-
EBM
-
Medical Education in the New Century
Bioinformatics
Patient-centered care
Problem-based learning
Evidence-based medicine
-
(EBM, Evidence-based Medicine)
-
1972Archie Cochrane~ Randomized controlled trials
1992Archie Cochrane1993Cochrane Collaboration(Iain Chalmers,
David Sackett)
Lancet Cochrane Collaboration
-
Dr. Sydney Burwell, Dean of Harvard Medical School
Half of what you are taught as medical students will in ten
years have been shown to be wrong. And the trouble is, none of your
teachers knows which half.
-
Use of current best evidence in making decisions about the care
of individual patients
Not only a skill but also an attitude change
Conscientious, explicit, and judicious use of current best
evidence in making decisions about individual patients. ~ Archie
Cochrane 1972E B M
-
McMaster UniversityHIRUHealth Information Research UnitCochrane
Collaboration http://hiru.mcmaster.ca/ Oxford University Centre for
Evidence-Based Medicinehttp://cemb.jr2.ox.ac.uk American College of
PhysicianACP ACP Journal Club Onlinehttp://www.acpjc.org
-
Step 1. Converting the need for information (about prevention,
diagnosis, prognosis, therapy, causation, etc.) into an answerable
question.
Step 2. Searching the best evidence with which to answer that
question.
Step 3. Critically appraising the evidence for its validity
(closeness to the truth), impact (size of the effect), and
applicability (usefulness in our clinical practice).
Step 4. Integrating the evidence with our clinical expertise and
patients unique biology, values and circumstances.
Step 5. Evaluating our effectiveness and efficiency in executing
steps 1-4 and seeking ways to improve them both for next time.Five
Steps to Practice EBM
-
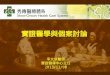
The Evidence PyramidAnimal researchIn vitro (test tube)
researchCase series/ReportsIdeas, Editorials, OpinionsCase Control
StudiesCohort studiesRandomized Controlled StudiesRandomized
Controlled Double Blind Studies Meta - analysis
-
asking an answerable question
searching the best evidence
critical appraisal the evidence
evaluation
-
Asking Answerable Clinical QuestionsWell-built clinical
question
Background questionAsk general knowledge about a disorderHave
two essential components:A question root (who, what, why, when)
with a verbA disorder, or an aspect of a disorderForeground
questionAsk for specific knowledge about managing patients with a
disorderHave four (or three) essential components:1. Patient and/or
problem2. Intervention (treatment)3. Comparison intervention4.
Clinical outcomes
-
Patient ~ Who is the patient or what is the problem being
addressed?
Intervention ~ What is the intervention?
Comparison ~ What are the alternatives?
Outcome ~ What are the outcomes?There are four elements of a
well-formulated question
-
Searching The Best Evidence(primary journals or databases) ~
Medline, NEJM, Lancet
(secondary journals or databases) ~ ACP journal club,
Cochrane.
(level of evidence)
-
update
-
ACP Journal Club: ACP Journal ClubAmerican College of Physicians
Evidence-Based MedicineACP British Medical Journal Group50
DARE: Database of Abstracts of Reviews of Effectiveness National
Health Services' Centre for Reviews and DisseminationNHS CRD
DARE
CDSRCochrane Database of Systematic Reviews Cochrane Cochrane
Collaboration
CCTRCochrane Central Register of Controlled Trials 300,000
RCTRandomized Controlled Trials CCT Clinical Controlled Trials
Cochrane groups Medline EMBASE
-
EBM
-
CGMH PubMed: http://www.ncbi.nlm.nih.gov/PubMed/
1. ACP Journal Club: http://www.acpjc.org/ (1-4, 7)2. Cochrane ~
DARE (Database of Abstracts of Reviews of Effects)3.CDSR (Cochrane
Database of Systematic Reviews) ~ Collaborative Review Groups
http://www.cochrane.org/cochrane/revabstr/crgindex.htm 4.CCTR
(Cochrane Central Register of Controlled Trials): 5.Cochrane
collaberation 6.NGC (National Guideline Clearinghouse):
http://guideline.org 7.Micromedex (CCIS) 8.Centre for
Evidence-Based Medicine: http://www.cebm.net/ =
http://cemb.jr2.ox.ac.uk 9.McMaster UniversityHIRUHealth
Information Research UnitCochrane Collaboration:
http://hiru.mcmaster.ca/10. American College of PhysicianACP:
http://www.acponline.org 11.Bandolier: http://www.ebandolier.com =
http://www.jr2.ox.ac.uk/bandolier/12.AHRQ website:
http//www.ahrq.gov13.InfoPOEMs: http://www.infopoems.com 14.Other
resources: http://www.google.com.tw/ www.yahoo.com/
http://www.mdconsult.com/15. 16.17. (HINT):
http://www.hint.org.tw
-
The Evidence PyramidAnimal researchIn vitro (test tube)
researchCase series/ReportsIdeas, Editorials, OpinionsCase Control
StudiesCohort studiesRandomized Controlled StudiesRandomized
Controlled Double Blind Studies Meta - analysis
-
Grade of RecommendationLevel of EvidenceTherapy[A]1aSystemic
review of RCTs1bSingle RCT1cAll-or-none[B]2aSystemic review of
cohort studies2bCohort study or poor RCT2cOutcomes
research3aSystemic review of case-control studies3bCase-control
study[C]4Case series[D]5Expert opinion, physiology, bench
research
-
sensitivityspecificitylikelihood ratiopre-test
probabilitypost-test probability
ARR (Absolute risk reduction) = EER (Experimental Event Rate) -
CER (Control Event Rate) Number needed to treat, NNT=1/ARR relative
risk reductionRRR
absolute risk increaseARI= EER (Experimental Event Rate) - CER
(Control Event Rate) Number needed to harm, NNH=1/ARI
(Relative risk) (Odds) (Odds ratio) (confidence interval)
-
DiagnosisSensitivity = a/a+c = 731/809 = 90%Specificity= d/b+d =
1500/1770 = 85%Positive predictive value = a/a+b = 731/1001 =
73%Negative predictive value = d/c+d = 1500/1578 = 95%
LR+for a positive result = sens/(1- spec) = 90%/15% = 6LR- for a
negative result = (1-sens)/spec = 10%/85% = 0.12Pre-test
probability (prevalence)= a+c/a+b+c+d= 31%Pre-test odds =
prevalence/(1-prevalence) = 31%/69% = 0.45Post-test odds = Pre-test
odds Likelihood RatioPost-test probability= Post-test
odds/(Post-test odds + 1)
-
Calculation of OR/RREER = a/a+b = 0.033CER = c/c+d =
0.30Relative risk= EER/CER = (a/a+b)/(c/c+d) = 0.11
Experimental event Odds = a/b = 0.034Control event Odds = c/d =
0.43Relative Odds = Odds ratio= (a/b)/(c/d) = ad/bc = 0.08Odd: a
ratio of non-events to events
-
Asking Answerable Clinical Question
Patient/ProblemInsulin-dependent diabeticsInterventionIntensive
insulin regimenComparisonRegular insulin
regimenOutcomesRetinopathySymptomatic hypoglycemia
-
Treatment EffectsOccurrence of diabetic retinopathy at 5 years
among insulin-dependent diabetic in the DCCT trialUsual insulin
regimen (CER: control event rate): 38%Intensive insulin regimen
(EER: experimental event rate): 13%
Risk Reduction (calculation)Absolute risk reduction (ARR) =
CER-EER = 38%-13% = 25%Relative risk reduction (RRR) = CER-EER/CER
= 25%/38% =66%Number needed to treat (NNT) = 1/ARR = 1/25% = 4
patientsThe number of patients that need to be treated to prevent
one bad outcome or get one good outcome.
-
HarmThe proportion of patients with at least one episode of
symptomatic hypoglycemia Usual insulin regimen (CER: control event
rate): 23%Intensive insulin regimen (EER: experimental event rate):
57%
Risk Increase (calculation)Absolute risk increase (ARI) = EER -
CER = 57% - 23% = 34% Relative risk increase (RRI) = EERCER/CER =
57% - 23%/23% = 148%Number needed to harm (NNH)=1/ARI = 1/0.34= 3
patients ()The number of patients that need to be treated to cause
one bad outcome (being harmed)
-
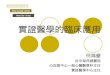
Treatment of Class III-IV Lupus Nephritis
Meta-Analysis
Treatment of diffuse proliferative lupus nephritis: A
meta-analysis of randomized controlled trialsAm J Kidney Dis. 2004
Feb;43(2):197-208. Cochrane Renal Group Cochrane Database of
Systematic Reviews. 1, 2004.
-
Values of RR less than 1 indicate a reduction in risk for the
outcome with the experimental treatment. Conversely, values of RR
more than 1 indicate an increase in risk. The 95% CIs are a measure
of variability in the precision of the RR estimate and its
statistical significance. Heterogeneity of treatment effects
between studies was investigated by visual examination of graphic
meta-analysis plots and from the Cochran Q (heterogeneity
chi-square) and I2 statistic.This is a forest plot, with a vertical
line at 1.0 representing equivalence in risk for an outcome with
experimental and control treatment (null hypothesis). The RR for
each outcome and its 95% CI are indicated by a solid square and a
line. The size of the solid square represents the contribution
(weight) of the trial to the analysis. Diamond-shaped symbols
represent the summary estimator of overall effect pooling the
weighted effect of individual RCTs.
-
medical decision making technique accessing medical information
assessing the validity of medical information (RCT randomized
controlled trials) guidelineclinical pathway
-
(health care-provider)
(clinical practice guideline) Clinical Practice Guidelines
-
Resource Centers for GuidelinesNGC - National Guideline
Clearinghouse http://www.guideline.govAGREE - appraisal of
guideline research & evaluation
http://www.agreecollaboration.org/Guidelines International Network
http://www.g-I-n.net/SIGN - Scottish Intercollegiate Guidelines
Network http://www.sign.ac.uk/
-
Decision tree analysis
-
~
()
-
EBMEBM introduction94.03 EBM workshop
14()
929PGY186-10PGY112:00~13:008A-8BEBMPGY1
-
Interpretation of evidence is subjective: it dependents on how
you view it.
-
Clinical Practice GuidelinesSystemically developed statements to
assist practitioner and patient decisions about appropriate health
care for specific clinical circumstances.
Purpose ~ to make explicit recommendations with a definite
intent to influence what clinicians do.