Embed Size (px)
Citation preview

[CANCER RESEARCH 52, 4987-4994, September 15, 1992)
A New Tumor-associated Antigen Useful for Serodiagnosis of Hepatocellular
Carcinoma, Defined by Monoclonal Antibody KM-2
Yasuyuki Kumagai, Joe Chiba, Tetsutaro Sata, Sachi Ohtaki,1 and Keiji Mitamura2
Department of Infectious Diseases, The Institute of Medical Science, The University of Tokyo, Tokyo [Y. K., K. M.J, Department of Biological Science and Technology, Science University of Tokyo, Chiba fJ. C.J, and Department of Pathology, National Institute of Health, Tokyo [J. C., T. S., S. O.], Japan
ABSTRACT
After immunization of mice with the human hepatocellular carcinoma(HCC) cell line PLC/PRF/5, we produced monoclonal antibody KM-2,which allowed us to characterize a new IK ( -associated antigen (KM-2antigen) and to develop a sandwich-type radioimmunoassay. The KM-2antigen was strongly expressed on the cell surface of HCC cell lines.Immunofluorescence staining of frozen sections of different tissues andtumors confirmed its specific expression on the cell surface of a group ofHCC. The antigen was also detected in the bile canaliculi of normalliver. Its biochemical characterization revealed a high molecular weight(Mr ~900,000) glycoprotein with an .V-linked carbohydrate chain closeto the peptide epitope recognized by the KM-2 monoclonal antibody. Bythe radioimmunoassay for the KM-2 antigen, the antigen was detectedin sera of 72 (47%) of 154 patients with HCC and 3 (3%) of 102 patientswith liver cirrhosis; it was not detected in 96 patients with chronichepatitis or in 100 healthy control individuals. The positive rate ofKM-2 antigen (72 of 154, 47%) was significantly (/' < 0.01) higher thanthat (51 of 154, 33%) of a-fetoprotein (AFP) when the cut-off level ofAFP was taken as the widely accepted 400 ng/ml. No significant correlation was recognized between serum levels of the KM-2 antigen andAFP (r = 0.15; P > 0.05). In addition, among 103 patients with HCCwhose AFP levels were less than 400 ng/ml, 31 (30%) were positive forthe KM-2 antigen. Determination of the serum KM-2 antigen would beuseful for the serodiagnosis of patients with HCC, particularly in caseswith normal or low AFP levels.
INTRODUCTION
HCC3 is one of the most common malignant tumors in the
world, and has a particularly high incidence in the Far East andsub-Saharan Africa (1). Recently, hepatic imaging by such techniques as ultrasound imaging and computed axial tomographyhas made it possible to reliably detect small HCC lesions of lessthan 3 cm in diameter and in screening programs for patientswith chronic liver diseases (2). Early detection of small HCClesions has proven to be important for the treatment of patientswith partial hepatectomy, and to result in better prognosis(3, 4). However, imaging techniques are not suitable for large-scale surveys of the general population. AFP is now usedthroughout the world for the early detection of HCC, followingthe finding that 69% of patients with HCC have serum AFP
Received 3/3/92; accepted 7/8/92.The costs of publication of this article were defrayed in part by the payment of
page charges. This article must therefore be hereby marked advertisement in accordance with 18 U.S.C. Section 1734 solely to indicate this fact.
1Present address: Department of Pathology, Hatano Research Institute, Foodand Drug Safety Center, Kanagawa, Japan.
2 Present address: Second Department of Internal Medicine, Showa UniversitySchool of Medicine, 1-5-8, Hatanodai, Shinagawa-ku, Tokyo 142, Japan. Towhom requests for reprints should be addressed.
3 The abbreviations used are: HCC, hepatocellular carcinoma; AFP, a-fetoprotein; LC, liver cirrhosis; mAb, monoclonal antibody; RIA, radioimmunoassay;DMEM, Dulbecco's modified Eagle's medium; PCS, fetal calf serum; PB, 50 IHMphosphate buffer, CH, chronic hepatitis; NP-40, Nonidet P-40; CEA, carcinoem-bryonic antigen; HBsAg, hepatitis B surface antigen; HBcAg, hepatitis B coreantigen; PBL, peripheral blood lymphocytes; BPA, Bauhinia purpurea agglutinin;GS, Griffonia simplicifolia agglutinin; PHA, phytohemagglutinin; RCA^, Ricinoscommuais agglutinin II; RCA12o, Ricinus communis agglutinin I; UEA, Ulex eu-ropaeus agglutinin; WGA, wheat germ agglutinin; AU, arbitrary unit; HBs, hepatitis B surface; HBc, hepatitis B core.
levels over 400 ng/ml (5, 6). However, recent reports showedthat only 36% of patients with HCC had serum AFP levels over320 ng/ml (7), and the prevalence of patients with HCC whohave normal or slightly elevated AFP levels has increased (8). Inaddition, in one follow-up study on patients with LC who developed to HCC, patients whose AFP level exceeded 400 ng/mlaccounted for only 10 of 40 cases (9). These findings point tothe limits of serum AFP level in the early detection of HCC.Des-7-carboxyprothrombin is also used for the diagnosis ofHCC, and plasma levels of this marker are elevated in 55-74%of patients with HCC (10-13). However, measurement ofplasma des-7-carboxyprothrombin levels alone is not sufficientfor the early detection of HCC ( 13). Therefore, to find an additional highly specific HCC-associated marker is still an important objective. Since the first antitumor mAb was generated(14), many attempts have been made by numerous investigatorsto generate mAbs that may have potential clinical applicationsin the diagnosis and therapy of HCC (15-22). However, nomAb has yet been generated that is useful for the serologicaldiagnosis of HCC.
In this paper, we report a new HCC-associated antigen defined by a mAb termed KM-2, which was raised against thewell-characterized human HCC cell line PLC/PRF/5 (23). Wealso report the development and clinical usefulness of a newsandwich-type RIA for this antigen with the use of the KM-2mAb.
MATERIALS AND METHODS
Cell Lines and Cell Culture. The following human cell lines wereused in this study: five HCCs [PLC/PRF/5, HuH-7 (24), Hep G2(25), Hep 3B (25), and Mahlavu (26)]; one gastric carcinoma (SC-1);one colon carcinoma (COLO-205); one pancreatic carcinoma (PANC-1); one gallbladder carcinoma (G-415); one lung carcinoma (A-549);one mammary carcinoma (ZR-75-1); one melanoma (G-361); one cervix carcinoma (HeLa); two Burkitt's lymphomas (Daudi and Raji);
one myeloma (GM1500); one of normal liver cells (Chang liver); one ofskin fibroblasts (BUD-8); one of amniotic membrane cells (FL); andtwo of lung diploid fibroblasts (HAIN-55 and IMR-90). PLC/PRF/5and Mahlavu cells were the generous gift of Dr. R. H. Purcell(NIH, Bethesda, MD); HuH-7 cells were from Dr. J. Sato (CancerInstitute, Okayama University Medical School, Okayama, Japan);SC-1 and G-415 cells were from Dr. S. Koyama (University of TsukubaSchool of Medicine, Tsukuba, Japan); HeLa, Raji, Chang liver, and FLcells were from Dr. S. Hayakawa (Dainabot Co., Tokyo, Japan); Daudicells were from Dr. H. Hamaguchi (University of Tsukuba School ofMedicine); GM1500 cells were from Dr. C. M. Croce (Wistar Institute,Philadelphia, PA); and HAIN-55 cells were from Dr. H. Okumura(National Institute of Health, Tokyo, Japan). Hep G2, Hep 3B, COLO-205, PANC-1, A-549, ZR-75-1, G-361, BUD-8, and IMR-90 cellswere obtained from the American Type Culture Collection (Rockville,MD). PLC/PRF/5 cells were cultured in minimum essential medium(GIBCO) supplemented with 45% basal medium Eagle (GIBCO)and 10% FCS. All other cell lines were grown in Dulbecco's modifiedEagle's medium (GIBCO, Grand Island, NY) containing 10% PCS
(GIBCO) and 0.1 ITIMnonessential amino acids (GIBCO). MouseSP2/0 myeloma cells and hybridomas were cultured in Dulbecco's
4987
on July 17, 2018. © 1992 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
MONOCLONAL ANTIBODY TO HEPATOCELLULAR CARCINOMA
modified Eagle's medium containing 20% NCTC 109 medium (GIB-
CO), 20% PCS, 1 mivisodium pyruvate, and 0.4 unit/ml bovine insulin(Sigma Chemical Co., St. Louis, MO).
mAb Production. A mAb, designated KM-2, that reacted with PLC/PRF/5 cells but not with human diploid fibroblasts (HAIN-55) was
obtained by fusing of SP2/0 mouse myeloma cells (27) and spleen cellsof a BALB/c mouse immunized with PLC/PRF/5 cells as described byKöhlerand Milstein (28) with a minor modification (29). Screening wasperformed by a complement-mediated cell lysis assay to obtain theHCC-associated antigen expressed on the HCC cell surface (30). Hy-bridomas were grown as ascites fluid in BALB/c mice using 2,6,10,14-
tetramethylpentadecane (pristane) (Aldrich, Chemical Co., Milwaukee,WI), and the KM-2 mAb was purified from ascites fluid by precipitationwith 50% saturated ammonium sulfate, followed by gel filtration on acolumn of Sephadex G-200 (Pharmacia LKB, Uppsala, Sweden) withPB, pH 7.4. Purified KM-2 mAb was used for capture and tracer antibodies for sandwich-type RIA (below). lodination of the purified KM-2mAb was carried out as described by Hunter and Greenwood (31). Theisotype of immunoglobulin was determined by the Ouchterlony methodby using a Mouse Monoclonal Typing Kit (The Binding Site Ltd.,Birmingham, United Kingdom), as well as anti-mouse Kand anti-mouseX light chain antibodies (Bethly Laboratory, Montgomery, TX). Theisotype of the KM-2 mAb was IgG2a and its light chain was K.
Tissue and Serum Specimens. Tissue specimens used in this studywere obtained from the following sites: 20 HCCs; 14 livers adjacentto HCC; 12 livers from patients with CH; two livers from patientswith acute hepatitis; two gastric cancers; two colon cancers; two lungcancers; and one ovarian cancer. These tissues were obtained fresh frompatients who underwent resection or needle biopsy for the respectivediseases, and were stored at -80°C until use. In addition, some of
normal tissues were obtained as rapidly as possible from autopsies. Thisstudy was approved by the Ethical Review Committee of the Institute ofMedical Science, the University of Tokyo. Serum specimens were obtained from 154 patients with HCC, 102 patients with LC, and 96patients with CH at the time of diagnosis, and 100 healthy controlindividuals. All sera were stored at -20°Cuntil use. Patients with liver
diseases were diagnosed on the basis of clinical and laboratory findings,including echography, computerized axial tomography, hepatic angiog-raphy, and/or liver histology according to the criteria by Leevy et al.(32).
Complement-mediated Cell lysis. Complement-mediated cell lysiswas determined as previously described (30). MCr-Labeled cells (5 xIO5) in 50 /¿Iof RPMI 1640 (Nissui Co., Tokyo, Japan) containing 5%
PCS were distributed in microplate wells with 50 id of appropriatediluted ascites fluid and 50 ß\of rabbit complement (1:4 dilution, Ce-darlane Laboratory, Ontario, Canada). After incubation for 45 min. at37°C,the supernatant was collected from each well with a Titertek
supernatant collection system (Flow Laboratories, Osaka, Japan) andcounted in a gamma counter. The percentage of complement-mediatedcell lysis with the KM-2 mAb was calculated by using the following
formula:
i of cytotoxicity :Test cpm —¿�background cpm
Maximal release cpm - background cpm x 100
Maximal release cpm was obtained by incubating 5lCr-labeled cells with0.05% NP-40 instead of rabbit complement.
Reactivity of KM-2 MAb with AFP, CEA, HBsAg, HBcAg andBlood Cells. To determine the reactivity of the KM-2 mAb with AFPand CEA, the KM-2 mAb, mAb to AFP (positive control), or mAb toCEA (negative control), was mixed with polystyrene beads (6.4 mm indiameter) coated with anti-mouse IgG antibody. Then each bead wasincubated with AFP or CEA labeled with 125I(31), and the radioactivity
on each bead was counted. Positive and negative controls gave 6027 and228 cpm, respectively. The reactivity with CEA was tested by the samemethod. Positive (mAb to CEA) and negative (mAb to AFP) controlsgave 2368 cpm and 80 cpm, respectively. Reactivity with HBsAg andHBcAg was determined with sandwich-type RIA for anti-HBs antibodyand competitive RIA for anti-HBc antibody (AUSAB and CORAB,
Dainabot Co., Tokyo, Japan), respectively. Human plasmas reactivewith anti-HBs antibody (positive control) and nonreactive with anti-HBs antibody (negative control) gave 8006 cpm and 90 cpm in the assayfor anti-HBs antibody. Human plasmas reactive with anti-HBc antibody (positive control) and nonreactive with anti-HBc antibody (negative control) gave 660 and 24,048 cpm in the competitive assay foranti-HBc antibody, respectively. Reactivity with PBL was determinedaccording to the method of human leukocyte antigen typing by thecomplement-dependent microcytotoxicity assay (33), using PBL obtained from 31 individuals with different human leukocyte antigen hap-lotypes. RBC were obtained from 10 individuals: 3 with blood type O,3 with type A, 3 with type B, and 1 with type AB. After the RBC wereincubated with the KM-2 mAb, the cells were stained with fluoresceinisothiocyanate-conjugated anti-mouse IgG antibodies. The stained cellswere analyzed by flow cytometry with a FACS IV (Becton Dickinson,San Jose, CA). Reactivity with blood group substances other than theABO blood groups was determined by using a panel of RBC (Selecto-gen, Ortho Diagnostics Systems, Raritan, NJ) according to the manufacturer's instructions.
Sandwich-type RIA. To detect the antigen recognized by the KM-2mAb in vitro, a sandwich-type RIA was developed with the use of theKM-2 mAb. PLC/PRF/5 cells were disrupted by repeated freezing andthawing followed by centrifugation at 10,000 x g for 10 min. Thesupernatant was used as the assay standard. The protein concentrationin the supernatant was determined by absorbance at 280 nm, and 1.0absorbance was defined as 1 AU of the antigen. Polystyrene beads(6.4 mm in diameter) were coated with the purified KM-2 mAb, andthen the beads were washed three times with PB, pH 7.4. Each bead wasincubated with the PLC/PRF/5 cell supernatant. After being washed inthe same manner, the beads were incubated with the 125I-labeled KM-2
mAb. Each bead was washed again and counted in a gamma counter. Anassay standard curve was constructed by plotting KM-2 antigen concentrations (AU/ml) versus cpm. Experimental results were convertedinto AU of KM-2 antigen per ml by comparison with this standardcurve.
Solubilization and Gel Filtration of Antigen. The supernatant of disrupted PLC/PRF/5 cells (above) was treated with 2% (v/v) of Tween-80for 60 min at 4°C.The soluble extract was recovered by ultracentrifu-gation at 105,000 x g for l h at 4°Cand the antigenic reactivity in the
extract was tested by the sandwich-type RIA. The solubili/ed antigensolution was eluted on a column of Sephacryl S-400 (Pharmacia) withPB, pH 7.4, containing 0.05% Tween-80. Fractions were assayed forantigen activity by the sandwich-type RIA and protein concentration byabsorbance at 280 nm. The column was calibrated by molecular weightmarkers: catalase (M, 232,000) (Pharmacia); ferritin (Mr 440,000)(Pharmacia); thyroglobulin (Mr 669,000) (Pharmacia); human IgM (Mr900,000) (Protogen AG, Läufelfingen,Switzerland); and Blue Dextran2000 (Pharmacia). The fractions containing the antigen recognized bythe KM-2 mAb were pooled and used for determination of the biochemical characteristics below.
Enzymatic Treatment of Antigen. The antigen was treated at 37°C
for the respective times with an equal volume of the following enzymesolutions: /3-chymotrypsin (2 units/ml) from bovine pancreas (EC 3.4.21.1) (Sigma) in PB, pH 7.4, for 2 h; /V-glycanase (10 units/ml) fromFlavobacterium meningosepticum (EC 3.5.1.52) (Genzyme Co., Boston,MA), in PB, pH 7.4, for 4 h; mixture of O-glycanase (25 milliunits/ml)from Diplococcus pneumoniae (EC 3.2.1.97) (Genzyme) and neuramini-dase (1 unit/ml) from Clostridium perfringens (EC 3.2.1.18) (Sigma) inPB, pH 6.0, for 4 h, according to the manufacturer's instructions. After
each treatment, antigenic reactivity in the reaction mixture was assayedby the sandwich-type RIA.
Inhibition Test with Lectins. The effect of various lectins was testedon the reaction of the KM-2 mAb with the antigen solubili/ed andpurified by gel filtration. The lectins used in the inhibition test were asfollows: BPA, concanavalin A, Dolichos biflorus agglutinin, GS-I, GS-II, /.inulina polyphemus agglutinin, Madura pomÃferaagglutinin, peanut agglutinin, soybean agglutinin, UEA-I, and WGA (all from E-YLaboratories, San Mateo, CA); and Lens culinaris agglutinin, PHA-E4,PHA-L4, RCA60, RCA,20, and UEA-II (all from Honen Co., Tokyo,
4988
on July 17, 2018. © 1992 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
MONOCLONAL ANTIBODY TO HEPATOCELLULAR CARCINOMA
Japan). Each lectin was dissolved in PB, pH 7.4, containing 1.5 IHMCaCl2. The lectin solution containing 1 mg/ml of the lectin was addedto an equal volume of the antigen solution. The antigenic reactivity inthe mixture was assayed by the sandwich-type RIA.
Indirect Immunofluorescence Tests. Cultured cells and frozen tissuesections were fixed in acetone for 10 min at room temperature. Thefixed cells and tissue sections were reacted with the KM-2 mAb, stainedwith fluorescent isothiocyanate-conjugated anti-mouse IgG antibodies(Organon Teknika Co., West Chester, PA), and observed with a fluorescence microscope (Olympus Optics Industries, Tokyo, Japan).
Measurement of KM-2 Antigen in Sera. The level of the KM-2antigen was tested in serum specimens obtained from 154 patients withHCC, 102 patients with LC, and 96 patients with CH, using the sandwich-type RIA described above. The level was also tested in 100 healthycontrol individuals. Each serum specimen was incubated with a beadcoated with the KM-2 mAb. After washing the bead, it was incubatedwith the I25l-Iabeled KM-2 mAb, washed again, and counted in agamma counter. The level of the KM-2 antigen in the serum specimenwas calculated from the standard curve, and expressed in AU/ml.
Levels of AFP and KM-2 Antigen in Sera. Levels of AFP in sera of154 patients with HCC were assayed by using a commercially availableRIA kit for AFP (a-FETO-RIABEAD, Dainabot). The results wereexpressed in ng/ml. The sera used in this assay were the same 154 serumspecimens in which levels of the KM-2 antigen were determined by thesandwich-type RIA. The comparison of serum levels of AFP and theKM-2 antigen was analyzed by Student's t test and the x2 test. A P value
of less than 0.05 was considered statistically significant (34). Levels ofAFP in sera of 102 patients with LC and 96 patients with CH weredetermined by the same methods.
RESULTS
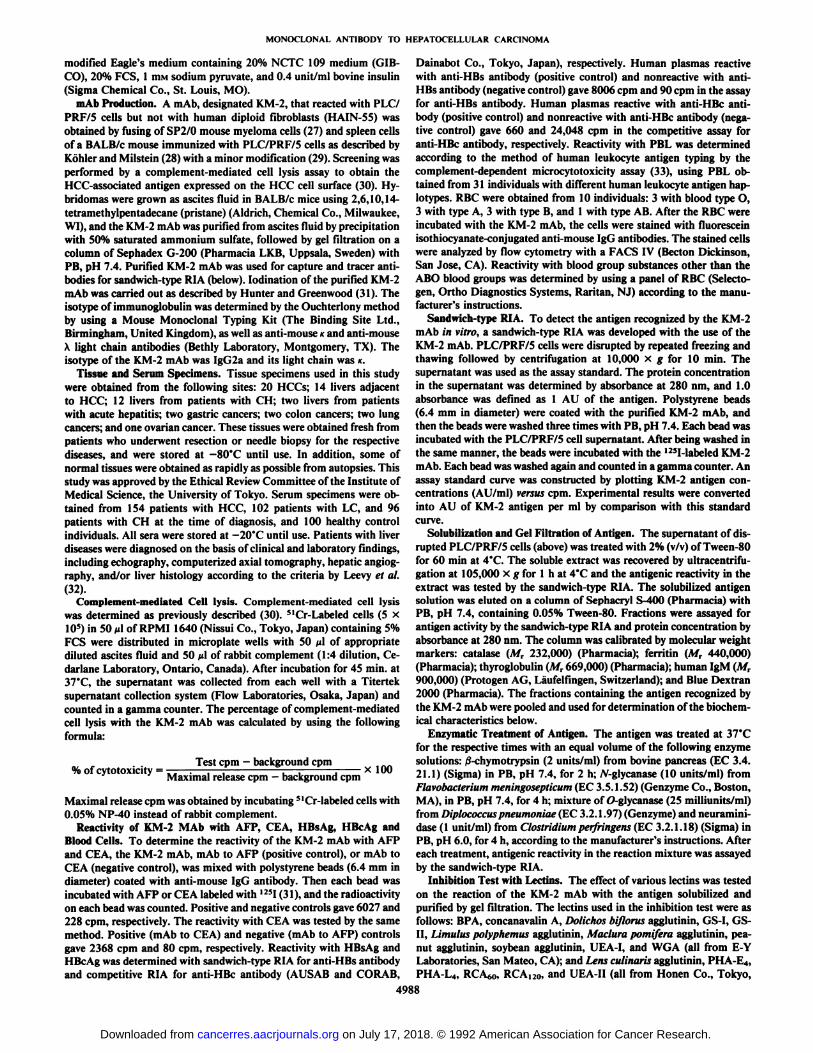
Specificity of KM-2 MAb. The reactivity of the KM-2 mAbwas studied by the complement-mediated cell lysis method(Fig. I). About 45% of 51Cr was released from PLC/PRF/5 cellsor HuH-7 cells by the KM-2 mAb in the presence of rabbitcomplement. Little or no cell lysis was observed at any dilutionof the KM-2 ascites fluid when Mahlavu cells, Chang liver cells,or human diploid IMR-90 cells were used as target cells. HepG2 and Hep 3B cells were also killed by the KM-2 mAb in thepresence of rabbit complement. All 14 of the other cell linestested were found to be negative by the complement-mediatedcell lysis assay (Table 1). All results obtained by cell lysis assay
Table 1 Reactivity of KM-2 mAb with human cell lines and blood cells
10'
DilutionFig. 1. Reactivity of the KM-2 mAb determined by complement-mediated cell
lysis assay. 51Cr-labeled PLC/PRF/5 (•),HuH-7 (O), Mahlavu (•).Chang liver(D), and IMR-90 (A) cells were distributed in microplate wells with appropriatedilutions of KM-2 ascites fluid and rabbit complement. After incubation, thesupernatant was collected from each well and counted in a gamma counter.
CelllinePLC/PRF/5HuH-7HepG2Hep
3BMahlavuSC-1COLO-205PANC-1G-415A-549ZR-75-1G-361HeLaDaudiRajiGM1500Chang
liverBUD-8FLHAIN-55IMR-90OriginHepatocellular
carcinomaHepatocellularcarcinomaHepatocellularcarcinomaHepatocellularcarcinomaHepatocellularcarcinomaGastriccarcinomaColoncarcinomaPancreaticcarcinomaGallbladdercarcinomaLungcarcinomaMammarycarcinomaMelanomaCervix
carcinomaBurkitt'slymphomaBurkitt'slymphomaMyelomaLiverSkin
fibroblastAmnioticmembraneLung
diploidfibroblastLungdiploid fibroblastReactivityCell
lysis" IFstaining'1+
+++++++——¿�——¿�——¿�——¿�——¿�-—¿�——¿�——¿�——¿�----——¿�——¿�——¿�——¿�--—
—¿�
Reactivity
Blood cells (individuals number) Cell lysisc IF staining*
PBL(3I)RBC(IO)
" Reactivity was determined by complement-mediated cell lysis assay with 100-fold diluted KM-2 mAb ascites fluid.
'' Reactivity was determined by indirect immunofluorescence staining with 100-fold diluted KM-2 mAb ascites fluid.
c Reactivity was determined by complement-dependent microcytotoxicity assay
with the human leukocyte antigen typing methods.d Reactivity was determined by flow cytometry.
were confirmed by immunofluorescence staining (Table 1).Amounts of the antigen defined by the KM-2 mAb (hereafterreferred to as KM-2 antigen) in 5 HCC cell lines and Changliver cells were determined by sandwich-type RIA (below). Theorder of KM-2 antigen per wet weight of cells was: PLC/PRF/5> Hep G2 > Hep 3B > HuH-7. Antigen was not detected inMahlavu and Chang liver cells (data not shown). The antigendefined by KM-2 mAb was detected by indirect immunofluorescence on the surface of almost all PLC/PRF/5 cells (Fig. 2a)and HuH-7 cells (not shown). None of the PBL from 31 individuals or RBC from 10 individuals were positive for the KM-2antigen (data not shown). The KM-2 mAb did not react withAFP, CEA, HBsAg, or HBcAg (data not shown). In addition,the KM-2 mAb was nonreactive with a panel of blood groupsubstances tested (data not shown).
Expression of KM-2 Antigen in Vivo. Expression of the antigen recognized by the KM-2 mAb in vivo was further investigated by indirect immunofluorescence.
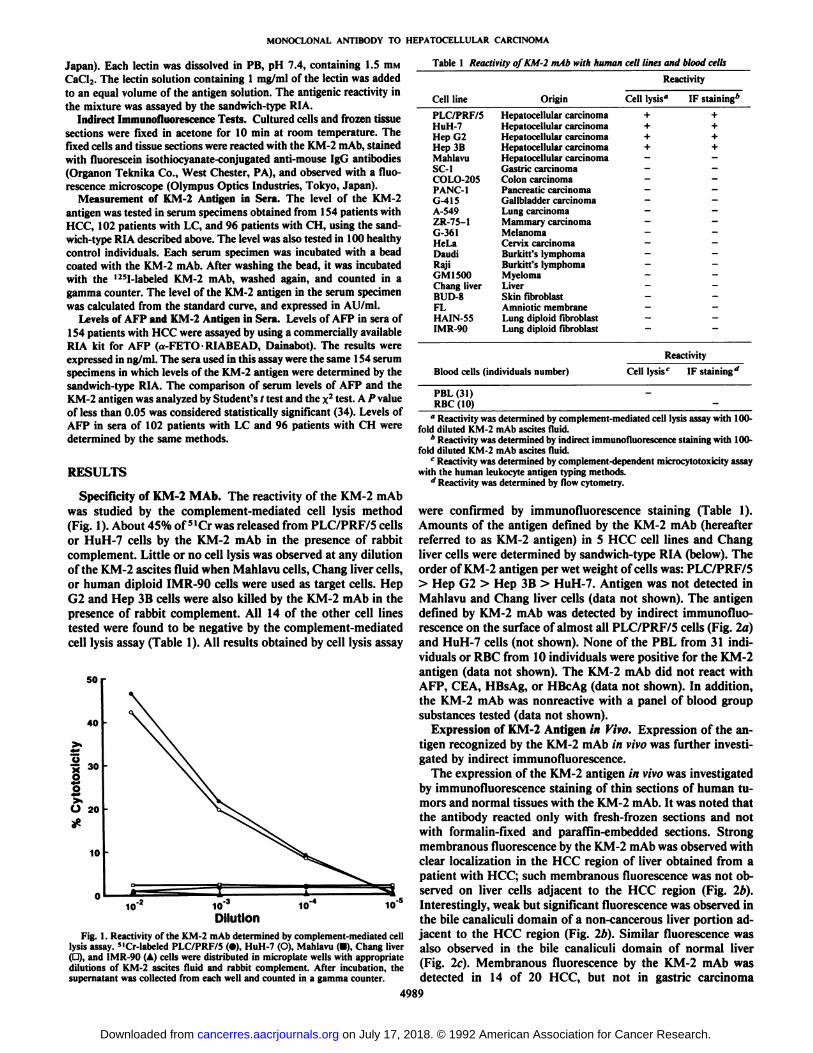
The expression of the KM-2 antigen in vivo was investigatedby immunofluorescence staining of thin sections of human tumors and normal tissues with the KM-2 mAb. It was noted thatthe antibody reacted only with fresh-frozen sections and notwith formalin-fixed and paraffin-embedded sections. Strongmembranous fluorescence by the KM-2 mAb was observed withclear localization in the HCC region of liver obtained from apatient with HCC; such membranous fluorescence was not observed on liver cells adjacent to the HCC region (Fig. 2¿>).Interestingly, weak but significant fluorescence was observed inthe bile canaliculi domain of a non-cancerous liver portion adjacent to the HCC region (Fig. 2¿>).Similar fluorescence wasalso observed in the bile canaliculi domain of normal liver(Fig. 2c). Membranous fluorescence by the KM-2 mAb wasdetected in 14 of 20 HCC, but not in gastric carcinoma
4989
on July 17, 2018. © 1992 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
MONOCLONAL ANTIBODY TO HEPATOCELLULAR CARCINOMA
Fig. 2. Indirect immunofluorescence staining of PLC/PRF/5 HCC cells, andHCC and normal liver tissues. PLC/PRF/5 cells (a, x 400) and the frozen tissuesections (b and c, X 200) were fixed with acetone, reacted with the KM-2 mAb,and stained with fluorescein isothiocyanate-conjugated anti-mouse IgG antibody.Strong membranous staining was observed on both PLC/PRF/5 cells (a) and theHCC region in liver tissue obtained from a patient with HCC (A). Note weak butsignificant fluorescence (arrow) in the bile canaliculi domain of a noncancerousliver portion adjacent to the HCC region (b) and liver from a subject without liverdisease (c). In c, many granules which show yellow nonspecific fluorescence are
(2 cases), colon adenocarcinoma (2 cases), lung carcinoma(2 cases), or ovarian carcinoma (1 case). In addition, no membranous fluorescence was detected in the non-cancerous liverportion of 14 liver specimens obtained from patients with HCC,12 from CH, and 2 from acute hepatitis. No staining was foundon normal tissues tested: liver (2 biopsy and 4 autopsy cases),
stomach (1 biopsy and 3 autopsy cases), colon (2 biopsy and4 autopsy cases), lung (1 biopsy and 2 autopsy cases), kidney(2 biopsy and 5 autopsy cases) and pancreas (4 autopsy cases)(Table 2). Expression of the KM-2 antigen in carcinoma but notin normal tissue parts of liver obtained from HCC patients wasconfirmed by absorption analysis by using the paired HCC andliver adjacent to the HCC from the same patients (data notshown).
Development of Sandwich-type RIA for Antigen. We havedeveloped a solid-phase sandwich-type RIA in which the KM-2mAb is used both as a capture antibody and as an 125I-labeled
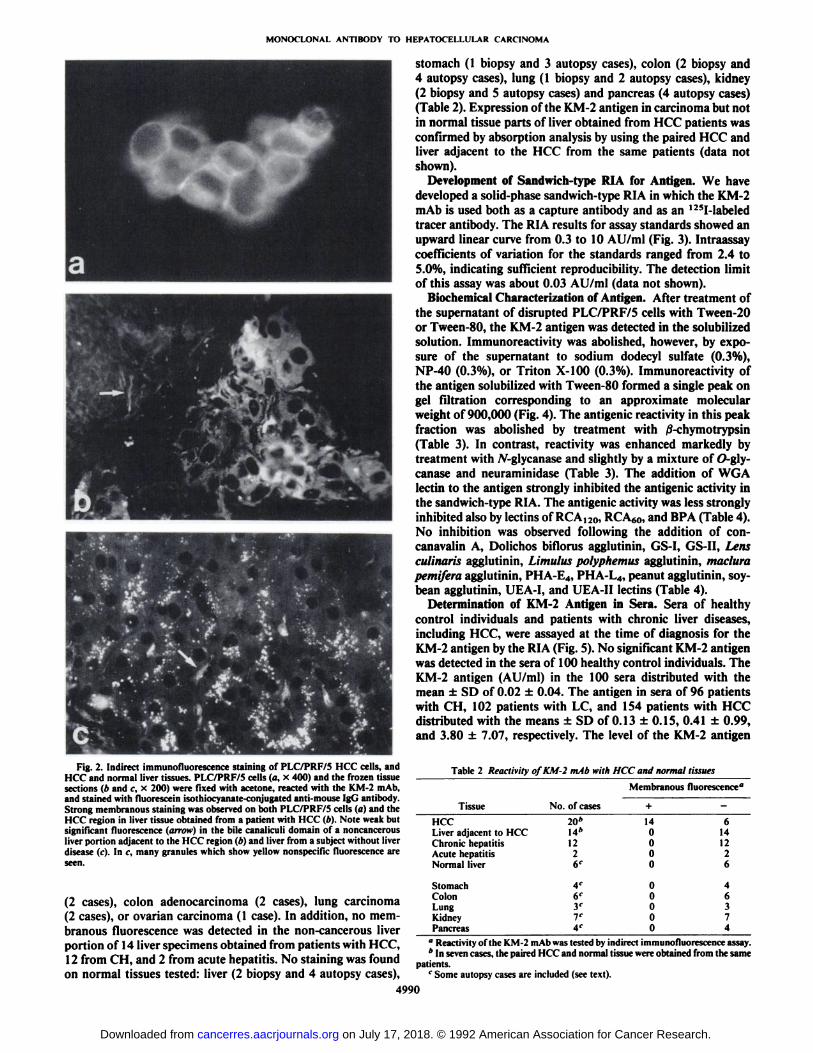
tracer antibody. The RIA results for assay standards showed anupward linear curve from 0.3 to 10 AU/ml (Fig. 3). Intraassaycoefficients of variation for the standards ranged from 2.4 to5.0%, indicating sufficient reproducibility. The detection limitof this assay was about 0.03 AU/ml (data not shown).
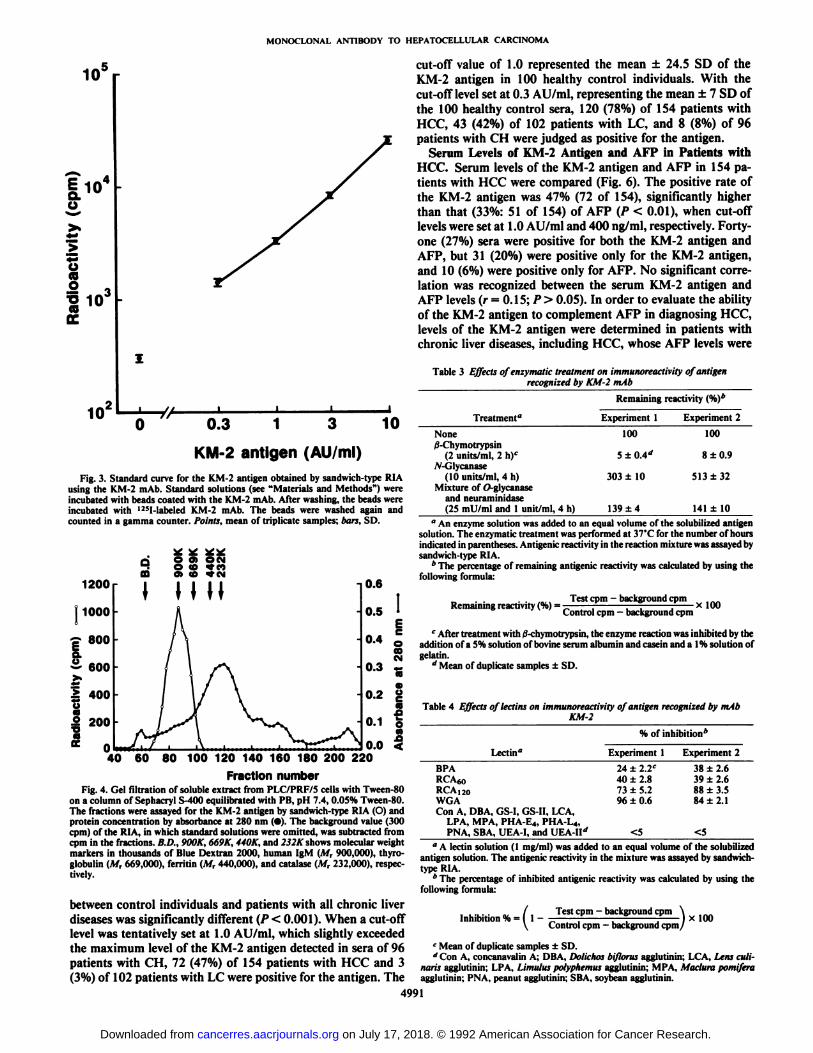
Biochemical Characterization of Antigen. After treatment ofthe supernatant of disrupted PLC/PRF/5 cells with Tween-20or Tween-80, the KM-2 antigen was detected in the solubili/edsolution. Immunoreactivity was abolished, however, by exposure of the supernatant to sodium dodecyl sulfate (0.3%),NP-40 (0.3%), or Triton X-100 (0.3%). Immunoreactivity ofthe antigen solubilized with Tween-80 formed a single peak ongel filtration corresponding to an approximate molecularweight of 900,000 (Fig. 4). The antigenic reactivity in this peakfraction was abolished by treatment with /3-chymotrypsin(Table 3). In contrast, reactivity was enhanced markedly bytreatment with jV-glycanase and slightly by a mixture of O-gly-canase and neuraminidase (Table 3). The addition of WGAlectin to the antigen strongly inhibited the antigenic activity inthe sandwich-type RIA. The antigenic activity was less stronglyinhibited also by lectins of RCA,20, RCA60, and BPA (Table 4).No inhibition was observed following the addition of con-canavalin A, Dolichos biflorus agglutinin, GS-I, GS-II, Lensculinaria agglutinin, Limulus polyphemus agglutinin, madurapemifera agglutinin, PHA-E4, PHA-L4, peanut agglutinin, soybean agglutinin, LJEA-I, and UEA-II lectins (Table 4).
Determination of KM-2 Antigen in Sera. Sera of healthycontrol individuals and patients with chronic liver diseases,including HCC, were assayed at the time of diagnosis for theKM-2 antigen by the RIA (Fig. 5). No significant KM-2 antigenwas detected in the sera of 100 healthy control individuals. TheKM-2 antigen (AU/ml) in the 100 sera distributed with themean ±SD of 0.02 ±0.04. The antigen in sera of 96 patientswith CH, 102 patients with LC, and 154 patients with HCCdistributed with the means ±SD of 0.13 ±0.15, 0.41 ±0.99,and 3.80 ±7.07, respectively. The level of the KM-2 antigen
Table 2 Reactivity of KM-2 mAb with HCC and normal tissues
Membranous fluorescence0
TissueHCCLiver
adjacent toHCCChronichepatitisAcutehepatitisNormalliverStomachColonLungKidneyPancreasNo.
ofcases20*14*1226C4C6'y7e4e+14000000000-614122646374
" Reactivity of the KM-2 mAb was tested by indirect immunofluorescence assay.* In seven cases, the paired HCC and normal tissue were obtained from the same
patients.c Some autopsy cases are included (see text).
4990
on July 17, 2018. © 1992 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
MONOCLONAL ANTIBODY TO HEPATOCELLULAR CARCINOMA
E •¿�au>»">so(O
10'0.3 1 3
KM-2 antigen (AU/ml)
10
Fig. 3. Standard curve for the KM-2 antigen obtained by sandwich-type RIAusing the KM-2 mAb. Standard solutions (see "Materials and Methods") wereincubated with beads coated with the KM-2 mAb. After washing, the beads wereincubated with I25l-labeled KM-2 mAb. The beads were washed again andcounted in a gamma counter. Points, mean of triplicate samples; bars, SD.
1200
| 1000
ç 800a.a eoo
i 400u
I 200
0.6
0.5
0.4 0co«M°-3e«0.2 "
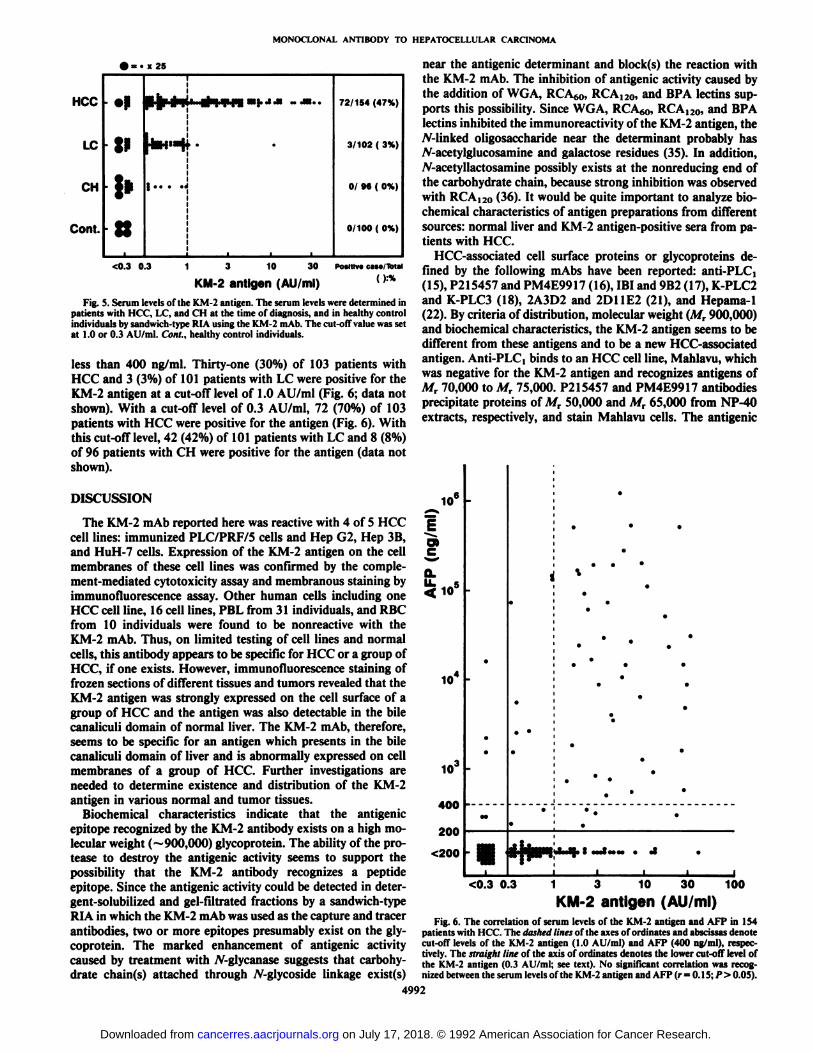
cut-off value of 1.0 represented the mean ±24.5 SD of theKM-2 antigen in 100 healthy control individuals. With thecut-off level set at 0.3 AU/ml, representing the mean ±7 SD ofthe 100 healthy control sera, 120 (78%) of 154 patients withHCC, 43 (42%) of 102 patients with LC, and 8 (8%) of 96patients with CH were judged as positive for the antigen.
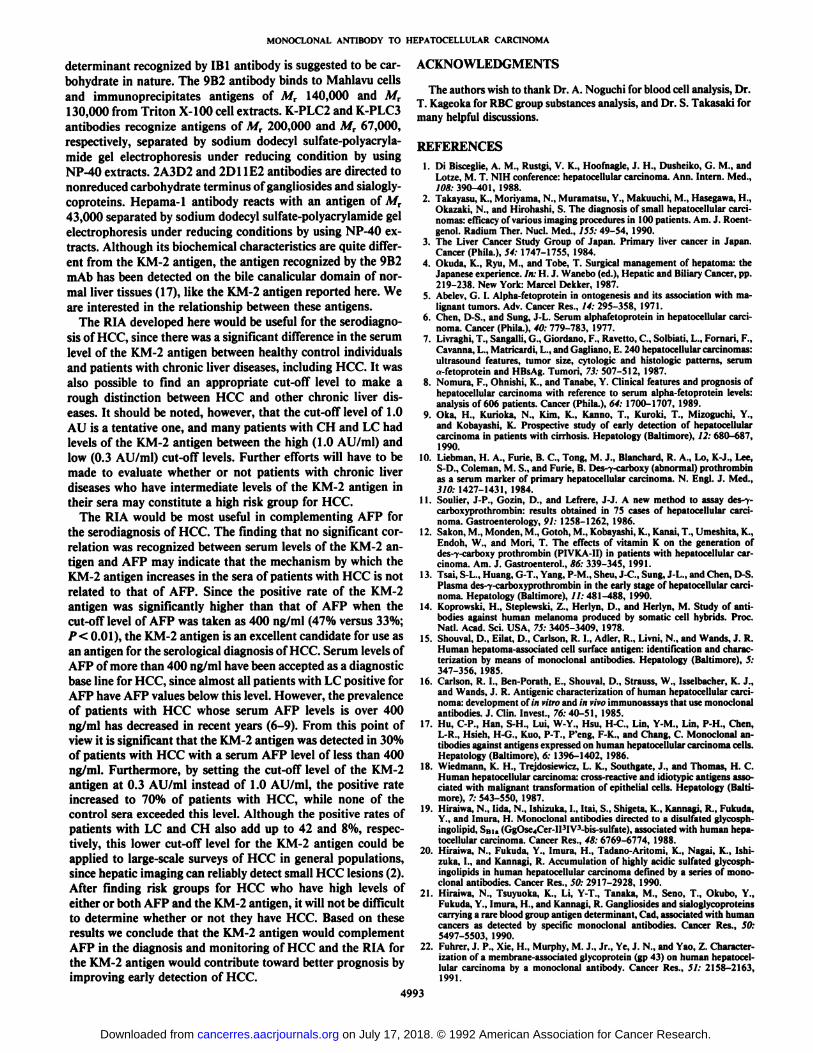
Serum Levels of KM-2 Antigen and AFP in Patients withHCC. Serum levels of the KM-2 antigen and AFP in 154 patients with HCC were compared (Fig. 6). The positive rate ofthe KM-2 antigen was 47% (72 of 154), significantly higherthan that (33%: 51 of 154) of AFP (P < 0.01), when cut-offlevels were set at 1.0 AU/ml and 400 ng/ml, respectively. Forty-one (27%) sera were positive for both the KM-2 antigen andAFP, but 31 (20%) were positive only for the KM-2 antigen,and 10 (6%) were positive only for AFP. No significant correlation was recognized between the serum KM-2 antigen andAFP levels (r = 0.15; P > 0.05). In order to evaluate the abilityof the KM-2 antigen to complement AFP in diagnosing HCC,levels of the KM-2 antigen were determined in patients withchronic liver diseases, including HCC, whose AFP levels were
Table 3 Effects of enzymatic treatment on immunoreactivity of antigenrecognized by KM-2 mAb
Remaining reactivity (%)*
°-1g0.0 <'40 60 80 100 120 140 160 180 200 220
Fraction numberFig. 4. Gel filtration of soluble extract from PLC/PRF/5 cells with Tween-80
on a column of Sephacryl S-400 equilibrated with PB, pH 7.4, 0.05% Tween-80.The fractions were assayed for the KM-2 antigen by sandwich-type RIA (O) andprotein concentration by absorbance at 280 nm (•).The background value (300cpm) of the RIA, in which standard solutions were omitted, was subtracted fromcpm in the fractions. B.D., 900K, 669K, 440K, and 232K shows molecular weightmarkers in thousands of Blue Dextran 2000, human IgM (M, 900,000), thyro-globulin (M, 669,000), ferritin (M, 440,000), and catalase (M, 232,000), respectively.
between control individuals and patients with all chronic liverdiseases was significantly different (P < 0.001). When a cut-offlevel was tentatively set at 1.0 AU/ml, which slightly exceededthe maximum level of the KM-2 antigen detected in sera of 96patients with CH, 72 (47%) of 154 patients with HCC and 3(3%) of 102 patients with LC were positive for the antigen. The
Treatment"None
/3-Chymotrypsin(2 units/ml, 2 h)c
W-Glycanase(10 units/ml, 4 h)
Mixture of O-glycanaseand neuraminidase(25 mU/ml and 1 unit/ml, 4 h)Experiment
1100303
±10139
±4Experiment
2100
8 ±0.9
513±32141
±10" An enzyme solution was added to an equal volume of the solubilized antigen
solution. The enzymatic treatment was performed at 37°Cfor the number of hours
indicated in parentheses. Antigenic reactivity in the reaction mixture was assayed bysandwich-type RIA.
'' The percentage of remaining antigenic reactivity was calculated by using the
following formula:
Remaining reactivity (%) =Test cpm —¿�background cpm
Control cpm - background cpm x 100
c After treatment with 0-chymotrypsin, the enzyme reaction was inhibited by the
addition of a 5% solution of bovine serum albumin and casein and a 1% solution ofgelatin.
d Mean of duplicate samples ±SD.
Table 4 Effects oflectins on immunoreactivity of antigen recognized by mAbKM-2
% ofinhibition*Lectin"BPA
RCA60RCA I20WGAExperiment
124±2.2C
40 ±2.873 ±5.296 ±0.6Experiment
238
±2.639 ±2.688 ±3.584 ±2.1
Con A, DBA, GS-I, GS-II, LCA,LPA, MPA, PHA-E4, PHA L4,PNA, SBA, UEA-I, and UEA-IIrf <5
" A lectin solution (1 mg/ml) was added to an equal volume of the solubilizedantigen solution. The antigenic reactivity in the mixture was assayed by sandwich-type RIA.
'' The percentage of inhibited antigenic reactivity was calculated by using the
following formula:
lnIliIlilion ",iTest cpm - background cpm \
Control cpm —¿�background cpm/ x 100
c Mean of duplicate samples ±SD.''Con A, concanavalin A; DBA, Dolichos bifloras agglutinin; LCA, Lens culi
narii agglutinin: LPA, Limulus polyphemus agglutinin; MPA, Madura pomÃferaagglutinin; PNA, peanut agglutinin; SBA, soybean agglutinin.
4991
on July 17, 2018. © 1992 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
MONOCLONAL ANTIBODY TO HEPATOCELLULAR CARCINOMA
•¿�= •¿�x 25
HCC
LC
CH
Cont.
•¿�P
IP
«"!•"'•"-•*•72/154 (47%)
3/102 ( 3%)
0 96 ( 0%)
0/100 ( 0%)
<0.3 0.3 10 30 Positive can/Total
KM-2 antigen (AU/ml)
Fig. 5. Serum levels of the KM-2 antigen. The serum levels were determined inpatients with HCC, LC, and CH at the time of diagnosis, and in healthy controlindividuals by sandwich-type RIA using the KM-2 mAb. The cut-off value was setat 1.0 or 0.3 AU/ml. Cont., healthy control individuals.
less than 400 ng/ml. Thirty-one (30%) of 103 patients withHCC and 3 (3%) of 101 patients with LC were positive for theKM-2 antigen at a cut-off level of 1.0 AU/ml (Fig. 6; data notshown). With a cut-off level of 0.3 AU/ml, 72 (70%) of 103patients with HCC were positive for the antigen (Fig. 6). Withthis cut-off level, 42 (42%) of 101 patients with LC and 8 (8%)of 96 patients with CH were positive for the antigen (data notshown).
DISCUSSION
The KM-2 mAb reported here was reactive with 4 of 5 HCCcell lines: immunized PLC/PRF/5 cells and Hep G2, Hep 3B,and HuH-7 cells. Expression of the KM-2 antigen on the cellmembranes of these cell lines was confirmed by the complement-mediated cytotoxicity assay and membranous staining byimmunofluorescence assay. Other human cells including oneHCC cell line, 16 cell lines, PBL from 31 individuals, and RBCfrom 10 individuals were found to be nonreactive with theKM-2 mAb. Thus, on limited testing of cell lines and normalcells, this antibody appears to be specific for HCC or a group ofHCC, if one exists. However, immunofluorescence staining offrozen sections of different tissues and tumors revealed that theKM-2 antigen was strongly expressed on the cell surface of agroup of HCC and the antigen was also detectable in the bilecanaliculi domain of normal liver. The KM-2 mAb, therefore,seems to be specific for an antigen which presents in the bilecanaliculi domain of liver and is abnormally expressed on cellmembranes of a group of HCC. Further investigations areneeded to determine existence and distribution of the KM-2antigen in various normal and tumor tissues.
Biochemical characteristics indicate that the antigenicepitope recognized by the KM-2 antibody exists on a high molecular weight (~ 900,000) glycoprotein. The ability of the protease to destroy the antigenic activity seems to support thepossibility that the KM-2 antibody recognizes a peptideepitope. Since the antigenic activity could be detected in deter-gent-solubilized and gel-filtrated fractions by a sandwich-typeRIA in which the KM-2 mAb was used as the capture and tracerantibodies, two or more epitopes presumably exist on the glycoprotein. The marked enhancement of antigenic activitycaused by treatment with TV-glycanase suggests that carbohydrate chain(s) attached through jV-glycoside linkage exist(s)
near the antigenic determinant and block(s) the reaction withthe KM-2 mAb. The inhibition of antigenic activity caused bythe addition of WGA, RCA60, RCA120, and BPA lectins supports this possibility. Since WGA, RCA60, RCA120, and BPAlectins inhibited the immunoreactivity of the KM-2 antigen, theY linked oligosaccharide near the determinant probably hasjV-acetylglucosamine and galactose residues (35). In addition,yV-acetyllactosamine possibly exists at the nonreducing end ofthe carbohydrate chain, because strong inhibition was observedwith RCA ,20 (36). It would be quite important to analyze biochemical characteristics of antigen preparations from differentsources: normal liver and KM-2 antigen-positive sera from patients with HCC.
HCC-associated cell surface proteins or glycoproteins defined by the following mAbs have been reported: anti-PLC]( 15), P215457 and PM4E9917 ( 16), IBI and 9B2 ( 17), K-PLC2and K-PLC3 (18), 2A3D2 and 2D11E2 (21), and Hepama-1(22). By criteria of distribution, molecular weight (Mr 900,000)and biochemical characteristics, the KM-2 antigen seems to bedifferent from these antigens and to be a new HCC-associatedantigen. Anti-PLC, binds to an HCC cell line, Mahlavu, whichwas negative for the KM-2 antigen and recognizes antigens ofA/r 70,000 to Mr 75,000. P215457 and PM4E9917 antibodiesprecipitate proteins of MT 50,000 and Mr 65,000 from NP-40extracts, respectively, and stain Mahlavu cells. The antigenic
10°
<10=
io-
400
200
<200 l ¿H»* |MM . 4
<0.3 0.3 1 3 10 30 100KM-2 antigen (AU/ml)
Fig. 6. The correlation of serum levels of the KM-2 antigen and AFP in 154patients with HCC. The dashed lines of the axes of ordinales and abscissas denotecut-off levels of the KM-2 antigen (1.0 AU/ml) and AFP (400 ng/ml), respectively. The straight line of the axis of ordinales denotes the lower cut-off level ofthe KM-2 antigen (0.3 AU/ml; see text). No significant correlation was recognized between the serum levels of the KM-2 antigen and AFP (r = 0.15; P > 0.05).
4992
on July 17, 2018. © 1992 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
MONOCLONAL ANTIBODY TO HEPATOCELLULAR CARCINOMA
determinant recognized by IBI antibody is suggested to be carbohydrate in nature. The 9B2 antibody binds to Mahlavu cellsand immunoprecipitates antigens of Mr 140,000 and A/r130,000 from Triton X-100 cell extracts. K-PLC2 and K-PLC3
antibodies recognize antigens of A/r 200,000 and A/r 67,000,respectively, separated by sodium dodecyl sulfate-polyacryla-
mide gel electrophoresis under reducing condition by usingNP-40 extracts. 2A3D2 and 2D11E2 antibodies are directed tononreduced carbohydrate terminus of gangliosides and sialogly-coproteins. Hepama-1 antibody reacts with an antigen of A/r43,000 separated by sodium dodecyl sulfate-polyacrylamide gelelectrophoresis under reducing conditions by using NP-40 extracts. Although its biochemical characteristics are quite different from the KM-2 antigen, the antigen recognized by the 9B2mAb has been detected on the bile canalicular domain of normal liver tissues (17), like the KM-2 antigen reported here. Weare interested in the relationship between these antigens.
The RIA developed here would be useful for the serodiagno-
sis of HCC, since there was a significant difference in the serumlevel of the KM-2 antigen between healthy control individualsand patients with chronic liver diseases, including HCC. It wasalso possible to find an appropriate cut-off level to make arough distinction between HCC and other chronic liver diseases. It should be noted, however, that the cut-off level of 1.0
AU is a tentative one, and many patients with CH and LC hadlevels of the KM-2 antigen between the high (1.0 AU/ml) andlow (0.3 AU/ml) cut-off levels. Further efforts will have to bemade to evaluate whether or not patients with chronic liverdiseases who have intermediate levels of the KM-2 antigen intheir sera may constitute a high risk group for HCC.
The RIA would be most useful in complementing AFP forthe serodiagnosis of HCC. The finding that no significant correlation was recognized between serum levels of the KM-2 antigen and AFP may indicate that the mechanism by which theKM-2 antigen increases in the sera of patients with HCC is notrelated to that of AFP. Since the positive rate of the KM-2
antigen was significantly higher than that of AFP when thecut-off level of AFP was taken as 400 ng/ml (47% versus 33%;P< 0.01), the KM-2 antigen is an excellent candidate for use asan antigen for the serological diagnosis of HCC. Serum levels ofAFP of more than 400 ng/ml have been accepted as a diagnosticbase line for HCC, since almost all patients with LC positive forAFP have AFP values below this level. However, the prevalenceof patients with HCC whose serum AFP levels is over 400ng/ml has decreased in recent years (6-9). From this point ofview it is significant that the KM-2 antigen was detected in 30%of patients with HCC with a serum AFP level of less than 400ng/ml. Furthermore, by setting the cut-off level of the KM-2antigen at 0.3 AU/ml instead of 1.0 AU/ml, the positive rateincreased to 70% of patients with HCC, while none of thecontrol sera exceeded this level. Although the positive rates ofpatients with LC and CH also add up to 42 and 8%, respectively, this lower cut-off level for the KM-2 antigen could beapplied to large-scale surveys of HCC in general populations,since hepatic imaging can reliably detect small HCC lesions (2).After finding risk groups for HCC who have high levels ofeither or both AFP and the KM-2 antigen, it will not be difficultto determine whether or not they have HCC. Based on theseresults we conclude that the KM-2 antigen would complement
AFP in the diagnosis and monitoring of HCC and the RIA forthe KM-2 antigen would contribute toward better prognosis byimproving early detection of HCC.
ACKNOWLEDGMENTS
The authors wish to thank Dr. A. Noguchi for blood cell analysis, Dr.T. Kageoka for RBC group substances analysis, and Dr. S. Takasaki formany helpful discussions.
REFERENCES1. Di Bisceglie. A. M., Rustgi, V. K., Hoofnagle, J. H., Dusheiko, G. M., and
Lotze, M. T. NIH conference: hepatocellular carcinoma. Ann. Intern. Med.,108: 390-401, 1988.
2. Takayasu, K., Moriyama, N., Muramatsu, Y., Makuuchi, M., Hasegawa, H.,Okazaki, N., and Hirohashi, S. The diagnosis of small hepatocellular carcinomas: efficacy of various imaging procedures in 100 patients. Am. J. Roent-genol. Radium Ther. NucÃ.Med., 755:49-54, 1990.
3. The Liver Cancer Study Group of Japan. Primary liver cancer in Japan.Cancer (Phila.), 54: 1747-1755, 1984.
4. Okuda, K., Ryu, M., and Tobe, T. Surgical management of hepatoma: theJapanese experience. In: H. J. Wanebo (ed.), Hepatic and Biliary Cancer, pp.219-238. New York: Marcel Dekker, 1987.
5. Abelev, G. I. Alpha-fetoprotein in ontogenesis and its association with malignant tumors. Adv. Cancer Res., 14: 295-358, 1971.
6. Chen, D-S., and Sung, J-L. Serum alphafetoprotein in hepatocellular carcinoma. Cancer (Phila.), 40: 779-783, 1977.
7. Livraghi, T., Sangalli, G., Giordano, F., Ravetto, C., Solbiati, L., Fornari, F.,Cavanna, L., Matricardi, L., and Gagliano, E. 240 hepatocellular carcinomas:ultrasound features, tumor size, cytologie and histologie patterns, seruma-fetoprotein and HBsAg. Tumori, 73: 507-512, 1987.
8. Nomura, F., Ohnishi, K., and Tanabe, Y. Clinical features and prognosis ofhepatocellular carcinoma with reference to serum alpha-fetoprotein levels:analysis of 606 patients. Cancer (Phila.), 64: 1700-1707, 1989.
9. Oka, H., Kurioka, N., Kim, K., Ranno, T., Kuroki, T., Mizoguchi, Y.,and Kobayashi, K. Prospective study of early detection of hepatocellularcarcinoma in patients with cirrhosis. Hepatology (Baltimore), 12: 680-687,1990.
10. Liebman, H. A., Furie, B. C., Tong, M. J., Blanchard, R. A., Lo, K-J., Lee,S-D., Coleman, M. S., and Furie, B. Des-i-carboxy (abnormal) prothrombinas a serum marker of primary hepatocellular carcinoma. N. Engl. J. Med.,310: 1427-1431, 1984.
11. Soulier, J-P., Gozin, D., and Lefrere, J-J. A new method to assay des-i-carboxyprothrombin: results obtained in 75 cases of hepatocellular carcinoma. Gastroenterology, 91: 1258-1262, 1986.
12. Sakon, M., Monden, M., Gotoh, M., Kobayashi, K., Kanai, T., Umeshita, K.,Endoh, W., and Mori, T. The effects of vitamin K on the generation ofdes-T-carboxy prothrombin (PIVKA-H) in patients with hepatocellular carcinoma. Am. J. Gastroenterol., 86: 339-345, 1991.
13. Tsai, S-L., Huang, G-T., Yang, P-M., Sheu, J-C, Sung, J-L., and Chen, D-S.Plasma des-^-carboxyprothrombin in the early stage of hepatocellular carcinoma. Hepatology (Baltimore), //: 481-488, 1990.
14. Koprowski, H., Steplewski, Z., Herlyn, D., and Herlyn, M. Study of antibodies against human melanoma produced by somatic cell hybrids. Proc.Nati. Acad. Sci. USA, 75: 3405-3409, 1978.
15. Shouval, D., Eilat, D., Carlson, R. L, Adler, R., Livni, N., and Wands, J. R.Human hepatoma-associated cell surface antigen: identification and characterization by means of monoclonal antibodies. Hepatology (Baltimore), 5:347-356, 1985.
16. Carlson, R. I., Ben-Porath, E., Shouval, D., Strauss, W., Isselbacher, K. J.,and Wands, J. R. Antigenic characterization of human hepatocellular carcinoma: development of in vitro and ;';/vivo immunoassays that use monoclonal
antibodies. J. Clin. Invest., 76:40-51, 1985.17. Hu, C-P., Han, S-H., Lui, W-Y., Hsu, H-C, Lin, Y-M., Lin, P-H., Chen,
L-R., Hsieh, H-G., Kuo, P-T., P'eng, F-K., and Chang. C. Monoclonal an
tibodies against antigens expressed on human hepatocellular carcinoma cells.Hepatology (Baltimore), 6: 1396-1402, 1986.
18. Wiedmann, K. H., Trejdosiewicz, L. K., Southgate, J., and Thomas, H. C.Human hepatocellular carcinoma: cross-reactive and idiotypic antigens associated with malignant transformation of epithelial cells. Hepatology (Baltimore), 7: 543-550, 1987.
19. Hiraiwa, N., lida, N., Ishizuka, I., Itai, S., Shigeta, K., Kannagi, R., Fukuda,Y., and Imura, H. Monoclonal antibodies directed to a disulfated glycosph-ingolipid, SBU (GgOse4Cer-II3IV3-bis-sulfate), associated with human hepatocellular carcinoma. Cancer Res., 48: 6769-6774, 1988.
20. Hiraiwa, N., Fukuda, Y., Imura, H., Tadano-Aritomi, K., Nagai, K., Ishizuka, I., and Kannagi. R. Accumulation of highly acidic sulfated glycosph-ingolipids in human hepatocellular carcinoma defined by a series of monoclonal antibodies. Cancer Res., 50: 2917-2928, 1990.
21. Hiraiwa, N., Tsuyuoka, K., Li, Y-T., Tanaka, M., Seno, T., Okubo, Y.,Fukuda, Y., Imura, H., and Kannagi, R. Gangliosides and sialoglycoproteinscarrying a rare blood group antigen determinant, Cad, associated with humancancers as detected by specific monoclonal antibodies. Cancer Res., 50:5497-5503, 1990.
22. Fuhrer, J. P., Xie, H., Murphy, M. J., Jr., Ye, J. N., and Yao, Z. Characterization of a membrane-associated glycoprotein (gp 43) on human hepatocellular carcinoma by a monoclonal antibody. Cancer Res., 51: 2158-2163,1991.
4993
on July 17, 2018. © 1992 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

MONOCLONAL ANTIBODY TO HEPATOCELLULAR CARCINOMA
23. Alexander, J. J., Bey, E. M., Geddes, E. W., and Lecatsas, G. Establishmentof a continuously growing cell line from primar)' carcinoma of the liver. S.Afr. Med. J., 50: 2124-2128, 1976.
24. Nakabayashi, H., Taketa, K., Miyano, K., Yamane. T., and Sato, J. Growthof human hepatoma cell lines with differentiated functions in chemicallydefÃnedmedium. Cancer Res., 42: 3858-3863. 1982.
25. Aden, D. P., Fogel, A., Plotkin, S., Damjanov, I., and Knowles, B. B. Controlled synthesis of HBsAg in a differentiated human liver carcinoma-derivedcell line. Nature (Lond.), 282: 615-616, 1979.
26. Prozesky, O. W., Brits, C, and Grabow, W. O. K. In vitro culture of cell linesfrom Australia antigen positive and negative hepatoma patients. /;/: S. J.Saunders and J. Terblanche (eds.), Liver, pp. 358-360. London: PitmanMedical Publishing Co., 1973.
27. Shulman, M., Wilde, C. D., and Kohler, G. A better cell line for makinghybridomas secreting specific antibodies. Nature (Lond.), 276: 269-270,1978.
28. Köhler,G., and Milstein, C. Continuous cultures of fused cells secretingantibody of predefined specificity. Nature (Lond.), 256: 495-497, 1975.
29. Oi, V. T., and Herzenberg, L. A. Immunoglobulin-producing hybrid celllines. In: B. B. Mishell and S. M. Shiigi (eds.). Selected Methods in Cellular
Immunology, pp. 351-372. San Francisco, CA: Freeman, 1980.30. Chiba, J., Chused, T. M., Leiserson, W. M., Zweig, S. E., and Shevach, E. M.
Production and characterization of monoclonal antibodies to guinea pig lym-phoid differentiation antigens. J. Inumino]. Methods, 63: 247-261, 1983.
31. Hunter, W. M., and Greenwood, F. C. Preparation of iodine-131 labeledhuman growth hormone of high specific activity. Nature (Lond.), 194: 495-496, 1962.
32. Leevy, C. M., Popper, H., and Sherlock, S. Diseases of the Liver and BiliaryTract: Standardization of Nomenclature, Diagnostic Criteria, and DiagnosticMethodology, Chicago, IL: Year Book Medical Publishers, Inc., 1976.
33. Terasaki, P. I., Bernoco, D., Park, M. S., Ozturk, G., and Iwaki, Y. Micro-droplet testing for HLA-A, -B, -C, and -D antigens. Am. J. Clin. Pathol., 69:103-120, 1978.
34. Armitage, P. Statistical Methods in Medical Research [4th printing]. Oxford,United Kingdom: Blackwell Scientific Publications, 1977.
35. Wu, A. M., Sugii, S., and Herp, A. A guide for carbohydrate specificities oflectins. Adv. Exp. Med. Biol., 22«:819-847, 1988.
36. Baenziger, J. U., and FÃete,D. Structural determinants of Ricinus communisagglutinin and toxin specificity for oligosaccharides. J. Biol. ( 'hem., 254:
9795-9799, 1979.
4994
on July 17, 2018. © 1992 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
1992;52:4987-4994. Cancer Res Yasuyuki Kumagai, Joe Chiba, Tetsutaro Sata, et al. KM-2Hepatocellular Carcinoma, Defined by Monoclonal Antibody A New Tumor-associated Antigen Useful for Serodiagnosis of
Updated version
http://cancerres.aacrjournals.org/content/52/18/4987
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerres.aacrjournals.org/content/52/18/4987To request permission to re-use all or part of this article, use this link
on July 17, 2018. © 1992 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from




























