Embed Size (px)
DESCRIPTION
Mối quan hệ giữa chất lượng dịch vụ và hài lòng bệnh nhân tại bệnh viện Nhị Hải Dương
Citation preview

Shu - Te University
College of Management
Graduate School of Business Administration
Master
A Relationship Study between healthcare
quality and patient’s key caretaker satisfaction
for Hai Duong children’s hospital in Viet Nam.
Student: Nhu Ngoc Thanh
ID: 99733427
Advisor: Dr.Jau-Shyong Wang
Co-Advisor: Dr. Pham Vu Thang
September, 2013

Shu-Te University
Graduate School of
Business A
dministration
Thesis
A
relationship study between healthcare quality and
patient’s key caretaker satisfaction for Hai D
uong children’s hospital in V
iet Nam
Nhu N
goc Thanh
September, 2013

A relationship study between healthcare quality and patient’s key
caretaker satisfaction for Hai Duong children’s hospital in
Viet Nam.
Student : Nhu Ngoc Thanh
Advisor : Dr.Jau-Shyong Wang
Co-Advisor : Dr. Pham Vu Thang
A Thesis
Submitted to the
Graduate School of Business Administration
College of Management
Shu-Te University
In Partial Fulfillment of the Requirements
For the Degree of
Master of Science in
Business Administration
September, 2013

i
Shu-Te University
Graduate School of Business Administration
A relationship study between healthcare quality and patient’s key
caretaker satisfaction for Hai Duong children’s hospital in
Viet Nam. Student : Nhu Ngoc Thanh
Advisor : Dr.Jau-Shyong Wang Co-advisor : Dr. Pham Vu Thang
Abstract
The main purpose of this thesis is to research on the satisfaction of the patients
with factors of service quality in SERVQUAL model in Hai Duong Children’s Hospital
in Vietnam.
The research method used in this thesis is quantitative research with some
statistical step of data analysis and processing such as: descriptive statistics, scale
verification, factor analysis, correlation analysis, and regression analysis. The
supporting software is SPSS 20.0.
The research results showed that the satisfaction of patients with disease diagnosis
and treatment of the hospital was affected by four factors including: (1) assurance, (2)
empathy, (3) responsiveness, and (4) tangibles. The factor “reliability” has no impact on
general satisfaction of the patients. These factors positively influence the satisfaction of
the patients with services.
The research results also showed no differences between groups of different age,
income, job and education level.
In addition, the research also pointed out the limitations and directtions for further
researches.
Keywords: the satisfaction of patients, healthcare, service quality, SERVQUAL.

ii
Acknowledgements
I am so happy having chance to express my gratitude and my deep thanks to those
who have supported and encouraged me to complete this study. Without them it could
be difficult for me to fulfill this thesis.
Firstly, I would like to thank and appreciate the advices of Dr. Jau-Shyong Wang
and Dr. Sheng-Jung Li in the Faculty of the School of Business Administration, Shu-te
University and Dr. Pham Vu Thang, who have enthusiastically guided me in this
research process. Hints and tips by Dr. Wang, Dr. Li and Dr. Thang have great
importance for me to perform this research. Dr. Wang, Dr. Li and Dr. Thang are willing
to help me at any time and in any situation.
Secondly, I would like to thank the team of doctors, hospital staffs at Hai Duong
Hospital as well as my colleagues and especially the patients who took the time to
discuss and complete the questionnaire and gave advices for my research.
Finally I would like to express my sincere gratitude to my family, wife and
children, who have always encouraged me during the course of this study.
Nhu Ngoc Thanh
September, 2013

iii
Table of Contents
Abstract ......................................................................................................................... i
Acknowledgements ....................................................................................................... ii
Table of Contents ......................................................................................................... iii
List of Tables ............................................................................................................... vi
List of Figures ............................................................................................................. vii
CHAPTER 1 INTRODUCTION ................................................................................... 1
1.1 Research Background.................................................................................... 1
1.2 Research Motivations .................................................................................... 1
1.3 Research Purposes ........................................................................................ 5
1.4 Research Procedures ..................................................................................... 5
CHAPTER 2 LITERATURE REVIEW ........................................................................ 8
2.1 The concepts and characteristics of service.................................................... 8
2.2 Service quality ............................................................................................ 10
2.3 Customer satisfaction .................................................................................. 11
2.4 The relationship between service quality and customer satisfaction ............. 11
2.5 Research models of service quality and customer satisfaction...................... 11
2.5.1 The service quality five gap model ..................................................... 12
2.5.2 SERVQUAL model ........................................................................... 14
2.5.3 European Customer Satisfaction Index model .................................... 14
2.6 Some recent researches on customer satisfaction in the field of health care . 16
CHAPTER 3 RESEARCH METHODOLOGY ........................................................... 18
3.1 Research model ........................................................................................... 18
3.2 Research Hypotheses .................................................................................. 19
3.3 Measurement of observed variables ............................................................. 19
3.4 Research Design ......................................................................................... 21
3.4.1 Discussion for scale adjustment.......................................................... 21
3.4.2 Scale selection ................................................................................... 22
3.4.3 Research sample selection .................................................................. 23

iv
3.5 Method of data analysis............................................................................... 25
3.5.1 Descriptive Statistics .......................................................................... 25
3.5.2 Testing the reliability of scales ........................................................... 25
3.5.3 Explore factor analysis ....................................................................... 25
3.5.4 Building the regression function ......................................................... 26
3.5.5 Testing the research hypotheses ......................................................... 26
CHAPTER 4 RESEARCH RESULTS ........................................................................ 28
4.1 Descriptive statistics ................................................................................... 28
4.1.1 Sample classification by age of patients ............................................. 28
4.1.2 Sample classification by the education level of patient’s parents (the
carers) ......................................................................................................... 29
4.1.3 Sample structure by job of parents ..................................................... 30
4.1.4 Sample classification by the income of patient’s parents .................... 31
4.2 The research results from questionnaire....................................................... 32
4.3 Testing the reliability of research scales for factors ..................................... 33
4.4 Explore factor analysis ................................................................................ 34
4.4.1 Explore factor analysis with independent variables ............................ 35
4.4.2 Explore factor analysis with the dependent variable ........................... 36
4.5 Correlation analysis..................................................................................... 37
4.6 Regression analysis ..................................................................................... 38
4.6.1 The results from regression analysis by Enter ..................................... 39
4.6.2 Testing the research hypotheses ......................................................... 40
4.7 The differences between groups of patients according to classification signals
42
4.7.1 Testing the differences between groups of different age ..................... 42
4.7.2 Testing the differences between different groups according to the
education level of patient’s parents .............................................................. 43
4.7.3 Testing the differences between groups of different job ...................... 44
4.7.4 Testing the differences between groups of different income ............... 45
4.8 Discussion about the research results........................................................... 46

v
CHAPTER 5 CONCLUSIONS AND RECOMMENDATIONS .................................. 49
5.1 Conclusions ................................................................................................ 49
5.2 Recommendations ....................................................................................... 51
5.3 Contributions and the importance of the study ............................................. 53
5.3.1 Contributions of the study .................................................................. 53
5.3.2 Importance of the study ...................................................................... 54
5.4 Limitations of the study............................................................................... 54
5.5 Directions for further studies ....................................................................... 55
REFERENCES ........................................................................................................... 56
QUESTIONNAIRE .................................................................................................... 60

vi
List of Tables
Table 1. Summary of some recent related studies on the satisfaction of patients with the
health care services ............................................................................................. 16
Table 2. The observed variables .................................................................................. 20
Table 3:Table Sample distribution by age and k-formula results .................................. 24
Table 4. Summary of results from questionnaire ......................................................... 32
Table 5. Results from testing the reliability of scales for factors .................................. 33
Table 6. KMO and Bartlett's Test with independent variables...................................... 35
Table 7. Total Variance Explained with independent variables .................................... 35
Table 8. Rotated Component Matrix with independent variables ................................. 35
Table 9. KMO and Bartlett's Test with the dependent variable .................................... 36
Table 10. Total Variance Explained with the dependent variable ................................. 37
Table 11. Component Matrix with the dependent variable ........................................... 37
Table 12. Pearson correlation coefficient..................................................................... 38
Table 13. Summary of estimated model by Enter ........................................................ 39
Table 14. ANOVA by Enter ........................................................................................ 39
Table 15. Coefficients of the estimated model by Enter ............................................... 39
Table 16. Summary of average value of groups by age ................................................ 42
Table 17. Results from variance analysis by age.......................................................... 42
Table 18. Summary of average values by education level ............................................ 43
Table 19. The results from variance analysis by education level .................................. 43
Table 20. Summary of average values by job .............................................................. 44
Table 21. The results from variance analysis by job .................................................... 45
Table 22. Summary of average values by income ........................................................ 45
Table 23. The results from variance analysis by income .............................................. 46
Table 24. The statistical values of factors .................................................................... 47

vii
List of Figures
Figure 1. The research procedures 6
Figure 2. The Service Quality Five Gap Model 13
Figure 3. The European Customer Satisfaction Index – ECSI 15
Figure 4. The research model 19
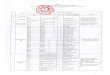
Figure 5. The rate of child patients by age 29
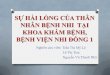
Figure 6. Sample structure by the education level of patient’s parents 30
Figure 7. Sample structure by the parent’s job 31
Figure 8. Sample structure by the income of patient’s parents 31
Figure 9. The graph of average points of satisfaction level by age 43
Figure 10. The graph of average points by education level 44
Figure 11. The graph of average values of groups by different jobs 45
Figure 12. The graph of average values by income 46
Figure 13. The relationship between factors in the model 48

1
CHAPTER 1 INTRODUCTION
This chapter will present the research background, research motivations, research
purposes and research procedure as follows:
1.1 Research Background
Service quality has been studied for a very long time, typically in the research
field of Japanese quality service (e.g.: Deming, 1964, Ishikawa, 1974. Taguchi, 1972,
Kano, 1984), in the field of product quality management (e.g.: Crosby, 1979, Stewart,
1935, quoted from Nguyen Dinh Phan, 2006), in the field of service quality by
Parasuraman et al. in America (1985, 1988, 1991), by Gronroos in Europe (1984), by
Kano in Japan (1984), etc. Nowadays, the researches on service quality and customer
satisfaction also have been done by various researchers in many different fields such as:
the field of retail selling services (Naik et al., 2010; Durvasula and Lysonski, 2010); the
field of insurance services (Bala et al., 2011; Siami & Gorji, 2012; Tahmouri, 2012);
health care service (Babakus and Mangold, 1992; Mostafa, 2005; Ahuja et al., 2011;
Chakraborty and Majumdar, 2011; Ahmad and Samreen, 2011; Barser and Joshi, 2011;
Zarei et al, 2012; Soita, 2012), etc. The studies on service quality have become an
important topic because they have relationship with the “cost” (Crosby, 1979), “benefit”
(Buzzell and Gale, 1987; Rust and Zahorik, 1993), “customer satisfaction” (Bollton and
Drew, 1991; Boulding et al., 1993), the buy-back-possibility of customers (Reichelheld
and Sasser, 1990) (quoted from Buttle, 1996). These detections play an important role
for managers and service providers in improving their products and services in order to
better meet customer’s needs.

2
In the field of health care services in Vietnam, the methods of traditional
medicine currently have applied and used by various places such as state hospitals,
private hospitals and many other doctors. Along with the success of the family planning
program, the birth rate reduced from 2.3% / year down to 1.2%/ year in the 1990s, and
the rate of poverty and malnutrition in children also reduced in the 2000s (Report of
Ministry of Health, 2006). The development of the economy requires the higher quality
of services, especially in the health sector and health care services for children. The
reason for this special carings with children is that the current income of household
increases, and the number of childs in a family is also much fewer than before. For this
reason, it is needed for providers who provide services for children to improve their
service quality in order to meet higher and higher needs of the parents. The medical and
health care services are not an exception.
Hai Duong Children's Hospital
Hai Duong Children’s Hospital is a grade II hospital under Hai Duong
Department of Health. Every year, the hospital performs the tasks as follows:
To get, examine and treat diseases belongingthe hospital's speciality for resident or
non-resident child patients in the province and neighboring provinces;
To do health examination and forensic medicine examination in the field of
paediatrics for the Provincial Medical Evaluation Board or when competent authorities
request information;

3
Is a practical unit to train medical staffs and train pediatric medicine at the school
levels as prescribed; Organize to ongoing train for the medical staffs in the hospital and
other sub-units to improve their speciality skills;
To organize the implementation of research titles and application of science and
technology in the field of pediatrics for the examination, treatment and protection of
people's health care;
To build plans and directions as well as to guide the pediatrics for sub-units and also
for private medical practitioners related to pediatrics in the province in order to develop
and improve the pediatrics in the division of the Department of Health;
To co-ordinate with health care unit do to some medical avtitives such as the
implementation of primary health care programs and the pediatrics program in the
community as assigned by the Department of Health;
To combine with other health care unit to perform regularly the works of disease
prevention and treatment as assigned by the Department of Health;
Currently the researches on customer satisfaction with services have been done in
Vietnam in many different fields (e.g.: Nguyen Thi Phuong Tram, 2008; Nguyen Trung
Kien, 2005, Pham Duc Ky, 2007, etc.), however, there have been few studies on
customer satisfaction with the quality of hospital’s services and just only focused on
adults (e.g.: Bui Thi Thu Huong, 2009; Pham Nhat Yen, 2008). Thus, the research on
children’s hospital is necessary and through it we will have real views on the state of the

4
service providers and assessments on the differences between service quality for the
group of child patients and services for other groups.
1.2 Research Motivations
Why researching on customer satisfaction with service quality? Like other types
of services, health services also require the service providers (hospitals) to meet higher-
and-higher needs and requirements of customers. It is proven that the quality of services
has impact on the cost (Crosby, 1979), benefit (Buzzell and Gale, 1987; Rust and
Zahorik, 1993), customer satisfaction (Bollton and Drew, 1991; Boulding et al., 1993),
and the possibility of buy-back of customers (Reichelheld and Sasser, 1990) (quoted
from Buttle, 1995). Therefore, researching on customer satisfaction with service quality
is needed for every business to better improve their service supplying ability and create
competitive advantage or their brand positioning (Ries and Trout, 2001). Nowadays
when life standards of employees are better improved and with the implementation of
the policy of family planning by Government, the birth rate becomes lower and then
requirements health services for young children are increasingly interested. In addition,
besides State hospitals, the private hospitals are being opened to make competition with
services of other public hospitals. Therefore, it is needed to do systematical researches
to find solutions for satisfying customer needs.
Why selecting Hai Duong Children’s hospital? Hai Duong Children’s Hospital is
a level-2 hospital in Hai Duong Department of Health. Until now, there have not been
any studies on assessment of service quality in the hospitals. Some surveys have also
been done but just only stopped at evaluating in statistic description, not in-deep-
researching on the nature of relationships between factors affecting patient’s satisfaction
on the services of the hospitals. Thus, a systematical study on this field is needed to
done in order to detect factors and answer the questions that the research posed.
Why using SERVQUAL model? The SERVQUAL is a popular model in
measuring service quality in many different research fields, including the field of health
care services (e.g.: Babakus and Mangold, 1992; Mostafa., 2005; Ahuja et al., 2011;

5
Chakraborty and Majumdar, 2011; Ahmad. and Samreen., 2011; Barser and Joshi, 2011;
Zarei. et al., 2012) and is proven as an appropriate and reliable scale. Thus, the
application of SERVQUAL to assess and measure the quality of services and customer
satisfaction with services of Hai Duong Children’s Hospital is appropriate and
reasonable.
1.3 Research Purposes
This study posed some main purposes as follows:
The first, to evaluate the status of service quality provided by Hai Duong
Children’s hospital based on main aspects of SERVQUAL model and general
assessments of customer on the quality of the services.
The second, to detect and explore meaningful and meaningless factors that
influence the satisfaction of patients with services of the hospital.
The third, assess differences among demographic factors that affect the level of
patient’s satisfaction.
1.4 Research Procedures
The research procedures are described as follows:

6
Figure 1. The research procedures
Step 1: Define the research issues. At this step, the author defined issues posed
in the parts of research motivation, research purposes and research procedures in the
thesis based on experiences and instructions of advisors and co-advisors. The results of
this step were that the author outlined main contents of the two first chapters: chapter 1
and chapter 2.
Step 2: Research and design the research model: After defining the research
issues, research motivations, purposes and procedures at the step 1, the author
considered theories of service quality and other research models on customer
satisfaction from previous researches. It was needed to select an appropriate and reliable
research model as the basic theoretical research model of the thesis. In details in this
thesis, the author selected SERVQUAL as the basic model because it reliability was
proven through many different researches (see more in chapter 2).
Step 3: Develop survey questions for the data collection. After building the
theoretical research model, the author developed survey questions. The questions
inherited from questionnaires of previous researched and were adjusted to suit specific
Research issues
Research and design the model
Develop survey questions for the data collection
Distribute questionnaire and collect answers
Collect, analyze and process data
Complete the thesis
Write chapter 1, 2
Write chapter 3 Write chapter 4
Complete chapter 1.2.3
Write chapter 5

7
research conditions of the research field of children’s health care. To adjust aspects in
the theoretical model, the author made a group discussion.
Step 4: Investigate and collect data. After final questionnaire were completed, the
author distributed them to customers and got actual data. The method used here was
distributing paper questionnaire directly to the patient’s relatives who were taking care
of them in the hospital. The questionnaire after being interviewed and answered would
be collected, tested and cleaned in order to use in the next step of data processing.
Along with the data collection, the author edited and wrote chapter 1, 2 and 3 according
to the instruction of teachers.
Step 5: Collect and analyze data. Data after being cleaned and coded would be
collected and analyzed with the various statistical analysis methods. Applied PASW
(SPSS) 18.0 with the statistical analysis steps such as: descriptive statistics, testing the
reliability of the scale, factor analysis, regression analysis and testing the research
hypotheses.
Step 6: Complete the thesis. At this last step, the author evaluated the contribution
of the thesis in the domain of learning and reality, suggestions from research results,
limitations of the thesis and directions for future researches in the same field.

8
CHAPTER 2 LITERATURE REVIEW
This chapter will present general theories of service, service quality, customer
satisfaction, the relationship between service quality and customer satisfaction with
services, related research models and some other recent researches on customer
satisfaction. The contents in details are as follows:
2.1 The concepts and characteristics of service
Service is a special kind of economic goods, intangible and different from other
tangible goods. Different researchers have different viewpoints of service, and in this
study the author will introduce some popular concepts of service as follows:
According to Zeithaml and Britner (2000), a service is an act or performance
offered by one party to another to create value for customers to use service and satisfy
needs and expectations of customers.
According to Lovelock (2001, quoted from Oliveira, 2010), service is an
economic activity that creates values and brings benefit to customers in a specific time
and place as a result of a desired change or on behalf of the service recipient (user).
According to Kotler & Armstrong (2004), service is an activity or benefits that
business can offer to customers to build, strengthen and expand the long-term
partnerships with them.
Accordting to Mairelles (2006, quoted from Oliveira, 2010), a service has
intangible characteristics and is evaluated in combination with other functions such as
the production process and tangible products.
In this study, health care service can be understood as the whole processes and
solutions that bring utilities, advantages for patients in order to meet their needs of
health care.
In conclusions, we can understand that services are activities which are created to
bring benefits to satisfy customer’s needs of a specific activity. Researchers can have
different concepts of service but in general, they al agree in the characteristics of
service. In the book “Quality management in the organization” of Nguyen Dinh Phan et
al. (2006), service has some following characteristics:

9
(1) Intangibility: The products of service are “intangible” products, that they
cannot be touched, gripped, handled, looked at, smelled, tasted or heard.
Quality of service is only shown in the interactive process between customers and
employees of the company. Because of this characteristic, customers are difficult
to know in advance the quality of service which they intend to buy. In the other
words, service quality depends much on subjective perceptiveness of customers,
and it is difficult to measure it accurately with the specific technical criteria.
(2) Heterogeneity: Service quality has no heterogeneity between the times
of service performance and depends on individual perceptiveness on service. With
the same providing process, each customer has different perceptiveness of the
service quality at different specific time. Also with the same service, each
individual has one particular feeling about it. Service is assessed from bad to
excellent level because it also depends on customer’s expectation. This
characteristic makes the standardization of services more difficult than other
tangible goods.
(3) Inseparability: The inseparability of service is reflected in the difficulty of
distinguishing the service creation process and service usage. They are
two separate processes. A service cannot be separated into two separate processes:
(1) service creation process and (2) service usage process. They are simultaneous.
The creation and usage of a service simultaneously occur. This is the big
differences with other tangible goods: Tangible goods are produced and put in
storage or distributed to customers. They are two separate processes and can be
clearly separated. In contrast, service is a process of creating, using at the same
time, customers and service providers involved throughout the service creation
process.
(4) Non-ownership: Service has production process and using process which
occur in the same period of time, so it cannot store. In other words, the consumers
do not secure ownership of the service and not set up warehouses to store goods.

10
(5) Simultaneity: The simultaneity of services expresses that services are
rendered and consumed during the same period of time. We cannot separate these
two processes.
2.2 Service quality
Service quality is different levels between the expectations of customers of
services and their awareness of service outcome (Parasuraman, 1988). Service quality
does not formed by many different factors, but is a concept which has many different
aspects. Parasuraman et al. (1985) gave out ten determinants of service quality
including: (1) reliability; (2) responsiveness; (3) assurance; (4) access, (5) courtesy, (6)
communication, (7) credibility, (8) security; (9) understanding customer; and (10)
tangibles. Based on these ten determinants, later researches have receded to five main
determinants of service quality (e.g. Parasuraman et al., 1988, 1991) including:
(1) Reliability: expresses the ability to perform the promised service dependably
and accurately.
(2) Responsiveness: expresses the willingness and/ or readiness of employees to
help customers and to provide prompt service, timeliness of service.
(3) Assurance: expresses the knowledge and courtesy of employees and their
ability to convey trust and confidence
(4) Empathy: expresses the provision of caring, individualized attention to
customers.
(5) Tangibles: expresses physical evidence of the service: appearance of physical
facilities, tools and equipments used to provide the service, appearance of
personnel and communication materials.
Some researches in the field of mobile telecommunications (Kim et al., 2004,
Pham Duc Ky, 2008) showed that the quality of services in mobile telecommunications
includes following aspects: (1) Call quality, (2) value-added services, (3) price structure,
(4) convenience, and (5) customer support.
In conclusions, we can see that service quality is a concept including many
aspects, and also a general indicator of the different factors. In different service fields,
the quality of services is measured by different factors (standards).

11
2.3 Customer satisfaction
Customer satisfaction is the emotional state of products and services that
customers used to use (Spreng et al., 1996). Bachelet (1995) defined customer
satisfaction as an emotional reaction of customers in response to their experiences of a
product or service. Customer satisfaction is the level of a person's state of feeling
derived from the comparison of the results obtained from the consumption of products /
services with his expectations (Kotler, 1996).
In general, researchers considered customer satisfaction as comfortable feelings
when customer’s expectations of services and products are met. General satisfaction
with services is also considered as a separate variable in the relationship with other
determinants of service quality (e.g.: Andaleeb and Simmonds (1998); Kassim and
Bojei (2002), Atilgan et al. (2003), Gilbert and Wong (2003), Chow and Luk (2005),
Lee and Lin (2005), Durvasula and Lysonski (2010), Bala et al. (2011), etc).
2.4 The relationship between service quality and customer satisfaction
Many researches showed that service quality and customer satisfaction have close
relationship with each other, in which service quality is the cause and customer
satisfaction if the effect (e.g.: Spereng, 1996, Andaleeb and Simmonds (1998), Atilgan
et al. (2003), Chow and Luk (2005), Bala et al. (2011), Amad and Samreen (2011),
Meybodi (2012), Tahmouri (2012), etc). The relationship between service quality and
customer satisfaction is a same-direction relationship, service quality has positive
impact on peceiveness of customers.
According to Zeithaml and Bitner (2000), “service quality” and “customer
satisfaction” are two different concepts. If service quality just specifically focuses on
the determinants of service, in contrast, customer satisfaction is a generic concept.
According to Cronin and Taylor (1992), and Spereng (1996), between service quality
and customer satisfaction there is a relationship.
2.5 Research models of service quality and customer satisfaction
In the research field of service quality and customer satisfaction, many studies
have been done in recent time. There are some popular and famous models such as The
service quality five gap model (Parasuraman et al., 1985), the model of quality

12
functional / technical quality (Gronroos, 1984), the product attributes model of Kano
(1984), SERVQUAL (Parasuraman et al, 1988), Models of customer satisfaction index
(CSI) of nations (Fornell, 2000, Martesen el al., 2000, Le Van Huy, 2007). Therefore,
this study will introduce some common research models which were applied in many
researches.
2.5.1 The service quality five gap model
The service quality five gap models have been introduced by Parasuraman
et al. since 1995 in the magazine Journal of Marketing. According to Parasuraman
et al, expectations are considered as customers hope and belief that are based on
outside information, individual needs, and their experiences.
Gap 1 is the distance between what customers expect and what service providers
think they expect.
Gap 2 occurs when service provider has difficulty in changing their perception of
customer expectations of customer expectations into the feature of service quality.
It means, in many cases, service providers may be aware of customer expectations
but they cannot always transfer these expectations to the specific criteria of
quality and transfer them right as customers expected.
Gap 3 occurs when the staffs of the company do not transfer services to customer
right according to the determined criteria. Because service providing process is an
inter-relationship between service provider and customers, this gap depends much
on the quality of the staffs that directly provide the service to customers. In many
cases, attitudes and professional skills of the staffs do not satisfy their customers
or make them feel nuisance, so services cannot be transferred to customer right
according to the determined criteria.
Gap 4 is the gap between the delivery of the customer experience and what is
communicated to customers. Advertisements make customer expectations change
in the direction of much more satisfaction on services, so if real quality of services
is not as ads, perceived quality of services will be lower..
Gap 5 is the gap between a customer's perception of the experience and the
customer's expectation of the service. After using the service, customers will draw

13
comparisons between the qualities of service that they actually receive and
perceive with the quality they expected before using it. To ensure the quality of
the service, the values that customers received during using process must be good
or much better than they expected. Thus, service quality is depreciated or
appreciated, that depends on actual feelings of customers compared with what
they expected about the service.
Experience
CO
NSU
MER
Personal Needs
Gap 5
Perceived Service
MA
KET
ER
Expected Service
Gap 2
Word of mouth communications
Communications to customers
Service Delivery
Gap 4
Change the company’s feeling into quality standard
Gap 3
Gap
1
Management perceptions of consumer expectations

14
Source: A.Parasuraman, Valarie A.Zeithaml and Leonard L. Berry (1985), a
conceptual model of service quality and its implications for future research, Journal of
Marketing, 49, 44
2.5.2 SERVQUAL model
In 1988, Parasuraman et al. introduced SERVQUAL model which was
applied in the field of retail selling. Service includes five following determinants:
Reliability: The ability to perform the promised service dependably and
accurately
Responsiveness: The willingness and readiness of the staffs to help
customers and to provide prompt service, timeliness of service.
Assurance: The knowledge and courtesy of employees and their ability to
convey trust and confidence.
Empathy: The provision of caring, individualized attention to customers.
Tangibles: Physical evidence of the service: appearance of physical
facilities, tools and equipments used to provide the service, appearance of
personnel and communication materials.
SERVQUAL scale has quickly become the most popular model to measure
service quality in many different fields such as: retail sales (Parasuraman et al,
1988, Bala et al, 2011; Duvasula and Lysonski, 2010), telecommunications
(Seth,Momaya and Gupta, 2008; Khan, 2010; Loke et al, 2011; Zekiri, 2011),
education sector (Stodnick and Rogers, 2008; Hasan et al, 2008; Hanaysha et al,
2011; Oliveira, 2009; Miller and Brooks, 2010) or health care services (Mostafa,
2005; Amad and Samreen, 2011). Thus in this study, the author will use five
factors in SERVQUAL model to assess how they affect the satisfaction of patients
in the hospital.
2.5.3 European Customer Satisfaction Index model
Perceived
values Customer satisfaction
(SI)
Perceved quality-Prod
Perceved quality–Serv
Loyalty
Image
Expectations

15
Figure 3. The European Customer Satisfaction Index – ECSI
Source: Martensen. A., Gronholdt, L. and Kristensen, K. (2000), The drivers of
customer satisfaction and loyalty. Cross-industry findings from Denmark, Total Quality
Management, 11, 8544-8553
The ECSI model explains that perceived value is directly affected by: (1)
organization image, (2) desire, (3) perceived product quality, and (4) perceived
service quality. Satisfaction is directly affected by four following determinants:
(1) image, (2) perceived value, (3) perceived product quality, and (4) perceived
service quality. In other hand, customer satisfaction directly influences customer
loyalty.
In which:
Image: Image expresses the relationship between brand and customer
associations on the attributes of the brand. The image of companies, organizations
is reflected through their reputation, prestige, and customer loyalty with the
company’s brand (trademark). It is a signal for customers to the trust of the
business as well as services of the business. The image of businesses and
organizations positively or negatively affects perceived value of customer on the
service and customer satisfaction.
Expectations: expresses customer hope and beliefs of services that they will
get when seeing and getting in touch with the service provider through their
image. Customer expectations have impact on perceived value on service quality.
If responsiveness level of the business is equal or more than what customers
expected, perceived value will be higher, and in contrast, perceived value will be
lower.
Perceived quality: There are two kinds of perceived quality including (1)
perceived product quality and (2) perceived service quality. Perceived product
quality is recent consumer-based assessments of product of customers and
perceived service quality is assessments of related services such as during and

16
after sales service, terms of supply and delivery, etc. Perceived quality is customer
evaluations compared with their expectations about services before using them. It
has direct influence on customer satisfaction. The better customer’s perceptions of
service quality are, the higher satisfaction level is and vice versa.
Perceived value: is defined as the benefit customers believe they receive
relative to the costs associated with its consumption. It is also the comparison of
financial and non-financial cost that customers must pay to use the service.
Perceived value is not necessarily equated with low prices because services with a
perceived high value may in practice carry high or low prices.
Customer satisfaction: is defined as responses of customers to being met
their expectations when using the service. Customer satisfaction is thus a function
of relative level of expectation and perceived performance.
Loyalty: expresses that customers voluntarily continue using the service of
the business when the business meets customer needs and has good
responsiveness for customers as they expected when using the service of the
company.
2.6 Some recent researches on customer satisfaction in the field of health care
In the research field of health care services, many studies have been done and
model popularly used has been SERVQUAL. Some studies added other new factors into
the research model. Below is the summary of some recent researches on the satisfaction
of patients with the quality of services.
Table 1. Summary of some recent related studies on the satisfaction of patients
with the health care services
No. Author Article Research model
1 Emin Babakus .E and Mangold.F(1992),
Adapting the SERVQUAL scale to hospital services: An empirical investigation, Heath service research, 26(6), 767 - 786
1. Reliability 2. Responsiveness 3. Assurance 4. Empathy 5. Tangibles
2 Mostafa. M.M (2005)
An empirical study of patients expectations and satisfactions in
1. Human performance quality

17
Egyptian hospitals, International journal of health care quality assurance, 18 (7), 516 - 532
2. Human Reliability 3. Facility quality
3 Ahuja.M et al. (2011),
Study of service quality management with SERVQUAL model: An empirical study of GOVT/NGO`S eye hospitals in Haryana, Indian journal of commerce and management studies, 2(2) 310 - 318
1. Reliability 2. Responsiveness 3. Assurance 4. Empathy 5. Tangibles
4 Chakraborty.R and Majumdar. A (2011),
Measuring consumer satisfaction in heath care sector: The applicability of SERVQUAL, International refereed research journal, 2(4), 149 -160
1. Reliability 2. Responsiveness 3. Assurance 4. Empathy 5. Tangibles
5 Ahmad.R and Samreen. H (2011),
Assessing the service quality of some selected hospitals in Karachi based the SERVQUAL model, Pakistan review, Juny, 266 - 314
1. Tangibles and Profesionalism 2. Reliability and Responsiveness 3. Assurance and Empathy 4. Feedback and Guidance 5. Affordability
6 Brahmbohatt, Barser and Joshi (2011),
Adapting the SERVQUAL scale to hospital service: An empirical investigation of patients` perception of service quality, International Journal of Multidisciplinary Research, 1(8), 27 -42
1. Physical Aspects. 2. Encounter (Responsiveness, Empathy) 3.Process 4.Policy
7 Zarei et al. (2012),
Service quality of private hospitals: The Iranian patients` perspective, BMC Health service Research, 1 -7
1. Reliability and Responsiveness 2. Assurance 3. Empathy 4. Tangibles
8 Soita .P.W (2012)
Measuring perceived service quality using SERVQUAL: A case Uganda Health and Fitness sector, International Journal of Business and Social Science, 3(5), 261 -277
1. Reliability 2. Responsiveness 3. Assurance 4. Empathy 5. Tangibles

18
CHAPTER 3 RESEARCH METHODOLOGY
This chapter will present the contents of research methodology such as research
model, research hypotheses, research design and other methods of data analysis. The
contents in details are as follows:
3.1 Research model
This study selected SERVQUAL as the theoretical research model combined with
the hypothesis of the relationship between service quality and customer satisfaction
(Spereng et al., 1996) which was tested in many different research fields such as: retail
selling (e.g: Naik et al., 2010; Durvasula and Lysonski, 2010); insurance sector (Bala et
al., 2011; S.Siami and Gorji, 2012; Tahmouri, 2012); telecommunications (Kassim and
Bojei, 2002; Seth, Momaya and Gupta, 2008, Ahmed et al., 2011; Zekiri, 2011; Islam,
2012); restaurant services (Chow and Luk, 2005; Andaleeb and Conway, 2006;
Markovic et al., 2010), and also the field of health care services (Mostafa, 2005; Ahuja
et al., 2011; Chakraborty and Majumdar, 2011; Ahmad and Samreen, 2011; Barser and
Joshi, 2011; Zarei et al., 2012; Soita, 2012). Therefore, the author proposed the research
model with following factors:
(1) Reliability
(2) Responsiveness
(3) Assurance
(4) Empathy
(5) Tangibles

19
Figure 4. The research model
3.2 Research Hypotheses
H1: The factor reliability of the hospital positively affects general satisfaction of
patients.
H2: The factor assurance of the hospital positively affects general satisfaction of
patients.
H3: The factor empathy positively affects general satisfaction of patients.
H4: The factor responsiveness positively affects general satisfaction of patients.
H5: The factor “tangibles” of the hospital positively affects general satisfaction of
patients.
Besides above hypotheses, the author also considered the differences between
different groups of patients through the analysis of variance (ANOVA).
3.3 Measurement of observed variables
Observed variables (survey questions) used in the study inherited from previous
researches. The questionnaire includes 26 observed items which were standardized by
Parasuraman et al. (1988) and referenced from questionnaire of the research of Mostafa
(2005) in Egypt, the research of Amad and Samreen (2011) in Pakistan in the field of
Reliability
Assurance
Tangibles
Responsiveness
Empathy Customer satisfaction
H2
H3
H4
H5
H1

20
health care services. In addition, the author also used a group discussion with the
patient’s relatives who are taking care of the patients in order to adjust the measurement
aspects of factors. The contents in details are as follows:
Table 2 the observed variables
No. Code Contents of question I Reliability
01 REL1 You trust the results of diagnosis and treatments of the hospital. 02 REL2 You see that the hospital staffs tried not to make mistakes when
implementing treatments for patients. 03 REL3 You see that the quality of health care services is as good as the notice
of the hospital. 04 REL4 You find the medical examinations of the hospital are precisely done. 05 REL5 You find if the staffs of the hospital promise to do something in a fix
time, they will do it. II Assurance 06 ASS1 You see that the doctors and nurses are never too busy to meet the
needs of the patients (for example: medical procedures, asking the place to test, etc.).
07 ASS2 You are informed by medical staffs about the done-time of the services will be carried out (for example: time to response the test results, etc.).
08 ASS3 You see that the doctors and nurses always show their courtesy and willingness to help the patients.
09 ASS4 You find that the services of the hospital are always provided fully and promptly.
III Empathy 10 EMP1 You find that the doctors devotedly care for each patient. 11 EMP2 You feel that the doctors and nurses always understand the worry and
special needs of the patients. 12 EMP3 You find that the patients are treated and cared enthusiastically and
thoughtfully. 13 EMP4 You find the time of medical examination is convenient for the
patients. IV Responsiveness 14 RES1 You think that the behaviors of the physicians create the trust to
patients. 15 RES2 You feel safe when diagnosing and treating diseases in the hospital.

21
16 RES3 You think that the hospital has good doctors and nurses. 17 RES4 You think that the medical staffs have sufficient knowledge to answer
all questions of patients. V Tangibles 18 TAN1 You find that the hospital is always clean. 29 TAN2 You see that the uniforms of the medical staffs are always neat and
courteous. 20 TAN3 You think the facilities of the hospital are attractive. 21 TAN4 You think that the facilities (tools, equipments…) of the hospital are
modern and sufficiently provided. VI General satisfaction with medical examination services 22 SAT1 You feel satisfied with the facilities of the hospital.
23 SAT2 You feel satisfied with the assurance of the hospital. 24 SAT3 You will use the medical examination services of the hospital for your
children when needed. 25 SAT4 You will introduce the hospital to others. 26 SAT5 In general, you feel satisfied with the services of the hospital.
3.4 Research Design
3.4.1 Discussion for scale adjustment
To build the survey questions, the author inherited the questionnaire from
the research of Parasuraman et al. (1988) and the questionnaire of Mostafa (2005)
in Egypt, questionnaire of Amad and Samreen (2011) in Pakistan. These questions
were translated from English into Vietnamese and distributed for the patients’
relatives to collect opinions through a group discussion (because of the features of
a children’s hospital, we cannot directly ask the patients, but the relatives of the
patients who are taking care of them) and then adjusted the questions in order to
get the final questionnaire for the research.
The discussion results showed that all opinions agreed with aspects (items)
posed in the trial questionnaire. It is just needed to adjust questions in semantics
and words to be more understanding for interviewees. Some groups of opinions
are as follows:

22
For the factor “tangibles”, the patient’s relatives pay attention to issues such
as: the application of modern equipments, the clean environment of the hospital,
the uniforms of the medical staffs must be neat; the facilities of the hospital must
be attractive. They are factors they supposed to have impact on their feelings
when making the medical examinations for your children in the hospital.
For the factor “reliability”, the patient’s relatives care the precision of the
medical examination methods, the careful style of work of the staffs, the quality of
services compared with ads information of the hospital. They are factors affecting
their feelings of the service quality.
For the factor “responsiveness”, the patient’s relatives pay attention to the
knowledge of the doctors and nurses when instructing and answering their
questions, the attitudes of doctors, and their feelings of the safety of medical
treatment methods. In their opinion, these factors need to be ensured and create
the safe feelings for the patients.
For the factor “assurance”, the patient’s relatives pay attention to the
timeliness of services, the caring of the medical staffs, the willingness to help
patients, etc. They are factors that are meaningful and important for them when
evaluating the service quality of the hospital.
For the factor “empathy”, the patient’s relatives care the enthusiasm and
thoughtfulness of the doctors, the convenient time, or the understanding of the
doctors with special needs of each patient.
In conclusions, we can see that most of opinions agree with posed items for
each factor. At once, the author adjusted questions in semantics. To get the final
questionnaire, the trial questionnaires would be adjusted once again through
collecting opinions of the patient’s relatives.
3.4.2 Scale selection
This study is a quantitative research, so scales must be hierarchical scales or
ratio scales, not identification ones. Hierarchical scales can be used here are
Stapel or Likert; however Likert scale is selected because it has advantage of

23
using a sequence of positive numbers. In details in this study, the five point Likert
scale is selected as the scales for survey items in the questionnaire.
3.4.3 Research sample selection
Sampling method
In this study, the author used the stratified sampling. After defining an
appropriate sample size, the samples would be distributed to each group of
patients depending on their age. The reason for stratifying samples on the age
group is that for the child patients there are similarities of the level of illness and
the diseases suffered by certain age groups. In details in this study, the patients
were divided into five small groups including the group at the age under 1, from 1
to 2, from 2 to 3, from 3 to 5 and the group at the age above 5. The structure of
samples was divided by the corresponding percentage of patients for each age
group.
The sample size of the study is determined by the principle of minimum
sample size to get the necessary reliability of the study. There are many different
opinions of a minimum sample size. Maccallum et al. (1999) summed up opinions
of previous researchers about the principle of minimum sample size with Factor
Analysis. According to Kline (1979) the minimum number of samples is 100,
Guiford (1954) supposed 200, Comrey and Lee (1992) gave the sample size for
the respective views with same opinions: 100 = bad, 200 = pretty, 300 = good,
500 = very good, 1000 or more = excellent. In this research, sampling was based
on the rule of Comrey and Lee (1992), the sample size was defined = 200 is a
good sample size.
Research objectives: Because the patients of the children’s hospital are child
patients, so the author did not make survey with them but with their relatives
(persons who directly take care of them in the hospital). These research objectives
are reasonable because for child patients, their parents are those who decide which
hospital to test. Moreover, child patients cannot understand much and answer all
questions.

24
Method of data collection: First of all, the author listed a name list of
patients who are diagnosing and treating diseases in the hospital, then divided
them into small groups of different age to get the overall number of each group.
Next, based on the number of samples for each group, the author listed patients to
investigate. In this step, the author divides child patients into following groups:
Group 1 included patients less than 1 year old, group 2 includes patient from 1 to
2 years old, group 3 includes patients from 2 to 3 years old, group 4 includes
patients from 3 to 5 years old, and group 5 includes patients more than 5 years
old. The reason for dividing those groups is that biological characteristics of the
patient's diseases base on recommendations from the Department of Health. And
the list of patients depends on the distribution of sample size for each age group.
The ratio of distribution of the questionnaire was divided by the proportion of
patients hospitalized at the time of the survey. At that time, there are 487 patients
diagnosing at the hospital, the author distributes 220 questionnaires to these five
groups base on the age of patients as above table. The selection of patients for
each group was based the k-jump formula as follows: k = m/n, in which m the
number of patient determined in an age group, n – the total of patients in this
group, k will be rounded to the smaller number (for example: k = 2.7 will be
rounded to 2). After that, from the list of each patient group, the author selected in
turn k, 2k, 3k,…, mk. This method will ensure the randomness of collected
samples. The results of distribution of samples by age group and k-formula to
select survey patients are as follows:
Table 3: Table Sample distribution by age and k-formula results
Patient group Quantity(n)
Estimated ratio of
distribution
Actual number of patients(m)
Estimated k Actual k
< 1 year 122 55.1129 55 2.21818 2 1 - 2 years 119 53.7577 55 2.16364 2 2 - 3 years 81 36.5914 35 2.31429 2 3 - 5 years 79 35.6879 35 2.25714 2 > 5 years o 86 38.8501 40 2.15 2

25
Total 487 220
After sample classified, questionnaires will be distributed to different groups to
make interviews with main interviewees. The obtained results will be summed up and
cleaned (wrong questionnaires removed) and then analyzed. The author classifies
sample by different age groups because of different features about the biology and
pathology of child patients. According to the Ministry of Health's recommendations on
child health care, children who usually have the same pathological will be divided into
following five groups: less than 1 year old, from 1 to 2 years old, from 2 to 3 years old,
from 3 to 5 years old, and above 5 years old.
3.5 Method of data analysis
The actual data were cleaned and analyzed SPSS 20.0 for Window through
statistical steps as follows:
3.5.1 Descriptive Statistics
The collected samples would be analyzed by descriptive statistics:
classifying the samples according to the classification criteria, calculating the
average point, maximum value, and standard deviation of the answers in collected
questionnaire.
3.5.2 Testing the reliability of scales
To test the reliability of scales used in the research, the author used
Cronbach`s Alpha coefficient and the total correlation coefficient. The observed
variables which did not ensure the reliability would be removed from the scale
and do not appear in the explore factor analysis (EFA). The standards were:
Cronbach`s Alpha must be at least 0.6 (Hair et al., 2006), the total correlation
coefficient less than 0.3 would be a “spam” variable and removed from the scale
(Nunally and Burstein, 1994).
3.5.3 Explore factor analysis
After factors were tested by Cronbach`s Alpha, they would be analyzed by
EFA method. Factor analysis would help the author detect implicit factors from a

26
set of smaller observed variables. Some standards applied in analyzing the EFA in
the study are as follows:
- Testing the suitability of factor analysis with data set through the value of
Kaiser-Meyer-Olkin (KMO). IF KMO is greater than 0,5, factor analysis with this
factor is appropriate (Garson, 2002), in contrast, if KMO is less than 0,5, the
application of factor analysis with that factor is not appropriate with the data set.
- The number of factor: The number of factors is determined based on the
eigenvalue index which represents the variation explained by each factor.
According to Kaiser’s standards, the factors with an eigenvalue index less than 1
will be removed from the research model (Garson, 2002).
- Variance explained criteria: The total variance explained criteria must be
greater than 50 % (Hair et al., 1998).
- The convergence value: To meet the convergence value of the scale, the
single correlation coefficient between variables and the factor loading must be
greater than or equal to 0.5 within a factor (Garbing and Anderson, 1988).
- Principal components method with Varimax rotation to ensure the number
of factors is smallest (Hoang Trong and chu Nguyen Ngoc, 2008).
3.5.4 Building the regression function
After the scales of factors were tested, the author would build the linear
regression function by the method of Ordinary least squares (OLS) with the
support of Enter method. According to Nguyen Dinh Tho (2011), Enter is more
appropriate for the testing researches.
3.5.5 Testing the research hypotheses
The research hypotheses would be tested through the research data from
regression function. The testing standards used the t statistics and the p-value
(sig.). With the reliability coefficient = 95%, the p-value would be directly
compared with 0.05 to conclude the acceptance or rejection of research
hypotheses. For testing the difference between subtotals, the study used t-test and
ANOVA to test each hypothesis, and the testing standards based on the value of
the corresponding p-value for each specific testing step. To test the suitability of

27
data and model, the author used F statistics, t statistics, and the adjusted R-square.
In addition, to assess the importance of factors, the author checked the Beta
coefficient in the regression function, which was built by research data.

28
CHAPTER 4 RESEARCH RESULTS
This chapter will present main results from data set which was collected by
statistical methods such as: descriptive statistics, scale verification, explore factor
analysis, correlation analysis, regression analysis, and testing research hypotheses. The
software analysis tool used here is SPSS 20.0. The contents in details are as follows:
4.1 Descriptive statistics
The expected sample size of the study is 200. To get this size, the author
distributed 220 samples, and got back 211 answered questionnaires. From these 211
ones, the author started cleaning them and then collected 204 valid ones which would be
analyzed in the next step. The results according to different sample groups are as
follows:
Patient group
Questionnaire number
Collected questionnaire
Questionnaire removed
Valid questionnaire
< 1 year old 55 52 2 50 1 - 2 years old 55 54 0 54 2 - 3 years old 35 34 1 33 3 - 5 years old 35 32 2 30 > 5 years old 40 39 2 37 Total 220 211 7 204
4.1.1 Sample classification by age of patients
In 204 valid answered questionnaires, the results showed that there were
two groups which had the biggest number of patients including the group of
patients at the age under 1 (50 patients) and the group at the age from 1 to 2 (54
patients) (corresponding with 25% and 26%), the left three groups including the
group at the age from 2 to 3, from 3 to 5, and above 5 had lower proportion and
were approximately equal to each other (corresponding with 33, 30 and 37
patients) (16%, 15% and 18%) (Figure 5). This result also reflected the tendency

29
of health of the child patients, the groups of newborn babies and children under 2
years old were the groups which were endangered of getting a disease more easily
than other groups. .
Figure 5. The rate of child patients by age
4.1.2 Sample classification by the education level of patient’s parents (the
career)
In 204 patient’s relatives (mostly the patient’s parents) there are over 50%
persons who are at college-level (105 persons, 52%), next is the group at
university-level with 39 persons (19%), the group at high school-level includes 33
persons (16%), the group at intermediate-level has 18 persons (9%), and the last
group has 9 persons (4%). This proves that the education level of the patient’s
parents currently is at quite high level.

30
Figure 6. Sample structure by the education level of patient’s parents
4.1.3 Sample structure by job of parents
In these 204 valid questionnaires, there are 105 ones belonging to the group
of persons who work in the office (52%), next is the group of workers with 57
persons (28%), the group of farmers includes 27 persons (13 %), and the last
group has 15 persons (7%). This proves that majority of persons who diagnose
and treat diseases in the hospital are mostly from urban areas and have parents
working in the office or working as workers. The number of children whose
parents are farmers has a low proportion. The reason comes from the restrictions
on economic conditions so that the children in rural areas are often treated their
diseases at home or in local medical stations.

31
Figure 7 Sample structure by the parent’s job
4.1.4 Sample classification by the income of patient’s parents
In 204 valid questionnaires, there are 135 persons who have income from 5
to 10 mil./month (66%), 55 persons have income less than 5 mil./month (27%), 12
persons have income from 10 to 15mil./month (6%), and only 2 persons have
income more than 15 mil./month (1%). This also reflects the fact that the parents
of child patients are still quite young, they are the new working group and have
not so high income in the society.
Figure 8. Sample structure by the income of patient’s parents

32
4.2 The research results from questionnaire
The results from questionnaire showed that the answers were from level 2
(minimum) to level 5 in the five point Likert scale, the standard deviation was quite
small (less than 1), and the average point was more than 3. This proved that the
perception level of patient’s relatives with the norms in the questionnaire was quite
alike (the standard deviation is small) and also at good level.
Table 4. Summary of results from questionnaire
Item N Minimum Maximum Mean Std. Deviation REL1 204 2.00 5.00 4.2402 .57549 REL2 204 2.00 5.00 4.1127 .64482 REL3 204 2.00 5.00 3.8922 .70055 REL4 204 2.00 5.00 3.5098 .77199 REL5 204 2.00 5.00 3.7500 .78862 ASS1 204 2.00 5.00 3.9902 .56140 ASS2 204 2.00 5.00 3.9314 .57467 ASS3 204 2.00 5.00 3.9216 .56475 ASS4 204 3.00 5.00 3.8382 .58580 EMP1 204 2.00 5.00 3.9069 .64031 EMP2 204 2.00 5.00 3.5441 .70398 EMP3 204 2.00 5.00 3.5539 .73077 EMP4 204 2.00 5.00 3.5735 .69444 RES1 204 2.00 5.00 3.3284 .76563 RES2 204 2.00 5.00 3.4706 .77784 RES3 204 2.00 5.00 3.3775 .78764 RES4 204 2.00 5.00 3.2353 .78378 TAN1 204 2.00 5.00 3.8725 .59838 TAN2 204 2.00 5.00 3.5588 .68154 TAN3 204 2.00 5.00 3.8873 .57195 TAN4 204 2.00 5.00 3.7598 .71998 SAT1 204 2.00 5.00 3.7990 .58200 SAT2 204 2.00 5.00 3.7598 .63257 SAT3 204 2.00 5.00 3.7598 .61680 SAT4 204 2.00 5.00 3.5245 .73235 SAT5 204 2.00 5.00 3.7598 .65552

33
4.3 Testing the reliability of research scales for factors
Each factor in the research model is formed by many other observed items
(questions). To test the reliability of scales for each factor, we use Cronbach`s Alpha
coefficient. To test if the item in the factor really belongs to this factor or not, we test
the correlation of this item with other items. This will be tested by the total correlation
coefficient. The standards here include: Cronbach`s Alpha coefficient must be at least
0.6 (Hair et al., 2006), the total correlation coefficient must be at least 0.3 (Nunnally,
1994), factors have Cronbach`s Alpha less than 0.6 will be considered as inappropriate
factors or in other words, they will not be formed in the research environment. Observed
items (questions) if have the total correlation coefficient less than 0.3 will be considered
as “spam” variables and then be removed from the factor. The results from testing the
reliability of scales for factors are as follows:
Table 5. Results from testing the reliability of scales for factors
Observed item
Scale Mean if Item Deleted
Scale Variance if Item Deleted
Corrected Item-Total Correlation
Cronbach's Alpha if Item Deleted
I. The factor “Reliability”: α = 0.702, N = 5 REL1 15.2647 4.235 .437 .664 REL2 15.3922 3.786 .557 .615 REL3 15.6127 3.569 .582 .599 REL4 15.9951 3.887 .367 .695 REL5 15.7549 3.782 .390 .687 II. The factor “Assurance” α = 0.660, N = 3 (removed item ASS1) ASS1 11.6912 1.771 .128 .660 ASS2 11.7500 1.312 .483 .382 ASS3 11.7598 1.356 .458 .406 ASS4 11.8431 1.424 .365 .484 III. The factor “empathy”: α = 0.770, N = 4 EMP1 10.6716 3.394 .316 .832 EMP2 11.0343 2.772 .547 .728 EMP3 11.0245 2.339 .750 .610 EMP4 11.0049 2.517 .704 .642 IV. The factor “Responsiveness”: α = 0.824, N = 4 RES1 10.0833 3.929 .605 .798

34
RES2 9.9412 3.878 .610 .796 RES3 10.0343 3.649 .692 .758 RES4 10.1765 3.673 .687 .760 V. The factor “Tangibles”: α = 0.759, N = 4 TAN1 11.2059 2.411 .596 .685 TAN2 11.5196 2.320 .526 .722 TAN3 11.1912 2.402 .647 .663 TAN4 11.3186 2.287 .491 .746 VI. The dependent variable “general satisfaction”: α = 0.886, N =5 SAT1 14.8039 5.252 .587 .890 SAT2 14.8431 4.557 .815 .840 SAT3 14.8431 4.813 .726 .861 SAT4 15.0784 4.467 .696 .871 SAT5 14.8431 4.468 .815 .839
The results from testing the reliability of scales from data set showed that the
scales for factors are appropriate with Cronbach`s Alpha coefficient greater than 0.6 and
the total correlation coefficient greater than 0.3 (excluding the item ASS1). So, the
factors in the research model are reliable and appropriate (see table 5).
4.4 Explore factor analysis
Explore factor analysis will help the author collect a set of fewer implicit variables
(factors) from the data set of observed variables. Appropriate standards for explore
factor analysis are: KMO coefficient must be at least 0.5, Bartlett-test has p-value less
than .05, factor loading coefficient must be at least 0.5, the variance extracted must
equal to at least 50%. Because the method of factor analysis does not consider the
distinguishing relationship between the dependent variable with independent variables
(Hoang Trong and Chu Nguyen Mong Ngoc, 2008) but the reciprocal relationship
between all factors, so we will do factor analysis particularly with the dependent
variable and the independent variables. Factor extraction method is Principal
Component with Varimax. The results from factor analysis in details are as follows:

35
4.4.1 Explore factor analysis with independent variables
From the data set, data will be analyzed with the support of SPSS software,
after removing factors which have factor loading coefficient less than 0.5, and
then we get final results as follows:
Table 6. KMO and Bartlett's Test with independent variables
Kaiser-Meyer-Olkin Measure of Sampling Adequacy. .775
Bartlett's Test of Sphericity Approx. Chi-Square 1374.793 Df 153 Sig. .000
Table 7. Total Variance Explained with independent variables
Component Initial Eigenvalues Rotation Sums of Squared Loadings
Total % of Variance Cumulative % Total % of Variance Cumulative % 1 4.944 27.469 27.469 2.732 15.180 15.180 2 2.229 12.384 39.853 2.490 13.835 29.015 3 1.960 10.888 50.740 2.252 12.509 41.523 4 1.444 8.020 58.760 2.150 11.947 53.470 5 1.030 5.724 64.484 1.983 11.014 64.484 6 .925 5.139 69.624 7 .762 4.234 73.858 8 .628 3.489 77.348 9 .607 3.370 80.718 10 .558 3.102 83.819 11 .517 2.871 86.691 12 .501 2.786 89.477 13 .471 2.615 92.092 14 .366 2.035 94.127 15 .340 1.887 96.014 16 .320 1.775 97.789 17 .229 1.273 99.062 18 .169 .938 100.000
Table 8. Rotated Component Matrix with independent variables
Component 1 2 3 4 5

36
RES3 .857 RES4 .826 RES2 .693 RES1 .657 TAN3 .804 TAN1 .794 TAN2 .727 TAN4 .689 EMP4 .794 EMP3 .784 EMP2 .753 ASS3 .787 ASS2 .772 ASS4 .632 EMP1 .586 REL2 .824 REL1 .780 REL3 .722 Extraction Method: Principal Component Analysis. Rotation Method: Varimax with Kaiser Normalization. a. Rotation converged in 6 iterations.
The analysis results show that KMO = 0.775 > 0.5, Batlett-test has p-value
= 0.000 < 0.05 (table 5), the variance extracted is 64.484% > 50% (table 7), factor
loading coefficients are greater than 0.5, and observed variables form five factors
(table 8). Therefore, the standards when doing factor analysis are appropriate with
the data set.
4.4.2 Explore factor analysis with the dependent variable
The results from EFA show that KMO = 0.761 > 0.5, Bartlett-test has p-
value = 0.000 < 0.05 (table 9), the variance extracted is 69.181% > 50% (table
10), and observed items form only one factor (table 11). Thus, using EFA with the
dependent variable is appropriate and the scale for factor “general satisfaction” is
a unidirectional scale.
Table 9. KMO and Bartlett's Test with the dependent variable
Kaiser-Meyer-Olkin Measure of Sampling Adequacy. .761

37
Bartlett's Test of Sphericity Approx. Chi-Square 872.871 Df 10 Sig. .000
Table 10. Total Variance Explained with the dependent variable
Component Initial Eigenvalues Extraction Sums of Squared Loadings
Total % of Variance Cumulative % Total % of Variance Cumulative % 1 3.459 69.181 69.181 3.459 69.181 69.181 2 .643 12.870 82.050 3 .569 11.389 93.440 4 .293 5.869 99.308 5 .035 .692 100.000 Extraction Method: Principal Component Analysis.
Table 11. Component Matrix with the dependent variable
Component 1
SAT5 .902 SAT2 .900 SAT3 .822 SAT4 .805 SAT1 .714 Extraction Method: Principal Component Analysis. a. 1 component extracted. So, after doing factor analysis with the set of observed items, there are no
factors being changed. The research model and hypotheses still be kept like in the
original model.
4.5 Correlation analysis
To test the relationship between the dependent variable “general satisfaction” and
factors in the research model, we use single correlation coefficient (Pearson correlation
coefficient). If the correlation coefficient is differ from 0 and p-value of two-sided test
less than 0.05, factors in the model have relationship with each other. A positive
correlation coefficient reflects a positive relationship, and in contrast, a negative
correlation coefficient reflects a negative relationship, and the bigger the correlation

38
coefficient between factors is, the closer the relationship between them is. The results
from data set are as follows:
Table 12. Pearson correlation coefficient
RES TAN EMP ASS REL SAT Pearson Correlation 1 .180** .540** .318** .138* .619** Sig. (2-tailed) .010 .000 .000 .050 .000 N 204 204 204 204 204 204 Pearson Correlation .180** 1 .204** .203** .137 .334** Sig. (2-tailed) .010 .003 .004 .051 .000 N 204 204 204 204 204 204 Pearson Correlation .540** .204** 1 .368** .336** .492** Sig. (2-tailed) .000 .003 .000 .000 .000 N 204 204 204 204 204 204 Pearson Correlation .318** .203** .368** 1 .313** .405** Sig. (2-tailed) .000 .004 .000 .000 .000 N 204 204 204 204 204 204 Pearson Correlation .138* .137 .336** .313** 1 .263** Sig. (2-tailed) .050 .051 .000 .000 .000 N 204 204 204 204 204 204 Pearson Correlation .619** .334** .492** .405** .263** 1 Sig. (2-tailed) .000 .000 .000 .000 .000 N 204 204 204 204 204 204 **. Correlation is significant at the 0.01 level (2-tailed). *. Correlation is significant at the 0.05 level (2-tailed).
Note: RES is responsiveness; TAN is tangibles, EMP is empathy; ASS is
assurance; REL is reliability, and SAT is general satisfaction.
The research results show that factors in the model have relationship with the
dependent variable “general satisfaction”, in which the factor has biggest correlation is
RES (0.619, p < 0.05) and the factor has smallest correlation is REL (0.263, p < 0.05).
Between factors there is also relationship with each other, the two-sided test also shows
p-value < 0.05 (table 12). This suggests that it is needed to test the multicollinearity in
the multi regression function.
4.6 Regression analysis

39
Regression analysis will show the relationships between factors however, we
cannot know exactly which relationship they have to test the research hypotheses. Thus,
we need to use the regression analysis to test this. The analysis method used here is the
ordinary least squares (OLS), and the method of adding variables into regression is
Enter (adding all variables at a time). Because this is a testing research, so Enter method
will be more appropriate than Stepwise (Nguyen Dinh Tho, 2011).
4.6.1 The results from regression analysis by Enter
The estimated results from data set are as follows:
Table 13. Summary of estimated model by Enter
Model R R Square Adjusted R Square
Std. Error of the Estimate
Durbin-Watson
1 .700a .490 .477 .38685 1.964 a. Predictors: (Constant), REL, TAN, RES, ASS, EMP b. Dependent Variable: SAT
Table 14. ANOVA by Enter
Model Sum of Squares
Df Mean Square
F Sig.
1 Regression 28.482 5 5.696 38.063 .000b Residual 29.632 198 .150 Total 58.114 203
a. Dependent Variable: SAT b. Predictors: (Constant), REL, TAN, RES, ASS, EMP
Table 15. Coefficients of the estimated model by Enter
Model Unstandardized Coefficients
Standardized Coefficients
T Sig. Collinearity Statistics
B Std. Error Beta Tolerance VIF
1
(Constant) .181 .328 .552 .582 RES .391 .052 .461 7.506 .000 .683 1.463 TAN .200 .057 .184 3.505 .001 .933 1.072 EMP .106 .056 .122 1.886 .041 .616 1.622 ASS .186 .071 .149 2.617 .010 .790 1.266 REL .090 .058 .087 1.559 .121 .836 1.196

40
a. Dependent Variable: SAT
The regression function is determined as follows:
SAT = 0.181 + 0.391RES + 0.200TAN + 0.106EMP + 0.186 ASS + 0.090REL
F statistics of variance analysis has p-value = 0.000 (table), it means that the
estimated results are appropriate. Adjusted R –square = 0.477 shows that the
model explains 47.7% of the variability of the dependent variable “general
satisfaction”. .
4.6.2 Testing the research hypotheses
Testing the hypothesis H1
Hypothesis H1: The factor “reliability” of the hospital positively affects
general satisfaction of patients. It means Beta coefficient of the variable REL must
be positive. From the results of regression analysis, Beta coefficient = 0.090 > 0,
however p- value = 0.121 > 0.05 (table 15), so with the reliability coefficient =
95% we have not enough basics to conclude that Beta coefficient of REL positive.
In other words, we reject the hypothesis H1. The result shows that in this research
condition with hospital services for child patients, the factor “reliability” is not a
factor that has clear impact on patient’s satisfaction. This is explained that for
child patients in Vietnam, patient’s family often has tendency to choose the most
reliable hospital. Therefore, the feature” reliability is considered as a “must-be”
feature of the hospital, if there is lack of this feature, the relatives of patients will
feel dissatisfied or will not use the services of hospital (Kano, 1984)
Tesitng the hypothesis H2
Hypothesis H2: The factor “assurance” of the hospital positively affects
general satisfaction of patients. It means Beta coefficient of the variable ASS must
be positive. From the results of regression analysis, Beta coefficient = 0.186 > 0,
and p-value = 0.010 < 0.05 (table 15), so with the reliability coefficient = 95% we
have enough basics to conclude that Beta coefficient of ASS positive. In other
words, we accept the hypothesis H2. This result shows that if the hospital
improves the factor “assurance” and makes patient’s satisfaction level increase 1

41
unit (in 5-point Likert scale), the satisfaction level of patients will increase by
0.186.
Testing the hypothesis H3
Hypothesis H3: The factor “empathy” positively affects general satisfaction
of patients. It means Beta coefficient of the variable EMP must be positive. From
the results of regression analysis, Beta coefficient of the variable EMP = 0.106 >
0, and p –value = 0.041 < 0.05 (table 15), so with the reliability coefficient = 95%
we have enough basics to conclude that Beta coefficient of EMP positive. In other
words, we accept the hypothesis H3. This result shows that factor “empathy”
positively affects to satisfaction patients. If the hospital improves the factor
“empatthy” and makes patient’s satisfaction perceived level increase 1 unit (in 5-
point Likert scale), the satisfaction level of patients will increase by 0.106 unit
Testing the hypothesis H4
Hypothesis H4: The factor “responsiveness” positively affects general
satisfaction of patients. It means Beta coefficient of the variable RES must be
positive. From the results of regression analysis, Beta coefficient of the variable
RES = 0.391> 0, and p –value = 0.000 < 0.05 (table 15), so with the reliability
coefficient = 95% we have enough basics to conclude that Beta coefficient of RES
positive. In other words, we accept the hypothesis H4. This result shows that if the
hospital improves the factor “responsiveness” and makes patient’s satisfaction
level increase 1 unit , the satisfaction level of patients will increase by 0.391 unit.
Testing the hypothesis H5
Hypothesis H5: The factor “tangibles” of the hospital positively affects
general satisfaction of patients. It means Beta coefficient of the variable TAN
must be positive. From the results of regression analysis, Beta coefficient of the
variable TAN = 0.200 > 0, and p –value = 0.001< 0.05 (table 15), so with the
reliability coefficient = 95% we have enough basics to conclude that Beta
coefficient of TAN positive. In other words, we accept the hypothesis H5. This
results shows that factor “tangibles” positively influences to satisfaction patients.

42
If the hospital improves the factor “tangibles” and makes patient’s satisfaction
level increase 1 unit , the satisfaction level of patients will increase by 0.200 unit.
4.7 The differences between groups of patients according to classification signals
To test the differences between groups of patients according to classification
signals, we use the method of Analysis Of Variance (ANOVA) and get following
results:
4.7.1 Testing the differences between groups of different age
The results from ANOVA between groups of patient of different age show
that
Table 16. Summary of average value of groups by age
N Mean Std. Deviation Std. Error 95% Confidence Interval for
Mean Lower Bound Upper Bound
< 1 year 50 3.7120 .50976 .07209 3.5671 3.8569 1 to 2 years 54 3.6296 .47010 .06397 3.5013 3.7579 2 to 3 years 33 3.6848 .63054 .10976 3.4613 3.9084 3 to 5 years 30 3.7333 .49919 .09114 3.5469 3.9197 > 5 years 37 3.8865 .58222 .09572 3.6924 4.0806 Total 204 3.7206 .53505 .03746 3.6467 3.7945
Table 17. Results from variance analysis by age
Sum of Squares Df Mean Square F Sig. Between Groups 1.516 4 .379 1.332 .259 Within Groups 56.598 199 .284
Total 58.114 203

43
AGE GROUP
Figure 10. The graph of average points of satisfaction level by age
The analysis results show p-value of F test between groups = 0.259 > 0.05
(table 16), thus there are no differences between groups of different age. The
deviation of average value between these two groups is insignificant (see table 15
and figure 10).
4.7.2 Testing the differences between different groups according to the
education level of patient’s parents
The results from ANOVA based on the education level of patient’s parents
are as follows:
Table 18. Summary of average values by education level
N Mean Std.
Deviation Std. Error
95% Confidence Interval for Mean
Lower Bound Upper Bound High school 9 3.5333 .96437 .32146 2.7921 4.2746 Intermediate 18 3.4778 .43999 .10371 3.2590 3.6966 College 105 3.7352 .49185 .04800 3.6401 3.8304 University 39 3.7641 .60675 .09716 3.5674 3.9608 Other 33 3.8061 .45134 .07857 3.6460 3.9661 Total 204 3.7206 .53505 .03746 3.6467 3.7945
Table 19. The results from variance analysis by education level

44
Sum of Squares Df Mean Square F Sig. Between Groups 1.714 4 .429 1.512 .200 Within Groups 56.399 199 .283 Total 58.114 203
High school Vocational School colledge university other
Education Figure 11. The graph of average points by education level
The analysis results show that F test between groups has p – value = 0.200 >
0.05 (table 18), So, we can suppose that there are no differences between sample
groups of different education level. This is also reflected in a very small deviation
of the average value of each group (see table 17 and figure 11).
4.7.3 Testing the differences between groups of different job
The results from ANOVA based on job of the patient’s parents are:
Table 19. Summary of average values by job
N Mean Std.
Deviation Std. Error
95% Confidence Interval for Mean
Lower Bound Upper Bound Farmer 27 3.7852 .66778 .12851 3.5210 4.0493 Worker 57 3.6386 .52296 .06927 3.4998 3.7774 Officer 105 3.7467 .52350 .05109 3.6454 3.8480 Other 15 3.7333 .39036 .10079 3.5172 3.9495 Total 204 3.7206 .53505 .03746 3.6467 3.7945

45
Table 20. The results from variance analysis by job
Sum of Squares df Mean Square F Sig. Between Groups .570 3 .190 .660 .578 Within Groups 57.544 200 .288 Total 58.114 203
Famer worker officer other
Job Figure 12. The graph of average values of groups by different jobs
From the analysis results, F test between groups has p – value = 0.578 >
0.05 (table 20), so we can suppose that there are no differences between groups of
different job. This is also reflected in a very small deviation of the average value
of each group (see table 19 and figure 12).
4.7.4 Testing the differences between groups of different income
The research results from ANOVA with different groups based on the
income of patient’s parents are as follows:
Table 21. Summary of average values by income
N Mean Std. Deviation
Std. Error 95% Confidence Interval for Mean
Lower Bound Upper Bound < 5 mil 55 3.6800 .56778 .07656 3.5265 3.8335 5 - 10 mil 135 3.7481 .53530 .04607 3.6570 3.8393 10 - 15 mil 12 3.5500 .38258 .11044 3.3069 3.7931 > 15 mil 2 4.0000 .00000 .00000 4.0000 4.0000 Total 204 3.7206 .53505 .03746 3.6467 3.7945

46
Table 22. The results from variance analysis by income
Sum of Squares df Mean Square F Sig. Between Groups .698 3 .233 .811 .489 Within Groups 57.415 200 .287 Total 58.114 203
<5m 5-10m 10-15m >15m
Income
Figure 13. The graph of average values by income
From the analysis results, F test between groups has p –value = 0.489 > 0.05
(table 22), so we can conclude that there are no differences on the satisfaction
level between groups of different income. This is also reflected in a very small
deviation of the average value of each group (see table 21 and figure 13)
4.8 Discussion about the research results
The research results show that there are four factors affecting general satisfaction
of patients including: (1) responsiveness, (2) tangibles, (3) empathy, and (4) assurance.
The investigation results at Hai Duong Children’s Hospital also show different
assessment level for each factor, in which the best point belongs to the factor
“assurance” (the average point = 3.8995), the worst point belongs to the factor
“responsiveness” (3.3529). The equal level of answers between variables is also
different from each other: the factor “assurance” has lowest fluctuation level, (σ =
0.42874) and the factor “responsiveness” has highest fluctuation level (σ = 0.63007)
(table 23).

47
Table 23. The statistical values of factors
N Minimum Maximum Mean Std. Deviation Responsiveness 204 2.00 5.00 3.3529 .63007 Tangibles 204 2.00 5.00 3.7696 .49216 Empathy 204 2.00 5.00 3.5572 .61410 Assurance 204 2.50 5.00 3.8995 .42874 General satisfaction 204 2.00 5.00 3.7206 .53505
With these results, we can see that the assessment level on factors affecting the
quality of services is above mean level, and it can increase through policies of
improving service quality.
The research results also show that the importance of each factor on general
satisfaction of the patients is different. This is reflected in Beta coefficients of each
variable in the regression function. From the regression function: SAT = 0.181 +
0.391RES + 0.200TAN + 0.106EMP + 0.186 ASS, we can easily see that the factor
“responsiveness” has biggest impact (Beta = 0,391), next is the factor “tangibles” (Beta
= 0,200), the factor “assurance” (Beta = 0.186), and the last is the factor “empathy”
(Beta = 0,106) (in this function, the variable REL was removed because it had no
statistical meaning).
According to the assessment results, the variable REL “reliability” has no
influence on the satisfaction of patients with the services of the hospital. This can be
explained because the services of the hospital require the very high reliability, and it
affects the health even the life of patients. Thus, the feature “reliability” of the service is
consider as an obligatory feature for the patients (patient’s relatives), and plays an
important role in the patient’s decision in choosing hospital to examine and treat. It can
be considered as a must-be feature in Kano model (1984), it means without this feature,
customers will feel dissatisfied but with it, customers do not also feel more satisfied.
The research results also show that there are no clear differences on general
satisfaction of the patient’s relatives according to the classification signals (age, job,
education level, income). This proves that the requirements of the quality of services for
child patients do not depend on these variables (factors). This is because Vietnamese

48
families always have the tradition of emphasis on children, regardless of that family
comes from what walk of life in the society. Children are always considered as the most
valuable "asset" of the family.
The research results also show Adjusted R –square =0.477, it means we can add
other factors into the research model in order to improve the explanation ability on the
variability of the dependent variable “general satisfaction”. Some other factors such as
the hospital fees, support activities after examination, etc. can be added into the model
to measure their impact intensity on the satisfaction of patients with services.
Statistically significant Statistically insignificant
*: The significance level 5% (0.05)
Figure 14. The relationship between factors in the model
Reliability
Assurance
Tangibles
Responsiveness
Empathy Customer satisfaction
0.186*
0.106*
0.391*
0.200*

49
CHAPTER 5 CONCLUSIONS AND RECOMMENDATIONS
This chapter will present main conclusions from the research results,
recommendations, contributions and the importance of the study as well as limitations
and directions for further researches in the same field. The contents in details are as
follows:
5.1 Conclusions
The study has reached the targets posed in the part of research purposes
including: (1) detect and explore factors affecting the satisfaction of patients with the
services of the hospital, (2) measure the real satisfaction level on the service quality of
the hospital based on main factors and general satisfaction, (3) the impact intensity of
factors of service quality on general satisfaction of customers.
The research results show that in five original factors in SERVQUAL there are
only four factors affecting general satisfaction of patients including: (1) assurance, (2)
empathy, (3) responsiveness, and (4) tangibles. The factor “reliability” has no impact on
general satisfaction. The patients consider this factor as a must-be feature for services of
the hospital. These results also have similarity with the results from the research of
Mostafa (2005) in Egypt. The research of Mostafa showed three in five main factors of
SERVQUAL affecting the satisfaction of customers. They are (1) human performance
quality, (2) human reliability, and facility quality. The differences between results from
Mostafa’s study and the results from this study are that the factor “reliability” in the
research of Mostafa is considered as a very important factor that influences the
satisfaction of patients on the disease diagnosis and treatment services. In this study,
this factor in contrast has no impact on the satisfaction of the patients. The reasons may
come from the differences on the culture and the research objects. In this study, the
research objects are child patients so that the requirements of the reliability of services
can be higher. These results are also different from the research results from the study of
Amad and Samreen (2011) in Pakistan. The study of Amad and Samreen showed that

50
there are 5 factors in SERVQUAL affecting the satisfaction of the patients, besides
other factors such as: Professionality, Feedback and Guidance, Affordability.
With regard to the question of real assessment on factors of service quality and
customer satisfaction on services of Hai Duong Children’s Hospital, the average
assessment point is above the mean point (above 3 in the five point Likert scale) for
every factor. Customer response level is quite focused (the deviation level of answers is
quite small). These results compared with results from other researches in Vietnam
show that the satisfaction level of the patients with disease diagnosis and treatment
services of Hai Duong Children’s Hospital is higher, but not so much. For example, the
research of Bui Thi Thu Huong in Tien Du General Hospital in Bac Ninh province has
the average point = 3.43 but in study = 3.72, corresponding to factors of service quality:
Responsiveness (3.35 compared with 3.5), Assurance (3.89 compared with 3.25),
Empathy (3.55 compared with 3.39), Tangibles (3.76 compared with 3.53). So, we can
see that the satisfaction level of patients on the services of the hospital in this study is
higher than in the research of Bui Thi Thu Huong (2009) (excluding the factor
“responsiveness”). However the differential level is not high and the research of Bui Thi
Thu Huong was done three years ago when the economic conditions of the medical
branch of Vietnam are not as good as today.
For the impact intensity of factors on general satisfaction of the patients, the
factor “responsiveness” is the most important (β = 0.391), next is the factor “tangibles”
(β = 0.200), the factor “assurance” (β = 0.186), and the last is the factor “empathy” (β =
0.106). These research results are also similar with the results from the study of Amad
and Samreen (2011) which show that the factor “responsiveness and reliability” has the
biggest impact (β = 0.343), next is the factor “tangibles and professionality” (β = 0.222),
and the factor “assurance and empathy” has smallest impact (β = 0.189). This proves
that the assessment levels on the impact intensity of factors affecting the satisfaction of
patients with medical services of hospital in Vietnam (Hai Duong) in Pakistan fairly
resemble each other though the culture between these two countries is different
(Pakistan has Muslim tradition, Vietnam has Confucian and Buddhist tradition).
Moreover a very big similarity between these two societies is that both Pakistan and

51
Vietnam are developing countries, per capita income is low (1300usd/person for
Vietnam and 1378usd/person for Pakistan). (Source: the World Bank Data).
In addition, the research results also show no differences between demographic
factors on the satisfaction of patients with the disease diagnosis and treatment services
of the hospital. Besides this, there are still some other factors which may be added into
the research model to better improve the variability of the dependent variable “general
satisfaction”.
5.2 Recommendations
The research results show that to improve the quality of disease diagnosis and
treatment services of the hospital and customer satisfaction, it is needed to focus on
factors which have biggest impact first and then factors with lower assessment point as
a priority. From these results, the author recommends some following solutions for
increasing service quality and customer satisfaction:
(1) Solutions for improving the responsiveness. According to the assessment of
patient’s relatives, this is the most important factor that influences their satisfaction with
the service. The results also show that the assessment point for this factor is lowest (the
average point = 3.35), so to improve the satisfaction on this factor, the hospital needs to
do some solutions as follows:
+ Create truth for patients and their relatives by polite and right behaviors. To do
this, it is needed to adjust and standardize healthcare processes towards simplicity.
Build a culture of service and uniform code of conduct in the hospital. Create an
information channel (notifications, via email, feedback letter) in order that the hospital
leaders can know exactly the feelings and expectations of the patients, solve the
difficulties of the patients and therefore create trust from them.
+ Recruit good and professional doctors to the hospital. Have frequent
professional training programs for the staffs of the hospital. Owning good doctors will
bring trust and loyalty to the patients with the disease diagnosis and treatment services,
so the hospital needs to have policies for attracting professional doctors and nurses or
having collaboration with physicians from the major hospitals in examining and treating
the patients. At the same time, it is necessary for implementing of expertise capacity as

52
well as accessing to modern methods for existing staffs through training programs and
short and long-term training. The importance of the recruitment and expertise training is
to bring this information to the patients through propagation and dissemination of
medical knowledge and the achievements of the doctors working in the hospital.
+ Training the knowledge and answering skills for the nurses and staffs of the
hospital. Because the questions of patients often come to these persons first, so it is
needed for them to have professional and right knowledge to create trust on the disease
diagnosis and treatment services of the hospital.
(2) Solution for improving the factor “tangibles”. The factor “tangibles” is the
second important factor in the p\opinion of the patients. To improve this factor, the
hospital needs to do some following solutions:
+ The hospital need to be clean always. Hygiene requirement is a mandatory
requirement for the hospital. There is not only the place for treating diseases but also the
source of the risk of infection if it is not cleaned well, especially for child patients. To
ensure the hygienic conditions, the hospital needs to comply with the provisions of
health, regular do inspection and monitoring activities of the labor part to timely correct
when sanitation problems occur.
+ Require the staffs of the hospital to wear neat and polite uniforms.
+ Purchase and use modern medical equipments. During the operation, the
hospital facilities should be maintained and checked periodically to ensure no problems
and work well. The use of modern equipments of the hospital when diagnosing and
treating diseases will create huge trust from patients
+ Organize the using the facilities of the hospital scientifically, economically and
simply.
(3) Solutions for improving the factor “assurance”. This is also an important
factor affecting the satisfaction of the patients. To improve this factor, the hospital
should note some aspects as follows:
+ Need to notify accurately the time of diagnosing and treating diseases as well as
time for getting examination results for the patients. The creation of the accuracy in the
time of notification will create huge trust from patients, reduce the waiting time without

53
knowing when the service will be served, that may create discomfort to the patients and
their family.
+ Team of nurses and doctors in the hospital must always be ready to help the
patients. The requirements of services always need to be met fully and timely.
+ The hospital staffs must take care each patient carefully, show their sharing for
the difficulties of the patients when they are hospitalized.
(4) Solutions for improving the factor “empathy”. This is also an important
factor in the opinions of the patients. From the research results, the author recommends
some following suggestions:
+ Building the serving cultures for doctors, nurses and staffs of the hospital. They
need to understand the concerns and special needs of patients for appropriate
counseling. The serving attitudes must always be appreciated. And it will be better if the
hospital has incentive policies for special mirrors of caring patients. The creation of
honor awards will create the proud from the hospital staffs. They are expressed
themselves to others to satisfy their own perfection demand (Maslow, 1943).
+ Arrange suitable time of disease diagnosis and treatment for many different
objects. It is needed to have policies for receiving clinical diseases in any time to
facilitate the patients and their relatives.
Besides those solutions, the hospital also needs to concentrate on the factor
“reliability” of the hospital. Although the research results show that this factor has no
impact on the satisfaction of the patients with the services of the hospital, it is still a
must-be feature of the service, because if the hospital does not meet this requirement,
the customers (patients) will feel dissatisfied with the services.
5.3 Contributions and the importance of the study
5.3.1 Contributions of the study
SERVQUAL model has become a popular model to measure service
quality and test the relationship between service quality and customer satisfaction.
The main purpose of the study is to explore and test this relationship. The research
results show that there are relations between aspects of service quality in

54
SERVQUAL and customer satisfaction, at the same time proves that the factor
“reliability” has no impact on the satisfaction of the patients.
Main contributions of this study are:
Firstly is to test the reliability of SERVQUAL model in measuring service
quality and customer satisfaction in the health sector in a developing country like
Vietnam, especially the health care services for child patients.
Secondly, this study points out differences in awareness of Vietnamese
patients (customers) compared with other studies. In this study, the factor
“reliability” is considered as a must-be feature for health care services.
Thirdly, the study also provides useful reference documents for other studies
in the health sector.
5.3.2 Importance of the study
In the domain of learning, this study once again proved that SERVQUAL is
a good model for measuring the quality of the service and customer satisfaction.
Moreover, the detections of the study show that in a special field like healthcare
services, there are some factor in the original model that have no impact on the
satisfaction of customers (factor “reliability”). The study also suggests other
factors into the model to better explain the variability of the dependent variable
“general satisfaction”.
In the domain of reality, the research results helped the hospital leaders
know the status of the quality of the hospital’s services and the satisfaction level
of patients. This study also answered questions posed in the first part: Which
factors affect the satisfaction of patients with the services of the hospital? How is
the impact intensity of these factors? In addition, the study suggested some
solutions for improving the quality of the services and customer satisfaction with
the hospital.
5.4 Limitations of the study
Like other researches, the study also has some certain limitations as follows:

55
Firstly, the study just focused on one hospital and the research objects were only
inpatients, so there was no basic to compare the satisfaction level between hospitals
with each other and the differences between the group of inpatients and group of
outpatients. .
Secondly, the sample size of the study was still quite small and the sampling
method was non-probability, therefore it might lead to uncontrolled errors affecting the
results of the study.
Thirdly, because the research objects were the patient’s relatives, so it might be
lacked of the real perceptions and feelings of the patients with the quality of the
services.
Fourthly, the study was just done in a time point and not be tested again, so it
might not also evaluate the changing tendency of patient’s feelings about the quality of
the hospital’s services.
5.5 Directions for further studies
From above limitations, the author proposes some direction for future researches
as follows:
The first, it is need to expand the research scope to a group of different hospitals
to compare the public hospitals and private hospitals as well as the hospitals in different
areas.
The second, it is necessary for further studies to enlarge the sample size. They
can determine the sample size through probability theory and multiple sampling
(determine the minimum sample standard deviation of the first sample size) to increase
the accuracy of the statistical process.
The third, future studies can do repeated researches to detect the changing
tendencies in the long term and short term and explore “basic” factors affecting the
satisfaction of the patients with the hospital’s services.
The fourth, further researches should consider to add other new factors into the
research model to better improve the explanation ability of the existing model.

56
REFERENCES
Ahuja, M., MahlawatS & Masood.R.Z (2011), Study of service quality management
with SERVQUAL model: An empirical study of GOVT/NGO`S eye hospitals in
Haryana, Indian journal of commerce and management studies, 2(2) 310 – 318.
Ahmad, R & Samreen, H. (2011), Assessing the service quality of some selected
hospitals in Karachi based the SERVQUAL model, Pakistan Review, Juny, 266 –
314.
Al Ries and Jack Trout (1983), Positioning: The Battle for Your Mind, Edition 1,
McGraw-Hill/Al Ries and Jack Trout (2001), Positioning: The Battle for
Customer Mind, Statistics Publisher.
Atilgan, E., Akinci, S., & Arsoy, S. (2003), Mapping service quality in the tourism
industry, Managing Service Quality, 13 (5), 412 – 422
Andaleeb.S.S & Conway.S (2006), Customer satisfaction in the restaurant industry: an
examination of transaction - specific model, Journal of Services Marketing, 20(1),
3 – 11.
Anderson, E. W. & Fornell, C. (2000), Foundation of the American Customer
Satisfaction Index, Total Quality Management, 11, 7, 8869-8882.
Babakus.E & Mangold.W.G (1992), Adapting the SERVQUAL scale to hospital
services: An empirical investigation, Heath Service Research, 26(6), 767 – 786.
Brahmbohatt.M, Barser.N & Joshi.G.N (2011), Adapting the SERVQUAL scale to
hospital service: An empirical investigation of patients` perception of service
quality, International Journal of Multidisciplinary Research, 1(8), 27 – 42.
Butle F (1996), SERVQUAL review, critique, research agenda, European Journal of
Marketing, 30 (1), 8 -32
Bui Thi Thu Huong (2009), Evaluate the satisfaction of patients in the disease
diagnosis room, Tien Du General Hospital, Bac Ninh, Public Health Master’s
thesis, The University of Public Health.

57
Chakraborty.R & Majumdar.A (2011), Measuring consumer satisfaction in heath care
sector: The applicability of SERVQUAL, International Refereed Research
Journal, 2(4), 149 -160.
Cronin &Taylor (1992), Measuring service quality; A reexamination and extension,
Journal of Marketing, 56 (3), 55 – 68
Chow.C.C & Luk.P (2005), A strategic service quality approach using analytic
hierarchy process, Management Service Quality, 15(3), 278 – 289.
Durvasula.S & Lysonski.S (2010), Diagnosing service quality in retailing; The case of
Singapore, Journal of International Business Entrepreneurship Development,
5(1), 1- 17.
Garson GD (2002), Guide to Writing Empirical Papers, Theses, and Dissertations, New
York: Marcel Dekker.
Gerbing WD and Anderson JC (1988), An update paradigm for scale development
incorporating unidimensionality and its assessments, Journal of Marketing
Research, 25(2), 186 -192.
Grönroos,G (1984) A Service Quality Model and its Marketing Implications, European
Journal of Marketing, 18(4), 36 – 44.
Hoang Trong & Chu Nguyen Mong Ngoc (2008), Analysis of research data with SPSS
– Vol. 1, Hong Duc Publisher, Ho Chi Minh, Vietnam.
Hoang Trong & Chu Nguyen Mong Ngoc (2008), Analysis of research data with SPSS
– Vol. 2, Hong Duc Publisher, Ho Chi Minh, Vietnam
Harford.T (2004), The Undercover Economist (Vietnamese translation, 2008), Social
Labor Publisher
Kouthouris.C & Alexandris.K (2005), Can service quality predict customer satisfaction
and behavioral intentions in the sport tourism industry? An application of the
SERVQUAL model in the outdoors setting, Journal of Sport Tourism, 10(2), 101
– 111
Mostafa.M.M (2005), An empirical study of patients expectations and satisfactions in
Egyptian hospitals, International Journal of Health Care Quality Assurance, 18
(7), 516 – 532.

58
Mankiw.N.G (2005), Principles of Economics, International Student Edition, 3th ed,
Thomson.
Martensen. A., Gronholdt, L. & Kristensen, K. (2000), The drivers of customer
satisfaction and loyalty. Cross-industry findings from Denmark, Total Quality
Management, 11, 8544-8553
Maccallum.R.C, Widaman.K.F, Zhang.S & Hong.S (1999), Sample size in factor
analysis, Psychological Methods, 4, 84 - 99
Nunally & Bernstein (1994), Psychometric Theory, 3th ed, Mc Graw – Hill, New York.
Nguyen Thi Phuong Tram (2008), The quality of e-banking: Compare SERVQUAL and
Gronroos model, Master`s thesis, Ho Chi Minh University of Economics,
Vietnam.
Nguyen Dinh Phan, Truong Doan The & Dang Ngoc Su (2006), the textbook “Total
Quality Management in organizations”, Social Labor Publisher.
Nguyen Trung Kien (2005), Evaluate the satisfaction of students on the training quality
University of Economics and Business Administration – Thai Nguyen university,
Master’s thesis, Thai Nguyen university.
Nguyen Dinh Tho (2011), The scientific method in business research, Social Labor
Publisher, Vietnam.
Oliveira.O.J.D (2009), Adaptation and application of the SERVQUAL scale in higher
education, POMA 20th Annual Conference, Orlando Florida USA.
Pham Nhat Yen (2008), Evaluate the satisfaction of patients on the disease diagnosis
and treatment in the department of medical examination and treatment as
required in Bach Mai hospital, Public Health Master’s thesis, University of Public
Health.
Parasuraman, A. V. A. Zeithaml, & L.L.Berry (1985): A conceptual Model of Service
Quality and its Implications for Future Research, Journal of Marketing, 49, 41-
50.
Soita.P.W (2012), Measuring perceived service quality using SERVQUAL: A case
Uganda Health and Fitness sector, International Journal of Business and Social
Science, 3(5), 261 -277.

59
Spreng, R. A., and Mackoy, R. D., (1996), An Empirical Examination of a Model of
Perceived Service Quality and Satisfaction, Journal of Retailing, 72(2), 201-214.
Seth.A, Momaya.K & Gupta.H.M (2008), Managing the customer perceived service
quality for Cellular mobile Telephony: An Empirical investigation, VIKALPA,
3(1), 19 - 34
Wheeland.C (2002), Naked Economics, Vietnamese translation (2008), Social Labour
Publisher
Zarei.A, Arab.M, Froushani.A.R, Rashidian.A & Tabatabaei.S.M.G (2012), Service
quality of private hospitals: The Iranian patients` perspective, BMC Health service
Research, 1 – 7.
Zeithaml, V.A., & Bitner, M.J (2000), Services marketing; integrating customer focus
across the Firm, 2nd ed, Mc Graw Hill. New York
Zekiri.J (2011), Applying SERVQUAL Model and factor analysis in assessing customer
satisfaction with service quality: The case of Mobile Telecommunications in
Macedonia, International Bulletin of Business Administration, 10(11), 86 -10

60
QUESTIONNAIRE
Hello!
I am Thanh. a Master student at Shu-Te University, Taiwan. At this time, I am
doing Master’s thesis research under the title "A relationship study between healthcare
quality and patient’s key caretaker satisfaction for Hai Duong children’s hospital in
Vietnam."
Under the direction of Dr. Jau-Shyong Wang and Dr. Sheng-Jung Li in the
Faculty of the School of Business Administration, Shu-te University and Dr. Pham Vu
Thang, To complete this thesis, I would like to invite you, the patient’s relatives in Hai
Duong Children’s Hospital to answer questions in this questionnaire. All your private
information will be kept strictly confidential and will not be attributed to the individual
or organization. All responses will be stored in a secure environment. The results of this
research would be used for academic purposes only. This thesis is a non-profit research,
so if you need to know about research results, please contact me via email address….
1. The contents of questions
Please rate the extent to which you agree with each statement below. Circle the
number that best indicates for each statement (the higher agreement level you choose,
the more you agree with). In which:
(1) Strongly disagree
(2) Disagree
(3) Neutral
(4) Agree
(5) Strongly agree
No. Code The contents of question Agreement level
1 2 3 4 5 I Reliability 1 REL1 You trust the results of diagnosis and treatments of the
hospital.. 1 2 3 4 5 2 REL2 You see that the hospital staffs tried not to make
mistakes when implementing treatments for patients. 1 2 3 4 5

61
3 REL3 You see that the quality of health care services is as good as the notice of the hospital. 1 2 3 4 5
4 REL4 You find the medical examinations of the hospital are precisely done. 1 2 3 4 5
5 REL5 You find if the staffs of the hospital promise to do something in a fix time, they will do it. 1 2 3 4 5
II Assurance 6 ASS1 You see that the doctors and nurses are never too busy
to meet the needs of the patients (for example: medical procedures, asking the place to test, etc.). 1 2 3 4 5
7 ASS2 You are informed by medical staffs about the done-time of the services will be carried out (for example: time to response the test results, etc.). 1 2 3 4 5
8 ASS3 You see that the doctors and nurses always show their courtesy and willingness to help the patients. 1 2 3 4 5
9 ASS4 You find that the services of the hospital are always provided fully and promptly. 1 2 3 4 5
III Empathy 10 EMP1 You find that the doctors devotedly care for each
patient. 1 2 3 4 5 11 EMP2 You feel that the doctors and nurses always understand
the worries and special needs of the patients. 1 2 3 4 5 12 EMP3 You find that the patients are treated and cared
enthusiastically and thoughtfully. 1 2 3 4 5 13 EMP4 You find the time of medical examination is convenient
for the patients. 1 2 3 4 5 IV Responsiveness 14 RES1 You think that the behaviors of the physicians create
the trust to patients. 1 2 3 4 5 15 RES2 You feel safe when diagnosing and treating diseases in
the hospital. 1 2 3 4 5 16 RES3 You think that the hospital has good doctors and
nurses. 1 2 3 4 5 17 RES4 You think that the medical staffs have sufficient
knowledge to answer all questions of patients. 1 2 3 4 5 V Tangibles

62
18 TAN1 You find that the hospital is always clean. 1 2 3 4 5 19 TAN2 You see that the uniforms of the medical staffs are
always neat and courteous. 1 2 3 4 5 20 TAN3 You think the facilities of the hospital are attractive.
1 2 3 4 5 21 TAN4 You think that the facilities (tools, equipments…) of
the hospital are modern and sufficiently provided. 1 2 3 4 5 VI General satisfaction with disease diagnosis and treatment
services 22 SAT1 You feel satisfied with the facilities of the hospital 1 2 3 4 5 23 SAT2 You feel satisfied with the assurance of the hospital. 1 2 3 4 5 24 SAT3 You will use the medical examination services of the
hospital for your children when needed. 1 2 3 4 5 25 SAT4 You will introduce the hospital to others. 1 2 3 4 5 26 SAT5 In general, you feel satisfied with the services of the
hospital. 1 2 3 4 5 2. Personal information
Please share with us your personal information by answering following questions:
- The age of your relative (patient):
1. < 1; 2. From 1 to 2; 3. From 2 to 3; 4. From 3 to 5; 5. > 5
- Your education level:
1. High school; 2. Intermediate; 3. College; 4. University and above; 5. Other
- Your job:
1. Farmer; 2. Worker; 3. Officer; 4. other
- Your montSATy income (both husband and wife) (vnd):
1. < 5 mil.; 2. From 5 -10 mil.; 3. From 10 -15 mil.; 4.> 15 mil.
Thank you for your cooperation!