Embed Size (px)
Citation preview

PEPTIC ULCER
By JES JENI..GROUP 8

INTRODUCTION A peptic ulcer is a distinct breach in the
mucosal lining of the stomach (gastric ulcer) or the first part of the small intestine (duodenal ulcer), a result of caustic effects of acid and pepsin in the lumen.
Histologically, peptic ulcer is identified as necrosis of the mucosa which produces lesions equal to or greater than 0.5 cm.
It is the most common ulcer of an area of the gastrointestinal tract that is usually acidic and thus extremely painful.
Helicobacter pylori is one of the most common causes of peptic ulcer. Ulcers can also be caused or worsened by drugs such as aspirin, ibuprofen, and other NSAIDs.

PEPTIC ULCERS INCLUDE:
Gastric ulcers that occur on the inside of the stomach
Esophageal ulcers that occur inside the hollow tube (esophagus) that carries food from your throat to your stomach
Duodenal ulcers that occur on the inside of the upper portion of your small intestine (duodenum)

ETIOLOGY Peptic ulcer disease (PUD) may be due to
any of the following: H pylori infection Drugs Lifestyle factors Severe physiologic stress Genetic factor Excess acid production from
gastrinomas, tumors of the acid producing cells of the stomach that increases acid output

EPIDEMIOLOGY PUD affects between 3.5 and 7.5 million people in the
U.S., with approximately 0.5 million new cases diagnosed every year.
Despite improvements in treatment, widespread use of NSAIDs and low-dose aspirin means that the economic burden of PUD remains significant
The incidence of PUD has declined significantly in the U.S., Europe, and Australia. From 1992 to 1999, the annual rate of hospitalization for PUD decreased from 205 admissions per 100,000 people to 7.7 admissions per 100,000 people.
During the same period, the annual mortality rate for PUD decreased from 165 deaths per 100,000 people to 6 deaths per 100,000 people. This observed trend may be attributable to a consistent decrease in H. pylori infection in several populations, especially in wealthy western societies.

EPIDEMIOLOGY In the United States about four million people have
active peptic ulcers and about 350,000 new cases are diagnosed each year. Four times as many duodenal ulcers as gastric ulcers are diagnosed. Approximately 3000 deaths per year in the United States are due to duodenal ulcer and 3000 to gastric ulcer.
In the past, duodenal ulcer was 10 times as common in men as in women and gastric ulcer had a male preponderance of 3:2.
PUD affects between 3.5 and 7.5 million people in the U.S., with approximately 0.5 million new cases diagnosed every year.
In the U.S., the prevalence of H. pylori among patients over age 60 is reported to range from 40% to 60% compared to only 10% among patients aged 20 years

CLINICAL SYMPTOMS An ulcer may or may not have symptoms. When
symptoms occur, they may include: A gnawing or burning pain in the middle or upper
stomach between meals or at night Bloating Heartburn Nausea vomiting In severe cases, symptoms can include: Dark or black stool (due to bleeding) Vomiting blood (that can look like "coffee-
grounds") Weight loss Severe pain in the mid to upper abdomen



MORPHOLOGY
Esophageal Erosions
The characteristic histological finding of PUD is full ulceration of the gastric or small intestinal mucosa to the level of the sub-mucosa.
Although the term ulceration typically refers to any erosion of the surface epithelium, the term "Peptic Ulcer" is reserved for deeper extents of erosion, into the sub-mucosa.

This is a more typical acute gastritis with a diffusely hyperemic gastric mucosa. There are many causes for acute gastritis: alcoholism, drugs, infections, etc.

Gross usually less than 20 mm in diameter
but they may > 100 mm in diameter.
The classic peptic ulcer is a round to oval, sharply punched-out defect
In contrast, heaped-up margins are more characteristic of cancers
Microscopy the base consists of necrotic tissue
and polymorph exsudate overlying inflamed granulation tissue which merges with mature fibrous (scar) tissue.


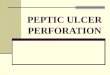
GROSS VIEW A 1 cm acute
gastric ulcer is shown here in the upper fundus. The ulcer is shallow and sharply demarcated, with surrounding hyperemia and some smaller ulcers. It is probably benign.

The endoscopic appearance of a similar acute peptic ulcer in the pre-pyloric region is seen .

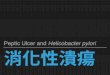
Here is a large 3 x 4 cm gastric ulcer that led to the resection of the
stomach shown here. This ulcer is quite deep with irregular margins.
Complications of gastric ulcers (either benign or malignant) include pain,
bleeding, perforation, and obstruction.

These are gastric ulcers of small, medium, and large size on upper endoscopy.

Microscopically, the ulcer here is sharply demarcated, with normal gastric mucosa on the left falling away into a deep ulcer whose base contains infamed, necrotic debris.
An arterial branch at the ulcer base is eroded and bleeding.



This has allowed corrosive stomach acid to splash upward into the lower esophagus causing the red inflammation and white
ulcers to form

ENDO-SCOPICALY DETECTED ULCERS IN SMALL INTESTINE MUCOSA

Chronic peptic ulcerHistologic section through the ulcer shows layers of acute inflammatory exudate including fibrin,acute inflammation, chronic inflammation, and fibrosis.

The ulcer at the right is penetrating through the muscularis and approaching an artery. Erosion of the ulcer into the artery will lead to another major complication of ulcers--hemorrhage. This hemorrhage can be life threatening.

Helicobacter gastritisHelicobacter organisms may be tested for urease activity.
Staining of the gastric biopsy showsthe characteristic curved rods embedded in the mucin layer of the stomach.

Peptic ulcerPeptic ulcer can be identified with a barium study which outlines the penetrating ulceration.

"Hourglass" stomachDue to chronic peptic ulceration there is fibrosis and contracture ofthe stomach leading to an hourglass shape as well as altered mobility.

RISK FACTORS The following factors raise your risk for peptic
ulcers:
Drinking too much alcohol Regular use of aspirin, ibuprofen, naproxen, or other
non steroidal anti-inflammatory drugs (NSAIDs). Taking aspirin or NSAIDs once in a while is safe for most people.
Smoking cigarettes or chewing tobacco Being very ill, such as being on a breathing machine Having radiation treatments A rare condition called Zollinger-Ellison syndrome
causes stomach and duodenal ulcers.

ZOLLINGER-ELLISON
SYNDROME Zollinger-Ellison syndrome is a condition in which
there is increased production of the hormone gastrin. Most of the time, a small tumor (gastrinoma) in the
pancreas or small intestine produces the extra gastrin in the blood.
Zollinger-Ellison syndrome is caused by tumors. These growths are most often found in the head of the pancreas and the upper small intestine.
The tumors produce the hormone gastrin and are called gastrinomas. High levels of gastrin cause production of too much stomach acid.

PROGNOSIS The mortality rate is 1 in 100,000, a figure which has
decreased modestly in the last few decades. When the underlying cause for peptic ulcer disease is
successfully treated, the prognosis (expected outcome) for patients with the condition is excellent. To help prevent peptic ulcers, avoid the following:
Alcohol Common sources of Helicobacter pylori bacteria (e.g.,
contaminated food and water, floodwater, raw sewage) Long-term use of non steroidal anti-inflammatory drugs
(NSAIDs) Smoking

COMPLICATION Severe blood loss Scarring from an ulcer may make it harder for the stomach to
empty Perforation or hole of the stomach and intestine perforation - A hole develops in the lining of the stomach or
small intestine and causes an infection. Signs of a perforated ulcer include sudden, severe abdominal pain.
internal bleeding - Bleeding ulcers can result in significant blood loss and lead to hospitalization. Signs of a bleeding ulcer include lightheadedness, dizziness, and black stools.
scar tissue - thick tissue that develops after an injury. This tissue makes it difficult for food to pass through your digestive tract. Signs of scar tissue include vomiting and weight loss.
melaena are associated with erosion of a large blood vessel