Embed Size (px)
Citation preview

2015 Annual Report
Venice Family Clinic
Children First Early Head Start
604 Rose Avenue
Venice, CA 90291
(310) 664-7534
http://www.venicefamilyclinic.org

Table of Contents
Our History……………………………………………………….. 2
Mission Statement……………………………………………. 2
Our Program…………………………………………………….. 3
School Readiness………………………………………………. 4
Independent Auditor’s Report………………………….. 8
Letter From the Director.………………………………….. 10
Budget and Expenditures………………………………….. 11
Health Services…………………………………………………. 12
Enrollment……………………………………………..………… 13
Transition…………………………………………………………. 14
Parent Involvement…………………………………………… 15

Head Start began as an eight week summer program in 1965. The project was funded by the Federal Government to provide services to preschool aged children ages 3 - 5. Head Start was designed to help break the cycle of poverty by providing comprehensive health, educational, nutritional, social, and other services to economically disadvantaged children and their families. Since then, Head Start has served more than 15 million children and families.
In 1994, the Early Head Start program was created by the U.S. Congress as an extension of the Head Start Act. The Early Head Start program serves pregnant women and children up to age three. The goals of Early Head Start focus on the healthy cognitive, physical, social and emotional development of infants and toddlers. Research on brain development has demonstrated that, to thrive, children from birth to age three need a variety of positive learning experiences provided in a secure and loving environment. In recognition that parents are the primary educators of their children, Early Head Start programs are designed to work with families to ensure that the developmental needs of each child are met. Since 1994, Early Head Start has grown nationwide to over 600 community-based programs serving over 50,000 children.
Early Head Start History 2
The mission of Children First Early Head Start is to optimize the quality of life for infants, toddlers, and pregnant women by enriching relationships among families, communities, and staff through child development education and parent empowerment. We promote a continuum of care including comprehensive health services, social services, and community referrals.
Mission Statement

Philosophy There are two key elements to the Early Head Start philosophy. First, every child can benefit from a comprehensive program to foster development. And second, the child’s entire family, as well as the community, must be involved in the program in order for it to be a success. Children First Early Head Start is designed to meet the special strengths and needs of each child and family.
The program provides the following comprehensive services:
Child Development and Early Childhood Education
Parent education, advocacy and involvement
Child health, safety and wellness
Nutrition and dental services
Networking families with community and social services and resources
Disabilities, wellness, and mental health services available
Our Program
Program Goals Children First Early Head Start believes the long-term goal of the program is healthy children and families, strong parent-child relationships, resourceful/self-sufficient families, and supportive communities.
To be eligible for the Children First Early Head Start program, families need to live in our service area comprised of various cities on the west side of Los Angeles, including Venice, Santa Monica, Culver City, Mar Vista, the Cadillac/Robertson area, Palms, and parts of Inglewood.
Our Program 3

During 2015, school readiness date was collected three times during the year to track progress for individual children and the program. Individual reports were shared with families and results were shared in the newsletter. Date collection #3 is shared below for 2015.
CUSTOM SOLUTIONS
WEB
EBUS
School Readiness
Social and Emotional Development: Infants and Toddlers will develop self-esteem through posi-tive relationships with those around them.
Language and Literacy Skills: Infants and Toddlers will increase their language skills through early literacy learning activities.
4

CUSTOM SOLUTIONS
WEB
Approaches to Learning: Infants and Toddlers will learn exploring their surroundings through repetition and experimenting.
Cognitive and General Knowledge: Infants and Toddlers will learn to be independent and responsible in the way they demonstrate their experiences.
School Readiness 5
CUSTOM SOLUTIONS
WEB
School Readiness 6
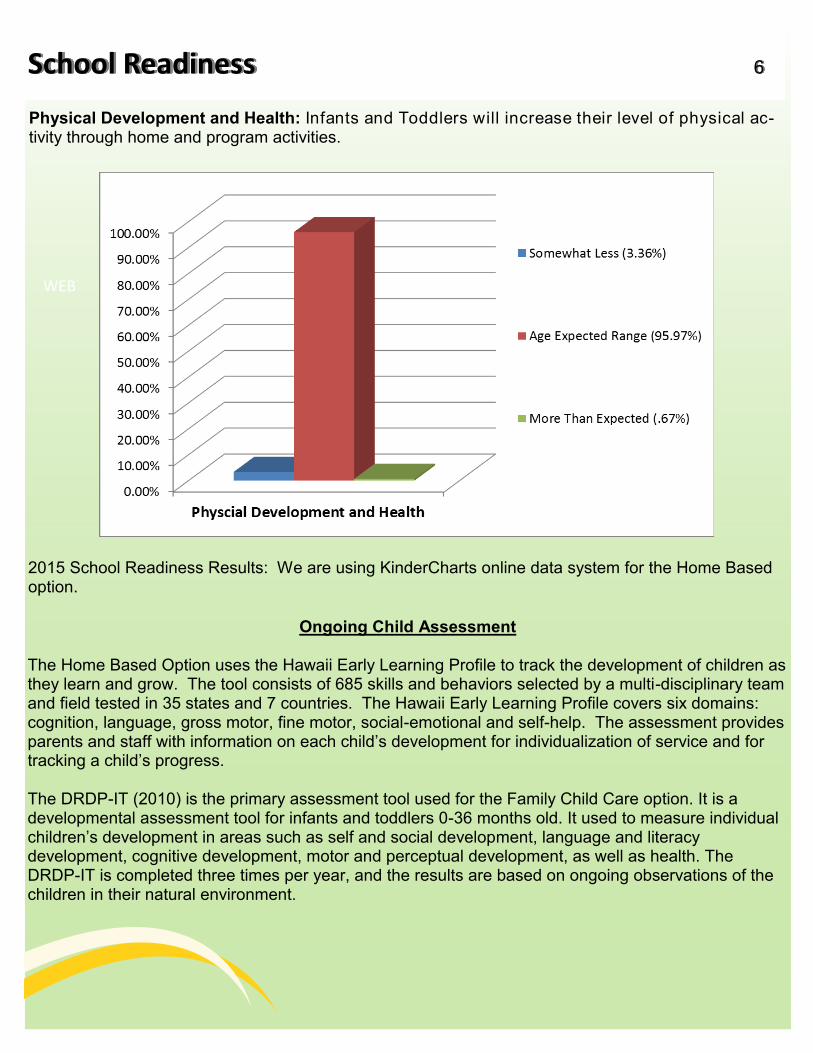
Physical Development and Health: Infants and Toddlers will increase their level of physical ac-tivity through home and program activities.
2015 School Readiness Results: We are using KinderCharts online data system for the Home Based option.
Ongoing Child Assessment The Home Based Option uses the Hawaii Early Learning Profile to track the development of children as they learn and grow. The tool consists of 685 skills and behaviors selected by a multi-disciplinary team and field tested in 35 states and 7 countries. The Hawaii Early Learning Profile covers six domains: cognition, language, gross motor, fine motor, social-emotional and self-help. The assessment provides parents and staff with information on each child’s development for individualization of service and for tracking a child’s progress. The DRDP-IT (2010) is the primary assessment tool used for the Family Child Care option. It is a developmental assessment tool for infants and toddlers 0-36 months old. It used to measure individual children’s development in areas such as self and social development, language and literacy development, cognitive development, motor and perceptual development, as well as health. The DRDP-IT is completed three times per year, and the results are based on ongoing observations of the children in their natural environment.

CUSTOM SOLUTIONS
School Readiness (DRDP Tech) Family Child Care 7
(ALT-REG) Approaches to Learning Self-Regulation
Responding Earlier
Responding Later
Exploring Earlier
Exploring Later
Building Earlier
6% / 0% / 5% 11% / 14% / 5% 24% / 14% / 35% 49% / 57% / 35% 16% / 14% / 20%
(SED) Social and Emotional Development
Responding Earlier
Responding Later
Exploring Earlier
Exploring Later
Building Earlier
9% / 0% / 5% 8% / 14% / 10% 20% / 14% / 25% 72% / 50% / 35% 15% / 21% / 25%
(LLD) Language and Literacy Development
Responding Earlier
Responding ater
Exploring Earlier
Exploring Later
Building Earlier
6% / 0% / 5% 17% / 7% / 20% 8% / 21% / 30% 24% / 64% / 25% 28% / 7% / 20%
(COG) Cognition, Including Math and Science
Responding Earlier
Responding Later
Exploring Earlier
Exploring Later
Building Earlier
4% / 0% / 5% 11% / 21% / 20% 20% / 7% / 30% 46% / 71% / 25% 19% / 0% / 20%
(PD-HLTH) Physical Development - Health
Responding Earlier
Responding Later
Exploring Earlier
Exploring Later
Building Earlier
4% / 0% / 5% 5% / 7% / 20% 10% / 21% / 10% 35% / 14% / 25% 42% / 57% / 40%
Group Summary by Percent for
Winter 2014-2015 / Spring 2015 / Fall 2015
DRDP (2015) Infant Toddler

CUSTOM SOLUTIONS Independent Auditor’s Report 11
To the Board of Directors Venice Family Clinic Venice, California
Report on the Financial Statements
We have audited the accompanying consolidated financial statements of Venice Family Clinic and affiliate (the “Clinic”), which comprise the consolidated statement of financial position as of June 30, 2015, and the related consolidated statements of activities, functional expenses and cash flows for the year then ended and the related notes to the financial statements.
Management’s Responsibility for the Financial Statements
Management is responsible for the preparation and fair presentation of these consolidated financial statements in accordance with accounting principles generally accepted in the United States of America; this includes the design, implementation and maintenance of internal control relevant to the preparation and fair presentation of consolidated financial statements that are free from material misstatement, whether due to fraud or error.
Auditor’s Responsibility
Our responsibility is to express an opinion on these consolidated financial statements based on our audit. We conducted our audit in accordance with auditing standards generally accepted in the United States of America and the standards applicable to financial audits contained in Government Auditing Standards, issued by the Comptroller General of the United States. Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement.
An audit involves performing procedures to obtain audit evidence about the amounts and disclosures in the consolidated financial statements. The procedures selected depend on the auditor’s judgment, including the assessment of the risks of material misstatements of the consolidated financial statements, whether due to fraud or error. In making those risk assessments, the auditor considers internal control relevant to the entity’s preparation and fair presentation of the consolidated financial statements in order to design audit procedures that are appropriate in the circumstances, but not for the purpose of expressing an opinion on the effectiveness of the entity’s internal control. Accordingly, we express no such opinion. An audit also includes evaluating the appropriateness accounting principles used and the reasonableness of significant accounting estimates made by management, as well as evaluating the overall financial statement presentation of the consolidated financial statements. We believe that the audit evidence we have obtained is sufficient and appropriate to provide a basis for our audit opinion.
Opinion
In our opinion, the consolidated financial statements referred to above present fairly, in all material respects, the consolidated financial position of the of Venice Family Clinic and affiliate as of
Independent Auditor’s Report 8

9
(cont’d.) June 30, 2015, and the changes in its net assets and its cash flows for the year then ended in accordance with accounting principles generally accepted in the United States of America.
Report on Summarized Comparative Information
We have previously audited the Clinic’s 2014 consolidated financial statements, and we expressed an unmodified audit opinion on those audited financial statements in our report dated ed December 7, 2014. In our opinion, the summarized comparative information presented here-in as of and for the year ended June 30, 2014 is consistent in all material respects with the audited consolidated financial statements from which it has been derived.
Other Matters
Our audit was conducted for the purpose of forming an opinion on the consolidated financial statements as a whole. The accompanying schedule of expenditures of federal awards, as required by U.S. Office of Management and Budget (“OBM”) Circular A-133, Audits of States, Local Governments and Non-profit Organizations, and consolidating and other supplementary information is presented for purposes of additional analysis and is not a required part of the consolidated financial statements. Such information is the responsibility of management and was derived from and relates directly to the underlying accounting and other records used to prepare the consolidated financial statements.
The schedule of expenditures of federal awards and consolidating and other supplemental information has been subjected to the auditing procedures applied in the audit of the consolidated financial statements and certain additional procedures, including comparing and reconciling such information directly to the underlying accounting and other records used to prepare the consolidated financial statements or to the consolidated financial statements themselves, and other additional procedures in accordance with auditing standards generally accepted in the United States of America. In our opinion, the information is fairly stated in all material respects in relation to the consolidated financial statements as a whole.
Other Reporting Required by Government Auditing Standards
In accordance with Government Auditing Standards, we have also issued our report dated December 12, 2015 on our consideration of the Clinic’s internal control over financial reporting and our tests of its compliance with certain provisions of laws, regulations, contracts and grant agreements and other matters. The purpose of that report is to describe the scope of our testing of internal control over financial reporting and compliance and the results of that testing, and not to provide an opinion on the internal control over financial reporting or on compliance. That report is an integral part of an audit performed in accordance with Government Auditing Standards in considering the Clinic’s internal control over financial reporting and compliance.
SINGER LEWAK LLP
Los Angeles, California December 12, 2015

A Letter From The Director...
Children First Early Head Start underwent a review by the Office of Head Start in December 2015 for Environmental Health & Safety. One concern was noted and no follow-up was required.
Federal Review
Community members,
Venice Family Clinic Children First Early Head Start is proud to share our 2015 accomplishments with
you. We implemented Family Outcomes and the measurement process to help our families make gains in
seven areas that are linked to children being successful in school. We continued to measure for School
Readiness and we are appreciative of the support of a part-time Speech Therapist to help our children who
do not qualify for West Side Regional Center but still need extra support in this important domain for
development. We attended two Practice Based Coaching academies and we are implementing a Coaching
program for our education staff. We will be moving to the Children’s Health and Wellness Center to offer
our Play Groups in the fall of 2016. We welcomed 12 new Policy Council members. We have a new
Family Child Care Provider in the Inglewood area. We continue to use our quality measurement tools-
HOVRS for Home Visiting, FCCERS for Family Child Care Environments, and our Health and Safety
Checklists in each home and site. We are proud that at the end of enrollment we had 97% children up to
date with well-child visits. We had a busy and productive 2015 and we continue to do our best to partner
with children and families to be ready for a successful school career and healthy life. Thank you for your
support and involvement.
Stacey Scarborough, Children First Early Head Start Director
10

Budget & Expenditures
EARLY HEAD START
STATEMENT OF FUNCTIONAL EXPENSES FOR YEAR ENDED JUNE 30, 2015
EARLY HEAD START
2016 PROPOSED BUDGET
Salaries
$1,446,038
Personnel $1,514,511
Employee Benefits
$699,988
Fringe $686,579
Utilities & Rent
$104,796
Contractual $25,807
Telephone $10,926
Travel $19,646
Professional and contractual fees $44,311
Supplies $39,384
Postage, printing and subscriptions $17,588
Other Costs $124,385
Computer/Software/Office Supplies
$9,967
Direct
$2,432,927
Travel, training and workshops $66,767
Indirect Cost
$42,261
Repairs and maintenance $59,249
TA $60,042
Insurance $12,519
Approved Budget $2,492,969
Licenses, fees and dues $1,495
Non Federal Share $623,243
Transportation of patients/clients $1,105
EARLY HEAD START
2015 IN-KIND QUARTERLY DONATIONS
Participant supplies/activities/incentives
$23,418
January 1, 2015 – March 31, 2015 $76,008.49
Miscellaneous
$9,132 April 1, 2015 – June 30, 2015 $70,318.43
Total before depreciation and Expenses
$2,634,341
July 1, 2015 – September 30, 2015 $100,350.07
Total functional expenses
$2,712,070
October 1, 2015 – December 31, 2015 $83,104.59
STATE OF CALIFORNIA DEPARTMENT OF EDUCATION
SCHEDULE OF EXPENDITURES OF FEDERAL
AND STATE AWARDS JUNE 30, 2015
Indirect Cost $132,678
Program Title Contract
Amount Total Donations $462,459.58
Child Development
Services – General July 1st 2014 –Center Child Care June 30th 2015
$178,782
July 1st 2015 –
June 30th 2016 $188,972
Budget & Expenditures 11

EARLY HEAD START______________________________________________________________________________________
Physical Health 1. Number of children up-to-date at the end of enrollment ……………………………………………..246 (97%) 2. Children diagnosed with a chronic condition and referred for medical treatment …………………………..21 3. Of the children diagnosed number of children who received or are receiving medical treatment……… ………………..21 4. Number of children who received treatment for the following conditions:
Preventive Dental Services/Dental Services for Pregnant Women 5. Number of children who received dental screenings and professional dental examinations………………181
Number of children with continuous, accessible dental care provided by a dentist…………………...67% Number of all children who are up-to-date on a schedule of age-appropriate preventive & primary oral health care according to your state's EPSDT schedule………………………………...88% 6. Number of pregnant women who completed Early Head Start………………………………………………….5
EARLY HEAD START_________________________________________________________________________________________________ 1. Number of children determined by a multi-disciplinary team to have a disability EHS Prior to enrollment………………………………………………………………………………………………..28 Between time of enrollment and end of enrollment year……………………….........................................15 2. Total children determined to have a disability(ies)
Of the children determined to have a disability the number of
children with an Individualized Family Service Plan (IFSP)……………………………………………..43
Of the children reported, the number determined eligible by Local Education Agency (LEA) or Part C agency to receive special education or related services or Part C services under an Individualized Education Program (IEP) or Individualized Family Service Plan (IFSP)………………………………………………..43
3. Total number of children determined to have a disability who have not received special education and related services ...…………………………………………………..………….... 0
Health Services 12
Disability Services
■ Anemia 27
■ Asthma 5
■ Hearing Difficulties 3
■ Vision Problems 3
■ High Lead 0
■ Diabetes 0

Early Head Start Enrollment 13 FUNDED AND ACTUAL ENROLLMENT
ELIGIBILITY_____________________________________________________________________________________ Number of children and pregnant women who were enrolled based on receipt of public assistance……. ………... …..35
Number of children and pregnant women enrolled based on income eligibility…………………………………………. . 223
Number of children and pregnant women who were enrolled although their families were over income ……………….11
Number who were enrolled due to status as foster child………………………………………………………..................... .. 2 Number who were enrolled due to status as homeless ..……………………………………………………………………..11 PREGNANT WOMEN SERVED______________________________________________________________________ Total number of enrolled pregnant women………………………………………………………………………………………23
Enrollment by Ethnicity
Hispanic or Latino Origin…………………………..268
Non-Hispanic/Non-Latino Origin...………….….….. 14
Enrollment by Race
White……. …………………………………………. 221 American Indian or Alaskan Native ..……………...34 Native Hawaiian or Pacific Islander ……………… .1
Biracial/Multi-Racial .....……………………………. 15 Asian ...………………………………… ………...… 1 Black or African American…….....………............… 8 Other... ………………………………………....... .... 0
Primary Language
English…………………………….....……………… 49 Spanish…………………………………………….. 215 Native Central/South American/Mexican…….…...12 African ………………………………………………. . 2 Middle Eastern & South Asian…..…………………. 3 European & Slavic Languages.....…………………..0
Family Child Care Attendance
Home Based
20 92.8%
160
Funded Enrollment
January – August 2015
September – December 2015
Actual Enrollment
180
180
283
Eligible Population Served
2015 Monthly Enrollment
January – August 2015
September – December 2015
1.44%
100%
99%

EARLY HEAD START _
Children First Early Head Start works to assure a smooth transition into the program, between program options (Home Based and Family Child Care) at each of the child’s developmental transitions (from crawling, to cruising, to walking, etc.), and ultimately to the next enriching community environment. The child’s transition from Children First Early Head Start to a pre-school program begins no later than six months prior to the child’s third birthday. This is a collaborative process between parents, staff, relevant agency members and others who have played a role in providing care and nurturance to the child.
This year’s transition activities included:
Updated transition forms/procedure.
Annual Picnic and Resource Fair – various com-munity partners attended including –Connections for Children, Santa Monica Malibu Unified School District – Child Development Services, 211, Wells Fargo Bank, Training and Research Foundation, Venice Family Clinic’s Health Education and Health Insurance Outreach Programs.
Training for all EHS staff
Individualized EHS-curriculum used on home visits to assist families through transitions on an on-going basis.
Partnerships developed to assist in the seamless transition from Early Head Start to Head Start or other quality preschool programs in our service area.
Transition packets including the child’s health and developmental assessment records are given to the parent (one for them to keep and one to pass on to the child’s next educational setting). Packets also include: activity cards that give parents ideas on how interactive, educational and creative play can be used at home to prepare a child for preschool; a preschool toolkit, which includes a book titled, “My First Day at Preschool”; local resource information; and an Early Head Start certificate of completion.
Transition 14

Parent Involvement 15 PARENT TRAININGS
1. Play Groups 0-16 Months Inglewood
11 Groups
FATHER INVOLVEMENT
Of the children enrolled in the Early Head Start program, 152 fathers participated in regularly scheduled father involvement activities.
2. Play Groups 17-36 Months Inglewood
12 Groups
3. H V Play Groups Inglewood
26 Groups
4. Play Groups 0-16 Months Well Baby Center
11 Groups
5. Play Groups 17-36 Months Well Baby Center
12 Groups
6. H V Play Groups Well Baby Center 61 Groups
7. Father’s Groups 1 Group
8. Policy Council Meetings 15 Meetings
9. Parent Committee Meetings
Inglewood: 10 Simms Mann: 17
10. Newsletter Monthly
11. Domestic Violence Two
12. Child Abuse, Neglect & Prevention
Annually
13. Advocacy Three
14. What is Infant Mental Health Three
15. Dental Six
16. Substance Abuse Annually
17. Literacy Training
Two
18. School Readiness Outcomes Training
Two
19. Dealing with Holiday Stress
Two
20. Immigration Three





























