Embed Size (px)
Citation preview
Queen Mary Hospital
瑪麗醫院
Queen Mary Hospital
瑪麗醫院1
Acute Myocardial Infarction Clinical Pathway -
The QMH Experience
Dr Raymond ChanConsultant Cardiologist
Queen Mary Hospital, Hong Kong8th Jun 2011 HA Convention
急性心肌梗塞臨床路徑
id18690656 pdfMachine by Broadgun Software - a great PDF writer! - a great PDF creator! - http://www.pdfmachine.com http://www.broadgun.com
Queen Mary Hospital
瑪麗醫院
Queen Mary Hospital
瑪麗醫院2
Part 1 : What is it?What are the Results?
Part 2 : How we do it?How to run a AMI_CP.
It is worth doing & you can do it.Sharing of some difficulties & problem Solving

3
PART 1: WHAT?

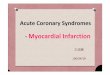
M/57 Acute MIM/57 Acute MI
M/57 Severe Intense Pain, AMI M/57 Severe Intense Pain, AMI ��EEmergent PPCI (mergent PPCI (PPrimary rimary PPercutaneous ercutaneous CCoronary oronary IIntervention) done.ntervention) done.Patient well. Discharge home 3 daysPatient well. Discharge home 3 days
LADLAD
CIRCIRCIRCIR
Before PCI After PCI
LAD locked

Queen Mary Hospital
瑪麗醫院
Queen Mary Hospital
瑪麗醫院5
Unstable Angina心絞痛
Non-ST Elevation MI
ST Elevation MI
心肌梗塞
急性冠狀動脈綜合症Acute Coronary Syndrome
SPECTRUM

Queen Mary Hospital
瑪麗醫院
Queen Mary Hospital
瑪麗醫院
6
The Scope:The Scope:
ACS Accounts for 10,000admissions to HA Hospitals
QMH (2009) -617 AMI�s (227 STEMI + 390 NSTEMI)

Queen Mary Hospital
瑪麗醫院
Queen Mary Hospital
瑪麗醫院7
The Significance :The Significance :
Half of AMI�s are fatal.
Out of all fatalities, majority died before patients arrive to Hospital
(WHO Monica Study & AIHW Database)

It is a well-written clinical protocol based on updated international guidelines.
It�s placed & starts at the AED, consist of a booklet of practical, didactic clinical instructions with check boxes on what the doctors & nurses should do starting atDay 1-5 aiming to cater for >90% ofpatients of Uncomplicated AMI.
The Clinical Pathway The Clinical Pathway �� What is it ?What is it ?
8
PART 1: WHAT?
1. Decision making criteria for the use & Contraindications of Lytics or PPCI
2. Logistics to activate the operation team3. Use of medications4. Step down criteria 5. Daily care map until discharge

Inception of AMI_CP 2006
With the Vision of Dr WH Seto & Dr Lawrence Lai, the QMH sent a team of 10 delegates to Singapore Changi Hospital to learn about their Practice of Clinical pathways
10 members: WH Seto, Alan Wong, Kate Choi, Patricia Ching, Sania, WC Ho, NF Shum, TW Lau, T Li, SK Leung, R Chan
Acute Myocardial Infarction Acute Myocardial Infarction -- Clinical PathwayClinical Pathway
9
Acute Myocardial Infarction Acute Myocardial Infarction -- Clinical PathwayClinical Pathway
107.2006
Prof Fock Kwong Ming

(1.2.2007 1st version)
11

12
� When a coronary artery is blocked, the most important Rx is to open it ASAP
� Timing is critical
� Given the right time, right place, PPCI is better, the matter is resource & logistics
� Patients triaged by the CP to Lytics (SK or TNK) or PPCI
� Daily Care-map

Daily Drug(Class 1) PrescriptionBoxes

(1.2.2007 1st version)
14

(1.2.2007 1st version)
15

16
UnCx AMI 2007 2008 2009 2010
No. recruit 201 160 174 119
No. Completed 166 123 113 89
= 654
75.1% (491) of the patients completed the CP from 2007-2010
Patients completed CP 491Patients receiving Thrombolytics 95 (38 +36 +16 + 5)Patients receiving PPCI 176 (23 +36 +57 +60)
2007 2008 2009 2010
654 Un-Complicated AMI pts were recruited since 2007

17
Total AMI 2007-2010 = 617 x 4 = 2468(CP Recruits) 654/ 2468 = 26.5%(Excl fallout pts) 491/ 2468 = 20% of AMI in the CP
We hypothesized that by running a AMI_CP on a targeted group of STEMI patients, it exerts a �TRAILER TRUCK� effect on the Q.O.C. of
other AMI patients � STEMI & NSTEMI alike
How can we tell?By examining the Clinical outcome of ALL the AMI patients throughout the years since the inception of the AMI CP.

Circulation, AHA, Guidelines for Management of STEMI Update 2011Door to Needle Time(DNT) ≤ 30 min Door to Balloon Time(DBT) ≤ 90 min
Mortality(%) of 2,245 pts in National Infarct Angioplasty Project (NIAP), UKPrimary PCI better than Thrombolytics with better outcome :
Caveat � right place, right time DBT � DNT <= 60�
Stroke 2000; 31; 1802Stroke 2000; 31; 1802--18111811Risk Factors for Intracranial haemorrhage (ICH) after Thrombolytics:
Age >=75y BW F<=65kg M<=80kg Female SBP>=160mmHgPrior Stroke TNK use Black Race INR>=4
Numerous Drugs Trials for AMI Numerous Drugs Trials for AMI ��Aspirin, Plavix, Beta Blocker, ACEI, ARB, StatinsAspirin, Plavix, Beta Blocker, ACEI, ARB, Statins 18
Treatment 30 days 1 year 18 monthsPPCI 5.6 8.7 9.9Thrombolysis 7.9 12.4 14.8No Reperfusion 16.4 28.3 31.0
EBM � Fundamental of AMI Clinical Pathway

QMH AMI_CLINICAL PATHWAY :
Queen Mary Hospital
瑪麗醫院
Queen Mary Hospital
瑪麗醫院19
RESULTS
PART 1: WHAT?

2007 2008 2009 2010 1-4/2011 International Benchmark
No. Recruited 201 160 174 119
No. Completed 166 123 113 89
Age (mean) 68.1 65.8 63 65.3
Lytics 38 (22.9%) 36(29%) 16(14%) 5 (5.6%) xD-N-T (mean) 86 42 40 43 x 30
PPCI 23(13.9 %) 36(29%) 57(50%) 60(67.4%)
D-B-T (mean) 277 113 101 96 90
LOS (mean) 5.2 4.2 3.9 4
Readmission Rate
6.6 4.1 4.4 5.6
Hosp Mortality(All AMI)
13.2 10.5 10.2 9.8 See Chart
Results 1: AMI Clinical Pathway 2007 - Present:

2007 2008 2009 2010 1-4/2011 International Benchmark
No. Recruited 201 160 174 119
No. Completed 166 123 113 89
Age (mean) 68.1 65.8 63 65.3
Lytics 38 (22.9%) 36(29%) 16(14%) 5 (5.6%) xD-N-T (mean) 86 42 40 43 x 30
PPCI 23(13.9 %) 36(29%) 57(50%) 60(67.4%)
D-B-T (mean) 277 113 101 96 90
LOS (mean) 5.2 4.2 3.9 4
Readmission Rate
6.6 4.1 4.4 5.6
Hosp Mortality(All AMI)
13.2 10.5 10.2 9.8 See Chart
Results 1: AMI Clinical Pathway 2007 - Present:

International Database of AMI Mortality
16.00% 9.80% 7.20%
48.9%
14.5%
49.4%
19.00%22%
0%20%40%60%80%
100%
AIHW TotalCFR
AIHW hospCFR
WHOMONICA28d CFR
(Men)
WHOMONICA28d CFRHosp pts
(Men)
YALEMedicare30d, JGIM
2006
Yale 201030d RSMR,Circ Cardio
Outcome2010
HK HA AmiMortality
Study 2009,in progress
HK QMH2010 In-
Hosp CFR
SwedishSTEMI
Registry1996-2007In-HospMortality
JAMA 2011
per
cen
tag
e
Circulation 1997:WHO Project withA population view 1985-1990
Australian Institute of Health & Welfare 9.2002: 1/2 of 48,313 events were fatal (1999-00) & 87% occurred outside hospital
THE IMPACT
LIMITATIONS: AIHW 2002 WHO 1990 MEDICARE FFS CCU Pt only½US AMI Pts
MortalityTrend
MortalityTrend
* * *

International Database of AMI Mortality
16.00% 9.80% 7.20%
48.9%
14.5%
49.4%
19.00%22%
0%20%40%60%80%
100%
AIHW TotalCFR
AIHW hospCFR
WHOMONICA28d CFR
(Men)
WHOMONICA28d CFRHosp pts
(Men)
YALEMedicare30d, JGIM
2006
Yale 201030d RSMR,Circ Cardio
Outcome2010
HK HA AmiMortality
Study 2009,in progress
HK QMH2010 In-
Hosp CFR
SwedishSTEMI
Registry1996-2007In-HospMortality
JAMA 2011
per
cen
tag
e
Circulation 1997:WHO Project withA population view 1985-1990
Australian Institute of Health & Welfare 9.2002: 1/2 of 48,313 events were fatal (1999-00) & 87% occurred outside hospital
THE IMPACT
LIMITATIONS: AIHW 2002 WHO 1990 MEDICARE FFS CCU Pt only½US AMI Pts
MortalityTrend
MortalityTrend
* * *

QMH EXPERIENCE : Causes Overall AMI Mortality :
367
65
44
30
361
104
63
25
465
64
93
10
476
36
87
5
110
13
40
0
2007 2008 2009 2010 2011
ELECTIVE
URGENT
EMERGENCY
LYTICS
EMERGENT PCI :Procedure be performed ASAP/ within 24h(Maj = PrimaryPCI)
URGENT PCI :Procedure be performed within index hospitalisation
(Jan-Mar)
*
E-PCI : ∑ Mort RateNon UR ( =NON ULTRA RISK)UR (Shock, Post Arrest, Intub, VT)Elective PCI :
∑ 4.3%(4/93)2.8%(2/72)9.5%(2/21)
0%
∑ 8.1%(7/87)0%(0/66)
33.3 %(7/21)0%
∑ 6.8% ∑ 7.9%
13.2% 10.5% 10.2% 9.8%OverallAMI Mortality
(E-PCI)
24 Hour PPCI7.11.2010

25
% within 24h Non-Compliance Reason
Aspirin 94.3 Allergy to Aspirin; Anaemia on admissionBleeding tendency on admission e.g. low PLT countAlready on anti-coagulation drug e.g. Warfarin
Plavix 85.4 Patients started Plavix on Day 2,6,8 and 16
% Upon Discharge Non-Compliance Reason
Aspirin 97.6 Allergy to Aspirin; Anaemia Bleeding tendency e.g. low PLT countAlready on anti-coagulation drug e.g. Warfarin
Plavix 88 Stopped Plavix for performing CABG
Beta Blocker 84.6 Lowish BP; Relative low heart rate; Heart BlockHistory of COPD or COPD on exacerbation
ACEI / ARB 73.2 Lowish BP; Deranged renal function; Already on ARB
Statins 95.9 Normal lipid levelFasting lipid profile result not available on discharge from QMH & would be follow up in CRP bed or in cardiac SOPD
Results 2 : Drug Compliance Audit 2007 (UK NICE Criteria)

26
AMI CP (Key Performance Indicators)
0
50
100
150
200
250
300
Year
DNT DBT (min)
0
2
4
6
8
10
QuarterLOS (days)
DNT DBT LOS
DNT 86 111 114 41 45 35 35 39.5 42 20 40 50 0 43 43 61 0
DBT 277 127 188 106 120 104.5 106 97 101 101 105 105.5 96 89 99.5 101 119
LOS 4 4 4 3 3 3 3 5 3 4 4 3 4 4.6 3.52 4 2
MOR 13.19 10.49 10.23 9.76
RAM 6.63 4.07 4.42 5.62
2007 2008 2009 2010 2011
* Declining Mortality Trend in ALL AMI Patients
*

Mortality Trend � Contributing factors :
Short DNT � phased out 7.11.2010 Short DBT Near 100% compliance for eligible pts receiving medications of
Class I indications Strategic phasing out of administration of IV Lytics & the 24 hour
Emergent Primary PCI Program
(High percentage of high risk patients achieve target LDLC <70mg/dL = 82.9% ) � Complex Correlation, Not discussed in the present context
Acute Myocardial Infarction : Clinical PathwayAcute Myocardial Infarction : Clinical Pathway
27
END OF PART 1: �WHAT� & THE IMPACT

Queen Mary Hospital
瑪麗醫院
Queen Mary Hospital
瑪麗醫院28
Part 2
How To Do It?
PART 2: HOW?

Queen Mary Hospital
瑪麗醫院
Queen Mary Hospital
瑪麗醫院29
It is Labour Intensive but HAPPY!

Queen Mary Hospital
瑪麗醫院
Queen Mary Hospital
瑪麗醫院
��QMH Acute Myocardial Infarction QMH Acute Myocardial Infarction Clinical Pathway TeamClinical Pathway Team��
ER
Audit & CQI
MSW
CARDIOLOGISTS
Radiographers, CCL Nurses
CCU & Ward
Physio, OT, Dietitian

Queen Mary Hospital
瑪麗醫院
Queen Mary Hospital
瑪麗醫院31
1.Open, Fair & Transparent �
How to do that ?
PART 2: HOW TO RUN A AMI CP?

QMH Audit, Training & Development TeamQMH Audit, Training & Development Team Review & develop Review & develop SOPSOP & C& Care Mapsare Maps Root cause analysisRoot cause analysis of Variances ( of Variances ( DNT, DBT & LOS)DNT, DBT & LOS) Case managerCase manager : Data acquisition, Analysis, Variance audit: Data acquisition, Analysis, Variance audit
Queen Mary Hospital
瑪麗醫院
Queen Mary Hospital
瑪麗醫院
Selina WongDOM
Pearl ChanSNO T&D Patricia Ching
SNO Q & S
Kate ChoiSNO CAM
Sania KwanQRI
Wong So ManCase Manager

QMH Audit, Training & Development TeamQMH Audit, Training & Development Team Review & develop Review & develop SOPSOP & C& Care Mapsare Maps Root cause analysisRoot cause analysis of Variances ( of Variances ( DNT, DBT & LOS)DNT, DBT & LOS) Case managerCase manager : Data acquisition, Analysis, Variance audit: Data acquisition, Analysis, Variance audit
Queen Mary Hospital
瑪麗醫院
Queen Mary Hospital
瑪麗醫院
Selina WongDOM
Pearl ChanSNO T&D Patricia Ching
SNO Q & S
Kate ChoiSNO CAM
Sania KwanQRI
Wong So ManCase Manager
B R A I NB R A I N

RESULTS
REVIEW& AUDIT
CHANGE & INTERVENE
CLNICAL PRACTICE
PART 2: HOW?
Form the Basisof Interactive
Model

Queen Mary Hospital
瑪麗醫院
Queen Mary Hospital
瑪麗醫院35
2. Strategic Reviews are Essential
Highlight How the Interactive Model works?
PART 2: HOW?

Lytics may result in Fatal Complications Lytics may result in Fatal Complications ��
36
2003 (TNK) 2005 (TNK)2007 (TNK) 2007 (SK)2008 (TNK)
We performed extensive review into previous clinical data.
Lytic is dangerous
RESULTS
REVIEW& AUDIT
CHANGE & INTERVENE
CLNICAL PRACTICE

PPRIMARY RIMARY PPERCUTANEOUS ERCUTANEOUS CCORONARY ORONARY IINTERVENTIONNTERVENTION
37
Symptom onset : 11:20 3/11/07 VFDoor time : 12:08 3/11/07 QMH
Balloon time : 13:35 3/11/07 Door-to-Balloon Time : 87min
Mechanical VentilationShock, IABP
Normal Flow Re-establishedPt in ICU 2 weeksAcute Renal FailureNo Urine, depend on HD
No Left SystemTotal Blocked LAD
*1******* 2
3 4
PPCI is moreEfficacious & safer& may represent the only optione.g. when Lytics are C/I, shock, late presentation
Major Issue isresource
*1*******
*1******* *1*******
RESULTS
REVIEW& AUDIT
CHANGE & INTERVENE
CLNICAL PRACTICE

38
Balloon time : 13:35 3/11/07 Door-to-Balloon Time : 87min
Normal Coro Flow EstablishedPt in ICU Acute Renal Failure 6wFull recovery
*1******* 2
3 4
*1*******
*1******* *1*******
6 weeks later, in the clinic, he told me�Doctor, its Dribbling� � I did not believe
1w later, he told me �Doctor its like a Fountain�He tried to convince me and took out
a bottle of yellow liquid � O Yes I believe!
TO OUR TEAM, THIS IS A MIRACLE.HOWEVER WE KNOW THAT
IF WE DID NOT DO IT, MIRACLES WON�T HAPPEN!
xxxxxxxx xxxxxxxxxx

From international studies & our own Hospital Data, we know that Lytics are potentially hazardous & PPCI superior
We took a cautious start on1/2/2007 9A � 5P PPCI
1st Upgrade 1/8/2008 8A � 8P(*ICH = Intracranial bleeding)
2nd Upgrade 15/4/2009 24h PPCI (Pts ≧2 Risk Factors ICH*)
3rd Upgrade 7/11/2010 24h PPCI for all eligible Pts
Prior to each Upgrades, we perform PRESSURE TESTING39
PART 2: HOW?
18m
8m
18m

40
9a 5p
8A 8P 8A
PPCI 2007(No. of Patients)
2008(No. of Patients)
2009(No. of Patients)
2010(No. of Patients)
08:00 � 08:59 1 2 2 5
09:00 � 17:00 17 23 34 32
17:01 � 20:00 3 10 9 8
20:01 20:01 �� 07:5907:59 1 1 12 15
Lytics 2007(No. of Patients)
2008(No. of Patients)
2009(No. of Patients)
2010(No. of Patients)
08:00 � 08:59 0 1 0 0
09:00 � 17:00 11 8 1 1
17:01 � 20:00 7 5 2 0
20:01 20:01 �� 07:5907:59 20 22 13 5
E-PPCI System PRESSURE TESTING & Contextualization
1.2.2007
1.8.2008 15.4.2009
7.11.2010` 1.8.2008 15.4.2009
NightFall
DawnDawn
(18m) (8m)
(18m)

41
9a 5p
8A 8P 8A
PPCI System Pressure Testing & Contextualization Process
1.2.2007
1.8.2008 15.4.2009
7.11.2010
Change of number of patients undergoing PPCI in different period
0
10
20
30
40
50
60
70
2007 2008 2009 2010
Num
ber
of p
atie
nts
08:00 � 08:59 09:00 � 17:00 17:01 � 20:00 20:01 � 07:59
25

42
9a 5p
8A 8P 8A
PPCI System Pressure Testing & Contextualization Process
1.2.2007
1.8.2008 15.4.2009
7.11.2010
Change of the number of patients using LYTICS in different period
0
5
10
15
20
25
2007 2008 2009 2010
Num
ber
of p
atie
nts
08:00 � 08:59 09:00 � 17:00 17:01 � 20:00 20:01 � 07:59
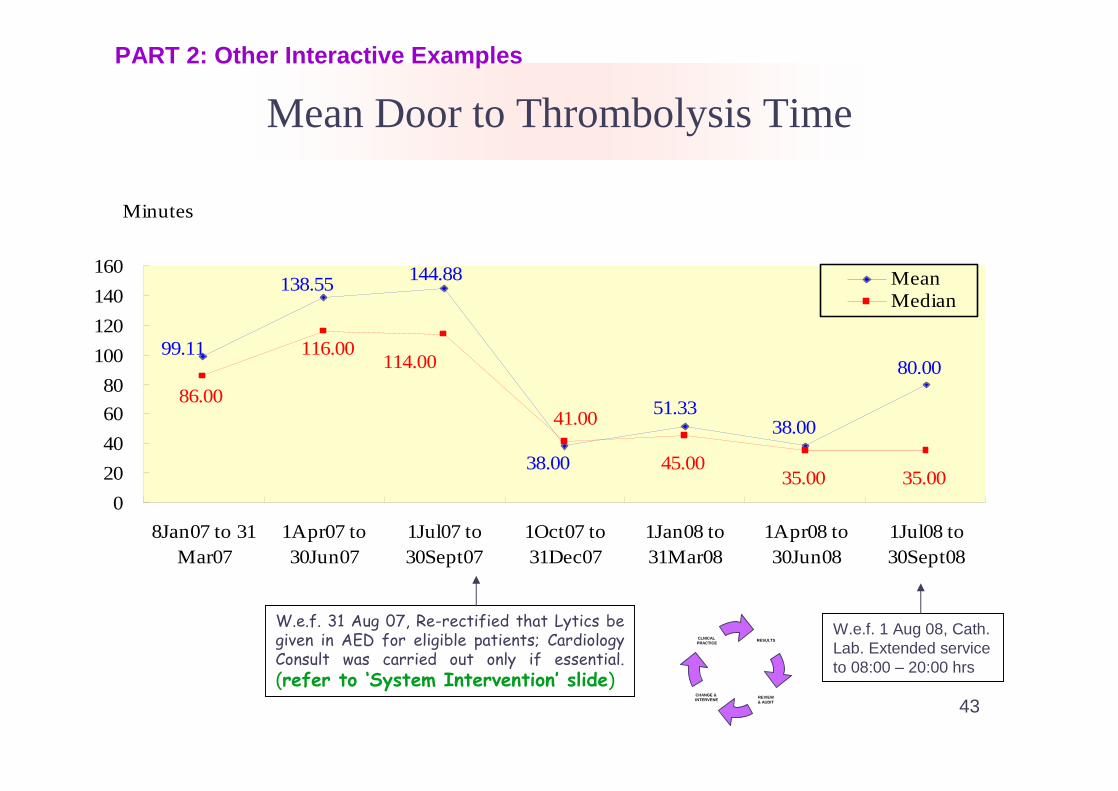
Mean Door to Thrombolysis Time
W.e.f. 31 Aug 07, Re-rectified that Lytics be given in AED for eligible patients; Cardiology Consult was carried out only if essential. (refer to �System Intervention� slide)
W.e.f. 1 Aug 08, Cath. Lab. Extended service to 08:00 � 20:00 hrs
Minutes
45.0035.00 35.00
99.11
138.55 144.88
38.00
51.3338.00
80.00
86.00
116.00
41.00
114.00
0
20
40
60
80
100
120
140
160
8Jan07 to 31Mar07
1Apr07 to30Jun07
1Jul07 to30Sept07
1Oct07 to31Dec07
1Jan08 to31Mar08
1Apr08 to30Jun08
1Jul08 to30Sept08
MeanMedian
43
RESULTS
REVIEW& AUDIT
CHANGE & INTERVENE
CLNICALPRACTICE
PART 2: Other Interactive Examples

Door to Balloon Time
124.78117.13
153.43140.88182.25131.00
277.00
127.00104.50
120.00106.00
188.00
127.00
277.00
0
50
100
150
200
250
300
8Jan07 to31 Mar07
1Apr07 to30Jun07
1Jul07 to30Sept07
1Oct07 to31Dec07
1Jan08 to31Mar08
1Apr08 to30Jun08
1Jul08 to30Sept08
Minutes
Mean
Median
44
RESULTS
REVIEW& AUDIT
CHANGE & INTERVENE
CLNICAL PRACTICE
Regular Review Meetings & seek for improvements

Queen Mary Hospital
瑪麗醫院
Mean LOS
Implementation of AMI CP w.e.f.
8Jan07
4.58
2.803.68
3.934.03
5.28
4.09
5.02
4.66
0
1
2
3
4
5
6
2005 2006 1Q 2007 2Q 2007 3Q 2007 4Q 2007 1Q2008 2Q 2008 3Q 2008
No. of Days
45
RESULTS
REVIEW& AUDIT
CHANGE & INTERVENE
CLNICALPRACTICE
Examine all Variance cases

4 Cardiology specialty trainees were recruited into the team since 1 Jul 2007 A B C
With effect from 31 Aug 07, we re-rectify the practice to administer Lytics in AED; Cardiology Consult was carried out only if essential.
A W.e.f. 1 July 2007, AED sent an Emergency Medicine Fellow for elective to
CCU for 3m A B Enhanced Division communication by weekly frontline team meeting in CCU
A B C Regular case review meetings with AED
A B Case Manager involvement in patient education & risk factors identification
C Stepwise Extension of Catheterization Laboratory service since 1.8.2008
C
System Interventions 2007, 2008: A Summary
Queen Mary Hospital
瑪麗醫院
Queen Mary Hospital
瑪麗醫院
A. Shorten DN-T B. Shorten DB-T C. Shorten LOS46
PART 2:

Queen Mary Hospital
瑪麗醫院
Queen Mary Hospital
瑪麗醫院47
3. Manpower Logistics
PART 2: HOW TO RUN A AMI CP?

Queen Mary Hospital
瑪麗醫院
Queen Mary Hospital
瑪麗醫院48
To Run a PPCI Program, Prerequisites
1. Unit (Program) has to have a critical no.of staff *
2. Expertise, Staff Training & Update3. Commitment: Intense Collaborations
* It can be Program based, with team up of expert persons - Nurses, Radiographers, Doctors alike from cluster hospitals & work on a destined site.
PART 2: HOW?

QMH 24 Hour Emergent Primary PCI for STEMI
3 Teams to run Emergency Cath Lab 24 hours =
Cath Lab Nurses : 5 (no �Technician� post in QMH CCL)3 Nursing Teams (2 nurses each, 1 additional nurse from the CCU) - weekly rotations
Radiographer : 1 (Daily standby rota)
Cardiologists : (For PCI = Need 1 Interv Cardiologist + 1 Cardiac Fellow)
Interv Cardiologist A � All Mon, Wed, FridaysInterv Cardiologist B � All Tues, Thurs, Sat, Sun
� SERVICE PLEDGE� OFF Site Call - ALL personnels on site within 1 h of call *
PART 2: HOW?

Important Principles in Team Building
法 理 情
Is it Legitimate? Is it Reasonable? Is it Considerate?
50
Discussion Slides
51
法On Call system & Compensation:We have three Team of Nurses on weekly off-site call.Each Team is composed of 2 nurses.Therefore they will have 52 x 2 Sundays + 17 x 2 PH (Total = 138 days) to compensate.
Now the compensation system is =For Sundays:If the staff does not need to come back or come back to work less than 4h � One Saturday off will be compensatedIf the staff comes more than 4h � One Weekday will be compensated
For PH:If the staff does not need to come back � One Saturday off will be compensatedIf the staff comes back to work for whatever length of time � One Weekday off will be compensated
Discussion Slides

52
理 情Compassionate off after on-call work:
If the staff come back to work & off before 12 Midnight �she should work as usual the next day.
If the staff come back to work & off before 4am �she may take the next day morning off for rest
If the staff come back to work & off after 4 am �she may take the next day off for rest.
(Our previous emergency patient statistics is = Staff need to work after 4 am ~ once every 2 months).
TENSILITY & FLEXIBILITYImportant Rule of Thumb : * YOU MUST consider your staff first *
Discussion Slides

53
38 37
67
50
6
24 25 26
02
6
11
0
10
20
30
40
50
60
70
80
08:01 - 16:00 16:01 - 24:00 00:01 - 08:00
2007
2008
2009
2010
Time of Performing E-PPCI
Time
No.
of
Cas
es
2007 2008 2009 2010 2007 2008 2009 2010
24 Hour Emergent Primary PCI for STEMI
Resource Issues, some Thoughts
It will be upto the individual Hospital�s Strategic Planning & internal allocation of resource
Central Support + a �Direction Sense� is Important (Cannot be didactic because of local differences)
Re-organisation of Service model eg Program/Cluster base may be further explored
PART 2: HOW?

QMH AMI_CLINICAL PATHWAY :
Queen Mary Hospital
瑪麗醫院
Queen Mary Hospital
瑪麗醫院55
4. Human Touch
PART 2: HOW?

QMH AMI_CLINICAL PATHWAY :
Queen Mary Hospital
瑪麗醫院
Queen Mary Hospital
瑪麗醫院56
� Our Experience, the CP is not a Top-down process, rather an experiential ( experimental) journey of the frontliner
�We know that by following the CP, patients will have a better chance of survival.
�We see miracles
�In the process, we build up an enviable Team with motivation, determination & highly professional.
�We feel we are doing the right thing
PART 2: HOW?

QMH AMI_CLINICAL PATHWAY :
Queen Mary Hospital
瑪麗醫院
Queen Mary Hospital
瑪麗醫院57
CONCLUSIONS
Part 1 & 2

THE QMH HEART CENTREBird�s eye view of the Present & Future; (Original version 24.3.2007) Updated 28.5.2011
ADULT CARDIOLOGYCARDIOTHORACIC
SURGERYPAEDIATRIC
CARDIOLOGY
K19N Cath Lab x2CCU 8 bed Cardiac Ward 16 bed
F5-OT D5-Ward C5/E5-ICU CG-Cath Lab x1 A5-Ward
Joint venture- Heart Transplant Program- Tues am Pre-op Echo- Tues pm Join Preop con- PAC at D5
OPD�SS6 Cardiac x2S6 ICD/PPMS7 Arrhythmia x1C1 GS/PenJ1 Private
Laboratories
Non-Invasive InvasiveAG/ K19S-side Cath Lab K19N
2 echos 2 echos2 treadmill 1 treadmillHoltersCardiomemos LindaAmbu BP�s Sam (NO)
Yin Wah (NO)Peter Chan (NO) SharfaHau Yee, Cecilia, Yuen Yee EstherKelly, Winnie, Dorothy Wah Fong
Alta Kan (WM)
Florence (NO)Siu Kum (NO)Lorraine (NO)
Mei LinHarbinderOliverPui MingJackieWai LingMei YiPik SamMan SinVeniceDoraBeckyWinnyNancyPun TuenCorinaGraceLee Wai ManEdwinChung YanAu Tat LongRaymond WanEugenia LawAh Bo (PT)
SUBSPECIALTIES
INTERVEN PACE Clin car Clin Car Heart Failure ECMO Congenital StemCARDIO & Echo & CMR & Transplant Heart Ds Cell
S Lee R Chan YM Lam C Chan YM Lam KL Wong YM Lam D SiuR Chan HF Tse C Chan YM Lam C Chan HF Tse L Lam D Siu K ChanYM Lam
(Fellows: PH Chan, JJ Hai, S Lam, K Chan, KL Wong, Frankie Tam, Arthur Yung, Anthony Wong)
YC Pan,TF Tse,R Wang,W Chen,PK Lee,KK Chan,CK Lau,SF Chow,KK Hui,KS Ho,CH Cheng,SL Lo,YT Tai,CK Wong,D Ho,CP Lau,W Ng,PY Lee,WH Chen
Pwh- Yu, Eugene Fung(N), Joseph Yu,G Yip - Yu mo(Brompton) -Qeh- Duncan, Mike,KT Sam,Tsang(o),So(o) Ho - - Boron -Pyn- Tse Tat Sun, Kin KK Chan,Choi (Aus) Tsui Ko(Berlin) - - -Uch- CK Chan Yu Chiu Sun Leung - - - -Pmh- Wu cw,Tsui pt Mok, Chan ny Ting,choi - - - -Tmh- Chow Liang, Tse Steve Lai -Gh � Chow WH ,Jim K Fan - - (Elaine Chau 2sessions/w) - -Rh � Lau Wong mh Keung - - - -Kwh-Leung Sum kin Leung Sum kin - - - - -
GH Adult Cardiology/ TWH Cardiology / CRPMedical Rehab beds
20 + 20 6 + 62 Con, 2 AC, 5 MO�s (1 Con) 1 MO
(KLC,, TM Tse,CW Lo,OH Kwok,P Hon,FL Kay,CH Lee,WF Lam)
Ground-workAMI Pathway Dg policy(SFI/Special): Statin,Bosentan,Via
CMS-coro,Holter Human Resources- RA,CO,RNPAC system HAHO/ CCC / CTDAG / HKCPCommunity: Legco/PRO/Black/News/Firewall
ICU 1: 1 CCU/HDU/BMT - 1: 2.1
CCU / K19A / P 3 / 3 + NO
N 3 / 1
17 CCU + 7 CWJoint venture ACHD- Adult Congenital Heart Clinic
J1 Structural Monday pmJ2 Arrhythmia Tuesday pmJ3 Echo Clinic Wed pm

59
CONCLUSION:
AMI is a disease that haunts the developed world & carries a high Mortality & Morbidity. Our experience is that the Clinical Pathway fosters an efficient & responsible management with favourable outcomes. It is a mangement system that is labour intensive & require sophistication, determination & collaborations. It is achievable in QMH & we believe it will also be achievable in other HA Hospitals.

�Serve With Heart�Queen Mary Hospital
瑪麗醫院
Queen Mary Hospital
瑪麗醫院
��QMH Acute Myocardial Infarction QMH Acute Myocardial Infarction Clinical Pathway TeamClinical Pathway Team��
ER
Audit, T & D, CQIMSW
CARDIOLOGISTS
Radiographers, CCL Nurses
CCU & Ward Physio, OT, Dietitian
THANK YOU!