Embed Size (px)
DESCRIPTION
Contracted pelvis
Citation preview

CONTRACTED PELVIS
PROF. M.C. BANSALPROF. M.C. BANSALM.B.B.S , M.S. , M.I.C.O.G, F.I.C.O.G.M.B.B.S , M.S. , M.I.C.O.G, F.I.C.O.G.
Founder Principal& Controller;Founder Principal& Controller;
Jhalawar Medical College and Hospital Jhalawar.Jhalawar Medical College and Hospital Jhalawar.
Ex. Principal & Controller;Ex. Principal & Controller;
Mahatma Gandhi Medical college And Hospital, Sitapura, Jaipur.Mahatma Gandhi Medical college And Hospital, Sitapura, Jaipur.
DR. RIDHI KATHURIADR. RIDHI KATHURIA
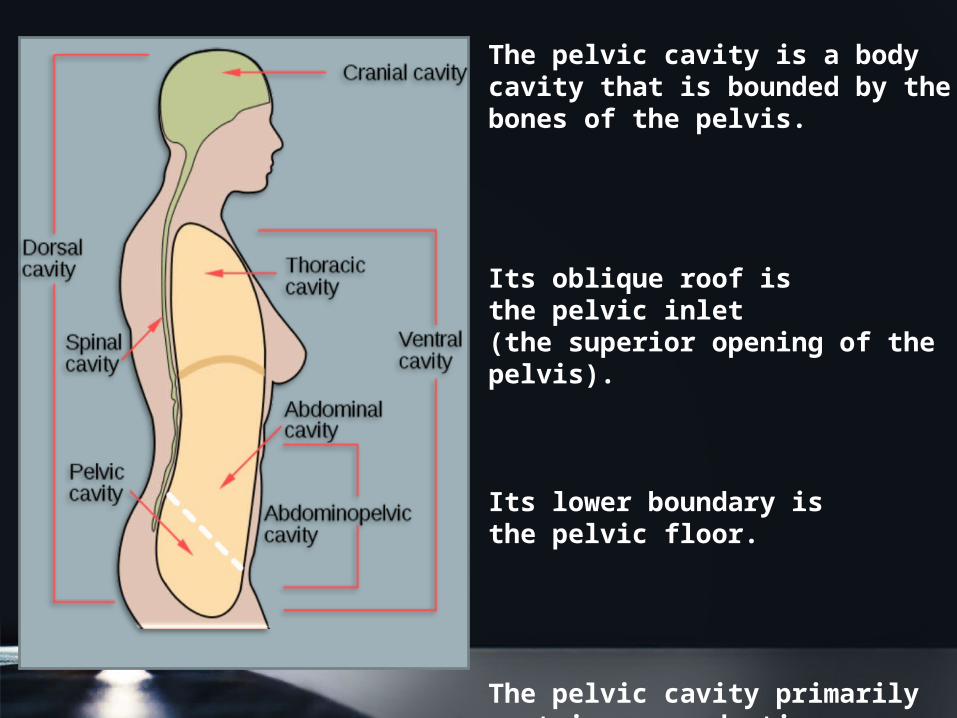
The pelvic cavity is a body cavity that is bounded by the bones of the pelvis.
Its oblique roof is the pelvic inlet (the superior opening of the pelvis).
Its lower boundary is the pelvic floor.
The pelvic cavity primarily contains reproductive organs, the urinary bladder, the pelvic colon, and the rectum.
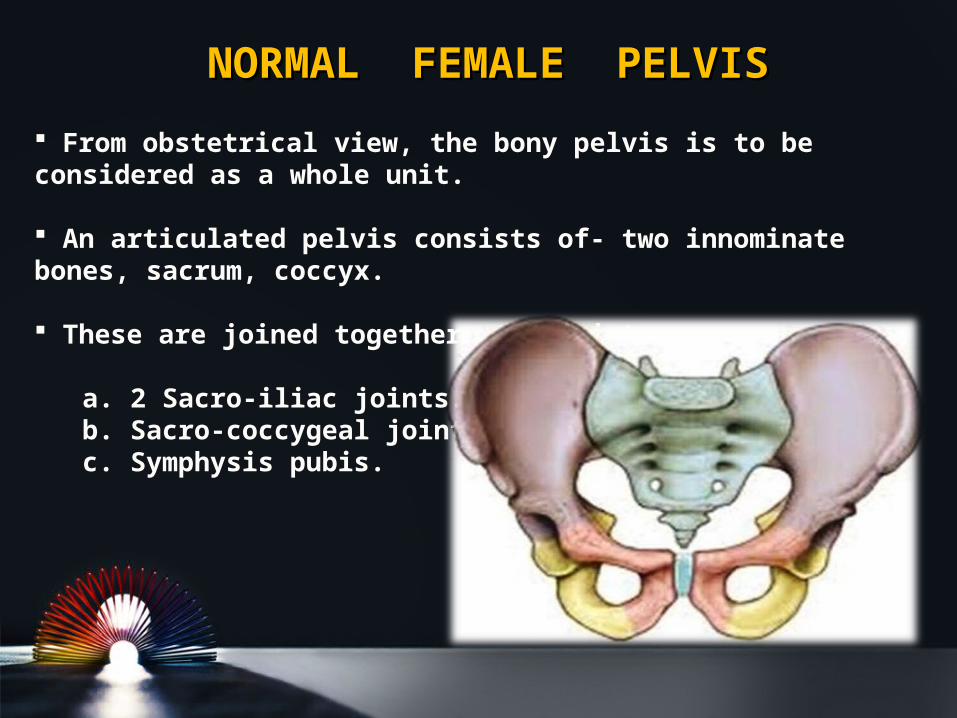
NORMAL FEMALE PELVISNORMAL FEMALE PELVIS
From obstetrical view, the bony pelvis is to be considered as a whole unit.
An articulated pelvis consists of- two innominate bones, sacrum, coccyx.
These are joined together at 4 joints- a. 2 Sacro-iliac joints. b. Sacro-coccygeal joints. c. Symphysis pubis.
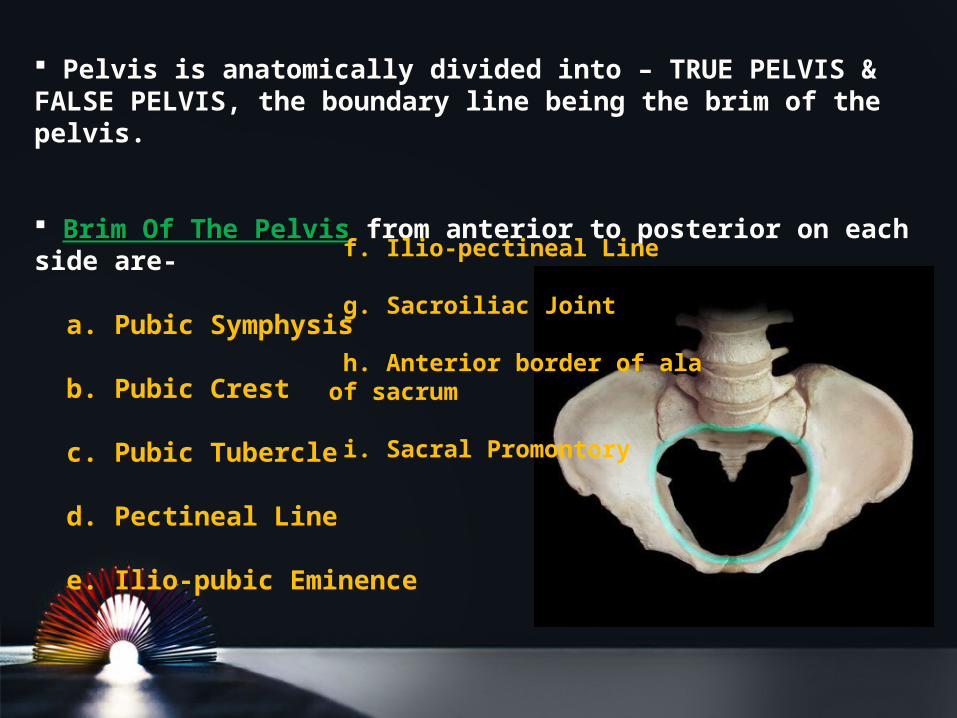
Pelvis is anatomically divided into – TRUE PELVIS & FALSE PELVIS, the boundary line being the brim of the pelvis.
Brim Of The PelvisBrim Of The Pelvis from anterior to posterior on each side are- a. Pubic Symphysis
b. Pubic Crest
c. Pubic Tubercle
d. Pectineal Line
e. Ilio-pubic Eminence
f. Ilio-pectineal Line
g. Sacroiliac Joint
h. Anterior border of ala of sacrum
i. Sacral Promontory
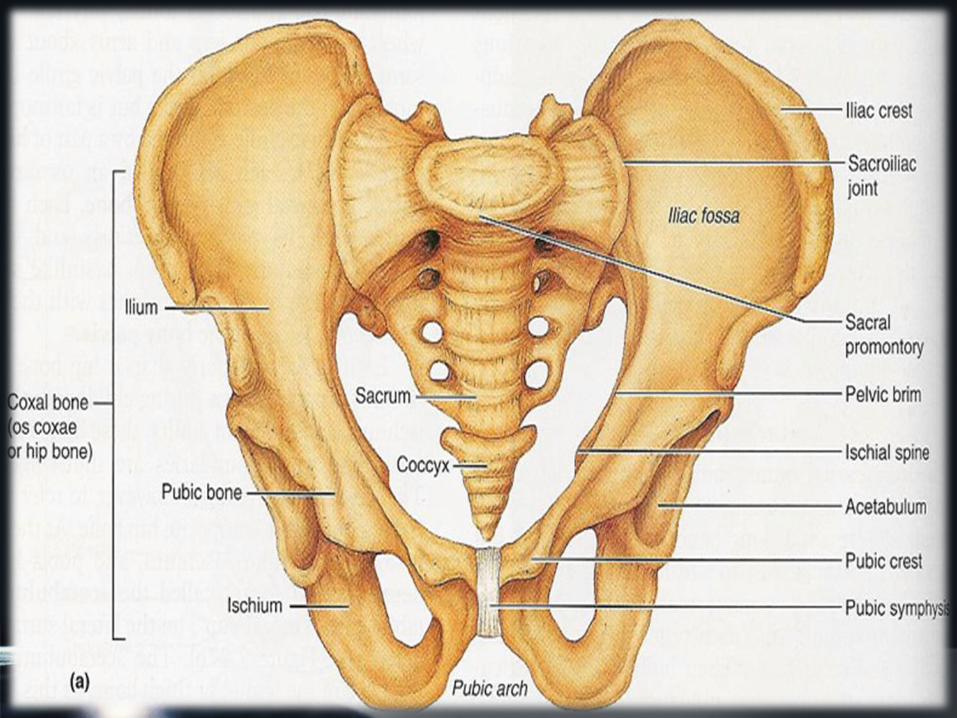
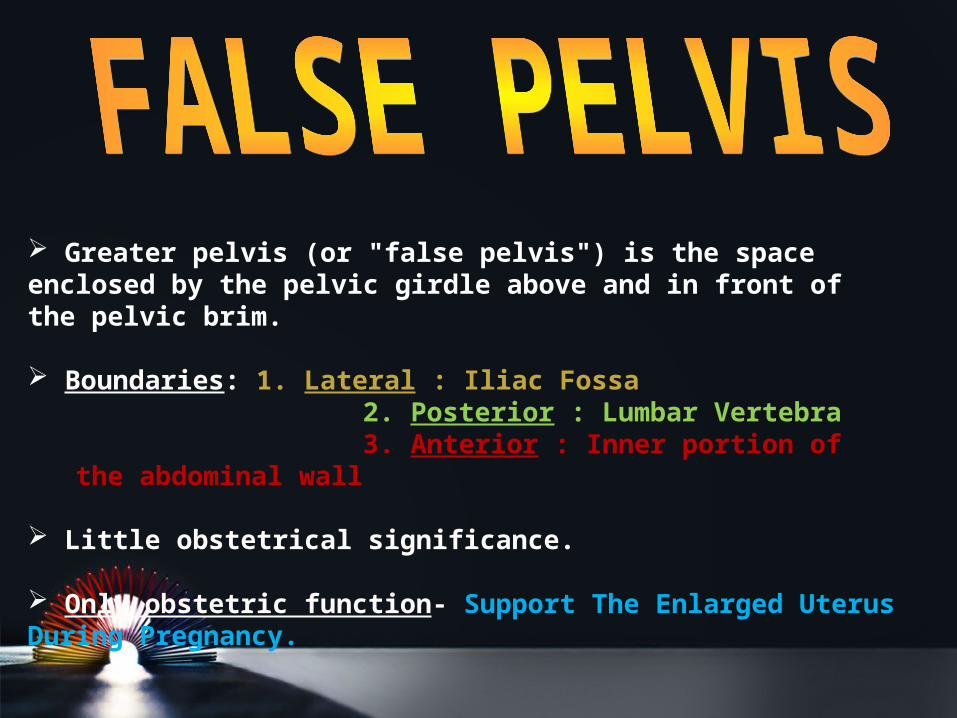
Greater pelvis (or "false pelvis") is the space enclosed by the pelvic girdle above and in front of the pelvic brim.
Boundaries: 1. Lateral : Iliac Fossa 2. Posterior : Lumbar Vertebra 3. Anterior : Inner portion of the abdominal wall
Little obstetrical significance.
Only obstetric function- Support The Enlarged Uterus During Pregnancy.
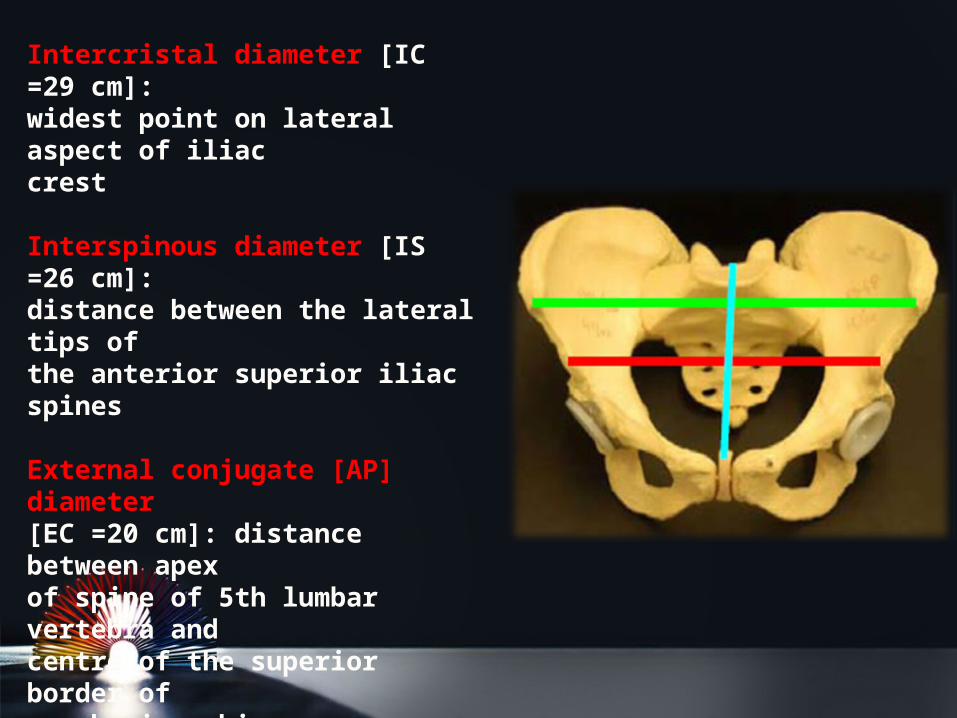
Intercristal diameter [IC =29 cm]:widest point on lateral aspect of iliaccrest
Interspinous diameter [IS =26 cm]:distance between the lateral tips ofthe anterior superior iliac spines
External conjugate [AP] diameter[EC =20 cm]: distance between apexof spine of 5th lumbar vertebra andcentre of the superior border ofsymphysis pubis.
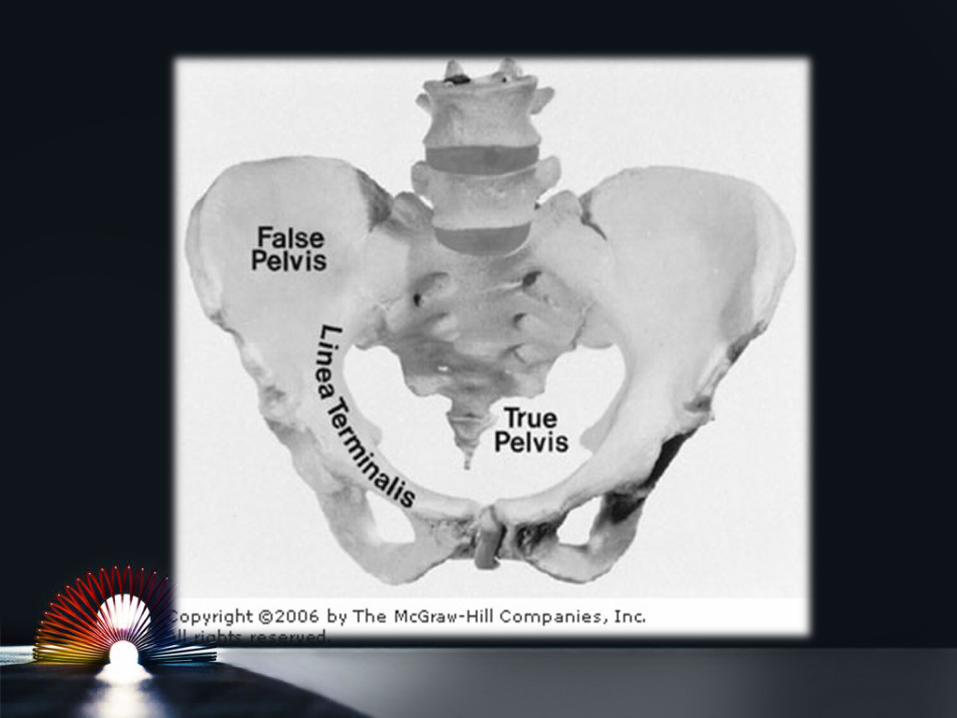
It is the obstetrically significant pelvis.
Forms the canal through which the fetus has to pass.
Bounded above by : Promontory And Alae Of The Sacrum
Linea Terminalis Upper Margins Of The Pubic Bones Bounded below by : Pelvic Outlet
Cavity is obliquely truncated, bent cylinder with anterior wall measuring 5 cm, and posterior wall is about 10 cm
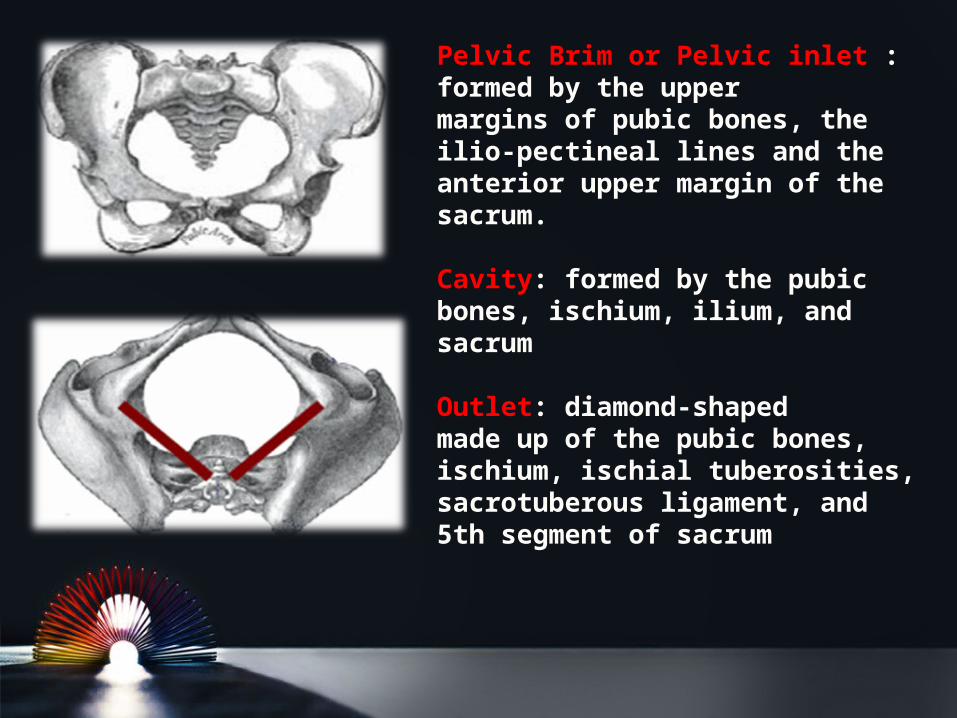
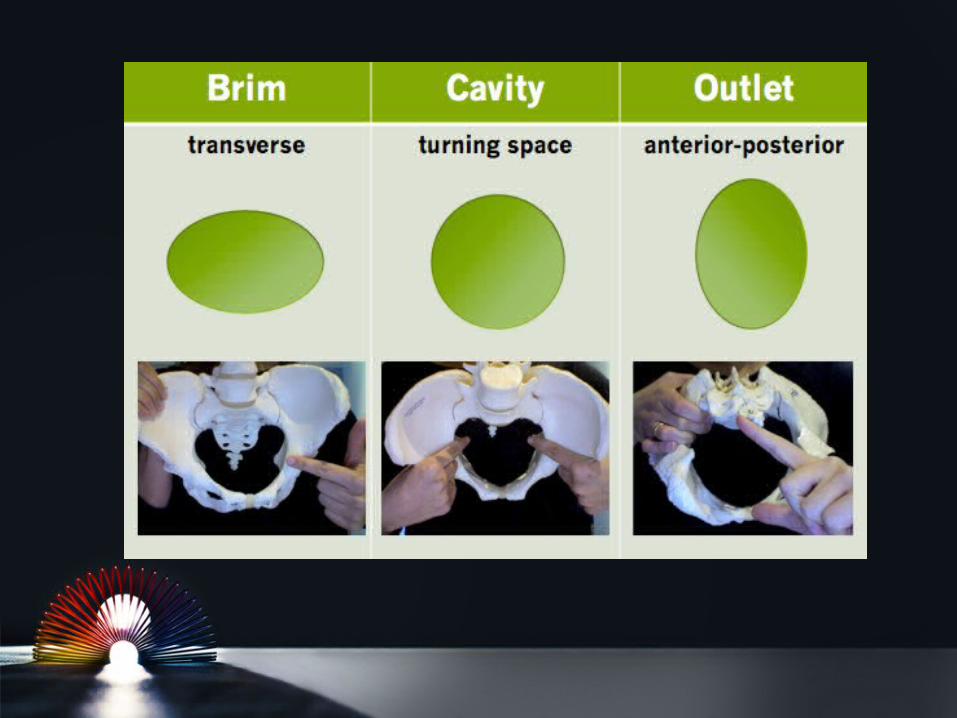
Pelvic Brim or Pelvic inlet : formed by the uppermargins of pubic bones, theilio-pectineal lines and theanterior upper margin of thesacrum.
Cavity: formed by the pubicbones, ischium, ilium, andsacrum
Outlet: diamond-shapedmade up of the pubic bones,ischium, ischial tuberosities,sacrotuberous ligament, and5th segment of sacrum
Four Imaginary Planes
1.Plane of the pelvic inlet— The Superior Strait
2.Plane of the pelvic outlet— The Inferior Strait
3.Plane of the midpelvis— The Least Pelvic Dimension
4.Plane of greatest pelvic dimension— No obstetrical significance
BoundariesBoundaries•Sacral Promontory
•Alae Of The Sacrum
•Sacroiliac Joints
•Iliopectineal Lines
•Iliopectineal Eminencies
•Upper Border Of The Superior Pubic Rami
•Pubic Tubercles
•Pubic Crests
•Upper Border Of Symphysis Pubis.
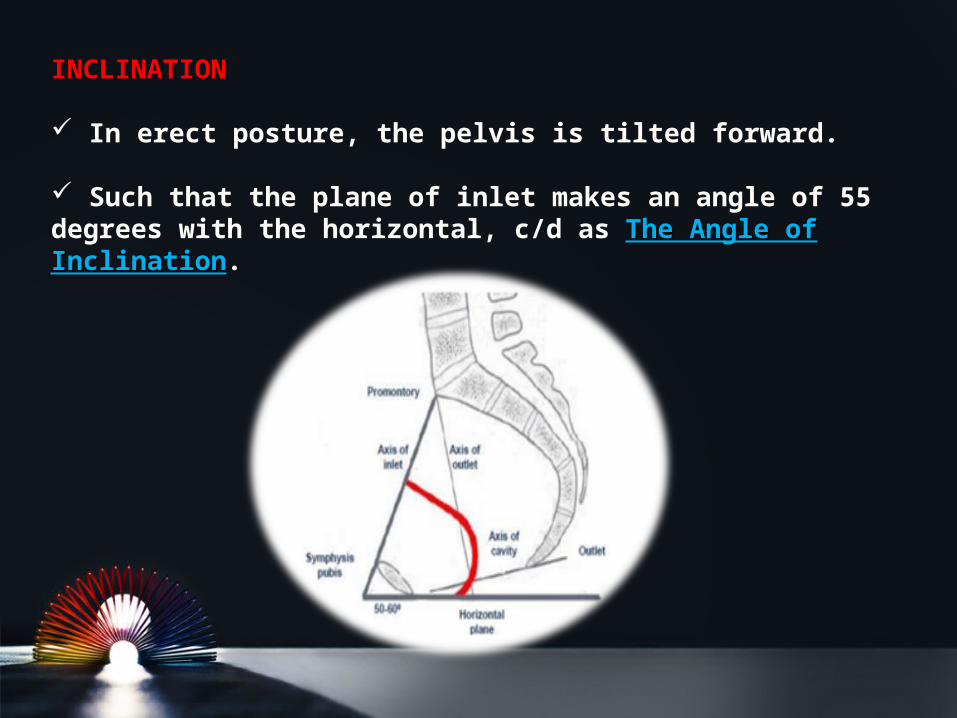
INCLINATIONINCLINATION
In erect posture, the pelvis is tilted forward.
Such that the plane of inlet makes an angle of 55 degrees with the horizontal, c/d as The Angle of The Angle of InclinationInclination.
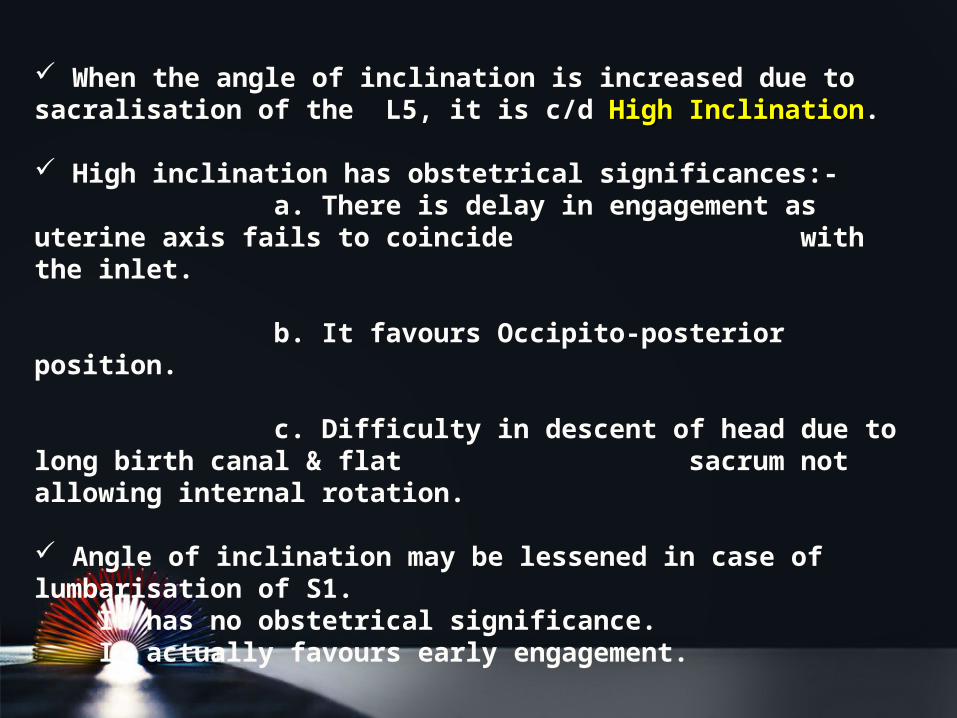
When the angle of inclination is increased due to sacralisation of the L5, it is c/d High InclinationHigh Inclination.
High inclination has obstetrical significances:- a. There is delay in engagement as uterine axis fails to coincide with the inlet. b. It favours Occipito-posterior position. c. Difficulty in descent of head due to long birth canal & flat sacrum not allowing internal rotation.
Angle of inclination may be lessened in case of lumbarisation of S1. It has no obstetrical significance. It actually favours early engagement.
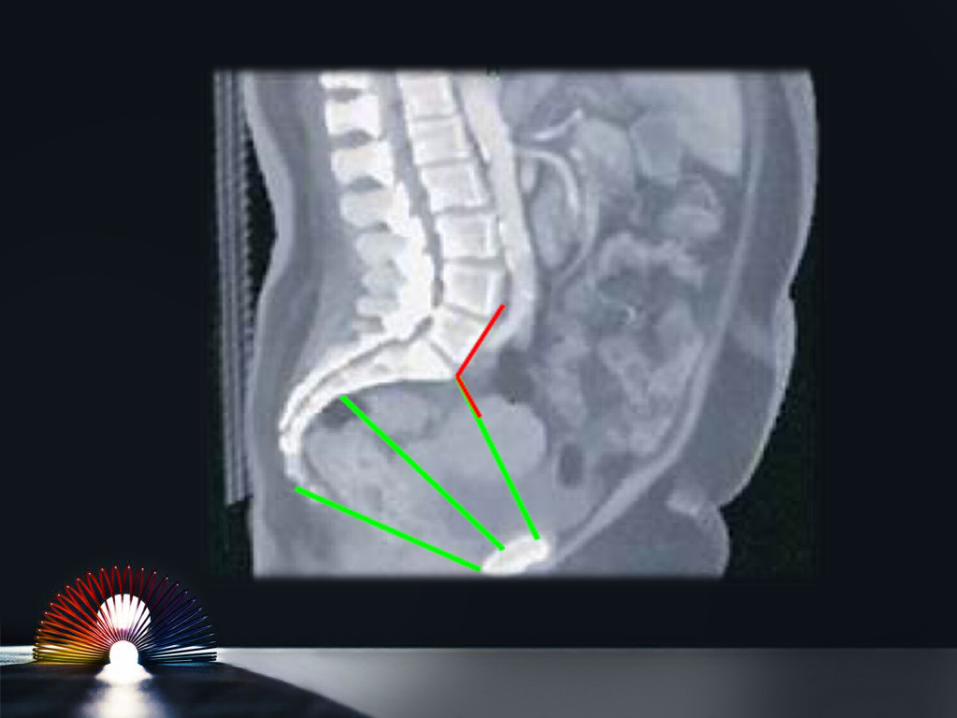
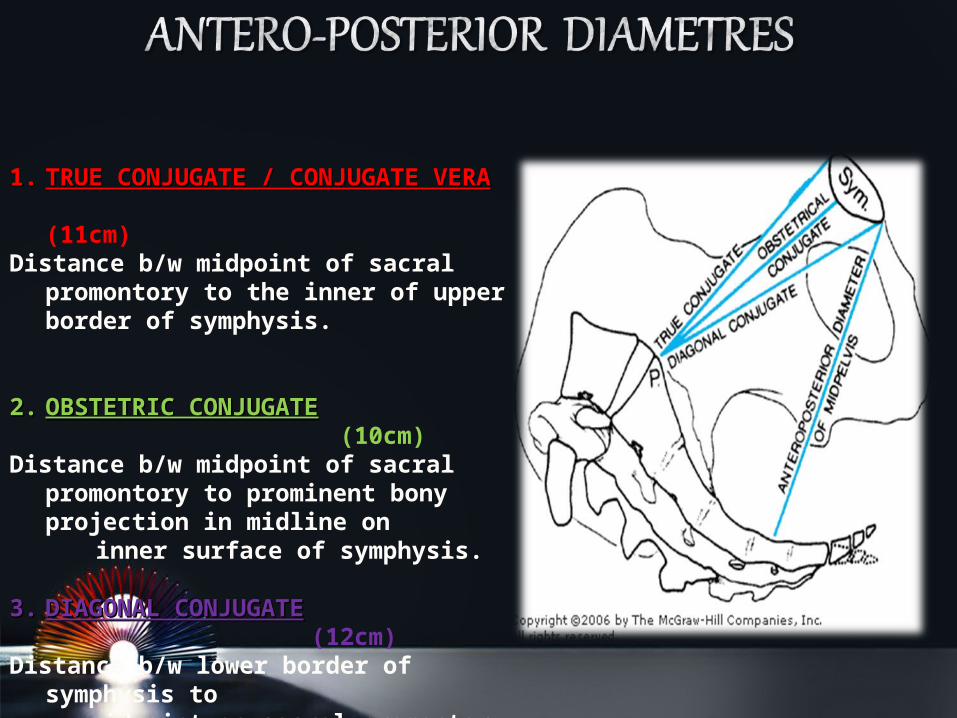
1.1. TRUE CONJUGATE / CONJUGATE VERATRUE CONJUGATE / CONJUGATE VERA (11cm)Distance b/w midpoint of sacral
promontory to the inner of upper border of symphysis.
2.2. OBSTETRIC CONJUGATEOBSTETRIC CONJUGATE (10cm)Distance b/w midpoint of sacral
promontory to prominent bony projection in midline on
inner surface of symphysis.
3.3. DIAGONAL CONJUGATEDIAGONAL CONJUGATE (12cm)Distance b/w lower border of
symphysis to midpoint on sacral promontory
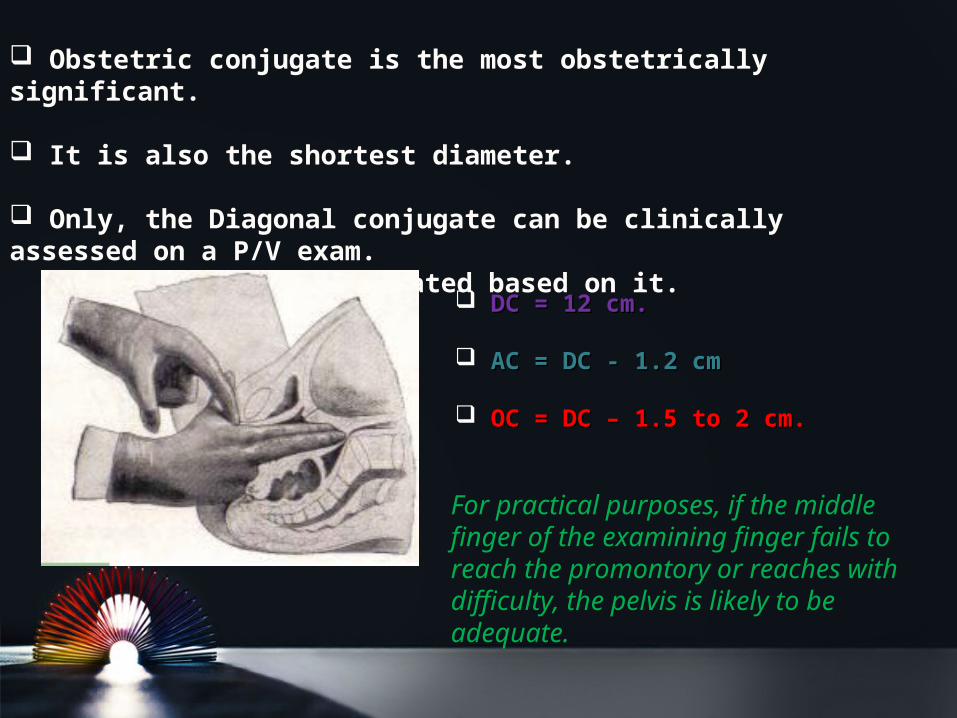
Obstetric conjugate is the most obstetrically significant.
It is also the shortest diameter.
Only, the Diagonal conjugate can be clinically assessed on a P/V exam. Remaining are calculated based on it.
DC = 12 cm.DC = 12 cm.
AC = DC - 1.2 cmAC = DC - 1.2 cm
OC = DC – 1.5 to 2 cm.OC = DC – 1.5 to 2 cm.
For practical purposes, if the middle finger of the examining finger fails to reach the promontory or reaches with difficulty, the pelvis is likely to be adequate.
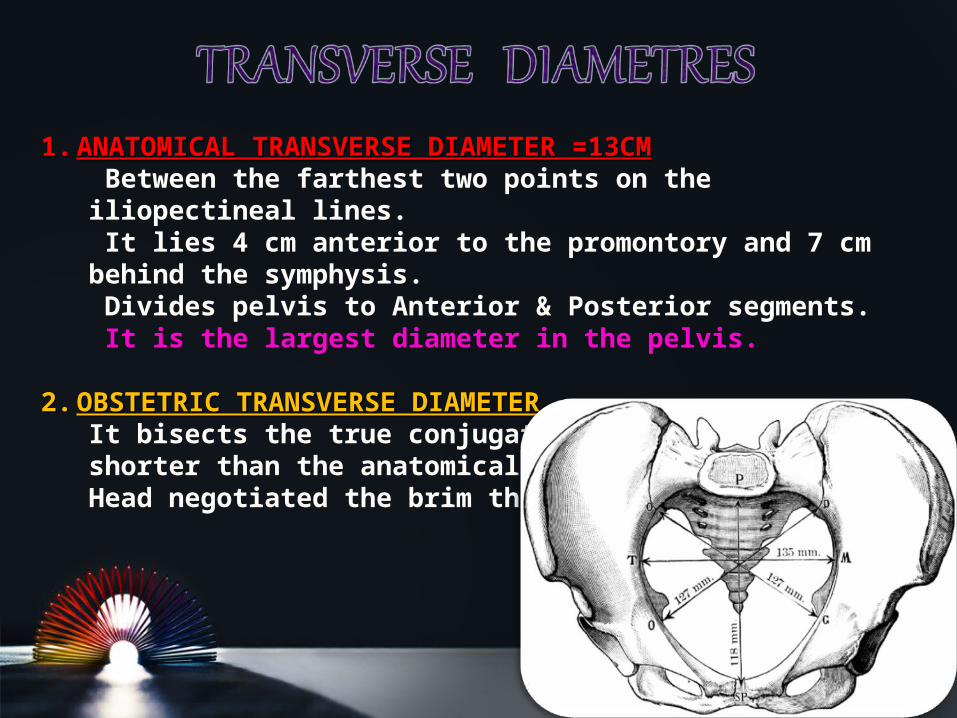
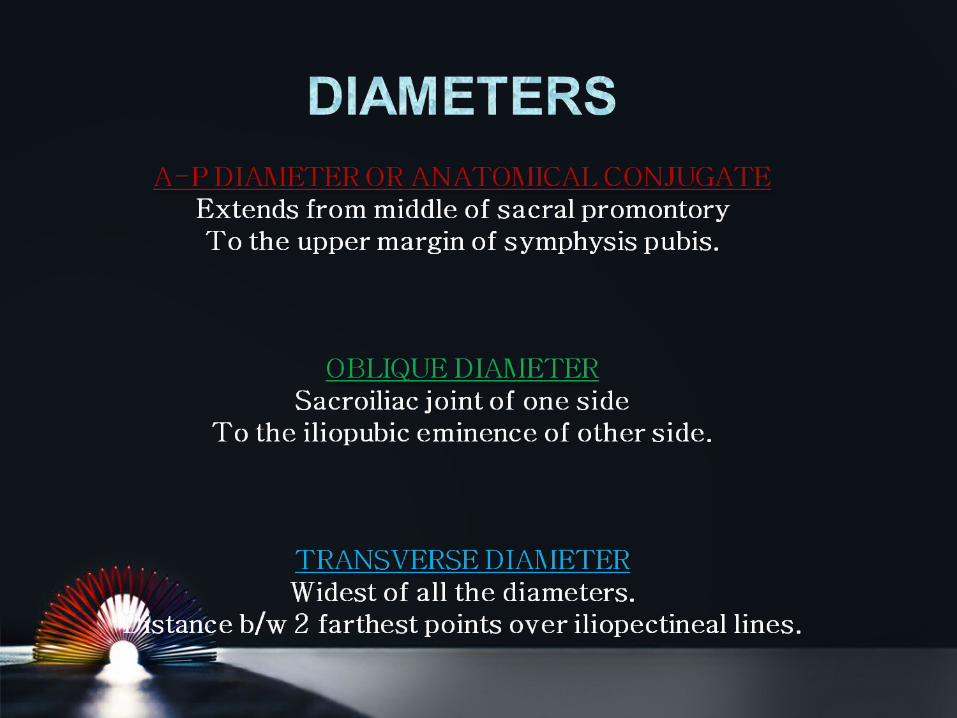
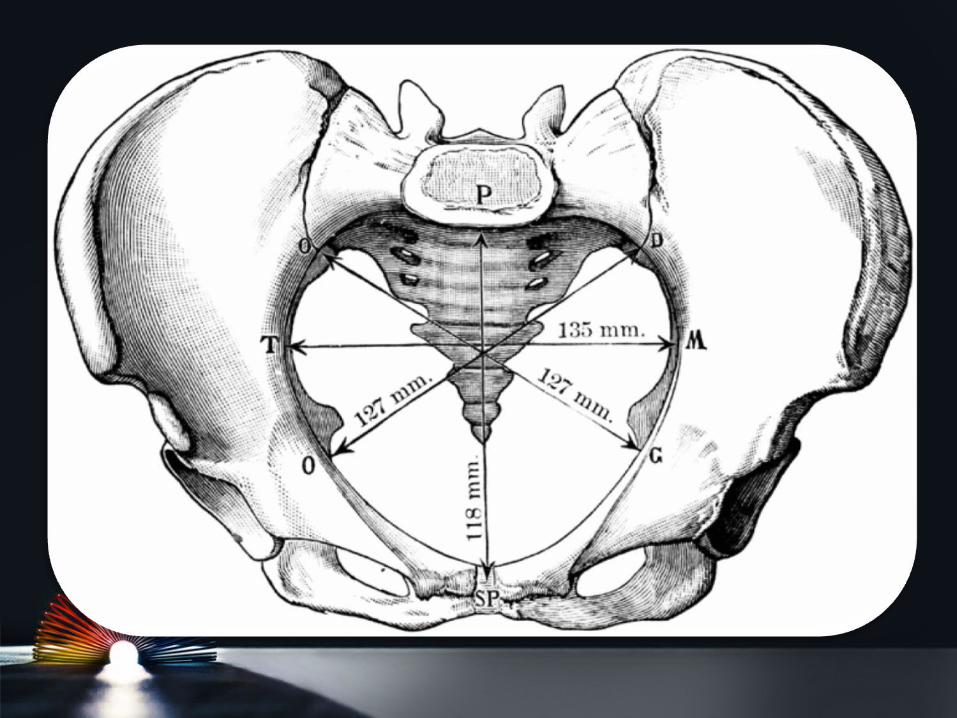
1.1. ANATOMICAL TRANSVERSE DIAMETER =13CMANATOMICAL TRANSVERSE DIAMETER =13CM Between the farthest two points on the iliopectineal lines. It lies 4 cm anterior to the promontory and 7 cm behind the symphysis. Divides pelvis to Anterior & Posterior segments. It is the largest diameter in the pelvis.
2.2. OBSTETRIC TRANSVERSE DIAMETEROBSTETRIC TRANSVERSE DIAMETERIt bisects the true conjugate and is slightly shorter than the anatomical transverse diameter.Head negotiated the brim through it.
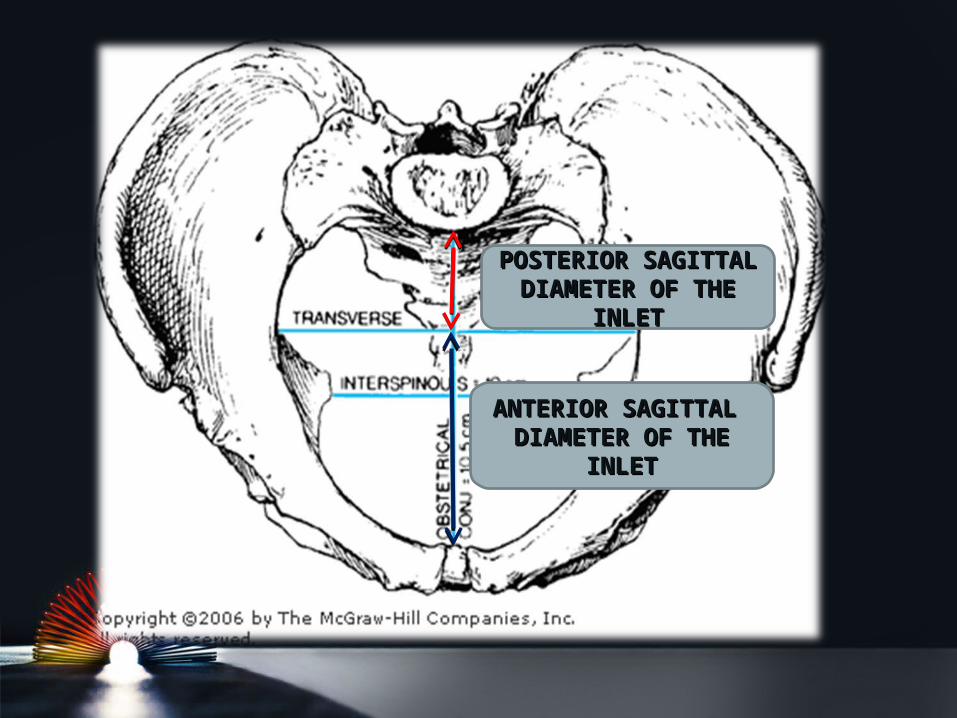
POSTERIOR POSTERIOR SAGITTAL SAGITTAL
DIAMETER OF THE DIAMETER OF THE INLETINLET
ANTERIOR SAGITTAL ANTERIOR SAGITTAL DIAMETER OF THE DIAMETER OF THE
INLETINLET
a. RIGHT OBLIQUE DIAMETER =12 CMRIGHT OBLIQUE DIAMETER =12 CMfrom the right sacroiliac joint to the left iliopubic eminence.
b. LEFT OBLIQUE DIAMETER = 12 CMLEFT OBLIQUE DIAMETER = 12 CMfrom the left sacroiliac joint to the right iliopubic eminence.
c. SACRO-COTYLOID DIAMETERS = 9-9.5 CMSACRO-COTYLOID DIAMETERS = 9-9.5 CMfrom the promontory of the sacrum to the right and left iliopectineal eminence, so the right diameter ends at the right eminence and vice versa.
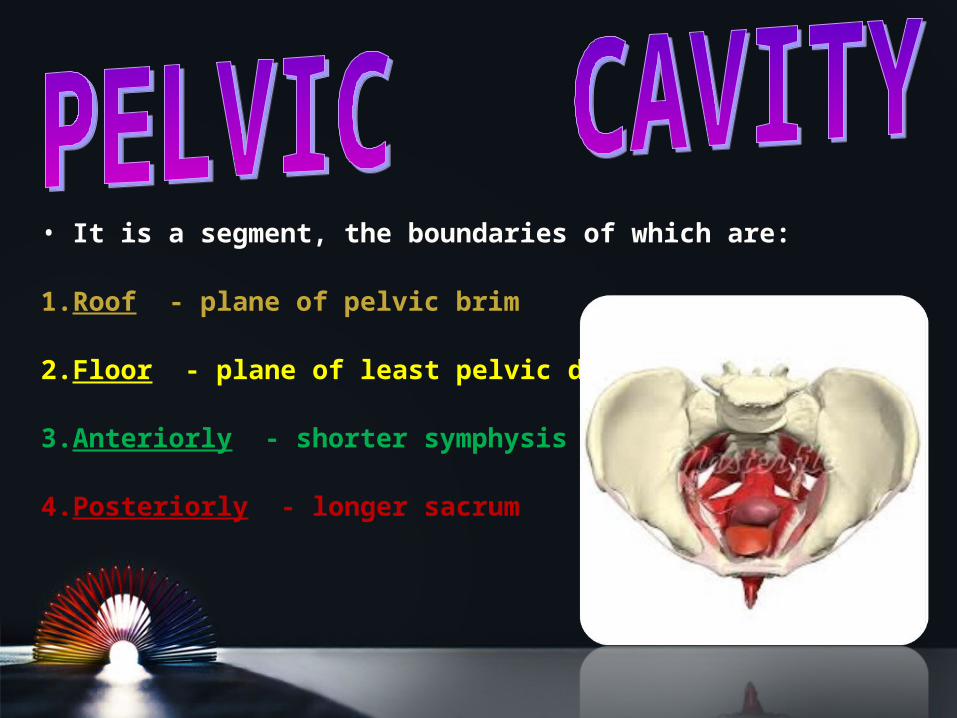
• It is a segment, the boundaries of which are:
1.Roof - plane of pelvic brim
2.Floor - plane of least pelvic dimension
3.Anteriorly - shorter symphysis pubis
4.Posteriorly - longer sacrum
Anterior posterior diameter:From midpoint on posterior surface of symphysis pubis to junction of S2 and S3.
Oblique diameter:Lower end of sacroiliac joint to the centre of obturator membrane.
Transverse diameter:Across the lateral bony walls of pelvic cavity.Cant be accurately measured.
ANATOMICAL OUTLETIt is lozenge-shaped bounded by:-
Front - lower border of symphysis pubis & pubic arch Laterally - ischial tuberosities, sacrotuberous and sacrospinous ligaments
Posterior - tip of the coccyx.
OBSTETRIC OUTLETIt is a segment, the boundaries of which are: Roof - plane of least pelvic dimension Floor - anatomical outlet Anteriorly - lower border of
symphysis pubis
Posteriorly - Saccrum.
Laterally - ischial spines.
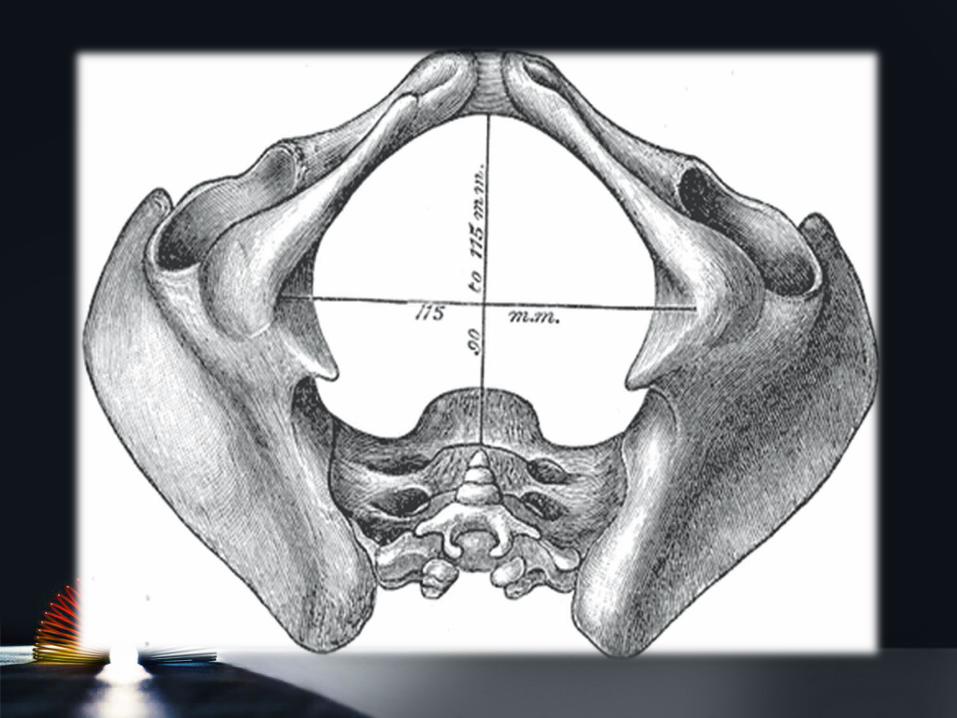
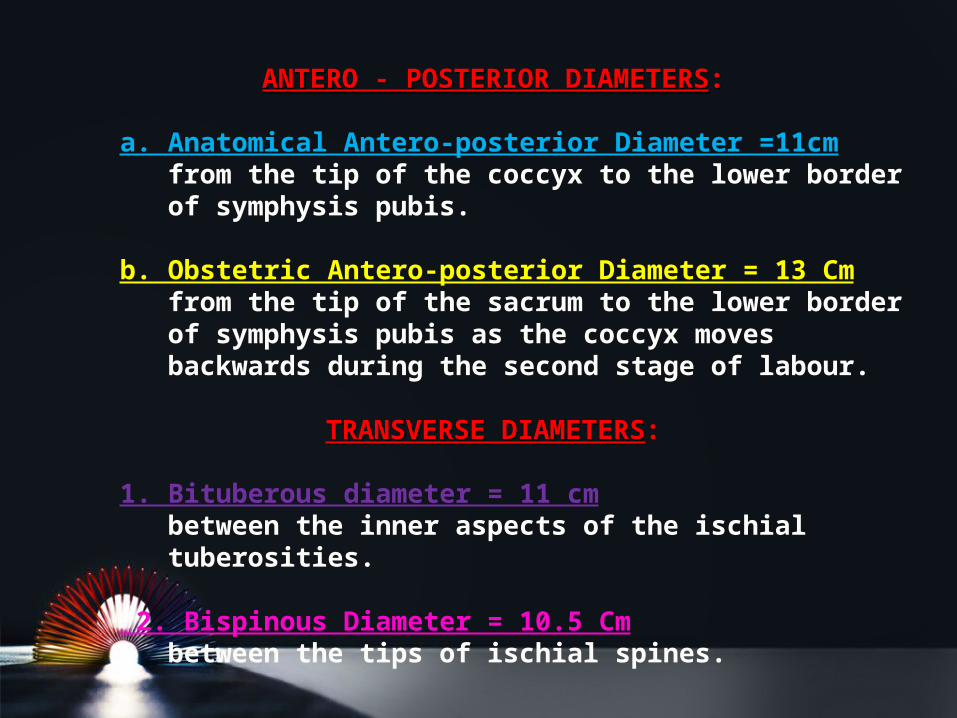
ANTERO - POSTERIOR DIAMETERSANTERO - POSTERIOR DIAMETERS::
a. Anatomical Antero-posterior Diameter =11cmfrom the tip of the coccyx to the lower border of symphysis pubis.
b. Obstetric Antero-posterior Diameter = 13 Cmfrom the tip of the sacrum to the lower border of symphysis pubis as the coccyx moves backwards during the second stage of labour.
TRANSVERSE DIAMETERSTRANSVERSE DIAMETERS:
1. Bituberous diameter = 11 cmbetween the inner aspects of the ischial tuberosities.
2. Bispinous Diameter = 10.5 Cmbetween the tips of ischial spines.
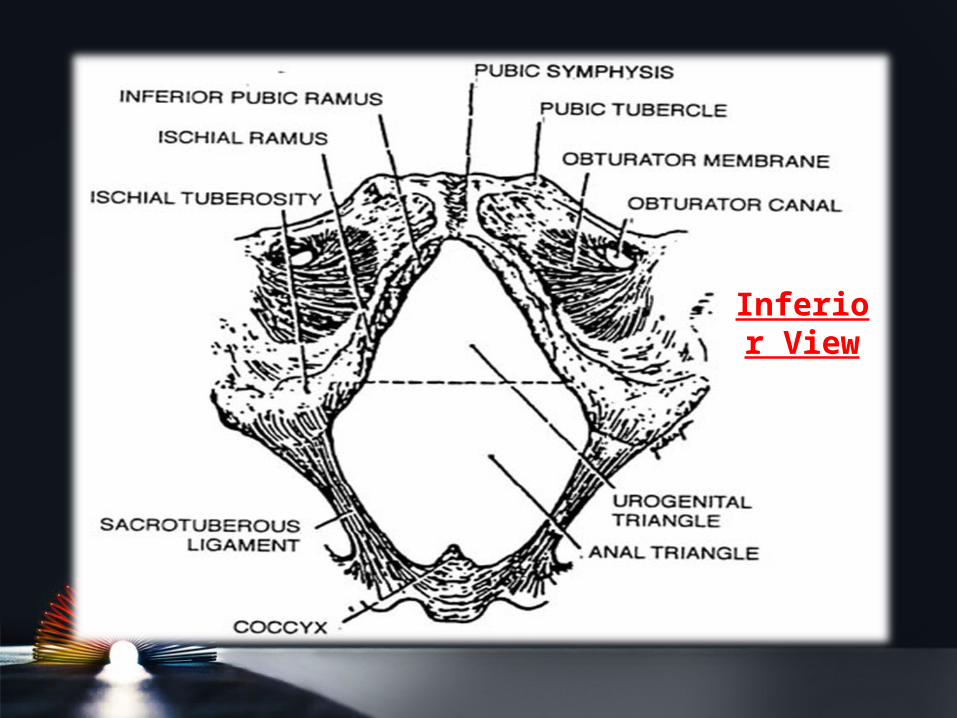
Inferior View
OBSTETRIC AXIS
It is an imaginary line representing the way passed by the head during labour.
It is J shaped
Passes downwards and backwards along the axis of the inlet till the ischial spines where it passes downwards and forwards along the axis of the pelvic outlet.
ANATOMICAL DEFINITION It is a pelvis in which one or more of its diameters is reduced below the normal by one or more centimeters.
OBSTETRIC DEFINITIONIt is a pelvis in which one or more of its diameters is reduced so that it interferes with the normal mechanism of labour.
HISTORY
* Rickets: is expected if there is a history of delayed walking and dentition.
* Trauma or diseases: of the pelvis, spines or lower limbs.
* Bad obstetric history: e.g. prolonged labour ended by;
• difficult forceps,• caesarean section or• still birth.
PRELIMINARY DIAGNOSISPRELIMINARY DIAGNOSIS
EXAMINATION
General examination
1.Gait: abnormal gait suggesting abnormalities in the pelvis, spines or lower limbs.
2. Stature: women with less than 5feet height / shoe size less than 4 usually have contracted pelvis.
3. Spines and lower limbs: may have a disease or lesion.
4. Manifestations of rickets * Square head * Rosary beads in the costal ridges * Pigeon chest * Harrison’s sulcus & Bow legs
5. Dystocia dystrophia syndrome: the woman is * Short * Stocky * Subfertile * Android pelvis * Masculine hair distribution * History of delayed menarche. * More exposed to occipito-posterior position and dystocia.
ABDOMINAL EXAMINATION
Nonengagement of the head - in the last 3-4 weeks in primigravida.
Pendulous abdomen - in a primigravida.
Malpresentations - are more common.
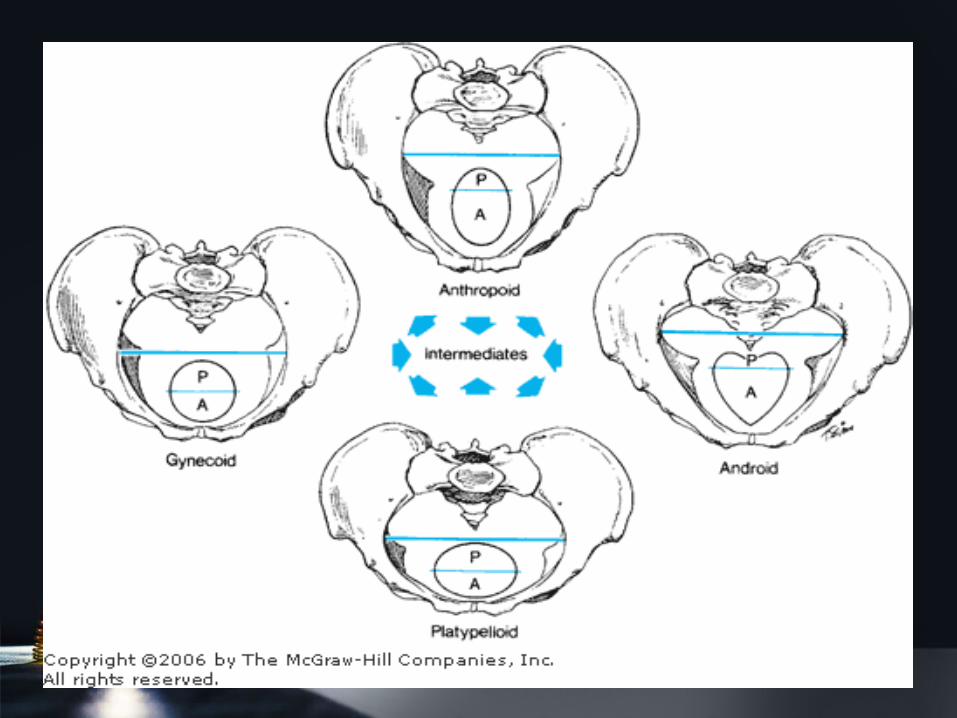
CALDWELL AND MOLOY CLASSIFICATIONCALDWELL AND MOLOY CLASSIFICATION
• Divided pelvis into anterior and posterior segments based on the greatest transverse diameters of the inlet.
• Posterior segment determines the type of pelvis.
• Anterior segment determines the tendency.
• Many pelvis are not pure but of mixed types. Eg. A gynaecoid pelvis with an android tendency
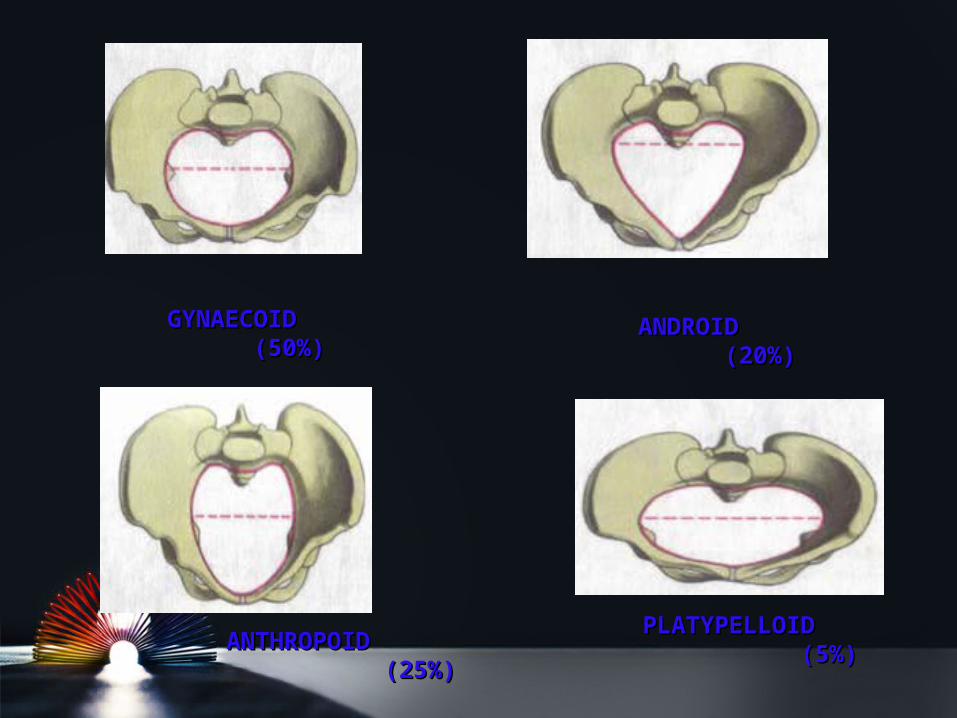
GYNAECOIDGYNAECOID (50%)(50%)
ANTHROPOIDANTHROPOID (25%)(25%)
ANDROIDANDROID (20%)(20%)
PLATYPELLOIDPLATYPELLOID (5%)(5%)
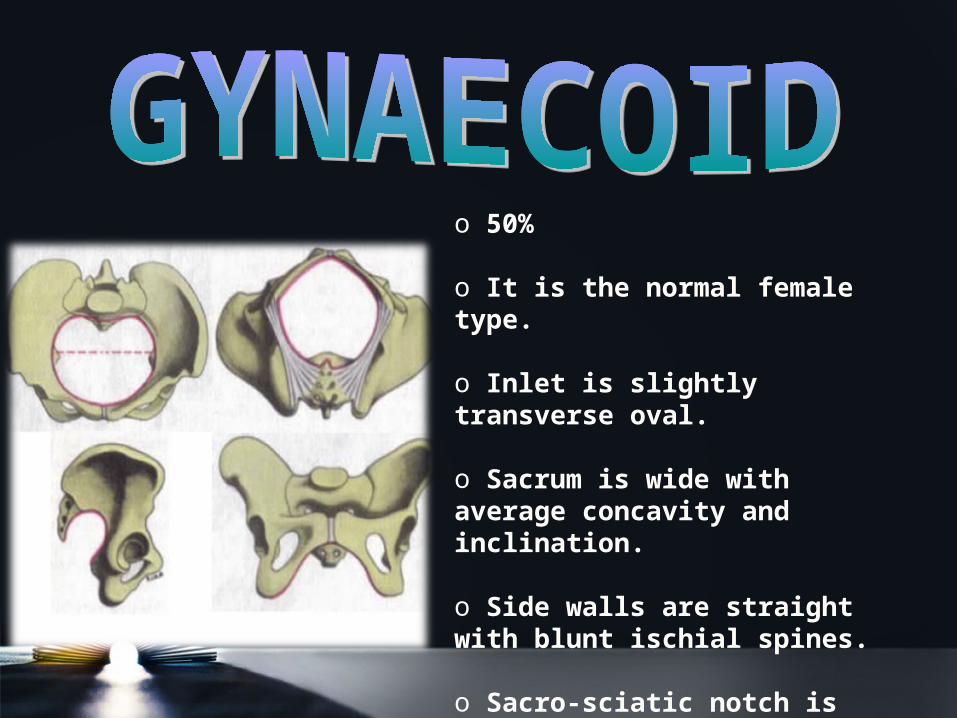
o 50%
o It is the normal female type.
o Inlet is slightly transverse oval.
o Sacrum is wide with average concavity and inclination.
o Side walls are straight with blunt ischial spines.
o Sacro-sciatic notch is wide.
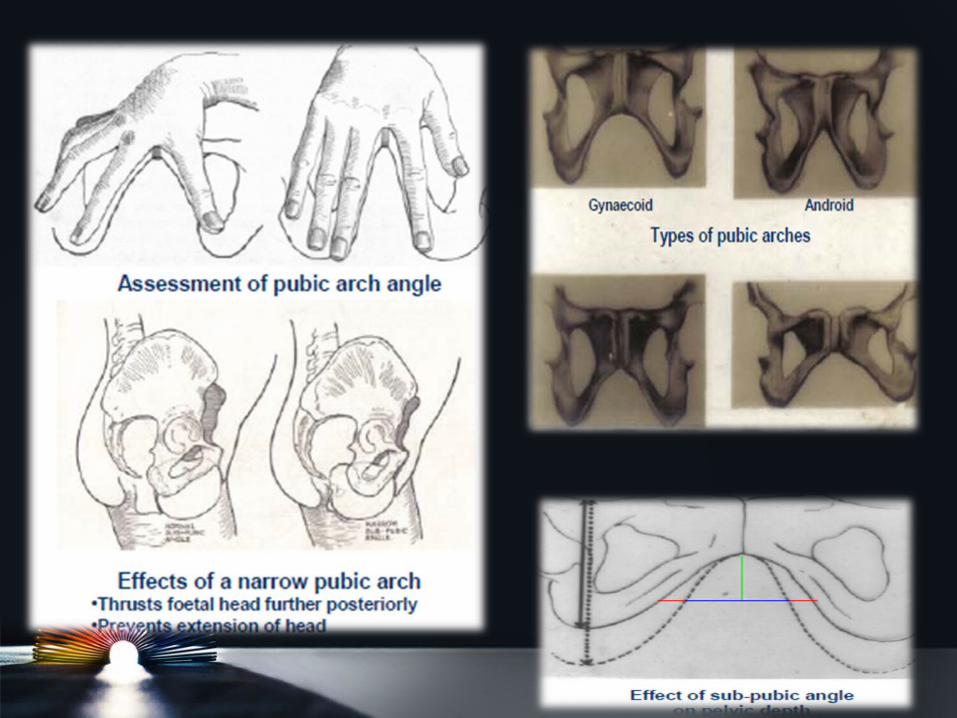
o Sub pubic angle is 90-100 degrees.
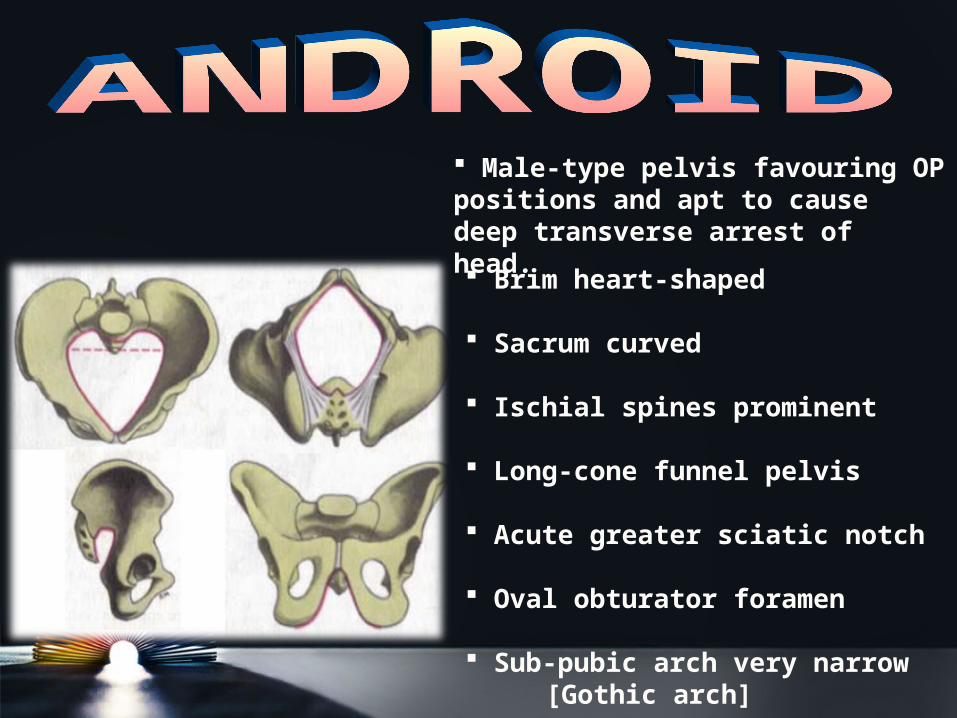
Male-type pelvis favouring OP positions and apt to cause deep transverse arrest of head.
Brim heart-shaped
Sacrum curved
Ischial spines prominent
Long-cone funnel pelvis
Acute greater sciatic notch
Oval obturator foramen
Sub-pubic arch very narrow [Gothic arch]
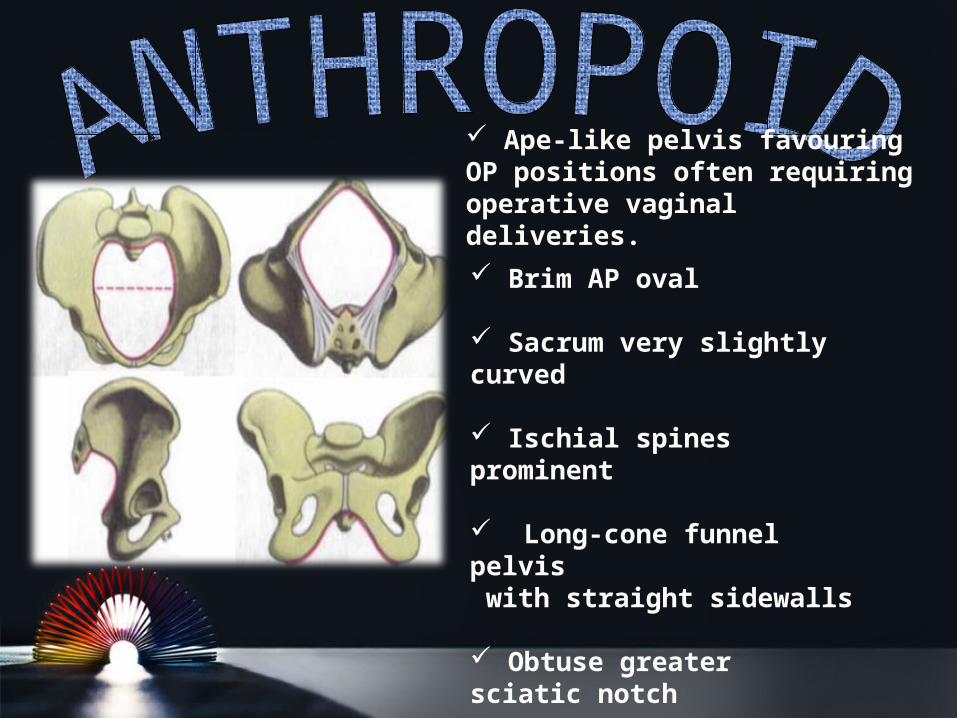
Ape-like pelvis favouring OP positions often requiring operative vaginaldeliveries. Brim AP oval Sacrum very slightly curved
Ischial spines prominent
Long-cone funnel pelvis with straight sidewalls Obtuse greater sciatic notch
Oval obturator foramen
Sub-pubic arch narrow
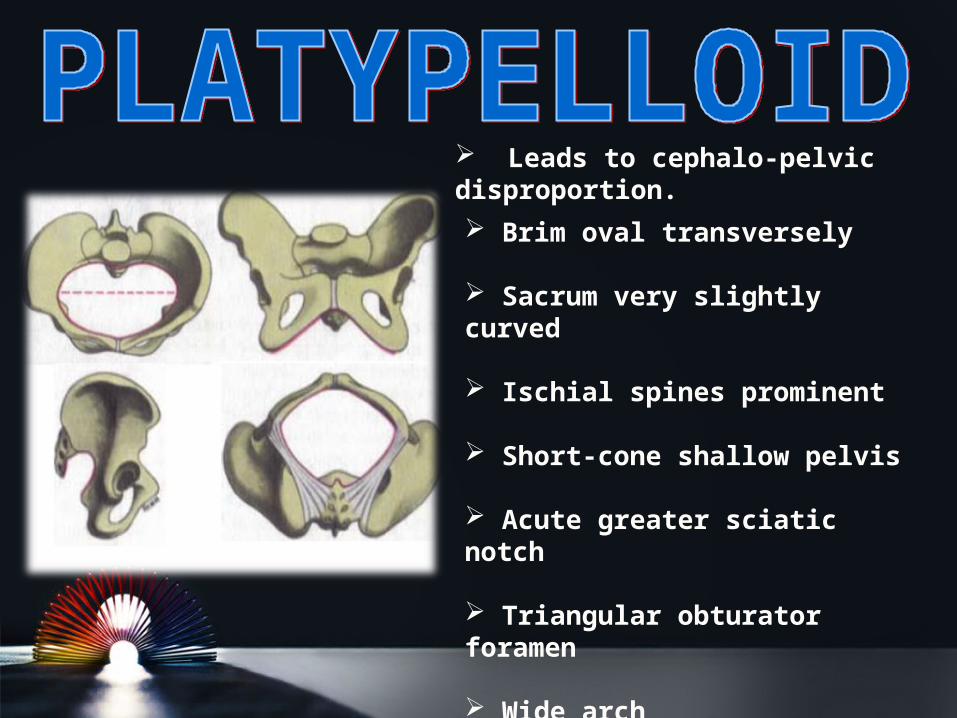
Brim oval transversely
Sacrum very slightly curved
Ischial spines prominent
Short-cone shallow pelvis
Acute greater sciatic notch
Triangular obturator foramen
Wide arch
Leads to cephalo-pelvic disproportion.
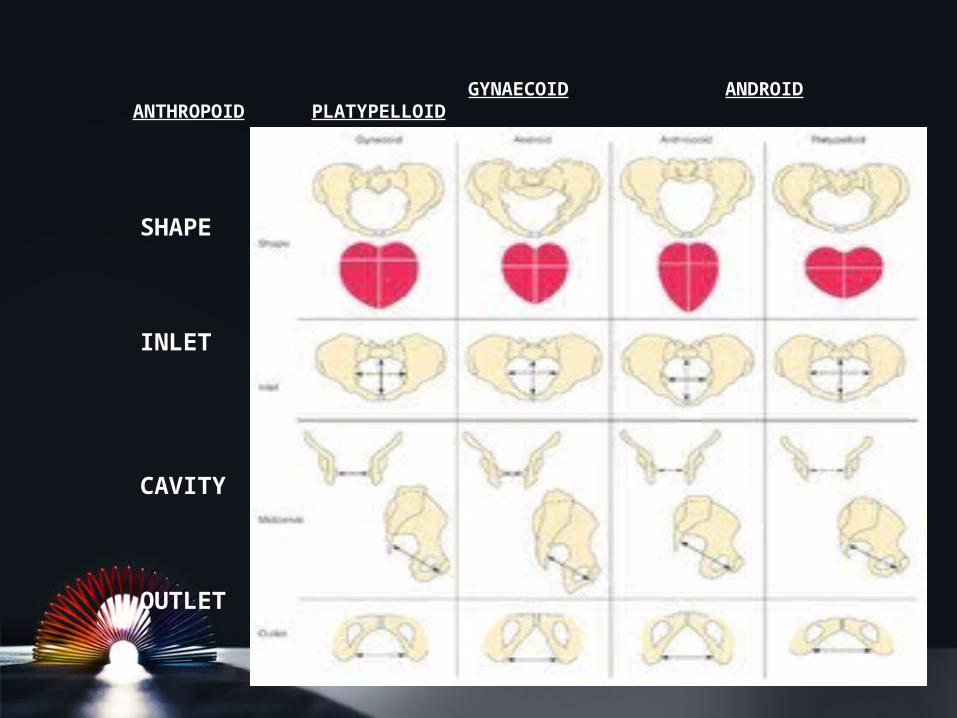
GYNAECOID ANDROID ANTHROPOID PLATYPELLOID
SHAPE
INLET
CAVITY
OUTLET
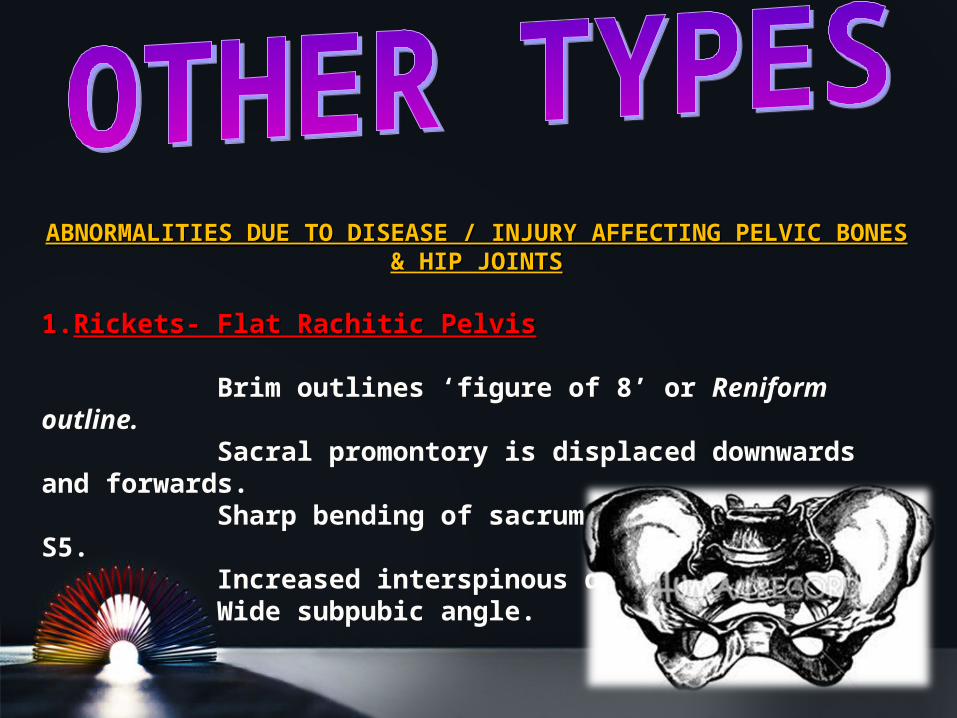
ABNORMALITIES DUE TO DISEASE / INJURY AFFECTING PELVIC ABNORMALITIES DUE TO DISEASE / INJURY AFFECTING PELVIC BONES & HIP JOINTSBONES & HIP JOINTS
1.1.Rickets- Flat Rachitic PelvisRickets- Flat Rachitic Pelvis Brim outlines ‘figure of 8’ or Reniform outline. Sacral promontory is displaced downwards and forwards. Sharp bending of sacrum at level of S4 and S5. Increased interspinous diameter. Wide subpubic angle.
2. 2. Scolio-rachitic PelvisScolio-rachitic Pelvis If there is, any marked lateral spinal curvature, it
produces such a pelvis.
3.3. Osteomalacia Pelvis = Beaked pelvis = Rostrate = Osteomalacia Pelvis = Beaked pelvis = Rostrate = TriradiateTriradiate
Commonly found in women abiding by the Purdah System.
Promontory pushed downwards & forwards. Lateral pelvic walls pushed inwards. Anterior wall pushed forwards to form a beak. Brim assumes ‘trifoliate’ shape. Sub pubic angle narrowed. Swinging gait.
3.3. PolioPolio
4.4. Changes with postureChanges with posture
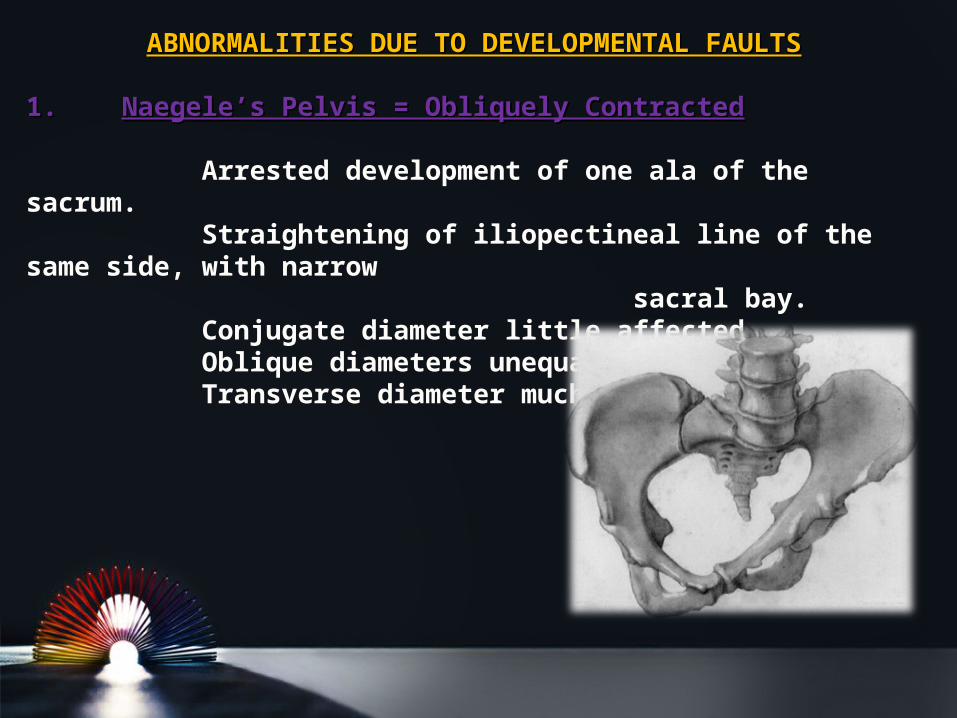
ABNORMALITIES DUE TO DEVELOPMENTAL FAULTSABNORMALITIES DUE TO DEVELOPMENTAL FAULTS
1.1. Naegele’s Pelvis = Obliquely ContractedNaegele’s Pelvis = Obliquely Contracted Arrested development of one ala of the sacrum. Straightening of iliopectineal line of the same side, with narrow sacral bay. Conjugate diameter little affected. Oblique diameters unequal. Transverse diameter much reduced.
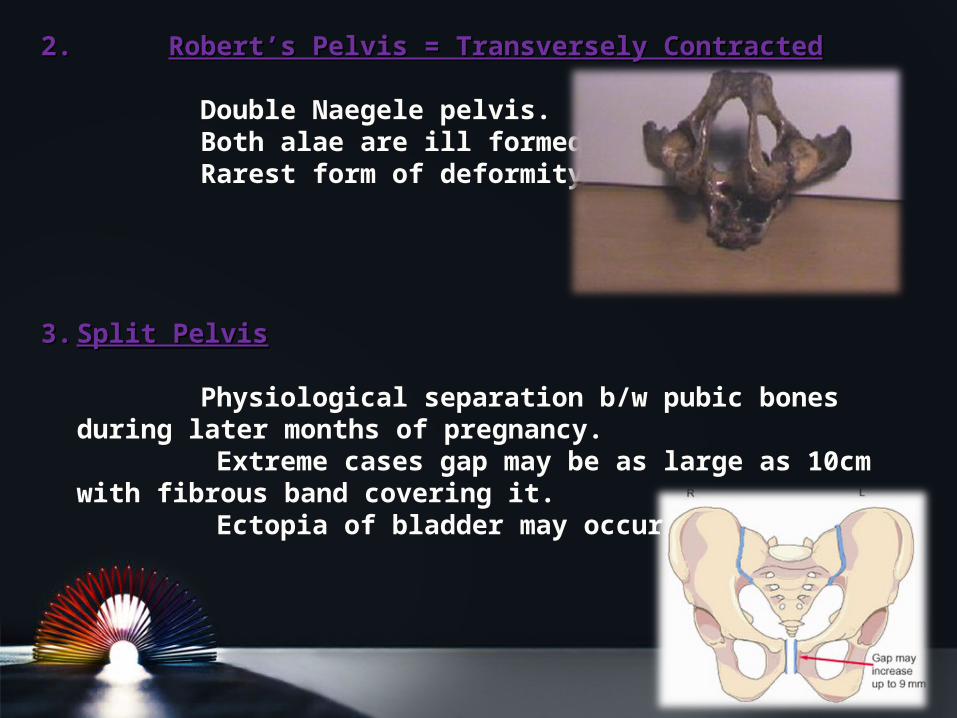
2. 2. Robert’s Pelvis = Transversely ContractedRobert’s Pelvis = Transversely Contracted Double Naegele pelvis. Both alae are ill formed. Rarest form of deformity.
3.3. Split PelvisSplit Pelvis Physiological separation b/w pubic bones during
later months of pregnancy. Extreme cases gap may be as large as 10cm with
fibrous band covering it. Ectopia of bladder may occur.
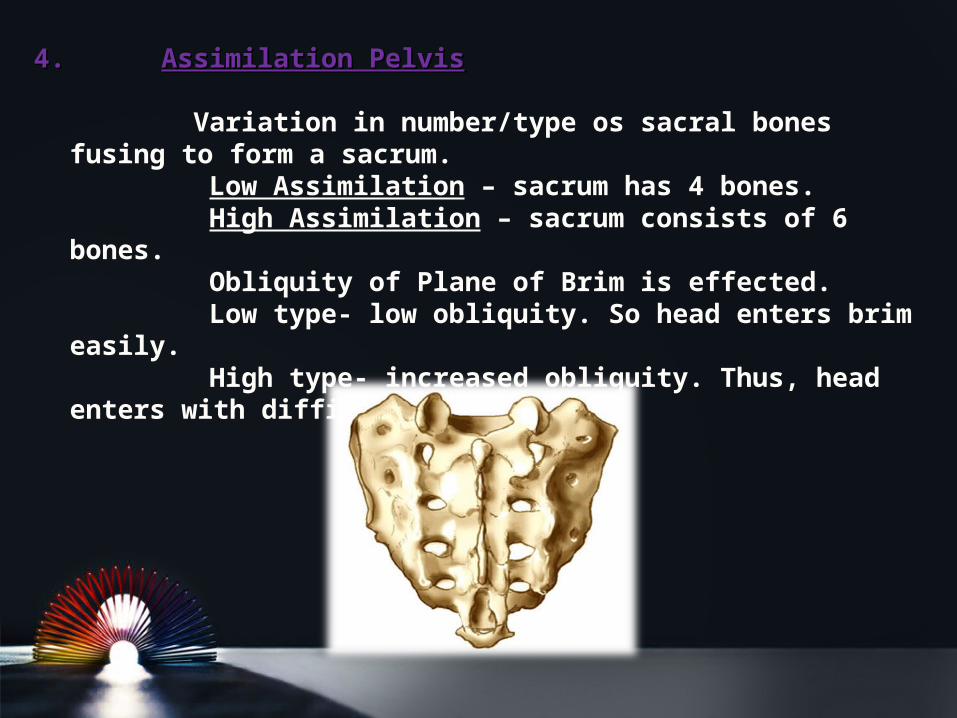
4. 4. Assimilation PelvisAssimilation Pelvis Variation in number/type os sacral bones fusing to
form a sacrum. Low Assimilation – sacrum has 4 bones. High Assimilation – sacrum consists of 6 bones. Obliquity of Plane of Brim is effected. Low type- low obliquity. So head enters brim easily. High type- increased obliquity. Thus, head enters
with difficulty.
ABNORMALITIES OF THE VERTEBRAL COLUMNABNORMALITIES OF THE VERTEBRAL COLUMN
a)a)KyphosisKyphosisb)b)ScoliosisScoliosisc)c)SpondylolisthesisSpondylolisthesisd)d)Coccygeal deformity.Coccygeal deformity.
ABNORMALITIES OF DISEASE OR DEFORMITY OF LOWER ABNORMALITIES OF DISEASE OR DEFORMITY OF LOWER LIMBLIMB
1)1)Hip joint disease.Hip joint disease.2)2)Dislocation of femur.Dislocation of femur.3)3)Atrophy or limb loss.Atrophy or limb loss.
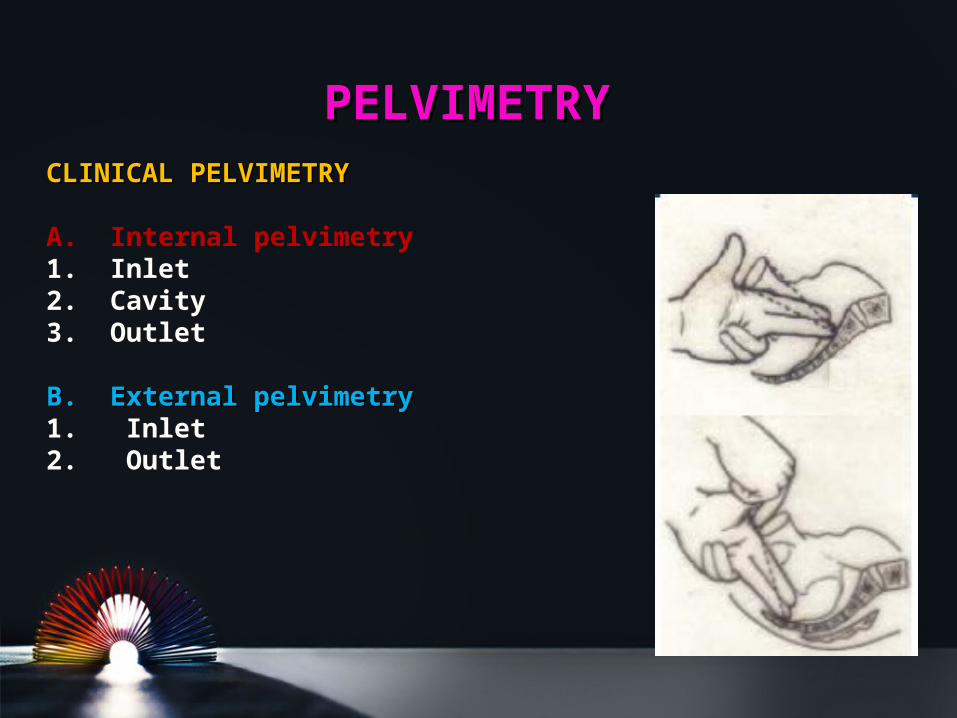
PELVIMETRYPELVIMETRYCLINICAL PELVIMETRYCLINICAL PELVIMETRY
A. Internal pelvimetry 1. Inlet2. Cavity3. Outlet
B. External pelvimetryB. External pelvimetry1. Inlet 2. Outlet
IMAGING PELVIMETRYIMAGING PELVIMETRY
a) X-ray.
b) Computed Tomography (CT).
c) Magnetic Resonance Imaging (MRI) .
CT and MRI are recent and accurate but expensive and not always available so they are not in common use.
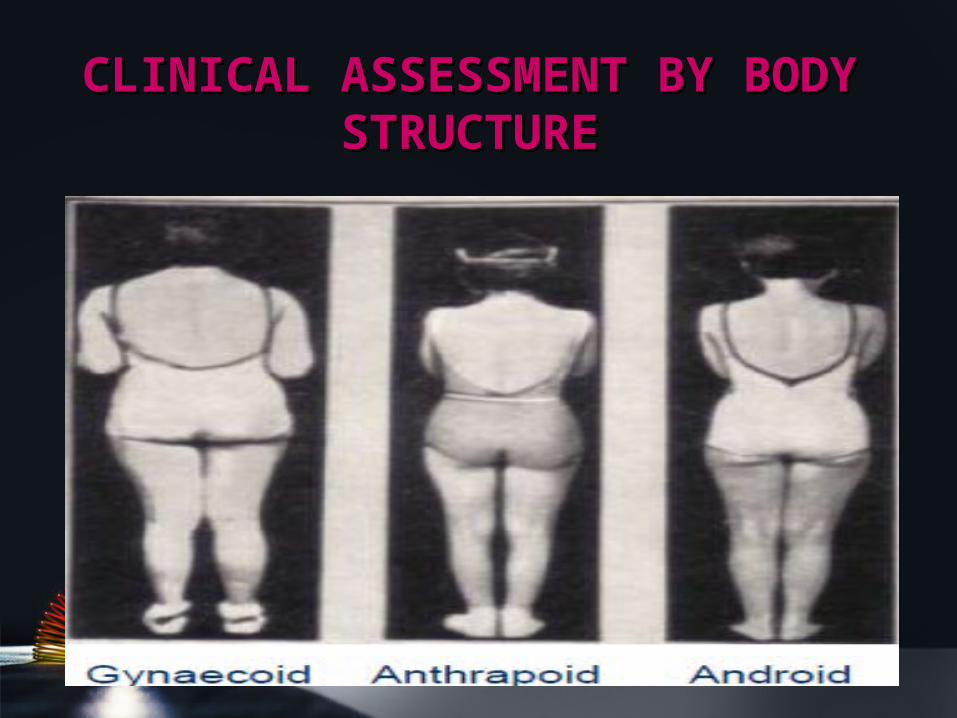
CLINICAL ASSESSMENT BY CLINICAL ASSESSMENT BY BODY STRUCTUREBODY STRUCTURE
Best done beyond 37 weeks or better at start of labour.
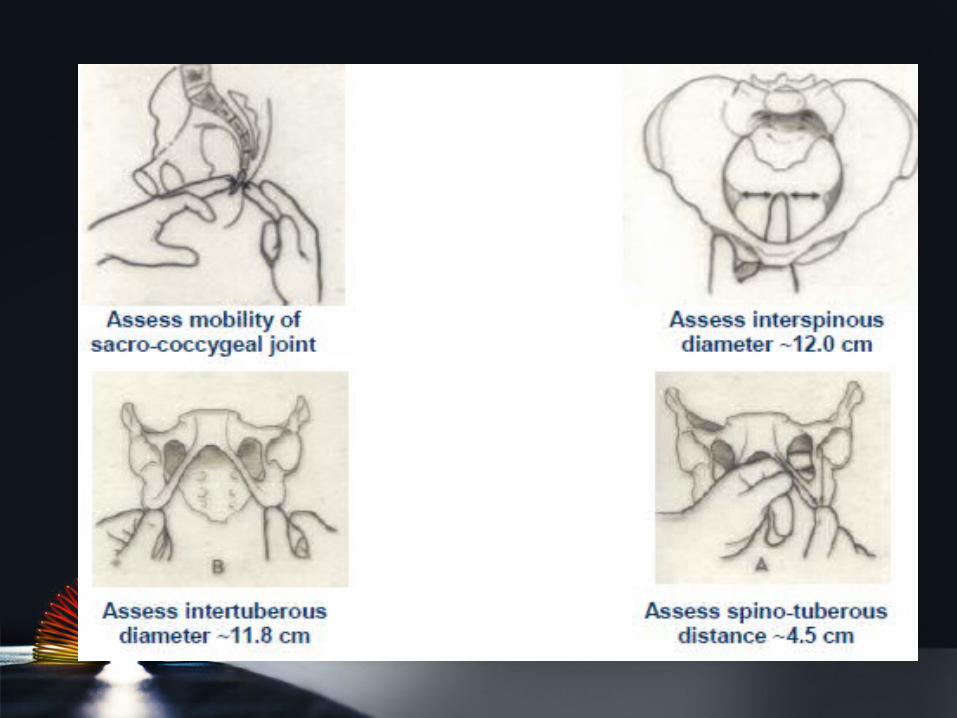
1.1.SACRUMSACRUM – smooth, well curved, seldom reached beyond lower 3 pieces.
2.SACRO-SCIATIC NOTCH – is sufficiently wide such that 2 fingers can be easily placed over sacrospinous ligament, covering the notch.
3.ISCHIAL SPINES – difficult to tough tips of both fingers at the same time.
4.ILIO-PECTINEAL LINES- note for any beaking.
5. SIDE WALLS - normally not palpable by sweeping fingers, unless convergent.
6.POSTERIOR SURFACE OF PUBIC SYMPHYSIS - smooth rounded. Any beaking or angulation is abnormal.
7.SACRO-COCCYGEAL JOINT - mobility noted.
8.PUBIC ARCH - normally rounded accommodating palmar aspect of two fingers.
9.DIAGONAL CONJUGATE
10. PUBIC ANGLE - inferior pubic rami of females is well defined.
11.TRANSVERSE DIMAETER OF OUTLET – place knuckles of clinched fist b/w ischial tuberosities.
DISPARITY IN RELATION B/W THE FETAL HEAD AND THE MATERNAL PELVIS.
ᴥ May be due to average size baby with a small pelvis, or big baby with normal pelvis.
ᴥ Clinical assessment can be done with :-
a)CLINICAL
b)IMAGING TECHNIQUES
c) CEPHALOMETRY- Ultrasound, MRI, X-Ray
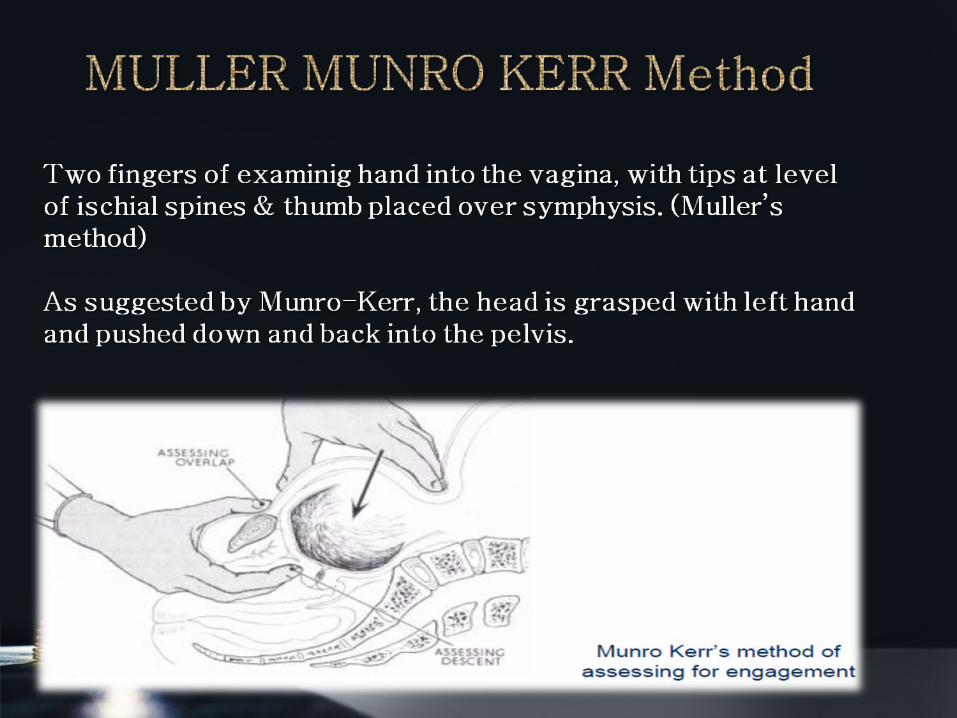
Patient made to lie in dorsal position, with thighs slightly flexed & separated.
Head grasped with left hand.
Index & Middle fingers of the right hand placed above symphysis, keeping inner surface of fingers in line with anterior surface of symphysis, to judge degree of overlapping.
1. Head can be pushed down without overlapping- NO DISPROPORTION.
2. Head can be pushed down with slight overlapping- MODERATE DISPROPORTION.
3. Head cant be pushed down, with overhanging of parietal bones- SEVERE DISPROPORTION.
Patient evacuates her bladder and rectum.
Placed in semi-sitting position to bring the foetal axis perpendicular to the brim.
Left hand pushes the head downwards and backwards into the pelvis while the fingers of the right hand are put on the symphysis to detect disproportion.
I. Head can be pushed down upto level of ischial spines without overlapping of parietal bone over symphysis- No DisproportionNo Disproportion.
II. Head can be pushed a little but not upto level of the spines, with mild overlapping- Mild / Moderate Disproportion.
III. Head cant be pushed, and instead parietal bone overhangs the symphysis, replacing the thumb- Severe Disproportion.
PRETERM INDUCTIONPRETERM INDUCTION
• Only for mild degree of contraction.
• Not favoured in present day practice.
• In multigravidae, with prior history, done 2-3 weeks prior to due date.
ELECTIVE CS AT ELECTIVE CS AT TERMTERM
Major inlet contraction
Moderate degree with complications.
With doubtful maturity, withheld till pains start or ROM, whichever is early.
TRIAL LABOURTRIAL LABOUR
Conducting spontaneous labour in moderate disproportion under supervision, with facilities of intervention available at hand.
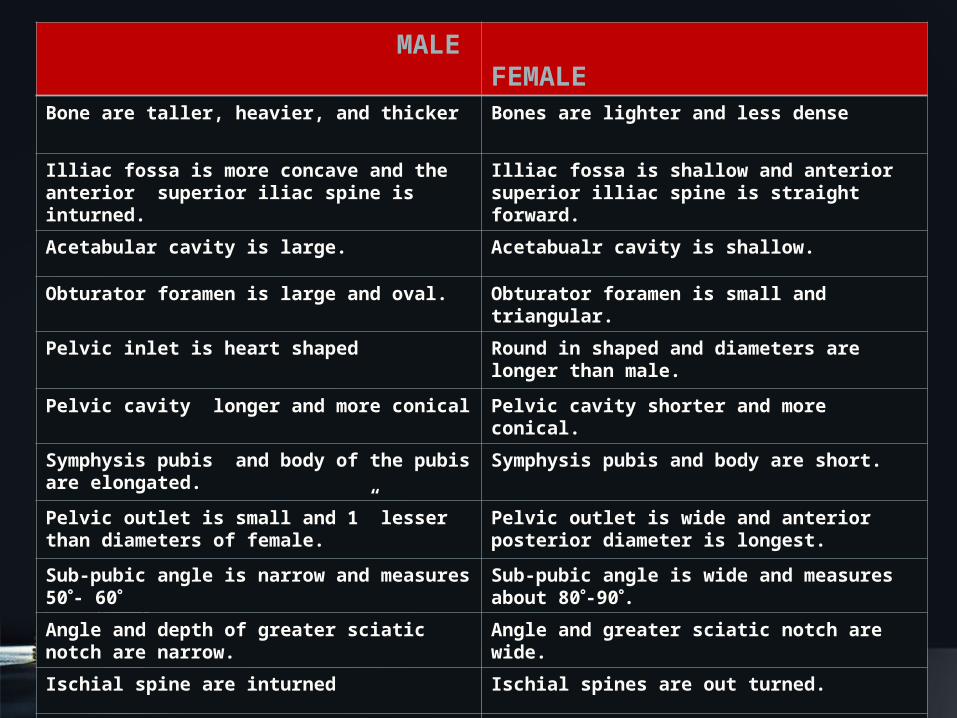
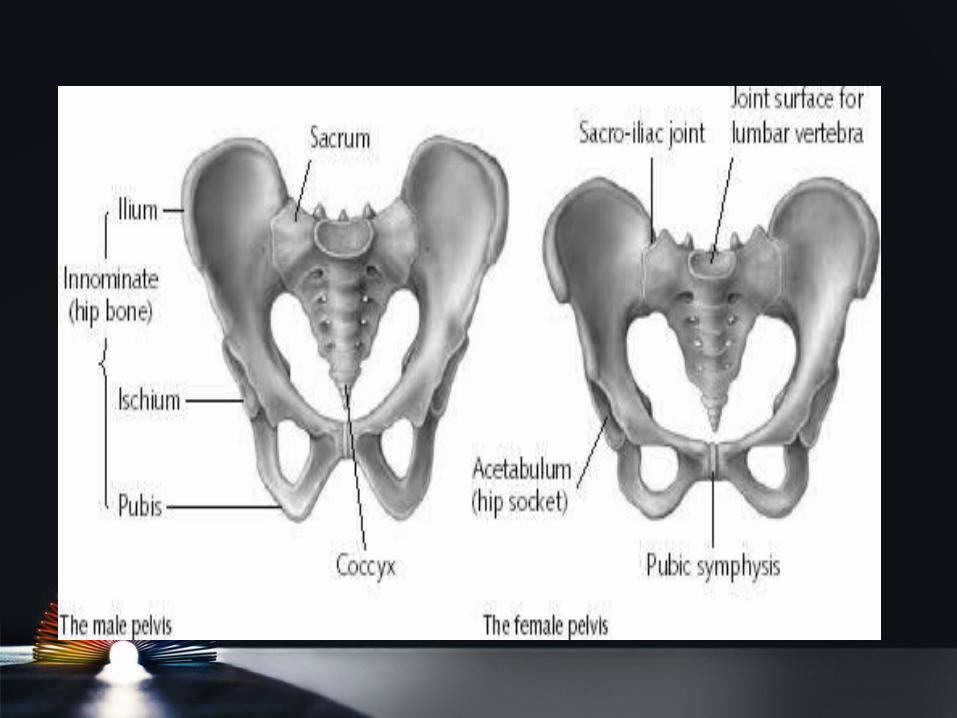
MALE FEMALE
Bone are taller, heavier, and thicker Bones are lighter and less dense
Illiac fossa is more concave and the anterior superior iliac spine is inturned.
Illiac fossa is shallow and anterior superior illiac spine is straight forward.
Acetabular cavity is large. Acetabualr cavity is shallow.
Obturator foramen is large and oval. Obturator foramen is small and triangular.
Pelvic inlet is heart shaped Round in shaped and diameters are longer than male.
Pelvic cavity longer and more conical Pelvic cavity shorter and more conical.
Symphysis pubis and body of the pubis are elongated.
Symphysis pubis and body are short.
Pelvic outlet is small and 1” lesser than diameters of female.
Pelvic outlet is wide and anterior posterior diameter is longest.
Sub-pubic angle is narrow and measures 50- 60
Sub-pubic angle is wide and measures about 80-90.
Angle and depth of greater sciatic notch are narrow.
Angle and greater sciatic notch are wide.
Ischial spine are inturned Ischial spines are out turned.
Curvature of the pelvic surface of sacrum is uniformly concave.
The upper part is more flat and lower part is abruptly concave.