-
8/4/2019 04.Cong-Thuoc Chen Calci
1/79
TNG HUYT P NGI LN TUI
CP NHT IU TR
VI THUC CHN CALCI
PGS.TS.Nguyn c Cng
Bnh Vin Thng Nht
i hcy dc Tp H Ch Minh
-
8/4/2019 04.Cong-Thuoc Chen Calci
2/79
I. TNG HUYT P
NGI LN TUI
-
8/4/2019 04.Cong-Thuoc Chen Calci
3/79
Tui th Tui th ngy cng tng
c tnh n 2030, ngi > 65 tui chim 20% dn sHoa K.
-
8/4/2019 04.Cong-Thuoc Chen Calci
4/79
Tui i v bnh tt
Tui cng caocng tng t l bnh tt vmc nng ca bnh.
-
8/4/2019 04.Cong-Thuoc Chen Calci
5/79
NGUYN NHN GY T VONG (US)
Accidents5%
Pneumonia3%
COPD3%
CVD50%
Other18%
Cancer21%
-
8/4/2019 04.Cong-Thuoc Chen Calci
6/79
TNG HUYT P L MT TRONG NHNGYU T NGUY C QUAN TRNG NHT
BP > 140/90 mmHg is associated with:
277,000 deaths in 2003
BP, blood pressure; CHF, congestive heart failure;
MI, myocardial infarction.
Rosamond W et al. Circulation. 2007;115:1-103.
-
8/4/2019 04.Cong-Thuoc Chen Calci
7/79
-
8/4/2019 04.Cong-Thuoc Chen Calci
8/79
Tnh hnh bnh tng huyt pti Vit Nam
iu tra dch t: t l bnh THA gia tng nhanh trongcng ng.
* 1960: 1% dn s trng thnh min Bc.* 1976: 1,9% dn s trng thnh min
Bc.
* 1992: 11,7% ngi ln c nc.
* 1999: 16,05% ti ni & ngoi thnh HNi.* 2002: 16,32% ngi 25
tui pha Bc VN.
* 2008: 27,2% ngi 25 tui (iu tra ti 8 tnh/thnhph VN)
-
8/4/2019 04.Cong-Thuoc Chen Calci
9/79
II. THAY I HUYT P
& H THNG TIM MCHTHEO TUI
-
8/4/2019 04.Cong-Thuoc Chen Calci
10/79
HUYT P
HA tm thu khuynh hng tng dn theo tui. Tng 5-8 mm Hg cho mi thp
nin sau tui 40-50.
HA tm trng tng nh n 60 tui, sau nnh v gim nh.
(Generally increases 1 mm Hg per decade)
-
8/4/2019 04.Cong-Thuoc Chen Calci
11/79
0
20
40
60
80
100
0 2 4 6 8 10 12 14 16 18 20Ris
kofhypert
ension(%)
Residual lifetime risk of developinghypertension among people
with bloodpressure 65 tui
Men Women
Vasan RS, et al. JAMA. 2002; 287:1003-1010.Copyright 2002,
American Medical Association.
-
8/4/2019 04.Cong-Thuoc Chen Calci
12/79
Partners in Healthcare Education, LLC 2009 12
Vin cnh xut hin bnh tng HA
90% ngi > 55 tui s xut hin tng HA thi im no trong cuc i.
TNG HUYT P TM THU
-
8/4/2019 04.Cong-Thuoc Chen Calci
13/79
Nhp tim
Khng thay i khi nm ngh, gim t thngi (gim p ng vi h giao cm) D b
h HA tth
Khi gng sc, nhp tim gim theo tui. 200 beats/min tui 20
140 beats/min tui 80
(Tn s tim c tinh theo tui = 220 tui)
-
8/4/2019 04.Cong-Thuoc Chen Calci
14/79
Thay i h thng ng mch
Thnh ng mch dy v km n hi. Tng HA
Tng khng lc mch mu ngoi bin
-
8/4/2019 04.Cong-Thuoc Chen Calci
15/79
p ng vi kch thch giao cm
Gim p ng vi cc kch thch bta giaocm. Gim tn s tim ti a.
1 & 2 effect Gim kh nng gin mch ngoi bin.
2 effect
-
8/4/2019 04.Cong-Thuoc Chen Calci
16/79
Cung lng tim
Khng c s thay i quan trng theo tui trng thi ngh ngi, c th gim
khi hot ngth lc.
C th do gim th tch cui tm trng tht tri dothnh tht tri dy v km n
hi.
-
8/4/2019 04.Cong-Thuoc Chen Calci
17/79
III. Y HC BNG CHNG
-
8/4/2019 04.Cong-Thuoc Chen Calci
18/79
-
8/4/2019 04.Cong-Thuoc Chen Calci
19/79
Tng huyt p tm thu v nguy ct vong do bnh l tim mch.
Adapted from Neaton JD et al. Arch Intern Med.
1992;152:56-64.
SBP versus DBP in Risk of CHD Mortality
Diastolic BP(mm Hg)
Systolic BP(mm Hg)
CHD Death Rate
100+
90998089
75797074
-
8/4/2019 04.Cong-Thuoc Chen Calci
20/79
Disease Relative Risk
Kidney failure (ESRD) 2.8
Stroke 2.7Heart failure 1.5Peripheral vascular disease
1.8Myocardial infarction* = 1.6Coronary artery disease 1.5
ESRD = end-stage renal disease; SBP 165 mm Hg.*Men only.
Adapted from Kannel WB. Am J Hypertens. 2000;13:3S-10S; Perry HM
Jr et al. Hypertension. 1995;25(part1):587-594;
Klag MJ et al. N Engl J Med. 1996;334:13-18; Nielsen WB et al.
Ugeskr Laeger. 1996;158:3779-3783; NeatonJD et al.Arch Intern Med.
1992;152:56-64.
Tng huyt p tm thu n c gytng nguy c bnh l tim mch v
bnh thn.
-
8/4/2019 04.Cong-Thuoc Chen Calci
21/79
LI IM KHI IU TRTNG HUYT P
BN < 60 tui (gim HA 10/5-6 mmHg) Gim nguy c t qu 42%
Gim nguy c xut hin bin c bnh MV 14%
BN > 60 tui (gim HA 15/6 mmHg) Gim t vong ton b 15%
Gim t vong do bnh l TM 36%
Gim t qu 35%
Gim bnh l ng mch vnh 18%Lancet 1990;335:827-38 Arch Fam Med
1995;4:943-50
-
8/4/2019 04.Cong-Thuoc Chen Calci
22/79
LI IM KHI IU TR T
HUYT P MC TIU BN > 60 tui
(SBP 160 mm Hg and DBP < 90 mm Hg)
Gim nguy c t qu 42% Gim nguy c xut hin bin c bnh l ng
mch vnh 26%
Lancet 1997;350:757-64
-
8/4/2019 04.Cong-Thuoc Chen Calci
23/79
Meta-analysis of 61 prospective, observational studies*
1 million adults
12.7 million person-years
*Epidemiologic studies, not clinical trials of HTN agents.
BP, blood pressure; IHD, ischemic heart disease.
Lewington S et al. Lancet2002;360:1903-1913.
H p l vn then cht
Gim 2 mm HgHATTh trung
bnhGim 10% nguyc t vong do
t qu
Gim 7%nguy c tvong bnhtim thiumu cc b
-
8/4/2019 04.Cong-Thuoc Chen Calci
24/79
*LV Hypertrophy, Angina, MI, PTCA, Bypass; Sroke or TIA,
Peripheral Arterial Disease, retinopathy, carotid plaque,
microalbuminurea
2007 Guidelines for the Management of Arterial Hypertension: The
Task Force for the Management of Arterial Hypertension of the
EuropeanSociety of Hypertension (ESH) and of the European Society
of Cardiology (ESC). J Hypertens. 2007;25(6):1105-87
Mc HA mc tiu cn t n ty theo din tinbnh v tn thng c quan ch
-
8/4/2019 04.Cong-Thuoc Chen Calci
25/79
NHNG TH NGHIM LM SNG
-
8/4/2019 04.Cong-Thuoc Chen Calci
26/79
The Hypertension Optimal
Treatment Study (HOT Study)
-
8/4/2019 04.Cong-Thuoc Chen Calci
27/79
S lng bnh nhn tham gia NCA total of 18.790 patients from 26
countries were randomised
Country/ No. of randomised Country/ No. ofrandomisedarea
patients area patients
Argentina 47 Israel 411Austria 628 Italy 2.702Belgium 755 Mexico
49
Canada 838 Norway 432Denmark 503 South East Asia 71East Asia 134
Spain 806
Finland 373 Sweden 492France 1.574 Switzerland 797Germany 4.269
The Netherlands 603
Great Britain 131 USA 2.646Greece 335Hungary 194
-
8/4/2019 04.Cong-Thuoc Chen Calci
28/79
Tiu ch chnh.
nh gi mi lin quan gia nhng bin c vtim mch vi 3 tr s HA tm trng
ch ( 140mmHg v/hay DBP > 90mmHg
N khng mang thai hay cho con b.
Khng s dng Plendil t nht 4 tun l.
-
8/4/2019 04.Cong-Thuoc Chen Calci
46/79
Cc bc nghin cu
1st step Plendil5mg*
Plendil10mg + Betaloc25mg BID/Low dose of ACEI
Plendil10mg + Betaloc50mg BID/High dose of ACEI
Plendil10mg + Betaloc50mg BID/High dose of ACEI+ Low dose of
other anti-hypertensive drugs(-blocker/ACEI)/Diuretic
* Target DBP < 90mmHg after 2 weeks treatment.
2nd step
3rd step
4th step
5th step
*
*
*
Plendil5mg + Betaloc25mg BID /Low dose of ACEI
-
8/4/2019 04.Cong-Thuoc Chen Calci
47/79
Dn s nghin cu
Unqualified data(age, gender or baseline BP missing)
1,530
Data
sum58,289
Repeated data321
Qualifieddata
56,438
Intention-to-treatpopulation (ITT)
53,040
-
8/4/2019 04.Cong-Thuoc Chen Calci
48/79
KT QU
-
8/4/2019 04.Cong-Thuoc Chen Calci
49/79
KT QU
-
8/4/2019 04.Cong-Thuoc Chen Calci
50/79
TC DNG PH
AE = Ankle Edema
-
8/4/2019 04.Cong-Thuoc Chen Calci
51/79
HOT China: Kt lun
Cc bc iu tr tng HA trong NC HOT ph hpvi bnh tng HA nguyn pht ngi
Trung Quc.Cc bc iu tr c tnh an ton, hiu qu v dung
np tt. Kt hp thuc liu thp gia cc nhm thuc nh
Plendil + Betaloc / ACEI khng lm tng thm hiuqu h HA nhng lm gim
c tc dng ph khi
tng liu thuc trong ch iu tr 1 thucBnh nhn tng HA nguyn pht ngi
Trung Qucc kim sot HA an ton v hiu qu hn.
-
8/4/2019 04.Cong-Thuoc Chen Calci
52/79
1338 Z
The Felodipine Event Reduction (FEVER) Study
A Randomized Long-Term Placebo-Controlled Trial
in Chinese Hypertensive Patients
Design and Principal Results
Lisheng Liu, Yuqing Zhang, Guozhang Liu, Wei Li, Xuezhong Zhang
and
Alberto Zanchetti for the FEVER Study Group
(Beijing, China and Milan, Italy)
-
8/4/2019 04.Cong-Thuoc Chen Calci
53/79
FEVER: MC TIU
1340 Z
1.
2.
So snh hiu qu trn bin c v bnh l tim mch ca Plendil liuthp
5mg/ngy vi placebo BN tng HA c iu tr bngthuc li tiu liu thp (HCTZ
12,5mg/ngy).
So snh hiu qu h HA tch cc t c mc HA mc tiu theocc khuyn co.
-
8/4/2019 04.Cong-Thuoc Chen Calci
54/79
FEVER: Inclusion Criteria
1342 Z
50-79 tui, c nam v n
i tng < 60 tui: c t nht 1 bin c tim mch nhNMCT, t qu, autht
ngc, suy tim, bnh ng mch ngoi vi, cn thieesyu mu no thongqua hoc c
2 yu t nguy ctim mch (nam, ht thuc l, TC > 5.7 mmol/l,tiu ng,
LVH (voltage), proteinuria > +, BMI > 27 kg/m2)
i tng > 60 tui: c t nht mt bin c tim mch hoc mt yu t
nguyc.
Khm sng lc: Bnh nhn iu tr: SBP/DBP < 210/115 mmHg
: Bnh nhn cha iu tr : SBP 160-210 mmHg hoc DBP 95-115mmHg
Chn ngu nhin: SBP 140-180 or DBP 90-100 mmHg, sau 6 tun dngHCTZ
12.5 mg/ngy (ct thuc dng trc y)
-
8/4/2019 04.Cong-Thuoc Chen Calci
55/79
-
8/4/2019 04.Cong-Thuoc Chen Calci
56/79
Giam tai bien mach mau nao
Theo doi (thang)
HR = 0.732, 95% CI: 0.601-0.891, p = 0.0019
Ty le benh nhan xay ra bien co (%)
0 6 12 18 24 30 36 42 48 54 60
0
2
4
6
8
10
-26.8%
(the FEVER Study Group)
Xanh: Placebo
Chm: Plendil
-
8/4/2019 04.Cong-Thuoc Chen Calci
57/79
Giam tong bien co tim mach
Theo doi (thang)
Ty le benh nhan xay ra bien co (%)
0 6 12 18 24 30 36 42 48 54 60
0
3
6
9
12
15
HR = 0.726, 95% CI: 0.612-0.860, p = 0.0002
-27.4%
(the FEVER Study Group)
Xanh: Placebo
Chm: Plendil
-
8/4/2019 04.Cong-Thuoc Chen Calci
58/79
-
8/4/2019 04.Cong-Thuoc Chen Calci
59/79
Giam t vong do nguyen nhan tim mach
Theo doi (thang)
Ty le benh nhan xay ra bien co (%)
HR = 0.668, 95% CI: 0.489-0.912, p = 0.0112
0 6 12 18 24 30 36 42 48 54 600
1
2
3
4
-33.2%
(the FEVER Study Group)
Xanh: Placebo
Chm: Plendil
FEVER: Endpoint Analysis
-
8/4/2019 04.Cong-Thuoc Chen Calci
60/79
FEVER: Endpoint Analysis(first time occurrence in each
category)
1355 Z
Stroke
Fatal
Non-fatal
All CV events
All cardiac events
All cause death
CV death
Coronary events
Heart failure
New onset diabetesCancer
Felodipine
11.2
2.1
9.1
15.2
4.6
7.1
4.6
4.5
1.1
3.62.6
Placeb
o
15.9
3.1
12.7
21.2
6.6
9.6
6.4
6.2
1.7
3.53.9
Hazard Ratio (95% CI)Per 1000 patient-years
0.4 0.6 0.8 1.0 1.5 2.0
Felodipine better Placebo better
0.72
0.70
0.72
0.72
0.66
0.70
0.68
0.68
0.76
1.030.60
FEVER KT LUN
-
8/4/2019 04.Cong-Thuoc Chen Calci
61/79
FEVER: KT LUN
1362 Z
BN tng HA ngi Trung Quc iu tr bng HCTZ (12.5mg/d) v Felodipine
liu thp 5mg/ngy gim c HA nhiu
hn (SBP/DBP # 4/2 mmHg) v gim quan trng cc bin c
t qu (28%), bin c v bnh tim mnh (28%), bin c v
bnh ng mch vnh (32%), gim t vong do tt c cc
nguyn nhn (30%), gim tvong do bnh l tim mch (17%).
iu tr kt hp liu thp UC knh Ca v HCTZ cho kt qutt hn n tr liu
HCTZ liu thp.
iu tr vi liu thp ch c 1% xut hin bnh l T mimc.
-
8/4/2019 04.Cong-Thuoc Chen Calci
62/79
IV. NHNG KHUYNCO IU TR
TNG HUYT P
BHS IV, 2004 and Update of the NICE Hypertension Guideline,
2006
BHS Guidelines for the management of hypertension
-
8/4/2019 04.Cong-Thuoc Chen Calci
63/79
BHS Guidelines for the management of hypertension
-
8/4/2019 04.Cong-Thuoc Chen Calci
64/79
ESH
-
8/4/2019 04.Cong-Thuoc Chen Calci
65/79
Compelling and possible indications, contraindications, and
cautions for the major classes of antihypertensive drugs
Class of drugCompellingindications
Possibleindications Caution
Compellingcontraindications
Beta-blockers MI,Angina
Heart failure Heart failure,PVD,
Diabetes(except with
CHD)
Asthma/COPD,Heart block
CCBs(dihydropyridine)
Elderly, ISH Angina - -
CCBs(rate limiting)
Angina Elderly Combinationwith beta-blockade
Heart blockHeart failure
Thiazide/thiazide-like diuretics ElderlyISHHeart failure2 o
strokeprevention
Gout
ESH
2007 ESH/ESC Guidelines
Combination between some classes of
-
8/4/2019 04.Cong-Thuoc Chen Calci
66/79
Thiazide diuretics
ACE inhibitors
Calcium antagonists
-blockers AT1-receptor antagonists
-blockers
Combination between some classes ofantihypertensive drugs
J Hypertens. 2007;25:1105-1187.
-
8/4/2019 04.Cong-Thuoc Chen Calci
67/79
Bnh nhn ln tui
Nnbt u iu tr bng thay i li sng.
Nn khi u dng thuc vi liu thp.
HA mc tiu < 140/90 mm Hg.
Nhm thuc c ch knh Ca l mt trongnhng thuc chn la u tin.
JNC 7.
Tng HA v cn ph bin nht:
Hng dn iu tr tng HA theo Hi
-
8/4/2019 04.Cong-Thuoc Chen Calci
68/79
Hng dn iu tr tng HA theo HiTng HA Canada 2010
Hng dn iu tr tng HA theo Hi
-
8/4/2019 04.Cong-Thuoc Chen Calci
69/79
Hng dn iu tr tng HA theo HiTng HA Canada 2010
-
8/4/2019 04.Cong-Thuoc Chen Calci
70/79
V. KT LUN Tng huyt p ngi ln tui rt thng gp.
Thng l tng huyt p tm thu n c.
Tng huyt p tm thu cng gy ra nhng bin c v
tim mch trm trng v t vong. iu tr tt tng HAtm thu lm gim quan
trng t xut v ccbin chngtng HA.
Nhm thuc c ch knh calci dihydropyridines tcdng ko di (nh
Felodipine - Plendil) c vai trquan trng trong kim sot tt HA ngi ln
tui.
Chn thnh cm n s ch
-
8/4/2019 04.Cong-Thuoc Chen Calci
71/79
Chn thnh cm n s ch ca Qu v
T L NHP VIN V T VONG
-
8/4/2019 04.Cong-Thuoc Chen Calci
72/79
Number of Admissions Deaths
Total Age > 65 Age > 65
Acute MI 858 562 (65.5%) 63 (81.2%)
Coronary disease 1280 685 (53.5%) 12 (85.7%)Arrhythmias 731 519
(71.0%) 11 (73.3%)
Heart failure 1040 805 (77.4%) 38 (92.7%)
Cerebrovascular Dz 1044 758 (72.6%) 47 (74.6%)
(numbers in thousands)> 65 yo 13% population
National Hospital Discharge Survey, 2000.
T L NHP VIN V T VONG
V BNH L TIM MCH
-
8/4/2019 04.Cong-Thuoc Chen Calci
73/79
Thay i tim
Dy thnh tm tht tri nng ln khi ckm tng huyt p.
Ph i tm tht tri c th gy chm th gintrong thi k tm trng.
Gin nh tri th pht sau ph i tm tht tri.
Sites of Clinical Centers of FEVER
-
8/4/2019 04.Cong-Thuoc Chen Calci
74/79
Sites of Clinical Centers of FEVER
Al ith f T t t f H t iJNC 7.
-
8/4/2019 04.Cong-Thuoc Chen Calci
75/79
Algorithm for Treatment of Hypertension
Not at Goal Blood Pressure (100 mmHg)
2-drug combination for most (usuallythiazide-type diuretic
and
ACEI, or ARB, or BB, or CCB)
Stage 1 Hypertension(SBP 140159 or DBP 9099 mmHg)
Thiazide-type diuretics for most.May consider ACEI, ARB, BB,
CCB,
or combination.
Without CompellingIndications
Not at GoalBlood Pressure
Optimize dosages or add additional drugsuntil goal blood
pressure is achieved.
Consider consultation with hypertension specialist.
FEVER: TIU CH NGHIN CU
-
8/4/2019 04.Cong-Thuoc Chen Calci
76/79
FEVER: TIU CH NGHIN CU
1345 Z
Chnh:
Ph :
t qu (fatal and nonfatal)
1)
2)
3)
4)
5)
6)
Total cardiovascular events (composite of CV death,
non-fatalstroke, non-fatal MI, dissecting aortic aneurysm, HF
requiringtreatment, PTCA, CABG, interventions for PAD, s.
creatinine >355 mol/l)Total cardiac events (composite of death
by CHD, non-fatal MI,death by HF, HF requiring treatment, PTCA,
CABG)
Death by any cause (composite of CV death and non-CV death)
Any of the event categories in composite outcomesa) fatal
stroke, b) non-fatal stroke, c) CHD events (fatal and non-
fatal MI and sudden death), d) HF, e) CV death, f) renal
failure
New onset diabetes (FBG > 7.0 mmol/l or treatment)
Cancer
FEVER: TIU CH NGHIN CU
-
8/4/2019 04.Cong-Thuoc Chen Calci
77/79
FEVER: TIU CH NGHIN CU
1345 Z
Chnh:
Ph :
t qu (fatal and nonfatal)
1)
2)
3)
4)
5)
6)
Total cardiovascular events (composite of CV death,
non-fatalstroke, non-fatal MI, dissecting aortic aneurysm, HF
requiringtreatment, PTCA, CABG, interventions for PAD, s.
creatinine >355 mol/l)Total cardiac events (composite of death
by CHD, non-fatal MI,death by HF, HF requiring treatment, PTCA,
CABG)
Death by any cause (composite of CV death and non-CV death)
Any of the event categories in composite outcomesa) fatal
stroke, b) non-fatal stroke, c) CHD events (fatal and non-
fatal MI and sudden death), d) HF, e) CV death, f) renal
failure
New onset diabetes (FBG > 7.0 mmol/l or treatment)
Cancer
FEVER: THIT K V S NC
-
8/4/2019 04.Cong-Thuoc Chen Calci
78/79
FEVER: THIT K V S NC
1344 Z
+ Felodipine 5 mg/d
+ Placebo
HCTZ
12.5 mg/d
visits
weeks
1
-6
2
-4
3
-2
4
0
5
1
6
2
7
3
8
4
9
5
10
6
11
9
12
12
16
24
20
36
24
48
28
60 months
Screening Randomization
Add-on diuretic or other agents (not CA)
if BP > 160/90 mmHg, at investigators discretion
FEVER: TIU CH NGHIN CU
-
8/4/2019 04.Cong-Thuoc Chen Calci
79/79
FEVER: TIU CH NGHIN CU
Chnh:
Ph :
t qu (fatal and nonfatal)
1)
2)
3)
4)
5)
6)
Total cardiovascular events (composite of CV death,
non-fatalstroke, non-fatal MI, dissecting aortic aneurysm, HF
requiringtreatment, PTCA, CABG, interventions for PAD, s.
creatinine >355 mol/l)Total cardiac events (composite of death
by CHD, non-fatal MI,death by HF, HF requiring treatment, PTCA,
CABG)
Death by any cause (composite of CV death and non-CV death)
Any of the event categories in composite outcomesa) fatal
stroke, b) non-fatal stroke, c) CHD events (fatal and non-
fatal MI and sudden death), d) HF, e) CV death, f) renal
failure
New onset diabetes (FBG > 7.0 mmol/l or treatment)
Cancer








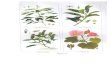
![[Duoc ly] thuoc chong lao thuoc dieu tri phong - ts tung](https://img.pdfslide.tips/doc/110x75/58a4937c1a28ab741b8b4fe5/duoc-ly-thuoc-chong-lao-thuoc-dieu-tri-phong-ts-tung.jpg)