Embed Size (px)
Citation preview

1307
□ CASE REPORT □
A Case of Gliomatosis Cerebri Mimicking LimbicEncephalitis: Malignant Transformation to Glioblastoma
Riya Nagata, Ken Ikeda, Yoshikazu Nakamura, Yuichi Ishikawa, Ken Miura, Ryuta Sato,Yuji Kawase, Kiyokazu Kawabe and Yasuo Iwasaki
Abstract
Gliomatosis cerebri (GC) is a specific entity defined as diffuse infiltration of neoplastic glial cells into atleast three cerebral lobes and preservation of the surrounding neuronal architecture. We report a patient withsecondary GC that mimicked clinicoradiological features of limbic encephalitis (LE). A 72-year-old man haddeveloped headache and disorientation insidiously 2 weeks previously. On admission, neurological examina-tion showed confusion and hyperreflexia in the right extremities. Brain magnetic resonance imaging (MRI)revealed T2-hyperintensity in bilateral frontal, the left parietal, the left temporal lobes and bilateral posteriorperiventricular zones. Slight enhancement existed in the left lower temporal region. Cerebral angiography ex-hibited no tumor stains. Repeated cerebrospinal fluid studies showed mild pleocytosis and cytology of class I.There were no infectious pathogenic agents. His neurological symptoms were ameliorated at 7 days aftertreatment with dexamethasone and glycerol. Follow-up MRI showed no pathognomonic changes. Mild mem-ory dysfunction remained. He was diagnosed as LE of unknown cause. Three months later he became disori-entated. Brain CT revealed a hemorrhagic mass with surrounding edema in the left temporal, frontal and pa-rietal lobes. MRI displayed marked enhancement in these regions. Urgent neurosurgery was performed andglioblastoma multiforme (GM) was confirmed pathologically. The early clinicoradiological course of this pa-tient suggested similarities to LE. At 3 months after clinical onset, the neuroradiological features reflectedrapid transformation from secondary GC to massive GM. Thus, it is important to pay more attention to thedifferential diagnoses of GC and LE in patients who have memory deficits and widespread MRI lesions.
Key words: gliomatosis cerebri, secondary type, limbic encephalitis, glioblastoma multiforme
(Inter Med 49: 1307-1310, 2010)(DOI: 10.2169/internalmedicine.49.3278)
Introduction
Gliomatosis cerebri (GC) is a rare form of glioma de-scribed by Nevin (1) in 1938. According to the WorldHealth Organization (WHO) classification of brain tumorsGC is identified as a clinicopathological entity. In the fourthedition of the WHO classification of tumours of the centralnervous system, published in 2007, GC (code 9381/3) is de-fined as diffuse infiltration of neoplastic glial cells into atleast three lobes and preservation of the surrounding neuro-nal architecture (2). Neuroradiological profiles have been de-scribed in reports of pathology-proven GC patients (3-6).Here, we report a patient who had secondary GC which
mimicked the clinicoradiological course of limbic encephali-tis (LE).
Case Report
A 72-year-old man had developed headache, fever anddisorientation insidiously 2 weeks previously, and was ad-mitted to our department. Physical examination showedblood pressure of 148/90 mmHg and body temperature of37.8℃. Japan coma scale was 2 with confusion. Musclestretch reflexes were brisk in the right upper and lower ex-tremities without Babinski’s sign. The remaining neurologi-cal examination was normal. On routine laboratory testing,white cell count was increased to 17,000/mm3 (neutrophilic
Department of Neurology, Toho University Omori Medical Center, TokyoReceived for publication December 17, 2009; Accepted for publication April 19, 2010Correspondence to Dr. Ken Ikeda, [email protected]

Inter Med 49: 1307-1310, 2010 DOI: 10.2169/internalmedicine.49.3278
1308
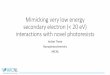
Figure 1. (A, B) CT shows unclear cerebral gyri in the left frontal and temporal regions. (C, D) Three months later CT shows a hemorrhagic mass with surrounding low density areas in the left frontal, parietal and temporal lobes.
leukocytes of 94.5%) and C-reactive protein was 1.1 mg/dL.Brain CT disclosed obscure cerebral gyri in the left frontaland temporal regions (Fig. 1A and 1B). Fluid-attenuated in-version recovery (FLAIR) imaging revealed hyperintensitysignal areas in bilateral frontal, the left parietal and the lefttemporal lobes. Hyperintense signal areas were also foundaround the posterior regions of bilateral lateral ventricles(Fig. 2A and 2B). Hyperintense lesions spread to the leftcerebral hemisphere, predominantly in the white matter(Fig. 2C). Slight enhancement was found in the left lowertemporal region (Fig. 2D-2F). Cerebral angiography exhib-ited no tumor stains. Repeated cerebrospinal fluid studiesshowed mild pleocytosis of 11-20 cells/mm3, increased pro-tein levels of 74-84 mg/dL, cytology of class I and negativeresults of infectious pathogenic tests, including herpes sim-plex, bacteria and fungus. Gallium scintigraphy of wholebody revealed no abnormal accumulation. Intravenous ad-ministration of dexamethasone and glycerol was performed.At 7 days after admission, his consciousness state becamenormal. A mild degree of short-term memory impairment re-mained at 2 months after clinical onset. Follow-up magneticresonance imaging (MRI) showed no remarkable changes.The clinical and neuroradiological courses suggested LE ofunknown origin. One month later, his disorientation was ex-acerbated. Brain CT showed a high density mass surroundedby low density areas in the left frontal, parietal and temporallobes (Fig. 1C and 1D). FLAIR imaging disclosed hypoin-tense and hyperintense signal massive lesions with surround-
ing hyperintense signal areas in the left temporal, frontaland parietal lobes. Hyperintense signal areas were notchanged in the right frontal and the right periventricular re-gions (Fig. 3A and 3B). Remarkable and irregular enhance-ment was seen in the left temporal, frontal and parietal lobes(Fig. 3C-3E). Urgent neurosurgery was performed and theneuropathological diagnosis of glioblastoma multiforme(GM) was confirmed.
Discussion
We report a patient with secondary GC mimicking LE attwo months after clinical onset. One month later, our patientshowed malignant transformation to massive GM, togetherwith exacerbation of disorientation.GC is divided into primary and the secondary types. Pri-mary GC is considered as de novo formation of glioma.Secondary GC results from the spreading of a focal glioma.In general, neuroradiological features of GC are known toreveal extensive lesions into the corpus callosum. MRI ap-pearances of typical GC show widespread T2-hyperintensityin the cerebral white matter without enhancement (3, 4).The initial MRI of the present patient displayed whitematter-predominant and infiltrative lesions in at least threelobes of the left cerebral hemisphere. Focal enhancement ormass effects have been described in several GC patientswhen malignant transformation was generated from a part ofGC (5-8). Therefore, the neuroradiological hallmarks of the

Inter Med 49: 1307-1310, 2010 DOI: 10.2169/internalmedicine.49.3278
1309
Figure 2. (A, B) Axial FLAIR imaging shows hyperintensity signal areas in bilateral frontal, the left parietal and temporal lobes. Ill-defined hyperintensity areas are shown in bilateral posterior periventricular regions. (C) Sagittal FLAIR imaging shows continuous hyperintense signal areas in the left temporal, frontal and parietal lobes. (D-F) Gadolinium-enhanced T1-weighted imaging shows faint enhancement in the left lower temporal lobe.
Figure 3. (A, B) Three months later FLAIR imaging shows a mixed signal intense mass and sur-rounding hyperintense signal areas in the left temporal, frontal and parietal lobes. Hyperintense signal areas are not altered in the right frontal and right periventricular regions. (C-E) Gadolinium-enhanced T1-weighted imaging shows marked enhancement in the left temporal, fron-tal and parietal lobes.

Inter Med 49: 1307-1310, 2010 DOI: 10.2169/internalmedicine.49.3278
1310
present patient were compatible with secondary GC. Itwould be of pathological importance to determine how oftenGC transforms to GM or malignant astrocytoma. Recentstudies highlight somatic mutations of isocitrate dehydroge-nases 1 and 2 genes in a majority of malignantgliomas (9, 10). Thus, genetic and neuropathological analy-ses are needed to elucidate the frequency of malignant trans-formation in GC patients.In general, the differential diagnosis of GC includes mul-tiple sclerosis, viral encephalitis, adrenoleukodystrophy,metachromatic leukodystrophy and subacute sclerosingpanencephalitis because cerebral lesions are confluent andextensive on CT and MRI. LE is characterized by infectious
or autoimmune inflammation in the limbic system. The mostcardinal sign is short-term memory impairment. Neurologi-cal symptoms typically develop over a few weeks. In thepresent case, despite the widespread MRI lesions, he hadonly a mild degree of short-tem memory dysfunction at 2months after clinical onset. This clinicoradiological profileled to the initial misdiagnosis of LE. The following month,massive lesions were revealed on CT and MRI. Thus, physi-cians should pay more attention to the differential diagnosesof GC and LE in patients who have minor memory deficitsand diffuse infiltrative MRI lesions. A brain biopsy is rec-ommended for an early diagnosis of GC when MRI lesionsare not attenuated on follow-up MRI.
References
1. Nevin S. Gliomatosis cerebri. Brain 61: 170-191, 1938.2. Louis DN, Ohgaki H, Wiestler OD, Cavenee WK. WHO Classifi-cation of Tumours of the Central Nervous System. 4th ed. IARCPress, Lyon, France, 2007.
3. Felsberg GJ, Silver SA, Brown MT, Tien RD. Gliomatosis cerebri:radiologic-pathologic correlation. AJNR Am J Neuroradiol 15:1745-1753, 1994.
4. delCarpio-O’Donovan R, Korah I, Salazar A, Melançon D.Gliomatosis cerebri. Radiology 198: 831-835, 1996.
5. Shin YM, Chang KH, Han MH, et al. Gliomatosis cerebri: com-parison of MR and CT features. AJR Am J Radiol 161: 859-862,1993.
6. Geremia GK, Wotlman R, Foust R. Computed tomography ofgliomatosis cerebri. Comput Assist Tomogr 12: 698-701, 1988.
7. Schwartz RB, Mantello MT. Primary brain tumors in adults.Semin Ultrasound CT MR 13: 449-472, 1992.
8. Kaloshi G, Guillevin R, Martin-Duverneuil N, et al. Gray matterinvolvement predicts chemosensitivity and prognosis in gliomato-sis cerebri. Neurology 73: 445-449, 2009.
9. Yan H, Parsons DW, Jin G, et al. IDH1 and IDH2 mutations ingliomas. N Engl J Med 360: 765-773, 2009.
10. Sonoda Y, Kumabe T, Nakamura T, et al. Analysis of IDH1 andIDH2 mutations in Japanese glioma patients. Cancer Sci 100:1996-1998, 2009.
Ⓒ 2010 The Japanese Society of Internal Medicinehttp://www.naika.or.jp/imindex.html