Embed Size (px)
Citation preview

7/23/2019 02-143
http://slidepdf.com/reader/full/02-143 1/9
27
Facial Characterization of Infants With Cleft Lip and Palate Using a
Three-Dimensional Capture Technique
C.A. HOOD, M.SC.D., F.D.S., R.C.P.S., B.D.S.
M.T. HOSEY, D.D.S. , M.SC. (MED SCI), F.D.S., R.C.P.S., B.D.S.
M. BOCK, PH.D., B.SC., B.MATH.(HONS)
J. WHITE, M.ORTH., F.D.S., R.C.P.S., B.D.S.
A. RAY, M.B.B.S., M.S., F.R.C.S.(PLAST)
A.F. AYOUB, PH.D., M.D.S., F.D.S., R.C.P.S., F.D.S.R.C.S., B.D.S.
Objective: To characterize the soft tissue features of infants with unilateral
cleft lip (UCL) and unilateral complete cleft lip and palate (UCLP) prior to pri-
mary surgery and compare with noncleft controls.
Design: Prospective controlled capture of the facial morphology of infants
using a noninvasive three-dimensional stereophotogrammetry method.
Participants: 23 children with presurgical cleft: 11 UCL (M 6, F 5); 12
UCLP (M 9, F 3), and 21 noncleft controls (M 7, F 14) were imaged at
approximately 3 months of age (range 10 to 16 weeks).
Main Outcome Measure: Accurate, repeatable quantification of facial soft tis-
sues in infants with clefts prior to surgery.Results: Significant differences (p .05) were found between the UCLP
group and UCL and control groups in anatomical and soft nose width, cleft-
side alar wing length, and nasal tip horizontal displacement. Both cleft groups
were significantly different from controls and from each other in cleft-side nos-
tril dimensions, alar wing angulation, columella angle, and alar base to corner
of mouth dimension; alar base width; and soft tissue defect in nose and the
lip and philtrum length bordering the cleft. Significant differences between
clefts and controls were identified in the nostril and philtrum on the noncleft
side.
Conclusions: The use of children with UCL as controls for UCLP studies is
inappropriate. This technique overcame the limitations of direct measurement
of infant faces to aid the surgeon in the planning and subsequent re-evaluation
of surgical rationale.
KEY WORDS: children, cleft lip, cleft lip and palate, facial morphology, infants,
presurgical, soft tissues, 3D, unilateral
The goals of surgical intervention for the repair of cleft lip
and palate are the restoration of normal morphology and func-
tion, without disruption of growth potential. However, the im-
pact of primary cleft surgery on facial growth is a subject of
continued debate. Attempts to unravel the compounding ef-
Dr. Hood is a Clinical Lecturer and Dr. Hosey is a Senior Clinical Lecturer/ Honorary Consultant in Pediatric Dentistry, Dr. Bock is a Lecturer, Department
of Statistics, Mr. White is a Clinical Lecturer in Orthodontics, and Professor
Ayoub is a Senior Clinical Lecturer/Honorary Consultant in Oral and Maxil-
lofacial Surgery and Head of Biotechnology and Craniofacial Research Group,
University of Glasgow, Glasgow, Scotland. Mr. Ray is a Consultant in Plastic
Surgery, Canniesburn Hospital, Glasgow.
This project has been funded by a grant from The Chief Scientist Office in
Scotland and The National Lottery Charities Board through CLAPA, UK. Grant
K/OPR/2/2/O366.
Submitted November 2002; Accepted February 2003.
Address correspondence to: Dr. Ashraf F. Ayoub, Glasgow Dental Hospital
and School, 378 Sauchiehall Street, Glasgow G2 3JZ, United Kingdom. E-mail
fects of tissue hypoplasia associated with the cleft defect itself,
and the consequences of surgery have been hindered by a lack
of objective means to quantify facial parameters in infancy. A
paucity of comparative normative data, and the perception that
early assessment of surgical outcome is not possible, further
complicates the picture.
Cephalometric studies have provided valuable information
about hard tissues and limited soft tissue information in youngchildren with clefts (Dahl et al., 1982; Hermann et al., 1999).
The use of cephalometric radiography, particularly in the
young patient, has been questioned (Shaw et al., 1992a, 1992b;
Mackay et al., 1994). Examination of the soft tissue profile of
individuals with orofacial clefts may indicate the extent of
maxillary hypoplasia and provide more significant information
about suture growth patterns than examination of hard tissues
(Shaw et al., 1992b). However, examination of soft tissue pro-
file provides only limited understanding of the relationships of
structures in the midline and cannot quantify aberrant anatom-

7/23/2019 02-143
http://slidepdf.com/reader/full/02-143 2/9
28 Cleft Palate–Craniofacial Journal, January 2004, Vol. 41 No. 1
ical position or asymmetry (Molsted et al., 1992). A full ap-
preciation of the complex deficiencies and 3-dimensional (3D)
nature of the cleft malformation is a prerequisite for quanti-
fying the magnitude of the anomaly and measuring change
following surgical repair.
Facial soft tissue characteristics of infants with untreated
cleft lip and cleft lip and palate have been reported by variousresearchers, employing a diversity of data collection methods
(Bacher et al., 1998; Fisher and Mann, 1998; Fisher et al.,
1999; Hermann et al., 1999; Hurwitz et al., 1999; Yamada et
al., 1999). With the exception of direct anthropometry studies
(Farkas, 1994; Mulliken et al., 2001), few have compared their
findings to a matched control group. When planning such in-
vestigations, quantitative examination methods require com-
parison with appropriate population norms (Farkas, 1997).
Moreover, the influence of racial or ethnic diversity on mor-
phometric findings should not be underestimated (Hajnis et al.,
1994).
Whatever method is adopted, the capture of an image of a
3-month-old infant remains a challenge. Despite considerableadvances in laser-scanning techniques (O’Grady and Antony-
shyn, 1999; Duffy et al., 2000), the time required for image
acquisition (10 to 13 seconds) precludes their use in young
children. Researchers have resorted to image capture or direct
measurement of facial morphology under general anesthesia,
immediately prior to operative procedures, despite the likeli-
hood of facial distortion by the presence of an endotracheal
tube (Hurwitz et al., 1999; Mulliken et al., 2001). Infant se-
dation has been necessary to allow collection of certain an-
thropometric measurements using calipers, particularly around
the eyes and nose (Farkas et al., 1993). Facial alginate im-
pressions, a technique so potentially hazardous as to require
an emergency intubation kit and the presence of a neonatolo-
gist, has also been advocated as a suitable data-gathering meth-
od in infants (Bacher et al, 1998). Although these various tech-
niques are noninvasive with respect to exposure to x-rays, they
require pharmacological intervention together with additional
support staff and facilities, which renders them less useful for
long-term monitoring of surgical outcome (Poswillo, 1990;
American Academy of Pediatric Dentistry 1999; Cote et al.,
2000).
The three-dimensional stereophotogrammetry (C3D) system
has been developed to overcome these difficulties. The system
allows noninvasive capture of 3D photorealistic facial mor-
phology in 50 milliseconds without the need for sedation. This
allows collection of serial records for monitoring treatment,
and comparing progressive outcomes in a practical, user-
friendly way. The development, clinical application, and re-
producibility of this technique have been previously reported
(Ayoub et al., 1997, 1998, 2003; Al-Omari et al., 2003; John-
son et al., 2003).
The aims of this investigation were to characterize the facial
soft tissue features in infants with unilateral cleft lip (UCL)
and complete unilateral cleft lip and palate (UCLP), prior to
cheiloplasty, and compare these soft tissue findings with a peer
group control.
METHOD
Ethical approval was granted from North Glasgow Univer-
sity Hospitals NHS Trust and Royal Hospital for Sick Children
NHS Trust local ethics committees. There are comprehensive
mechanisms for the recording and documentation of all cleft
births in Scotland (Scottish Congenital Anomalies Register atthe Information and Statistics Division of the Common Ser-
vices Agency).
Identification and recruitment of children with cleft was un-
dertaken in consultation with National Managed Clinical Net-
work for Cleft Services in Scotland (CLEFTsis).
Twenty-three children with unilateral clefts, 11 (six boys,
five girls) with UCL and 12 (nine boys, three girls) with UCLP,
had 3D images captured prior to surgical intervention, at ap-
proximately 3 months of age (range 10 to 16 weeks). 21 age-
matched infant controls (7 boys, 14 girls) were recruited
through maternity units and baby clinics in Glasgow.
The C3D system configured for clinical facial imaging con-
sists of two pods, each with three cameras. Two monochromecameras serve to form a stereo baseline and are synchronized
to capture images illuminated by special texture flash projec-
tors. A third color camera captures the natural photographic
appearance of the subject under normal white-light flash.
The system was calibrated before and after each capture
session. A calibration target of accurately known dimensions
was imaged in a variety of target poses, built, and attached to
the sets of captured images. This contains the necessary in-
formation required to create a depth map. Several sets of facial
images were captured in the same session and those with facial
expression at rest (minimal muscle activity) selected and built
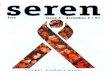
at low resolution (0.005 voxel size). Built 3D range data were
examined for smoothness, integrity (Fig. 1C) and evidence of
intrinsic or extrinsic movement (such as blinking, changes in
facial expression during image capture). The desired models
were then edited to remove extraneous background material
and built at high resolution (0.002 voxel size). The final part
of the selection process involved examination of the color tex-
ture map, and the best quality model for each individual was
then selected for analysis. This final C3D output can be viewed
as a solid wire frame or shaded model (Fig. 1A through 1C).
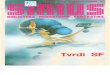
Infants were photographed at rest, on a parent’s lap, looking
slightly upward toward the operator (Fig. 2). 3D models were
built and anthropometric landmarks (Table 1, Fig. 3) identified
on each using the Facial Analysis Tool, custom software that
allows model manipulation and analysis on a computer screen.
To facilitate direct comparison, models of children with right-
sided clefts were reflected so that every cleft appeared on the
left side. Models were orientated to a standard position, and
two operators (C.A.H., J.W.) systematically identified highly
reproducible sets of 35 landmarks (average placement error 0.5
mm). Operators were trained in placement of anthropometric
landmarks and calibrated (intraoperator error 0.5 mm, inter-
operator error 0.81 mm). Selection of landmarks on screen
generates a set of x, y, and z coordinates, which describe the
spatial orientation of facial features. Linear distances angles

7/23/2019 02-143
http://slidepdf.com/reader/full/02-143 3/9
Hood et al., 3D PRESURGICAL FACIAL CHARACTERIZATION 29
FIGURE 1. Output of three-dimensional stereophotogrammetry (C3D) system. A. Photorealistic solid C3D model. B. Wire frame. C. Shaded C3D model
illustrating smooth range data.
FIGURE 2. Three-dimensional stereophotogrammetry camera set-up.
Child is imaged, unrestrained, on a parent’s lap. Capture time is 50 mil-
liseconds.
and ratios defining key facial parameters were generated (Table
2) using the Facial Analysis software.
One-way analysis of variance statistical tests were per-
formed to compare mean individual measurements in all three
groups ( p .05). Tukey’s multiple comparison test calculated
confidence intervals for each possible pair of groups.
RESULTS
In an effort to report on the findings in this study in a clin-
ically meaningful way, the results are grouped according to
facial region. These are presented in terms of the cleft defor-
mity (i.e., UCL and UCLP) and then compared with the con-
trol group. The ear landmarks were difficult to identify in some
models and excluded from this analysis. The complete expo-
sition of the results is shown in Table 3.
Upper Face
Compared with controls, intercanthal width was significant-
ly increased in the UCLP group but not the UCL group. On
the cleft side, the distance from nasion to endocanthion was
longer in UCL and UCLP, compared with controls. Although
this was more marked in the UCLP group, the difference be-
tween cleft groups was not significant. There were no differ-
ences in ocular and biocular widths between cleft groups and
controls.
Nostril Dimensions
In both cleft groups, the cleft-side nostril was significantly
increased in all dimensions, compared with controls. There
were highly significant differences in the noncleft side nostril,
compared with controls. Nostril long axis and nostril floor
widths were increased in UCL and UCLP, relative to controls,
but there were no significant differences between the cleft
groups.
Nose: Horizontal Dimensions
Both cleft groups had significantly increased alar base
widths, compared with controls. This dimension was also sig-
nificantly wider in the UCLP group than the UCL group.
Soft nose width (al-al) and anatomic nose width (ac-ac)
were increased in the UCLP group but not the UCL group.
There were no differences in soft nose width: mouth width
ratios between groups but, as expected, an increased anatomic
nose base width; mouth width ratio was detected in the UCLP
group.
The size of the soft tissue defect in the nose is gauged by
the difference in cleft and noncleft side nostril floor widths.

7/23/2019 02-143
http://slidepdf.com/reader/full/02-143 4/9
30 Cleft Palate–Craniofacial Journal, January 2004, Vol. 41 No. 1
TABLE 1 Landmark Definitions*
Region Landmark Definition
Eyes
Eyes
Eyes
Eyes
Forehead
1
2
3
4
5
enL
enR
exL
exR
n
Endocanthion, left
Endocanthion, right
Exocanthion, left
Exocanthion, right
Nasion
NoseNose
Nose
Nose
Nose
67
8
9
10
prnsn
sn0R
sn0L
cR
PronasaleSubnasale
Edge of the collumellar base right
Edge of the collumellar base left
Highest point of the collumella (reflected onto nostril) right
Nose
Nose
Nose
Nose
Nose
11
12
13
14
15
cL
sbalL
sbalR
acL
acR
Highest point of the collumella (reflected onto nostril) left
Subalare left
Subalare right
Alar left
Alar right
Nose
Nose
Nose
Nose
Nose
16
17
18
19
20
alL
alR
al0oL
al0oR
al0iL
Alare left
Alare right
Midpoint on outer margin of left ala, opposite al0iL
Midpoint on outer margin of right ala, opposite al0iR
Midpoint on outer margin of nostril left
Nose
Lips
LipsLips
Lips
21
22
2324
25
al0iR
chR
chLcphR
Is
Midpoint on outer margin of nostril right
Cheilion right
Cheilion leftCrista philtri right
Labiale superioris
Lips
Lips
Lips
Lips
Lips
26
27
27
28
29
cph0R
cphL
cphL
stoi
li
Crista philtri landmark surrogate on major segment, bordering cleft (left-sided cleft)
Crista philtri landmark surrogate on minor segment, cleft side (left-sided cleft)
Crista philtri left, controls only
Stomion inferioris
Labiale inferioris
Lips
Other
Other
Other
Other
Other
30
31
32
33
34
35
sl
pg
obsR
obsL
obiR
obiL
Sublabialis
Pogonion
Otobasion superior right
Otobasion inferior left
Otobasion superior right
Otobasion superioris left
* Farkas, 1990, 1994; Hurwitz et al., 1999; Duffy et al., 2000.
FIGURE 3. Photokey showing positions of anthropometric landmarks.
On average, there was a 2-mm discrepancy in the UCL group,
rising to 10 mm in the UCLP group.
Nose: Vertical Dimensions
In the UCL group, there were no differences in nose dorsum
length or nasal tip base (sn-prn), in comparison with controls.
In the UCLP group, nose dorsum length was longer than in
both the controls and UCL group.
As with the UCL group, there was no difference in nasal
tip–base distance in the UCLP group; however, nasal tip an-
gulation was increased in both cleft groups, highlighting flat-
tening and skewing of the nasal tip in the preoperative face.
Lateral nose dorsum lengths were similar in clefts and controls.
Alar Wing
The length of the alar wing on the cleft side was increased
only in the UCLP group. The UCL group had normal alar
lengths on both the cleft and noncleft sides.
Alar wing angulation was more acute on the noncleft side,
with a corresponding obtuse angle on the cleft side in the
UCLP group. However, this feature was not found in the UCL
group, reflecting the lesser degree of nasal tip displacement
and alar wing flattening in these children.
Columella
The width and height of the columella were normal in the
cleft groups. The columella angle on the cleft side, however,
was more obtuse in both cleft groups. There was no corre-
sponding decrease in columella angle on the noncleft side.

7/23/2019 02-143
http://slidepdf.com/reader/full/02-143 5/9
Hood et al., 3D PRESURGICAL FACIAL CHARACTERIZATION 31
TABLE 2 Facial Measurements, Ratios, and Angle Definitions*
Measurement Definition
Upper face
Biocular width
Ocular width
Intercanthal width
Endocanthion to nasion
ex-ex
ex-en
en-en
en-n
Nostril Dimensions
Nostril floor width
Nostril long axis 1
Nostril width 2
sbal to sn0
sbal-c
sn0-al0i
Nose horizontal dimensions
Alar base width
Anatomic nose width (alar base facial insertion width)
Soft nose width
Anatomic nose base/mouth width ratio
Soft nose/mouth width ratio
Size of soft tissue defect in the nose difference between L&R nasil floor widths
Nasal tip horizontal displacement (angle)
sbal-sbal
ac-ac
al-al
ac-ac:ch-ch
al-al:ch-ch
(sbalL-sn-0L)-(sbalR-sn0R)
acR-prn-acL
Nose vertical dimensions
Nose dorsum length
Lateral nasal length
Nasal tip-base
Nasal tip angulation
n-prn
en-ac
sn-prn
n-prn-sn
Alar wing
Projective alar length
Alar wing angulation (R&L)
ac-prn
ac-prn-sn
Columella
Columella height
Columella thickness
Columella angulation (R&L)
sn0-c
sn0-sn0
sbal-c-sn0
Mouth
Lower lip length
Lower lip vermillion height
Mouth width
stoi-sl
stoi-li
ch-ch
Philtrum
Size of defect in midportion of upper lip difference in paramedial vertical upper lip heights on noncleftand cleft sides
Size of cleft in upper lip distance between philtral points
Medial height of upper lip skin
Philtral point to ipsilateral corner of mouth
Philtral point to ipsilateral alar base
Alar base to ipsilateral corner of the mouth
(sn0-cph0)-(sn0-cph)
cph-cph
sn-ls
cph-ch (noncleft side) chp-ch (cleft side)
cph-sbal (noncleft side) cph-sbal (cleft side)
sbal-ch
Others
Nasolabial angle
Protrusion of Is relative to sn
Upper face height
Face height
prn-sn-Is
Is-n-sn
n-sn
n-pg
Mouth
Mouth width was unaffected by the presence of a cleft.
Compared with controls, cph-ch (corner of mouth to high point
Cupid’s bow) was shorter on cleft side in UCL but not on the
noncleft side. In contrast, in UCLP this distance was shorter
on both the cleft and noncleft sides.
There were no differences in upper lip lengths on the cleft
side between controls and UCLP or UCL groups. However, on
the noncleft side, this dimension was significantly shorter in
the UCL group.
Philtrum
The paramedial philtrum length on the noncleft side was sig-
nificantly shorter in the UCL group, compared with controls.
There were no significant differences seen in the UCLP group,
however. On the opposite side of the philtrum, bordering the cleft,
both the UCL and UCLP groups showed significant shortening
of the opposite side of the philtrum.
Comparison of the paramedial philtrum dimensions, on the
noncleft side and bordering the cleft, gave an indication of the
quantitative defect in the midportion of the upper lip. In the

7/23/2019 02-143
http://slidepdf.com/reader/full/02-143 6/9
32 Cleft Palate–Craniofacial Journal, January 2004, Vol. 41 No. 1
TABLE 3 Facial Measurements: UCL, UCLP, and Control Groups at 3 Months†
Measurements
Mean (mm)
Control UCL UCLP
ANOVA
Value
Tukey’s Confidence Interval
UCL:Control UCLP:Control UCL:UCLP
Upper face
exL-exR
exL-enL
exR-enRenL-enR
enL-n
enR-n
65.75
20.39
20.2726.71
14.70
15.51
65.65
20.43
20.1926.77
16.42
15.93
67.12
20.25
19.9128.42
17.53
15.68
.429
.932
.801
.043*
.000***
.772
2.88/ 0.56
3.4/ 0.02
3.96/ 1.70
Nostril dimensions
sbalL-sn0L
sbalR-sn0R
sbalL-cL
sbalR-cR
sn0L-al0iL
sn0R-al0iR
4.54
4.20
6.08
5.81
4.39
4.75
7.19
5.05
7.84
6.99
6.09
5.18
16.20
5.53
15.33
7.74
9.65
5.05
.000***
.000***
.000***
.000***
.000***
.486
4.44/ 0.85
1.55/ 0.15
3.4/ 0.12
1.99/ 0.37
2.55/ 0.83
13.41/ 9.92
2.01/0.65
10.84/ 7.65
2.71/ 1.14
6.09/ 4.42
11.03/ 7.0
9.32/ 5.65
4.53/ 2.59
Nose horizontal dimensions
sbalL-sbalR
acL-acR
alL-alR
acL-acR:chL-chR
alL-alR:chL-chR(sbalL-sn0L)-(sbalR-sn0R)
10.80
24.85
22.44
0.87
0.780.25
15.21
25.14
20.30
0.88
0.702.14
23.77
30.45
25.12
0.97
0.8010.68
.000***
.000***
.002**
.000***
0.71.000***
6.63/ 2.2
3.66/ 0.14
15.12/ 10.82
7.41/ 3.78
5.3/ 0.06
0.18/ 0.04
12.14/ 8.72
11.04/ 6.07
7.4/ 3.21
7.83/ 1.8
0.18/ 0.02
10.51/ 6.56
Nose vertical dimensions
n-prn
enL-acL
enR-acR
sn-prn
n-prn-sn
19.59
19.42
19.45
9.85
111.18
21.15
19.43
18.94
9.28
118.42
21.55
20.56
20.51
9.14
122.15
.015*
.165
.080
.100
.000*** 12.14/ 2.33
3.69/ 0.25
15.74/ 6.2
Alar wing
acL-prn
acR-prn
(acR-prn)-(acL-prn)
acR-prn-sn
acL-prn-sn
acR-prn-acL
16.13
16.80
0.67
53.81
53.99
98.30
16.82
16.38
0.44
46.32
60.29
98.32
21.23
16.80
4.43
43.43
74.51
105.72
.000***
.660
.000***
.000***
.000***
.001**
1.82/13.16
11.14/ 1.46
6.72/ 3.49
3.49/6.71
4.85/15.89
25.22/ 15.81
12.17/ 2.68
6.27/ 2.54
2.13/5.85
19.64/ 8.79
12.87/ 1.93
Collumella
sn0L-cLsn0R-cR
sn0R-sn0L
sbalL-cL-sn0L
sbalR-cR-sn0R
2.222.35
5.13
37.84
36.41
1.852.61
4.93
62.16
32.59
1.982.76
4.68
114.49
29.63
.312
.382
.354
.000***
.449
43.53/ 9.94 90.55/ 57.87 66.15/ 28.8
Mouth
chR-chL
cphR-chR
cphL-chL
28.91
17.90
17.78
28.78
16.62
14.01
31.39
15.68
11.61
.052
.025*
.000*** 1.0/6.55
0.3/4.17
3.47/8.87
Lower lip
sl-stoi
li-stoi
10.86
5.62
9.97
4.04
10.28
4.23
.090
.000*** 0.75/2.39 0.59/2.18
Philtrum
cphR-sn0R
cphR-sbalR
cphL-sn0L vs cph0R-sn0L
ls-sn
sbalL-chL
11.99
10.41
11.97
10.76
22.65
9.26
8.13
6.32
6.91
20.07
11.16
10.19
4.60
6.95
17.57
.003**
.020*
.000***
.000***
.000***
0.94/4.53
0.33/4.22
4.14/7.16
2.43/5.27
0.6/4.57
5.9/8.84
2.42/5.18
3.16/7.02
0.02/3.42
0.28/4.73
sbalR-chR
cphL-cphR vs cphL-cphR
cph-ls vs cph0R-ls
cphL-sbalL
cphR-ls
23.08
6.38
3.31
9.93
3.37
20.07
15.28
2.79
11.17
2.84
20.44
19.95
3.03
8.33
3.70
.000***
.000***
.090
.111
.217
1.04/4.97
11.72/ 6.09
0.73/4.55
16.31/ 10.83 7.83/ 1.51
Other
prn-sn-ls
ls-n-sn
n-pg
n-sn
138.74
2.64
58.08
24.88
137.50
2.31
58.80
26.83
136.21
2.92
58.82
27.53
.716
.658
.879
.001** 3.75/ 0.16 4.4/ 0.91
† VCL unilateral cleft lip; UCLP complete unilateral cleft lip and palate; ANOVA analysis of variance.
* p .05; ** p .01; *** p .001.

7/23/2019 02-143
http://slidepdf.com/reader/full/02-143 7/9
Hood et al., 3D PRESURGICAL FACIAL CHARACTERIZATION 33
UCL group, the mean was 2.94 mm on average, and in the
UCLP group, the mean was 6.56 mm.
Medial philtrum length (sn-ls) was significantly shorter in
both UCL and UCLP, regardless of severity of cleft.
In both cleft groups, the distance from the alar base to the
corner of the mouth on the cleft and noncleft sides was shorter,
compared with controls. Furthermore, on the cleft side, thisdistance was significantly shorter in the UCLP group, com-
pared with the UCL group.
The average size of the cleft in the upper lip was greater in
the UCLP group, 19.95 mm, compared with 12.46 mm in the
UCL group.
Lower Lip
There were no significant differences among the three
groups in respect of total lower lip length. However, lower
vermillion length was significantly shorter in both cleft groups,
compared with controls.
Other Features
Nasolabial angles in the cleft groups were similar to con-
trols. There were no significant differences in upper lip prom-
inence between cleft groups and controls, measured by the
position of the center of Cupid’s bow relative to the columella
base.
Upper face height (n-sn) was increased in the cleft groups.
Face height, measured from nasion to pogonion (n-pg), was
similar in both the cleft and control groups.
DISCUSSION
Dahl (1970) described the differences found in UCL as mild
and limited to the cleft region. Other hard tissue studies of
children with clefts have supported the use of the child with
UCL as a ‘‘control’’ (Hermann et al., 1999). This approach
cannot be adopted for the study of soft tissues because of the
heterogeneity of clefts affecting the lip and primary palate. Our
study found significant differences among the UCL, UCLP,
and control groups in a number of soft tissue parameters.
Where the UCL group differed from controls, this was also
expressed as a significant difference in the UCLP group, com-
pared with controls, with one notable exception: philtrum di-
mensions on the noncleft side.
In general, significant differences between the UCL and
UCLP groups occurred in soft tissue parameters in which the
UCL group was more like controls (anatomical and soft nose
width, cleft-side alar wing length, and nasal tip horizontal dis-
placement). In addition, significant differences were found in
which cleft groups differed not only from controls but also
from each other (cleft-side nostril dimensions, alar wing an-
gulation, columella angle, alar base to corner of mouth dimen-
sion, alar base width; soft tissue defect in the nose and lip,
philtrum cleft border).
Comparison of other cleft groups with a UCL ‘‘control’’
group will cloud the analysis of the effects of surgical inter-
ventions on facial growth. The findings in this study reinforce
the need for peer group comparison with matched children
without cleft.
Scotland has a particular predilection for congenital malfor-
mations, and approximately 100 new cases of orofacial clefting
occur each year. In common with Northern Ireland, there is aremarkably high ratio (almost 1:1) of cleft lip and cleft lip and
palate to isolated cleft palate in the Scottish population (Wom-
ersley and Stone, 1987; FitzPatrick et al., 1994; Gregg et al,
1994; Stone and Dolk, 1994). This is not typical of the United
Kingdom or other cleft centers, generally, in which the ratio
is 2:1. Farkas (1997) recommended that ethnically and racially
differing regions should develop their own control population
norms for statistical analysis. This is the first report to char-
acterize the facial soft tissues of Caucasian infants with cleft
lip and cleft lip and palate in the Scottish population, prior to
primary repair.
Although the children were matched for age, there were
more girls than boys in the control group. The possibility of sexual dimorphism was not explored. However, a recent study
by Yamada (Yamada et al., 2002a) demonstrated few sex dif-
ferences in the facial soft tissues in infants. Moreover, the se-
verity of the cleft deformity may ‘‘mask’’ sex differences pre-
operatively, as has been reported in hard tissue studies (Krog-
man et al., 1982). Much larger sample sizes will be required
to consider this further.
Increased intercanthal width has been previously described
in studies of children with cleft lip (Dahl et al., 1982; Friede
et al., 1986). In this study, increased intercanthal width was a
feature of the UCLP group but not the UCL group. Biocular
width (exR-exL) and right and left ocular widths were of nor-
mal proportion. The increased intercanthal width in the UCLP
group could be explained by an apparent increased distance
from inner canthus to nasion on the cleft side. This dimension
was also significantly increased in the UCL group, which sug-
gests subtle variation in anteroposterior position of the eye
between cleft types. Linear analysis alone cannot explain this
fully, and a more comprehensive 3D analysis is warranted.
The increase in the upper face height in both cleft groups
in this study is in agreement with that reported by other re-
searchers (Farkas, 1990).
Although our study did not examine individual landmark
positions, our finding of increased nasal floor width on the
noncleft side confirms that the noncleft subalare (sbal) is dis-
placed in relation to the columellar base. Indeed, Fisher et al.
(1999) noted that this point was farther from the midline than
that on the cleft side and that there was a marked deviation of
the columellar base, subnasale (sn), from the midline. Given
that the surgeon uses the noncleft side as a frame of reference
to correct asymmetry, increased nostril dimensions could have
implications for residual nasal deformity, particularly in func-
tion. This may require consideration at the time of cleft repair.
During cleft surgery, the alar base is an important clinical
dimension to correct. The width of the alar base of the nose
(sbal-sbal) in UCLP was more than twice that found in con-

7/23/2019 02-143
http://slidepdf.com/reader/full/02-143 8/9
34 Cleft Palate–Craniofacial Journal, January 2004, Vol. 41 No. 1
trols. In the UCL group, this dimension was also increased,
but the alar base facial insertion (ac-ac) was similar to controls.
These findings can be explained by the more lateral and in-
ferior position of the subalare point on the cleft side and ever-
sion of the alar base. This is in response to the torque effect
produced by contraction of facial muscles that have lost their
medial insertion, but deeper soft tissue remains anchored toperiosteum (Malek, 2001). An exaggeration of this effect is
seen in UCLP and compounded by flattening and elongation
of the ala on the cleft side, evident in the increased anatomical
and soft nose widths and shortening of the distance from the
corner of mouth to the alar base on the cleft side.
Proportion ratios of nose base and mouth widths have been
advocated in the assessment of surgical outcome and residual
deformity (Vegter et al., 1997). Farkas et al. (1993) proposed
that anatomical nose width was better determined between ac-
ac, as opposed to al-al, because this is really a measure of soft
nose width. In our study we chose to measure both dimensions
and then calculate proportion indices (Table 2). We found that
mouth widths were similar in both cleft groups and controls.Even though both al-al and ac-ac were significantly increased
in the UCLP group, the nose base: mouth width ratio did not
reflect this, when the al-al:ch-ch was used as a basis for the
proportion calculation. In contrast, a proportion index based
on ac-ac:ch-ch showed significant differences between the
UCLP group and controls. The use of soft nose width (al-al)
in calculations of nose:mouth width ratios may render the mea-
sure too insensitive for the detection of subtle morphological
differences in young children.
Both cleft groups’ collumellae were displaced but of normal
height and width. A more obtuse angle was found on the cleft
side in both the cleft groups, but there was no corresponding
decrease in columellar angle on the noncleft side. The displace-
ment of the noncleft subalare point may be masking this feature.
In infants with UCLP, nose dorsum dimensions, cleft-side
alar wing dimensions, and nasal tip angulation characterize the
flattening and horizontal skewing of the nasal tip in one di-
rection and the columella base in the other. In common with
other studies (Hurwitz et al., 1999; Duffy et al., 2000; Yamada
et al., 2002a), the point chosen to represent the most prominent
anterior point of the nose (prn) does not necessarily coincide
with the anatomical tip. Inherent difficulties in the identifica-
tion and reproducibility of the anatomical tip necessitate the
selection of a close surrogate.
Few researchers have managed to quantify nostril shape in
children. Using this morphometric approach, we were able to
map important nostril parameters in young children with cleft
lip and palate prior to surgical intervention.
Hermann et al. (1999) reported a more prominent upper lip
in UCLP measured in profile from cephalometric radiographs.
This feature was not found in this study. In children with clefts,
unopposed cleft orbicularis oris fibers together with major
maxillary segment rotational displacement combined to pro-
duce unilateral shortening of the upper lip. This becomes even
more striking because of the tilt or inclination of Cupid’s bow
(Fisher and Mann, 1998; Fisher et al., 1999; Hermann et al.,
1999; Hurwitz et al., 1999; Yamada et al., 1999). The present
study showed that short philtrum and upper lip dimensions
were a feature of the UCL group on the noncleft as well as
on the cleft side. In contrast, the UCLP group had normal
philtrum dimensions on the noncleft side, although signifi-
cantly decreased distances bordering the cleft. We can postu-
late that this is the result of outward rotational muscular pullon the lip soft tissues in UCL, whereas in UCLP there is com-
plete bone separation of the segments, with concomitant major
segment displacement; the net effect is less tension on the lip
soft tissues on the noncleft side.
Mouth widths in infants with cleft were similar to noncleft
controls. This is an important baseline to establish because
mouth width is a useful outcome measure following surgery.
Indeed, significantly narrower mouth widths have been re-
ported in studies of older children and adults with cleft (Farkas
and Lindsay, 1973; Zhu et al., 1994)
The width of the lower lip was significantly shorter in both
cleft groups, compared with controls. All children in this study
were photographed at rest, with a lip-apart posture. Anthro-pometric measurements relating to lower lip and vertical
mouth dimensions should not rely on the stomion landmark
(sto), which must be identified with the lips together. It is well
documented that young children with clefts are obligate mouth
breathers (Hairfield et al., 1988), and a posture of ‘‘lips to-
gether at rest’’ is not achievable. Many of the authors who use
an anthropometric landmark-based approach fail to acknowl-
edge this point (Hurwitz et al., 1999; Mishima et al., 2002;
Yamada et al., 2002a, 2002b). In view of this, the stomion
inferior (stoi) landmark was selected for our analysis. Stomion
superior (stos) does not exist in the preoperative cleft face,
but, in practical terms, measuring lower vermillion height
helps estimation of upper vermillion height, which has impli-
cations for the design of surgical approach.
A quantitative assessment of facial asymmetry should be
included in any evaluation of craniofacial anomaly. This is an
area for future study (Hood et al., 2002). Nevertheless, the
indirect C3D anthropometry technique can overcome many of
the limitations of direct measurement of infant faces, with the
added benefit of a 3D coordinate–based analysis. Accurate,
repeatable soft tissue measurement can be used to quantify
characteristics of the cleft condition in advance of surgery and
so aid the surgeon in the planning and subsequent re-evalua-
tion of surgical rationale.
CONCLUSIONS
This study demonstrated the use of a noninvasive C3D ap-
proach to facilitate the objective comparison of cleft defects.
Significant differences were identified between infants with
unilateral clefts of the lip and primary palate and UCLP and
age-matched noncleft peer group controls.
The development of appropriate local baselines to establish
the normal facial character within any given population should
be seen as a prerequisite for comparison of surgical outcomes.
The C3D system provides a possible solution to the problem

7/23/2019 02-143
http://slidepdf.com/reader/full/02-143 9/9
Hood et al., 3D PRESURGICAL FACIAL CHARACTERIZATION 35
of standardization of methods of interpretation of findings be-
fore surgery and during follow-up. This will facilitate objec-
tive comparison of results of different surgical techniques and
timings of cleft repair in the future.
REFERENCES
Al-Omari I, Millett D, Ayoub A, Bock M, Ray A, Dunaway D, Crampin L.
An appraisal of three methods of rating facial deformity in-patients with
repaired complete unilateral cleft lip and palate. Cleft Palate Craniofac J.
2003;40:530–537.
American Academy of Pediatric Dentistry. Guidelines for the elective use of
conscious sedation, deep sedation and general anesthesia in pediatric dental
patients: reference manual 1999–2000. Pediatr Dent. 1999;21:68–73.
Ayoub AF, Garrahy A, Hood CA, White J, Bock M, Siebert P, Spencer R, Ray
A. Validation of a vision based three-dimensional facial imaging system.
Cleft Palate Craniofac J. 2003;40:523–527.
Ayoub AF, Siebert P, Moos KF, Wray D, Urquhart C, Niblett TB. A vision-
based three-dimensional capture system for maxillofacial assessment and
surgical planning. Br J Oral Maxillofac Surg. 1998;36:353–357.
Ayoub AF, Wray D, Moos KF, Jin J, Niblett TB, Urquhart C, Mowforth P,
Siebert P. A three-dimensional imaging system for archiving dental studycasts: a preliminary report. Int J Adult Orthodon Orthognath Surg. 1997;
12:79–84.
Bacher M, Goz G, Pham T, Bacher U, Werner O, Buchner P, Bacher A. Three-
dimensional analysis of cleft palate topology in newborn infants with ref-
erence to the cranial skeleton. Cleft Palate Craniofac J. 1998;35:379–395.
Cote C, Karl HW, Notterman DA, Weinberg JA, McCloskey C. Adverse se-
dation events in pediatrics: analysis of medications used for sedation. Pe-
diatrics. 2000;106:633–644.
Dahl E. Craniofacial morphology in congenital clefts of the lip and palate. Acta
Odontol Scand. 1970;28(Suppl):57.
Dahl E, Kreiborg S, Jensen BL, Fogh-Andersen P. Comparison of craniofacial
morphology in infants with incomplete cleft lip and infants with isolated
cleft palate. Cleft Palate J. 1982;19:258–266.
Duffy S, Noar JH, Evans RD, Sanders R. Three-dimensional analysis of the
child cleft face. Cleft Palate Craniofac J. 2000;37:137–144.
Farkas LG. Anthropometry of the face in cleft patients. In: Bardach J, Morris
HL, eds. Multidisciplinary Management of Cleft Lip and Palate. Philadel-
phia: Saunders; 1990:474–482.
Farkas LG. Anthropometry of the Head and Face. 2nd ed. New York: Raven
Press; 1994.
Farkas LG. Clinical evaluation of facial morphology in cleft lip palate patients.
Plast Reconstr Surg. 1997;99:262–263.
Farkas LG, Hajnis K, Posnick JC. Anthropometric and anthroposcopic findings
of the nasal and facial region in cleft patients before and after primary lip
and palate repair. Cleft Palate Craniofac J. 1993;30:1–12.
Farkas LG, Lindsay WK. Morphology of the adult face following repair of
unilateral cleft lip and palate in childhood. Plast Reconstr Surg. 1973;52:
652–655.
Fisher DM, Lo LJ, Chen YR, Noordhoff MS. Three-dimensional computed
tomographic analysis of the primary nasal deformity in 3-month-old infants
with complete unilateral cleft lip and palate. Plast Reconstr Surg. 1999;103:1826–1834.
Fisher DM, Mann RJ. A model for the cleft lip nasal deformity. Plast Reconstr
Surg. 1998;101:1448.
FitzPatrick DR, Raine PA, Boorman JG. Facial clefts in the west of Scotland
in the period 1980–1984: epidemiology and genetic diagnoses. J Med Genet.
1994;31:126–129.
Friede H, Figueroa AA, Naegele ML, Gould HJ, Kay C N, Aduss H. Cranio-
facial growth data for cleft lip patients infancy to 6 years of age: potential
applications. Am J Orthod Dentofacial Orthop. 1986;90:388–409.
Gregg T, Boyd D, Richardson A. The incidence of cleft lip and palate in North-
ern Ireland from 1980–1990. Br J Orthod. 1994;21:387–392.
Hairfield WM, Warren DW, Seaton DL. Prevalence of mouth breathing in cleft
lip and palate. Cleft Palate J. 1988;25:135–138.
Hajnis K, Farkas LG, Ngim RCK. Racial and ethnic morphometric differences
in the craniofacial complex. In: Farkas LG, ed. Anthropometry of the Head
and Face. New York: Raven Press; 1994:201–218.
Hermann NV, Jensen BL, Dahl E, Bolund S, Kreiborg S. A comparison of the
craniofacial morphology in 2-month-old unoperated infants with unilateral
complete cleft lip and palate, and unilateral incomplete cleft lip. J Craniofac
Genet Dev Biol. 1999;19:80–93.
Hood CA, Bock M, Hosey MT, Ayoub A. Facial Asymmetry—3D assessment
of infants with cleft lip and palate. Presented at the Annual Scientific Meet-
ing of BSPD; Sheffield, United Kingdom; 2002. Int J Paed Dent. 2002;12:
381–382.
Hurwitz DJ, Ashby ER, Llull R, Pasqual J, Tabor C, Garrison L, Gillen J,
Weyant R. Computer-assisted anthropometry for outcome assessment of
cleft lip. Plast Reconstr Surg. 1999;103:1608–1623.
Johnston D, Millett D, Ayoub A, Bock M. Are facial expressions reproducible?
Cleft Palate Craniofac J. 2003;40:291–296.
Krogman WM, Jain RB, Long RE. Sex differences in craniofacial growth from
one month to ten years of cleft lip and palate. Cleft Palate J. 1982;19:62–71.
Mackay F, Bottomley J, Semb G, Roberts C. Dentofacial form in the five-year-
old child with unilateral cleft lip and palate. Cleft Palate Craniofac J. 1994;
31:372–375.
Malek R. The lip and nose. In: Cleft Lip and Palate: Lesions, Pathophysiologyand Primary Treatment. London: Martin Dunitz, 2001:29–102.
Mishima K, Mori Y, Yamada T, Sugahara T. Anthropometric analysis of the
nose in the Japanese. Cells Tissues Organs. 2002;170:198–206.
Molsted K, Asher-McDade C, Brattstrom V, Dahl E, Mars M, McWilliam J,
Plint DA, Prahl-Andersen B, Semb G, Shaw WC. A six-center international
study of treatment outcome in patients with clefts of the lip and palate: Part
2. Craniofacial form and soft tissue profile. Cleft Palate Craniofac J. 1992;
29:398–404.
Mulliken JB, Burvin R, Farkas LG. Repair of bilateral complete cleft lip: intra-
operative nasolabial anthropometry. Plast Reconstr Surg. 2001;107:307–314.
O’Grady KF, Antonyshyn OM. Facial asymmetry: three-dimensional analysis
using laser surface scanning. Plast Reconstr Surg. 1999;104:928–937.
Poswillo DE. General Anaesthesia, Sedation and Resuscitation in Dentistry.
Report of an expert working party prepared for the Standing Dental Advi-
sory Committee. London, UK: Central Health Services Council; 1990.Shaw WC, Asher-McDade C, Brattstrom V, Dahl E, McWilliam J, Molsted K,
Plint DA, Prahl-Andersen B, Semb G, The RP. A six-center international
study of treatment outcome in patients with clefts of the lip and palate: Part
1. Principles and study design. Cleft Palate Craniofac J. 1992a;29:393–397.
Shaw WC, Dahl E, Asher-McDade C, Brattstrom V, Mars M, McWilliam J,
Molsted K, Plint DA, Prahl-Andersen B, Roberts C. A six-center interna-
tional study of treatment outcome in patients with clefts of the lip and palate:
Part 5. General discussion and conclusions. Cleft Palate Craniofac J. 1992b;
29:413–418.
Stone DH, Dolk H. High reported prevalence of congenital abnormalities in a
Scottish city. Scott Med J. 1994;39:170–172.
Vegter F, Mulder JW, Hage JJ. Major residual deformities in cleft patients: a
new anthropometric approach. Cleft Palate Craniofac J. 1997;34:106–110.
Womersley J, Stone DH. Epidemiology of facial clefts. Arch Dis Child. 1987;
62:717–720.
Yamada T, Mori Y, Minami K, Mishima K, Tsukamoto Y. Surgical results of
primary lip repair using the triangular flap method for the treatment of
complete unilateral cleft lip and palate: a three- dimensional study in infants
to four-year-old children. Cleft Palate Craniofac J. 2002a;39:497–502.
Yamada T, Mori Y, Minami K, Mishima K, Tsukamoto Y. Three-dimensional
analysis of facial morphology in normal Japanese children as control data
for cleft surgery. Cleft Palate Craniofac J. 2002b;39:517–526.
Yamada T, Sugahara T, Mori Y, Minami K, Sakuda M. Development of a 3D
measurement and evaluation system for facial forms with a liquid crystal
range finder. Comput Methods Programs Biomed. 1999;58:159–173.
Zhu NW, Senewiratne S, Pigott RW. Lip posture and mouth width in children
with unilateral cleft lip. Br J Plast Surg. 1994;47:301–305.


![Elsurtidocomovariablede clasificación:unaaplicaciónala ... · 2010-09-02 · [143 ] 10 411 mayo·agosto2010·esicmarket Elsurtidocomovariablede clasificación:unaaplicaciónala](https://img.pdfslide.tips/doc/110x75/5f3502ecc1d40b3822473c3a/elsurtidocomovariablede-clasificacinunaaplicacinala-2010-09-02-143-.jpg)