- 1. AAllll aabboouutt ppllaatteelleett iimmmmuunnoollooggyy
2. 2014/10/5 09:00~09:30 Nelson Hirokazu TsunoImmune-mediated
Thrombocytopenia andDetection of Anti-platelet Alloantibodies 3.
Platelet antigen Platelet antibody Disease associated
plateletimmunology Detection of anti-plateletantibodies Q&A 4.
RBC antigens ( ABO antigens, Rh, Lewis, Duffy .)Human leukocyte
antigen (HLA)Human platelet antigens (HPA)Glycoprotein IV (CD36,
Naka ) 5. Antigens on human platelets are categorizedaccording to
their biochemical nature into:carbohydrate antigens on glycolipids
andglycoproteins (A, B, O, P, Lewis antigens),protein antigens (HLA
Class-I; GPIIb/IIIa,GPIb/IX/V)Many platelet antigens are shared
with other bloodcells, e.g.,ABO and HLA class I antigens, but some
ofthe glycoprotein antigens are expressedpredominantly on
platelets. These antigens arecommonly referred to as
platelet-specificalloantigens or human platelet alloantigens
(HPAs),although some of these are also present to a lesserextent on
other blood cells, e.g., HPA-5 on activatedT lymphocytes. 6.
Platelet-specific alloantigens are located on plateletmembrane GPs
involved in hemostasis throughinteractions with extracellular
matrix proteins in thevascular endothelium and plasma
coagulationproteins.CD36 is found on platelets, erythrocytes,
monocytes,differentiated adipocytes, skeletal muscle,
mammaryepithelial cells, spleen cells and some skinmicrodermal
endothelial cells.The majority of these antigens are on the
GPIIb/IIIacomplex, which plays a central role in
plateletaggregation as a receptor for fibrinogen,
fibronectin,vitronectin, and von Willebrand factor. 7. Other
important GPs are GPIb/IX/V,the main receptorfor von Willebrand
factor involved in platelet adhesionto damaged vascular
endothelium; GPIa/IIa, which isinvolved in adhesion to collagen;
and CD109, whichalso appears to be a collagen receptor.Congenital
deficiency of these GPs results in bleedingdisorders, e.g., lack of
GPIIb/IIIa causes Glanzmannsthrombasthenia, and absence of
GPIb/IX/V results inBernard-Soulier syndrome.CD36 is also known as
glycoprotein IV (gpIV) orglycoprotein IIIb (gpIIIb) in platelets
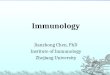
and gives rise tothe Naka antigen. 8. 28 systems34 antigens6
systems with two antigens (a,b)HPA-1~5 and HPA-15On 6
Glycoproteins14 systems on GPIIIa7 systems on GPIIb4 systems on
GPIa1 system on GP1ba1 system on GP1bb1 system on CD109 9. 4 7 14 1
1 199660000 mmooll//pplltt 80,000 mol/plt 25,000 mol/plt 1,000
mol/pltBritish Journal of HaematologyVolume 161, Issue 1, pages
314, 10. TRANSFUSION 2001;41:1553-1558. 11. Platelet membrane
glycoprotein (GP) IV (also calledCD36 and GPllb) deficiency is
associated with Nak"-negative plateletsDepending on the nature of
the mutation in codon 90CD36 may be absent either on both platelets
andmonocytes (type 1) or platelets alone (type 2).The CD36-negative
is a phenotype observed in mostAsian countries, and the risks
associated withalloimmunization to this isoantigen. 12. Platelet
antigen Platelet antibody Disease associated plateletimmunology
Detection of anti-plateletantibodies Q&A 13. Alloantigens
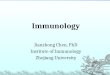
implicated in allo immune thrombocytopeniaAntigen NAIT PTR PTP PAIT
TAATPHPA (+) (+) (+) (+) (+)ABH (+) (+) (-) (?) (?)Class I HLA (+)?
(+) (-) (?) (?)CD36 (+) (+) (+)? (?) (?)Neonatal alloimmune
thrombocytopenia (NAIT)Platelet transfusion refractoriness
(PTR)Post-transfusion thrombocytopenic purpura (PTP)Passive
alloimmune thrombocytopenia (PAT)Transplantation-associated
alloimmune thrombocytopenia (TAATP)Dr. N.H. Tsuno presentedin 24th
regional congress of ISBT 14. NAIT due to anti-HLA antibodiesCase
of NAIT suspectedly due to anti-HLA are reported,but the
association needs to be confirmed.Class I HLA Abs are found in
about one third ofmultiparous women (15~31%), and anti-HPA Abs
lessfrequency; however, platelet destruction is usuallycaused by
the anti-HPA AbsProtective immune mechanism of the placenta :
anti-HLAantibodies adsorbed by the stromal cells of
placentaexpressing paternal antigens; routinely, the infants
areborn with normal platelet counts.Dr. N.H. Tsuno presentedin 24th
regional congress of ISBT 15. The risk of ICHwas the highestwith
anti-HPA-3Antibody specificity Nmber of cases %HPA-1a 1 7000, CCI :
( -) X BSA/ 34. HLA matched platelet: for anti-HLAantibodyplatelet
cross-match 35. TTTTPPmetalloprotease,ADAMTS-13von
Willebrandsthrombospondin-1thrombospondin-1like
domainsthrombospondinADAMTS 13Von Willebrand'smetalloproteaseADAMTS
13Von Willebrand'spentad 36. HIT is caused by the formation
ofabnormal antibodies that activateplatelets. 37. ITP PTR TTP HIT
DITAnti-plateletantibodyscreen+/-Auto ant-plateletantibody (+)+ - -
-+drug incubation(+)SpecialantibodiesAutoantibodiesAllo antibodies
Anti-ADMATS-13Anti-PF4 Anti-drugantibodiesPlateletspecific targetGP
Ib-IX,IIb-IIIa,Ia-Iia,IVGP Ib-IX,IIb-IIIa,Ia-Iia,IV( include
HLA)ADMATS-13PF4heparincomplex
onplateletDetectionmethodSPRCAFIPAELISAMAIPA, SPRCA,ELISA,
FIPA,MPHAFRET Gel CATELISASPRCA( Capture-Por MASPAT) 38. Disease
Common symptoms Differential symptomsHemolytic
uremicsyndromeThrombocytopenia,hemolytic anemia
withschistocytosisGastrointestinal infections: E.coli
0157:H7,Shigella dysenteriaHemorrhagic colitis High
serumcreatinineHELLP syndrome Hemolytic
anemia,thrombocytopeniaElevated liver
enzymesPre-eclampsia,eclampsiaThrombocytopenia,proteinuriaHypertension
Peripheral edemaProteinuria Increased
D-dimerDisseminatedintravascularcoagulationThrombocytopenia
Markedly increased D-dimerProlonged prothrombin
timeCatastrophicantiphospholipidsyndromeThrombocytopenia
Positivelupus-like anticoagulantAntinuclear and
antiphospholipidantibodiesEvans syndrome Hemolytic
anemia,thrombocytopeniaPositive Coombs test Usually absenceof
end-organ ischemic
symptomsHeparin-inducedthrombocytopeniaThrombocytopenia Thrombosis
mainly in large arteriesand veins Antiplatelet antibodies 39. Major
pathogenesis of TRALI isknown to be related with anti-HLAclass I,
anti-HLA class II, oranti-HNA in donor's plasma.However, anti-HLA
or anti-HNA inrecipient against transfuseddonor's leukocyte
antigens alsocause TRALI in minor pathogenesisand which comprises
about 10% ofTRALI. 40. SSppeecciiffiicciittiieess ooff
lleeuukkooccyyttee aannttiibbooddiieessaassssoocciiaatteedd
wwiitthh TTRRAALLII ccaasseeTotal n=30 Fatalities
Leuko-agglutininsHLA class I 6 1 6HLA class II 13 2 0HNA-1a,2a 2 0
1HNA-3a 9 5 9 41. Platelet antigen Platelet antibody Disease
associated plateletimmunology Detection of anti-plateletantibodies
and antigen typing Q&A 42. Antigen typing Platelet antibody
detectionmethod Concordance of antibody detection Other platelet
disease associatedtest Differential test of plateletdisease 43.
ELISA methode.g. Bio-RadHPA1a TypingAssay 44. Some SSP kit provided
HPAgenotypeE.g. innotrain HPA-readygene 45. PCR-SSP5'
TCACAGCGAGGTGAGGCCA 3'5' TCACAGCGAGGTGAGGCCG 3'5'
GGAGGTAGAGAGTCGCCATAG 3'HPA-1 46. MAPIAMonoclonal Antibody-specific
Immobilization of platelet antigensGold standard methodModified
Antigen capture ELlSA (MACE)Commercial kit :GTI diagnosticsPurified
platelet glycoproteins ELlSA/bead methodCommercial kit :GTI
diagnostics (Pakplus, PakLx)Specific platelet glycoprotein
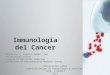
(IIb/IIIa,Ib/Ix,Ia/IIa,GPIV,HLA))Flowcytometry or FIPA 47. Sample
Consensus results % concordance MPHA MAIPA Overall1 Negative 100
(18/18) 100 (13/13) 100 (18/18)2 Anti- HLA-class I 83.3 (15/18)
71.4 (10/14) 100 (18/18)3 Anti-Nak a 100 (18/18) 76.9 (10/13) 100
(18/18)4 Anti-HPA-5b 88.9(16/18) 100(14/14) 94.4 (17/18)Anti-
HLA-class I 50(9/18) 21.4(3/14) 44.4(8/18)5 Anti-HPA-4b 100(18/18)
53.8(7/13) 100(18/18)6 Anti-HPA-1a - 100(14/14) 83.3(15/18)For
IPIWP workshop, HPA-1b/b and HPA-5b/5b plateletswere distributed to
the labs by Dr. Santoso 48. By measuring ADAMTS13 in plasma,it has
been clearly shown thatpatients with inherited TTP havesevere
ADAMTS13 deficiency. However, patients with acquiredTTP present
with clinical andlaboratory heterogeneity, andthere are unequivocal
cases ofacquired TTP with measurableplasma levels of ADAMTS13. 49.
Test characteristics: very rapid: result in less than20 min
(including 10 mincentrifugation) very simple procedure very
reliable performance* economical: unused microtubes inthe card can
be used at a latertime (if the aluminium seal isintact) 50. PTR
NAITP HIT DIT TTP ITP TRALITest orinvestigationCCI CBC, DC
CBC,DCHeparin historyDrug history DATBUNCBC,DCDAT
BNPCBCX-raySerological testPRA(class I)ELISA(Pakplus)SPRCA
(capture-P,MASPAT):anti-plateletantibodyscreening, andcross
matchingPIFALuminex PRAclass IMAIPAMPHAMother and fetusPRA(class
I/II)ELISA(Pakplus)SPRCA
(capture-P,MASPAT):anti-plateletantibodyscreeningPIFALuminex
PRAMAIPAMPHAMother serum Vs.Father/baby plat.SPRCA, PIFA
crossmatchingELISA (PF4)CAT (PF4)Serum + drug, oreluentSPRCA (
Capture-P, MASPAT)FRET:ADMATS-13 activityELISA(Pakauto)ELISA
(Pakplus)SPRCA( Capture-P,MASPAT ): autoantibody andallo
antibodyPIFA (auto)Donor serum( and/or patient)Luminux PRA( class
I/classII/HNA)ELISA PRA(class I/II)flowPRA
(classI/II)Leuko-agglutinintestMAIGAGIFAAntigen HLA class I
typingHPA typingCD36 typingParent and fetus:HLA class
I/IItyping,HPA typingCD 36 typing 51. Platelet antigen Platelet
antibody Disease associated plateletimmunology Detection of
anti-plateletantibodies Q&A 52. Email:
[email protected],[email protected], Plurk :
[email protected] : jschang12QQ: 1150352697Line:
jschang12Blog: http://www.jschang.idv.twYoutube :
http://tw.youtube.com/ntuh-tmWebsite:
http://www.jschang,idv.twMobilephone -0928825645Office
0223123456ex65404