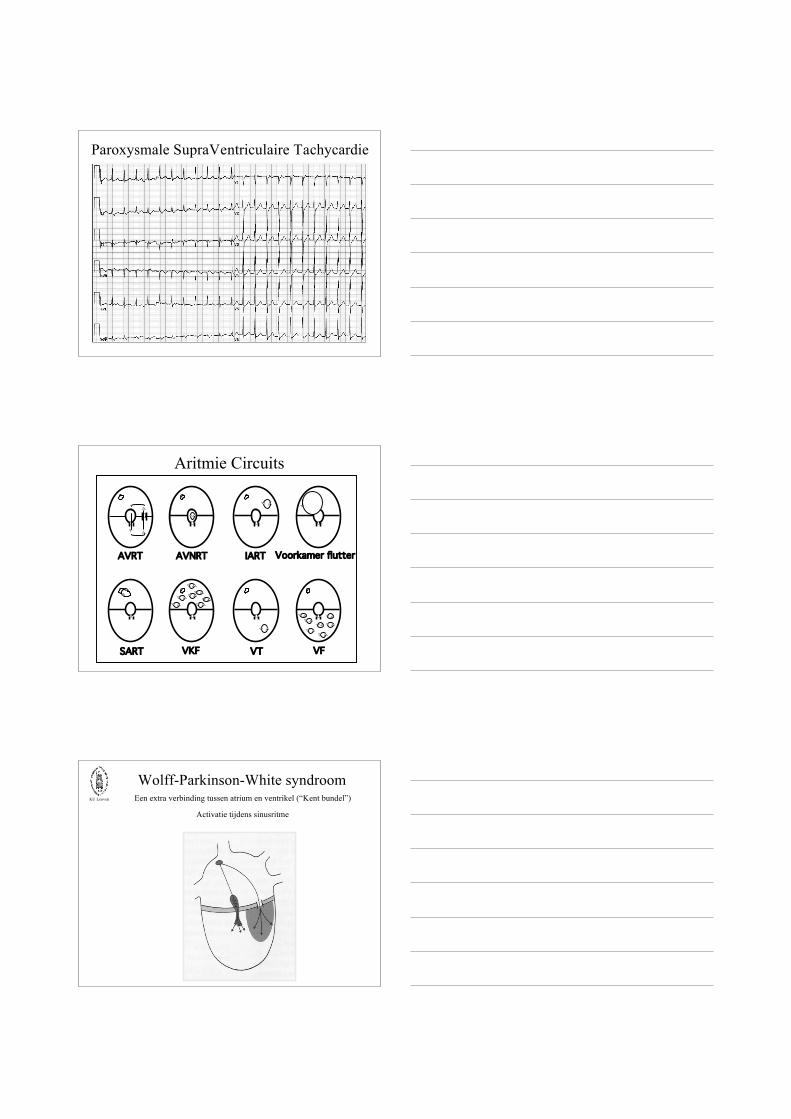
Paroxysmale SupraVentriculaire Tachycardie
Aritmie Circuits
AVRT AVNRT IART Voorkamer flutter
SART VKF VT VF
KU Leuven
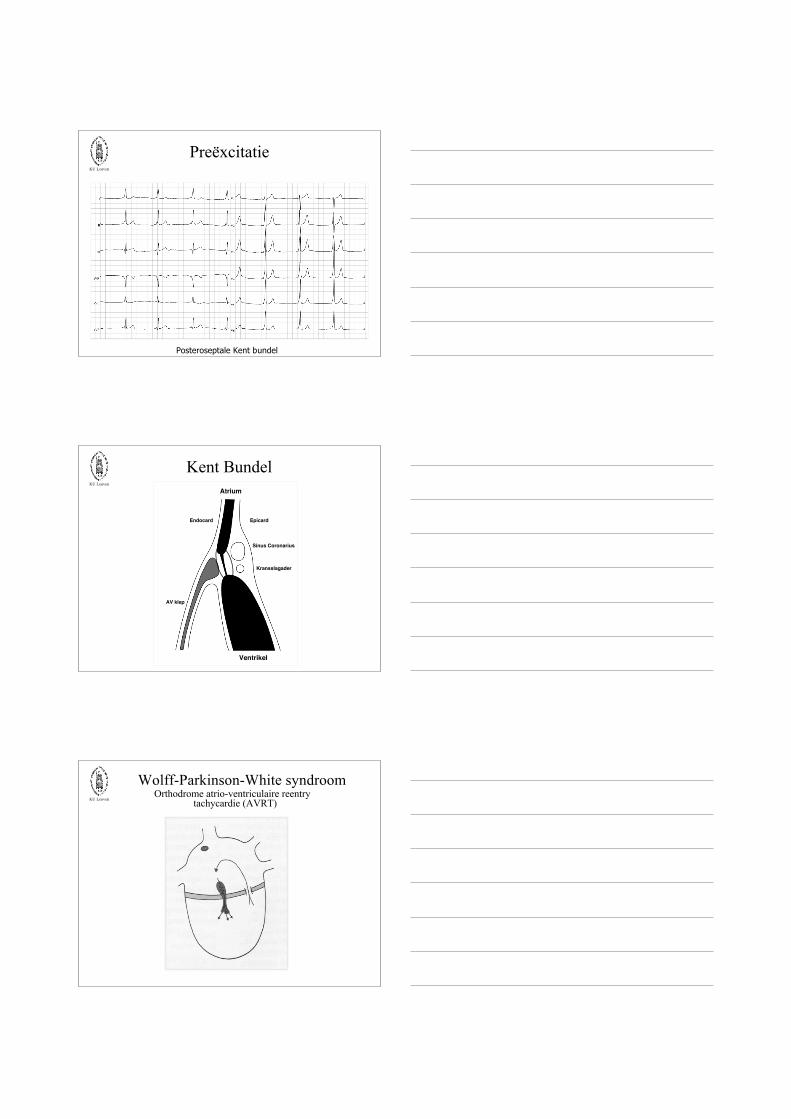
Wolff-Parkinson-White syndroomEen extra verbinding tussen atrium en ventrikel (“Kent bundel”)
Activatie tijdens sinusritme
KU Leuven
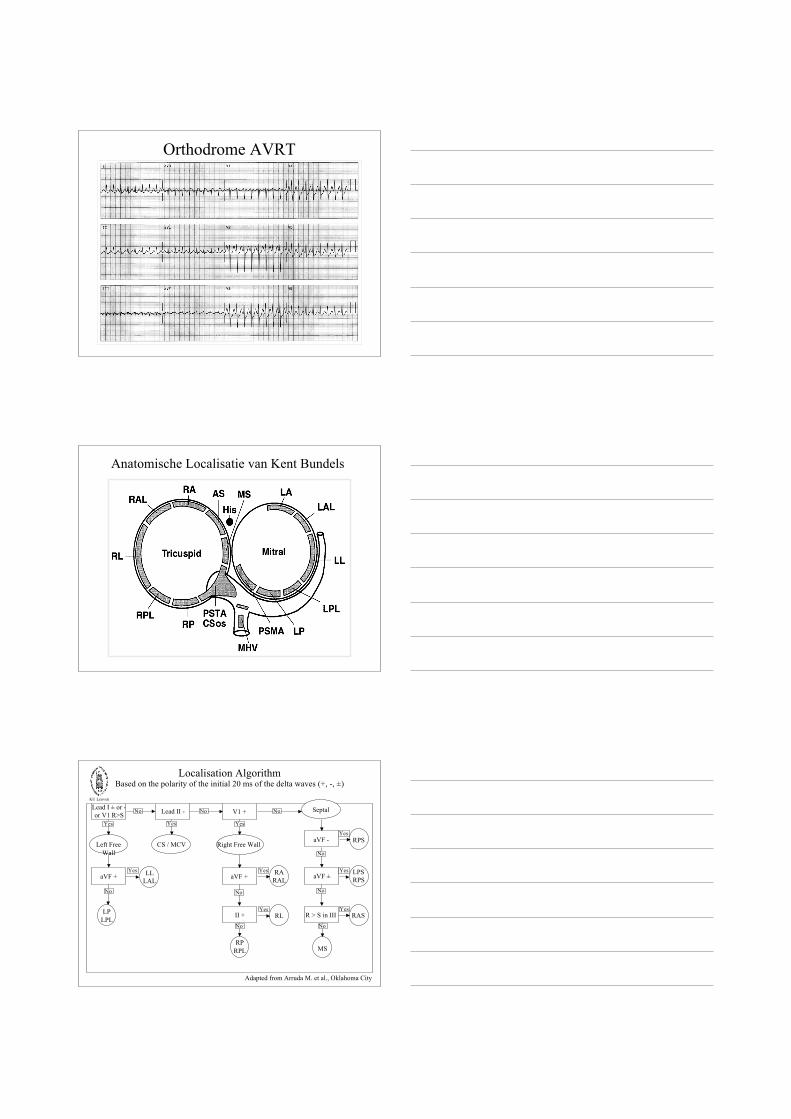
Preëxcitatie
Posteroseptale Kent bundel
KU Leuven
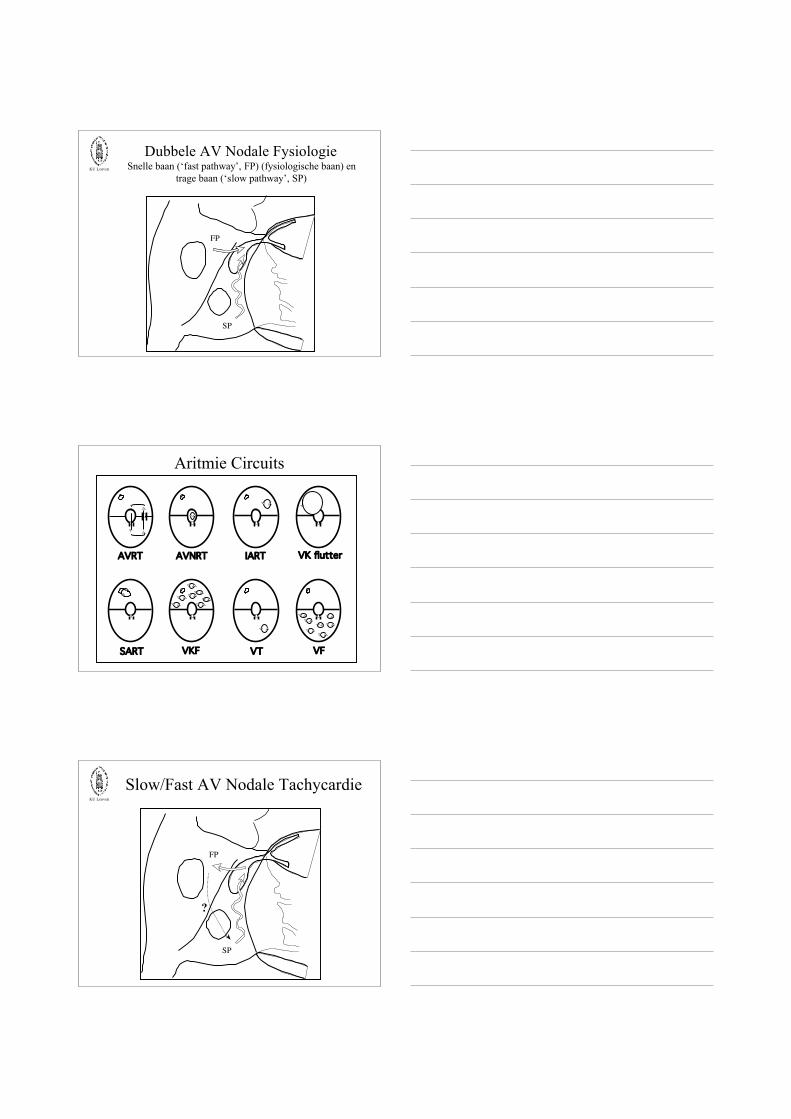
Kent BundelAtrium
Ventrikel
Sinus Coronarius
Kransslagader
AV klep
Endocard Epicard
KU Leuven
Wolff-Parkinson-White syndroomOrthodrome atrio-ventriculaire reentry
tachycardie (AVRT)
Orthodrome AVRT
Anatomische Localisatie van Kent Bundels
KU Leuven
Localisation AlgorithmBased on the polarity of the initial 20 ms of the delta waves (+, -, ±)
Lead I ± or -or V1 R>S Lead II - V1 +
aVF + aVF +
II +
aVF ±
R > S in III
aVF -Left Free
WallCS / MCV Right Free Wall
Septal
LLLAL
LPLPL
RPRPL
RL
RARAL
RPS
LPSRPS
RAS
MS
Yes
No
Yes
Yes Yes
Yes
Yes
Yes
Yes
Yes
No No
No
No No
No
No
No
Adapted from Arruda M. et al., Oklahoma City
KU Leuven
SP
FP
Dubbele AV Nodale FysiologieSnelle baan (‘fast pathway’, FP) (fysiologische baan) en
trage baan (‘slow pathway’, SP)
Aritmie Circuits
AVRT AVNRT IART VK flutter
SART VKF VT VF
KU Leuven
SP
FP
Slow/Fast AV Nodale Tachycardie
?
KU Leuven
PSVT…
KU Leuven
… gestopt door carotis-massage
KU Leuven
AVNRT: ECG Patterns
KU Leuven
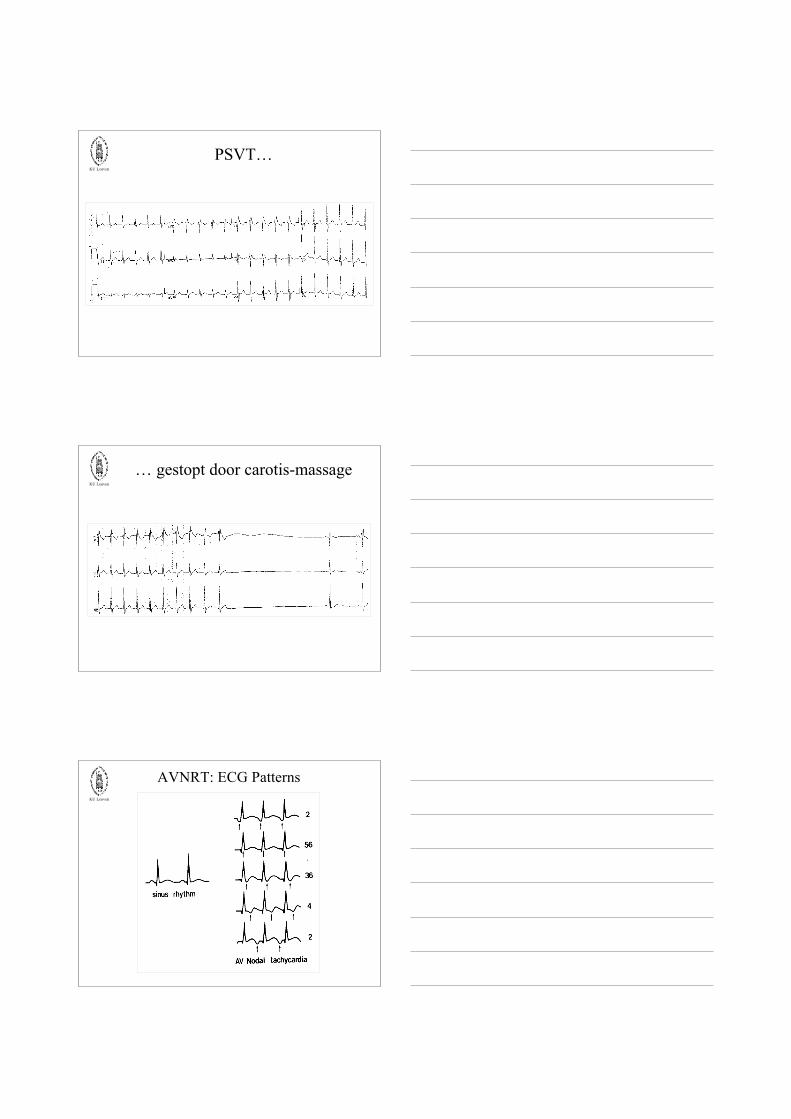
QRS Alternans
KU Leuven
Carotismassage
KU Leuven
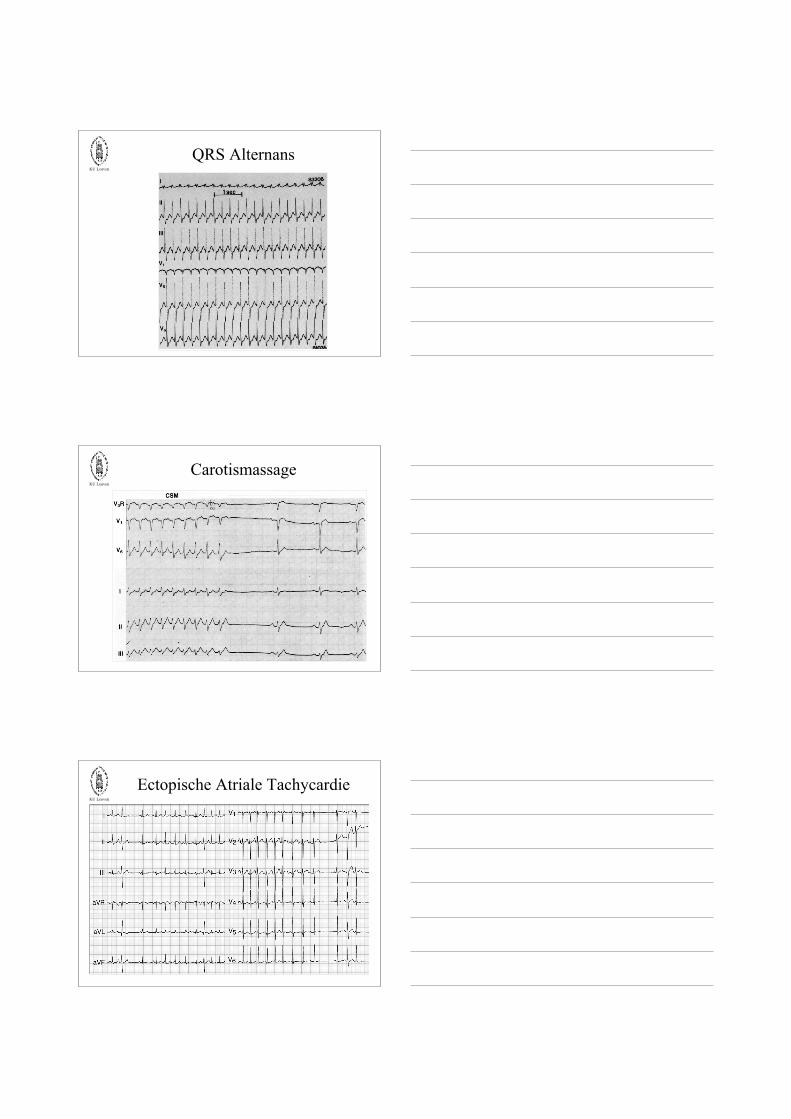
Ectopische Atriale Tachycardie

KU Leuven
Localisation of EATbased on the polarity of the P-wave
• V1:– positive ⇒ left atrium– neg., biphasic or isoelectric ⇒ right atrium
• aVL:– positive or biphasic ⇒ right atrium– negative or isoelectric ⇒ left atrium
• Note:– if V1 = positive and aVL is also positive
(“conflicting”)⇒ right superior pulmonary vein⇒ P-wave will be biphasic in V1 during NSR
PJRTPermanente Junctionele Reentry Tachycardie
Recommended

















