Embed Size (px)
DESCRIPTION
Anerkendte binokulære synslidelser lever en skyggetilværelse i Danmark. Ved hjerneskade optræder synslidelserne særdeles hyppigt. Enhver form for rehabilitering, som ikke iagttager disse, resulterer i unødvendig lidelse og heling under patientens potentielle niveau.
Citation preview

Binokulære synslidelser:Et overset problemefter hjerneskade
Torben Helstrup
Neurooptometrist FCOVD
www.privatsyn.dk

Dagens program
• Fra øjne til synshjerne
• Øjnenes sigtesystem (fiksation)
• Binokulære synslidelser (WHO)
• Undersøgelser
• Neurooptometri
• Terapi
• Konklusion
Binokulære lidelser. 2013. Helstrup 2

Sensoriske system
Centrale og perifere syn
Binokulære lidelser. 2013. Helstrup3

Synsbaner
Synsfelter
Binokulære lidelser. 2013. Helstrup 4

To signalstrømmeHVOR og HVAD
De visuelle motorveje
Binokulære lidelser. 2013. Helstrup 5

Kredsløb
Sensoriske og motoriske systemer i samspil.
Input og outputSamtidigt
Binokulære lidelser. 2013. Helstrup 6

Synssans
1. Input-output samtidigt.
2. Fiksationsfeltet er det samme som hjernens fokus”minds eye”.
3. Forudse og kompetent handling
Øjnenes biomekanik erden synbare part.
Okulær fiksation er trin 1
Input
Output
Put - put
Binokulære lidelser. 2013. Helstrup 7

Det hele starter med Okulær fiksation
Binokulære lidelser. 2013. Helstrup
Sigtemekanik til trådløs online rumlig sansning
8

Optisk system
Neuromuskulært system
Elektrisk system
Kontrol af intenderede bevægelser
Koordineret signal til muskler
Processering af visuelle signaler
Kommando til fiksationog bevægelse
Input
Output
Put-put
Øjnenes biomekanik
9

Fiksationsområde = SpotlightAnkerpunkt og trådløse perceptuelle kontakt i fysiske verden
Binokulære lidelser. 2013. Helstrup 10

Binokulære ankerpunkt (fiksationsfelt)
2
40 %
Motorisk triangulation
Stereopsis
Binokulære lidelser. 2013. Helstrup 11

Ballistisk saccade til nyt objekt Bi-fiksation: Smooth pursuit– og
vergensfunktionen samarbejder(bi-fiksation indenfor Panums område)
Vergens vinkel
Fiksationsfelt (Mind’s eye)Input-output drevet
Nærtriade Selvstændige og gensidigt modulerende reaktioner:• Vergens / version• Akkommodation• Pupil
Biomekanik til fiksation (to øjne)Binokulære syn
Binokulære lidelser. 2013. Helstrup 12

Binokulære lidelser. 2013. Helstrup
Versionsubsystem
Vergencesubsystem
Conjugatemovements
Disconjugatemovements
Fast eyemovements
Slow eyemovements
Vestibular
Proprioceptive
Vergence eyemovements
X,Y Z
Ocular motor systemIn 3D space
13

Binokulære synslidelser
Binokulære lidelser. 2013. Helstrup 14

World Health Organisation: ICD 2007
• Diseases of the eye and adnexa(H00-H59)
• H00-H06Disorders of eyelid, lacrimal system and orbit
• H10-H13Disorders of conjunctiva
• H15-H22Disorders of sclera, cornea, iris and ciliary body
• H25-H28Disorders of lens
• H30-H36Disorders of choroid and retina
• H40-H42Glaucoma
• H43-H45Disorders of vitreous body and globe
• H46-H48Disorders of optic nerve and visual pathways
• H49-H52Disorders of ocular muscles, binocular movement, accommodation and refraction
• H53-H54Visual disturbances and blindness
• H55-H59Other disorders of eye and adnexa
Lidelser som afhjælpes med optisk behandling – og/eller terapi
Medicin eller kirurgi har ingen eller begrænset virkning
Binokulære lidelser. 2013. Helstrup 15

Ortho
Basic eso(378.41)
AF=NF @ ACA norm
(WHO H 50,3)Afst. + nær problem
Divergensinsufficiens
(378.85)AF>NF @ ACA lav
(WHO H 51,8)Afst. problem
Konvergens insufficiens
(378.83)NF>AF @ ACA lav
(WHO H 51.1)Nærproblem
Basic exo(378.42)
AF=NF @ ACA norm
(WHO H 50,3)Afst. + nær problem
Divergens Excess(378.85)
AF>NF @ ACA høj(WHO H 51,8)Afst. problem
Konvergens excess(378.84)
NF>AF @ ACA høj(WHO H 51.1)Nærproblem
Udvidet Duane klassifikation
Eso
Exo
ICD 9 og 10koder
Binokulære lidelser. 2013. Helstrup
Se konsensus testprotokollerAOA og AAO
16

Asthenopia (aesthenopia) or eye strain is an condition that manifests itself through nonspecific symptoms such as fatigue, pain in or around the eyes, blurred vision, headache and occasional double vision.
Symptoms often occur after reading, computer work, or other close activities that involve tedious visual tasks.
http://en.wikipedia.org/wiki/Asthenopia
Asthenopia (WHO ICD 10; H 53,1)
Binokulære lidelser. 2013. Helstrup 17

Tørt øje
Asthenopi
Ergonomi refraktion Binokularitet
AmetropiAstigmatismeAkkomodationPresbyopi
HeteroforiFusionACASuppression
ICHD 11.3.2 ICHD 11.3.3
IndretningSynsafstandBlikvinkelBelysning
Årsagssammenhænge
Binokulære lidelser. 2013. Helstrup
http://journals.lww.com/optvissci/Fulltext/2003/11000/Is_all_Asthenopia_the_Same_.8.aspx 18
http://www.ncbi.nlm.nih.gov/pubmed/14627938

The International Classification ofHeadache Disorders, 2nd Edition. (ICHD-II).
IHS WHO Diagnosis
ICHD-II Code ICD-10NA Code
11.3.2 G 44.843 Headache attributed to refractive errors (H 52,0 – H 52,7)
11.3.3 G 44.843 Headache attributed to heterophoria or heterotropia (latent or manifest squint) (H 50,3 – H 50,5)
Binokulære lidelser. 2013. Helstrup 19

General approach to diplopia.
Danchaivijitr C , Kennard C J Neurol Neurosurg Psychiatry
2004;75:iv24-iv31©2004 by BMJ Publishing Group Ltd
TBI/CVA
20

Undersøgelser
Binokulære lidelser. 2013. Helstrup 21

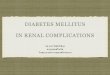
Occurrence of oculomotor dysfunctions in acquired brain injury: A retrospective analysis
Kenneth J. Ciuffreda, O.D., Ph.D: Optometry (2007) 78, 155-161
Table 3. Summary of the percentage of individuals in each subgroup (where for TBI n= 160 and for CVA n= 60) within a given category of ocular motor dysfunction and the most common anomaly present
Ocular motor dysfunction TBI (%) Most common anomaly CVA (%) Most common anomaly
Accommodation 41.1 Accommodative insufficiency 12.5 Accommodative infacility
Versional 51.3 Deficits of saccades 56.7 Deficits of saccades
Vergence 56.3 Convergence insufficiency 36.7 Convergence insufficiency
Strabismus 25.6 Strabismus at near 36.7 Strabismus at far
CN palsy 6.9 CN III 10 CN III
Note: The “n” represents the number of persons tested for accommodation, which onlyincluded those under the age of 40 years (i.e., prepresbyopic),TBI = 51 and CVA= 8.
Binokulære lidelser. 2013. Helstrup 22

OPTOMETRIC CARE OF THE PATIENT WITH ACQUIRED BRAIN INJURY (1)
Vision dysfunctions are among the most common sequelae associated with acquired brain injury (BI). The anatomy and physiology of the vision system, the vascular and neural network of the brain, and the dynamics of head trauma all contribute to the high incidence of visual dysfunction with brain injury. Causes of brain injury which may contribute to visual dysfunction include blunt, penetrating, or acceleration/deceleration trauma; suffocation/hypoxia; pharmacological toxicity; and cerebral vascular accidents. Injury to the eye or the sensory, motor or associated areas of the visual system of the BI patient may result in the development of the following:
Strabismus Binocular vision dysfunctions Reduced visual acuity at far Accommodative disorders Ocular motility disordersintegration
Reduced visual acuity at near Visual field loss Deficits in visual motor integration Difficulties in visual perception
www.aoa.org
Binokulære lidelser. 2013. Helstrup 23

OPTOMETRIC CARE OF THE PATIENT WITH ACQUIRED BRAIN INJURY (2)
Since activities of daily living involve effective integration of visual information processing and visual motor performance, the BI patient is frequently handicapped as a consequence of disruption in the visual system. A significant number of patients with BI will present with signs and symptoms which indicate a vision problem. These include, but are not limited to, the following:
Symptoms Double vision Blurred vision Reduced ability to sustain attention on visual tasks Dizziness Headaches Eye strain Confusion related to visual tasks Difficulty reading
Signs Eye turn Closing or covering one eye Head tilts or turns Bumping into objects Abnormal posture Balance and coordination problems Poor judgement of depth Reduced ability to accuratelylocalize objects
www.aoa.org
Binokulære lidelser. 2013. Helstrup24

Snarligt kommende / Artikel til Danske Fysioterapeuter
Behandling af en patient med dobbeltsyn og balancebesvær i akut og subakut fase efter en apopleksi - et samarbejde mellem fysioterapeut og neurooptometrist – en case rapport
Eriksen K udviklingsfysioterapeut1,*; Helstrup T neurooptometrist f.c.o.v.d.2 ; Meden P overlæge 3
1 Fysio- og ergoterapiafdelingen, Bispebjerg Hospital opg. 10, Bispebjerg Bakke 23, 2400 København NV2 Københavns Private Synsplejeklinik, Rødovre Centrum 247, 2610 Rødovre 3 Apopleksiklinikken Bispebjerg Hospital. Bispebjerg Hospital opg. 1, Bispebjerg Bakke 23, 2400 København NV
Binokulære lidelser. 2013. Helstrup 25

Neurooptometri
Binokulære lidelser. 2013. Helstrup 26

Neurooptometri
• Neurooptometriske disciplin:
– Læren om sammenhængen mellem hjerneprocesser og adfærd, med særlig henblik på visuel perception og efterfølgende meningsfyldte handlinger.
– Fokus på udvikling og helbredelse frem for sygdom.
Binokulære lidelser. 2013. Helstrup 27

Syn og kompetent aktion:Uendeligt loop
input
output
put-putYdre verden Indre verden
Bottum-up
Top-downSansesignaler
Kompetent aktion
Behandling:Reparere – hvad repareres kan
Behandling:(Gen)lære nye skemaer
Binokulære lidelser. 2013. Helstrup 28

Terapi
Binokulære lidelser. 2013. Helstrup 29

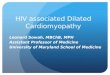
Synstræning i Danmark: Skønsmæssigt fordelt på fagdicipliner Fysio- ergoterapeuter
mv. 80 %
Optikere (papegøje princippet) 10 %
Øjenlæger / skeleterapeuter 2 %
Optometrister (grovmotor princippet) 5 %
Neurooptometrister (Naturvidenskabelige) 3 %
Binokulære lidelser oversete
Binokulære lidelser. 2013. Helstrup 30

yx
z
Binokulære lidelser. 2013. Helstrup 31
Version
Vergens(nærtriade ? )

Klassiske konvergensøvelser
Tvivlsom prognose: Træner totalrespons•Fastholder kompensation•Forhindrer normalisering
Binokulære lidelser. 2013. Helstrup 32

VergensøvelserGod prognose: Træner svage delfunktion•Kontrol af fokusindstilling•Kontrol af centralsyn
Binokulære lidelser. 2013. Helstrup33

Visuomotorisk aktivitet i 4DBi-fiksationsevne (3D syn) bør være afklaret før aktiviteter i nær-fjern dimensionen (tid-rum)
Binokulære lidelser. 2013. Helstrup 34

Filtre, prismer og sektorokklusion
Binokulære lidelser. 2013. Helstrup 35

Konklusion
• Binokulære synslidelser afstedkommer synsforstyrrelser og udtrætning (trætte øjne, koncentrationssvigt, hovedpine, sløret/ dobbeltsyn, svimmelhed: Mild - svær)
• Masser af synstræning afvikles dagligt – uden at vergensfunktionen og binokulære lidelser iagttages.
• Al form for rehabilitering risikerer - dels at uønskede adaptationer konserveres i stedet for afhjælpes, dels en masse unødig lidelse og tidsforbrug som, alt i alt, ikke imødekommer patientens potentiale
Binokulære lidelser. 2013. Helstrup 36

http://c.ymcdn.com/sites/www.covd.org/resource/resmgr/position_papers/acquired-brain-injury_-_aoa.pdf
OPTOMETRIC CARE OF THE PATIENT WITH ACQUIRED BRAIN INJURY (COVD + AOA)
http://nora.cc/
Consensus clinical guidelines: Vergens- og akkommodationsfunktionernehttp://www.aoa.org/documents/CPG-18.pdf
Erhvervet hjerneskade:Tre væsentlige kilder til yderligere information
Binokulære lidelser. 2013. Helstrup 37
Tværfaglig rehabilitering efter hjerneskade