Embed Size (px)
Citation preview

EXTERN CONFERENCE
นศพ. ศิวพร เลิศสาครประเสรฐิคณะแพทยศาสตรโ์รงพยาบาลรามาธบิดี
2 ธนัวาคม 2559
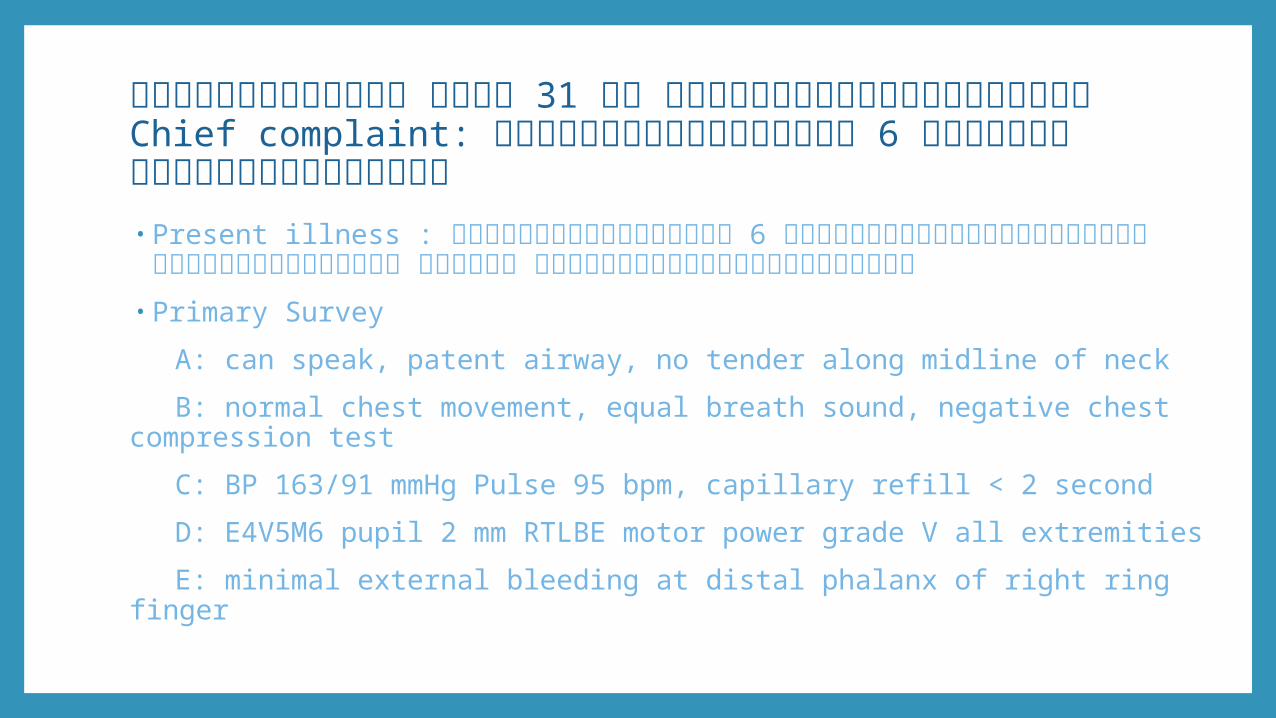
ผู้ป่วยชายไทย อายุ 31 ปี ภมูลิำาเนานครราชสมีา Chief complaint: ยางรถระเบดิใสม่อื 6 ชัว่โมงก่อนมาโรงพยาบาล• Present illness : ยางรถระเบดิใสม่อื 6 ชัว่โมงก่อนมาโรงพยาบาล จำาเหตกุารณ์ได้ ไมส่ลบ เจบ็
ท่ีมอืขวาและมอืซา้ย• Primary Survey
A: can speak, patent airway, no tender along midline of neck
B: normal chest movement, equal breath sound, negative chest compression test
C: BP 163/91 mmHg Pulse 95 bpm, capillary refill < 2 second
D: E4V5M6 pupil 2 mm RTLBE motor power grade V all extremities
E: minimal external bleeding at distal phalanx of right ring finger
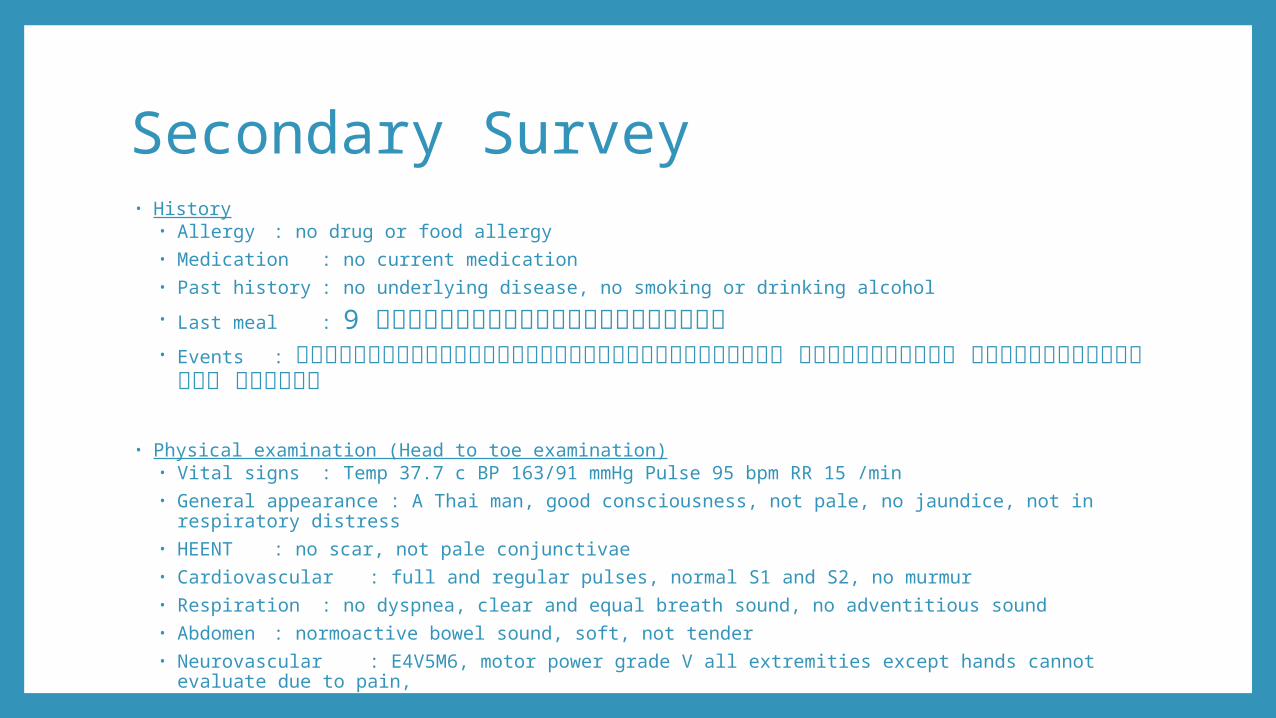
Secondary Survey• History
• Allergy : no drug or food allergy• Medication : no current medication• Past history : no underlying disease, no smoking or drinking alcohol
• Last meal : 9 ชัว่โมงก่อนมาโรงพยาบาล• Events : ยางรถระเบดิขณะเติมยางรถมอเตอรไ์ซค์ มแีผลท่ีมอื จำาเหตกุารณ์ได้ ไมส่ลบ
• Physical examination (Head to toe examination)• Vital signs : Temp 37.7 c BP 163/91 mmHg Pulse 95 bpm RR 15 /min• General appearance : A Thai man, good consciousness, not pale, no jaundice, not in respiratory distress• HEENT : no scar, not pale conjunctivae• Cardiovascular : full and regular pulses, normal S1 and S2, no murmur• Respiration: no dyspnea, clear and equal breath sound, no adventitious sound• Abdomen : normoactive bowel sound, soft, not tender• Neurovascular : E4V5M6, motor power grade V all extremities except hands cannot evaluate due to pain,
normal Pinprick sensation
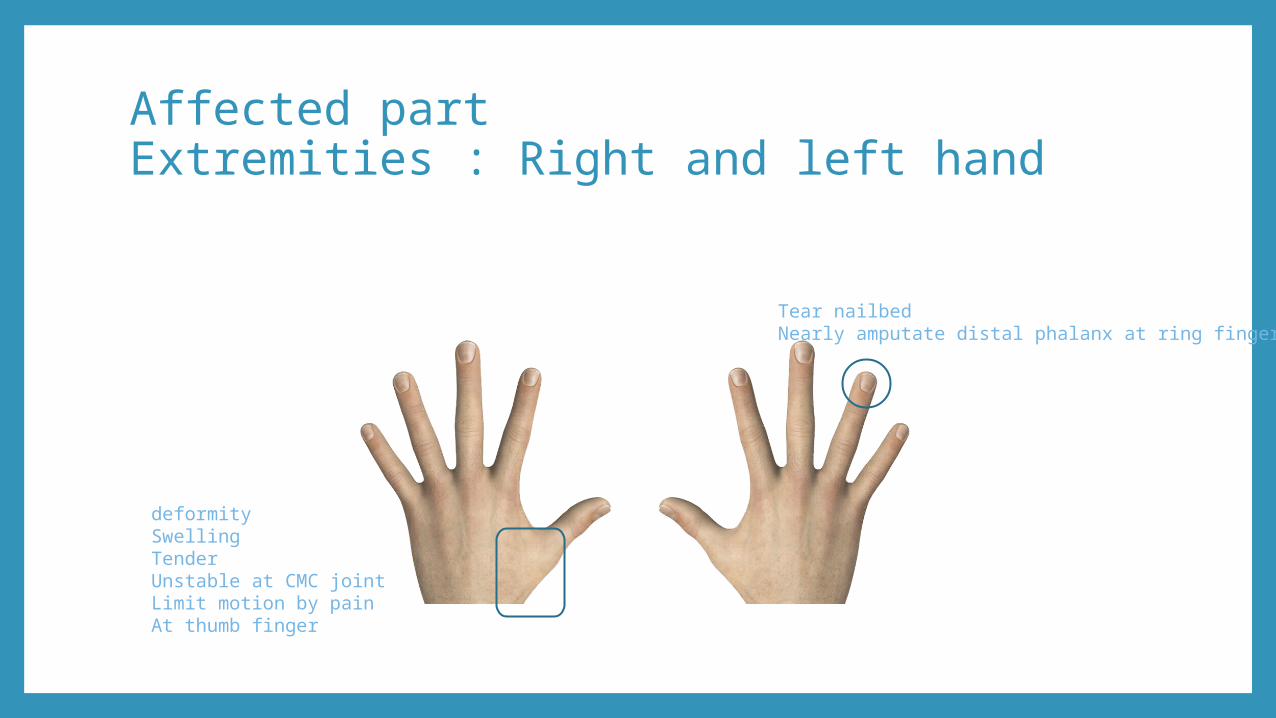
Affected partExtremities : Right and left hand
Tear nailbedNearly amputate distal phalanx at ring finger
deformitySwellingTenderUnstable at CMC jointLimit motion by painAt thumb finger
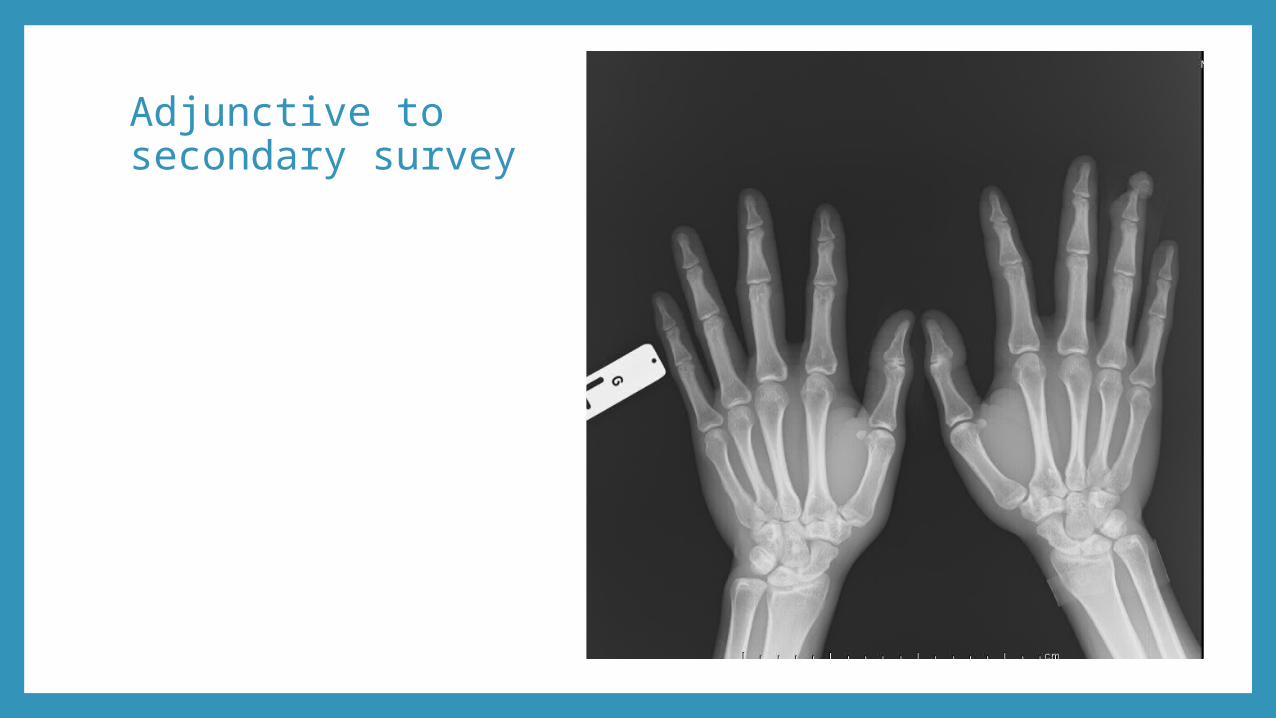
Adjunctive to secondary survey
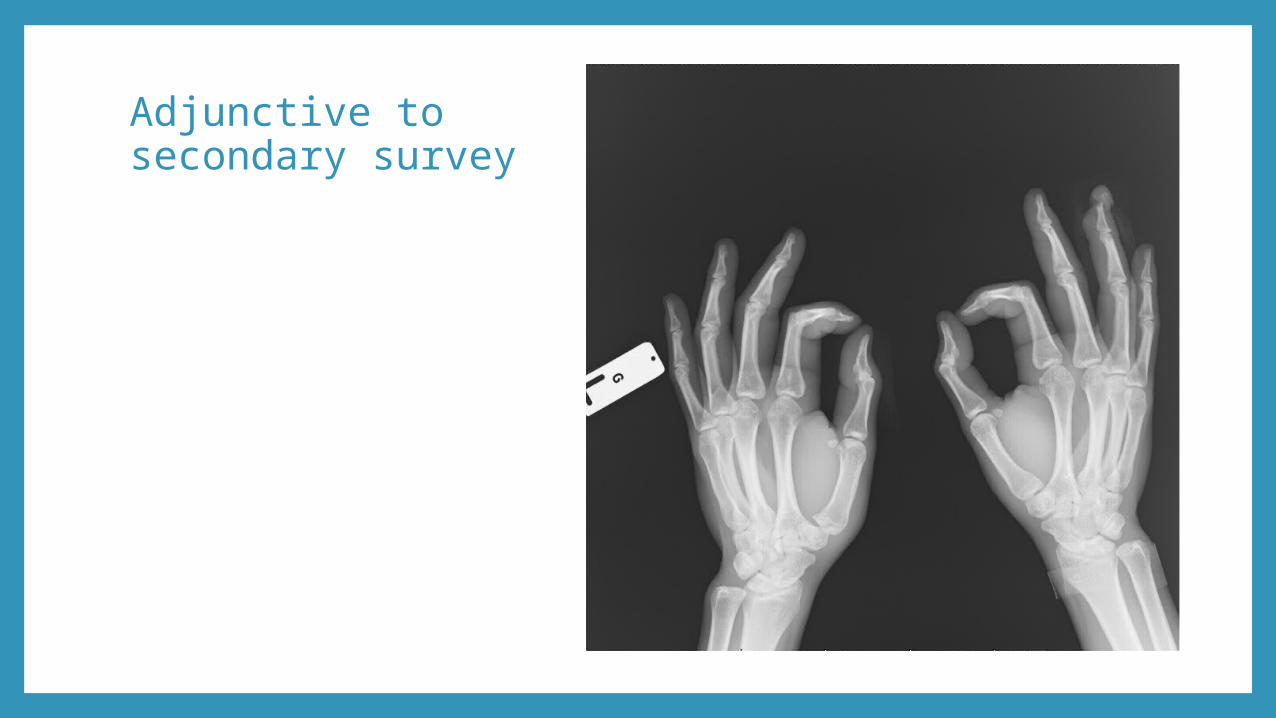
Adjunctive to secondary survey
Diagnosis• Close fracture of carpometacarpal of Left thumb finger • Open fracture distal phalanx of Right ring finger
Management• Specific treatment
• Open fracture distal phalanx of Right ring finger • Debridement
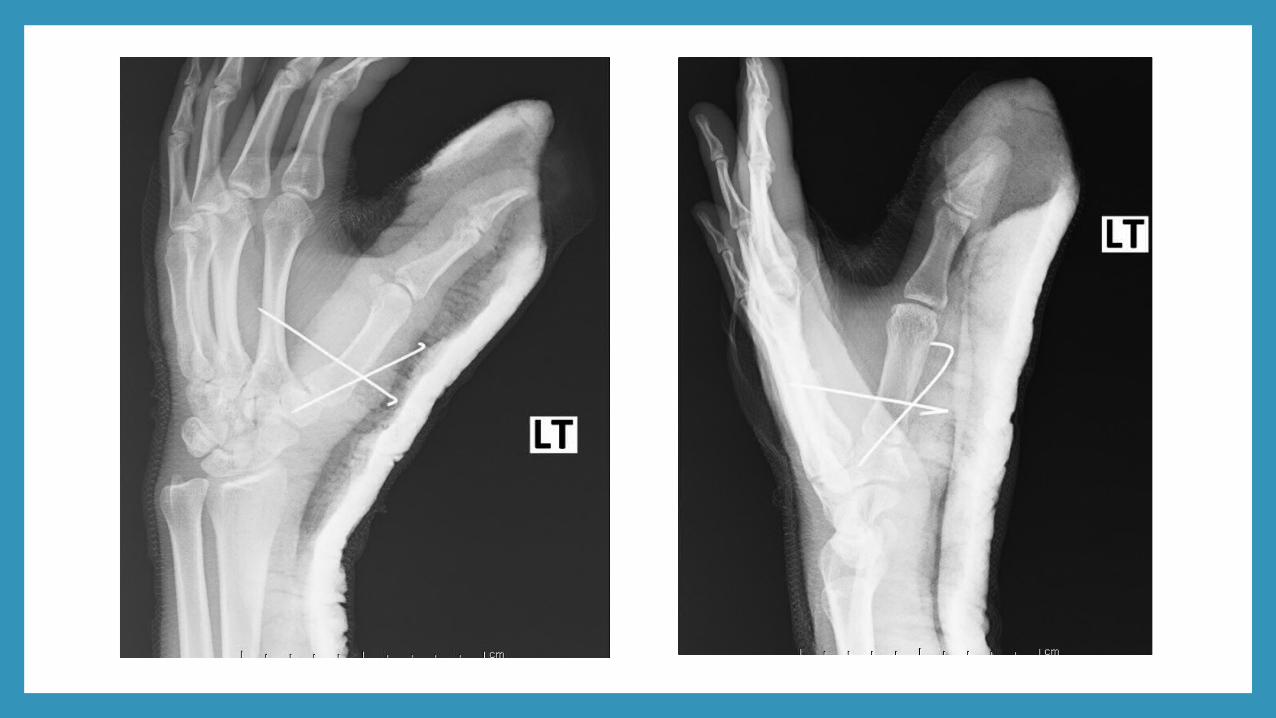
• Close fracture of carpometacarpal of Left thumb finger • K-wire fixation with close pinning
• Supportive treatment• Pain control• Wound dressing
• Follow up OPD

HAND INJURYBones
Ligaments
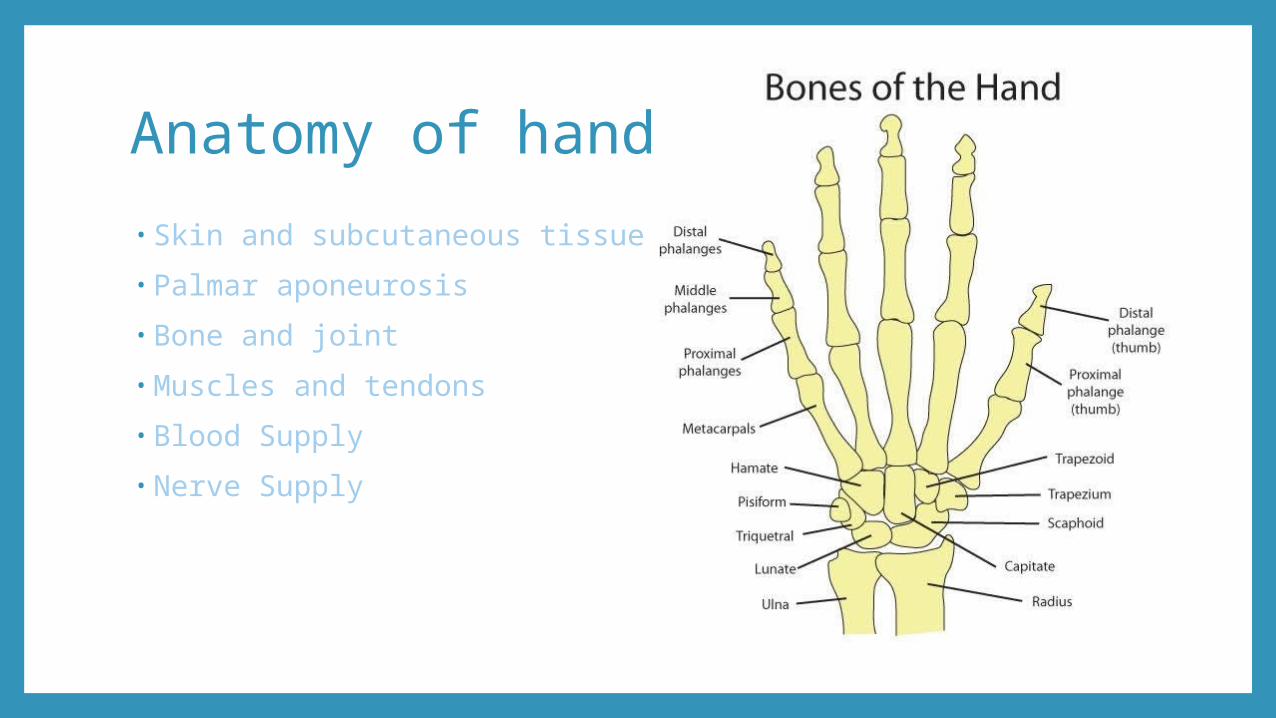
Anatomy of hand• Skin and subcutaneous tissue
• Palmar aponeurosis
• Bone and joint
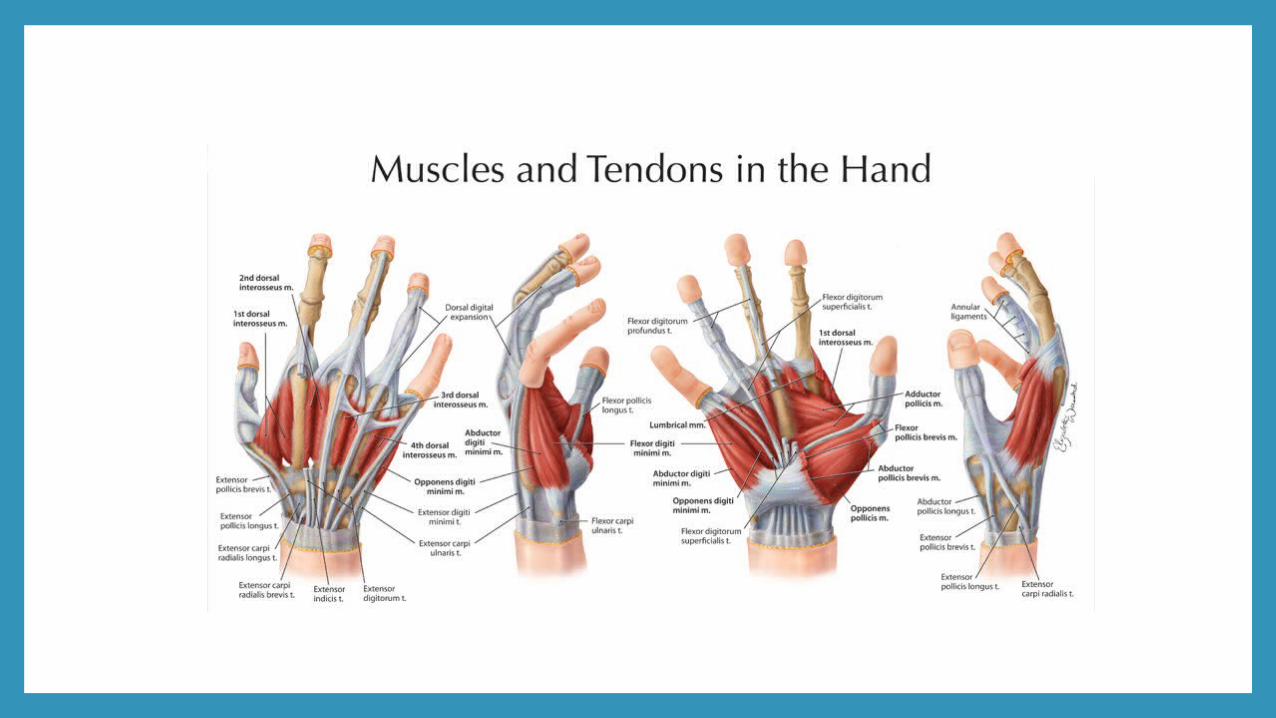
• Muscles and tendons
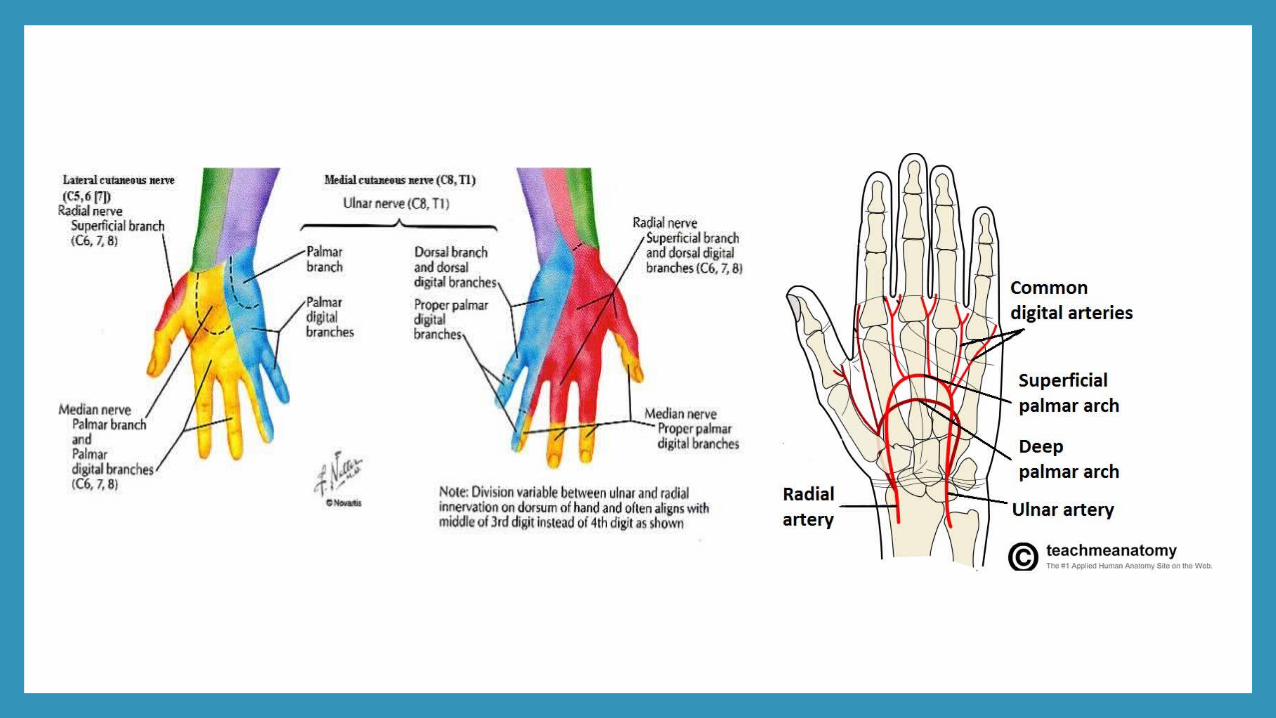
• Blood Supply
• Nerve Supply
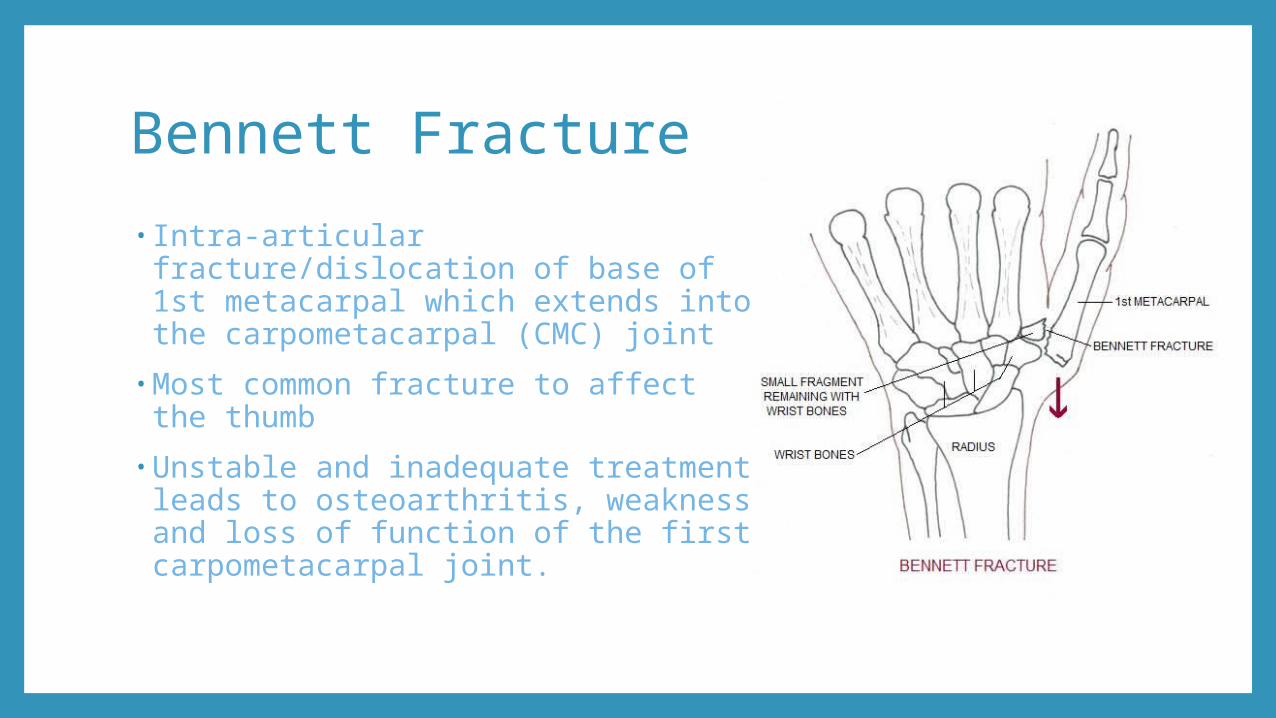
Bennett Fracture• Intra-articular fracture/dislocation of base of 1st metacarpal which extends into the carpometacarpal (CMC) joint
•Most common fracture to affect the thumb
•Unstable and inadequate treatment leads to osteoarthritis, weakness and loss of function of the first carpometacarpal joint.
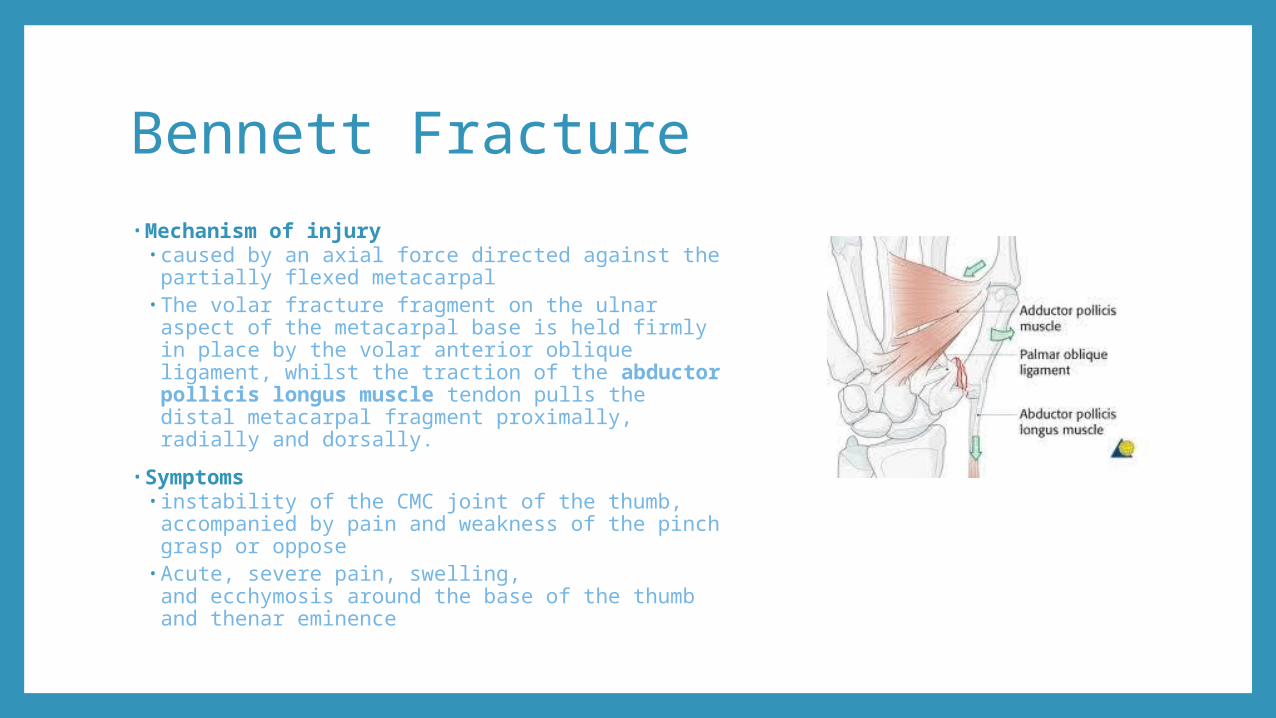
Bennett Fracture• Mechanism of injury
• caused by an axial force directed against the partially flexed metacarpal
• The volar fracture fragment on the ulnar aspect of the metacarpal base is held firmly in place by the volar anterior oblique ligament, whilst the traction of the abductor pollicis longus muscle tendon pulls the distal metacarpal fragment proximally, radially and dorsally.
• Symptoms• instability of the CMC joint of the thumb,
accompanied by pain and weakness of the pinch grasp or oppose
• Acute, severe pain, swelling, and ecchymosis around the base of the thumb and thenar eminence
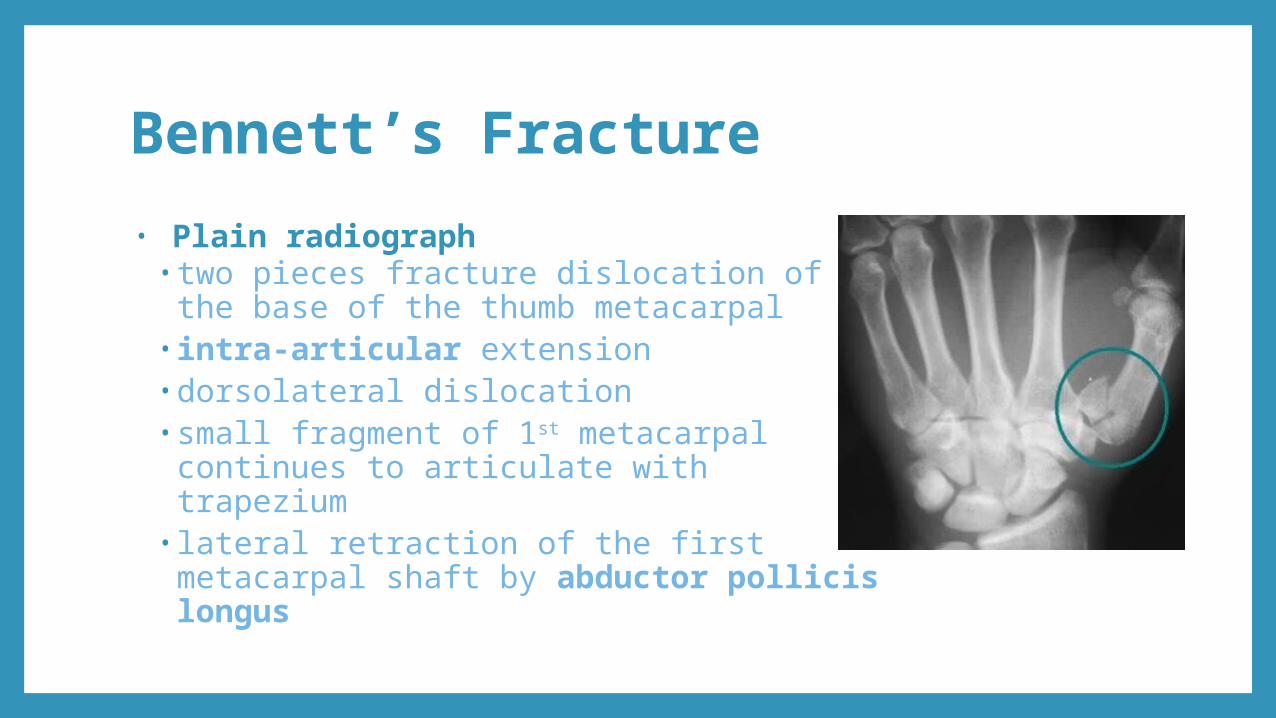
Bennett’s Fracture• Plain radiograph
• two pieces fracture dislocation of the base of the thumb metacarpal
• intra-articular extension •dorsolateral dislocation•small fragment of 1st metacarpal continues to articulate with trapezium
• lateral retraction of the first metacarpal shaft by abductor pollicis longus
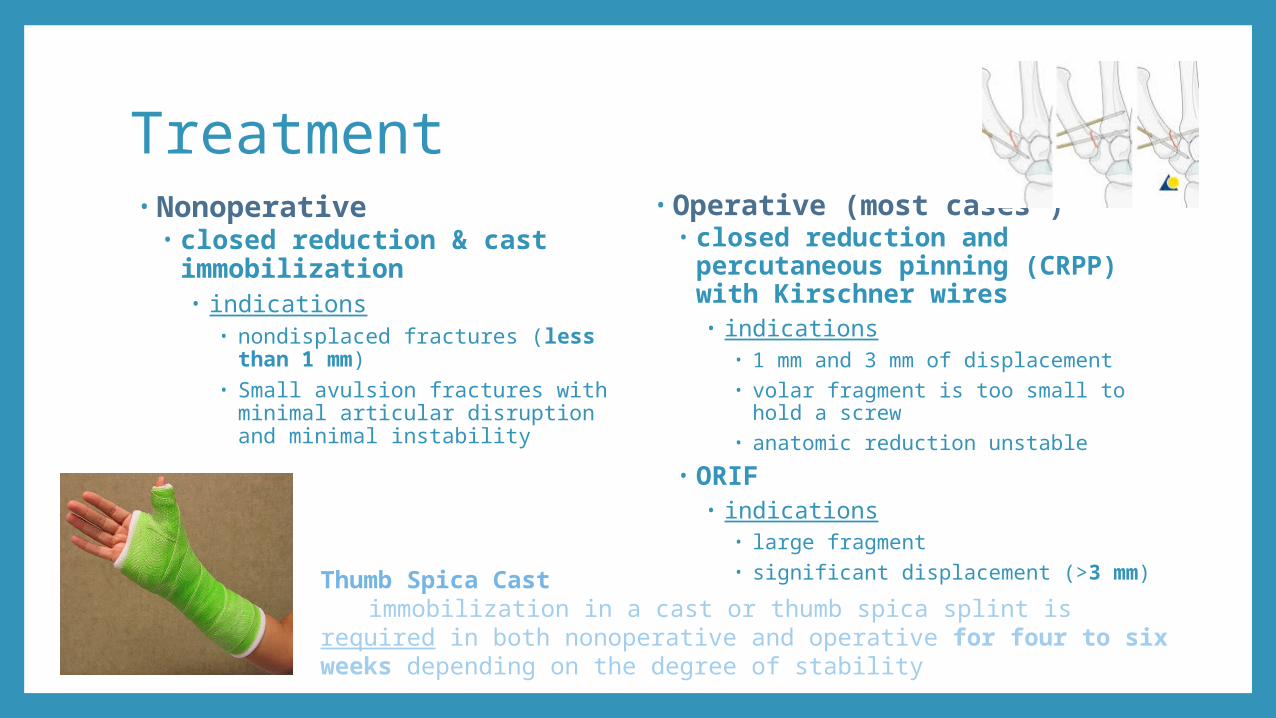
Treatment• Nonoperative
• closed reduction & cast immobilization• indications
• nondisplaced fractures (less than 1 mm)
• Small avulsion fractures with minimal articular disruption and minimal instability
• Operative (most cases*)• closed reduction and
percutaneous pinning (CRPP) with Kirschner wires• indications
• 1 mm and 3 mm of displacement• volar fragment is too small to hold a
screw• anatomic reduction unstable
• ORIF• indications
• large fragment• significant displacement (>3 mm)Thumb Spica Cast
immobilization in a cast or thumb spica splint is required in both nonoperative and operative for four to six weeks depending on the degree of stability
Complications• Reduced movement at the carpometacarpal / severe long-term dysfunction
of the hand• Many important activities of daily life are dependent on the ability to
grasp, pinch, and oppose the thumb. In fact, thumb function constitutes about 50% of overall hand function.
• Osteoarthritis/post-traumatic arthritis• result of osteocartilaginous injury
• Recurrent joint subluxation/instability.• Postoperative infection of skin/carpometacarpal joint/osteomyelitis• Dorsal sensory branches of radial nerve injury causing anaesthesia• pseudoarthrosis
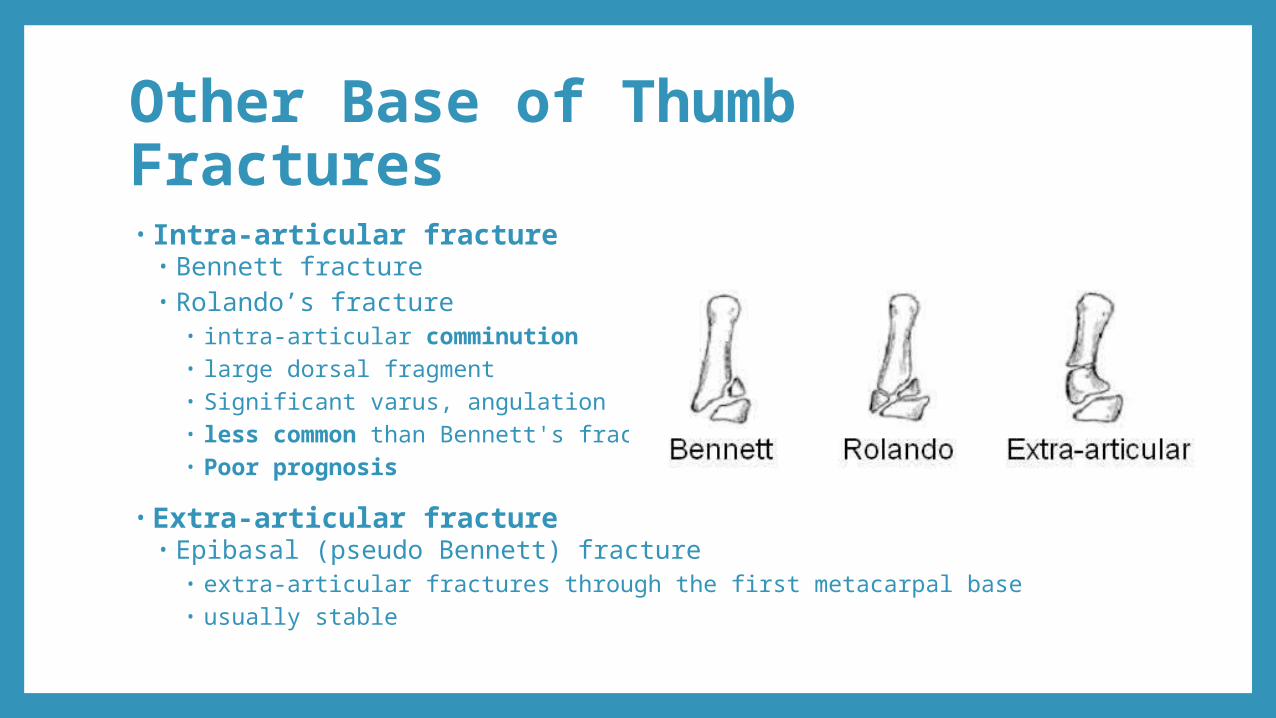
Other Base of Thumb Fractures• Intra-articular fracture
• Bennett fracture• Rolando’s fracture
• intra-articular comminution• large dorsal fragment• Significant varus, angulation • less common than Bennett's fracture• Poor prognosis
• Extra-articular fracture • Epibasal (pseudo Bennett) fracture
• extra-articular fractures through the first metacarpal base • usually stable
References• Orthobullets เรื่อง Base of Thumb Fractures• radiopaedia.org


![Extern conference. tung[1]](https://img.pdfslide.tips/doc/110x75/587eb10c1a28abbb688b5191/extern-conference-tung1.jpg)