Embed Size (px)
Citation preview
ACTA ODONTOLOGICALATINOAMERICANAVol. 30 Nº 2 2017
ISSN 1852-4834 on line versionversión electrónica
AOL22017:32011 29/11/2017 14:29 Página 1

AOL22017:32011 29/11/2017 14:29 Página 2

Honorary EditorEditor honorarioRómulo Luis Cabrini(Universidad de Buenos Aires, Argentina)
Scientific EditorEditor CientíficoMaría E. Itoiz(Universidad de Buenos Aires, Argentina)
Associate EditorsEditores AsociadosRicardo MacchiAngela M. Ubios(Universidad de Buenos Aires, Argentina)Amanda E. Schwint(Comisión Nacional de Energía Atómica, Argentina)
Assistant EditorsEditores AsistentesPatricia MandalunisSandra J. Renou(Universidad de Buenos Aires, Argentina)
Technical and Scientific AdvisorsAsesores TécnicoCientíficosLilian Jara TracchiaLuciana M. SánchezTammy SteimetzDelia Takara(Universidad de Buenos Aires, Argentina)
Editorial BoardMesa EditorialEnri S. Borda (Universidad de Buenos Aires, Argentina)
Noemí E. Bordoni (Universidad de Buenos Aires, Argentina)
Fermín A. Carranza (University of California, Los Angeles, USA)
José Carlos Elgoyhen (Universidad del Salvador, Argentina)
Andrea Kaplan (Universidad de Buenos Aires, Argentina)
Andrés J.P. KleinSzanto (Fox Chase Cancer Center, Philadelphia, USA)
Susana Piovano (Universidad de Buenos Aires, Argentina)
Guillermo Raiden (Universidad Nacional de Tucumán, Argentina)
Sigmar de Mello Rode (Universidade Estadual Paulista,Brazil)
Hugo Romanelli (Universidad Maimónides, Argentina)
Cassiano K. Rösing (Federal University of Rio Grande do Sul, Brazil)
PublisherProducción Gráfica y PublicitariaImageGraf / email: [email protected]
Acta Odontológica Latinoamericana is the officialpublication of the Argentine Division of the InternationalAssociation for Dental Research.
Revista de edición argentina inscripta en el RegistroNacional de la Propiedad Intelectual bajo el N° 284335.Todos los derechos reservados.Copyright by:ACTA ODONTOLOGICA LATINOAMERICANAwww.actaodontologicalat.com
ACTA ODONTOLÓGICA LATINOAMERICANAAn International Journal of Applied and Basic Dental Research
POLÍTICA EDITORIAL
El objetivo de Acta OdontológicaLatinoamericana (AOL) es ofrecer a lacomunidad científica un medio adecuadopara la difusión internacional de los trabajos de investigación, realizados preferentemente en Latinoamérica, dentro delcampo odontológico y áreas estrechamente relacionadas. Publicará trabajos originales de investigación básica, clínica yepidemiológica, tanto del campo biológico como del área de materiales dentales ytécnicas especiales. La publicación de trabajos clínicos será considerada siempreque tengan contenido original y no seanmeras presentaciones de casos o series. Enprincipio, no se aceptarán trabajos de revisión bibliográfica, si bien los editorespodrán solicitar revisiones de temas departicular interés. Las ComunicacionesBreves, dentro del área de interés de AOL,serán consideradas para su publicación.Solamente se aceptarán trabajos no publicados anteriormente, los cuales no podránser luego publicados en otro medio sinexpreso consen timiento de los editores.
Dos revisores, seleccionados por lamesa editorial dentro de especialistas encada tema, harán el estudio crítico de losmanuscritos presentados, a fin de lograr elmejor nivel posible del contenido científico de la revista.
Para facilitar la difusión internacional,se publicarán los trabajos escritos eninglés, con un resumen en castellano o portugués. La revista publicará, dentro de laslimitaciones presupuestarias, toda información considerada de interés que se lehaga llegar relativa a actividades conexasa la investigación odontológica del árealatinoamericana.
EDITORIAL POLICY
Although Acta Odontológica Lati noamericana (AOL) will accept originalpapers from around the world, the principal aim of this journal is to be an instrumentof communication for and among LatinAmerican investigators in the field of dental research and closely related areas.
AOL will be devoted to original articlesdealing with basic, clinic and epidemiological research in biological areas or thoseconnected with dental materials and/orspecial techniques.
Clinical papers will be published aslong as their content is original and notrestricted to the presentation of singlecases or series.
Bibliographic reviews on subjects ofspecial interest will only be published byspecial request of the journal.
Short communications which fall within the scope of the journal may also besubmitted. Submission of a paper to thejournal will be taken to imply that it presents original unpublished work, not underconsideration for publication elsewhere.
By submitting a manuscript the authorsagree that the copyright for their article istransferred to the publisher if and whenthe article is accepted for publication. Toachieve the highest possible standard inscientific content, all articles will be refereed by two specialists appointed by theEditorial Board. To favour internationaldiffusion of the journal, articles will bepublished in English with an abstract inSpanish or Portuguese.
The journal will publish, within budgetlimitations, any data of interest in fieldsconnected with basic or clinical odontological research in the Latin America area.
Este número se terminó de editar el mes de Octubre de 2017
Vol. 30 Nº 2 / 2017 ISSN 1852-4834 Acta Odontol. Latinoam. 2017
AOL22017:32011 29/11/2017 14:29 Página 47

CONTENTS / ÍNDICE
Morphological characteristics of the facial bone wall related to the tooth position in the alveolar crest in the maxillary anteriorCaracterísticas morfológicas de la tabla ósea vestibular en relación a la posición dentaria en la cresta alveolar en la zona anterior del maxilar superiorHernán Bonta, Nelson Carranza, Ariel F. Gualtieri, Mariana A. Rojas ........................................................................................................................................................................................................................ 49
Postural alterations as a risk factor for temporomandibular disordersAlteraciones posturales como factor de riesgo para trastornos témporomandibularesSilvina Cortese, Ana Mondello, Ricardo Galarza, Ana Biondi...................................................................................................................................................................................................................................... 57
The impact of oral health on quality of life in individuals with head and neck cancer after radiotherapy: the importance of dentistry in psychosocial issuesO impacto da condição bucal sobre a qualidade de vida de indivíduos com câncer de cabeça e pescoço após radioterapia: a importância da odontologia nos aspectos psicossociaisPaulo S.S. Santos, Adrielle L. Cremonesi, Reyna A. Quispe, Cássia M. F. Rubira ...................................................................................................................................................................................................... 62
Evaluation of an experimental remineralizing agent for repairing enamel surfacesEvaluación de un agente remineralizante experimental reparador de superficie de esmalteMargarita V. Úsuga Vacca, Carolina TorresRodríguez, Edgar DelgadoMejía ............................................................................................................................................................................................................ 68
Dental skeletal effects of the metallic splinted Herbst appliance after growth spurt: a lateral oblique cephalometric assessmentEfeitos dentoesqueléticos do aparelho splint metálico de Herbst apóssurto de crescimento: estudo com telerradiografias em 45oTaisa B. Raveli, Dirceu B. Raveli, Luiz G. Gandini, Ary SantosPinto ........................................................................................................................................................................................................................ 76
Edentulism and its relationship with selfrated health: secondary analysis of the SABE Ecuador 2009 StudyRelación del edentulismo con la autoevaluación del estado de la salud: un análisis secundario del estudio SABE Ecuador 2009Miguel Germán Borda, Nicolás CastellanosPerilla, JudyAndrea Patiño, Sandra Castelblanco, Carlos Alberto Cano, Diego ChavarroCarvajal, Mario U PérezZepeda ........................................................................................................................................................................................................................................................ 83
Surface wear of resin composites used for Invisalign® attachmentsDesgaste superficial de las resinas compuestas utilizadas en los “attachments” de la técnica Invisalign®
Graciela J. Barreda, Elizabeth A. Dzierewianko, Karina A. Muñoz, Gisela I. Piccoli .................................................................................................................................................................................................. 90
Acta Odontol. Latinoam. 2017 ISSN 1852-4834 Vol. 30 Nº 2/ 2017
ACTA ODONTOLÓGICA LATINOAMERICANAAn International Journal of Applied and Basic Dental Research
Contact us Contactos: Cátedra de Anatomía Patológica, Facultad de Odontología, Universidad de Buenos AiresM.T. de Alvear 2142 (1122) Buenos Aires, Argentina Fax: (5411) 4 508[email protected] http://www.actaodontologicalat.com/contacto.html
ACTA ODONTOLÓGICA LATINOAMERICANA
A partir del Volumen 27 (2014) AOL se edita en formato digital con el Sistema de Gestión de Revistas Electrónicas (Open Journal System, OJS). La revista es de accesoabierto (Open Access). Esta nueva modalidad no implica un aumento en los costos de publicación para los autores.
Comité Editorial
ACTA ODONTOLÓGICA LATINOAMERICANA
From volume 27 (2014) AOL is published in digital format with the Open Journal System (OJS). The journal is Open Access. This new modality does not implyan increase in the publication fees.
Editorial Board
AOL22017:32011 29/11/2017 14:29 Página 48

Características morfológicas de la tabla ósea vestibular en relación a la posición dentaria en la cresta alveolar en la zona anterior del maxilar superior
Morphological characteristics of the facial bone wall related to the tooth position in the alveolar crest in the maxillary anterior
Hernán Bonta1, Nelson Carranza1, Ariel F. Gualtieri2, Mariana A. Rojas1
1 Universidad de Buenos Aires, Facultad de Odontología, Cátedra de Periodoncia, Argentina.2 Universidad de Buenos Aires, Facultad de Odontología, Cátedra de Biofísica, Argentina.
Vol. 30 Nº 2 / 2017 / 49-56 ISSN 1852-4834 Acta Odontol. Latinoam. 2017
49
ABSTRACTThe purpose of this study was to analyze whether the positionof the tooth in the alveolar ridge influences the thickness of thefacial bone wall and the distance between the cementoenameljunction (CEJ) and osseous zenith (OZ). Conebeam computed tomography (CBCT) scans from fifty fourdentate patients were included in the study (22 male and 32 female,mean age 41.5 years). The measurements taken included: (1).TheFacial bone thickness at 7 different equidistant levels measuringlevels (ML 17) between OZ and the root apex (A). (2) The CEJ OZ distance. (3) Facial position of the tooth (FPT) relative to astraight line traced from mesial to distal interproximal depressionsof the alveolar plate at the level of the CEJ. The Facial bone wall thickness ranged between 0 mm and 3.8mm, with greater values at more apical levels. Mean values
were smaller than 1 mm at every level except ML7. The CEJOZ distance varied between 0.5 mm and 6.9 mm (mean 2.9mm). The Mean of FPT value was 0.6 mm.No statistically significant correlation was found between FPTand the CEJOZ distance. Weak negative statistically significantcorrelations were found between FPT and the thickness of thefacial bone wall at MP1 and MP3. Within the limits of this study, no clinically relevant correlationbetween FPT and facial bone thickness – CEJOZ distance wasfound.More studies should be conducted to evaluate a greater numberof teeth, especially those that may present misalignment withgreater FPT values.
Key words: Alveolar bone, Computed tomography, maxilla.
RESUMENEl objetivo del presente estudio fue analizar si la posición dela pieza dentaria en el reborde alveolar influencia el espesorde la tabla ósea vestibular y la distancia entre el limite amelocementario (LAC) y el cenit óseo (CO).Tomografías computadas haz de cono (TC) de 54 pacientesdentados fueron incluidas en el estudio (22 hombres y 32mujeres, edad promedio 41.5 años). Las medidas registradasfueron: (1) espesor de la tabla ósea vestibular en 7 diferentesniveles de medición (NM 17) entre CO y el ápice radicular(AR). (2) La distancia LACCO. (3) Posición vestibular de lapieza dentaria (PVD) en relación a una línea recta trazadadesde la depresión interproximal mesial a la depresióninterproximal distal de la tabla ósea a nivel del LAC.El espesor de la tabla ósea vestibular fue 03.8mm, con valoresmayores registrados a nivel más apical. El valor promedio fue
menor a 1 mm excepto en NM7. La distancia LACCO varióentre 0.5 y 6.9mm (promedio 2.9mm). El promedio de PVD fuede 0.6mm.No se encontró correlación estadísticamente significativa entrela PVD y la distancia LACCO. Se halló una correlación débilnegativa estadísticamente significativa entre la PVD y elespesor de la tabla ósea vestibular en NM1 y NM3.Dentro de las limitaciones de este estudio, no se encontró unacorrelación clínicamente significativa entre PVD y espesor dela tabla ósea vestibular – distancia LACCO.Se deben llevar a cabo más estudios para evaluar un mayornúmero de piezas dentarias, especialmente aquellas que seencuentran desalineadas con valores PVD mayores.
Palabras clave: Hueso alveolar, tomografía computada,maxilar.
INTRODUCTIONImplant placement in the anterior maxilla presentsa considerable challenge to clinicians because ofpatients’ high esthetic expectations. The thicknessof the facial bone wall in this region is of crucial
importance for selecting the appropriate treatmentapproach.A number of studies have demonstrated thatdimensional changes occurs on the alveolar processfollowing tooth extraction and that they are more
AOL22017:32011 29/11/2017 14:29 Página 49

pronounced on the buccal aspect.14 This differencein the healing outcome may be related to the factthat the buccal wall is thinner than its palatalcounterpart.5
It has been suggested that immediate implantplacement into extraction sockets should preventthe resorption process of the buccal bone plate6, butthis has not been supported by findings fromexperiments in dogs79or by clinical trials4. Inaddition, the degree of facial reduction has beenshown to depend on the dimension of the buccalbone wall.10
It is important to consider that after implant bedpreparation, the facial bone should ideally be atleast 2 mm thick to ensure proper soft tissue supportand prevent resorption of the facial bone wallfollowing restoration.1113
It has been suggested that for a successful estheticoutcome, the implant should be placed in an idealthreedimensional position14 in order to maintainadequate buccal bone15 and tissue biotype.16
Since correct implant placement requires properunderstanding of the anatomy of the anterior region,diagnostic imaging data are essential. The thicknessof the facial bone wall17 and the position of theosseous zenith18 are two important variables fordetermining the most suitable treatment approach.Conebeam computed tomography (CBCT) iscurrently the preferred tool formeasuring thethickness of bone plate.19,20 Several studies haveexamined facial bone wall thickness, and althoughthey found statistically significant results, theyusually took few reference points (2 to 4) from the cementoenamel junction (CEJ)17,2125, oftenresulting in missing information about thicknessesat more points of the tooth.The purpose of this retrospective study was toanalyze whether the facial position of the tooth inthe alveolar ridge influences the thickness of thefacial bone wall and the distance between the CEJand OZ.Our hypothesis is that the more facial the positionof the tooth, the thinner the facial bone wall and thegreater the CEJOZ distance will be.
Additional purposes were to describe the bonethickness on the facial aspect of the anterior maxillaat seven equidistant measuring levels (ML) and tomeasure the CEJOZ distance.
MATERIALS AND METHODSThe present study included all CBCTs from patientsreferred to the Department of Periodontics, Uni versity of Buenos Aires, Buenos Aires, Argentinafor implant therapy from August to December 2015.Inclusion criteria were: 1) systemically healthypatients , 2) no contraindications for performing thetreatment , 3) patients having all upper front teethin the mouth at the time of the study 13 to 23 , 4)teeth without any injury or completely healthy intheir tooth structure .Exclusion criteria were: 1) patients with activeperiodontal disease or history of periodontal disease,2) patients with bone loss related to upper anteriorarea or with soft tissue recession, 3) patients whohad received orthodontic treatment, 4) patienttomography with scattered or distorted images, 5)teeth that had received apical surgery or with rootresorption and 6) patients who had received surgicaltreatment of any kind in the anterior upper area.A total 54 CBCTs met the inclusion criteria, providinga sample size of 203 teeth (Table 1).All patients in the study accepted the clinicalprocedures and signed the informed consent approvedby FOUBA Ethics Committee.
Radiographic image analysisThe CBCT images were analyzed on a certifiedmonitor. Slice orientation was adjusted to pass throughthe center of the examined tooth perpendicular to itslong axis (Fig. 1). The long axis of the tooth dictatedthe orientation of the vertical slice.To perform the measurements, sagittal scans fromthe reconstructed data showing the entire root and the CEJ of the examined tooth were displayed, with the largest zooming factor possible for therespective images.Image analysis was performed by image processingsoftware. The studies were performed with a 3Dconebeam volume CT (Promax 3D, Planmeca,Finland). Images were analyzed through the RomexisViewer 2.0.3 program (Romexis Viewer 2.0.3.R,Planmeca, Finland).First, total root length (L)was measured from theosseous zenith (OZ) to the apex (A). This distance
50 Hernán Bonta, et al.
Acta Odontol. Latinoam. 2017 ISSN 1852-4834 Vol. 30 Nº 2 / 2017 / 49-56
Table 1: Total number and position of analyzed teeth.
ToothNo. teethanalyzed
Canine68
Lateral64
Central71
Total203
AOL22017:32011 29/11/2017 14:29 Página 50

was divided into seven equidistant levels formeasuring the thickness of the facial bone wall ateach point (measuring levels 17 ML17) (Fig. 2).CEJOZ distance was also measured (Fig.2).To assess the facial position of the tooth (FPT), astraight line was determined from the facial mesialto the facial distal depressions of the interproximalalveolar crest. The shortest distance was measuredbetween the midfacial point of the tooth at the CEJlevel and the abovementioned line(Fig. 3).All measurements were taken by a single examinerwho was blinded to the clinical findings and thefollowup of the included patients. A preliminarytraining and calibration session on 20 CBCT revealedan intraclass coefficient of correlation ≥ 0.75.
Statistical analysisQuantitative variables were described by the samplesize (n), minimum, medium, maximum, mean andstandard deviation (SD).The relationship between quantitative continuousvariables was analyzed using the Spearman correlationtest (Spearman coefficient: ρ). Pearson´s correlation
test was not performed because the normalityassumption was not met.To compare quantitative variables between groups,the KruskalWallis test was performed, followed bypeer group comparisons when a significant resultwas obtained. Oneway ANOVA was not performedbecause assumptions of normality and homogeneity
Facial bone wall characteristics related to the tooth position 51
Vol. 30 Nº 2 / 2017 / 49-56 ISSN 1852-4834 Acta Odontol. Latinoam. 2017
Fig. 2: Measurement of facial bone wall thickness and CEJOZ distance. *CEJ = estimated position of the cementoenameljunction; L: (OZA) = length of root (osseous zenithapex);ML 17 = measuring levels 17.
Fig. 1: Slice location in the center of the respective root,perpendicular to the alveolar ridge.
Fig. 3: Measurement of the facial position of the tooth (FPT)*FPT =Facial position of the tooth.
AOL22017:32011 29/11/2017 14:29 Página 51

of variance were not met. The assumptions ofnormality and homogeneity of variance were tested by the ShapiroWilk test with modificationsand Levene, respectively. A statistically significantresult was considered when the pvalue was lessthan 0.05. The 2014 version Infostatsoftware wasused.26
RESULTSThe sample consisted of 54 subjects (22 males, 32females) with mean age 41.5 years (range 1865).Distribution of the analyzed teeth is presented inTable 1.Mean thickness of facial bone wall at different levelswas 1mm or less, except at ML7 (mean 1.3 mm).Mean facial position of the tooth in the alveolarcrest (FPT) was 0.6 mm (range 0.0 mm 2.7 mm).The distance between the CEJ and the OZ rangedfrom 0.5 mm to 6.9 mm (mean 2.9 mm) (Table 2).Vertically, no statistically significant correlationwas found between the FPT and the CEJOZvertical distance (Spearman coefficient ρ: 0.132;p value: 0.0595).
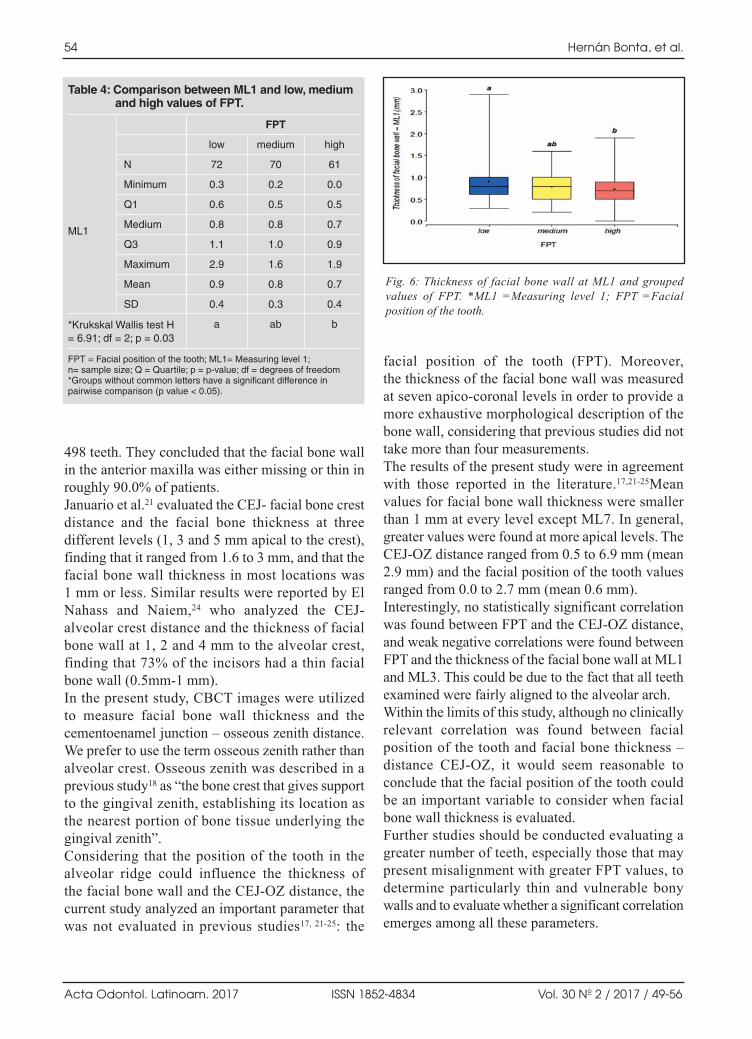
Horizontally, weak negative statistically significantcorrelations were found between FPT and facialbone wall thickness at ML1 and ML3. At the othermeasuring levels (ML2, ML4, ML5, ML6, ML7)no statistically significant correlation was found(Table 3).Facial bone wall thickness at ML1 and ML3 wascorrelated with FPT values (Fig. 4 and 5).These values were grouped into low, medium and high categories according to the followingparameters: • Low: FPT between 0 mm and 0.3 mm.• Medium: FPT greater than 0.3mm and equal to or
smaller than 0.8 mm.• High: FPT greater than 0.8 mm and equal to or
smaller than 2.7 mm.
Facial bone wall thickness at measuring level 1(ML1) varied significantly among the three groupsof FPT (Kruskal–Wallis test: H = 6.91; df = 2; p =0.03). Specifically, pairwise comparisons showedsignificant differences between the groups with lowand high values of FPT: facial bone thickness wall
52 Hernán Bonta, et al.
Acta Odontol. Latinoam. 2017 ISSN 1852-4834 Vol. 30 Nº 2 / 2017 / 49-56
Table 2: Thickness (mm) of the facial bone wall at seven measuring levels (ML 1-7), CEJ-OZ distance andFPT values.
N
Minimum
Median
Maximum
Mean
SD
ML1
203
0.0
0.8
2.9
0.8
0.4
ML2
203
0.0
1.0
2.9
1.0
0.5
ML3
203
0.0
0.8
2.4
0.9
0.5
ML4
203
0.0
0.8
3.0
0.7
0.5
ML5
203
0.0
0.6
2.2
0.8
0.7
ML6
203
0.0
0.8
2.6
0.8
0.5
ML7
203
0.0
1.3
3.8
1.3
0.7
FPT
203
0.0
0.6
2.7
0.6
0.5
CEJ-OZ
203
0.5
2.9
6.9
2.9
1.1
ML1-7 = Measuring level 1 to 7;CEJ-OZ = Cemento-enamel junction - osseous zenith; FPT = Facial position of the tooth; SD = Standard deviation
Table 3: Correlation between FPT and thickness of facial bone wall (ML 1-7).
Variable 1
FPT
FPT
FPT
FPT
FPT
FPT
FPT
Variable 2
ML1
ML2
ML3
ML4
ML5
ML6
ML7
n
203
203
203
203
203
203
203
ρ
-0.168
-0.107
-0.139
0.005
0.039
-0.05
-0.12
p-value
0.0168*
0.1273
0.0475*
0.9471
0.5762
0.4769
0.0871
* FPT = Facial position of the tooth; ML1-7 = Measuring level 1 to 7; n = sample size; P = Spearman coefficient. *p<0.05
AOL22017:32011 29/11/2017 14:29 Página 52

at ML1 was higher in the group with low FPTvalues (Fig.6,Table 4). No significant differencewas found for facial bone wall thickness at ML3compared among low, medium and high FPT values(KruskalWallis test: H = 1.88; df = 2; p = 0.386).
DISCUSSIONSeveral experimental and clinical studies haveshown that underlying bone structure plays a role
in the establishment and maintenance of estheticsoft tissue contours14, 2729. It is of clinical interest toexamine the facial bone wall dimensions of teethscheduled for extraction, especially those that areto be replaced with implants.Data concerning the thickness of the facial bonewall in the anterior maxilla could aid in designing a more accurate treatment plan. Brauntet al.17
evaluated the thickness of the facial bone wall in
Facial bone wall characteristics related to the tooth position 53
Vol. 30 Nº 2 / 2017 / 49-56 ISSN 1852-4834 Acta Odontol. Latinoam. 2017
Fig. 4: Relationship between thickness of facial bone wall at ML1 and FPT. The red vertical lines indicate the limits for thegrouping of values FPT at low, medium and high. *ML1 =Measuring level 1; FPT =Facial position of the tooth.
Fig. 5: Relationship between thickness of facial bone wall at ML3 and FPT.The red vertical lines indicate the limits for thegrouping of values FPT at low, medium and high. *ML3 =Measuring level 3; FPT =Facial position of the tooth.
AOL22017:32011 29/11/2017 14:29 Página 53
498 teeth. They concluded that the facial bone wallin the anterior maxilla was either missing or thin inroughly 90.0% of patients.Januario et al.21 evaluated the CEJ facial bone crestdistance and the facial bone thickness at threedifferent levels (1, 3 and 5 mm apical to the crest),finding that it ranged from 1.6 to 3 mm, and that thefacial bone wall thickness in most locations was 1 mm or less. Similar results were reported by ElNahass and Naiem,24 who analyzed the CEJalveolar crest distance and the thickness of facialbone wall at 1, 2 and 4 mm to the alveolar crest,finding that 73% of the incisors had a thin facialbone wall (0.5mm1 mm). In the present study, CBCT images were utilized to measure facial bone wall thickness and thecementoenamel junction – osseous zenith distance.We prefer to use the term osseous zenith rather thanalveolar crest. Osseous zenith was described in aprevious study18 as “the bone crest that gives supportto the gingival zenith, establishing its location asthe nearest portion of bone tissue underlying thegingival zenith”.Considering that the position of the tooth in thealveolar ridge could influence the thickness of the facial bone wall and the CEJOZ distance, thecurrent study analyzed an important parameter thatwas not evaluated in previous studies17, 2125: the
facial position of the tooth (FPT). Moreover, the thickness of the facial bone wall was measuredat seven apicocoronal levels in order to provide amore exhaustive morphological description of thebone wall, considering that previous studies did nottake more than four measurements. The results of the present study were in agreementwith those reported in the literature.17,2125Meanvalues for facial bone wall thickness were smallerthan 1 mm at every level except ML7. In general,greater values were found at more apical levels. TheCEJOZ distance ranged from 0.5 to 6.9 mm (mean2.9 mm) and the facial position of the tooth valuesranged from 0.0 to 2.7 mm (mean 0.6 mm).Interestingly, no statistically significant correlationwas found between FPT and the CEJOZ distance,and weak negative correlations were found betweenFPT and the thickness of the facial bone wall at ML1and ML3. This could be due to the fact that all teethexamined were fairly aligned to the alveolar arch.Within the limits of this study, although no clinicallyrelevant correlation was found between facialposition of the tooth and facial bone thickness –distance CEJOZ, it would seem reasonable toconclude that the facial position of the tooth couldbe an important variable to consider when facialbone wall thickness is evaluated. Further studies should be conducted evaluating agreater number of teeth, especially those that maypresent misalignment with greater FPT values, todetermine particularly thin and vulnerable bonywalls and to evaluate whether a significant correlationemerges among all these parameters.
54 Hernán Bonta, et al.
Acta Odontol. Latinoam. 2017 ISSN 1852-4834 Vol. 30 Nº 2 / 2017 / 49-56
Fig. 6: Thickness of facial bone wall at ML1 and groupedvalues of FPT. *ML1 =Measuring level 1; FPT =Facialposition of the tooth.
Table 4: Comparison between ML1 and low, medium and high values of FPT.
ML1
N
Minimum
Q1
Medium
Q3
Maximum
Mean
SD
*Krukskal Wallis test H= 6.91; df = 2; p = 0.03
FPT = Facial position of the tooth; ML1= Measuring level 1; n= sample size; Q = Quartile; p = p-value; df = degrees of freedom*Groups without common letters have a significant difference in pairwise comparison (p value < 0.05).
low
72
0.3
0.6
0.8
1.1
2.9
0.9
0.4
a
FPT
medium
70
0.2
0.5
0.8
1.0
1.6
0.8
0.3
ab
high
61
0.0
0.5
0.7
0.9
1.9
0.7
0.4
b
AOL22017:32011 29/11/2017 14:29 Página 54

REFERENCES1. Pietrokovski J, Massler M. Alveolar ridge resorption
following tooth extraction. J ProsthetDent 1967; 17: 2127.2. Schropp L, Wenzel A, Kostopoulos L, Karring T. Bone
healing and soft tissue contour changes following singletooth extraction: a clinical and radiographic 12monthprospective study. Int J Periodontics Restorative Dent 2003;23: 313323.
3. Pietrokovski J, Starinsky R, Arensburg B, Kaffe I. Morphologiccharacteristics of bony edentulous jaws. J Prosthodont 2007;16: 141147.
4. Sanz M, Cecchinato D, Ferrus J, Pjetursson, EB, Lang NP,Lindhe J. A prospective, randomized controlled clinicaltrial to evaluate bone preservation using implants withdifferent geometry placed into extraction sockets in themaxilla. Clin Oral Implants Res 2010 21: 1321.
5. Araujo MG, Lindhe J. Dimensional ridge alterationsfollowing tooth extraction. An experimental study in thedog. J Clin Periodontol 2005; 32: 212218.
6. Paolantonio M, Dolci M, Scarano A, D’Archivio D et al.Immediate implantation in fresh extraction sockets. Acontrolled clinical and histological study in man. JPeriodontol 2001; 72: 15601571.
7. Araujo MG, Sukekava F, Wennstrom JL, Lindhe JL. Ridgealterations following implant placement in fresh extractionsockets: an experimental study in the dog. J Clin Periodontol2005; 32: 645652.
8. Araujo MG, Sukekava F, Wennstrom JL, Lindhe J. Tissuemodeling following implant placement in fresh extractionsockets. Clin Oral Implants Res 2006; 17: 615624.
9. Araujo MG, Sukekava F, Wennstrom JL, Lindhe J. Modellingof the buccal and lingual bone walls of fresh extraction sitesfollowing implant installation. Clin Oral Implants Res2006; 17: 606614.
10. Tomasi C, Sanz M, Cecchinato D, Pjetursson B, et al. Bonedimensional variations at implants placed in fresh extractionsockets: a multivariate analysis. Clin Oral Implants Res2010; 21: 3036.
11. Grunder U, Gracis S, Capelli M. Influence of the 3D bonetoimplant relationship on esthetics. Int J PeriodonticsRestorative Dent 2005; 25:113119.
12. Buser D, Martin WD, Belser UC. Surgical considerationswith regard to singletooth replacements in the esthetic zone:Standard procedure in sites without bone defiencies. In:Buser D, Belser U, Wismeijer D (Eds). ITI Treatment Guide,Vol 1: Implant Therapy in the Esthetic Zone—SinglenTooth Replacements. Berlin: Quintessence, 2006:2637.
13. Belser UC. Replacement of an upper left persistingdeciduous canine with a regular neck implant, restored witha ceramometal crown, horizontally screwretained. In: BuserD, Belser U, Wismeijer D (Eds). ITI Treatment Guide, Vol
1: Implant Therapy in the Esthetic Zone—SingleToothReplacements. Berlin: Quintessence, 2006:159177.
14. Buser D, Martin W, Belser UC. Optimizing esthetics forimplant restorations in the anterior maxilla: anatomic andsurgical considerations. Int J Oral Maxillofac Implants2004; 19(Suppl): 4361.
15. Grunder U, Gracis S, Capelli M. Influence of the 3D bonetoimplant relationship on esthetics. Int J PeriodonticsRestorative Dent 2005; 25: 113119.
16. Chen ST, Darby IB, ReynoldsEC. A prospective clinicalstudy of nonsubmerged immediate implants: clinicaloutcomes and esthetic results. Clin Oral Implants Res 2007;18: 552562.
17. Braut V, Bornstein MM, Belser U, Buser D. Thickness ofthe anterior maxillary facial bone walla retrospectiveradiographic study using cone beam computed tomography.Int J Periodontics Restorative Dent 2011;31: 125131.
18. Carranza N, Bontá H, Gualtieri AF, Rojas MA, Galli FG,Caride F. Alveolar dimensional changes relevant to implantplacement after minimally traumatic tooth extraction withprimary closure. The osseous zenith concept and its displa cement. Acta Odontol Latinoam 2016;105114.
19. Loubele M, Van Assche N, Carpentier K. Comparativelocalized linear accuracy of smalleld conebeam CT andmultislice CT for alveolar bone measurements. Oral SurgOral Med Oral Pathol Oral Radiol Oral Endod 2008; 105:512518.
20. Menezes C, Janson G. Reproducibility of bone platethickness measurements with conebeam computed tomo graphy using different image acquisition protocols. DentPress J Orthodontics 2010; 15: 143149.
21. Januário AL, Duarte WR, Barriviera M, Mesti JC, et al.Dimension of the facial bone Wall in the anterior maxilla: aconebeam computed tomography study. Clin Oral ImplantsRes. 2011; 22: 11681171.
22. Shen JW, He FM, Jiang QH, Shan HQ. Measurement offacial bone wall thickness of maxillary anterior teethand premolars on cone beam computed tomographyimages. Zhejiang Da XueXueBao Yi Xue Ban. 201241:234238.
23. Yang G, Hu WJ, Cao J, Liu DG. Measurement of sagittalroot position and the thickness of the facial and palatalalveolar bone of maxillary anterior teeth. Zhonghua KouQiang Yi XueZaZhi. 2013 48:716720.
24. El Nahass H, N Naiem S. Analysis of the dimensions of thelabial bone wall in the anterior maxilla: a conebeamcomputed tomography study. Clin Oral Implants Res. 2015;26:5761.
25. Wang HM, Shen JW, Yu MF, Chen XYetal.Analysis offacial bone wall dimensions and sagittal root position in themaxillary esthetic zone: a retrospective study using cone
Facial bone wall characteristics related to the tooth position 55
Vol. 30 Nº 2 / 2017 / 49-56 ISSN 1852-4834 Acta Odontol. Latinoam. 2017
CORRESPONDENCEDra. Mariana A. RojasCátedra de Periodoncia, Facultad de Odontología, UBAMarcelo T. de Alvear 2142, 17º A, Buenos Aires, [email protected]
AOL22017:32011 29/11/2017 14:29 Página 55

beam computed tomography. Int J Oral MaxillofacImplants. 2014 29:11231129
26. Di Rienzo JA, Casanoves F, Balzarini MG, Gonzalez L, et al. InfoStat versión 2014. Grupo InfoStat, FCA, Univer sidad Nacional de Córdoba, Argentina. URL:http://www.infostat.com.ar
27. Berglundh T, Lindhe J. Dimension of the periimplantmucosa. Biological width revisited. J Clin Periodontol 996;23:971973.
28. Cochran DL, Hermann JS, Schenk RK, Higginbottom FL,et al. Biologic width around titanium implants. A histometricanalysis of the implantgingival junction around unloadedand loaded nonsubmerged implants in the canine mandible.J Periodontol 1997;68:186198.
29. Kan JY, Rungcharassaeng K, Umezu K, Kois JC. Dimen sions of periimplant mucosa: An evaluation of maxillaryanterior single implants in humans. J Periodontol 2003;74:557562.
56 Hernán Bonta, et al.
Acta Odontol. Latinoam. 2017 ISSN 1852-4834 Vol. 30 Nº 2 / 2017 / 49-56
AOL22017:32011 29/11/2017 14:29 Página 56

RESUMENLos objetivos de este estudio fueron estimar la frecuencia yevaluar las alteraciones posturales como factor de riesgo paratrastornos temporomandibulares (TTM).Se evaluaron pacientes de 10 a 15 años (N= 243, edad media 12.6)que concurrieron para atención odontológica integral utilizandolos protocolos CDI/TTM años. La evaluación postural estática, serealizó mediante fotografías analizadas por un fisioterapeutasiguiendo el modelo de Kendall. Los pacientes se dividieron endiferentes grupos según el diagnóstico: A: sin TTM (n = 133); B:con trastornos musculares (n = 61) y C: con desplazamiento deldisco (n = 49).No se observaron diferencias entre los grupos en la edad (p = 0,95). Se observó asociación significativa entre TTM
muscular y alteraciones en las curvas espinales, la posturade la cabeza y los miembros inferiores: OR: 3,40, 2,44 y 2,22respectiva mente. Los tipos más frecuentes fueron hiper lordosis lumbar 23,30 y 32,78%; anteversión cefálica 39.85 y 52.45%; y genu valgum 33,08 y 45,90% en A y B,respectivamente.Las alteraciones en la postura de la cabeza, las curvasvertebrales y los miembros inferiores podrían considerarsefactores de riesgo para los TTM musculares. Las alteracionesposturales más frecuentes fueron hiperlordosis lumbar,anteversión cefálica y genu valgo.
Palabras clave: Trastornos de la Articulación Temporomandi bular, postura, niño.
INTRODUCTIONThe American Academy of Pediatric Dentistry(AAPD) has recognized the multifactorial aetiologyof Temporomandibular Joint Disorders (TMJD), giventhe scant correlation between any given etiolo gicalfactor and the onset of signs and symptoms1. Theposture of the head and of the body as a whole playsan important role in the development of temporo mandibular disorders as a result of a chronicallyaltered craniocervical posture that leads to mandibularpostural changes through mechanical/biomechanicaland neuromuscular mechanisms2,3.
Findings reported by Ishii et al. in adult patientswith TMD suggest a “close relationship betweenstomatognathic function and the center of gravityof the body”4. Several studies have shown patientswith TMD to have a greater forward head posture,associated with shortening of extensor muscles inthe back of the neck3. Although a review publishedin 2006 suggests association between the cervicalspine, the stomatognathic system, and craniofacialpain, the work was based on data from poor qualitystudies with low levels of evidence (3b, 4 and 5).Better studies are therefore necessary to clarify the
ABSTRACT The aims of this study were to estimate frequency and assesspostural alterations as a risk factor for temporomandibulardisorders (TMD).Patients aged 10 to 15 years (N=243, mean age 12.6) seekingcomprehensive dental care were analyzed according to RDC/TMD. For static postural assessment, photographs were takenand analyzed by a physiotherapist following Kendall’s model.Patients were divided into: A: without TMD (n=133); B: withmuscle disorders (n=61); C: with disk displacement (N=49).No difference in age wasobserved between groups (p=0.95).Significant association was observed between muscular TMD
and alterations in spinal curves, head posture, and lower limbs:OR: 3.40, 2.44 and 2.22 respectively. The most frequent typeswere hyperlordosis 23.30 and 32.78%; forward head posture39.85 and 52.45%; and genu valgum 33.08 and 45.90% in Aand B respectively.Alterations in head posture, vertebral curves and lower limbscould be considered risk factors for muscular TMD. The mostfrequent postural alterations were lumbar hyperlordosis,forward head posture and genu valgus.
Key words: Temporomandibular Joint Disorders, posture,child.
57
Vol. 30 Nº 2 / 2017 / 57-61 ISSN 1852-4834 Acta Odontol. Latinoam. 2017
Postural alterations as a risk factor for temporomandibular disorders
Silvina Cortese, Ana Mondello, Ricardo Galarza, Ana Biondi
Universidad de Buenos Aires, Facultad de Odontología, Cátedra Odontología Integral Niños. Buenos Aires, Argentina
Alteraciones posturales como factor de riesgo para trastornos témporomandibulares
AOL22017:32011 29/11/2017 14:29 Página 57
influence of the cervical spine on the stoma tognathic system and craniofacial pain5. Cuccia and Caradonna recommend an interdisci plinary approach to TMD diagnosis and treatment,also involving experts in posture rehabilitation2. As shown by our literature review, there arereports suggesting an association between postureand TMD. Interestingly, the reviewalso showed thatthere are no interdisciplinary studies in childrenusing the diagnostic criteria for TMD recommendedby the IADR for epidemiological studies6. Thus, the aims of the present work were to estimatethe frequency of postural alterations, and assesstheir presence as risk factor for TMD in patientsaged 10 to 15 years seeking dental care at theComprehensive Dental Clinic for Children of theDepartment of Dentistry for Children of the Schoolof Dentistry, University of Buenos Aires (FOUBA).
MATERIALS AND METHODSA descriptive, prospective, crosssectional inter disci plinary study was conducted; the study wasapproved by the Ethics Committee of the FOUBA(26091227).
SubjectsThe study sample comprised boys and girls aged 10 to15 years seeking dental care at the ComprehensiveDental Clinic for Children of the Department ofDentistry for Children in the 20122013 period. Theparticipants’ caregivers provided informed consent.Children with developmental disorders, medicalcondition, and/or neurological or psychiatric disorderswere excluded.
Diagnosis of TMDWas performed by 4 paediatric dentists who werepreviously calibrated in the application of the
protocol for Research Diagnostic Criteria forTemporomandibular Disorders (RDC/TMD). Thekappa index was 0.88.
Static Postural assessmentPhotographs (front, back and both sides) were takenof the patients standing in a relaxed upright positionin front of a grid, and analysed by the teamphysiotherapist following Kendall’s postural typesconsidering head position, spinal curves, lowerlimbs, and anterior, lateral and posterior planes7.The camera was placed on a heightadjustabletripod with a standard distance of 1.5 m betweenthe camera and the subjects. The results were recorded and analyzed using mean,standard deviation, ANOVA, OR, percentages and95% confidence intervals.
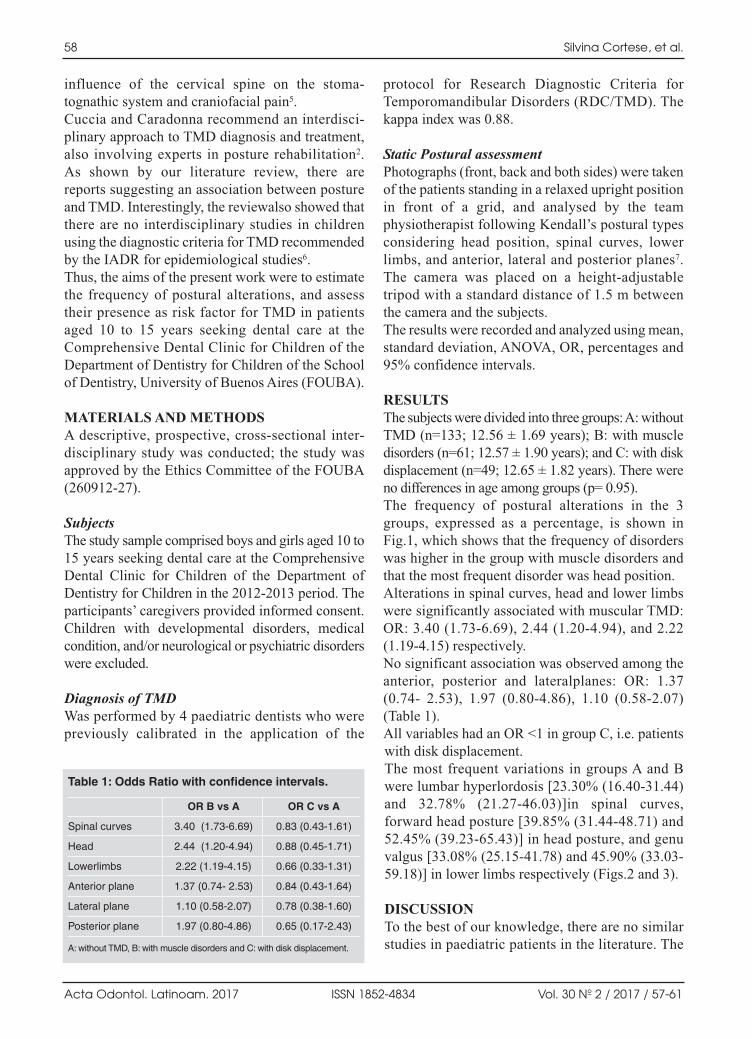
RESULTSThe subjects were divided into three groups: A: withoutTMD (n=133; 12.56 ± 1.69 years); B: with muscledisorders (n=61; 12.57 ± 1.90 years); and C: with diskdisplacement (n=49; 12.65 ± 1.82 years). There wereno differences in age among groups (p= 0.95).The frequency of postural alterations in the 3groups, expressed as a percentage, is shown inFig.1, which shows that the frequency of disorderswas higher in the group with muscle disorders andthat the most frequent disorder was head position. Alterations in spinal curves, head and lower limbswere significantly associated with muscular TMD:OR: 3.40 (1.736.69), 2.44 (1.204.94), and 2.22(1.194.15) respectively.No significant association was observed among theanterior, posterior and lateralplanes: OR: 1.37(0.74 2.53), 1.97 (0.804.86), 1.10 (0.582.07)(Table 1).All variables had an OR <1 in group C, i.e. patientswith disk displacement.The most frequent variations in groups A and Bwere lumbar hyperlordosis [23.30% (16.4031.44)and 32.78% (21.2746.03)]in spinal curves,forward head posture [39.85% (31.4448.71) and52.45% (39.2365.43)] in head posture, and genuvalgus [33.08% (25.1541.78) and 45.90% (33.0359.18)] in lower limbs respectively (Figs.2 and 3).
DISCUSSIONTo the best of our knowledge, there are no similarstudies in paediatric patients in the literature. The
58 Silvina Cortese, et al.
Acta Odontol. Latinoam. 2017 ISSN 1852-4834 Vol. 30 Nº 2 / 2017 / 57-61
Table 1: Odds Ratio with confidence intervals.
Spinal curves
Head
Lowerlimbs
Anterior plane
Lateral plane
Posterior plane
OR B vs A
3.40 (1.73-6.69)
2.44 (1.20-4.94)
2.22 (1.19-4.15)
1.37 (0.74- 2.53)
1.10 (0.58-2.07)
1.97 (0.80-4.86)
OR C vs A
0.83 (0.43-1.61)
0.88 (0.45-1.71)
0.66 (0.33-1.31)
0.84 (0.43-1.64)
0.78 (0.38-1.60)
0.65 (0.17-2.43)
A: without TMD, B: with muscle disorders and C: with disk displacement.
AOL22017:32011 29/11/2017 14:29 Página 58

Posture and temporomandibular disorders 59
Vol. 30 Nº 2 / 2017 / 57-61 ISSN 1852-4834 Acta Odontol. Latinoam. 2017
Fig. 1: Frequency of postural alterations in all groups. A: without TMD, B: with muscle disorders and C: with disk displacement.
Fig. 1: Frequencyof posturalalterations in allgroups. A: withoutTMD, B: withmuscle disordersand C: with diskdisplacement.
Fig. 3: Left kneetilted toward
the midline(Genu Valgum).
AOL22017:32011 29/11/2017 14:29 Página 59

methodology used to assess TMJ and posture inlarge samples is complex and requires theavailability of adequate physical space and sufficienttime to perform assessments on each child.A similar study conducted in a sample of 30 adultpatients with TMD and 20 adult patients withoutTMD, published in 2005, showed no significantresults on account of the great dispersion of dataresulting from the large number of variables usedto assess posture and the small sample size8. There are discrepancies among reports in theliterature on postural alterations in children. Arecent study on children aged 9 ± 1 reported a25.4% frequency, whereas a study conducted on11yearold children in the Czech Republic showed40.8% prevalence of postural disorders, with 32%corresponding to lumbar hyperlordosis. 9, 10.A systematic review seeking to evaluate thecontribution of posture and psychosocial factors tothe development of musculoskeletal pain inchildren and adolescents concluded that theduration of sitting posture may influence theexperience of musculoskeletal pain11.Saito et al. analysed posture in adult women withand without disk displacement. Their resultssuggest a close association between body postureand temporomandibular disorders, and that postureassessment could be an important component in anoverall approach to the prevention of TMD andtreatment of patients with TMD12.
A number of studies have used teleradiograph and/orphotograph analysis13. A recent study conducted byMotta et al. showed alterations in head posture inadolescents with TMD, evaluated using the HelkimoQuestionnaire and photogrammetry 14.The results of the present work are in agreementwith a study by Matheus et al. showing no relation ship between disk displacement and cervicalcurvature in adults, assessed using lateral cephalo grams and following RDC/TMD recommended bythe IADR15.The present study shows a high frequency ofpostural alterations in children aged 10 to 15 years,in keeping with previous reported results showingan association between head posture and TMD, andwith the conclusions of Saito with regard to theimportance of an overall approach to the preventionand treatment of TMD. An original finding of thecurrent study was the presence of musculardisorders and alterations in the lumbar spine andlower limbs in this age group.
CONCLUSIONSIn the present study, the most frequent types ofpostural alterations were lumbar hyperlordosis,forward head posture and genu valgus. In addition,our results suggest that the presence of alterationsin head posture, spinal curves and lower limbs arerisk factors for muscular temporomandibulardisorders.
60 Silvina Cortese, et al.
Acta Odontol. Latinoam. 2017 ISSN 1852-4834 Vol. 30 Nº 2 / 2017 / 57-61
ACKNOWLEDGMENTThis work was supported by the University of Buenos Aires,UBACyT program. Grant #20720120200008/BA
CORRESPONDENCEDra. Silvina CorteseFacultad de Odontología,UBAMarcelo T. de Alvear 2142 piso 15 A. C1122AAH. C.A.B.A, [email protected]
REFERENCES1. Clinical Guideline on Acquired Temporomandibular
Disorders in Infants, Children, and Adolescents. AmericanAcademy of Pediatric Dentistry, 2015.
2. Cuccia A, Caradonna C. The relationship between the stoma tognathic system and body posture. Clinics 2009; 64:6166.
3. Rocha CP., Croci CSand Caria P.H.Is there relationshipbetween temporomandibular disorders and head and cervicalposture? A systematic review. J Oral Rehabil 2013; 40: 875881.
4. Ishii H. A study on the relationships between imbalance ofstomatognathic function and asymmetry of craniofacial
morphology, and the center of gravity of the upright posture.Osaka Daigaku Shigaku Zasshi1990; 35:517556.
5. McNeely ML, Armijo Olivo S, Magee DJ. A systematicreview of the effectiveness of physical therapy interventionsfor temporomandibular disorders. Phys Ther 2006; 86:710725.
6. Dworkin S, Le Resche L. Research Diagnostic Criteria forTemporomandibular Disorders. J Craniomandib Disord.1992. Validación al español: González Y. y col. CriteriosDiagnósticos para la Investigación de los TrastornosTémporomandibulares.URL: http://www.rdcdinternational.org/
AOL22017:32011 29/11/2017 14:29 Página 60

7. Kendall FP, Mc Creary EK, Provance PG. Muscles: testingand function, Ed 4, Baltimore, 1993, Williams & Wilkins.
8. Munhoz WC, Marques AP, de Siqueira JT. Evaluation ofbody posture in individuals with internal temporomandi bularjoint derangement. Cranio 2005; 23:269277.
9. Trigueiro MJ, Massada L, Garganta R. Back pain inPortuguese schoolchildren: prevalence and risk factors. EurJ Public Health 2013; 23:499503.
10. Kratenova J, Zejglicova K, Maly M, Filipova V. Prevalenceand risk factors of poor posture in school children in theCzech Republic. J Sch Health 2007; 77: 131137.
11. Prins Y, Crous L, Louw QA. A systematic review of postureand psychosocial factors as contributors to upper quadrantmusculoskeletal pain in children and adolescents. PhysiotherTheory Pract 2008; 24:221242.
12. Saito ET, Akashi PM, Sacco Ide C. Global body postureevaluation in patients with temporomandibular joint disorder.Clinics 2009; 64: 3539
13. Olivo SA, Bravo J, Magee DJ, Thie NM, et al. The asso ciation between head and cervical posture and tempo ro man dibular disorders: a systematic review. J Orofac Pain2006; 20:923.
14. Jansisk Motta L, Porta Santos Fernandes K, AgnelliMesquita Ferrari R, et al Temporomandibular dysfunctionand cervical posture and occlusion in adolescents. Braz JOral Sci 2012; 11: 401405
15. Matheus, RA, RamosPerez FM, Menezes AV, AmbrosanoGM et al. The relationship between temporomandibulardysfunction and head and cervical posture. J Appl Oral Sci2009;17:204208.
Posture and temporomandibular disorders 61
Vol. 30 Nº 2 / 2017 / 57-61 ISSN 1852-4834 Acta Odontol. Latinoam. 2017
AOL22017:32011 29/11/2017 14:29 Página 61

62
Acta Odontol. Latinoam. 2017 ISSN 1852-4834 Vol. 30 Nº 2 / 2017 / 62-67
RESUMOO objetivo desta pesquisa foi avaliar o impacto da saúde bucalsobre a qualidade de vida de pacientes com câncer de cabeçae pescoço após radioterapia e comparar com pacientes semhistórico de neoplasias. Foram avaliados no total 75indivíduos, 30 indivíduos com câncer de cabeça e pescoço apósradioterapia (grupo de estudo), e 45 indivíduos sem históricode câncer (grupo controle).Todos receberam avaliação dacondição bucal de acordo com critérios da OrganizaçãoMundial de Saúde: a atividade de cárie pelo índice CPOD,presença de doença periodontal pelo índice IPC, índice deedentulismo e por fim o impacto da condição bucal sobre a
qualidade de vida, através do questionário OHIP14.Quandocomparados o grupo de estudo e grupo controle foi encontradadiferença estatística significativa para as condições deatividade de cárie (p<0,001), doença periodontal (p<0,001) eausência de dentes (p<0,001). Estas condições apresentaramimpacto médio sobre a qualidade de vida dos pacientes.Acondição de saúde bucal de indivíduos com câncer de cabeçae pescoço depois da radioterapia é deteriorada e impactadiretamente sobre a qualidade de vida destes pacientes.
Palavras chave: Qualidade de vida, Neoplasias de cabeça epescoço, Radioterapia, Saúdebucal.
IntroductionIn Brazil, approximately 17.500 new cases of headand neck cancer in males and 5.340 in females wereestimated in the year 20161. Treatment of head and neck cancer primarily involves surgery andradiotherapy, which may or may not be combinedwith chemotherapy, depending on the stage of thedisease2. The main oral complications caused by thesetherapies are oral mucositis, radiodermatitis, vascularlesions, tissue atrophy, dysgeusia, fibrosis of tissuesand muscles, mucosal edema, soft tissue necrosis,decreased saliva flow, opportunistic infections,radiation caries and osteoradionecrosis35.
The oral condition of head and neck cancer patientsdeteriorates due to the antitumor treatment and maycompromise the masticatory function as a result ofdamage to tooth integrity, periodontal structures,mandibular and maxillary support, temporo mandibular joint, masticatory musculature, facialexpression and tongue, as well as their tissues,innervation and vascularization6,7. The diagnosis of oral conditions and oral health care shouldthereforebe part of multidisciplinary cancer care, with the aim of providing comprehensivetreatment, including physical and emotional supportto patients5,8.
ABSTRACTThe aim of this study was to assess the impact of oral health onthe quality of life of patients with head and neck cancer afterradiotherapy, combined or not with chemotherapy, and tocompare it with that of patients with no history of neoplasia. Atotal 75 individuals were evaluated,including 30 with head andneck cancer after radiotherapy (study group) and 45 with nohistory of cancer (control group). All patients were evaluatedaccording to World Health Organization criteria: cariesactivity by DMTF index, presence of periodontal disease byCPI index, edentulism index and impact of oral condition on
quality of life through the OHIP14 questionnaire. Statisticallysignificant differences were found between the study group(SG) and the control group (CG)for caries activity conditions(p <0.001), periodontal disease (p <0.001) and missing teeth(p <0.001). These conditions had an average impact on thequality of life of cancer patients. The oral health condition ofindividuals with head and neck cancer deteriorates afterradiotherapy, with direct impact on their quality of life.
Key words: Quality of life, Head and neck neoplasms,Radiotherapy, Oral health.
The impact of oral health on quality of life in individuals with head and neck cancer after radiotherapy: the importance of dentistry in psychosocial issues
Paulo S.S. Santos, Adrielle L. Cremonesi, Reyna A. Quispe, Cássia M. F. Rubira
Universidade de São Paulo, Faculdade de Odontologia de Bauru, Departamento de Cirurgia, Estomatologia, Patologia e Radiologia, Brazil.
O impacto da condição bucal sobre a qualidade de vida de indivíduos com câncer de cabeça e pescoço após radioterapia: a importância da odontologia nos aspectos psicossociais
AOL22017:32011 29/11/2017 14:29 Página 62

Researchers have been developing tools to assessthe impact of oral health related to the quality oflife of systemically compromised individuals9.Within this context, the World Health Organization(WHO) has included this topic among their targetsfor 202010, to provide routine patient treatmentwhich includes both physical and psychosocialaspects related to oral problems1113. To date, wehave found only one article in the national andinternational literature relating the oral condition ofindividuals treated for head and neck cancer toimpact onquality of life 7.The aim of this study was to evaluate the oral healthof head and neck cancer patients after radiotherapy,combined or not with chemotherapy, and compareit to that of patients without a history of cancer inorder to trace the disease profile in the postcancerphase.
MATERIALS AND METHODSThe current research was approved by the HumanEthics and Research Committee of the School ofDentistry of Bauru of the University of São Paulo(nº 703.115). A total 75 patients were divided intotwo groups: the study group (SG) and the controlgroup (CG), matched according to age. The SGconsisted of 30 individuals with head and neckcancer after radiotherapy, combined or not withchemotherapy. The CG consisted of 45 individualswithout a history of cancer who were in good healthand received dental care at the Bauru School ofDentistry USP.
Evaluation of oral condition Oral condition was evaluated according to theDMFT index (Decayed, Missing and Filled Teeth),community periodontal index (CPI) and evaluationof the use and need of prostheses. Data werecollected by a calibrated dentist following the WHOOral Health Surveys: Basic Methods instructions.The individual DMFT index was calculated byadding the scores. The DMFT of the populationwas calculated by dividing the sum of theindividual DMFT values by the number of patientsexamined, which provided a classification ofcaries activity.The CPI was applied by using a blunt periodontalprobe recommended by the WHO, a flat dentalmirror and a disposable wooden spatula underartificial light. Presence of biofilm, dental calculus
and periodontal pockets was recorded for the buccaland lingual surfaces of six index teeth: right upperfirst molar (16), right upper central incisor (11), leftupper first molar (26), lower left first molar (36),lower left central incisor (31) and the first lowerright molar (46).The evaluation of edentulism followed WHOguidelines for epidemiological surveys. It consideredtype and site of prosthesis, mandibular or maxillary,according to the prosthetic spaces corresponding to the missing teeth observed in the physicalexamination.
Evaluation of the impact of oral health on quality of lifeThe assessment of the impact of oral health onquality of life was carried out using the Oral HealthImpact Profile (OHIP14), composed of 14 questionsproposed by Slade (1997)14and validated in thePortuguese language by Oliveira and Nadanovsky(2005)15. The OHIP14 analyzes the impact onquality of life by the dimensions of oral health, whichare the following: functional limitation, physicalpain, psychological discomfort, physical incapacity,psychological incapacity, social incapacity anddisability, according to the weights for the answersobtained.The response scale (0 = never, 1 = hardly ever, 2 =sometimes, 3 = almost always, 4 = always) wasmultiplied by the corresponding weight to calculatetotal impact. Impact was considered weak 0 1.33,average 1.33 2.68, and strong > 2.68. Overallimpact was given by the sum of the impact of thedimensions, and considered weak for scores of lessthan 9.33, medium 9.33 18.66 and strong > 18.66.
Statistical analysisThe KruskalWallis test was used for all multiplecomparison procedures by the Dunn method,considered significant when p <0.05.
RESULTSTable 1 shows the demographics, including age, sex,type and location of the neoplasia, submitted toradiotherapy combined or not with chemotherapy,and type of radiotherapy.In SG, DMFT ranged from 17 to 28 with a medianof 24, while in CG it ranged from 12 to 32 with amedian of 18. The difference between SG and CGwas statistically significant (p <0.001) (Table 2).
Quality of life in head and neck cancer patients 63
Vol. 30 Nº 2 / 2017 / 62-67 ISSN 1852-4834 Acta Odontol. Latinoam. 2017
AOL22017:32011 29/11/2017 14:29 Página 63
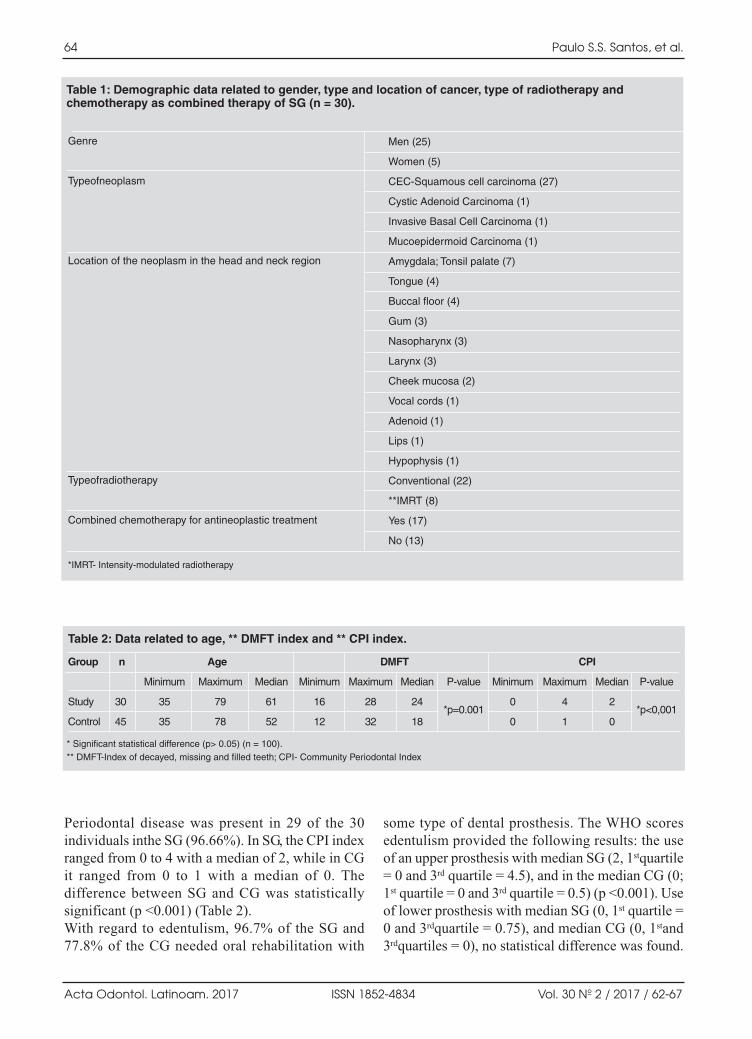
Periodontal disease was present in 29 of the 30individuals inthe SG (96.66%). In SG, the CPI indexranged from 0 to 4 with a median of 2, while in CGit ranged from 0 to 1 with a median of 0. Thedifference between SG and CG was statisticallysignificant (p <0.001) (Table 2).With regard to edentulism, 96.7% of the SG and77.8% of the CG needed oral rehabilitation with
some type of dental prosthesis. The WHO scoresedentulism provided the following results: the useof an upper prosthesis with median SG (2, 1stquartile= 0 and 3rd quartile = 4.5), and in the median CG (0;1st quartile = 0 and 3rd quartile = 0.5) (p <0.001). Useof lower prosthesis with median SG (0, 1st quartile =0 and 3rdquartile = 0.75), and median CG (0, 1stand3rdquartiles = 0), no statistical difference was found.
64 Paulo S.S. Santos, et al.
Acta Odontol. Latinoam. 2017 ISSN 1852-4834 Vol. 30 Nº 2 / 2017 / 62-67
Table 2: Data related to age, ** DMFT index and ** CPI index.
Group n Age DMFT CPI
Minimum Maximum Median Minimum Maximum Median P-value Minimum Maximum Median P-value
Study 30 35 79 61 16 28 24*p=0.001
0 4 2*p<0,001
Control 45 35 78 52 12 32 18 0 1 0
* Significant statistical difference (p> 0.05) (n = 100).** DMFT-Index of decayed, missing and filled teeth; CPI- Community Periodontal Index
Table 1: Demographic data related to gender, type and location of cancer, type of radiotherapy and chemotherapy as combined therapy of SG (n = 30).
Genre
Typeofneoplasm
Location of the neoplasm in the head and neck region
Typeofradiotherapy
Combined chemotherapy for antineoplastic treatment
Men (25)
Women (5)
CEC-Squamous cell carcinoma (27)
Cystic Adenoid Carcinoma (1)
Invasive Basal Cell Carcinoma (1)
Mucoepidermoid Carcinoma (1)
Amygdala; Tonsil palate (7)
Tongue (4)
Buccal floor (4)
Gum (3)
Nasopharynx (3)
Larynx (3)
Cheek mucosa (2)
Vocal cords (1)
Adenoid (1)
Lips (1)
Hypophysis (1)
Conventional (22)
**IMRT (8)
Yes (17)
No (13)
*IMRT- Intensity-modulated radiotherapy
AOL22017:32011 29/11/2017 14:29 Página 64

Need for upper prosthesis, with median SG (0,1stquartile = 0 and 3rd quartile = 1) and median CG(1, 1st quartile = 0 and 3rd quartile = 2) (p <0.001).Finally, the need for lower prosthesis with medianSG (2; 1stquartile = 2 and 3rdquartile = 2) and medianCG (0; 1stquartile = 0 and 3rdquartile = 1) (p <0.001).Values for impact of oral condition on quality of lifein the SG were 4.67 to12.94, with a median of 9.62,indicating medium impact. In contrast, the valuesin the CG were 0 to6.42, with median of 1.48,indicating weak impact. The impact of oralcondition on quality of life differed significantlybetween SG and CG (p <0.001).
DISCUSSIONTwo thirds of head and neck cancer patients havelocalized or regionally advanced disease, andalthough there is controversy regarding the besttreatment, they are usually treated with surgery, andradiotherapy, which may or may not be combinedwith chemotherapy (multimodal treatment). Thesetherapies have adverse effects on oral health,especially if oral diseases such as caries andperiodontal disease are already present, andinvariably compromise quality of life2.Among the most frequent complications thatcompromise patient quality of life are reduction orabsence of salivary flow, radiation cavities,periodontitis, odynophagia, dysphagia, pain andspeech difficulties17, which may compromise thepatient’s social, nutritional and global health andquality of life as a whole.The DMFT index estimated by the WHO is 1.2 to2.6, the current value for the Brazilian populationbeing 2.118. The present study reveals a noticeablediscrepancy between the national index and theindices for the population that received radiationfor the head and neck region The incidence foundin the literature was similar to that found in thisstudy (DMFT = 24 / median), which is a high index,considering that the individuals in these studiesended radiotherapy over 6 months ago1820. Theliterature includes studies conducted on patients ofspecific ethnicities, but in all of them, time aftertreatment seems to be a determining factor for theeffects of antineoplastic therapies on caries activity,which may be greater, especially when it is inducedby radiotherapy and chemotherapy1820.The incidence of periodontal disease in postantineoplastic therapy head and neck cancer
patients is poorly described in the literature, but itis about 64% to 78% 20,21. Our study found anincidence of 96.6%, and a significant difference inCPI between SG and CG (p <0.001), revealing thatperiodontal disease is also a matter of concern inthis group of patients, mainly due to infectioncontrol and evolution to tooth loss. Tooth loss iscommon in the evolution of periodontal diseasebecause it is difficult to control22. Many studiesmention the relevance of performing periodontaldisease prevention prior to treatment withradiotherapy / chemotherapy, because periodontaldisease is more difficult to control afterantineoplastic therapies5,20,22,23.Radiotherapy increases the risk of osteoradione crosis, especially when the dose exceeds 60 Gy andis associated with local trauma such as dentalextractions, and infections such as uncontrolledperiodontal disease, and compromised byhyposalivation24,25.Edentulism in individuals treated for head and neckcancer has not yet been evaluated, according to areview of the literature in English and Portuguese.Although the absence of teeth is described in oralrehabilitation studies after radiotherapy, theincidence of edentulism is not reported. Our studyfound significant differences between SG and CG(p <0.001) with a high incidence of oralrehabilitation (46.6%), mainly related to the needfor prostheses in the maxillary and mandibulararches. These results lead us to reflect on thelimitations related to missing teeth, often prior toradiotherapy and surgery. With regard to theevolution of radiation cavities and periodontaldisease as a consequence of radiotherapy, oralrehabilitation options are often denied by dentistsbecause of the limited therapeutic options.Prosthetic rehabilitation and/or dental implants arestill questioned in the literature; however, it ismentioned that having received radiotherapy is notan impediment for rehabilitation.It is clear that it isnecessary to establish strict criteria regarding thetype, dose and area of radiotherapy26in order toachieve adequate oral rehabilitation forthe patient.Edentulism itself impacts quality of life, leading tofunctional, aesthetic, social and psychologicalchanges.The psychosocial aspects related to oral problemshave been of interest to the WHO since the 1980s,when the consequences of diseases in people’s daily
Quality of life in head and neck cancer patients 65
Vol. 30 Nº 2 / 2017 / 62-67 ISSN 1852-4834 Acta Odontol. Latinoam. 2017
AOL22017:32011 29/11/2017 14:29 Página 65

lives were classified, and since 2000 these aspectshave been related to dentistry. In this context, theOHIP14 questionnaire provides answers related tothe dimensions of physical and psychosociallimitations that can diagnose the impact of oral healthon quality of life. The literature contains only onereport of research in the field of head and neck cancerin which the Oral Health Related to Quality of Life(OHRQoL) questionnaire was used to associate oralcondition and quality of life after radiotherapy7, andnone using the OHIP14. In the current study, theOHIP14 questionnaire showed that the impact oforal health on quality of life in SG was average(9.62), and differed significantly from CG (1.48) (p<0.001). These results reveal a clear diagnosis andan alert forthe need for care in the return to andmaintenance of oral health of individuals who undergo radiotherapy in the head and neck region, as wellas the need for further research on the relationshipbetween oral status and quality of life.Acute and late complications of antineoplastictherapy such as oral mucositis, dysgeusia, radiationcaries, periodontal disease and osteoradionecrosisof the maxilla5 have a relevant effect on the patient,
reducing his/herquality of life. Clearly thesecomplications can be appropriately reduced andcontrolled with prior dental treatment and properconservation.Considering the results of this study, it is importantto reflect on the biological limits of oral healthmaintenance and oral rehabilitation of patients who under go antineoplastic treatment, especiallyradiotherapy to treat head and neck cancer. It is alsoimportant to understand that the multidisciplinaryteam, including dentists, should be committed notonly to curing cancer, but also to returning quality oflife to patients, provided that everyone understandsthe limitations and the possibilities of applyingconsolidated techniques to return these patients tooral health.
CONCLUSIONSCaries activity, periodontal disease index andincidence of edentulism are high in individualsundergoing radiotherapy to treat head and neckcancer. These oral conditions significantly andnegatively compromise the quality of life of thesepatients.
66 Paulo S.S. Santos, et al.
Acta Odontol. Latinoam. 2017 ISSN 1852-4834 Vol. 30 Nº 2 / 2017 / 62-67
CORRESPONDENCEDr. Paulo Sérgio da Silva SantosAl. Dr. Octávio Pinheiro Brisolla, 975, Vila Universitária, Bauru, SP, Brasil, Zip Code: 17011136, [email protected]
REFERENCES1. INCA Instituto Nacional do Câncer. Available in:
http://www.inca.gov.br/estimativa/2016/sintesederesultadoscomentarios.asp. Accessed in: 09/10/2016.
2. Cohen EEW, LaMonte SJ, Erb NL, Beckman KL, SadeghiN,Hutcheson KA et al.American Cancer Society Head andNeck Cancer Survivorship Care Guideline. CA Cancer JClin 2016; 66:203239.
3. Hancock PJ, Epstein JB, Sadler GR.Oral and dentalmanagement related to radiation therapy for head and neckcancer. J CanDent Assoc 2003;69:585590.
4. Barry JM. The dentist’s role in managing oral complicationsof cancer therapies. Dent Today 2005;24:5861.
5. Ghelardi IR, Soares Jr LAV, Santos PSS, Teixeira SS et al. Anecessidade da avaliação e tratamento odontológico préradioterapia. Prática Hospitalar 2008;58:149151.
6. Psoter WJ, Aguilar ML, Levy A, Baek LS et al. A preliminarystudy on the relationships between global health/quality oflife and specific head and neck cancer quality of life domainsin Puerto Rico. J Prosthodont 2012;21: 460471.
7. Shavi GR, Thakur B, Bhambal A, Jain S et al. OralHealth Related Quality of Life in Patients of Head and Neck
Cancer Attending Cancer Hospital of Bhopal City, India. JInt Oral Health 2015;7:2127.
8. Huber MA, Terezhalmy GT. The head and neck radiationoncology patient. Quintessence Int 2003;34:693717.
9. Sischo L, Broder HL. Oral healthrelated quality of life:what, why, how, and future implications. J Dent Res 2011;90:12641270.
10. Hobdell M, Petersen PE, Clarkson J, Johnson N.Globalgoals for oral health 2020. Int Dent J 2003; 53:285288.
11. Petersen PE. The World Oral Health Report 2003: continuousimprovement of oral health in the 21st century—the approachof the WHO Global Oral Health Programme. CommunityDent Oral Epidemiol 2003; 31(Suppl 1):323.
12. Petersen PE. Priorities for research for oral health in the 21stcentury—the approach of the WHO Global Oral HealthProgramme. Community Dent Health 2005; 22(2):7174.
13. Petersen PE. Global policy for improvement of oral healthin the 21st centuryimplications to oral health research ofWorld Health Assembly 2007, World Health Organization.Community Dent Oral Epidemiol 2009; 37(1):18.
14. World Health Organization. Oral Health surveys: basicmethods. Geneva: World Health Organization, 1997.
AOL22017:32011 29/11/2017 14:29 Página 66

15. Slade GD. Derivation and validation of a shortform oralhealth impact profile. Community Dent Oral Epidemiol1997;25(4):284290.
16. Oliveira BH, Nadanovsky P. Psychometric properties of theBrazilian version of the Oral Health Impact Profileshortform. Community Dent Oral Epidemiol 2005; 33:307314.
17. Kamath MP, Hegde MC, Screedharan S, Salmi D, et al.Radiotherapeutic effect on oropharyngeal flora in head andneck cancer. Indian J Otolaryngol Head and Neck Surg2002;54(2):1931.
18. KonjhodžićPrcić A, Keros J , Ajanović M , Smajkić N etal. Incidence of Radiation Caries in Patients UndergoingRadiation Therapy in the Head and Neck Region. Pesq BrasOdontoped Clin Integr 2010;10:489492.
19. Lázos JP. Lesiones estomatológicas asociadas a terapiaoncológica. Rev Asoc Odontol Arg 2003;91:100103.
20. Rouers M, Dubourg S, Bornert F, Truntzer P et al. Orodentalstatus before radiation therapy of the head and neck area: Aprospective analysis on 48 patients. Cancer Radiother2016;20:199204.
21. Brasil Sorridente 2010. Available in: http://dab.saude.gov.br/CNSB/sbbrasil/arquivos/apresentacao_abbrasil_2010.pdf.Accessed in 07/15/2016.
22. Bertl K, Loidl S, Kotowski U, Heiduschka G, et al. Oralhealth status and dental care behaviours of head and neckcancerpatients: a crosssectional study in an Austriantertiary hospital.Clin Oral Investig 2016;20:13171327.
23. Magalhães MHCG, Candido AP, Araújo NS. Oral sequelaeresulting from head and neck radiotherapy: protocol forprevention and treatment. RPG Rev Pós Grad 2002;9:711.
24. Nabil S, Samman N. Incidence and prevention ofosteoradionecrosis after dental extraction in irradiatedpatients: a systematic review. Int J Oral Maxillofac 25.Faloni AP de S, Lorenzon AP, Margonar R, Fernandes JMAet al. Importance of the Periodontal Procedures Previouslyto Head and Neck Radiotherapy. Rev IntPeriodontiaClin2005;2:9399.
26. Zen Filho EV, Tolentino ES, Santos PS. Viability of dentalimplants in head and neck irradiated patients: A systematicreview. Head Neck 2016;38 Suppl 1:E222940.
Quality of life in head and neck cancer patients 67
Vol. 30 Nº 2 / 2017 / 62-67 ISSN 1852-4834 Acta Odontol. Latinoam. 2017
AOL22017:32011 29/11/2017 14:29 Página 67

68
Acta Odontol. Latinoam. 2017 ISSN 1852-4834 Vol. 30 Nº 2 / 2017 / 68-75
RESUMENEl mejor material para reparar defectos superficiales delesmalte es uno muy similar al original y que este interactúecon los mecanismos naturales de remineralización. Este noarregla daños extensos por lo que se requiere de una ayudaexterna para rellenar defectos grandes con un material queactive la remineralización salivar que sea eficiente pero demenor alcance. Para esto se emplearon cerámicas compuestasprincipalmente fosfocálcicas. La adhesión efectiva de lareparación puede depender de la cantidad de fluidos acuososexistentes en la porosidad del esmalte pues aparentementepermiten la nucleación y crecimiento de nuevos minerales paraasegurar adhesión y estabilidad. La cantidad de fluidos estágobernada por la presión osmótica. En este estudio se evaluóla influencia que tienen dos valores de presión osmótica de la saliva isotónica y hipotónica y dos composiciones
de agente remineralizante modificado: condicionador y agente remineralizante en composiciones de 90%/10% (A) y 50%/50%(B) respectivamente, sobre el llenado de grietas artificiales por perfilometría, estereomicroscopio ymicroscopía confocal láser. Se trabajó con un diseño factorial22 y tratamiento estadístico: modelo logístico. Solamente lacomposición de la sustancia remineralizante tuvo efectosignificativo en la eficiencia para reparar defectos. Lacomposición tiene un efecto reparador sobre los defectos del esmalte dental en sus dos composiciones, no obstante, la composición 50%/50% presenta niveles más altos dereparación y forma depósitos que al estereomicroscopio seobservan más compactos.
Palabras Clave: Esmalte dental; Materiales biocompatibles;Fosfatos de calcio; Remineralización dental.
INTRODUCTIONDental enamel is a bioceramic composite whichconsists of 96% minerals and 4% organic material(proteins) and water 1,2. Because it lacks cells, ratherthan being considered a tissue, it is considered to be ahighly mineralized extracellular substance incapableof regenerating itself when it suffers attacks 1,3.
Enamel may suffer superficial defects such asinfractions in response to mechanical overexertionor extreme conditions to which it is subjected in the oral cavity. To treat such injuries, reparativetechniques have been used,4including restorativematerials with different retention mechanisms5 suchas amalgam, metal alloys, ceramics, and composite
ABSTRACTThe best material for repairing enamel surface defects is one verysimilar to the original enamel and which interacts with naturalremineralization mechanisms. It does not repair extensivedamage, so in order to fill large defects,external help is requiredusing phosphocalcic ceramic composites that activate salivaryremineralization efficiently though on smaller in scale. Effectiveadhesion of the repair may depend on the amount of aqueousfluids present in the enamel, which apparently enable nucleationand growth of new minerals to ensure adhesion and stability. Theamount of fluids is governed by osmotic pressure. This studyevaluated the influence of two osmotic pressure values of isotonicand hypotonic saliva and two modified remineralizing agent
compositions: combinations of “conditioner” and “remineralizingagent” in proportions of 90%: 10% (A) and 50%: 50%(B), onfilling artificial cracks. Results were evaluated by profilometer,stereomicroscope and confocal laser microscope. A 22 factorialdesign and a logistic model for statistical analysis were used.Only the composition of the mineralizing agent had a significanteffect on efficiency in repairing defects. Compositions A and Bboth repaired dental enamel defects, but composition B presentedhigher levels of repair and more compact deposits as observedunder stereomicroscope.
Key words: Dental enamel, biomaterials, calcium phosphates,tooth remineralization.
Evaluation of an experimental remineralizing agent for repairing enamel surfaces
Margarita V. Úsuga Vacca1, Carolina Torres-Rodríguez2, Edgar Delgado-Mejía3
1 Magister en Odontología, Facultad de Odontología, Universidad Nacional de Colombia.
2 Universidad Nacional de Colombia, Facultad de Odontología, Departamento de Salud Oral. Bogotá D.C., Colombia.
3 Universidad Nacional de Colombia. Facultad de Ciencias, Departamento de Química, Bogotá D.C., Colombia.
Evaluación de un agente remineralizante experimental reparador de superficie de esmalte
AOL22017:32011 29/11/2017 14:29 Página 68

resins combined with dental adhesives6,7, all ofwhich have provided acceptable solutions forpreserving tooth integrity. However, small, shallowlesions that are thicker than 50μm8 do not warrantthe use of preparations that destroy even moredental structure and lead to the use of restorationsthat form interfaces with the dental substrate and facilitate microfiltration and tooth decay.Knowledge of the composition of enamel andbiomaterials has driven the search for moreconservative solutions to the problem of loss intooth integrity.Different bioceramics have been proposed forclinical use in view of their biocompatibility,bioactivity and dissolution rates. Supersaturatedsolutions of calcium, phosphate and magnesiumions9,10, fluorapatitegelatin11, electrodeposition12,apatite13 and fluorapatite cement have been studiedand proposed for tooth enamel repair14. Manystudies of these materials are currently still in the invitro phase, so their effects in clinical conditionsare as yet unknown.Agents containing mainly calcium phosphates, suchas a “modified conditioner” and a “remineralizingagent”, which have been tested in vitro on enamelcrack defects, decreased the size and number ofthese defects without creating an interface. The“modified conditioner” produced many adherentdeposits of irregular appearance and different colorof the enamel15,16, while the “remineralizing agent”created less abundant deposits and had a clearappearance and regular pattern17,18. Experimentswere conducted with each agent at two differenttime points on moist, freshly extracted teeth. Theagents were then tested on dry teeth one year afterextraction. Better results were obtained with wetteeth than with dry teeth. As a general result of theexperiments, it was suggested that the difference inthe results was due to the moisture level of thespecimens 1518. The seemingly complementary properties of thetwo ceramics “remineralizing agent” and “modifiedconditioner”,in addition to their ease of handlingand the low cost of their components, led to theproposal of combining them as a third substance,Modified Remineralizing Agent (MRA), whichcombines properties of the original componentsregarding volume, regularity and color of thedeposits formed. Different proportions of the twoceramics in the combination yield different results,
and must therefore be defined.Two compositionswere selected and called MRA1 (90% remine ralizing agent and 10%modified conditioner) andMRA2 (50% and 50%). The effects of these twoMRA compositions and two moisture contents onthe efficiency of the repair process on grooveshaped enamel defects (more or less deep straightcuts) in tooth enamel were studied. The aim of theseexperiments was to determine whether the level ofenamel repair depended on saliva composition(osmotic pressure), modified remineralizing agent(MRA) composition, or the interaction between them.This study seeks to advance the understanding ofthe behavior of the material under controlledlaboratory conditions.
MATERIALS AND METHODSSample collectionWith prior approval from the Ethics Committee ofthe School of Dentistry at Universidad Nacional deColombia (CIE0001711) and signed informedconsent from the donor patients, aged 15 to 45 years,104 human teeth without hypoplasia, fractures,endodontic treatment, rehabilitation, bleaching orvestibular restorations were collected.
Sample pretreatmentFollowing the Tooth Bank standards of the Schoolof Dentistry at Universidad Nacional de Colombia,the teeth were transported, cleaned, disinfected and preservaded in 0.5% chloramineT at 4°C19.The middle third of the vestibular surface wasestablished as the study zone, and delimited by fourmarks in a square made with a round ¼ carbide bur,17839SSWHITE, with a highspeed NSK (at200,000 rpm) handpiece. A cutter was used to creategrooveshaped enamel defects in mesiodistaldirection, 200 µm to 400 µm deep and 100 µm to260 µm wide. The profiles and dimensions of thedefects were established using a Veeco profilometer,Dektak model; a Nikon SMZ 800 CDS stereomi croscope and an LSM 700/Zeiss confocal lasermicroscope (Fig.1).Following the experimental design in a symmetrical22 factorial arrangement, there were two controlledfactors with two levels each: Compositions of themodified remineralizing agent MRA1and MRA2,and isotonic (IS) and hypotonic (HS)saliva. The twodifferent MRA compositions contained differentpercentages of preexisting components (products
Repairing enamel surfaces 69
Vol. 30 Nº 2 / 2017 / 68-75 ISSN 1852-4834 Acta Odontol. Latinoam. 2017
AOL22017:32011 29/11/2017 14:29 Página 69

of the ceramics laboratory, Department ofChemistry, Universidad Nacional de Colombia) andsaliva composition was established by varying itsosmotic pressure. Specimens were randomlydivided into four paired groups of 26 samples,labeled as MRA1IS, MRA1HS, MRA2IS andMRA2HS, where IS and HS are isotonic andhypotonic saliva respectively, according to thecorresponding combinations of treatment effects.
Sample treatmentTo evaluate the effect of the osmotic pressure of themoist environment on the outcome of fillingdefects, teeth were submerged in artificial isotonic(IS) or hypotonic (HS) saliva for two weeks, thenwashed with a toothbrush under running water, afterwhich they were subjected to surface abrasion withnumber 1000 silicon carbide sandpaper, washed inwater with a soft tooth brush and cleaned with 2propanol to remove impurities. To evaluate theefficiency of the MRA compositions, MRA1 andMRA2 were applied to randomly selected teeth forsix hours, with the treatment area isolated from theenvironment. After the treatment time, the teethwere washed again with a brush and running waterto remove any nonadherent deposited material.Teeth were observed and photographed via stereo mi croscopy at 4X magnification. A previouslycalibrated observer, with Kappa 1 intraexaminerreproducibility, assessed treatment results under astereomicroscope by classifying the filling of
defects into three levels: Low, when part of thefloor of the created defect was visible (not coveredwith filling material); Medium, when the filling didnot reach one or all of the external boundaries ofthe defect, but the floor was not visible; and High,when the filling level of the defect reached orexceeded the external boundaries.
Statistical analysisBecause the response variable was binary, a logisticmodel was used to identify the effect of treatments.Different analyses were performed using generalizedlinear models to determine the effects of salivacomposition (osmotic pressure) and composition(MRA1 or MRA2) on the level of tooth repair. Thechosen statistical hypotheses of interest (MRAcomposition, saliva, and their interaction) wereconsidered significant when p< 0.05. Goodness offit was verified with statistical procedures based onproperties of the chisquared distribution, and thequality of fit of the proposed model was validatedthrough a graphic review of Pearson and Devianceresiduals. The information obtained was processedusing R software, version 11.1.
RESULTSAll treated teeth presented some degree of repair,and only one tooth presented a low level of repair.This tooth was eliminated, and only medium andhigh levels of repair were considered; thus, theanalysis focused on modeling the probability that
70 Margarita V. Úsuga Vacca, et al.
Acta Odontol. Latinoam. 2017 ISSN 1852-4834 Vol. 30 Nº 2 / 2017 / 68-75
Fig. 1: A and B Grooveshaped enamel defects200400 µm deep and 100 260 µm wide were created in the mesiodistal direction.Defect profiles and dimensions were established using stereomicroscope and confocal laser microscope.
AOL22017:32011 29/11/2017 14:29 Página 70

the tooth would have a high level of repair. Agreater number of teeth was found to have a highlevel of repair (76% of the total). The proportion ofteeth with medium and high level of repair was thesame for each treatment; however, teeth treatedwith composition MRA2 (50%50%) seemed toattain a higher degree of repair (Table 1).Fitting the logistic model to the interaction showedno statistical significance (p = 0.43), meaning thatwhen salivary osmotic pressure varied, whether ornot the MRA composition was constant, there wasno change in the level of repair.Thus, the finaldefinitive study model additively incorporated theeffects of saliva composition and remineralizingagent only. For the model with interaction, changing theosmotic pressure did not statistically influence thelevel of repair, given that the p=0.82 value is veryhigh. In contrast, significant differences weredetected for MRA (p< 0.05), as shown in Table 2.With regard to differences in the effects achievedwith the two MRA compositions, MRA2 was foundto be more likely to achieve a high level of repair.Using the logistic model, the probability of repairfor each treatment is listed in Table 3. Bestoutcomes were achieved with hypotonic saliva,with 0.85 probability. The pvalue associated with Pearson’s chisquaredstatistic was 0.28, suggesting a good fit of the modeland validating the conclusions reached above.Diagnosis of the model residuals shows nounsuitability problems for the adjusted model.All teeth showed some degree of defect coverage.Fig.2 shows characteristics of enamel defect
fillings under a stereomicroscope, a confocal lasermicroscope and scanning electron microscopy(SEM). Composition MRA2 provided more regularand dense filling (Fig. 3A) than MRA1 (Fig. 3B).Observation of the agent deposited on the enameldefects revealed spherical particles (Fig. 3C) andirregular elongated shapes (Fig. 3D).
DISCUSSIONMost studies in the literature report promisingresults regarding the remineralizing capacity of theagents proposed for early management of artificialcavities9,2025. Unlike the previous studies, butfollowing similar principles, this study sought totest the repair capacity of MRA as compositionsMRA1 and MRA2 on mechanically created defects,toward the ultimate goal of creating an efficientmaterial that can be used in clinically visiblelesions.
Repairing enamel surfaces 71
Vol. 30 Nº 2 / 2017 / 68-75 ISSN 1852-4834 Acta Odontol. Latinoam. 2017
Table 1: Number of teeth according to repair level and treatment. Specimens with medium or high levels of repair.
Number of teeth according to repair level
Treatment Medium High
MRA1-IS 9 17
MRA1-HS 7 18
MRA2-IS 3 23
MRA2-HS 5 21
Total 24 79
MRA1-IS: Modified Remineralizing Agent (1,2) – isotonic salivaMRA2-HS: Modified Remineralizing Agent (1,2) – hypotonic saliva
Fig. 2: A and B show characteristics of enamel defect before and after filling with MRS under a stereomicroscope.
AOL22017:32011 29/11/2017 14:29 Página 71

72 Margarita V. Úsuga Vacca, et al.
Acta Odontol. Latinoam. 2017 ISSN 1852-4834 Vol. 30 Nº 2 / 2017 / 68-75
Fig. 3: A, MRA2: more regular and dense filling was observed. B, MRA1:irregular and no dense filling. Agent deposited on theenamel defects: C, spherical particles and D, irregular, elongated shapes.
Table 2: Statistical analysis of the model.
Variable Statistic Degrees of freedom p-value
Saliva composition (osmotic pressure) 0.0549 1 0.82
Remineralizing agent composition 43.437 1 0.04*
OP Interaction and Composition 1 0.428
OP: osmotic pressure
Table 3: Logistic Model. Probability of repair for each treatment.
Probability of repair MRA1-IS MRA1-HS MRA2-IS MRA2-HS
High repair probability 0.685 0.661 0.839 0.853
Medium repair probability 0.315 0.339 0.161 0.147
MRA1-IS: Modified Remineralizing Agent (1,2) – isotonic saliva MRA2-HS: Modified Remineralizing Agent (1,2) – hypotonicsaliva
AOL22017:32011 29/11/2017 14:29 Página 72

The agent tested in this study is composed ofconstitutive ions from enamel, mainly phosphatesand calcium, enabling it to bind chemically to theenamel substrate, based on the principle ofsecondary nucleation. Approximate particle size is515μm, determined by SEM at 500x, and particleshave irregular, elongated, spherical shapes that maycorrespond to amorphous phases or differentdegrees of crystallinity. Because ceramics are moredurable than polymers, which hydrolyze anddegrade over time, it is advantageous to use purelyceramic compositions. Additionally, because theceramics are mainly phosphocalcic, they play anactive role in remineralization with natural salivaand may simultaneously lead to remodeling of thestructure and surface porosity according to theOstwald ripening principle. Based on preliminary tests, an application time ofsix hours was established, which was the shortesttime that allowed abundant formation of adhesivedeposits within and around the defects.In 2001,Eisenburger et al. produced erosions with citric acidusing the same time period andobserved decreasedlesion depth after storage in artificial saliva andexposure to ultrasonic cleaning, suggesting thatstrong bonds were achieved between the dentalsubstrate and the applied material26. This isdesirablefor agents used for repairing the surface ofhard dental tissue. Li et al. 2008 observed a weakbond when using blocks of hydroxyapatitenanoparticles, perhaps due to differences in size anddevelopment time of the material formed comparedto those from original hydroxyapatite enamel3. Ourstudy tested whether the agent was easily removedby mechanic brushing with moderate pressureunder running tap water for five seconds, afterwhich the permanence of the material deposited onthe tooth surface was observed, particularly withinthe defects. This permanence could be explainedbased on nucleation principles, with the defect areahaving high binding energy compared to thesurfaces.Many studies have used different methods todemonstrate the repair capacity of biomimeticagents21, 24, 27, 28 such as supersaturated ionic solutionsthat favor the precipitation of calcium and phosphateions29. These solutions appear to be more efficientthan saliva itself, possibly due to the organiccomposition of saliva having an inhibitory effect oncrystal nucleation and growth30.
Immersing teeth with artificial cavities in synthetichydroxyapatite solution with a calcium/phosphateratio of 1.63 showed repair capacity not only in theenamel surface but also in the depth of the lesion,unlike the same treatment with human saliva (withor without fluoride), in which the effect was limitedto the surface31. Studies using toothpaste withhydroxyapatitecarbonated nanocrystals observedformation of a coating on the tooth enamel, withinferior crystallinity to that of the enamel butadequate capacity to repair the surface defectsdescribed20. Using natural caries lesions, Wei et al.14
tested a fluorapatite cement as a repair material fortooth enamel cavities previously acidetched with17% phosphoric acid for 30 minutes. They achieveda strong bond to the enamel with no apparent gapand the structural composition of apatite. Other studies seeking the same repair effectsachieved with mentioned agents and using ionicagents applied on superficial cracked tooth enamel,observed the formation of adhesive deposits thatcompletely or partially covered these defects, witheffectiveness that appeared to depend on themoisture used1518. Our study mixed remineralizingand conditioning agents in two different proportionsto prepare compositions MRA1 and MRA2,whichwere placed in direct contact with grooveshapedsurface defects of teeth. Both these compositionsprovided mostly high filling levels. Although nostatistically significant difference was observedbetween treatments in relation to reparativecapacity, teeth treated with composition MRA2
(50% and 50%) had the highest level of defectrepair. This could be because the agent is composedof two precursor agents in equal proportions, whichmay increase the potential of both: the fillingvolume of the restorative material and the fineness,low volume and substratebinding characteristicsof the conditioning agent, which had been pretestedas a bracketbonding material. Such combinedqualities couldalso explain why this compositionhas an aesthetically acceptable appearance, perhapsbecause the fine particles cover spaces that are leftbycompositions of larger volume. The fact that there does not appear to be asignificant effect of the aqueous medium to whichspecimens were previously subjected on therestorative capacity of MRA1 and MRA2 compo sitions in this study may indicate thatthe saliva
Repairing enamel surfaces 73
Vol. 30 Nº 2 / 2017 / 68-75 ISSN 1852-4834 Acta Odontol. Latinoam. 2017
AOL22017:32011 29/11/2017 14:29 Página 73

compositions used here might not be differentenough to establish their influence.The agent deposited on the tooth surface is chalkwhite in color and has a porous appearancecompared to tooth enamel. The white color is dueto the fact that the agents applied are colorlesscrystalline materials which produce the full rangeof visible colors due to the multiple angles at whichthey diffract light, perceived together by the eye aswhite. Its difference in color of human enamel isdue to the orientation, size and shape of the crystalsand to the fact that spaces between enamel prisms
are filled with organic material and the glass phaseof calcium phosphate crystals, which increasetranslucency, while in the repair area there areunfilled pores. Differences may also be related tothe short duration of the mineral formation processcompared to the biomineralization of hard tissues,which does not allow sufficient ripening to achievea higher degree of crystallinity. Further studiesshould consider filling pores in the restored areawith biomimetic glassy material which in additionto decreasing porosity, may improve appearanceand color.
74 Margarita V. Úsuga Vacca, et al.
Acta Odontol. Latinoam. 2017 ISSN 1852-4834 Vol. 30 Nº 2 / 2017 / 68-75
ACKNOWLEDGMENTSThis study was made possible thanks to the support of the Master’s in Dentistry Program at the School of Dentistry andCeramics Laboratory Department of Chemistry of UniversidadNacional de Colombia, Sede Bogotá. The authors would alsolike to thank Professor Luis Alberto López for statistical advice.
CORRESPONDENCEDr. Carolina Torres Rodríguez, Avenida Cra 30 # 4503, edif. 210, Of. Bogotá, [email protected]
REFERENCES1. Mihu CM, Dudea D, Melincovici C, Bocsa B. Tooth enamel,
the result of the relationship between matrix proteins andhydroxyapatite crystals. Appl Med Inform 2008;23:6872.https://ami.info.umfcluj.ro/index.php/AMI/article/view/108/75
2. Margolis HC, Beniash E, Fowler CE. Role of macromole cular assembly of enamel matrix proteins in enamelformation. J Dent Res 2006;85(9):775793.
3. Li L, Pan H, Tao J, Xu X, Mao C, Gu X, Tang R. Repair ofenamel by using hydroxyapatite nanoparticles as thebuilding blocks. J Mater Chem 2008;18:40794084.
4. Hannig M, Hanning C. Nanomaterials in preventivedentistry. Nat Nanotechnol 2010;5:565569.
5. Nicholson JW. Adhesive dental materials and theirdurability. Int J. Adhes 2000;20(1):1116.
6. Raskin A, MichotteTheall B, Vreven J, Wilson NH.Clinical evaluation of a posterior composite 10year report.J Dent 1999;27:1319.
7. Wilson NHF, MjorIA.The teaching of Class I and Class IIdirect composite restorations in European dental schools. JDent 2000;28:1521.
8. Kirkham J, Firth A, Vernals D, Boden N, et al. Selfassemblingpeptide scaffolds promote enamel remineralization. J Dent Res2007;86:426430.
9. Li H, Huang WY, Zhang YM, Zhong M. Biomimeticsynthesis of enamellike hydroxyapatite on selfassembledmonolayers. Mater Sci Eng C 2007;27:756761.
10. Fan Y, Sun Z, MoradianOldak J. Effect of fluoride on themorphology of calcium phosphate crystals grown on acidetched human enamel. Caries Res 2009;43:132136.
11. Busch S, Schwartz U, Kniep R. Morphogenesis andstructure of human teeth in relation to biomimetically growfluoapatitegelatine composites. Chem Mater 2001;13:32603271.
12. Liao YM, Feng ZD, Li SW. Preparation and characteri zation of hydroxyapatite coating on human enamel byelectrodeposition. Thin Solid Films 2008;516:61456150.
13. Onuma K, Yamagishi K, Oyane A. Nucleation andgrowth of hydroxyapatite nanocrystals for nondestructiverepair of early caries lesions. J Cryst Growth 2005;282:199207
14. Wei J, Wang J, Shan W. Lui X, et al. Development offluorapatite cement for dental enamel defects repair. JMater Sci Mater Med 2011;22:16071604.
15. Zambrano P, Herrera M, Delgado E. Comparación de lafuerza de adhesión de brackets entre dos métodos deacondicionamiento del esmalte [Tesis]. Bogotá: UniversidadNacional; 2009.
16. Flórez P, Herrera M, Delgado E. Comparación de la fuerzade adhesión de brackets cerámicos y metálicos entre dosmétodos de acondicionamiento del esmalte [Tesis]. Bogotá:Universidad Nacional; 2010.
17. Alfonso AM, Herrera M, Delgado E. Efectos de un nuevoproducto sobre daños en la superficie del esmalte causadospor la descementación de brackets metálicos [Tesis].Bogotá: Universidad Nacional; 2009.
18. Ramos L, Herrera M, Delgado E. Comparación de la super ficie del esmalte postdescementación de brackets metálicosdespués del acondicionamiento con una sustancia remine rali zante [Tesis]. Bogotá: Universidad Nacional; 2010.
19. GonzálezPita LC, RojasRamírez JS, ÚsugaVacca MV,TorresRodríguez C, et al. Protocolos diseñados para el Biobanco de Dientes de la Universidad Nacional deColombia. Acta Odontologógica Colombiana 2014; 4:7993.
20. Roveri N, Battistella E, Foltran I, Foresti E, Lafisco M,LelliM,Palazzo B, Rimondini L. Synthetic biomimeticcarbonatehydroxyapatite nanocrystals for enamel remine ra lization. Adv Mat Res 2008;4750:821824.
AOL22017:32011 29/11/2017 14:29 Página 74

21. Levine RS. Towards the chemotherapeutic treatment ofdental caries: a review. J R Soc Med 1980;73(12):876881.
22. Koulourides T, Feagin F, Pigman W. Remineralization ofdental enamel by saliva in vitro. Ann NY Acad Sci 1965;131:751757.
23. Nobre dos santos M, Rodrigues LKA, DelbelCury AA,Cury JA. In situ effect of a dentifrice with low fluorideconcentration and low pH on enamel remineralization andfluoride uptake. J Oral Sci 2007;49:147154.
24. Cochrane NJ, Saranathan S, Cai F, Cross KJ, et al Enamelsubsurface lesion remineralisation with casein phosphopeptidestabilized solutions of calcium, phosphate and fluoride. CariesRes 2008;42:8897.
25. Dong Z, Chang J, Deng Y, Joiner A. In vitro reminerali zation of acidetched human enamel with Ca3SiO5. ApplSurf Sci 2010;256:23882391.
26. Eisenburger M, Addy M, Hughes JA, Shellis RP. Effect oftime on the remineralisation of enamel by synthetic salivaafter citric acid erosion. Caries Res 2001;35:211215.
27. Arends J, Ten Bosch JJ. Demineralization and reminerali zation evaluation techniques. J Dent Res 1992;71:924928.
28. White DR, Faller RV, Bowman WD. Demineralization andremineralization evaluation techniques. Added considerations.J Dent Res 1992;71:929933.
29. Van der Reijden WA, Buijs MJ, Damen JJM, Veerman ECI, et al.Influence of polymers for use in substitute saliva on de andremineralization of enamel in vitro. Caries Res 1997;31:216223.
30. Moreno EC, Zahradnik RT. Demineralization and remine ra lization of dental enamel. J Dent Res 1979;58(2) 896903.
31. Silverstone LM. The effect of fluoride in the reminerali zation of enamel caries like lesions “in vitro”. J PublHealth Dent 1982;42:4252.
Repairing enamel surfaces 75
Vol. 30 Nº 2 / 2017 / 68-75 ISSN 1852-4834 Acta Odontol. Latinoam. 2017
AOL22017:32011 29/11/2017 14:29 Página 75

76
Acta Odontol. Latinoam. 2017 ISSN 1852-4834 Vol. 30 Nº 2 / 2017 / 76-82
RESUMO O objetivo é avaliar mudanças dento esqueléticas induzidaspelo uso do aparelho de Herbst considerando crescimentonatural através da telerradiografia cefalométrica em 45o emadultos jovens com Classe II divisão 1 e retrusão mandibular.Uma amostra de 46 indivíduos com idade entre 14 a 18 anos,após surto de crescimento pubertário, Classe II divisão 1 foramavaliados e divididos em dois grupos: grupo Experimental, 23indivíduos que foram tratados com Herbst splint metálico egrupo Controle, 23 indivíduos que foram acompanhados sem tratamento. Os grupos experimental e Controle forampareados por gênero e idade cronológica. Foram usadastelerradiografias cefalométrica em 45o dos lados esquerdo edireito da mandíbula antes do tratamento (T1) e após período
de 8 meses de tratamento e seguinte (T2) para avaliar asmudanças dento esqueléticas. Análise estatística foi realizadacom o índice de Correlação Intra Classe e teste t de Student deacordo com a hipótese do estudo. Os resultados mostraram quehouve correçãoda relação de Classe II no período de 8 mesespor movimento mesial do primeiro molar inferior. O aparelhoteve pequena influencia na estrutura mandibular e compri mento mandibular e nenhuma influência na estrutura maxilare molar superior. Em conclusão,o tratamento tardio da máoclusão de Classe II com o aparelho MESPHER foi alcançadoatravés de mudanças dento alveolares.
Palavras chave: Má oclusão de Angle Classe II; aparelhosAtivadores; ortodontia.
INTRODUCTIONThe concept of “jumping the bite” introduced byKingsley in 1880 has been widely used by cliniciansin the treatment of Angle Class II malocclusionassociated with mandibular retrusion1,2.Orthopedictreatment has improved over time, leading to betterremovable orthopedic appliances3. In 1979 a fixed
version was reinstated by Pancherz with the nameof its creator, Emil Herbst2,4.Orthopedic appliances are usually used for correctingmandibular retrusion when the patient is stillgrowing. It was formerly believed that it was notpossible to achieve orthopedic correction Class IImalocclusion with mandibular retrusion after
ABSTRACTThe aim of this study was to evaluate dental and skeletalchanges induced by the use of Herbst appliance compared tonatural growth in young adults with Class II division 1malocclusion with mandibular retrusion, by means of lateraloblique radiographs. Fortysix subjects, 14 18 years old, afterpubertal growth peak, with Class II division 1 malocclusionwere assessed. Subjects were divided into two groups: theExperimental group included 23 subjects treated with MetallicSplinted Herbst and the Control group included 23 subjectsfollowed without treatment. The Experimental and Controlgroups were paired by sex and chronological age. Obliquelateral cephalometric radiographs of the left and the right sideof the mandible before treatment (T1) and after 8 months’treatment (T2) were used to evaluate dental and skeletal
changes. Statistical analysis was performed with Intra ClassCorrelation and Student ttest, according to the studyhypothesis. The results showed that the appliance correctedthe Class II relationship in an 8month period by mesial tippingmovement of lower permanent first molars. It had littleinfluence on mandibular structure and mandibular length andno influence on maxillary structure and upper molar. Toconclude, late treatment of Class II malocclusion with theHerbst appliance was accomplished by means of dentoalveolarchanges. These findings suggest that this type of treatment canbe used in patients after growth has ceased because the resultsdo not depend upon skeletal changes.
Key words: Angle Class II Malocclusion; Orthodontic Appliances,Activator; Orthodontics.
Dental skeletal effects of the metallic splinted Herbst appliance after growth spurt: a lateral oblique cephalometric assessment
Taisa B. Raveli, Dirceu B. Raveli, Luiz G. Gandini, Ary Santos-Pinto
Universidade Estadual Paulista - UNESP, Araraquara, São Paulo, Brazil
Efeitos dentoesqueléticos do aparelho splint metálico de Herbst apóssurto de crescimento: estudo com telerradiografias em 45o
AOL22017:32011 29/11/2017 14:29 Página 76

growth had ceased5. A review of the literature showsconsensus that the best time for treatment would beimmediately after the pubertal growth spurt becauseof the short growth period remaining. This wouldmean shorter retention time and immediatepermanent intercuspation, which would preventrelapse511.There has been increasing attention to use of the Herbst appliance not only in children andadolescents, but also for late treatment, i.e. insubjects who are at the end of their growth periodor with no growth remaining5,10,1215.Most studies analyzing treatment with Herbstappliance use lateral radiographs. However,lateralto oblique radiographs offer the benefit of observingthe mandibular structure on each side separatelywith no superimpositions of bone and toothstructures16,17. The aim of this study was to evaluate changesinduced by late orthopedic treatment with Herbstappliance for Class II division 1 malocclusion withmandibular retrusion in subjects with permanentdentition who were at the end of their growth period,through the use of lateral oblique cephalometricradiography.
MATERIAL AND METHODSThis retrospective study was reviewed andapproved by the Ethics Committee under number39799514.3.0000.5416. The sample consisted of 46patients who had Class II division 1 malocclusionwith mandibular retrusion. Twentythree consecutivepatients (13 male and 10 female, mean age 15.6
years) were treated with a Metallic Splinted Herbst(MESPHER) appliance and assigned to theExperimental group.Another twentythree patientswithout treatment were selected from BurlingtonGrowth Centre archives and paired with the treatedgroup by gender, age and malocclusion, and usedas the Control group.Inclusion criteria were bilateral Class II molarrelationship; overjet greater than 5 mm andcomplete permanent dentition, except third molars.Exclusion criteria were patients with syndromes orextreme vertical growth pattern. Facial analysisconsisting of convex profile, straight nasolabialangle, short mentocervical line and occlusalcharacteristics consisting of molar and canines inClass II (more than half cusp) and large overjet wereused to determine that the subjects had skeletalClass II division 1 malocclusion. Subjects in the Experimental group used MetallicSplinted Herbst (MESPHER) appliance (Fig.1)foreight months (mean 8.50 ± 0.70 months) with onestep mandibular advancement to an incisor edgetoedge relationship. The telescopic mechanismused was the FlipLock Herbst
®(TP Orthodontics,
Inc.) model. The upper anchorage was a metallicsplint structure in which upper bicuspids and molarswere held together and united by a transpalatalwelded bar (Fig. 1A). The lower anchorage was ametallic splint structure in which lower bicuspidsand molars were held together and united by alingual welded bar (Fig. 1B).Lateraloblique cephalometric radiographs of bothsides of the mandible before treatment (T1) and after
An oblique assessment for Herbst appliance 77
Vol. 30 Nº 2 / 2017 / 76-82 ISSN 1852-4834 Acta Odontol. Latinoam. 2017
Fig. 1: Upper (1A) and lower (1B) metallic splint built as part of the anchorage system of the metallic splinted Herbst appliance(MESPHER).
AOL22017:32011 29/11/2017 14:29 Página 77

treatment (T2) were used to evaluate dental skeletalchanges induced by MESPHER. Radiographs weretaken with a Rotograph Plus MR05 device with 10%magnification. In the Control group, the sameradiographs of both sides of the mandible of untreatedpatients were used to evaluate dental skeletal changesdue to natural growth development at the same meanages as subjects in the Experimental group. Theradiographs were taken using a Kelet radiographicdevice with 9.84% magnification.Data from theControl and Experimental groups were adjusted tomatch the mean treatment time.Skeletal age was verified in carpal radiographs byone investigator (T.B.R.), following Greulich andPyle18, and indicated that patients were in the finalpubertal growth phase.Radiographs were digitized with Numonics AccuGrid table and the data were obtained using thesoftware Dentofacial Planner Plus 2.01. Measure ments were randomly reevaluated after two weeksby the same examiner and the error of the methodwas evaluated using Interclass CorrelationCoefficient (ICC).Cephalometric analysis consistedof 16 points marked on right and left lateral oblique
radiographs of the mandible. A Cartesian coordinatesystem was used where theXaxis was defined asthe horizontal line represented by the orbital planedetermined in the initial radiograph (T1) andtransferred to the subsequent radiograph throughsuperimposition of the cranial stable structures19.The Yaxis was defined as the vertical lineperpendicular to the orbital plane registered in aposterior fiducial point.The distance of a perpendicular projection ofselected dental and skeletal points in the T1 and T2superimposed radiographs to the XAxis and YAxis was measured to obtain horizontal and verticaldental and skeletal changes, respectively (Fig. 2),in both groups.
Statistical AnalysisThe following analyses were used to assess the studyhypothesis: 1. Interclass Correlation Coefficientevaluate measuring method reproducibility; 2.Student ttest test mean equality between twoindependent populations, to test the hypothesis thata population’s mean is equal to zero for each groupseparately and to test mean equality of twopopulations with independent samples; 3. Student ttest for mean equality of two populations withindependent sample preceded by Levene test forvariance equality. When Levene test showeddifferent variances, Student ttest was correctedaccordingly.
RESULTSThe effects of treatment (Experimental group)compared to natural growth (Control group) showedskeletal and dental changes. Analysis of thehorizontal and vertical mandibular changes on eachside (Tables 1 and 2) showed that variables related togonium (Go), mentonium (Me), mandibular length(Md length), horizontal length (Mdhor length),mandibular height (Md height) and mandibular angle(Md angle) underwent some small changes. Changesin the same variable differed on the right and left sideof the mandible. Only the condyle (Co) presented nosignificant change. Maxilla showed no significanthorizontal or vertical change regarding the pointsPNS and ANS (Table 1).Regarding dental movements (Table 1), there were nosignificant horizontal and vertical changes for UpperFirst Permanent Molar, either for crown (UMC) orapex (UMA). However, Lower First Permanent Molar
78 Taisa B. Raveli, et al.
Acta Odontol. Latinoam. 2017 ISSN 1852-4834 Vol. 30 Nº 2 / 2017 / 76-82
Fig. 2: Points projected on the Xaxis (for horizontal changes)and Yaxis (for vertical changes). The displacement betweenprojected points was measured. Examples for mandibularchanges (1 and 2), maxillary changes (3), dental changes (4).Md length (linear distance between Condilium andMentonium), Mdheight (linear distance between Condiliumand Gonium), Md horizontal length (linear distance betweenGonium e Mentonium), Md Angle (angle formed byintersection of the lines CoGo and GoMe).
AOL22017:32011 29/11/2017 14:29 Página 78

An oblique assessment for Herbst appliance 79
Vol. 30 Nº 2 / 2017 / 76-82 ISSN 1852-4834 Acta Odontol. Latinoam. 2017
Table 1: Measurement changes over 8 months in treated and control groups. Mean difference and standard error (SE) .
Horizontal Vertical
Variable side Control Experimental difference Control Experimental difference
Co R 1.70(1.4) 0.79(1.7) 0.91(0.5) ns 0.33(1.8) 0.54(1.3) 0.21(0.5) ns
L 1.39(1.1) 2.15(1.9) 0.76(0.5) ns 0.35(1.3) 1.43(2.7) 1.09(0.6) ns
Go R 1.35(1.8) 0.73(1.7) 0.62(0.5) ns 1.32(1.7) 0.13(1.5) 1.45(0.5) **
L 1.61(1.4) 0.53(1.5) 1.08(0.4) * 0.07(1.3) 0.45(1.5) 0.38(0.4) ns
Me R 0.24(0.7) 0.20(0.8) 0.04(0.2) ns 0.14(0.8) 0.38(0.8) 0.53(0.2) *
L 0.05(0.6) 0.09(0.6) 0.14(0.2) ns 0.34(0.6) 0.09(0.8) 0.25(0.2) ns
ANS R 0.15(2.6) 0.43(2.7) 0.57(0.8) ns 0.67(2.2) 0.24(3.3) 0.43(0.8) ns
L 0.36(2.2) 1.05(2.5) 0.69(0.7) ns 0.74(1.7) 0.63(3.5) 1.37(0.8) ns
PNS R 0.58(3.2) 1.29(4.3) 1.87(1.1) ns 0.15(2.6) 0.43(2.7) 0.57(0.8) ns
L 0.66(3.6) 0.98(4.9) 0.33(0.3) ns 0.36(2.2) 1.05(2.5) 0.69(0.7) ns
UMC R 0.34(3.7) 0.47(3.8) 0.13(1.1) ns 1.12(1.8) 0.89(1.6) 0.23(0.5) ns
L 0.43(2.3) 1.91(4.2) 1.48(1.0) ns 0.87(1.0) 0.04(1.9) 0.91(0.4) ns
UMA R 0.30(2.7) 0.97(2.6) 1.27(0.8) ns 1.07(1.7) 0.98(1.5) 0.09(0.5) ns
L 0.62(2.0) 0.85(3.7) 0.23(0.9) ns 0.89(1.0) 0.10(1.8) 0.79(0.4) ns
LMC R 0.32(0.9) 1.61(2.3) 1.93(0.5) *** 0.08(1.5) 0.20(1.8) 0.27(0.5) ns
L 0.28(1.0) 1.35(0.8) 1.63(0.3) *** 0.29(1.4) 0.00(1.6) 0.29(0.4) ns
LMA R 0.24(1.1) 0.57(0.2) 0.33(0.5) ns 0.12(2.6) 0.13(4.3) 0.02(1.0) ***
L 0.10(1.0) 0.19(1.3) 0.29(0.3) ns 0.66(1.7) 0.12(4.6) 0.78(1.0) ns
Student T Test:*** significant p< 0.001 ; ** significant p< 0.01 ; * significant p< 0.05 ; ns = not significantCo (Condilium); Go (Gonium); Me (Mentoniano); ANS (anterior nasal spine); PNS (posterior nasal spine); UMC (upper molar cuspid)UMA (upper molar appex); LMC (lower molar cuspid); LMA (lower molar appex)
Table 2: Mean and standard deviation of measurement changes over 8 months in treated and control groups. Mean difference and standard error (SE).
Variable side Control Experimental difference
Md length R 1.75(1.8) 0.78(2.2) 0.97(0.6) ns
L 1.08(1.7) 2.32(2.4) 1.23(0.6) *
Md height R 1.69(2.0) 0.41(2.0) 1.27(0.6) *
L 0.47(1.7) 2.15(3.0) 1.68(0.7) *
Md hor length R 1.14(2.0) 0.77(1.5) 0.38(0.5) ns
L 1.47(1.8) 0.23(1.5) 1.23(0.5) *
Md angle R 0.96(2.2) 0.39(2.4) 0.57(0.7) ns
L 0.95(1.4) 0.69(1.9) 1.64(0.5) **
Incl molar inf R 0.95(6.3) 3.494.6) 4.44(1.6) **
L 0.63(3.4) 4.81(3.5) 5.44(1.0) ***
Student T test: *** significant p <0.001 ; ** significant p< 0.01 ; * significant p< 0.05 ; ns = not significant
Md Length (mandibular length); Md height (mandibular heigth); md hor length (mandibular horizontal length)md angle (mandibular angle); incl molar inf (inclination of lower permanent molar)
AOL22017:32011 29/11/2017 14:29 Página 79

had a very significant horizontal change in crown(LMC) in mesial direction and showed no apexchanges (LMA), leading to a significant increase in itsinclination (Incl Molar Inf)as a result of the treatment(Tables 1 and 2). Additionally, there is statisticalevidence that a vertical change occurred on the rightside for Lower First Permanent Molar apex (LMA) butnot on the left side.
DISCUSSIONThis lateral oblique cephalometric study evaluateddental skeletal alterationsin subjects withClass IIdivision 1 with mandibular retrusion who weretreated with a metallic splinted Herbst appliance.Fortysix patients with mean age 15.6 years wereanalyzed and divided into treatment and controlgroups. Although there is an understanding that thiskind of treatment would be more appropriate duringthe pubertal growth peak7,8,2024, some studies haveshown that treatment through mandibular advance ment can be accomplished after this phase5,6,9,1115,25.The condyle region presented no significant verticaland horizontal changes after treatment on eitherside (right or left) in this sample of young adultpatients. In contrast, most studies with Herbstappliance using lateral cephalometric radiographsreport different results. In a systematic review,Cozzaet al.8 showed that supplementary condylargrowth is considerably higher when orthopedictreatment is performed during adolescence.Pancherz3observed horizontal condylar growth butno vertical change in the treatment group. Ruf andPancherz5examined two treatment groups with ages12 and 16 years, and observed condylar changes inboth groups; however, this change remained onlyin the 16yearold group after appliance removal.Subsequently, the same authors10reported thatpatients treated 1 or 2 years after pubertal growthpeak showed more horizontal condylar growth.Lateral oblique cephalometry allowsmore preciseanalysis of each side of the maxillamandibularstructures and dental components without thedisadvantage of superimposition.Mandible remodeling could be expected as an effectof the treatment. The gonium region showed some horizontal (left side) and vertical (right side)changes.In contrast, Hägglund, Segerdal andForsberg21 (2008) observed in 14yearold boys nodifference in mandibular angle after treatment.Inagreement withour results, Pancherz3 reported some
resorption of the posterior part of the mandibularbody that coincides with the gonial region and alsoobserved that the gonial angle opened in patientssubmitted to Herbst treatment and closed in thecontrol group. The symphysis region showed aslight vertical change on the right side. This regionwas used as a superimposition structure in this studybecause it was considered to be a stableregion3,15,and was not expected to change over the 8monthperiod of observation. As result of this remodeling,the mandibular angle increased on the left side.Rufand Pancherz11 reported similar results, observingan increase in mandibular angle during treatment inindividuals with ages raging from 15 to 44 years,although tit subsequently decreased slightly afterappliance removal. Nevertheless different responsesin mandibular structure were not enough to produceasymmetry in the final outcome. Considering effective mandibular length (Md length),a slight difference occurred on the left side. In asystematic review22, it was reported that some studiesfoundan increase in mandibular length whereas othersreported no change. Similarly, FloresMir et al.23,concluded that mandibular length increased in the studies analyzed. Hägglund, Segerdal andForsberg21found no skeletal change betweentreatment and control groups in a study on 14yearold boys. Likewise, Konik, Pancherz and Hansen9
reported no mandibular increase in a treatment groupafter pubertal growth peak. However, Pancherz3foundan increase in mandibular length three times higherin the treatment group than in the control group.Subsequently, Ruf and Pancherz5 reported lessmandibular increase and more dental movement in16yearold subjects. In 2003, the same authors10
reported an increase in mandibular length in patientstreated 1 or 2 years after the pubertal growth peak.This inconsistency was explained by the fact thatdifferent measure ments were used in each study. Mandibular horizontal length has not been widelydiscussed and has only been evaluated byPancherz3, who observed a decreasein the length ofmandibular corpus after treatment. This is inagreement with our results, which showed asmallchange in the gonium on the left side as part of themandible remodeling process.Mandibular height changed significantly in thevertical direction on both sides of the mandible. In agreement with this result, the systematic review by FloresMir et al.23found an increase in
80 Taisa B. Raveli, et al.
Acta Odontol. Latinoam. 2017 ISSN 1852-4834 Vol. 30 Nº 2 / 2017 / 76-82
AOL22017:32011 29/11/2017 14:29 Página 80

mandibular height in the studies analyzed.Pancherz3 also reported that in a retention periodafter 7 years of appliance removal, treated patientspresented increased mandibular height while thecontrol group did not.Horizontal and verticalgonium remodeling must have contributed to thisheight change, considering that the condyle did notundergo any modification.Information in the literature on maxillary bone onlyreports that there was restriction of its displacement asthe effect of treatment. Only Pancherz3reportedmaxillary restriction during treatment. Our resultsshow that the anterior and posterior nasal spine hadthe same pattern of horizontal and vertical movementsas in the control group, indicating that the treatmentdid not change the natural displacement of the maxilla,in agreement with other studies9,11,21,22. The stability ofthe maxillary position may be attributed to the metallicsplint utilized as anchorage. Dental movement appeared to be more marked.High significance was observed on both sides onlower permanent first molar for crown and nosignificance whatsoever for apex in horizontalassessment. It is understood that mesial inclinationoccurred, also confirmed by a measurement thatshowed great significance for axial movement.Barnett et al.22 also observed extrusion and mesialmovement of lower first permanent molars. Moststudies with Herbst appliance on subjects of thesame age agree with these results3,5,22,23, confirmingthat Class II is corrected mostly by dentalmovement. With regard to vertical assessment,significance was low for the apex region on the rightside. It is understood that extrusion might haveoccurred. This difference between sides in our studyis less than 1mm, being slightly greater on right sidethan on the left side in absolute values.This small
sample difference between sides is what causes thisapparent contradiction in the results.Upper first permanent molars, on the other hand,showed no change, indicating positional stabilitywhich could be attributed to the metallic splint used as anchorage. This result contrasts with theliterature, which reports intrusion22 and distalmovement3,23of the upper molar in conventionalHerbst anchorage.Overall, studies seem to be positive in relation tolate treatment for Class II with mandibularretrusion. A recent study7 concluded that treatmentof this kind of malocclusion with the Herbstappliance is equally efficient in adolescents andadults, opening a new option even for borderlinepatients, because most results for late treatment aremore dental than skeletal3,24. To paraphrasePancherz3, the Herbst appliance improves mandi bular positioning in the long term, but does notnormalize it. Dental sagittal relation, on the otherhand, is practically normalized. Therefore, in thelong term, dental effects compensate an unfavorablemandibular relation. It can be concluded from this study that the treatmentof Class II with mandibular advancement usingmetallic splinted Herbst showed small skeletalinfluence on the mandible in 14 to 18yearolds.Dental effects where more significant for thecorrection of Class II, emphasizing the correction bylower first molar tipping to mesial direction. There isevidence that the mandible responds differently oneach side when undergoing an 8month mandibularadvancement treatment. Nevertheless, this differen tial response is not marked enough to produce anasymmetric final outcome or compensate some smalldifferences between sides due to asymmetricfunctional masticatory balance.
An oblique assessment for Herbst appliance 81
Vol. 30 Nº 2 / 2017 / 76-82 ISSN 1852-4834 Acta Odontol. Latinoam. 2017
CORRESPONDENCEDr. Taisa RaveliAvenida Portugal, 887 – CentroCEP 14.801075 AraraquaraSP [email protected]
REFERENCES1. Angle EH. Classification of malocclusion.Dental Cosmos
1899; 41: 248264. https://quod.lib.umich.edu/d/dencos/acf8385.0041.001/266:56?rgn=main;view=image
2. Pancherz H. History, background and development of theHerbst appliance. Semin Orthod 2003; 9: 311.
3. Pancherz H. The effects, limitations and longtermdentofacial adaptations to treatment with the Herbstappliance.Semin Orthod 1997; 3: 232243.
4. Pancherz H. Treatment of Class II malocclusions by jumpingde bite with the Herbst appliance.A cephalometric investigation.Am J Orthod Dentofacial Orthop 1979; 76: 424442.
AOL22017:32011 29/11/2017 14:29 Página 81

5. Ruf S, Pancherz H. Dentoskeletal effects and facial profilechanges in young adults treated with the Herbst appliance.Angle Orthod 1999; 69: 239246.
6. Bock NC, Bremen J, Ruf S. Occlusal stability of adult ClassII Division 1treatment with the Herbst appliance. Am JOrthod Dentofacial Orthop 2010; 138: 146151.
7. von Bremen J, Bock N, Ruf S. Is Herbstmultibracketappliance treatment more efficient in adolescents than inadults?.Angle Orthod 2009; 79: 173177.
8. Cozza P, Baccetti T, Franchi L, Toffol L et al. Mandibularchanges produced by functional appliances in Class IImalocclusion: A systematic review. Am J OrthodDentofacial Orthop 2006; 129: 599.e 5991.e12.
9. Konik M, Pancherz H, Hansen K. The mechanism of ClassII correction in the late Herbst treatment. Am J OrthodDentofacial Orthop 1997; 112: 8791.
10. Ruf S, Pancherz H. When is the ideal period for the Herbsttherapyearly or late? Semin Orthod 2003; 9: 4756.
11. Jakobsone G, Latkauskiene D, McNamara Jr J. Mechanismsof Class II correction induced by the crown Herbstappliance as a singlephase Class II therapy: 1 year followup. Prog Orthod 2013, 14:27.
12. Pancherz H, Bjerklin K, Hashemi K. Herbst therapy: A 32year longitudinal followup study. Am J Orthod DentofacialOrthop 2015; 147:1928.
13. Pancherz H, Bjerklin K, LindskogStokland B, Hansen K.Thirtytwoyear followup study of Herbst therapy: Abiometric dental cast analysis. Am J Orthod DentofacialOrthop 2014; 145:1527.
14. Yang X, Zhu Y, Long H, Zhou Yet al. The effectiveness ofthe Herbst appliance for patients with Class IImalocclusion: a metaanalysis. Eur J Orthod 2015, 110.
15. Ruf S, Pancherz H. Herbst/multibracket appliancetreatment of Class II division 1malocclusions in early andlate adulthood. A prospectivecephalometric study ofconsecutively treated subjects. Eur J Orthod.2006; 28:352360.
16. Cartwright LJ, Harvold E. Improved radiographic resultsin cephalometry through the use of high kilovoltage. J CanDent Assoc 1954; 20: 261263.
17. Posen AL. Vertical height of the body of the mandible andthe occlusal level of the teeth in individuals with cleft andnoncleft palates. J Can Dent Assoc 1958; 1: 211218.
18. Greulich WW, Pyle SI. Radiographic atlas of skeletaldevelopment of the hand and wrist. California: StanfordUniversity Press; 1959.
19. Sakima MT, Sakima CG, Melsen B. The validity ofsuperimposing oblique cephalometric radiographs to assesstooth movement: an implant study. Am J OrthodDentofacial Orthop 2004; 126: 344353.
20. Franchi L, Baccetti T, McNamara Jr JA. Treatment andposttreatment effects of acrylic splint Herbst appliance therapy.Am J Orthod Dentofacial Orthop 1999; 115: 429438.
21. Hagg U, Pancherz H. Dentofacialorthopaedics in relation tochronological age, growth period and skeletal development.An analysis of 72 male patients with Class II division 1malocclusion treated with the Herbst appliance. Europ JOrthod 1988;10:169176.
22. Pancherz H. The effect of continuous bite jumping on thedentofacial complex: a followup study after Herbst appliancetreatment of Class II malocclusions. Europ J Orthod 1981; 3:4960.
23. Pancherz H, Hagg U. Dentofacial orthopedics in relation tosomatic maturation. An analysis of 70 consecutive casestreated with the Herbst appliance. Am J Orthod DentofacialOrthop 1985; 88: 273287.
24. Pancherz H, Hensen K. Occlusal changes during and afterHerbst treatment: a cephalometric investigation. Europ JOrthod 1986; 8: 215228.
25. Hägglund P, Segerdal S, Forsberg CM. The integratedHerbst appliance treatment effects in a group of adolescentmales with Class II malocclusions compared with growthchanges in an untreated control group. Europ J Orthod2008; 30: 120127.
82 Taisa B. Raveli, et al.
Acta Odontol. Latinoam. 2017 ISSN 1852-4834 Vol. 30 Nº 2 / 2017 / 76-82
AOL22017:32011 29/11/2017 14:29 Página 82

RESUMENEl edentulismo se ha asociado con una gran variedad decondiciones en los adultos mayores afectando el estado generalde su salud. Por lo tanto, afecta la calidad de vida de lapersona y su relación con el medio ambiente. Por otro lado, laautoevaluación de la salud ha demostrado ser un marcadorpreciso del estado general de la salud. Sin embargo, hay escasainformación sobre cómo estas dos condiciones se relacionanentre sí en adultos mayores de origen hispano.El objetivo de este estudio fue evaluar el impacto deledentulismo en la autoevaluación de la salud en adultosmayores.Se analizaron los datos de SABE Ecuador 2009, un estudiotransversal que incluyó una muestra probabilística yrepresentativa de 5.235 personas de 60 años de edad o más.La variable dependiente fue la salud autoevaluada yedentulismo fue la variable independiente, teniendo edad, sexoy comorbilidades como variables de confusión. Con el fin de
probar la asociación independiente de edentulismo con la autoevaluación de la salud un modelo de regresión logística seajustó.De la muestra entera, un 77,13% de los adultos mayoresreportaron tener salud autoevaluada regular / pobre. Seencontró una asociación independiente entre edentulismo ysalud autoevaluada con un riesgo incremental dependiendodel número de dientes ausentes de OR 1,35 (IC 95% 0,75 2,43)p 0,32, en adultos mayores con menos de 4 dientes ausenteshasta OR 1,88 (1,06 3,32) p 0,029, con más de la mitad dedientes ausentes.La salud oral se ha considerado de forma independiente delresto del cuerpo y la mente, es claro por nuestros resultadosque la salud oral es un componente muy importante del estadode salud global en las personas mayores.
Palabras clave: Salud oral, edentulismo, estado de salud,cuidado dental , envejecimiento.
ABSTRACTEdentulism is related to a number of conditions in older adults,impacting their overall health status and thus their quality oflife and relationship with the environment. At the same time,selfrated health has been shown to be an accurate marker ofoverall health status. However there is little information onhow edentulism relates to selfrated health in older adults ofHispanic origin. The aim of this study was to evaluate the impact of edentulismon selfrated health in older adults.We analyzed data from SABE Ecuador 2009, a crosssectionalstudy that included a probabilistic representative sample of5,235 communitydwelling older adults aged 60 years or older.The dependent variable was selfrated health and theindependent variable was edentulism, with age, sex andcomorbidities as confounding variables.In order to test the
independent association of edentulism with selfrated health, alogistic regression model was fitted.Out of the whole sample,77.13% of older adults reportedhaving fair/poor selfrated health. We found an independentassociation between edentulism and selfrated health withincremental risk according to number of missingteeth,rangingfrom OR 1.35 (CI 95% 0.75 2.43) p 0.32 for less than 4missing teeth to OR 1.88(1.06 3.32) p 0.029 for more thanhalf of teeth missing.Even though oral health has long been considered separatelyfrom the rest of the body and mind, it is clear from our resultsthat oral health is a very important component of global healthstatus in the elderly.
Keywords: Oral health, edentulous, health status, dental care,aging.
83
Vol. 30 Nº 2 / 2017 / 83-89 ISSN 1852-4834 Acta Odontol. Latinoam. 2017
Edentulism and its relationship with self-rated health: secondary analysis of the SABE Ecuador 2009 Study
Miguel Germán Borda1,2,3, Nicolás Castellanos-Perilla1,JudyAndrea Patiño2, Sandra Castelblanco2, Carlos Alberto Cano1,2,3, Diego Chavarro-Carvajal1,2,3,Mario U Pérez-Zepeda1, 4
1 Semillero de Neurociencias y Envejecimiento, Facultad de Medicina, Pontificia Universidad Javeriana, Bogotá, Colombia
2 Unidad de Geriatría, Hospital Universitario San Ignacio, Bogotá, Colombia3 Instituto de Envejecimiento, Pontificia Universidad Javeriana, Bogotá, Colombia4 Departamento de Investigación en Epidemiología Geriátrica,
Instituto Nacional de Geriatría, Ciudad de México, México.
Relación del edentulismo con la autoevaluación del estado de la salud: un análisis secundario del estudio SABE Ecuador 2009
AOL22017:32011 29/11/2017 14:29 Página 83

INTRODUCTION Oral health is an indicator of general healthcondition in older adults1. It is estimated that olderage brings a higher risk of losing teeth2, which leadsto nutritional alterations, swallowing disorders,variations in language modulation, low selfesteem,poor performance of the individual in society,infections,and changes in physical and mental state.In short, it affects theperson’s quality of life (QOL)and relationship with the environment25.Edentulism is defined as partial or total nontraumaticloss of teeth6, usually due to infectious pathologies(e.g.dental caries, parotitis and periodontal disease)chronic exposure to toxic substances, smoking, medi cations (e.g. antihistamines, diuretics, antipsychoticsand antidepressants), metabolic factors (e.g. malnu trition, Paget’s bone disease or osteoporosis withmaxillary involvement) and anatomical/functionalalterations such as bruxism7. However, asedentulismcommonly occurs in older adults, it has multifactorialetiology.Progressive loss of teeth has been considered partof normal aging because of the high prevalence oftooth loss in older adults3,8. However, this idea isinaccurate and several studies have related toothloss to etiological factors such as chronic disease,rural residence, functional dependence, neuro cognitive disorder, low educational level, poverty,poor access to health services, limited access tocultural property and inadequate hygiene habits. Inother words, losing teeth is not a part of aging but aconsequence of negative conditions existing sincechildhood, a time when it is important to establishoral health strategies that should continuethroughout life911.Edentulism has been documentedand found to exert significant effect on individualperformance, functionality and wellbeing4,12,13. Selfrated health (SRH) is the summary of allavailable information oncurrent health statusincluding clinical, mental and social characteristics,according to the patient’s circumstances. In recentyears, SRH has become an important research targetas it is a useful marker for a comprehensiveapproach to the geriatric patient14,15.Positive correlations have been found betweenobjective and subjective health assessments amongolder adults, mostly in those with disability,16
chronic diseases17 or depression18,19. Although there are studies on the impact of oralhealth on SRH in the elderly, the current study goes
further and looks at the impact of edentulism ontheir subjective assessment of their health. The aimof this study was to evaluate the impact ofedentulism on SRH in the elderly, in a secondaryanalysis of the SABE Ecuador study.
MATERIALS AND METHODS We analyzed data from the SABE (Salud, Bienestary Envejecimiento) Study conducted between Juneand August 2009in Ecuador. SABE was a crosssectional study that included 5,235 subjects aged60 years or more living in rural and urban areas ofEcuador (except Amazon and Galápagos). It wasconducted by theInstituto Nacional de Estadistica yCensos (INEC), Department of SociodemographicStatistics. Funding was provided by the Ministry ofSocial and Economic Inclusion of Ecuador. TheUniversity of San Francisco de Quito, the NationalInstitute of Statistics and Census, the Ministry ofPublic Health, and the Society of Geriatricsimplemented and supported the study.The instrument used in the SABE Ecuador study wasderived from the international instrument designedfor the original SABE study conducted in 5 LatinAmerican capital cities20. Probabilistic sampling byclusters (housing segments) and block stratificationrepresented 15 continental provinces, according tothe Costa and Sierra Regions, urban and rural areas,Quito and Guayaquil. The sample included 10,368households: 5,100 in the Sierra Region and 5,268 inthe Costa Region, including 864 sectors altogether.Of the sample, 85.8% corresponded to subjects withcomplete data, who were included for analysis21,22.Field staff was carefully selected and trained togather highquality data.The instruments (handbookand form) and the cartography used were managedefficiently.Inter and intraobserver reliability testswere performed, as well as testretest using simplecorrelations.The survey included questions onsociodemographic characteristics (age, sex,education, social support, work/income history),cognitive status, health(cognitive and physicalfunction status, number of medications, services),social networkand family support, work and incomehistory, housing conditions, physical performanceand exposure to violence and abuse.SRHwas evaluated by the question “Do you consideryour health status to be excellent, very good, good, fairand poor?” Answers were subsequently dichotomizedinto good (very good & good) and bad (fair & poor).
84 Miguel Germán Borda, et al.
Acta Odontol. Latinoam. 2017 ISSN 1852-4834 Vol. 30 Nº 2 / 2017 / 83-89
AOL22017:32011 29/11/2017 14:29 Página 84

Edentulism was used as the independent variable.It was defined as absence of teeth (total or onetooth) and evaluated by the question: “Now, I wouldlike to ask some questions about your mouth andyour teeth. Please tell me whether any of your teethare missing using the following response options:No I have all my teeth; Yes a few (up to four); Yesquite a few (more than four but less than half); Yesmost of them (more than half) or Yes all missing.Age was classified as 6069, 7079 and ≥80. Depression was evaluated on the Yesavage Scalefor screening depression in older adults, wherescores 05 indicate normal and 615 indicatedepression23,24.Medical conditions were assessed by askingparticipants whether they had been diagnosed by aphysician with diabetes mellitus (DM), chronicobstructive pulmonary disease (COPD) or arthritis.Pain was evaluated with the question: “Do you haveany pain in your back?”, “Do you ever haveheadache?”, ”Do you feel any pain in your joints?”25.For the analysis, answers were dichotomized (Yes/No).Initially, we used univariate analyses to exploreextreme values and a normal distribution to adjustand categorize variables. For descriptive statistics,categorical variables are presented using frequencies(absolute and relative), while means and standarddeviations (SD) are used for continuous variables.
Bivariate analysis was applied subsequently tocontrast SRH differences between groups. Chisquare tests were used for categorical variables andttests for continuous variables. Finally, multivariateanalysis logistic regression models were fitted inorder to obtain the odds ratio (OR) with 95%confidence intervals(95% CI). Estimates arepresented before and after adjustment by sex, ageand depression. Statistical level of significance wasset at p <0.05. Data were analyzed employingSTATA 12®.This study was approved by the Ethics andScientific Committee of the Ageing Institute atHospital Universitario San Ignacio and by theEthics Committee of the Pontificia UniversidadXaveriana. It was conducted in accordance with theethical standards set forth in the 1964 Declarationof Helsinki and its amendments. Details that mightdisclose the identity of the subjects under studyhave been omitted.
RESULTSOut of the total sample, 77.13% older adultsreported having poor/fair SRH (80.59% of womenand 73.26% of men). For edentulism, the higher thefrequency of poor/fair SRH, the higher the numberof missing teeth. Prevalence of poor/fair SRH was62.30% in persons who had complete dentures,
Edentulism and SRH in the older adult 85
Vol. 30 Nº 2 / 2017 / 83-89 ISSN 1852-4834 Acta Odontol. Latinoam. 2017
Fig. 1: Percentage of poor selfrated health status according to number of teeth present.
AOL22017:32011 29/11/2017 14:29 Página 85
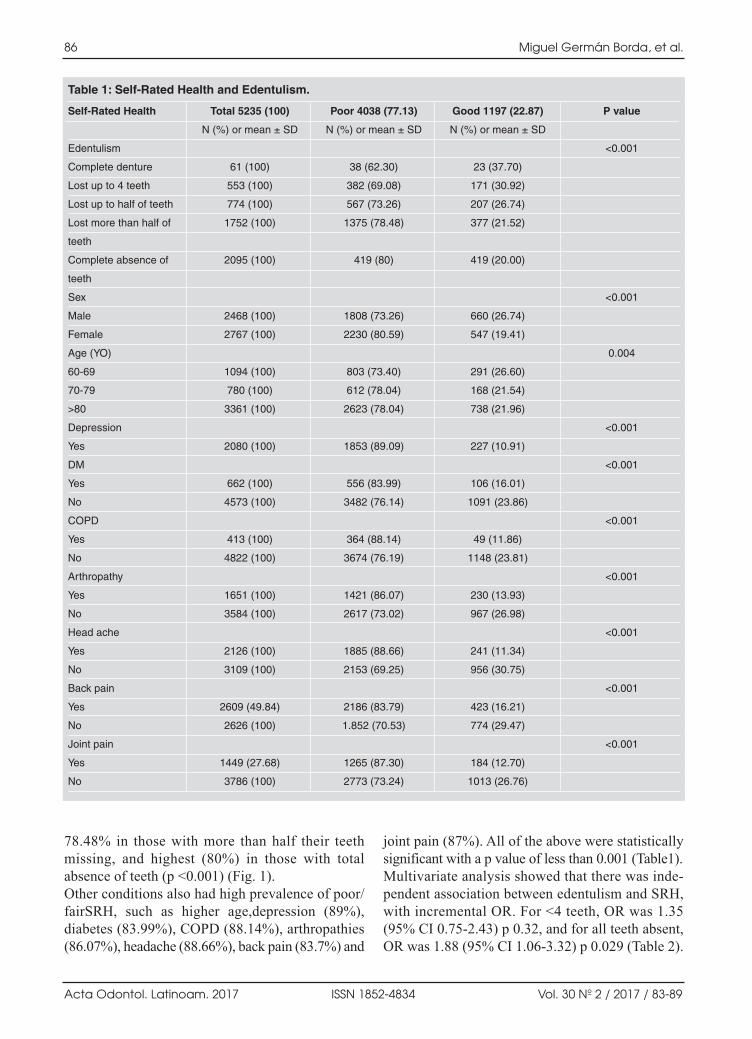
78.48% in those with more than half their teethmissing, and highest (80%) in those with totalabsence of teeth (p <0.001) (Fig. 1).Other conditions also had high prevalence of poor/fairSRH, such as higher age,depression (89%),diabetes (83.99%), COPD (88.14%), arthropathies(86.07%), headache (88.66%), back pain (83.7%) and
joint pain (87%). All of the above were statisticallysignificant with a p value of less than 0.001 (Table1). Multivariate analysis showed that there was inde pendent association between edentulism and SRH,with incremental OR. For <4 teeth, OR was 1.35(95% CI 0.752.43) p 0.32, and for all teeth absent,OR was 1.88 (95% CI 1.063.32) p 0.029 (Table 2).
86 Miguel Germán Borda, et al.
Acta Odontol. Latinoam. 2017 ISSN 1852-4834 Vol. 30 Nº 2 / 2017 / 83-89
Table 1: Self-Rated Health and Edentulism.
Self-Rated Health
Edentulism
Complete denture
Lost up to 4 teeth
Lost up to half of teeth
Lost more than half of
teeth
Complete absence of
teeth
Sex
Male
Female
Age (YO)
60-69
70-79
>80
Depression
Yes
DM
Yes
No
COPD
Yes
No
Arthropathy
Yes
No
Head ache
Yes
No
Back pain
Yes
No
Joint pain
Yes
No
Total 5235 (100)
N (%) or mean ± SD
61 (100)
553 (100)
774 (100)
1752 (100)
2095 (100)
2468 (100)
2767 (100)
1094 (100)
780 (100)
3361 (100)
2080 (100)
662 (100)
4573 (100)
413 (100)
4822 (100)
1651 (100)
3584 (100)
2126 (100)
3109 (100)
2609 (49.84)
2626 (100)
1449 (27.68)
3786 (100)
Poor 4038 (77.13)
N (%) or mean ± SD
38 (62.30)
382 (69.08)
567 (73.26)
1375 (78.48)
419 (80)
1808 (73.26)
2230 (80.59)
803 (73.40)
612 (78.04)
2623 (78.04)
1853 (89.09)
556 (83.99)
3482 (76.14)
364 (88.14)
3674 (76.19)
1421 (86.07)
2617 (73.02)
1885 (88.66)
2153 (69.25)
2186 (83.79)
1.852 (70.53)
1265 (87.30)
2773 (73.24)
Good 1197 (22.87)
N (%) or mean ± SD
23 (37.70)
171 (30.92)
207 (26.74)
377 (21.52)
419 (20.00)
660 (26.74)
547 (19.41)
291 (26.60)
168 (21.54)
738 (21.96)
227 (10.91)
106 (16.01)
1091 (23.86)
49 (11.86)
1148 (23.81)
230 (13.93)
967 (26.98)
241 (11.34)
956 (30.75)
423 (16.21)
774 (29.47)
184 (12.70)
1013 (26.76)
P value
<0.001
<0.001
0.004
<0.001
<0.001
<0.001
<0.001
<0.001
<0.001
<0.001
AOL22017:32011 29/11/2017 14:29 Página 86
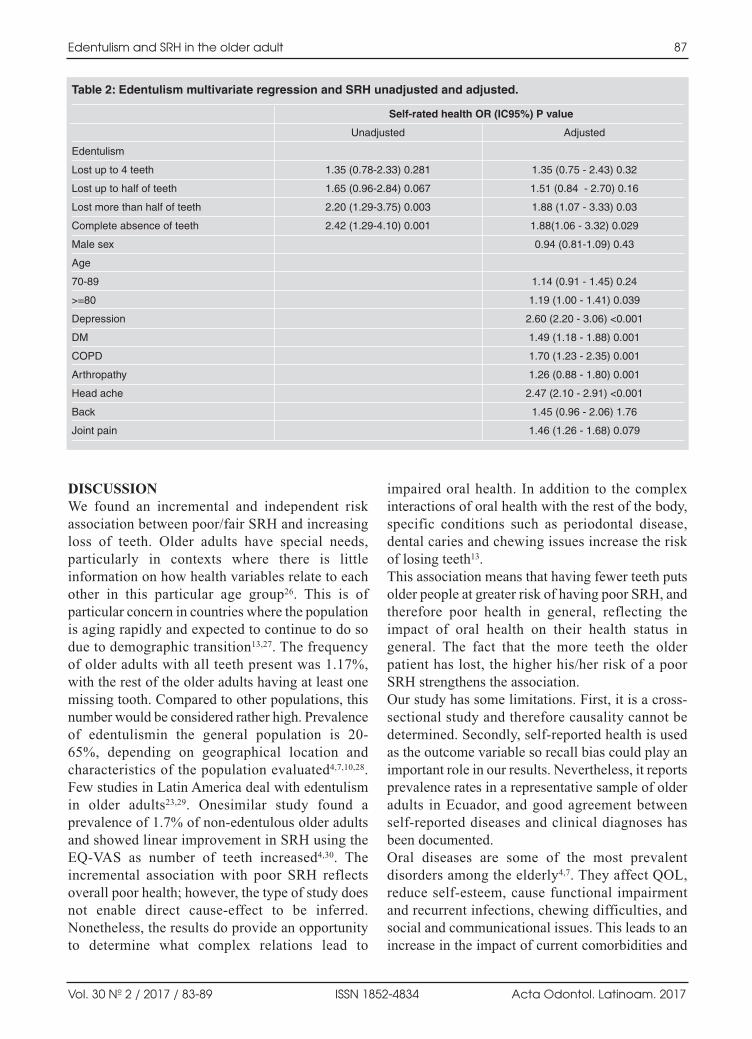
DISCUSSIONWe found an incremental and independent riskassociation between poor/fair SRH and increasingloss of teeth. Older adults have special needs,particularly in contexts where there is littleinformation on how health variables relate to eachother in this particular age group26. This is ofparticular concern in countries where the populationis aging rapidly and expected to continue to do sodue to demographic transition13,27. The frequencyof older adults with all teeth present was 1.17%,with the rest of the older adults having at least onemissing tooth. Compared to other populations, thisnumber would be considered rather high. Prevalenceof edentulismin the general population is 20 65%, depending on geographical location andcharacteristics of the population evaluated4,7,10,28.Few studies in Latin America deal with edentulismin older adults23,29. Onesimilar study found aprevalence of 1.7% of nonedentulous older adultsand showed linear improvement in SRH using theEQVAS as number of teeth increased4,30. Theincremental association with poor SRH reflectsoverall poor health ; however, the type of study doesnot enable direct causeeffect to be inferred.Nonetheless, the results do provide an opportunityto determine what complex relations lead to
impaired oral health. In addition to the complexinteractions of oral health with the rest of the body,specific conditions such as periodontal disease,dental caries and chewing issues increase the riskof losing teeth13.This association means that having fewer teeth putsolder people at greater risk of having poor SRH, andtherefore poor health in general, reflecting theimpact of oral health on their health status ingeneral. The fact that the more teeth the olderpatient has lost, the higher his/her risk of a poorSRH strengthens the association.Our study has some limitations. First, it is a crosssectional study and therefore causality cannot bedetermined. Secondly, selfreported health is usedas the outcome variable so recall bias could play animportant role in our results. Nevertheless, it reportsprevalence rates in a representative sample of olderadults in Ecuador, and good agreement betweenselfreported diseases and clinical diagnoses hasbeen documented.Oral diseases are some of the most prevalentdisorders among the elderly4,7. They affect QOL,reduce selfesteem, cause functional impairmentand recurrent infections, chewing difficulties, andsocial and communicational issues. This leads to anincrease in the impact of current comorbidities and
Edentulism and SRH in the older adult 87
Vol. 30 Nº 2 / 2017 / 83-89 ISSN 1852-4834 Acta Odontol. Latinoam. 2017
Table 2: Edentulism multivariate regression and SRH unadjusted and adjusted.
Self-rated health OR (IC95%) P value
Unadjusted Adjusted
Edentulism
Lost up to 4 teeth 1.35 (0.78-2.33) 0.281 1.35 (0.75 - 2.43) 0.32
Lost up to half of teeth 1.65 (0.96-2.84) 0.067 1.51 (0.84 - 2.70) 0.16
Lost more than half of teeth 2.20 (1.29-3.75) 0.003 1.88 (1.07 - 3.33) 0.03
Complete absence of teeth 2.42 (1.29-4.10) 0.001 1.88(1.06 - 3.32) 0.029
Male sex 0.94 (0.81-1.09) 0.43
Age
70-89 1.14 (0.91 - 1.45) 0.24
>=80 1.19 (1.00 - 1.41) 0.039
Depression 2.60 (2.20 - 3.06) <0.001
DM 1.49 (1.18 - 1.88) 0.001
COPD 1.70 (1.23 - 2.35) 0.001
Arthropathy 1.26 (0.88 - 1.80) 0.001
Head ache 2.47 (2.10 - 2.91) <0.001
Back 1.45 (0.96 - 2.06) 1.76
Joint pain 1.46 (1.26 - 1.68) 0.079
AOL22017:32011 29/11/2017 14:29 Página 87

new conditions such as malnutrition and frailty13,which in turn lead topoor oral health in older adults,constituting a public health issue14,26. SRH is areflection of objective health status,17,18 andedentulism is a condition associated with poor SRH.The determinants of poor oral health in the elderlyneed to be identified in order to reduce its burdenand consequences on them27. Studies like ours are
important to show the relevance of oral health in apopulation. Further research on oral health isneeded, particularly in developing countries, wherethere are impediments to access to healthcareservices, and pain or malaise added to the absenceof adequate treatment often lead to tooth extraction.Policymakers need to address the pubic issue oforal health26.
88 Miguel Germán Borda, et al.
Acta Odontol. Latinoam. 2017 ISSN 1852-4834 Vol. 30 Nº 2 / 2017 / 83-89
ACKNOWLEDGEMENTSThis work was supported by Pontificia Universidad Javeriana.
CORRESPONDENCEDr. Miguel Germán Borda Carrera 7 N. 4062. Hospital San Ignacio, Piso 8, Facultad de Medicina Bogota, Colombia [email protected]
REFERENCES1. Department of Health and Human Services NIoDaCR,
National Institutes of Health. Oral Health in America: Areport of the Surgeon General In: Services. USDoHaH,editor. 2000.
2. Vargas CM KE, JA. Y. Aging Trends: The Oral Health ofOlder Americans. In: Statistics NCfH, editor. Maryland:Centers For Disease Control And Prevention; 2001.
3. Hugo FN, Hilgert JB, de Sousa MaL, da Silva DD, et al.Correlates of partial tooth loss and edentulism in theBrazilian elderly. Community Dent Oral Epidemiol2007;35:224232.
4. CanoGutiérrez C, Borda MG, Arciniegas AJ, Borda CX.Edentulism and dental prostheses in the elderly: impact onquality of life measured with EuroQol—visual analog scale(EQVAS). Acta Odontol Latinoam 2015;28:149155.
5. Navazesh M, Mulligan R. Systemic dissemination as aresult of oral infection in individuals 50 years of age andolder. Spec Care Dentist 1995;15:1119.
6. Nordenram G, Davidson T, Gynther G, Helgesson G, et al.Qualitative studies of patients’ perceptions of loss of teeth,the edentulous state and prosthetic rehabilitation: asystematic review with metasynthesis. Acta OdontolScand 2013;71:937951.
7. Tyrovolas S, Koyanagi A, Panagiotakos DB, Haro JM, etal. Population prevalence of edentulism and its associationwith depression and selfrated health. Sci Rep. 2016;6:37083.doi: 10.1038/srep37083.
8. A N. Oral health status and self rated health in 80Yearoldcommunitydwelling people. Jyväskylä, Finlandia. Universityof Jyväskylä; 2012.
9. Hebling E, Pereira AC. Oral healthrelated quality of life: acritical appraisal of assessment tools used in elderly people.Gerodontology 2007;24:151161.
10. LimaCosta MF, Barreto SM, Giatti L. [Health status,physical functioning, health services utilization, andexpenditures on medicines among Brazilian elderly: adescriptive study using data from the National HouseholdSurvey]. Cad Saude Publica 2003;19:735743.
11. Peltzer K, Hewlett S, Yawson AE, Moynihan P, et al.Prevalence of loss of all teeth (edentulism) and associatedfactors in older adults in China, Ghana, India, Mexico,Russia and South Africa. Int J Environ Res Public Health2014;11:1130811324.
12. Shimazaki Y, Soh I, Saito T, Yamashita Y, et al. Influenceof dentition status on physical disability, mentalimpairment, and mortality in institutionalized elderlypeople. J Dent Res 2001;80:340345.
13. Benyamini Y. Selfratings of health and longevity: A healthpsychologist’s viewpoint onepidemiological findings. TheEuropean Health Psycologist. 2008;10:1013. http://www.ehps.net/ehp/index.php/contents/article/viewFile/ehp.v10.i1.p10/34
14. Ramsay SE , Whincup PH , Watt RG , Tsakos G, et al.Burden of poor oral health in older age: findings from apopulationbased study of older British men. BMJ Open2015;5:12.
15. Borim FS, Neri AL, Francisco PM, Barros MB. Dimensionsof selfrated health in older adults. Rev Saude Publica2014;48:714722.
16. Martinez DJ, Kasl SV, Gill TM, Barry LC. Longitudinalassociation between selfrated health and timed gait amongolder persons. J Gerontol B Psychol Sci Soc Sci 2010;65:715719.
17. Latham K, Peek CW. Selfrated health and morbidity onsetamong late midlife U.S. adults. J Gerontol B Psychol SciSoc Sci 2013;68:107116.
18. Ostbye T, Malhotra R, Chan A. Thirteen dimensions ofhealth in elderly Sri Lankans: results from a National SriLanka Aging Survey. J Am Geriatr Soc 2009;57:13761387.
19. RoseroBixby L, Dow WH. Surprising SES Gradients inmortality, health, and biomarkers in a Latin Americanpopulation of adults. J Gerontol B Psychol Sci Soc Sci2009;64:105117.
20. Albala C, Lebrão ML, León Díaz EM, HamChande R, etal. Encuesta Salud, Bienestar y Envejecimiento(SABE):metodología de la encuesta y perfil de la poblaciónestudiada. Rev Panam Salud Publica 2005;17:307–322.
AOL22017:32011 29/11/2017 14:29 Página 88

21. Desarrollo(SENPLADES) INdEyCISNdPy. ECUADOR Encuesta de Salud, Bienestar y Envejecimiento 2009. In:Financiamiento MdISyEM, editor. Ecuador: EstadisticasSociodemograficas; 2009.
22. Censos INdEy. Encuesta de Salud, Bienestar del AdultoMayor. Ecuador 2009.
23. CastrejónPérez R, JiménezCorona A, Bernabé E, VillaRomero AR. Oral Disease and 3Year Incidence of Frailtyin Mexican Older Adults. J Gerontol A Biol Sci Med 2017Jul 1;72:951957
24. Yesavage JA, Brink TL, Rose TL, Lum O, et al. Developmentand validation of a geriatric depression screening scale: apreliminary report. .J Psychiatr Res 19821983;17:3749.
25. Freire W, Rojas E, Pazmino L, Fornasini M, et al. Encuestanacional de salud, bienestar y envejecimiento SABE IEcuador 2009–2010. In: Quito QAEUSFd, editor. Ecuador2010.
26. Petersen PE, Yamamoto T. Improving the oral health ofolder people: the approach of the WHO Global Oral HealthProgramme. Community Dent Oral Epidemiol 2005;33:8192.
27. Molarius A, S. J. Selfrated health, chronic diseases, andsymptoms among middleaged and elderly men andwomen. J Clin Epidemiol. 2002;55:364370.
28. Müller F, Naharro M, Carlsson GE. What are theprevalence and incidence of tooth loss in the adult andelderly population in Europe? Clin Oral Implants Res2007;18 Suppl 3:214.
29. Borges Yáñez S A, Castrejón Pérez R C, A. LR. Condicionesde salud bucal en los adultos mayores y su asociación conelestado nutricional Odont Act 2013;10: 2430
30. Brazier J, Jones N, Kind P. Testing the validity of theEuroqol and comparing it with the SF36 health surveyquestionnaire. Qual Life Res 1993;2:169180.
Edentulism and SRH in the older adult 89
Vol. 30 Nº 2 / 2017 / 83-89 ISSN 1852-4834 Acta Odontol. Latinoam. 2017
AOL22017:32011 29/11/2017 14:29 Página 89

90
Acta Odontol. Latinoam. 2017 ISSN 1852-4834 Vol. 30 Nº 2 / 2017 / 90-95
RESUMENLos tratamientos ortodóncicos con alineadores Invisalign®
utilizan aditamentos construidos en resinas compuestasllamados “attachments” adheridos a la superficie dentaria. El“attachment” es una de las herramientas más potentes paramejorar la eficiencia del movimiento dental.El propósito de este estudio fue evaluar el desgaste superficialde dos resinas compuestas utilizadas para construir los“attachments” en el tratamiento de ortodoncia con la técnicade alineadores Invisalign®. Se evaluaron 40 “attachments” adheridos a la superficie vesti bular de piezas dentarias del maxilar superior en un período de 6meses. Los “attachments” fueron construidos en forma aleatoriay a doble ciego con dos resinas compuestas (Filtek Z350 XT de3M ESPE y Amelogen Plus TW Ultradent Products Inc) elegidasde acuerdo con las propiedades estéticas y mecánicas requeridas.Los “attachments” fueron impresionados con una técnicapreestablecida inmediatamente luego de ser adheridos y a los 6meses. Las muestras fueron preparadas para su observaciónmediante Microscopía Electrónica de Barrido (MEB) a 12aumentos. Se observaron los cambios producidos en la textura
superficial y la forma entre el inicio y los seis meses detratamiento. Los datos fueron analizados y comparados utilizandola prueba de MannWhitney, realizada en función del ordena miento global, de menor a mayor según el cambio producido enesas variables.Los materiales analizados mostraron una diferencia estadísti camente significativa (P<0,001) en el desgaste superficial,siendo el Amelogen Plus el material que evidenció mayorcambio. Las modificaciones en la forma de los “attachments”no fueron estadísticamente significativas en ambos materiales(P>0,05).Según los resultados obtenidos en este estudio, la modificaciónde la superficie de los “attachments” durante los primeros seismeses de tratamiento varía en función del composite empleado,en tanto la forma del “attachment” no parece ser afectada demanera similar, por lo que el desempeño clínico podría serconsiderado aceptable cuando se emplean los materialesevaluados.
Palabras clave: Alineadores invisibles; Ortodoncia, attachments;Invisalign; resina compuesta, desgaste superficial.
INTRODUCTIONIn recent decades there has been a remarkableincrease in the available range of orthodontictreatments for adult patients who demand estheticsand comfortable alternatives consistent with their
modern social and working lifestyles.1To satisfythese demands, in 1999 Align Technology (SantaClara, CA) introduced orthodontic treatments withclear aligners using sequential application of clearalignment devices made from thermoplastic material.
ABSTRACTOrthodontic treatments with Invisalign® require the use ofattachments, which are composite resin buttons attached totooth surfaces. Attachments constitute one of the most powerfultools for improving the efficiency of orthodontic tooth movement.The main purpose of this study was to evaluate surface wear oversix months in two resin composites (Filtek Z350 XT, 3M ESPEand Amelogen Plus TW, Ultradent Products Inc.) used formaking Invisalign® attachments. These composites wereselected for their esthetic and mechanical properties. Fortyattachments were bonded to the buccal surface of maxillaryteeth. Materials were randomized and assigned in a double blindmanner. Impressions were taken of the attachments using a preestablished technique immediately after bonding and following6 months of clinical use. The impressions were examined by
Scanning Electron Microscopy (SEM) at 12fold magnificationto identify changes in surface texture and attachment shape.Data were analyzed using MannWhitney’s test on the overallranking of detected changes in those variables.Statistically significant differences (P<0.001) were found forsurface wear, with greater changes in Amelogen Plus. Attachmentshape did not change significantly in either material (P>0.05).According to the results of this study, the alteration of theattachment surface during the first six months of treatmentdepends on the composite used, while attachment shape doesnot appear to be affected, so the clinical performance of thematerials evaluated could be considered acceptable.
Keywords: Clear aligner; Orthodontics, attachments; Invisalign;composite, surface wear.
Surface wear of resin composites used for Invisalign® attachments
Graciela J. Barreda1,2, Elizabeth A. Dzierewianko1,2, Karina A. Muñoz1,2, Gisela I. Piccoli1,2
1 Sociedad Argentina de Ortodoncia. Buenos Aires. Argentina.2 Universidad de Ciencias Empresariales y Sociales, Buenos Aires. Argentina.
Desgaste superficial de las resinas compuestas utilizadas en los “attachments” de la técnica Invisalign®
AOL22017:32011 29/11/2017 14:29 Página 90

Buttons made of composite resin, known as“attachments”, are placed on tooth surfaces asretentive elements and to improve the efficiency ofcomplex tooth movements. Since they are one ofthe most powerful tools for moving teeth efficiently,it is important that their integrity and shape shouldremain constant throughout the treatment. 25
An aligner attachment needs esthetic and mechanicalproperties. In addition to being resistant to stain, itshould be the same shade as the tooth or translucentenough to blend with the underlying tooth.6 It shouldalso be resistant to wear, and it is on this propertythat the current study focuses.Composite resin materials are made of an organicphase (matrix) and a ceramic phase (filler) consistingof admixtures of particles of different sizes, whichdetermine the material’s properties. According to theclinical requirements, fillers may make up 50% to70% of the volume, and particle size may range from20 nanometers to 5 micrometers. 79 Higher fillercontent results in better mechanical properties, whilesmaller average particle size provides better estheticproper ties.10 Composite resin surface wear has beenremarkably reduced through the recent developmentof nanoparticle resin. 1114This study compares twocomposites of high esthetic and mechanical characte ristics with the goal of finding an ideal material forattachments.The aim of this study was to use Scanning ElectronMicroscopy (SEM) to determine whether attachmentsurfaces remain unaltered during the first six monthsof treatment.
MATERIALS AND METHODSThis study was approved by “Sociedad Argentina deOrtodoncia” Research Ethics Committee resolutionnumber 60108/2015.Ten subjects were selected, male or female, aged 15to 50 years, who required orthodontic treatment,
with full upper dentition and mild or moderatecrowding. Patients with mixed dentition, maxillarycrown restorations, active periodontal disease and/oredentulous spaces in upper maxillary were excluded.All subjects were treated with Invisalign® aligners.Patients were instructed to brush their teeth with asoft toothbrush (Colgate® Slim Soft) and lowabrasive dentifrice (Sensodyne® Pro Enamel).The attachments were prepared from one of twolightcured resin composite types: Filtek Z350 XT,3M ESPE orAmelogen Plus TW, Ultradent ProductsInc., which have different mechanical and estheticproperties. Materials with high ceramic filler content(72% 76% by weight) were selected for theirtranslucency and physical properties (Table 1).Forty (40) attachments were made with Invisalign®
Templates on upper maxillary teeth. Materials wererandomized for each attachment.Before attachment preparation, dental enamel wastreated following total acid etching protocol with37% phosphoric acid (ScotchbondTM Etchant,3M),15second application. Acid was removed withwater spray for 30 seconds and the enamel surfacewas dried for bonding agent application. A layer ofbonding agent (Single Bond 2, 3M ESPE) wasapplied with a microbrush and any excess removedby blowing with compressed air. Each attachmentwas lightcured for 10 seconds (Bluephase G2 CuringLight, Ivoclar Vivadent®) following manufacturer’sinstructions. The attachment surface was notpolished after template removal (Fig 1).A customized device was designed to use as a trayfor attachment impressions. It was prepared from a6 mm x 6 mm x 6 mm cubic plastic block (Blocky®)customized in an improved stone cast with acrylic(DuraLay, Reliance) for each tooth on which anattachment was placed, in order to provide aconsistent insertion pathway for the first andsubsequent impressions (Fig. 2 a).
Surface wear of Invisalign® attachments 91
Vol. 30 Nº 2 / 2017 / 90-95 ISSN 1852-4834 Acta Odontol. Latinoam. 2017
Table 1: Materials tested.
Material
Filtek Z350 XT
Amelogen PlusTW
Type
Nanofilled
Micro-hybrid
Shade
AmberTranslucent
TranslucentWhite
Filler Content(by weight)
72.5%
76%
Monomer
Bis-GMA, UDMA, Bis-EMA,TEGDMA
Bis-GMA
Manufacturer
3M ESPE
Ultradent products, Inc.
Batch
N593705
D00B9
Bis-GMA: Bisphenol-A diglycidlethermethacrylate; UDMA: urethane – dimethacrylate; Bis-EMA: Ethoxylatedbisphenol-A dimethacrylate; TEGDMA: triethylene glycol dimethacrylate.
AOL22017:32011 29/11/2017 14:29 Página 91
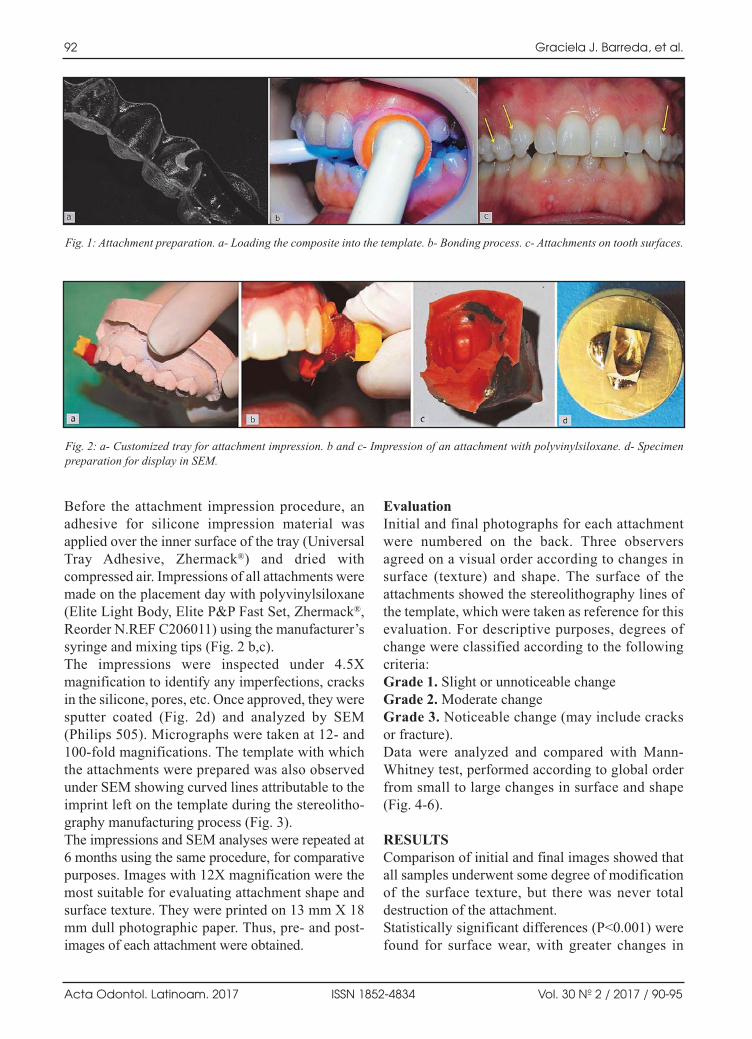
Before the attachment impression procedure, anadhesive for silicone impression material wasapplied over the inner surface of the tray (UniversalTray Adhesive, Zhermack®) and dried withcompressed air. Impressions of all attachments weremade on the placement day with polyvinylsiloxane(Elite Light Body, Elite P&P Fast Set, Zhermack®,Reorder N.REF C206011) using the manufacturer’ssyringe and mixing tips (Fig. 2 b,c).The impressions were inspected under 4.5Xmagnification to identify any imperfections, cracksin the silicone, pores, etc. Once approved, they weresputter coated (Fig. 2d) and analyzed by SEM(Philips 505). Micrographs were taken at 12 and100fold magnifications. The template with whichthe attachments were prepared was also observedunder SEM showing curved lines attributable to theimprint left on the template during the stereolitho graphy manufacturing process (Fig. 3).The impressions and SEM analyses were repeated at6 months using the same procedure, for comparativepurposes. Images with 12X magnification were themost suitable for evaluating attachment shape andsurface texture. They were printed on 13 mm X 18mm dull photographic paper. Thus, pre and postimages of each attachment were obtained.
EvaluationInitial and final photographs for each attachmentwere numbered on the back. Three observersagreed on a visual order according to changes insurface (texture) and shape. The surface of theattachments showed the stereolithography lines ofthe template, which were taken as reference for thisevaluation. For descriptive purposes, degrees ofchange were classified according to the followingcriteria:Grade 1. Slight or unnoticeable changeGrade 2. Moderate changeGrade 3. Noticeable change (may include cracksor fracture).Data were analyzed and compared with MannWhitney test, performed according to global orderfrom small to large changes in surface and shape(Fig. 46).
RESULTSComparison of initial and final images showed thatall samples underwent some degree of modificationof the surface texture, but there was never totaldestruction of the attachment.Statistically significant differences (P<0.001) werefound for surface wear, with greater changes in
92 Graciela J. Barreda, et al.
Acta Odontol. Latinoam. 2017 ISSN 1852-4834 Vol. 30 Nº 2 / 2017 / 90-95
Fig. 1: Attachment preparation. a Loading the composite into the template. b Bonding process. c Attachments on tooth surfaces.
Fig. 2: a Customized tray for attachment impression. b and c Impression of an attachment with polyvinylsiloxane. d Specimenpreparation for display in SEM.
AOL22017:32011 29/11/2017 14:29 Página 92

Amelogen Plus. Attachment shape showed nosignificant change (P>0.05). Results for changes intexture and shape are provided in Tables 2 and 3,respectively.
DISCUSSIONIn addition to the aligners themselves, treatments usinginvisible aligners require auxiliary “attachments” tohelp retain and move teeth.3,4,15
Surface wear of Invisalign® attachments 93
Vol. 30 Nº 2 / 2017 / 90-95 ISSN 1852-4834 Acta Odontol. Latinoam. 2017
Table 2: Texture change frequency category according to material.
Material
Filtek Z350 XT (3M ESPE)
Amelogen Plus TW(Ultradent Products Inc)
Total
Slight change
8
1
9
Texture
Moderate change
6
3
9
Noticeable change
4
18
22
Total
18
22
40
The difference between materials is statistically significant (p<0.001)
Table 3: Shape changes frequency category according to material.
Material
Filtek Z350 XT (3M ESPE)
Amelogen Plus TW(Ultradent Products Inc)
Total
Slight change
13
15
28
Shape
Moderate change
5
4
9
Noticeable change
1
2
3
Total
19
21
40
The difference between materials is not statistically significant (P>0.05).
Fig. 3: a Attachment Template image. 12X magnification. bStereolithography lines of the template can be seen onattachment surface.
Fig. 4: SEM images (12X) of an attachment showing slightchange; baseline (a) and at 6 months (b). Filtek Z350composite.
Fig. 5: SEM images (12X) of an attachment showing moderatechange; baseline (a) and at 6 months (b). Filtek Z350composite.
Fig. 6: SEM images (12X) of an attachment showing noticeablechange; baseline (a) and at 6 months (b). Amelogen Pluscomposite.
AOL22017:32011 29/11/2017 14:29 Página 93

In a systematic review, Rossini et al. concluded thattransparent aligner treatments require the use ofattachments to improve the predictability oforthodontic movement.2 Another study by the sameauthors compared complex orthodontic movementswith and without attachments, showing the relevanceof using attachments to improve the efficiency of theappliance.16 The composite selected must thereforehave adequate mechanical properties. There iscurrently no published study establishing minimalintegrity for proper attachment performance.6
Studies in vitro and in vivo have referred to wear ofcomposite resins in contact with the tooth structureantagonist in occlusal restorations and/or mechanicalaction of brushing, diet and salivary pH.1719We didnot find any analyses of abrasive wear against anantagonist such as the aligner material.In our study, all final SEM images showed surfacedifferences such as reduction and/or total absenceof lines related with the template stereolithographyimpression. The observed changes in the surfacesof the attachments may be produced by the frictiongenerated when placing and removing the aligner,among other causes. Filtek Z350 revealed lesssurface wear than Amelogen Plus TW after the firstsix months’ use, in agreement with Feinberg etal.6Attachment shape did not change significantlyfor either of the study materials, suggesting thattooth movement related to the attachment wouldstill be effective after six months. Further research using a larger number of resinmaterials and longer time periods is needed to
quantify the observed changes and their relation tothe efficiency of orthodontic tooth movement.We believe that the results of this study provide auseful contribution to be considered when materialsare being selected for making attachments.
CONCLUSIONAttachments used in the Invisalign® orthodontictechnique contribute to orthodontic tooth movement.According to the results of this study, the alterationof the surface of the attachments during the first sixmonths of treatment varies depending on thecomposite used, while the shape of the attachmentdoes not appear to be affected, so the clinicalperformance of the materials evaluated can beconsidered acceptable.
ACKNOWLEDGMENTSThe authors thank the following people and organizations fortheir valuable help in this study: D.D.S. Ricardo L. Macchi andNoemí E. Walsöe de Reca as consultants, D.D.S. LilianaRodríguez Bueno, Authorities of S.A.O. U.C.E.S., D.D.S.Gabriela Caldentey, Valeria Mazza, Rocío Moreno, Ariel E.Regidor and Hugo J. Romanelli, Karina Lloveras for assistancein reviewing the literature, Dental Assistant Rosalba Gómez,Mr. Dante Giménez for SEM technical support, CITEDEF,UNIDEF (Research Unit Defense), MINDEF (Ministry ofDefense) and CONICET (National Council for Scientific andTechnical Research).This research received a grant from the University ResearchAward Program 2015 (Align Technology) and was honoredwith the Prof. Dr. Héctor R. Maddalena Award conferred bythe “Sociedad Argentina de Investigación Odontológica”(SAIO), the Argentine Division of the International Association for Dental Research (IADR), in November 2016.
94 Graciela J. Barreda, et al.
Acta Odontol. Latinoam. 2017 ISSN 1852-4834 Vol. 30 Nº 2 / 2017 / 90-95
CORRESPONDENCEDr. Graciela J. BarredaGalileo 2460 PB 2 C.A.B.A.(1425). Buenos Aires.Argentina. [email protected].
REFERENCES1. Jeremiah HG, Bister D, Newton JT. Social perceptions of
adults wearing orthodontic appliances: A crosssectionalstudy. Eur J Orthod 2011; 33:476482.
2. Rossini G, Parrini S, Castroflorio T, Deregibus A, et al.Efficacy of clear aligners in controlling orthodontic toothmovement: A systematic review. Angle Orthod 2015; 85:881889.
3. Simon M, Keilig L, Schwarze J, Jung BA, et al. Treatmentoutcome and efficacy of an aligner technique regardingincisor torque, premolar derotation and molar distalization,BMC Oral Health 2014; 14:68.
4. Kravitz ND, Kusnoto B, Agran B, Viana G. Influence ofattachments and interproximal reduction on the accuracy of
canine rotation with Invisalign: A prospective clinical study.Angle Orthod 2008; 78:682687.
5. Dasy H, Dasy A, Asatrian G, Rózsa N, et al. Effects ofvariable attachment shapes and aligner material on alignerretention. Angle Orthod 2015; 85 :934940.
6. Bowman Feinberg K, Souccar NM, Kau CH, Oster RA et al.Translucency, Stain Resistance, and Hardness of compositesused for Invisalign Attachments. JCO 2016; 3:170176.
7. Lang BR, Jaarda M, Wang RF. Filler particle size andcomposite resin classification systems. J Oral Rehabil 1992;19:569584.
8. Van Landuyt KL,Hellack B, Van Meerbeek B, Peumans Met al. Nanoparticle release from dental composites. ActaBiomater 2014; 10:365374.
AOL22017:32011 29/11/2017 14:29 Página 94

9. Mitra SB, Wu D, Holmes BN. An application Nanotechnologyin advanced dental materials. J Am Dent Assoc 2003; 134:13821390.
10. Kim JJ, Moon HJ, Lim BS, Lee YK et al. The effect ofnanofiller on the opacity of experimental composites.JBiomed Mater Res B Appl Biomater 2007. 80:332338.
11. Nagarajan VS, Jahanmir S, Thompson. In vitro contactwear of dental composites. Dent Mater 2004; 20:6371.
12. Palaniappan S, Bharadwaj D, Lima Mattar D, Peumans M etal. Nanofilled and microhybrid composite restorations: fiveyear clinical wear performances. Dent Mater 2011; 27:692700.
13. Ferracane JL. Is the wear of dental composites still aclinical concern? Is there still a need for in vitro wearsimulating devices? Dent Mater 2006; 22:689692.
14. Tanimoto Y, Kitagawa T, Aida M, Nishiyama N. Experi mental and computational approach for evaluating the
mechanical characteristics of dental composite resins withvarious filler sizes. Acta Biomater 2006; 2:633639.
15. Ravera S, Castroflorio T, Garino F, Daher Set al. Maxillarymolar distalization with aligners in adult patients: a multi center retrospective study. ProgOrthod 2016; 17:12.doi:10.1186/s4051001601260.
16. Comba B, Parrini S, Rossini G, Castroflorio T et al. A ThreeDimensional Finite Element Analysis of UpperCanineDistalization with Clear Aligners, Composite Attachments,and Class II Elastics. JCO January 2017; 51:2428.
17. Kusy RP, Leinfelder KF. Pattern of wear in posteriorcomposite restorations.J Dent Res 1997; 56:5, 544.
18. Cao L, Zhao X, Gong X, Zhao S. An in vitro investigationof wear resistance and hardness of composite resins.Int JClinExp Med 2013; 26(6):423430.
19. Xu HC, Tong W, Song SQ. Wear patterns of compositerestorative resins in vivo, observations by scanning electronsmicroscopy. Oral Rehabilit. 1985; 12(5):389400.
Surface wear of Invisalign® attachments 95
Vol. 30 Nº 2 / 2017 / 90-95 ISSN 1852-4834 Acta Odontol. Latinoam. 2017
AOL22017:32011 29/11/2017 14:29 Página 95

AOL22017:32011 29/11/2017 14:29 Página 96
AOL22017:32011 29/11/2017 14:29 Página 97

AOL22017:32011 29/11/2017 14:29 Página 98

AOL22017:32011 29/11/2017 14:29 Página 99
AOL22017:32011 29/11/2017 14:29 Página 100