Embed Size (px)
DESCRIPTION
Citation preview

DISORDERS OF HAEM SYNTHESIS

Porphyrias
Lead Poisoning
Sideroblastic Anaemia

Structure of Haem

• Ferrous iron (Fe++)
• Protoporphyrin IX: contains 4 pyrrole rings linked together by methenyl bridges.

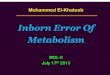
HAEM SYNTHESIS
• 85% haem synthesis occurs in red cell precursors.
• Reticulocytes continue to synthesize haemoglobin for 24-48hrs after release from bone marrow.
• Ceases when RBC’s mature because they lack mitochondria.
• Liver is the main non-RBC source of haem synthesis.

• 80% transferrin iron normally enters developing red cells for haem synthesis.
• Transferrin-receptor complex taken up into mitochondria by endocytosis.
• Iron released at low pH of endosome via DMT1 & reduced from Fe+++ to Fe++ by STEAP3, a ferrireductase.
• Transported into mitochondria by mitoferrin or enters ferritin.

Iron uptake by developing red cell

HAEM SYNTHESISMitochondrion Cytoplasm
Succinyl-CoA
Glycine
δ-Aminolaevulinic acid
Porphobilinogen
Hydroxymethylbilane
Uroporphyrinogen III
Coproporphyrinogen IIIProtoporphyrinogen III
Haem
Protoporphyrin IX
PBG-deaminase
Uro’gen III synthase
Uro’gen III decarboxylase
Copro’gen III oxidase
Proto’gen III oxidase
Ferrochelatase
δ ALA-synthasePyridoxal phosphate
ALA-dehydrogenase
+


Coordination of haem synthesis, globin synthesis & iron regulation.

• Reduced levels of haem rapidly trigger formation of haem-regulated inhibitor(HRI).
• HRI interacts with translation initiating factor eIF-2α & prevents translation of α & β chains.

PORPHYRIAS
• Group of inherited or acquired diseases.
• Each characterized by a partial defect in one of the enzymes of haem synthesis.
• Classified into two groups: Hepatic & Erythropoietic.

Hepatic Porphyrias
FORM
• Acute intermittent porphyria
• Hereditary coproporphyria
• Porphyria variegate
• Porphyria cutanea tarda (PCT)
ENZYME DEFECT
• Porphobilinogen deaminase (PBG)
• Coproporphyrinogen oxidase
• Protoporphyrinogen oxidase
• Uroporphyrinogen decarboxylase

Erythropoietic Porphyrias
FORM
• Congenital erythropoietic porphyria
• Erythropoietic protoporphyria
ENZYME DEFECT
• Uroporphyrinogen oxidase
• Ferrochelatase

Congenital Erythropoietic Porphyria
• Rare autosomal recessive disorder.
• Reduced uroporphyrinogen III synthase activity d/t mutations in the encoding gene.
• Males/females equally effected.
• Age of onset is variable but typically seen in infants & children.

Clinical presentation:
• Highly variable.
• Characterized by cutaneous photosensitivity & dermatitis (ranging from mild to severe).
• Spontaneous oxidation of accumulated porphyrinogens to photoactive porphyrins.
• Hemolytic anaemia, may be mild to severe with resultant splenomegaly & osseous fragility.

• Hypertrichosis
• Port-wine coloured urine
• Hydrops fetalis
• Blepharitis, conjunctivitis, corneal scarring & blindness.
• Inc. amounts of uroporphyrin & coproporphyrin in bone marrow, red cells, plasma, urine & faeces.

Management:
• Avoidance of sunlight
• Splenectomy (to improve red cell survival) is only partially effective.
• High level blood transfusions & iron chelation therapy (to suppress erythropoiesis) sufficiently improve symptoms.
• Allogeneic bone marrow transplantation has been successful.

Erythropoietic Protoporphyria
• Autosomal dominant disorder.
• Deficiency of ferrochelatase enzyme d/t mutations in the encoding gene.
• Males/females equally effected.
• Onset is usually in childhood.

• Inc. protoporphyrin concentrations in bone marrow, red cells, plasma & bile.
• Bone marrow reticulocytes are primary source of excess protoporphyrin.
• Photosensitivity & dermatitis range from mild or absent to severe.
• Little haemolysis but mild hypochromic anaemia may occur.
• Occasionally severe liver disease may occur.

• Urinary porphyrin levels are normal in patients without liver dysfunction.
• Management:
• Avoid sunlight.
• Beta-carotene may also diminish photosensitivity.
• Iron deficiency should be avoided as this may inc. amount of free protoporphyrin.

Porphyria Cutanea Tarda (PCT)
• Most common hepatic porphyria.
• Type I (acquired) - 80%• Type II (autosomal dominant)
• Dec. activity of uroporphyrinogen decarboxylase (UROD)
• More common in men.
• Precipitated in middle or later life by factors like alcohol, liver disease or estrogen therapy.

• Inc. amounts of uroporphyrins & carboxyl-porphyrins excreted in urine.
• Major morbidity is d/t photosensitivity & skin fragility & blistering, hampering daily activities.
• Iron is known to inhibit UROD.
• Removal of iron by repeated phlebotomy is standard treatment, usually leading to remission.

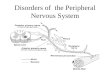
SIDEROBLASTICANAEMIA

• Group of refractory anaemias characterized by:
• Variable numbers of hypochromic cells in peripheral blood.
• Ring sideroblasts comprising 15% or more of marrow ertyhroblasts.

• Siderocyte
• Normal sideroblast
• Mature red cell containing 1 or more siderotic granules.
• Nucleated red cell containing 1 or more siderotic granules:
› Few & difficult to see.
› randomly distributed in cytoplasm.
› reduced proportion of sideroblasts in iron deficiency & anaemia of chronic disorders

Abnormal sideroblastsCytoplasmic iron deposits• Ferritin aggregates
• Numerous & larger granules
• Easily visible & randomly distributed
• Proportion of sideroblasts usually parallels % saturation of transferrin.
• E.g: haemolytic & megaloblastic anaemia, iron overload, thalassaemia disorders.
Mitochondrial iron deposit• Non-ferritin iron
• More than 4 perinuclear granules, covering 1/3rd or more of the nuclear circumference. (Ring sideroblasts)

CLASSIFICATION
ACQUIRED PRIMARY SECONDARY
MYELODYSPLASIA(RARS)
DRUGSTOXINS
HAEMATOLOGIC MALIGNANCIES
OTHER BENIGN CONDITIONS
HEREDITARY
X-LINKED
AUTOSOMAL
MITOCHONDRIAL

HEREDITARY SIDEROBLASTIC ANAEMIAS:
• Rare disorders
• Manifesting mainly in males
• Onset usually in childhood or adolescence
• Occasional late presentation

X-LINKED MUTATIONS
ABCB7 MUTATIONS
ALAS2 MUTATIONS

ALAS2 MUTATIONS:
• More than 25 mutations of the gene for erythroid specific ALAS2 on X chromosome.
• Most lead to changes in protein structure, causing instability or loss of function.
• Function may be rescued to a variable degree by administration of pyridoxal phosphate (B6).
• Response is better if iron overload is removed by phlebotomy or chelation.

• Hypochromic, often microcytic anaemia.
• Bone marrow shows; › erythroid hyperplasia › microcytic erythroblasts with vacuolated cytoplasm › more than 15% ringed sideroblasts
• Few circulating siderocytes, normoblasts & cells with punctate basophilia. ( pronounced only if spleen has been removed)

• Erythroid expansion may result in bossing of skull & enlargement of facial bones.
• Spleen may be enlarged.
• Severe iron overload may occur.
• Female carriers may show partial haematological expression, depending on the severity of defect in the enzyme & degree of lyonization of effected X-chromosome.

ABCB7 MUTATIONS
• Rare form of X-linked sideroblastic anaemia
• ABCB7, a transmembrane protein that binds & hydrolyses ATP, transfers iron-sulphur clusters from mitochondria to cytosol.
• Iron-sulphur clusters are part of IRP1, which controls ALAS2, & ferrochelatase enzyme.

• Early onset.
• Anaemia is mild to moderately severe.
• Non-progressive cerebellar ataxia. (may be due to iron damage to mitochondria in neural cells)
• Inc. red cells zinc protoporphyrin level.

THIAMINE TRANSPORTER
GENE MUTATION
SLC25A38
MUTATIONS
GLUTAREDOXIN-5 MUTATIONS
MITOCHONDRIAL MYOPATHY
AUTOSOMAL
MUTATIONS

THTR-1 MUTATIONS
• SLC19A2 gene mutations encoding for THTR-1
• Causes Roger syndrome, an autosomal recessive disorder.
• Responsible for thiamine responsive megaloblastic anaemia & DIDMOAD. (diabetes insipidus, diabetes mellitus, optic atrophy & deafness)
• Ring sideroblasts are typically seen.

• Onset is usually in childhood.
• SLC25A38 MUTATIONS:
• Transporter protein which transfers glycine to mitochondria.
• An essential step in synthesis of ALA.

GLUTAREDOXIN-5 (GLRX5) MUTATIONS
• Autosomal recessive disorder.
• This enzyme participates in iron-sulphur cluster formation.
• Hypochromic microcytic anaemia with ring sideroblasts.

MITOCHONDRIAL DNA M
•
MITOCHONDRIAL MUTATIONS
Pearson (marrow-pancreas) syndrome
Kearns-Syre syndrome

PEARSON SYNDROME
• Rare multisystemic cytopathy d/t mitochondrial gene deletions.
• Marrow failure is the 1st defining feature & all cell lineages may be effected.
• Macrocytic sideroblastic anaemia typically seen.
• Prominent vacuoles in cells of both myeloid & erythroid lineages.


• Exocrine dysfunction d/t fibrosis & acinar atrophy, resulting in chronic diarrhoea & malabsorption.
• Lactic acidemia d/t defect in oxidative phosphorylation.
• Death often occurs in infancy or early childhood d/t infection, metabolic crisis &/or multi-organ failure.
• Older survivals develop KSS.

KEARSON-SYRE SYNDROME (KSS)
• Rare neuromuscular disorder d/t mitochondrial gene mutations.
• Onset usually before the age of 20yrs.
• Skeletal muscle weakness.
• Short stature
• Hearing loss

• Heart block ( conduction defect)
• Ataxia
• Endocrine dysfunctions
• Impaired cognitive function
• Treatment is generally symptomatic & supportive.
• Prognosis is usually poor.

ACQUIRED
SECONDARY
DRUGSTOXINS
DEFICIENCIESSYSTEMIC DISEASE
PRIMARY
RARS

REFRACTORY ANAEMIA WITH RING SIDEROBLASTS (RARS)
• A myelodysplastic syndrome characterized by:
• Anaemia• Morphologic dysplasia in erythroid lineage• Ring sideroblasts comprising ≥15% of BM
erythroid precursors.
• No significant dysplasia in non-erythroid lineages.• Myeloblasts comprise ‹ 5% of nucleated BM cells
& are not present in PB.

Epidemiology
• Accounts for 3-11% of MDS cases.
• Occurs primarily in older individuals with a median age of 60-73yrs.
• Similar frequency in males & females.

• Etiology
• A clonal stem cell defect manifesting as abnormal iron metabolism in erythroid lineage.
• Acquired defects of mitochondrial DNA may underlie.
• In contrast to congenital X-linked defects, red cell protoporphyrin levels are raised.

Morphology
• Anaemia is often normochromic macrocytic.
• PB smear may manifest a dimorphic picture with a major population of normochromic RBC’s & minor population of hypochromic cells.
• BM aspirate shows erythroid hyperplasia & dysplasia, including nuclear lobation & megaloblastoid features.
• Haemosiderin laden macrophages are often abundant.

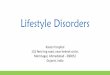
RING SIDEROBLASTS

Bone marrow aspirate
Erythroid precursors vary from mildly dyspoietic to large, bizarre multinucleated cells.

Bone marrow aspirate
Mild megaloblastoid changes but granulocytes have no dysplastic features.

Bone marrow biopsy
Mildly hypercellular with erythroid proliferation. Megakaryocytes are normal in number & morphology.

PB smear
Macrocytic RBC’s (MCV=104).Mild aniso & poikilocytosis

Ring sideroblasts & iron laden macrophages

• Granulocytes & megakaryocytes show no significant dysplasia.( ‹ 10% dysplastic forms)
• BM biopsy is normocellular to markedly hypercellular.
• 1-2% cases evolve into AML. (less than in other MDS forms)
• Median survival is 108 months.

DRUGS
• Anti-tuberculous chemotherapy, specially isoniazid & cycloserine
• (pyridoxine antagonists)
• Chloramphenicol inhibits mitochondrial protein synthesis.
• Penicillamine (copper chelating agent)
• Hormones (progesterone)
• Copper deficiency ( zinc suppliments)

MITOCHONDRIAL TOXINS
• Alcohol
• Lead poisoning

• LEAD TOXICITY
• Exposure to high levels of lead typically associated with severe health effects.
• Minimum Blood Lead Level (BLL) to cause lead poisoning is 10µg/dL. (WHO guidelines)
• Potential sources: toys, old lead pipes, cement, paint, lead fuel, canned food etc.


Mechanisms of action:
• Binds to sulfhydryl group of proteins causing denaturation of structural proteins.
• Binds Ca++ activated proteins & effects various transport systems & enzyme systems.
• Interferes with δ-ALAS & ferrochelatase enzymes.
• Interferes with release of neurotransmitters specially glutamate by blocking NMDA receptors.


• Anaemia is usually normochromic or slightly hypochromic.
• Haemolysis is often, with a mild rise in reticulocytes, but jaundice is rare.
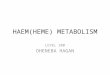
• Basophilic stippling on the ordinary (Romanowsky) stain is characteristic finding. (precipitation of denatured RNA d/t inhibition of the enzyme pyrimidine 5’-nucleotidase)
• Siderotic granules, & ocacasionally Cabot rings are found in circulating red cells.

Basophilic Stippling

Pappenheimer bodies ( Siderotic granules)

Siderotic granules

Management:
• Supportive care
• Reduce exposure
• Chelation therapy in extreme cases.

Treatment of Sideroblastic Anaemia
• Some patients with X-linked sideroblastic anaemia respond to pyridoxine.
• Some secondary sideroblastic anaemias may be completely reversed by pyridoxine therapy.
• Pyridoxine therapy almost always ineffective in refractory anaemia with ring sideroblasts.
• Folic acid may benefit patients with secondary anaemias.

• In cases of iron overload, anaemia may improve after phlebotomy or iron chelation therapy.
• Splenectomy usually does not benefit anaemia & leads to post-operative high platelet counts.