8/12/2019 Achalasie, achalasia
2/4
weight loss and dysphagia to liquids. About 60 to 90% of
patients regurgitate undigested food into the
esophagus shortly after a meal. Regurgitation may cause
nocturnal coughing and aspiration. About 30 to 50%
of patients have chest pain associated with eating. Elderly
patients may have had symptoms for months or
years before diagnosis. Complications include weight loss with
advanced disease and coughing,
bronchospasm, and pneumonia from aspirating esophageal
contents.
Achalasia is often suspected from the history. In the early
stages of the disease, chest x-ray findings can be
normal. In the later stages, chest x-rays can show a dilated
esophagus (mega-esophagus) with an air-fluid
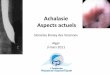
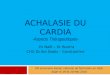
level caused by retained food and saliva. Elderly patients with
a long history of achalasia can have a dilated
and tortuous esophagus with a "bird-beak" narrowing at the
gastroesophageal junction on barium swallow.
Esophageal manometry usually shows the motility
abnormalities.
Endoscopy can eliminate the possibility of pseudo-achalasia,
which should be considered when patients are >
50 years, have had dysphagia for < 1 year, and have lost >
15 lb (> 7 kg). Other disorders that can mimic
achalasia include malignancy, amyloidosis, sarcoidosis, Chagas
disease, and postvagotomy disturbances.
Achalasia must also be differentiated from diffuse esophageal
spasm, which more typically affects younger
patients.
Treatment
Treatment is directed at relieving symptoms and preventing
complications. Various drugs that can decrease
lower esophageal sphincter pressure (eg, anticholinergics, amyl
nitrite, nitroglycerin, beta2-agonists) have
been used, but results have been inconsistent. Anticholinergics
are particularly difficult to use in the elderly
because of their adverse effects. Isosorbide nitrate (5 to 10 mg
po before meals) or nitroglycerin (0.4 mg
sublingually 5 minutes before meals) rapidly decreases lower
esophageal sphincter pressure and may lessen
dysphagia during meals. However, most patients with achalasia
require more definitive treatment.
Botulinum toxin, an inhibitor of the release of acetylcholine,
can be injected endoscopically into the lower
esophageal sphincter. This relatively new treatment appears to
approach the success rate of pneumatic
dilatation. The most benefit seems to occur in patients > 50.
The effects last 6 to 24 months; injection often
needs to be repeated.
Mechanical disruption of the lower esophageal sphincter using
pneumatic dilatation or surgical myotomy has
been the principle method of treatment when drug treatment and
botulinum toxin have not been effective.
About 60% of patients have a good response with pneumatic
dilatation; success rates > 95% have been
reported. Elderly patients and patients with a long history of
achalasia seem to have the most favorable
responses. Twenty to 40% of patients require repeated
dilatations. The incidence of immediate complicationsis 1 to 16%.
Perforation occurs in 1 to 13%; in most of these cases, the
perforation is small and localized.
Surgical myotomy is indicated when repeated pneumatic
dilatations over a relatively short duration are
necessary to maintain lower esophageal sphincter patency.
Surgical myotomy reduces lower esophageal
sphincter pressure more dependably than pneumatic dilatation but
causes more complications. A modified
Hellers procedure (anterior myotomy of the circular muscle
fibers of the lower esophageal sphincter,
preserving the sphincter competency) is successful in 80 to 90%
of patients. This procedure is increasingly
being performed laparoscopically or with video-assisted
thorascopic surgery. The most significant
complications are gastroesophageal reflux disease (< 10%) and
persistence of severe dysphagia (< 10%).
lasie http://www.med-info.nl/Afwijking_MDL - Slokdarm - acha
7/14/2014
8/12/2019 Achalasie, achalasia
3/4
Bron
T. Yamada, D.H. Alpers,L. Laine, C. Owyang & D.W. Powell.
Textbook of Gastroenterology 4th Ed.
2003. Lippincott Williams & Wilkins.
1.
A. Fauci, E. Braunwald, D. Kasper, S. Hauser, D. Longo, J.L.
Jameson & J. Loscalzo. Harrisons
Principle of Internal Medicine 17th Ed. 2008. McGraw-Hill.
2.
A. Avunduk. Manual of Gastroenterology: Diagnosis and Therapy
4th Ed. 2008. Lippincott Williams &
Wilkins.
3.
E. Kuntz & H.D. Kuntz. Hepatology, Principles and Practice
2nd Ed. 2006. Springer Science &
Business Media.
4.
Laatste update: 5-09-2011
lasie http://www.med-info.nl/Afwijking_MDL - Slokdarm - acha
7/14/2014