Embed Size (px)
Citation preview

松仁会医学誌 58 ⑴:15 ~ 20,2019
症例報告
A case report of neonatal craniotabes due to hypocalcemia and vitamin D deficiency related
to maternal lifestyle during pregnancy
Momoko Habu*, Masamichi Asazuma, Yukinori Watanabe, Satoshi Kidowaki, Kenichi Isoda
Department of Pediatrics, Matsushita Memorial Hospital *Clinical resident, Matsushita Memorial Hospital
Abstract: We present a case of neonatal craniotabes due to severe hypocalcemia and vitamin D deficiency. A female infant was born at 40 weeks of gestation by emergent cesarean section because of fetal dysfunction. The softened cranial bones were noticed at birth by the nursing care team. The edge of the wide anterior fontanel was unclear due to craniotabes of the markedly soft parietal bones, with abnormally separated sagittal sutures and delayed posterior fontanel fusion. There were no other orthopedic or neurological symptoms. The mother stayed at home and lost her appetite because of painful uterine contractions during pregnancy, resulting in reduced exposure to solar ultraviolet radiation and insufficient intake of calcium-rich food. Laboratory tests for the infant revealed serum concentrations of total calcium, ionized calcium, and 25-hydroxy
(OH) vitamin D of 7 .1 mg/dL, 0 . 96 mmol/L, and less than 4 .0 ng/mL, respectively. The serum intact parathyroid hormone level was elevated to 70 pg/mL, but the alkaline phosphatase level
(821 U/L) was within the normal range and no other rickets-associated changes were noted on radiography of her wrist and rib-bones. The infant was diagnosed with hypocalcemia secondary to vitamin D deficiency, and treated by oral supplementation of vitamin D (alfacalcidol, 0 . 1 µg/kg/day). The serum calcium level and 25-OH vitamin D level reached the normal range two days later after administration and remained kept stable after discontinuation of vitamin D supplementation. The craniotabes gradually improved by three months of age. We demonstrated the importance of examining the calcium levels in neonates with congenital craniotabes and in those with severe hypocalcemia due to serum vitamin D deficiency. It is also important to assess mothers with any high risk factors of sickness or malnutrition during pregnancy.
Key Words: Craniotabes, Hypocalcemia, Vitamin D, Rickets
2019 年 1 月 24 日受付連絡先:〒570-8540 大阪府守口市外島町 5 番 55 号 パナソニック健康保険組合 松下記念病院 小児科(磯田賢一) E-mail: [email protected] TEL: 06-6992-1231 利益相反:なし
Introduction
Craniotabes, the softening of skull bones, has largely been regarded as a physiological condi-tion of normal newborns not requiring treat-ment1). This condition is reported in up to 30% of normal neonates and is self-limiting, healing within 3 months1). On the other hand, craniota-bes is also found to be associated with the meta-

Kenichi Isoda16
bolic skeletal manifestation of rickets and several pathological conditions2, 3). In addition, previous studies demonstrated that lower levels of vita-min D as 25-hydroxy (OH) vitamin D in utero are associated with craniotabes2) and hypocalce-mia4) in normal neonates, leading to hypocalce-mic symptoms, including seizures5, 6). We present a case of neonatal craniotabes due to severe hy-pocalcemia and low vitamin D levels.
Case Presentation
A one-day-old full-term infant (at 40 week 0 day of gestation) was delivered by emergent caesarian section because of fetal distress weigh-ing 3,145 g with a healthy Apgar score of 9 pts at 1 min and 10 pts at 5 min. The nursing care team noticed softened cranial bones and consulted our department. This was the first pregnancy for the mother with her non-consanguineous husband. She had a normal body constitution (the weight [body mass index] during a non-pregnant period and during labor was 48 kg [18] and 63 kg [24], re-
spectively) without administration of tocolytic agents, such as magnesium sulfate, any history of smoking or alcohol use. She stayed at home dur-ing pregnancy because of painful uterine con-tractions, resulting in reduced exposure to solar ultraviolet radiation. Moreover, the mother lost her appetite during pregnancy and was restrict-ed to imbalanced diet by nature about calcium-rich foods, including seafood and dairy products, and she did not take nutritional or vitamin sup-plements. On physical examination, the baby had a normal birth weight of 3,145 g (+0.4 SD), height of 50.9 cm (+0.8 SD), and head circumference of 34.0 cm (+0.5 SD). The edge of the wide anterior fontanel was unclear due to craniotabes of the markedly soft parietal bones, with abnormally separated sagittal sutures and delayed posterior fontanel fusion. However, there were no other clinical signs of rickets or abnormal neurological findings. Laboratory blood tests on day 6 revealed a total calcium level of 7.1 mg/dL (normal values, 8.2 - 9.8 mg/dL), ionized calcium level of 0.96 mmol/L
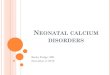
Fig. 1Radiographic studies of the skeleton revealed no splayed ribs (termed rachitic rosary) on chest X-ray (A), notable cupping, or fraying of the radial metaphysis (B; left arm, C; right arm of the infant).

17Neonatal craniotabes due to hypocalcemia and vitamin D deficiency
(normal values, 1.15 - 1.29 mmol/L), 25-OH vi-tamin D level of <4.0 ng/mL (normal values, more than 20 ng/mL), and parathyroid hormone (PTH) level of 70 pg/mL (normal values, 1-43 pg/mL). The thyroid hormone values, alkaline phosphatase lev-el (821 U/L; normal values less than 1,200 U/L), and phosphorus level were within normal limits
(Table 1). Urinalysis was normal. The biochemi-cal findings indicated marked hypocalcemia and vitamin D deficiency. Radiographic studies of the skeleton (Fig. 1) revealed no splayed ribs
(termed rachitic rosary), notable cupping, or fraying of the radial metaphysis. A small cardiac ventricular septal defect was found in the heart by ultrasound, but no other congenital abnormal-ity in the brain or kidney was observed. The bio-chemical examination for the infant suggested vitamin D deficiency in the mother, however, this possibility was not verified because the mother didn’t consent to the examination. The infant was treated by oral supplementation of vi-
tamin D (alfacalcidol; 1α(OH)D3) at 0.1 µg/kg/day, and was fed formula milk because the moth-er rejected breast feeding due to her beliefs and willingness. The serum calcium level immediate-ly increased to normal (Fig. 2, Table 1). On the thirty-ninth day from birth, the 25-OH vitamin D level reached 19.9 ng/mL and vitamin D was supplemented for 2 months in total. The cranio-tabes had gradually improved by three months of age. The infant was doing well with a normal total calcium level of 10.2 mg/dL and 25-OH vi-tamin D level of 26.5 ng/mL even after discon-tinuation of vitamin D supplementation (Fig. 2, Table 1). At the clinical follow-up at six months, the infant exhibited normal growth and develop-ment, and no signs of rickets.
Discussion
Our case suggests the importance of assessing the total and ionized calcium levels in
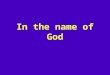
Fig. 2The graph shows the transition plots of the serum total calcium levels and vitamin D after alfacalcidol supplementation for the infant.
51015202530
2468
1012
Seru
m to
tal C
alsiu
m (m
g/dL
)
25-h
ydro
xy v
itam
in D
(µg/
mL)
Day 6 8 46 74
alphacalcidol
Serum total calsium 25-hydroxy vitamin D
Table 1
The biochemistry parameters of the infant are presented in the table.
Day 6 Day 8 Day 46 Day 74total calcium (mg/dL) 7.1 8.5 10.1 10.2ionized calcium (mmol/L) 0.96 1.23 1.40 1.3625-hydroxy vitamin D (µg/mL) <4.0 19.9 26.5alkaline phosphatase (U/L) 821 1,120 1,160phosphorus (mg/dL) 7.1 6.5 6.8

Kenichi Isoda18
neonates with congenital craniotabes, and the serum 25-OH vitamin D level in those with severe hypocalcemia. There were no complications of other metabolic/endocrine systems or other bone abnormalities besides the elevated serum PTH level, as reflected by a compensatory mechanism for hypocalcemia. Cupping of hand x-ray is represented as one of the earliest sign of rickets, but the radiographic exams were normal. In rickets, as in osteogenesis imperfecta, osteopathy of prematurity and other bone diseases, unexpected fractures occur with little or unrecognized injury and often with few clinical signs3). Moreover, primary hyperparathyroidism, congenital peudoparathyroidism, hypophosphatasia, osteogenesis imperfecta, hydrocephalus, and renal failure were excluded. Hypocalcemia secondary to vitamin D deficiency may present with neurological symptoms, including seizures or tetany4-6). The only source of vitamin D for the fetus is placental transfer from the mother. Maternal vitamin D deficiency was suggested to result in poor placental transfer of vitamin D during pregnancy, thereby reducing the storage of vitamin D in newborns7, 8). However, in our case, vitamin D deficiency in the mother was not confirmed because informed consent for maternal assessment was not obtained. Maternal vitamin D insufficiency during pregnancy is a common public health concern2, 3, 9, 10). The previous studies failed to show lower serum 25-OH vitamin D in mothers of newborns with craniotabes as compared with that of mothers of newborns without craniotabes11, 12). Paterson et al. reviewed that many cases of congenital rickets were identified because of the finding of craniotabes or an enlarged fontanelle, which has long been recognized as a physical sign of rickets3). The major source of vitamin D in adults is its synthesis in the skin under the influence of ultraviolet B radiation. Exposure to sunlight is inhibited by an indoor lifestyle and hospitalization due to sickness during pregnancy, including hyperemesis or
threatened premature delivery. The seasonal variation in incidence strongly suggests that craniotabes is associated with vitamin D deficiency in utero, and the seasonal variation most likely reflects the sun exposure time of pregnant women. Craniotabes was reported to be present in 22.0% neonates, and its incidence had obvious seasonal variations, highest in April-May and lowest in November in Japan2). In addition, vitamin D is obtained in part from the diet. Vitamin D deficiency in pregnant women can also result from other reasons such as an unbalanced diet (vegan, aversion to seafood, etc.) or administration of magnesium sulfate as a tocolytic agent. The recommended dietary intake of vitamin D during pregnancy is 7.0 µg/day in Japan (it remains a “recommendation”)13). However, Japan is a country in which systematic vitamin D supplementation is not performed either for pregnant women or for breast-fed infants and most food products are not fortified with vitamin D2). Some international studies have reported Vitamin D supplementation during pregnancy10, 14, 15), but it is controversial whether it improves the clinical outcomes of infants and mothers. Physicians should be aware of the nutritional condition during pregnancy, including vitamin D level, especially for mothers with high risk factors.
Conclusion
In conclusion, we demonstrated the importance of examining the calcium levels in neonates with congenital craniotabes, and in those with severe hypocalcemia due to serum 25-OH vitamin D deficiency. It is important to assess mothers with high risk factors such as sickness or malnutrition during pregnancy.
Conflict of Interest
The authors declare no conflicts of interest associated with this manuscript.

19Neonatal craniotabes due to hypocalcemia and vitamin D deficiency
References
1 ) Fox GN, Maier MK. Neonatal craniotabes. Am Fam Physician 1984 ; 30 : 149-151 .
2 ) Yorifuji J, Yorifuji T, Tachibana K, et al. Craniotabes in normal newborns: the earli-est sign of subclinical vitamin D deficiency. J Clin Endocrinol Metab 2008 ; 93 : 1784 -1788 .
3 ) Paterson CR, Ayoub D. Congenital rickets due to vitamin D deficiency in the mothers. Clin Nutr 2015 ; 34 : 793-798 .
4 ) Soliman A, Salama H, Alomar S, et al. Clini-cal, biochemical, and radiological manifesta-tions of vitamin D deficiency in newborns presented with hypocalcemia. Indian J En-docrinol Metab 2013 ; 17 : 697-703 .
5 ) Teaema FH, Al Ansari K. Nineteen cases of symptomatic neonatal hypocalcemia second-ary to vitamin D deficiency: a 2-year study. J Trop Pediatr 2010 ; 56 : 108-110 .
6 ) Camadoo L, Tibbott R, Isaza F. Maternal vi-tamin D deficiency associated with neonatal hypocalcaemic convulsions. Nutr J 2007 ; 6 : 23 .
7 ) Ladhani S, Srinivasan L, Buchanan C, et al. Presentation of vitamin D deficiency. Arch Dis Child 2004 ; 89 : 781-784 .
8 ) Misra M, Pacaud D, Petryk A, et al. Vita-min D deficiency in children and its man-agement: review of current knowledge and recommendations. Pediatrics 2008 ; 122 : 398-
417 .9 ) Shibata M, Suzuki A, Sekiya T, et al. High
prevalence of hypovitaminosis D in preg-nant Japanese women with threatened pre-mature delivery. J Bone Miner Metab 2011 ; 29 : 615-620 .
10) Roth DE, Leung M, Mesfin E, et al. Vitamin D supplementation during pregnancy: state of the evidence from a systematic review of randomised trials. BMJ 2017 ; 359 : j 5237 .
11) Kokkonen J, Koivisto M, Lautala P, et al. Se-rum calcium and 25-OH-D3 in mothers of newborns with craniotabes. J Perinat Med 1983 ; 11 : 127-131 .
12) Reif S, Katzir Y, Eisenberg Z, et al. Serum 25-hydroxyvitamin D levels in congenital craniotabes. Acta Paediatr Scand 1988 ; 77 : 167-168 .
13) “Nihonjin no Shokuji Sesshu Kijun (2015 year-version) Sakutei Iinkai Houkokusho, Chair person Hishida A” (in Japanease). ht tps ://wwwmhlwgojp/st f/houdou/ 0000041733html accessed on 2019/01/08 .
14) De-Regil LM, Palacios C, Lombardo LK, et al. Vitamin D supplementation for women during pregnancy. Cochrane Database Syst Rev 2016 : CD008873 .
15) Palacios C, De-Regil LM, Lombardo LK, et al. Vitamin D supplementation during preg-nancy: Updated meta-analysis on maternal outcomes. J Steroid Biochem Mol Biol 2016 ; 164 : 148-155 .

Kenichi Isoda20
母体生活様式に由来したと考えられるビタミンD欠乏と低カルシウム血症による新生児頭蓋癆の 1 例
羽生桃子*,浅妻正道,渡辺幸典,木戸脇智志,磯田賢一
パナソニック健康保険組合松下記念病院 小児科 *パナソニック健康保険組合松下記念病院 臨床研修医
抄録:ビタミンD欠乏症と低カルシウム血症による新生児頭蓋癆の一例を報告する.女児は,胎児機能不全のため緊急帝王切開で在胎 40 週,3,145gで出生した.出生時に軟らかい頭蓋骨を指摘された.頭蓋骨は過度に軟化し,大泉門辺縁が不明瞭,矢状縫合の開大と小泉門未閉鎖を認めた.頭蓋骨以外には骨軟化の所見はなく,また神経学的所見には異常を認めなかった.母は妊娠中自宅に閉じこもる機会が多く,食欲も減退していたため十分なカルシウム量の摂取が得られていなかった.日齢 6 の血液検査では,血清総カルシウム 7 .1mg/dL,イオン化カルシウム 0 .96mmol/Lおよび 25 水酸化ビタミンD 4 .0ng/mLといずれも著しい低値を示した.血清インタクト副甲状腺ホルモンは 70pg/mLに上昇していたが,アルカリフォスファターゼ(821U/L)は正常で,手根骨と胸郭レントゲンではくる病様変化を認めなかった.ビタミンD欠乏症性低カルシウム血症と診断し,経口ビタミンD製剤(アルファカルシドール,0.1µg/kg/日)による治療を開始した.血清カルシウム濃度と 25 水酸化ビタミンD濃度は 2 日後には正常化し,治療終了後も正常域に保たれたことを確認した.頭蓋癆は生後 3 か月までに次第に軽快した.新生児が先天性頭蓋癆を呈していた場合,血清カルシウム濃度の測定を行い,低値であった場合にはビタミンD欠乏症による重度の低カルシウム血症を念頭に置くことが重要である.妊娠期母体の体調不良による日光遮断や食欲不振のリスクファクターがみられる場合には注意が必要である.
キーワード:頭蓋癆,低カルシウム血症,ビタミンD,くる病