Embed Size (px)
Citation preview

통증 물리치료학 및 실습
Gachon University
Department of Physical Therapy Hwi-young Cho, PT, PhD
CH 14. 요통 재활 - 2

3. Stenosis

Spinal Stenosis
• Grouped as “spinal stenosis”
– Central stenosis
• Narrowing of the central part
of the spinal canal
– Foraminal stenosis
• Narrowing of the foramen,
resulting in pressure on the
exiting nerve root
– Far lateral recess stenosis
• Narrowing of the lateral part
of the spinal canal
http://www.whitechiropractic.info/spinalstenosis.html

Spinal Stenosis
http://www.nextavenue.org/article/2012-06/spinal-stenosis-painful-and-frequently-misdiagnosed-condition

Spinal Stenosis
• Symptoms – Leg pain
– Numbness, weakness, and cramping in the legs, feet, or buttocks.
– Stiffness in the legs and thighs.
– Low back pain.
– In severe cases, loss of bladder and bowel control.
http://www.mildprocedure.com/what-is-lss.html

Spinal Stenosis
• 진단 – MRI
– Computerized tomography (CT) scan
– Physical exam
• 비수술적 중재 – Rest during acute phase
– Physical therapy • Exercise/walking
• http://www.youtube.com/watch?v=mcv8lujBI20
– NSAID or Steroid injections
https://www.preferredpaincenter.com/spinal-stenosis.html

Spinal Stenosis
• 수술적 중재 – 비수술적 중재로 실패 시 시행함
– 최후의 선택임
– http://www.youtube.com/watch?v=Bm-MYMM2DBY
– Decompression

http://www.doereport.com/enlargeexhibit.php?ID=72242 Laminectomy & Foraminatectomy

4. Ankylosing spondylitis
• Progressive disease including the chronic pain and muscle spasm
• 20 age, male
• SI joint > Lumbar > Thoracic > Rib
• Bamboo Spine :
– Ossification of the annulus fibrosus, the anterior longitudinal ligament

5. Mechanical Low Back Pain
• http://www.youtube.com/watch?v=sUAHifmzvig
• = Non-specific low back pain
• Nondiscogenic back pain that is provoked by physical activity and relieved by rest.
• Cause
– strain and sprain
– Deconditioning and decompensation
• Overuse = insidious onset
• Pain
– Type: Chronic, dull, aching
– Progressive worsens during the day
• Intervention
– Therapeutic exercise • Yoga or Pilates
• Postural reeducation
• Abdomen and back muscle strengthening

6. Osteoarthritis
• Begin during the third decade of life
• Pain
- Centered in the lower back
- Increased with movement
- Morning stiffness(esp. extended period)
- Relieved by rest.
• Hypertrophic change or spur root compression
• Management
: Postural training
: Abdomen and back muscle strengthening
: when severe, back support for 6 wks (prefer isometric)

7. Scoliosis • A person's spine is curved from side to side (frontal
view).
• C-shape and S-shape
• Occuring : < 14 old
• Female > Male (3~5 times)
http://newbridgespine.com/pain-due-scoliosis/

http://www.fpnotebook.com/_media/BackScoliosisXRay.gif

Scoliosis
• Tx exercise
– http://www.youtube.com/watch?v=188PTlRq1Qo
– http://www.youtube.com/watch?v=wmk5Mvz4pe8

8. Lordosis
• L3 추간판에 가해지는 부하량 :
–누운 자세 < 서있는 자세 < 앉은 자세 <앉아서 앞으로 굽힌 자세
http://stronglifts.com/lordosis-why-it-causes-lower-back-pain-how-to-fix-it/

9. Degenerative disease
Degenerative disc DZ

Degenerative Disease
• The symptoms of pain and possibly radiating weakness or numbness stemming from a degenerated disc in the spine. While the definition sounds simple, many patients diagnosed with degenerative disc disease are left wondering exactly what this diagnosis means for them.
• http://www.youtube.com/watch?v=Q_5U7skcQeM
• http://www.youtube.com/watch?v=SEa4M29xeP4
http://www.doctorpinchback.com/backpain2.html
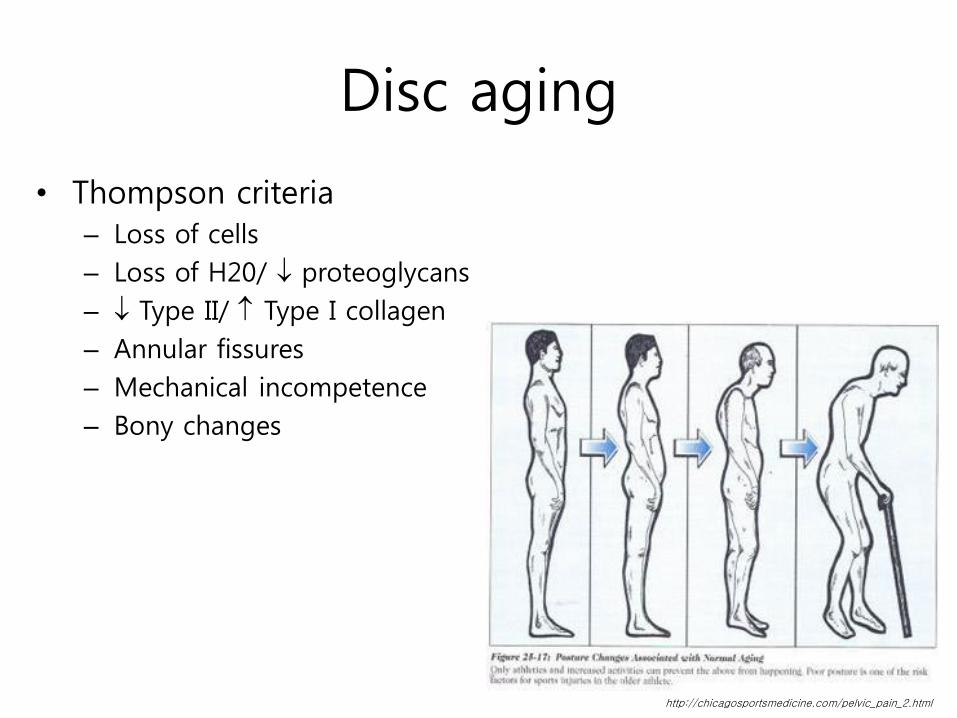
Disc aging
• Thompson criteria – Loss of cells
– Loss of H20/ proteoglycans
– Type II/ Type I collagen
– Annular fissures
– Mechanical incompetence
– Bony changes
http://chicagosportsmedicine.com/pelvic_pain_2.html
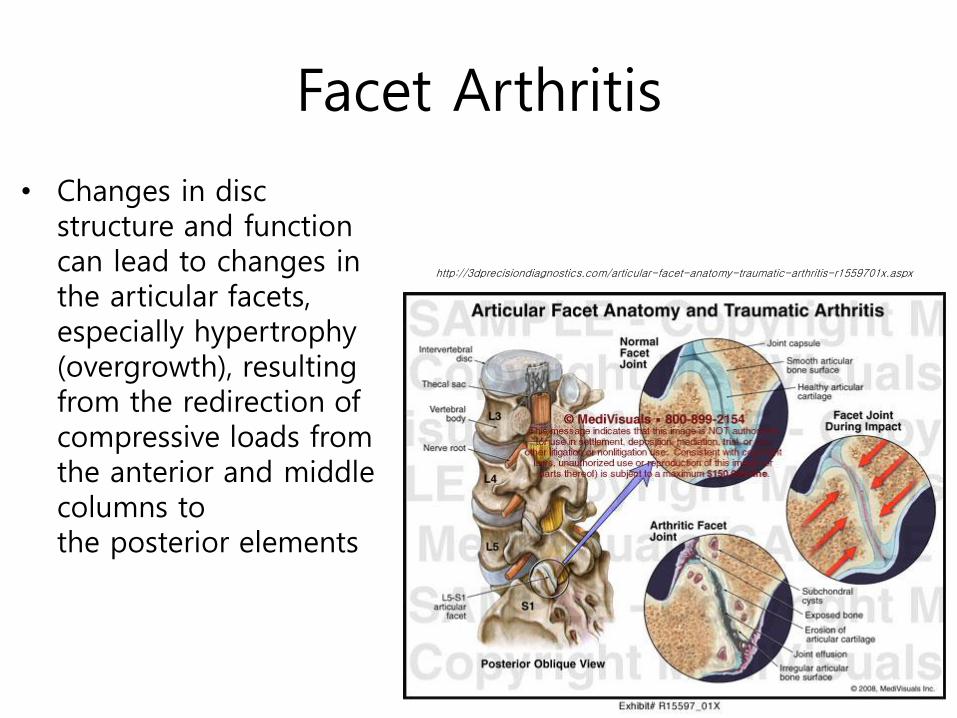
Facet Arthritis
• Changes in disc structure and function can lead to changes in the articular facets, especially hypertrophy (overgrowth), resulting from the redirection of compressive loads from the anterior and middle columns to the posterior elements
http://3dprecisiondiagnostics.com/articular-facet-anatomy-traumatic-arthritis-r1559701x.aspx

Disc height 과 Facet joint 는 상관관계가 있음을 나타냄.

Degenerative Disc Disease
• 진단 – MRI/CT
– Discography
– Physical examination
• 비수술적 중재 – 휴식: 급성의 경우
– Steroid & NSAID medication
– Physical therapy • Exercise/walking
• Low-impact aerobics
• Trunk strengthening

Degenerative Disc Disease
• Surgical care – Failure of nonoperative treatment
• Minimum of 6 weeks
– Fusion • Removal of disc and replacement with bone graft, or
a cage-filled bone graft, or a bone graft substitute – Anterior approach – Posterior approach – Combined approach
– http://www.youtube.com/watch?v=H8sK7ABcin4 – Arthroplasty
• Articulating disc replacement

Lumbar Fusion
• Fusion procedure used to treat:
– Spondylolisthesis
– Spondylolysis
– DDD
• Multiple approaches
– Posterior, anterior, transforaminal, combined anterior/posterior

Posterior Lumbar Fusion
• Posterolateral fusion (PLF) – 적용대상: Spondylolisthesis
and spondylolysis without disc involvement
– Involves adding bone graft to an area of the spine to set up a biological response that causes the bone to grow between the two vertebral elements and thereby stop the motion at that segment.
http://www.methodistorthopedics.com/posterior-lumbar-fusion
http://www.methodistorthopedics.com/posterior-lumbar-fusion

Lumbar Arthroplasty
• Total disc replacement (TDR)
– DDD
– Contraindicated for spondylolisthesis and spondylolysis
The CHARITÉ Artificial Disc is indicated for spinal arthroplasty in skeletally mature patients with DDD at one level from L4-S1.
http://www.jkma.org/search.php?where=aview&id=10.5124/jkma.2007.50.6.523&code=0119JKMA&vmode=PUBREADER#!po=10.0000

Tx procedure
Brief summary for diagnosis &
treatment

Outline
• List essential components of a LBP history,
including Red flags
• Review proper indications for imaging
analysis
• Review Physical Examination for LBP
– Identify Red flags
• Discuss acute or chronic management options

General Questions -Important-
Onset
Location
Mechanism of Injury
Radiation
Positional change
Numbness, tingling
Weakness

Red Flags
• Age > 50
• IV drug use
• Hx/o cancer
• Prolonged steroid use
• Osteoporosis
• Distal numbness
• Saddle anestesia
• Bowel or bladder loss
• Fever
• Trauma
• Unexplained wt loss
• Pain at rest/night
• Weakness

Diagnoses & Red Flags • Cancer
– Age > 50
– History of Cancer
– Weight loss
– Unrelenting night pain
– Failure to improve
• Infection – IVDU
– Steroid use
– Fever
– Unrelenting night pain
– Failure to improve
• Fracture – Age >50
– Trauma
– Steroid use
– Osteoporosis
• Cauda Equina Syndrome – Saddle anesthesia
– Bowel/bladder dysfunction
– Loss of sphincter control
– Major motor weakness

Diagnoses & Red Flags • Cancer
– Age > 50
– History of Cancer
– Weight loss
– Unrelenting night pain
– Failure to improve
• Infection – IVDU
– Steroid use
– Fever
– Unrelenting night pain
– Failure to improve
• Fracture – Age >50
– Trauma
– Steroid use
– Osteoporosis
• Cauda Equina Syndrome – Saddle anesthesia
– Bowel/bladder dysfunction
– Loss of sphincter control
– Major motor weakness

Outline
• List essential components of a LBP history,
including Red flags
• Review proper indications for imaging
analysis
• Review Physical Examination for LBP
– Identify Red flags
• Discuss acute or chronic management options

Tests
Imaging
XR
CT
MRI

Imaging
X Ray CT Scan MRI

Imaging Guidelines
Choice to do imaging based on:
Historical red flags
Trauma, chronic steroid use = XRay
Suspect abscess, cauda equina = MRI
Exam red flags
Midline TTP = Xray
New/severe sensory or strength loss = consider MRI

Outline
• List essential components of a LBP history,
including Red flags
• Review proper indications for imaging
analysis
• Review Physical Examination for LBP
– Identify Red flags
• Discuss acute or chronic management options
Physical Exam Rule-out most concerning things
• Concerning features
– Midline TTP
– Decreased strength
– Diminished reflexes
– Sensory loss
• Reassuring features
– Paraspinal muscle spasm
– Full strength
– No sensory deficits

Six-Point MSK Exam
• Inspection
• Palpation
• ROM
• Strength
• Neurovascular
• Special Tests

Inspection
Ensure
No obvious deformities
No erythema
Skin lesions (Zoster)
Palpation
Soft Tissue
4 clinical zones
Paraspinal muscles
Gluteal muscles
Sciatic area
Anterior abdomen/abdo
minal wall
• Bones
– Primarily palpating
spinous processes and
facets

Flexion - 80º
Extension - 35º
Side bending - 40º each side
Twisting - 3-18º
Range of Motion

Neurologic
Testing
• Sensation
• Strength
• Reflexes
http://mddirect.org/tag/dermatomes/
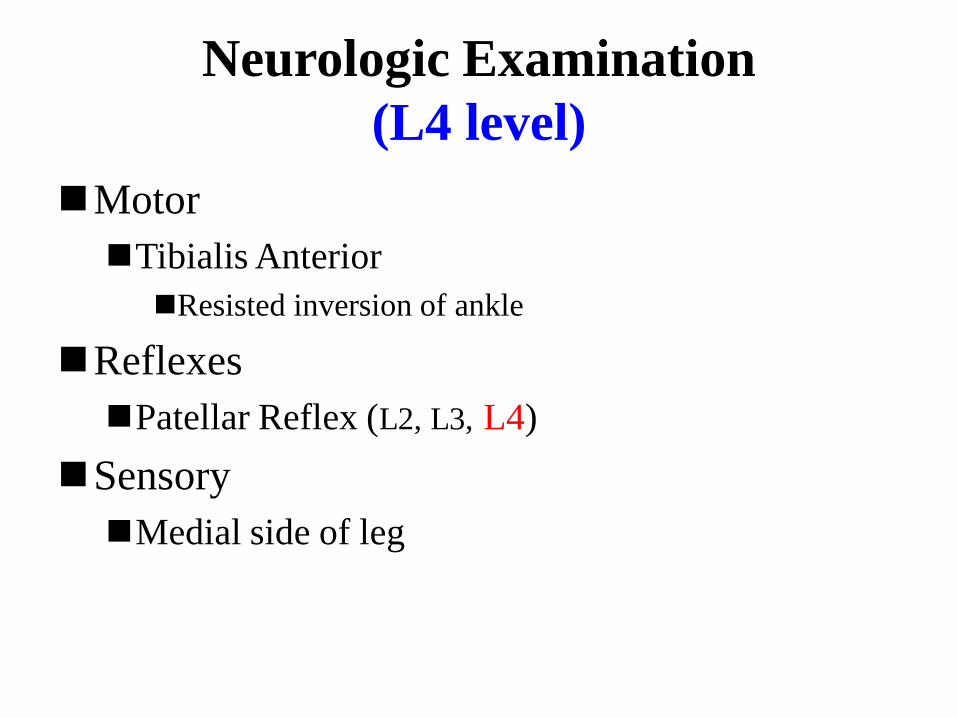
Neurologic Examination
(L4 level)
Motor
Tibialis Anterior
Resisted inversion of ankle
Reflexes
Patellar Reflex (L2, L3, L4)
Sensory
Medial side of leg

http://quizlet.com/15681576/phmd-6010-wk-1-4-written-no-tests-flash-cards/

Neurologic Examination
(L5 level)
Motor
Extensor Hallicus Longus
Resisted dorsiflexion of great toe
Reflexes - none
Sensory
Dorsum of foot in midline

http://quizlet.com/15681576/phmd-6010-wk-1-4-written-no-tests-flash-cards/

Neurologic Examination
(S1 level)
Motor
Peroneus Longus and Brevis
Resisted eversion of foot
Reflexes
Achilles
Sensory
Lateral side of foot

http://quizlet.com/15681576/phmd-6010-wk-1-4-written-no-tests-flash-cards/

Special Tests
Tests to stretch spinal cord or sciati
c nerve
Tests to stress the sacroiliac joint

Straight leg raise
Looking for lumbar disk herniation
Performed supine for best sensitivity
Positive when radiating pain observed at 30-70 degress of hip flexion
Very high sensitivity, but low specificity
Should also do the crossed-leg straight leg raise
Positive when they have pain when you lift and adduct the opposite leg

FABER Test
• = Patrick test
• Flexion Abduction External Rotation Test
• To assess for – both Sacroiliac Joint (SIJ) pain
– anterior/lateral hip capsular tightness
• Pain in the anterior thigh is indicative of Hip pain.
• Pain posteriorly is indicative of SIJ pain.
• http://www.youtube.com/watch?v=XCOD1dkcVk0
• http://www.youtube.com/watch?v=V1a0E0ssTqA

FABER test: Flexion A- Bduction External Rotation

FADIR Test
• Flexion Adduction Internal Rotation Test
• To assess for
– Hip impingement (Femoroacetabular impingement)
• Anterolateral Hip pain suggestive of hip
Impingement (Femoroacetabular impingement)
• http://www.youtube.com/watch?v=36hGS6xf_8Y

FADIR test:
Flexion
A-
Dduction
Internal
Rotation

Hoover Test
Helps to determine whether pt is malingering
Should be performed in conjunction with SLR
When pt is genuinely attempting to raise leg, h
e exerts pressure on opposite calcaneus to gain
leverage
http://www.youtube.com/watch?v=_cchOvhY
yxA


Inducing factors of LBP
AGE Trauma OA
Osteoporosis
smoking
obesity
dancer
W lifting
DM EXERCSIE
Rotation operation
LBP

Prolo
therapy
OP
Root
BLOCK
REST
EXTENSION
EX
PT DRUG
Therapeutic methods

Therapeutic goal

Operation
IDET(추간판내 열응고술)
PDN (Prosthetic disc nucleus)
연성디스크 삽입술
(고합성물 물질 – 폴리머)
TDR(인공디스크 전치환술)

PT materials for TX of LBP
• PT modalities
– Hot / cold pack
– Electrical modalities
• Manual therapy
–칼텐본, 메잇랜드, 추나, 카이로프락틱
• Exercise

History of Spine Rehabilitation
“Early on bed rest was the treatment of
choice for most back pain”
50’s and 60’s
* Flexion
* Posterior pelvic tilt

70’s – Extension (Robin McKenzie) – “Back school” – Modalities (Heat, US, ES, Traction, Massage) – Joint mobilization
80’s
- Stabilization Training
(Northern California)

Superficial layer Deep layer
http://www.netterimages.com/image/9986.htm https://bedahunmuh.wordpress.com/2010/05/11/muscles-of-back-deep-layers/

Abdomial muscles Erector spinae
http://www.hoopdaloop.com/hoopblog/ http://lyndseydesjardins.com/functional-anatomy-part-7-intrinsic-back-muscles/

Local and Global muscles
* Attaching directly to the lumbar vertebrae. * Controls curvature of spine * Responsible for segmental stability. * Maintain or decrease intervertebral motion
Local muscles (intersegmental muscles)

* The large torque producing muscle linking the pelvis to the thoracic cage. * Balance outer load (gravity, lifting object,etc) * Providing general trunk stabilization
Local and Global muscles
Global muscles
(multisegmental muscles)

Lumbar Stabilization
Stabilization implies the ability of an individual to control, consciously or unconsciously, macroscopic and microscopic movement at a joint.
- Magee(1999) -

Stabilization training is to eliminate repetitive injury to the intervertebral discs, facet joints and related structures.
Lumbar Stabilization

The three systems active spinal stabilization
PASSIVE SUBSYSTEM
- Spinal column
ACTIVE SUBSYSTEM
- Spinal Muscle
CONTROL SUBSYSTEM
- Neural
SPINAL STABILITY
Stability model Panjabi (1992)

Lumbar segmental stability
The local muscle system has a primary responsibility for segmental stability.
It appears that both multifidus(다열근) and transverse abdominis(복횡근) are important components of this system.

Multifidus
Multifidus demonstrated greater fatiguability relative to other parts of the erector spinae in Chronic back patients compared to a normal population.
Biederman et al (1991)

transverse abdominis
Hodges and Richardson (1995), EMG experiment, analyzing the onset of activity of the muscles of the abdominal wall in response to “arm movement” , the timing of onset of
transverses abdominis was delayed in chronic low back pain.
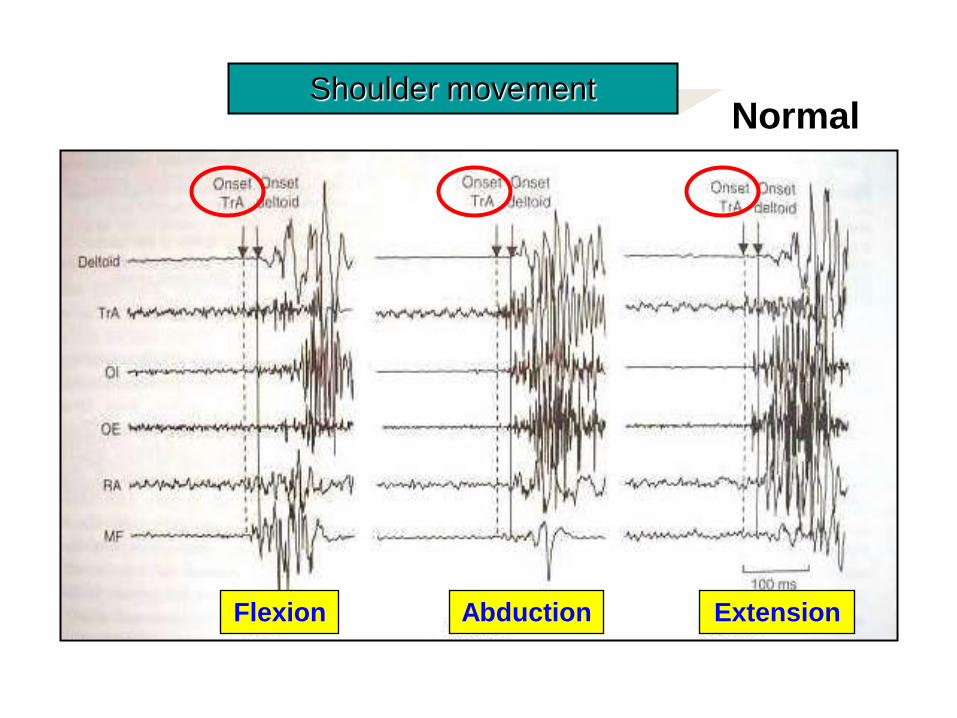
Shoulder movement Normal
Flexion Abduction Extension

the relaxed the drawn-in
The action of the transverse abdominis
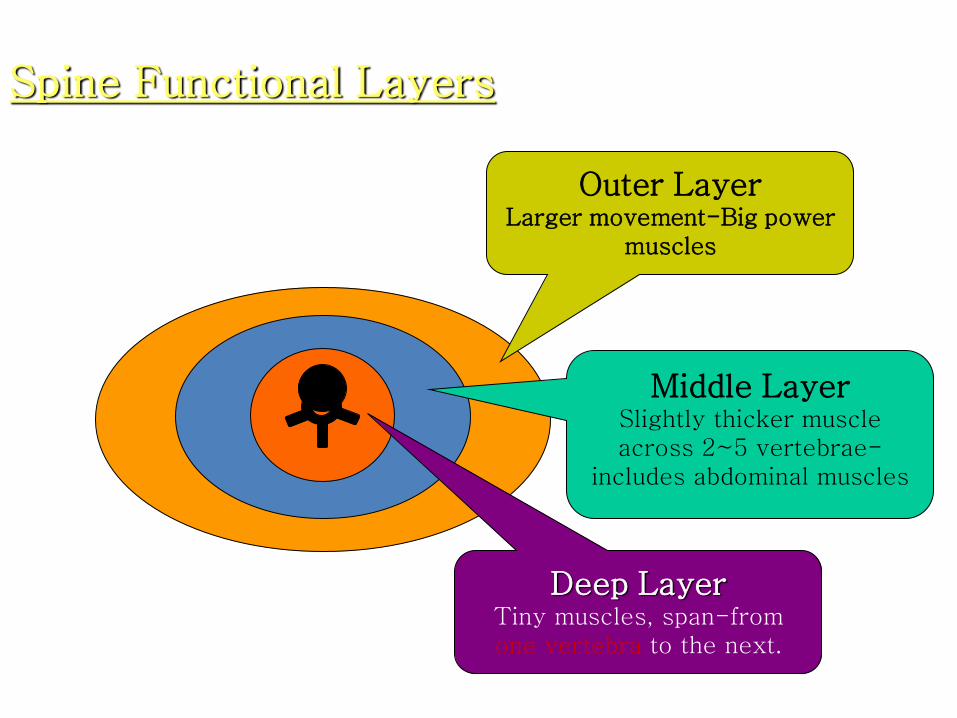
Spine Functional Layers
Outer Layer Larger movement-Big power
muscles
Middle Layer Slightly thicker muscle across 2~5 vertebrae-
includes abdominal muscles
Deep Layer Tiny muscles, span-from one vertebra to the next.

Current Trends
• Yoga
• Pilates
• Lumbar stabilization exercise
• Core exercise
• The CORE program

Peggy W. Brill, PT.

Purpose of exercise therapy
• Muscle strengthening in weak ms.
• Muscle Imbalance correction
• Stretching the shorten soft tissue
• Increase flexibility on the lumbar region
structures
• Correction of lumbar curvature

Exercise therapy
William ex. Emblass ex. Golthwaite ex. 신장 운동
· 체간 굴곡 운동 · 요추 전만 감소가 목적 · 전복부근, 대둔근, 슬 괵 근 능 동 적 근력강화 · 천극근, 고관절굴근, 대퇴직근 수동신장
· 요추 신전 운동 · HIVD·요통에 실시 · 운 동 강 도 의 점차적인 증가 · 휴식시간 및 운동 횟수 적절히 조정
· 만성 요통에 실시 · 척 추 배 부 근 의 근력강화
· 근육의 단축으로 자세이상을 가져왔을 때 실시 · 지속적 신장 권장

견인 시 고려사항
㉠ 견인력 : 누워있는 사람을 수평이동하기 위해 체중의 1/2에 해당하는 견인력 필요
㉡ 견인각 : Pelvic harness와 strap의 위치에 의해 결정
㉢ 견인자세 : 엎드려 누운 자세에서 실시

견인 치료시 적응증
적응증 금기증
· 추간판 탈출증 · 척추의 퇴행성 관절염 · 편타성 손상(채찍손상 · whiplash injury) · 오십견(frozen shoulder) · 사경(torticolis) · 변형성 척추증 · 추궁절제술 후 통증시 · 골연골증
· 척추 골절 · 종양 · 급성 염좌·좌상 · 심한 골다공증 · 식도열공 헤르니아(hiatus hernia) · 밀실공포증(Claustrophobia) · 척추분리증 · 임신 3~4개월경의 임산부

Recommend TX program
1. Precise diagnosis
2. Proper Intervention for reducing pain Ice or thermal TX
TENS (Pain) and U/S (Soft tissue)
Traction or other aiding material
3. Manipulation for fixing alignment of bony structures
4. Exercise Intervention for correct body alignment and recovery muscle function

Practice
• HNP (=SLR, compression)
• Facet syndrome (=extension)
• SI joint (=FABER test)
• Valsalva maneuver
• Pelvic alignment (leg length, PSIS)
• Palpation of spinous process (scoliosis)
• Correct vertebra

FABER test • Purpose: To assess for the sacroiliac joint or hip joint being the
source of the patient's pain.
• Test Position: Supine.
• Performing the Test: The patient's tested leg is placed in a "figure-
4" position, where the knee is flexed and the ankle is placed on
the opposite knee. The hip is placed in flexion, abduction, and
external rotation (which is where the name FABER comes from).
The examiner applies a posteriorly directed force against the
medial knee of the bent leg towards the table top. A positive test
occurs when groin pain or buttock pain is produced. Due to forces
going through the hip joint as well, the patient may experience
pain if pathology is located in the hip as well.
• http://www.youtube.com/watch?v=iYMqhWf7XVk

Sarcoiliac (SI) joint TX
• Mobilization
– http://www.youtube.com/watch?v=ptmt72Fxoq4&list
=PLee-9L8i_xLXbEnDXdWCnJnM4oMlG_aIb
– http://www.youtube.com/watch?v=tGDjpVvEo5Q
• Manipulation
– http://www.youtube.com/watch?v=NhwECwj3LDI





























