Embed Size (px)
Citation preview

Scott Mikesell, DO, FACC, FSCAIDirector, Cardiac Catheterization Laboratory St. Luke’s Cardiology AssociatesDuluth, Minnesota
A Piece of the Northland in the ICU

None

65-year-old male
At home working in his garden
Loses consciousness
Wife▪ Calls 911
▪ Initiates CPR
EMS arrives
Ventricular fibrillation
Perfusing rhythm within 10 minutes
Repeated episodes of VF resulting in multiple shocks and CPR

Unresponsive after restoration of spontaneous circulation (ROSC)
Initial ECG: inferior STEMI Further VT/VF in ED Taken to cath lab for PCI ER personnel
IV iced saline
Ice packs


Cath Lab – RCA culprit ICU
Surface cooling pads applied
Therapeutic hypothermia x 24 hours
Rewarmed
Day 7 – awake, alert, interactive Discharged home

EpidemiologyBiologyEvidenceManagement, expectations, side effects Patient selection


Out-of-hospital cardiac arrest (OHCA)
300,000 – 450,000 people annually in the US
40,000 survive to hospitalization
Systemic, neurologic & cardiac sequelae
One third survive to hospital discharge
Lloyd-Jones D, Adams R, Carnethon M et al. Heart disease and stroke statistics-2009 update. Circulation 2009;119:e21-e181
Holzer, M. Targeted Temperature Management for Comatose Survivors of Cardiac Arrest. NEJM 2010; 363:1256-64.

• 80% remain comatose for >1 hour post-resusciatation
• < 50% recover good neurologic activity as defined by the Cerebral Performance Category scale (CPC), range 1-5, higher scores = worse
Holzer, M. Targeted Temperature Management for Comatose Survivors of Cardiac Arrest. NEJM 2010; 363:1256-64.

– 1 = Good recovery
– 2 = Moderate disability (independent ADLs)
– 3 = Severe disability (dependent daily support)
– 4 = Coma or vegetative state
– 5 = Brain death
Holzer, M. Targeted Temperature Management for Comatose Survivors of Cardiac Arrest. NEJM 2010; 363:1256-64.

• 1950s - cardiac and neurologic surgeries
• Late 1950s - after cardiac arrest
– uncertain benefits
– difficulties with implementation
• 1990s - studies in animal models
– histological benefits
– functional benefits
• 2002 - randomized clinical trials of TH


A condition in which an organism's temperature drops below that required for normal metabolism and body function.
- Stratified into four categories: ▪ Mild (32 - 35ºC or 90 - 95ºF)
▪ Moderate (28 - 32ºC or 82.4 - 90ºF )
▪ Severe (20 - 28ºC or 68 - 82.4ºF)
▪ Profound ( < 20ºC or < 68ºF)

• Brain stores of oxygen lost in seconds• Glucose, ATP lost within 5 minutes• Loss of transmembrane electrochemical
gradient• Loss of synaptic, axonal function• Glutamate is released leading to excitotoxic cell
death• Intracellular calcium accumulates leading to cell
death (necrosis and apoptosis)• Vulnerable areas = hippocampus, neocortex,
cerebellum, corpus striatum, thalamusHolzer, M. Targeted Temperature Management for Comatose Survivors of Cardiac Arrest. NEJM 2010; 363:1256-64.

Restoration of circulation, reperfusion and reoxygenation – further neuronal damage due to -
– Microcirculation failure – transient hyperemia
– Followed by prolonged global/microfocalhypoperfusion
– Reactive oxygen species (lipid peroxidation, oxidative damage)
– Inflammatory response leading to endothelial activation, leukocyte infiltration → tissue injury
– Brain edema limiting perfusionHolzer, M. Targeted Temperature Management for Comatose Survivors of Cardiac Arrest. NEJM 2010; 363:1256-64.

ischemia
glutamate release
oxygen-free radicals
calcium shifts
mitochondrial dysfunction
reperfusion
excitotoxicity
inflammatory
cascades
cell death
blood brain barrier disruption & cerebral edema
hypothermia
lower metabolic rate
less oxygen consumption
Geocadin RG, Koenig MA, Jia X et al. Management of brain injury after resuscitation from cardiac arrest. Neurol Clin. 2008;22:487-506.

Limit neurologic injury– Reduction in brain metabolism (less oxygen and
ATP utilization)
– Inhibition of release of glutamate and dopamine
– Induction of brain-derived neurotrophic factor (less glutamate)
– Inhibition of calcium overload & pro-apoptotic factors
– Induction of anti-apoptotic factors
– Limited inflammation/edemaHolzer, M. Targeted Temperature Management for Comatose Survivors of Cardiac Arrest. NEJM 2010; 363:1256-64.

Scirica B M Circulation. 2013;127:244-250
Copyright © American Heart Association, Inc. All rights reserved.
Management of TH


Multicenter, randomized, controlled trial with blinded assessment of outcome.
Inclusion -▪ Positive ROSC
▪ Witnessed VT/VF arrest
▪ Age 18 – 75 years old
▪ Estimated time to resuscitation of 5 – 15 minutes by EMP
▪ Interval no greater than 60 minutes from collapse to restoration of spontaneous circulation
Holzer, M. Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. NEJM 2002; 346:549-56.

Multicenter, randomized, controlled trial with blinded assessment of outcome.
Exclusion -– Temperature < 30o C on admission
– Comatose state prior to arrest d/t drug administration
– Pregnancy
– Hypotension (MAP < 60 mmHg) for > 30 min. post-ROSC
– Hypoxemia (SpO2 < 85% for > 15 min. post-ROSC)
– Terminal illness
– “Factors that made participation in follow-up unlikely”
– Enrollment in another study
– Cardiac arrest post-EMP arrival
– Known coagulopathy
Holzer, M. Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. NEJM 2002; 346:549-56.

Primary outcome– Favorable neurologic outcome within 6 months
CPC Scale– 1, 2, 3, 4, 5
–Blinded assessment
Holzer, M. Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. NEJM 2002; 346:549-56.
Secondary end points– Mortality at 6 months– Rate of complications during the 1st 7 days post-ROSC– Bleeding of any severity, pneumonia, sepsis, pancreatitis,
renal failure, pulmonary edema, seizures arrhythmias and pressure sores were all recorded

Therapies –– ACS management– Standard ICU management– Sedation + paralysis (shivering), mechanical
ventilation– Temperature monitoring via bladder– Cooling via TheraKool device (cooling blanket) to 32 –
34o C within 4 hours post-ROSC– Ice packs if not at goal– 24 hours at target temperature– Passive rewarming
Holzer, M. Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. NEJM 2002; 346:549-56.

Holzer, M. Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. NEJM 2002; 346:549-56.

Holzer, M. Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. NEJM 2002; 346:549-56.

Holzer, M. Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. NEJM 2002; 346:549-56.

Inclusion –
– Initial rhythm of VT/VF
– Successful ROSC
Exclusion –
– Age < 18 for men, < 50 for women
– Cardiogenic shock (SBP < 90 mmHg despite Epi)
– Coma due to other causes
– No ICU bed
Bernard, S. et al. Treatement of comatose survivors of out-of-hospital cardiac arrest with induced hypothermia. NEJM 2002; 346:557-63.

Therapies –– Hypothermia versus normothermia– EMPs initiated hypothermia in the field with cold packs– Sedation, paralysis, mechanical ventilation– Standard ICU management– ACS therapy– Lidocaine bolus followed by infusion– PRN KCl for levels < 4.0– Insulin– Aspirin– PA catheter– Cooling via ice packs– Active rewarming
Bernard, S. et al. Treatement of comatose survivors of out-of-hospital cardiac arrest with induced hypothermia. NEJM 2002; 346:557-63.

Bernard, S. et al. Treatement of comatose survivors of out-of-hospital cardiac arrest with induced hypothermia. NEJM 2002; 346:557-63.

Bernard, S. et al. Treatement of comatose survivors of out-of-hospital cardiac arrest with induced hypothermia. NEJM 2002; 346:557-63.

Bernard, S. et al. Treatement of comatose survivors of out-of-hospital cardiac arrest with induced hypothermia. NEJM 2002; 346:557-63.
Good outcome of hypo- to normothermia = 49% to 26%; p = .046
Unadjusted odds ratio = 2.65 (1.02 – 6.88; p = .046)
Adjusted odds ratio (age, time to ROSC) = 5.25 (1.47 – 18.76; p = .011)
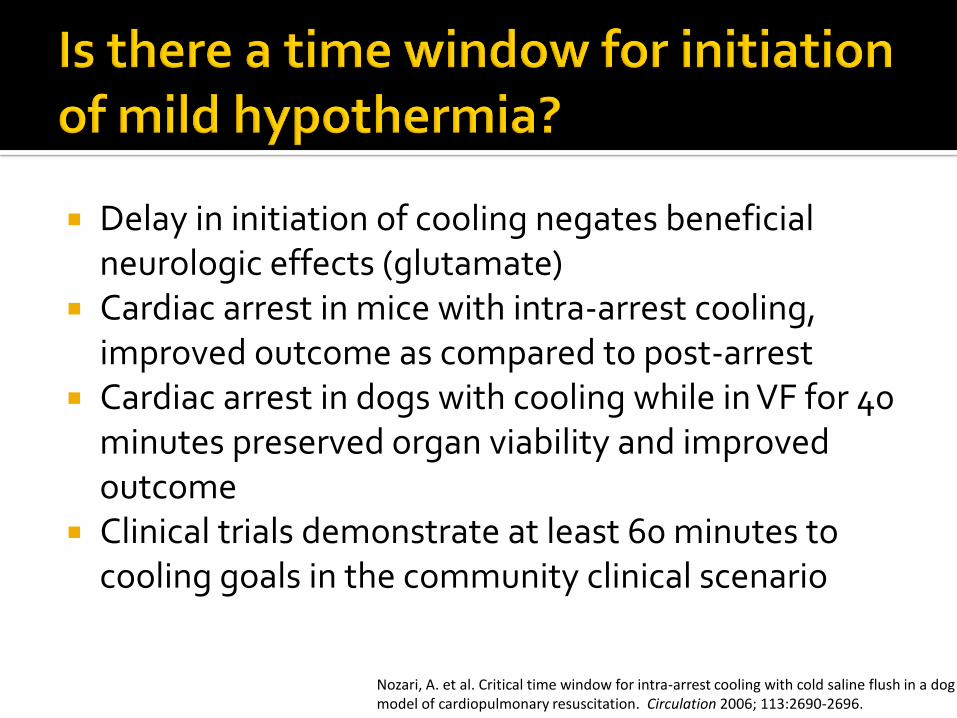
Delay in initiation of cooling negates beneficial neurologic effects (glutamate)
Cardiac arrest in mice with intra-arrest cooling, improved outcome as compared to post-arrest
Cardiac arrest in dogs with cooling while in VF for 40 minutes preserved organ viability and improved outcome
Clinical trials demonstrate at least 60 minutes to cooling goals in the community clinical scenario
Nozari, A. et al. Critical time window for intra-arrest cooling with cold saline flush in a dog model of cardiopulmonary resuscitation. Circulation 2006; 113:2690-2696.

Nozari, A. et al. Critical time window for intra-arrest cooling with cold saline flush in a dog model of cardiopulmonary resuscitation. Circulation 2006; 113:2690-2696.

Nozari, A. et al. Critical time window for intra-arrest cooling with cold saline flush in a dog model of cardiopulmonary resuscitation. Circulation 2006; 113:2690-2696.

Nozari, A. et al. Critical time window for intra-arrest cooling with cold saline flush in a dog model of cardiopulmonary resuscitation. Circulation 2006; 113:2690-2696.

Patients with cardiac arrest are at increased risk for refibrillation
Concern for refibrillation while cooled as well as increased risk for arrhythmias while hypothermic
Previous investigation demonstrated improved defibrillation with severe hypothermia (30oC) with less post-defibrillation ventricular asystole
Boddiker, K. et al. Hypothermia improves defibrillation success and resuscitation outcomes from ventricular fibrillation. Circulation 2005; 111:3195-3201.

Boddiker, K. et al. Hypothermia improves defibrillation success and resuscitation outcomes from ventricular fibrillation. Circulation 2005; 111:3195-3201.

Boddiker, K. et al. Hypothermia improves defibrillation success and resuscitation outcomes from ventricular fibrillation. Circulation 2005; 111:3195-3201.

Boddiker, K. et al. Hypothermia improves defibrillation success and resuscitation outcomes from ventricular fibrillation. Circulation 2005; 111:3195-3201.

Cooling improves neurologic outcome post-ROSC
Post-reperfusion injury rapidly evolves post-ROSC
Earlier cooling improves outcomes in animal models
Earlier and moderate hypothermia improves successful defibrillation and prevents post-ROSC arrhythmias in animal models

Retrospective analysis of patients with out-of-hospital cardiac arrest (OHCA)
Included if experienced non-traumatic OHCA and ≥ 18 years old
Excluded if pregnant, arrest secondary to drowning, DNR order or obvious signs of death
Garrett JS. et al. The association between intra-arrest therapeutic hypothermia and return of spontaneous circulation among individuals experiencing out of hospital cardiac arrest. Resuscitation 2010; 82:21-5.

Garrett JS. et al. The association between intra-arrest therapeutic hypothermia and return of spontaneous circulation among individuals experiencing out of hospital cardiac arrest. Resuscitation 2010; 82:21-5.

Garrett JS. et al. The association between intra-arrest therapeutic hypothermia and return of spontaneous circulation among individuals experiencing out of hospital cardiac arrest. Resuscitation 2010; 82:21-5.

Garrett JS. et al. The association between intra-arrest therapeutic hypothermia and return of spontaneous circulation among individuals experiencing out of hospital cardiac arrest. Resuscitation 2010; 82:21-5.
Volume of chilled saline versus likelihood of ROSC
Frequency of ROSC per initial rhythm

PEA/asystole may not behave similar to VT/VF
No harm, no foul No evidence for benefit in
PEA/asystole

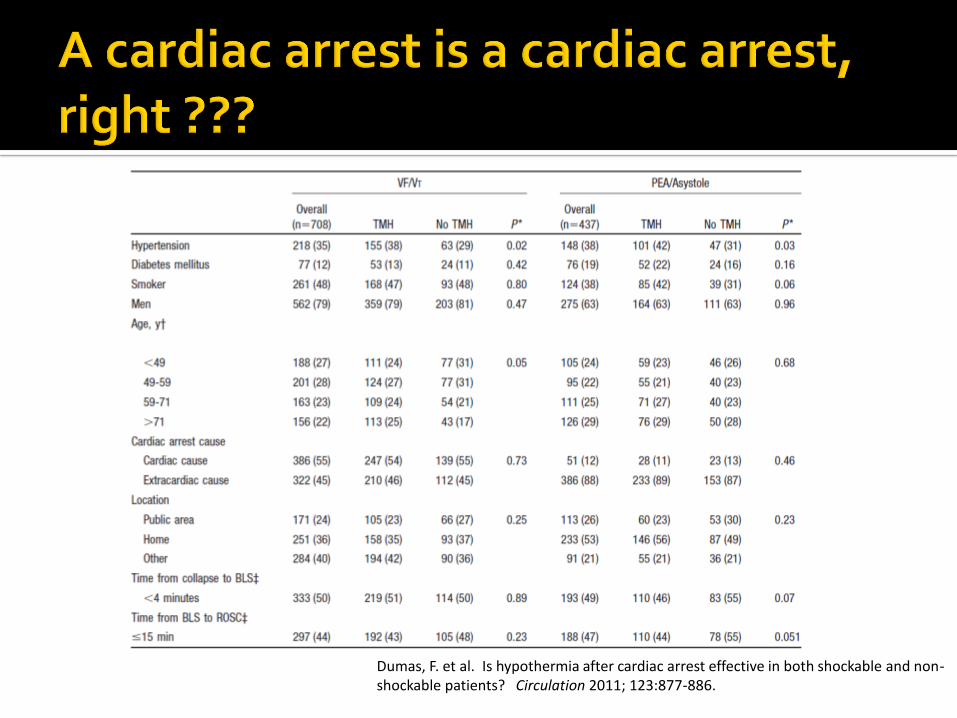
OHCA in Paris, France is managed by at least 1 physician, firefighters, paramedics
Post-ROSC, ICU or cardiac catheterization laboratory
Dumas, F. et al. Is hypothermia after cardiac arrest effective in both shockable and non-shockable patients? Circulation 2011; 123:877-886.

Dumas, F. et al. Is hypothermia after cardiac arrest effective in both shockable and non-shockable patients? Circulation 2011; 123:877-886.
Dumas, F. et al. Is hypothermia after cardiac arrest effective in both shockable and non-shockable patients? Circulation 2011; 123:877-886.

Dumas, F. et al. Is hypothermia after cardiac arrest effective in both shockable and non-shockable patients? Circulation 2011; 123:877-886.
PEA/Asystole
VT/VF



Multicenter RCT (36 hospitals, 10 countries, Europe and Asia)
N=939 T = 33 Co = 473
T = 36 Co = 466 Standardized rules for prognostication Standardized rules for withdrawal of life support Blinded prognostication and outcome assessment

Inclusion criteria Age ≥ 18y OHCA of presumed cardiac cause Sustained ROSC for 20 minutes GCS < 8 after sustained ROSC
Exclusion criteria Pregnancy Known bleeding diathesis (other
than medical coagulopathy, eg, warfarin)
Suspected/confirmed ICH or stroke
Unwitnessed cardicac arrest with initial rhythm asystole
DNR or known prognosis < 6 months
Pre-arrest CPC 3 or 4 > 4 hrs from ROSC to screening SBP < 80 despite pressor,
inotrope, IABP Temp < 30 C
oon admit

Intervention Group Target Temp at 33 C
o
Intervention period of 36 hrscommenced at randomization
Mandatory sedation Cooled to target in < 6 hrs
after randomization Maintained at 33 C
ountil 28
hours after screening, then rewarmed at 0.5C/hr
Mandatory sedation stopped/tapered at 36 hrs
Maintain temp below 37.5 Co
until 72 hrs after CA
Comparison Group Target Temp at 36 C
o
Similar treatment to intervention group

Body Temperature during the Intervention Period.

Outcomes
Primary: mortality at 180 days
Secondary
▪ Composite of poor neurologic function or death▪ CPC 3-5
▪ Modified Rankin scale 4-6
▪ At or around 180 days

Probability of Survival through the End of the Trial.

Results
No difference in mortality▪ T=33 C
o235/473 died (50%)
▪ T=36 Co
225/466 died (48%)
▪ HR=1.06 (95% CI 0.89-1.28), P = 0.51
No difference in composite mortality/poor neurologic outcomes▪ CPC: T=33 C
o54%, T36C 52%, RR=1.02 (0.88-1.16), P = 0.78
▪ mRS: T=33 Co
52%, T36C 52%, RR=1.01 (0.89-1.14), P = 0.87
Serious adverse events were common, and slightly higher in T=33 Co
(93%) vs T=36 Co
(90%), RR=1.03 (1.00-1.08), P = 0.09

Conclusions No difference found between Target Temp at T=36
Co
compared to T=33 Co
Good outcomes in both groups may reflect active prevention of hyperthermia
Modern aggressive care that includes attention to temperature works▪ Makes survival more likely than death when a patient
hospitalized after CPR

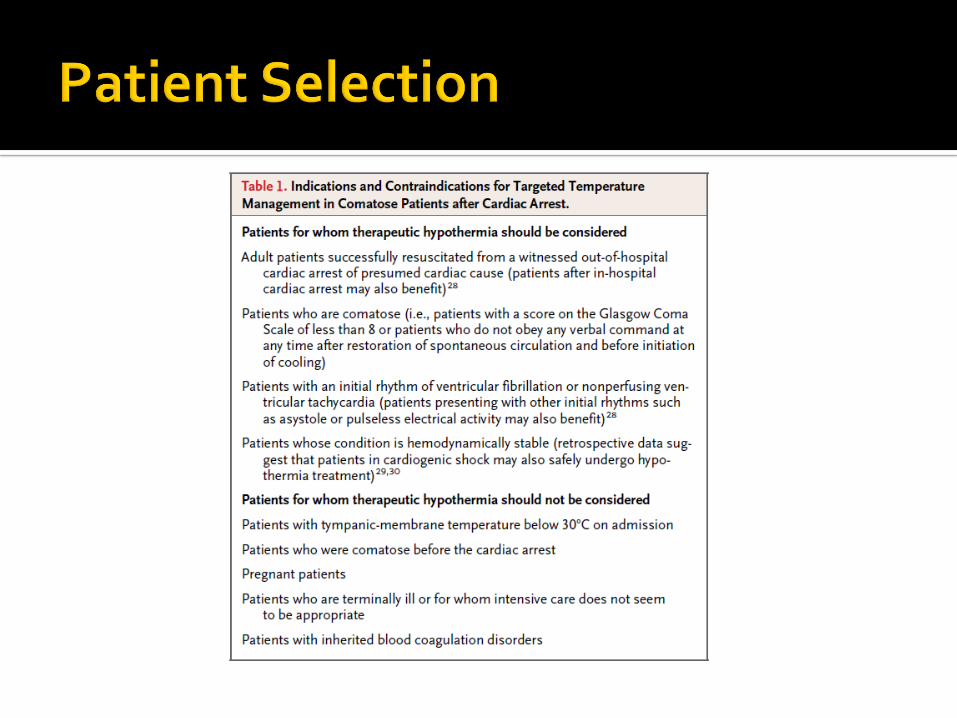
Remaining Issues
Patient selection
Optimum target temperature
Timing of cooling initiation
Duration of therapy
Rate of rewarming
In versus out-of-hospital
VT/VF versus non-VT/VF


American Heart Association post–cardiac arrest care algorithm.
Scirica B M Circulation. 2013;127:244-250
Copyright © American Heart Association, Inc. All rights reserved.


Cincinnati Sub-Zero Blankerol III Artic Sun

Bradycardia Oozing Hypotension Diuresis Arrhythmias Hypokalemia Hyperglycemia Prolonged drug metabolism




Mild hypothermia improve neurologic outcomes in witnessed VT/VF arrest
Intra-arrest hypothermia may be beneficial for improved ROSC
Neurologic outcomes after intra-arrest may be improved, randomized evidence is lacking