Embed Size (px)
Citation preview

Therapeutics, Targets, and Chemical Biology
Amplification of EGFR Wild-Type Alleles inNon–Small Cell Lung Cancer Cells ConfersAcquired Resistance to Mutation-SelectiveEGFR Tyrosine Kinase InhibitorsShigenari Nukaga1, Hiroyuki Yasuda1, Katsuya Tsuchihara2, Junko Hamamoto1,Keita Masuzawa1, Ichiro Kawada1, Katsuhiko Naoki3, Shingo Matsumoto2,Sachiyo Mimaki2, Shinnosuke Ikemura2, Koichi Goto4, Tomoko Betsuyaku1, andKenzo Soejima1
Abstract
EGFR-mutated lung cancers account for a significant subgroupofnon–small cell lung cancers overall. Third-generation EGFR tyro-sine kinase inhibitors (TKI) are mutation-selective inhibitors withminimal effects onwild-typeEGFR. Acquired resistancedevelops tothese agents, however, the mechanisms are as yet uncharacterized.In this study, we report that the Src–AKT pathway contributes toacquired resistance to these TKI. In addition, amplification of EGFR
wild-type alleles but not mutant alleles was sufficient to conferacquired resistance. These findings underscore the importance ofsignals from wild-type EGFR alleles in acquiring resistance tomutant-selective EGFR-TKI. Our data provide evidence of wild-type allele-mediated resistance, a novel concept of acquired resis-tance in response to mutation-selective inhibitor therapy in cancertreatment. Cancer Res; 77(8); 1–12. �2017 AACR.
IntroductionEGFR-mutated lung cancers comprise a significant subgroup of
non–small cell lung cancer (NSCLC; refs. 1–3). In general, EGFRtyrosine kinase domain somatic mutations activate EGFR bypromoting the active conformation of EGFR (4–7). ActivatedEGFR transduces signals to downstream pathways, such as thephosphoinositide 3-kinase (PI3K)–AKT and MEK–ERK mitogen-activated protein kinase (MAPK) pathways. After the identifica-tion of EGFR-activating mutations and response to first-genera-tion EGFR tyrosine kinase inhibitors (EGFR-TKI; refs. 8–10), thetreatment strategy for NSCLC patients harboring these mutationschanged dramatically. The significant improvement of prognosisof lung cancer patients with EGFR mutations by first- (gefitinib
and erlotinib) and second- (afatinib) generation EGFR-TKIs hasbeen repeatedly demonstrated bymultiple clinical trials (11–13).However, lung cancer cells inevitably acquire resistance to theseinhibitors after approximately one year (14–16).
Multiple mechanisms of acquired resistance to first- and sec-ond-generation EGFR-TKIs have been identified to date—includ-ing the EGFR T790M gatekeeper mutation (17, 18), transforma-tion to small cell lung cancer (SCLC; refs. 19, 20), and adaptivebypass pathway activation through the MET (21), AXL (22), andFGFR1 (23) axes. Of these, the EGFR T790M mutation is respon-sible for acquired resistance in approximately 50% of cases. TheT790 residue is located at the entrance to ahydrophobic pocket onthe posterior side of the ATP-binding cleft. As such, the T790Mmutation induces a conformational changewithin the EGFR ATP-binding pocket, resulting in the steric hindrance of first or second-generation EGFR-TKIs (17). Coincidentally, EGFR T790M alsoenhances the affinity between ATP and its binding pocket (24),thereby synergistically conferring resistance to EGFR-TKIs. Toaddress this issue, third-generation EGFR-TKIs, such as osimerti-nib (AZD9291; ref. 25), rociletinib (CO-1686; ref. 26), andnazartinib (EGF816; ref. 27), have been developed that irrevers-ibly bind the EGFR ATP-binding pocket by forming a covalentbond with the C797 residue at pocket periphery, simultaneouslyblocking ATP binding due to the increased affinity. Interestingly,these third-generation EGFR-TKIs are also effective for the major-ity of EGFR-activating mutations, such as in-frame deletions inexon 19 and the L858R point mutation in exon 21 (28). Further-more, mutation selectivity of third-generation EGFR-TKIs hasbeen reported in preclinical and clinical models (25–27). Thewide therapeutic window of third-generation EGFR-TKIs mirrorsthe significant efficacy and safety of these agents performed inmultiple clinical trials (29, 30). Third-generation EGFR-TKIs are
1Division of Pulmonary Medicine, Department of Medicine, Keio University,School of Medicine, Tokyo, Japan. 2Division of Translational Research, Explor-atory Oncology Research and Clinical Trial Center, National Cancer Center,Chiba, Japan. 3Keio Cancer Center, Keio University School of Medicine, Tokyo,Japan. 4Division of Thoracic Oncology, National Cancer Center Hospital East,Chiba, Japan.
Note: Supplementary data for this article are available at Cancer ResearchOnline (http://cancerres.aacrjournals.org/).
Corresponding Authors: Hiroyuki Yasuda, Keio University School of Medicine,35 Shinanomachi, Shinjuku-ku, Tokyo 160-8582, Japan. Phone: 813-3353-1211;Fax: 813-3353-2502; E-mail: [email protected]; Kenzo Soejima,[email protected]; and Katsuya Tsuchihara, Division of Transla-tional Research, Exploratory Oncology Research and Clinical Trial Center,National Cancer Center, 6-5-1 Kashiwanoha, Kashiwa, Chiba 277-8577, Japan.E-mail: [email protected]
doi: 10.1158/0008-5472.CAN-16-2359
�2017 American Association for Cancer Research.
CancerResearch
www.aacrjournals.org OF1

also subject to acquired resistance. It is important to fully clarifythe mechanisms of acquired resistance to third-generationEGFR-TKIs to improve the prognosis of lung cancer patientsharboring EGFR mutations. The mechanisms clarified to dateinclude C797S or L798I mutation (31, 32), constitutive MAPKpathway activation by mutated KRAS or MEK (33), or bypasspathway activation via MET or ERBB2 (32, 34–36). However,the mechanisms underlying acquired resistance to third-gener-ation EGFR-TKIs are not fully clarified.
In this study, we elucidated novel mechanisms underlyingacquired resistance to third-generation EGFR-TKIs by whole-exome sequencing analysis. Notably, we determined that Src–AKT pathway activation and EGFR wild-type allele amplificationcan both contribute to EGFR-TKI acquired resistance, the latter ofwhich might possibly be due to the decreased inhibitory pressurefor EGFR wild-type by mutation selective third-generation EGFR-TKIs. Our findings highlight the importance of EGFR wild-typeallele-mediated signaling in acquired resistance to mutant-selec-tive EGFR-TKIs.
Materials and MethodsReagents
Erlotinib, afatinib, rociletinib, andwortmanninwere purchasedfrom LC Laboratories. Osimertinib was purchased from SelleckChemicals (Houston). Nazartinib was purchased from ApexBio.Bosutinib was purchased from Cayman Chemical). Cetuximabwaspurchased fromKeioUniversityHospital (Tokyo, Japan).TotalEGFR antibody (#2232), EGFR E746-A750del–specific antibody(#2085), total AKT antibody (#9272), phospho-AKT (S473/D9E)antibody (#4060), total p44/42 MAPK antibody (#9102S), phos-pho-p44/42 MAPK (T202/204) antibody (#9101S), E-cadherinantibody (#3195S), vimentin antibody (#5741S), total Src anti-body (#2108), Phospho-(Tyr416)-Src antibody (#2101S), PTENantibody (#9559), and PI3 kinase p110 alpha antibody (#4255S)were purchased from Cell Signaling Technology). The HA-tag(ab18181) and integrin beta 1 (ab52971) antibodies were pur-chased fromAbcam).Phospho-EGFR(Y1068)antibody (44788G)was purchased from Invitrogen/Life Technologies. Actin antibodywas purchased from Sigma-Aldrich.
Cell linesThe PC9 (EGFR E746-A750del) and H1975 (EGFR L858R þ
T790M)humanNSCLC cell lines were obtained fromDr. SusumuKobayashi (Beth Israel Deaconess Medical Center, Boston, MA)and the ATCC, respectively. Cells were cultured in RPMI1640growth medium supplemented with 10% FBS at 37�C in ahumidified 5% CO2 incubator. Cell authentication for PC9 andH1975 was performed by the authors in June 2015 using geneticprofiling of polymorphic short tandem repeat (STR) loci (Takara).
Cell proliferation assayMTS cell proliferation assays were performed as previously
described (37). Briefly, 2 � 103 cells/well were seeded in 96-wellplates and treated with EGFR-TKI or dimethyl sulfoxide (DMSO)vehicle 24 hours later. Absorbance was measured 72 hours aftertreatment. All experiments were performed at least three times.
Phospho-receptor tyrosine kinase arrayThe human phospho-receptor tyrosine kinase (phospho-RTK)
array kit was purchased from R&D Systems) and screened accord-
ing to themanufacturer's protocol with 150 mg of protein for eachexperiment. Signal intensity was calculated using LumiVisionAnalyzer software.
Establishment of the H1975 EGFR stable cell lineH1975 cells with stable EGFR wild-type or C797S overexpres-
sion were generated by retroviral infection using MigR1-EGFRconstructs that harbor a GFP as previously described (5). Briefly,Phoenix-Ampho cells were transfected with 15 mg of wild-type orC797S EGFR using Lipofectamine 2000. Viral supernatant wascollected 2 days after transfection and applied to H1975 cells onretronectin-coated plates (Takara) for 24 hours. EGFR-overexpres-sing H1975 cells were sorted by a FACS MoFlo XDP (BeckmanCoulter) based on GFP expression. Purified cells were then grownin RPMI with 10% FBS.
Western blot analysisCells were treated with increasing concentrations of EGFR-TKIs
(0.1–1 mmol/L). Cetuximab was used at concentrations of10 mg/mL. Cells were lysed in Cell Lysis Buffer (Cell SignalingTechnology), andequivalent amountsofproteinwere separatedbySDS-PAGE and transferred to polyvinylidenefluoridemembranes.Themembraneswere incubatedovernightwithprimary antibodiesat 4�C and then with secondary antibodies for 1 hour. Immuno-reactive proteins were visualized with LumiGLO reagent andperoxide (Cell Signaling Technology), then exposed to X-ray film.
Apoptosis assayCells were seeded in 6-well plates (50,000/well) and were
treated with rociletinib (1 mmol/L) and cetuximab (10 mg/mL)individually or in combination for 72 hours. Control cells weretreated with DMSO. Apoptosis was monitored using the TACSAnnexin V–FITC Apoptosis Detection Kit (R&D Systems) accord-ing to the manufacturer's protocol. The proportion of apoptoticcells was evaluated by flow cytometric analysis using a GalliosFlow Cytometer system (Beckman Coulter).
Quantitative RT-PCR and quantitative PCRTotal RNA was isolated from cultured cells using an RNeasy
Mini Kit (Qiagen) and genomicDNAwas isolated using aDNeasyBlood & Tissue Kit (Qiagen). RNA was subjected to reversetranscription using the High-Capacity RNA-to-cDNA Kit (LifeTechnologies) according to the manufacturer's protocol. Quan-titative RT-PCR was performed using fluorescent SYBR Green andan ABI Prism 7000 Sequence Detection System (Life Technolo-gies). Human GAPDH was used to normalize input cDNA. TheLINE1 repetitive element was used as a reference gene for EGFRcopy-number analysis. The primers used in this study are shownin Supplementary Table S1.
FISHEGFR and chromosome 7 FISH analysis was performed by
Genetic lab Co., Ltd. using Vysis LSI EGFR SpectrumOrange andCEP 7 SpectrumGreen probes, respectively.
Standard Sanger sequencing of PIK3CAIsolated cDNA from H1975 cells was used as template in PCR
reactions for PIK3CA. Amplified PIK3CA was sequenced andcompared with the National Center for Biotechnology Informa-tion reference sequence NM_006218.3.
Nukaga et al.
Cancer Res; 77(8) April 15, 2017 Cancer ResearchOF2

PIK3CA siRNA knockdownCells were transfected with PIK3CA-specific siRNA (#S10520;
Life Technologies) or negative control siRNA (Ambion SilencerSelect Negative Control mix, Life Technologies) using siLentFecttransfection reagent (Bio-Rad) according to the manufacturers'protocols. PIK3CAqRT-PCRwas used to confirm gene knockdown.
Mouse xenograft modelAll animal experiments were approved by the Laboratory Ani-
mal Center, Keio University School of Medicine (Tokyo, Japan).Female BALB/c-nu mice were purchased from Charles River. Micewere anesthetized with ketamine and PC9-COR#9 cells weresubcutaneously injected in a Matrigel suspension. Calipers wereused to measure tumor volume. Once average tumor volumereached 150mm3, mice were randomized to receive vehicle alone,cetuximab (1 mg/mouse twice per week, intraperitoneally), roci-letinib (30mg/kgdaily, orally), or a combination of both. Animalswere humanely sacrificed and tumor tissues were harvested.
Whole-exome sequencingWhole-exome sequencing libraries were prepared with 3 mg
of DNA. The exomes were captured using the SureSelect HumanAll Exon V5þUTRs Kit (Agilent Technologies) according to themanufacturer's instructions and then sequenced using a HiSeq1500 system (Illumina) to generate 100-bp paired-end data.The whole-exome sequencing data were deposited in the DDBJdatabase. Accession numbers: DRA004904, PRJDB5021, andSAMD00056514-SAMD00056521
Variant callingSequence reads were aligned to the human reference genome
UCSC hg19 using the Burrows-Wheeler Aligner program (BWA,http://bio-bwa.sourceforge.net/). Single-nucleotide variants (SNV)and insertions and deletions (INDEL) were called and annotatedusing theGenomeAnalysis Toolkit softwarepackage (GATK,http://www.broadinstitute.org/gatk/). Sequencing artifacts were filteredout using custom filters (GATK confidence score, �50; number ofvariant reads ineachdirection,�1; variant allele frequency,�10%).Known germline variants were filtered out using data from dbSNPbuild 131, the 1,000 Genomes Project (Phase 1 exome data,released May 21, 2011), 1 Japanese genome, and 299 in-houseJapanese exomes.
Copy number analysisCNVs in resistant cells were analyzed from exome sequence
data. The log ratio of depth coverage between parental andresistant cells was calculated using the GATK Depth of Coveragetool. CNV segmentswere then called from the log ratio of depth ofcoverage using the ExomeCNV package (38).
Statistical analysisStatistical analysis was performed using GraphPad Prism soft-
ware, version 4.0 (GraphPad Software). Two-sided Student t testswere used for comparisons, with P < 0.05 regarded as statisticallysignificant.
ResultsEstablishment of third-generation EGFR-TKI–resistant cells
To clarify the mechanisms underlying acquired resistance tothird-generation EGFR-TKIs, such as osimertinib (AZD9291) and
rociletinib (CO-1686), we established third-generation EGFR-TKI–resistant cells using a dose-escalation method. PC9 andH1975 cells were cultured with rociletinib or osimertinib. Theinitial concentration was 0.03 mmol/L, and this was incremen-tally increased to 1 mmol/L. After several months of exposure,resistant cell lines, rociletinib-resistant PC9 (PC9-COR), osi-mertinib-resistant PC9 (PC9-AZDR), rociletinib-resistantH1975 (H1975-COR), and osimertinib-resistant H1975(H1975 AZDR) were established. Their resistance to a first-(erlotinib), third-generation (rociletinib, osimertinib, or nazar-tinib) EGFR-TKIs was confirmed by the MTS cell proliferationassay (Fig. 1). The calculated IC50 values are summarized inSupplementary Table S2. Notably, the resistant cells displayedcross-resistance to all third-generation EGFR-TKIs examined inthis study, suggesting that the mechanisms of resistance to third-generation drugs may not be inhibitor specific. Further, resistantcells also showed a diminished propensity to undergo treatment-induced apoptosis (Supplementary Fig. S1), indicating that thecells acquired resistance to third-generation EGFR-TKIs.
Whole-exome sequencing of parental and EGFR-TKI–resistantcells
Bypass pathway activation is consistently reported as one of themechanisms by which cells acquire resistance to EGFR-TKIs. Assuch, we first examined the phosphorylation levels of multiplereceptor tyrosine kinases in our resistant PC9 and H1975 cellswith a human phospho-RTK array kit, but did not observe anyactivation of reported bypass pathways (HER2, HGFR, IGF-1R,and AXL signaling; Supplementary Fig. S2).
To clarify the heterogeneity of potential resistance mechan-isms, the PC9-COR, PC9-AZDR, H1975-COR, and H1975-AZDR lines were subcloned to isolate resistant clones (Supple-mentary Fig. S3). DNA isolated from the parental and resistantcell clones was then subjected to whole-exome sequencing.Quality of the whole-exome sequencing results and copy num-ber alterations are summarized in Supplementary Table S3 andSupplementary Fig. S4. Several genetic alterations potentiallyrelevant to EGFR-TKIs sensitivity were detected (Table 1),including some already reported. For instance, osimertinibresistance can occur via oncogenic KRAS signaling (33). In ourmodel, KRAS G13D was identified in PC9-AZDR clones (Sup-plementary Fig. S5), supporting the validity of our findings.EGFR C797S or L798I was not found in the resistant cells.
Epithelial-to-mesenchymal transition phenotype and AKTpathway activation in third-generation EGFR-TKI–resistantcells
Parental H1975 cells harbor a heterozygous PIK3CA G118Dmutation. Interestingly, the PIK3CA wild-type allele was lost inthree of the resistant clones—H1975-AZDR#1 and #3, andH1975-COR#3, leading to a loss of heterozygosity (Supplemen-tary Table S4; Supplementary Fig. S6A and S6B). The activatingPIK3CA G118D mutation is found in various cancer types,including endometrium (39) and colorectal (40, 41) cancers. Inorder to investigate whether acquired homozygosity of PIK3CAG118D could functionally induce resistance to EGFR-TKIs, weexamined the impact of PIK3CA inhibition on EGFR-TKI resistantcells using the PIK3CA inhibitor wortmannin. Although effectivewhen used in combination with EGFR-TKI in parental H1975cells, wortmannin was unable to restore EGFR-TKI sensitivity inthe H1975-resistant clones (Supplementary Fig. S6C and S6D).
EGFR Wild-Type Allele Amplification Induces Resistance
www.aacrjournals.org Cancer Res; 77(8) April 15, 2017 OF3

Further, the siRNA-mediated knockdown of PIK3CA gene expres-sion in the H1975-resistant clones also failed to restore EGFR-TKIsensitivity (Supplementary Fig. S6E and S6F). These data indicatethat acquired homozygosity of the PIK3CA G118D mutation did
not contribute to the acquired resistance to EGFR-TKI in H1975-resistant cells.
While performing these experiments, we noticed a change incell morphology where the H1975-resistant cells exhibited aspindle cell-like morphology (Fig. 2A). Epithelial-to-mesenchy-mal transition (EMT) is reported to occur in EGFR-resistantNSCLC (42). To confirm whether H1975 cell clones acquired amore mesenchymal phenotype, we analyzed EMT markers byWestern blotting. Consistently, expression of the mesenchymalmarker vimentin and the epithelial E-cadherin was upregulatedand downregulated in the resistant clones at the protein level,respectively (Fig. 2B). Moreover, both total and phosphorylatedSrc were elevated in H1975-resistant cells. Next, we examined theeffect of EGFR-TKI treatment on EGFR downstream pathwayactivation, including AKT and MAPK, in H1975-resistant cells.EGFR and ERK1/2 phosphorylation were efficiently inhibited by
Table 1. Results from whole-exome sequencing show several geneticalterations potentially relevant to EGFR-TKI sensitivity
Cell line Genetic alterations
PC9 EGFR E746_A750delPC9-COR#9 EGFR E746_A750delþEGFR wild-type amplificationPC9-AZDR#4 EGFR E746_A750delþKRAS G13DPC9-AZDR#5 EGFR E746_A750delþKRAS G13DH1975 EGFR L858R/T790MþPIK3CA G118D (heterozygosity)H1975-COR#3 EGFR L858R/T790MþPIK3CA G118D (homozygosity)H1975-AZDR#1 EGFR L858R/T790MþPIK3CA G118D (homozygosity)H1975-AZDR#3 EGFR L858R/T790MþPIK3CA G118D (homozygosity)
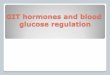
Figure 1.
Establishment of third-generation EGFR-TKI–resistant cells. MTS cell proliferation assays for PC9 and H1975 parental and resistant cells treated withincreasing concentrations of the indicated EGFR-TKIs for 72 hours. Error bars, SD.
Nukaga et al.
Cancer Res; 77(8) April 15, 2017 Cancer ResearchOF4

rociletinib and osimertinib treatment; however, limited effectswere observed in AKT phosphorylation in H1975-resistant cellswhen compared with H1975 parental counterparts (Fig. 2C).Integrin b1/Src/AKT-mediated bypass signaling has previouslybeen reported in erlotinib-resistant NSCLC (43). Consistent withthis report, we found that integrin b1 and phospho-Src wereincreased at the RNA and protein levels, respectively, in
H1975-resistant clones (Fig. 2B and D). A loss of PTEN andsubsequent AKT pathway activation facilitate EGFR-TKI resis-tance inmutant lung cancer (44); however, PTEN expression wasintact in H1975-resistant cells (Fig. 2B and E). To examinewhether Src–AKT pathway activation contributed to the acquiredresistance to third-generation EGFR-TKI resistance, we per-formed MTS proliferation assays on H1975 clones treated with
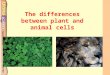
Figure 2.
EMT and Src–AKT pathway activationin third-generation EGFR-TKI–resistant cells. A, Representativepictures of parental and resistantH1975 cells.B,Western blot analysis ofH1975 parental and resistant (COR#3,AZDR#1) cells for E-cadherin,vimentin, integrin b1, total (t-) andphosphorylated (p-) Src, PTEN, andb-actin. C, Western blot analysis fortotal (t-) and phosphorylated (p-)EGFR, AKT, ERK1/2, and b actin inH1975 parental and resistant (COR#3,AZDR#1) cells. D, Integrin b1 (ITGB1)gene expression relative to that ofGAPDH in H1975 parental cells andresistant clones. Error bars, SD. E,PTEN gene expression relative to thatof GAPDH in H1975 parental cells andresistant clones. Error bars, SD. F,MTScell proliferation assays followingtreatment with the indicated EGFR-TKI concentrations with or withoutbosutinib or dasatinib in H1975parental cells and resistant clones(H1975-COR#3, H1975-AZDR#1). Errorbars, SD. G, Western blot analysis fortotal (t-) and phosphorylated (p-) Srcand b-actin in H1975 parental cellstreated with the indicatedconcentrations of bosutinib ordasatinib.
EGFR Wild-Type Allele Amplification Induces Resistance
www.aacrjournals.org Cancer Res; 77(8) April 15, 2017 OF5

third-generation EGFR-TKIs in the presence or absence of the Srcinhibitors dasatinib or bosutinib. Interestingly, both dasatiniband bosutinib partially restored sensitivity to third-generationEGFR-TKIs (Fig. 2F and G), suggesting that Src–AKT pathwayactivation may contribute to the acquired resistance to third-generation EGFR-TKIs.
EGFRwild-type allele amplification induces resistance to third-generation EGFR-TKIs
Notably, our exome sequencing data revealed an amplifi-cation of the EGFR gene locus on chromosome 7 (Fig. 3A). To
confirm this finding, chromosome 7 and the EGFR gene wereanalyzed by FISH and scored using the ratio EGFR signal tothat of chromosome 7 (Fig. 3B). PC9 parental cells harborEGFR gene amplification; however, the ratio of signals becamehigher in PC9-COR#9 clones when compared with parentalcounterparts (Supplementary Table S5). In addition, genomicDNA qPCR for the EGFR loci in the PC9-COR clones confirmedthe amplification (Fig. 3C). Furthermore, the EGFR wild-typecopy number and total EGFR expression were markedlyincreased in PC9-COR#9 cells (Supplementary Table S6; Fig.3D). The relative number of tags for the wild-type EGFR allele
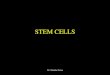
Figure 3.
EGFR wild-type allele amplification inrociletinib-resistant clones. A, Copy-number variants (CNV) in PC9-COR#9cells analyzed from exome sequencedata. B, Two-color FISH analysis ofPC9 parental and PC9-COR#9 cells.Green and red signals indicate CEP7and EGFR, respectively. C, Relativegene copy number of EGFR whencompared with LINE1. D,Western blotanalysis of total (t-) EGFR, exon 19deletion-specific EGFR (EGFRdel19),and b-actin in PC9 parental andresistant cells. E, Relative geneexpression in PC9 parental andresistant cells. Error bars, SD. F,Western blot analysis for total (t-) andphosphorylated (p-) EGFR, exon 19deletion–specific EGFR (EGFRdel19),total (t-), and phosphorylated (p-)AKT, ERK1/2, and b-actin in PC9parental and resistant cells.
Nukaga et al.
Cancer Res; 77(8) April 15, 2017 Cancer ResearchOF6

(31 tags) was about one fourth (0.25 times) that of the mutantallele (127 tags) in PC9 parental cells; however, the wild-typeallele was approximately 8.5-fold more prevalent in PC9-COR#9 cells (512 vs. 60 tags for the wild-type and mutantalleles, respectively). These data indicate that the amplifiedEGFR wild-type allele likely conveyed resistance to third-gen-eration EGFR-TKIs.
We next examined EGFR ligand expression to evaluate thepossibility of ligand-induced activation of EGFR (45). Untilnow, seven EGFR ligands have been identified: epithelialgrowth factor (EGF), amphiregulin, heparin-binding EGF-likegrowth factor (HB-EGF), epiregulin, TGFa, epigen, and beta-cellulin. Quantitative RT-PCR analysis revealed an increasedexpression of all seven ligands in PC9-COR cells and PC9-COR#9 cells compared with PC9 parental cells (Fig. 3E). Asexpected, the inhibition of phosphorylation of EGFR, AKT, and
ERK by rociletinib was attenuated in the PC9-COR#9 clonewhen compared with the PC9 parental cells (Fig. 3F). Theseresults indicated that EGFR wild-type allele amplification likelyinduces the acquired resistance to third-generation EGFR-TKIsthrough EGFR ligand-induced activation.
To ascertain the plausibility of the aforementioned situation,we expressed HA-tagged wild-type EGFR in H1975 parental cellsand evaluated their sensitivity to rociletinib andosimertinib in thepresence of EGF. When compared with mock-transfected H1975cells, wild-type EGFR-overexpressingH1975 cells developed resis-tance to rociletinib and osimertinib upon EGF administration(Fig. 4A andB), and rescued EGF-induced EGFR, AKT, andERK1/2phosphorylation (Fig. 4C). Thus, these data indicate that EGFRwild-type allele amplification and concomitant EGFR ligandexpression contribute to acquired resistance to third-generationEGFR-TKIs.
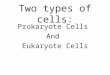
Figure 4.
EGFR wild-type allele amplification contributes to third-generation EGFR-TKI resistance. A, Western blot analysis of H1975 cells transduced with emptyvector (mock) or HA-tagged EGFR.B,MTS cell proliferation assays for H1975mock and H1975 EGFR cells treatedwith the indicated EGFR-TKI concentrationswith orwithout EGF (10 ng/mL, 100 ng/mL) for 72 hours. Error bars, SD. C, Western blot analysis of H1975 mock and H1975 EGFR cells treated with the indicatedconcentrations of EGF and rociletinib for phosphorylated (p-) and total (t-) EGFR, AKT, ERK1/2, and b-actin.
EGFR Wild-Type Allele Amplification Induces Resistance
www.aacrjournals.org Cancer Res; 77(8) April 15, 2017 OF7

Rociletinib/cetuximab cotreatment overcomes EGFR wild-type–mediated acquired resistance in vitro and in vivo
Concomitant EGFRwild-type amplification and ligand expres-sion promoted us to determine whether the inhibition of EGFR
ligand binding would be sufficient to restore sensitivity to roci-letinib in PC9-COR#9 cells. For this, we performed MTS assays inthe presence of cetuximab, an anti-EGFR antibody that blocksligand binding. As a single agent treatment, cetuximab had no
Figure 5.
Rociletinib and cetuximab combination treatment overcomes EGFR wild–type–mediated acquired resistance in vitro. A, MTS cell proliferation assays forPC9 and PC9-COR#9 cells treated with the indicated concentrations of cetuximab for 72 hours. Error bars, SD. B,MTS cell proliferation assays of PC9-AZDR#5 cellstreated with the indicated concentrations of cetuximab and osimertinib for 72 hours. Error bars, SD. C, MTS cell proliferation assays for PC9-COR#9 cellstreatedwith the indicated concentrations of rociletinib and cetuximab for 72hours. Error bars, SD.D,Westernblot analysis of phosphorylated (p-) and total (t-) EGFR,AKT, ERK1/2, and b-actin in PC9-COR#9 cells treated with the indicated concentrations of rociletinib and cetuximab for 8 hours. E, Flow cytometric datafor PC9-COR#9 cells treated with DMSO, rociletinib, cetuximab, and rociletinb/cetuximab in combination for 72 hours. The numbers (%) indicate the proportion ofAnnexin V–FITC- and/or propidium iodide-stained cells. F, MTS cell proliferation assays for PC9-COR#9 cells treated with the indicated concentrations ofrociletinib, nazartinib, or afatinib for 72 hours. Error bars, SD.
Nukaga et al.
Cancer Res; 77(8) April 15, 2017 Cancer ResearchOF8

effect on cell proliferation in PC9 parental cells and PC9-COR#9 cells (Fig. 5A), nor did rociletinib/cetuximab combi-nation therapy show a synergistic effect in PC9 parental cellsand PC9-AZDR#5 cells that harbor a KRAS G13D mutation(Fig. 5B). However, combination therapy effectively restoredrociletinib sensitivity in PC9-COR#9 cells (Fig. 5C). We usedWestern blotting to investigate whether rociletinib/cetuximabcotreatment suppressed pathway activation downstream ofEGFR in PC9-COR#9 cells and found that it efficiently inhibitedboth AKT and ERK1/2 phosphorylation (Fig. 5D). Analysis ofapoptosis by FACS revealed an increase in Annexin V–positivecells with the subsequent addition of cetuximab (12.5 % with1 mmol/L rociletinib alone, 32.7% with rociletinib/cetuximabcombination; Fig. 5E), indicating that ligand-mediated EGFRactivation contributed to the acquired resistance to third-gen-
eration EGFR-TKIs. We evaluated the effect of afatinib on PC9-COR#9 cells by MTS assay because we previously reported thedecreased mutation specificity of afatinib (28). The prolifera-tion of PC9-COR#9 cells was inhibited by lower concentrationsof afatinib than rociletinib or nazartinib (Fig. 5F). These find-ings also indicate that EGFR wild-type mediated signalingcontributes to PC9-COR#9 cell resistance.
Inaddition,weevaluated the efficacyof rociletinibandcetuximabor afatinib cotreatmentwithH1975 cells expressingwild-type EGFR(H1975 EGFR) or C797S EGFR (H1975C797S; Supplementary Fig.S7). As observed previously, wild-type EGFR overexpressioninduced rociletinib resistance following EGF stimulation. The addi-tion of afatinib or cetuximab restored rociletinib sensitivity to bothtransduced lines. However, the restoration of afatinib was moresignificant inH1975 EGFR cells comparedwithH1975C797S cells.
Figure 6.
Overcoming EGFR wild-type–mediated acquired resistance by rociletinib and cetuximab combination treatment in vivo. A and B, PC9-COR#9–derivedtumor-bearing mice were randomized into control, rociletinib, or rociletinib/cetuximab combination treatment groups. The body weight of the mice wasmonitored. Tumor size wasmeasured to calculate tumor volume. Values indicate average tumor volume in each group. �� , P <0.01 for the combination of rociletinib/cetuximab combination versus rociletinib alone. Error bars, SD. C, Representative images of tumor-bearing mice and tumors. D, Proposed model of EGFRwild-type–mediated acquired resistance.
EGFR Wild-Type Allele Amplification Induces Resistance
www.aacrjournals.org Cancer Res; 77(8) April 15, 2017 OF9

Finally,mouse xenograftmodelswere used to examinewhetherthe roclietinib/cetuximab combination treatment could suppressEGFRwild-type-mediated resistance in vivo. During treatment, thebody weight of the mice and PC9-COR#9 cells derived tumorvolumes were monitored (Fig. 6A–C). Notably, tumor volumesincreased in the control and rociletinib groups; however, roclie-tinib/cetuximab cotreatment significantly inhibited tumorgrowth. Collectively, these data support the possibility that com-bination therapymay be an effective approach to overcome EGFRwild-type-dependent acquired resistance.
DiscussionIn NSCLC, EGFR mutations activate EGFR, which induce
the transformation of lung epithelial cells. EGFR is ubiqui-tously expressed in organ epithelial cells, including lung,gastrointestinal tract, and skin. As such, it is essential toselectively inhibit mutant EGFR-derived signals to minimizeadverse effects of EGFR-TKIs, such as diarrhea and skin rash.Third-generation EGFR-TKIs selectively inhibit EGFR mutantsand minimally affect the wild-type EGFR (25, 26). Thismirrors the significant efficacy and safety of third-generationEGFR-TKIs observed in recent clinical trials. Specifically, osi-mertinib and rociletinib showed significant efficacy and safetyfor previously treated NSCLC patients harboring EGFR-acti-vating mutations, although rociletinib is no longer in devel-opment. The response rate and progression-free survival ofosimertinib for EGFR T790M-positive patients were 61% and9.6 months, respectively (29). The response rate of rociletinibfor EGFR T790M-positive patients was 45% (46). Neitherosimertinib nor rociletinib exhibited a dose-limiting toxicity;therefore, a maximum tolerated dose was not determined(29, 30). Thus, mutation-selective inhibitors offer a clinicallyrelevant advantage of EGFR-TKI treatment with minimaladverse effect.
In this study, we identified several novel mechanisms ofacquired resistance to third-generation EGFR-TKIs, includingSrc–AKT pathway activation and EGFR wild-type allele amplifi-cation (Fig. 6D and Supplementary Fig. S8). Most cancer-specificsomatic driver mutations, such as those in KRAS and EGFR, existin heterozygous. Until today, a limited number of studies havefocused on the function of the wild-type allele in cancer cells.Here, we show that cancer cells exploit this decreased inhibitorypressure for the wild-type allele.
The mechanisms underlying acquired resistance to third-gen-eration EGFR-TKIs have already been partially clarified. Theseinclude the C797S (26) and L798I (32) mutations that presum-ably prevent the covalent binding of EGFR-TKIs to EGFR, bypasspathway activation (33–35, 47), and mutant EGFR gene ampli-fication (48, 49). Specifically, Piotrowska and colleagues reportedEGFR T790M allele amplification in rociletinib-resistant clones(49). To our knowledge, this is the first report describing a role forwild-type EGFR in acquired resistance to mutant-selective third-generation EGFR-TKIs.
Recently, circulating tumor DNA in blood is becoming astudy sample for clarification of mechanisms underlyingacquired resistance to EGFR-TKIs (26, 32). By using recentnext-generation sequencing technology, the identification ofcancer cells derived genetic alterations including mutations andgene copy-number alterations become possible. Consideringthe convenient access to blood samples and sensitivity and
specificity of circulating tumor DNA, it will become commonlyused as reliable samples in the clinics. However, the contam-ination of nonmalignant cells derived DNA is inevitable andmay limit the accuracy of gene copy-number analysis in cancercells. Thus, to identify the EGFR wild-type allele amplification,we believe biopsies from either primary tumors or metastaticlesions are necessary.
In summary, the present study characterized novel mechan-isms of acquired resistance to mutant-selective third-genera-tion EGFR-TKIs. We propose a novel concept of acquiredresistance to mutation selective inhibitors, wild-type allelemediated resistance. In addition, we propose a preclinicalrationale for the use of more promiscuous EGFR-TKI, afatinib,or cetuximab combination therapy in EGFR inhibitor–resistantcancers. While these findings underscore the importance ofEGFR wild-type–mediated signals in acquired resistance, addi-tional preclinical and clinical trials are necessary to evaluatethe efficacy and safety of these treatments to avoid adverse sideeffects related to EGFR pathway inhibition in nonmalignantcells.
Disclosure of Potential Conflicts of InterestK. Soejima has received speakers bureau honoraria fromChugai,Ono, Taiho,
Eli Lilly, AstraZeneca, Pfizer, and Shionogi. No potential conflicts of interestwere disclosed by the others.
Authors' ContributionsConception and design: S. Nukaga, H. Yasuda, K. Tsuchihara, J. Hamamoto,I. Kawada, S. Ikemura, K. Goto, K. SoejimaDevelopment of methodology: S. Nukaga, H. Yasuda, K. Tsuchihara, J. Hama-moto, I. Kawada, S. Matsumoto, S. Ikemura, K. SoejimaAcquisition of data (provided animals, acquired and managed patients,provided facilities, etc.): S. Nukaga, H. Yasuda, K. Tsuchihara, J. Hamamoto,K. Masuzawa, K. Naoki, S. Mimaki, S. IkemuraAnalysis and interpretation of data (e.g., statistical analysis, biostatistics,computational analysis): S. Nukaga, H. Yasuda, K. Tsuchihara, J. Hamamoto,K. Masuzawa, K. Naoki, S. IkemuraWriting, review, and/or revision of the manuscript: S. Nukaga, H. Yasuda,K. Tsuchihara, I. Kawada, K. Naoki, S. Matsumoto, S. Ikemura, K. Goto,T. Betsuyaku, K. SoejimaAdministrative, technical, or material support (i.e., reporting or organizingdata, constructing databases): H. Yasuda, J. Hamamoto, S. Ikemura,T. BetsuyakuStudy supervision: H. Yasuda, K. Tsuchihara, I. Kawada, S. Ikemura, K. Goto,T. Betsuyaku, K. Soejima
AcknowledgmentsWe thank Ms. Mikiko Shibuya for her excellent technical assistance. We also
thank the Collaborative Research Resources, Keio University, School of Med-icine, for cell sorting.
Grant SupportThis work was supported in part by Grants-in-Aid for Scientific Research on
Priority Areas from the Ministry of Education, Culture, Sports, Science, andTechnology of Japan to S. Nukaga (Grant #16K19465), T. Betsuyaku (Grant#15H04833), K. Soejima (Grant #22590870), H. Yasuda (Grant #25860656,15H05666, and 15K14398) and the Practical Research for Innovative CancerControl from Japan Agency for Medical Research and Development to S.Matsumoto (16ck0106012h0003).
The costs of publication of this article were defrayed in part by thepayment of page charges. This article must therefore be hereby markedadvertisement in accordance with 18 U.S.C. Section 1734 solely to indicatethis fact.
ReceivedAugust 30, 2016; revised January 4, 2017; accepted January 23, 2017;published OnlineFirst February 15, 2017.
Nukaga et al.
Cancer Res; 77(8) April 15, 2017 Cancer ResearchOF10

References1. Sharma SV, Bell DW, Settleman J, Haber DA. Epidermal growth factor
receptor mutations in lung cancer. Nat Rev Cancer 2007;7:169–81.2. Kosaka T, Yatabe Y, Endoh H, Kuwano H, Takahashi T, Mitsudomi T.
Mutations of the epidermal growth factor receptor gene in lung cancer:biological and clinical implications. Cancer Res 2004;64:8919–23.
3. The Cancer Genome Atlas Research Network. Comprehensive molecularprofiling of lung adenocarcinoma. Nature 2014;511:543–50.
4. YunCH, BoggonTJ, Li Y,WooMS,GreulichH,MeyersonM, et al. Structuresof lung cancer-derivedEGFRmutants and inhibitor complexes:mechanismof activation and insights into differential inhibitor sensitivity. Cancer Cell2007;11:217–27.
5. Yasuda H, Park E, Yun CH, Sng NJ, Lucena-Araujo AR, Yeo WL, et al.Structural, biochemical, and clinical characterization of epidermal growthfactor receptor (EGFR) exon 20 insertion mutations in lung cancer.Sci Transl Med 2013;5:216ra177.
6. Jura N, Zhang X, Endres NF, Seeliger MA, Schindler T, Kuriyan J. Catalyticcontrol in the EGF receptor and its connection to general kinase regulatorymechanisms. Mol Cell 2011;42:9–22.
7. Zhang X, Gureasko J, Shen K, Cole PA, Kuriyan J. An allosteric mechanismfor activation of the kinase domain of epidermal growth factor receptor.Cell 2006;125:1137–49.
8. Paez JG, Janne PA, Lee JC, Tracy S, Greulich H, Gabriel S, et al. EGFRmutations in lung cancer: correlation with clinical response to gefitinibtherapy. Science 2004;304:1497–500.
9. Lynch TJ, Bell DW, Sordella R, Gurubhagavatula S, Okimoto RA, BranniganBW, et al. Activating mutations in the epidermal growth factor receptorunderlying responsiveness of non–small-cell lung cancer to gefitinib.N Engl J Med 2004;350:2129–39.
10. Pao W, Miller V, Zakowski M, Doherty J, Politi K, Sarkaria I, et al. EGFreceptor genemutations are common in lung cancers from"never smokers"and are associatedwith sensitivity of tumors to gefitinib and erlotinib. ProcNatl Acad Sci U S A 2004;101:13306–11.
11. Shepherd FA, Rodrigues Pereira J, Ciuleanu T, Tan EH, Hirsh V, Thong-prasert S, et al. Erlotinib in previously treated non–small-cell lung cancer.N Engl J Med 2005;353:123–32.
12. Mok TS, Wu YL, Thongprasert S, Yang CH, Chu DT, Saijo N, et al. Gefitinibor carboplatin–paclitaxel in pulmonary adenocarcinoma. N Engl J Med2009;361:947–57.
13. Sequist LV, Yang JC, Yamamoto N, O'Byrne K, Hirsh V, Mok T, et al. PhaseIII study of afatinib or cisplatin plus pemetrexed in patients withmetastaticlung adenocarcinoma with EGFR mutations. J Clin Oncol 2013;31:3327–34.
14. MaemondoM, Inoue A, Kobayashi K, Sugawara S, Oizumi S, Isobe H, et al.Gefitinib or chemotherapy for non–small-cell lung cancer with mutatedEGFR. N Engl J Med 2010;362:2380–8.
15. Rosell R, Carcereny E, Gervais R, Vergnenegre A, Massuti B, Felip E, et al.Erlotinib versus standard chemotherapy as first-line treatment for Euro-pean patients with advanced EGFRmutation-positive non–small-cell lungcancer (EURTAC): a multicentre, open-label, randomised phase 3 trial.Lancet Oncol 2012;13:239–46.
16. Miller VA, Hirsh V, Cadranel J, Chen YM, Park K, Kim SW, et al. Afatinibversus placebo for patients with advanced, metastatic non–small-cell lungcancer after failure of erlotinib, gefitinib, or both, and one or two lines ofchemotherapy (LUX-Lung 1): a phase 2b/3 randomised trial. Lancet Oncol2012;13:528–38.
17. Kobayashi S, BoggonTJ,DayaramT, Janne PA,KocherO,MeyersonM, et al.EGFRmutation and resistance of non-small-cell lung cancer to gefitinib. NEngl J Med 2005;352:786–92.
18. Pao W, Miller VA, Politi KA, Riely GJ, Somwar R, Zakowski MF, et al.Acquired resistance of lung adenocarcinomas to gefitinib or erlotinib isassociated with a second mutation in the EGFR kinase domain. PLoS Med2005;2:e73.
19. Niederst MJ, Sequist LV, Poirier JT, Mermel CH, Lockerman EL,Garcia AR, et al. RB loss in resistant EGFR mutant lung adenocarci-nomas that transform to small-cell lung cancer. Nat Commun 2015;6:6377.
20. Okamoto I, Araki J, Suto R, Shimada M, Nakagawa K, Fukuoka M. EGFRmutation in gefitinib-responsive small-cell lung cancer. Ann Oncol2006;17:1028–9.
21. Engelman JA, Zejnullahu K, Mitsudomi T, Song Y, Hyland C, Park JO, et al.MET amplification leads to gefitinib resistance in lung cancer by activatingERBB3 signaling. Science 2007;316:1039–43.
22. Zhang Z, Lee JC, Lin L, Olivas V, Au V, LaFramboise T, et al. Activation ofthe AXL kinase causes resistance to EGFR-targeted therapy in lung cancer.Nat Genet 2012;44:852–60.
23. Terai H, Soejima K, Yasuda H, Nakayama S, Hamamoto J, Arai D, et al.Activation of the FGF2-FGFR1 autocrine pathway: a novel mechanism ofacquired resistance to gefitinib in NSCLC. Mol Cancer Res 2013;11:759–67.
24. Yun CH, Mengwasser KE, Toms AV, Woo MS, Greulich H, Wong KK, et al.The T790M mutation in EGFR kinase causes drug resistance by increasingthe affinity for ATP. Proc Natl Acad Sci U S A 2008;105:2070–5.
25. CrossDA, Ashton SE,Ghiorghiu S, EberleinC,NebhanCA, Spitzler PJ, et al.AZD9291, an irreversible EGFR TKI, overcomes T790M-mediated resis-tance to EGFR inhibitors in lung cancer. Cancer Discov 2014;4:1046–61.
26. Walter AO, Sjin RT,HaringsmaHJ,OhashiK, Sun J, LeeK, et al.Discovery ofa mutant-selective covalent inhibitor of EGFR that overcomes T790M-mediated resistance in NSCLC. Cancer Discov 2013;3:1404–15.
27. Jia Y, Juarez J, Li J,ManuiaM,NiederstMJ, TompkinsC, et al. EGF816 exertsanticancer effects in non-small cell lung cancer by irreversibly and selec-tively targeting primary and acquired activating mutations in the EGFreceptor. Cancer Res 2016;76:1591–602.
28. Hirano T, Yasuda H, Tani T, Hamamoto J, Oashi A, Ishioka K, et al. In vitromodeling to determine mutation specificity of EGFR tyrosine kinaseinhibitors against clinically relevant EGFRmutants in non–small-cell lungcancer. Oncotarget 2015;6:38789–803.
29. Janne PA, Yang JC, Kim DW, Planchard D, Ohe Y, Ramalingam SS, et al.AZD9291 in EGFR inhibitor-resistant non–small-cell lung cancer. N Engl JMed 2015;372:1689–99.
30. Sequist LV, Soria JC, Goldman JW,Wakelee HA, Gadgeel SM, Varga A, et al.Rociletinib in EGFR-mutated non–small-cell lung cancer. N Engl J Med2015;372:1700–9.
31. Thress KS, Paweletz CP, Felip E, Cho BC, Stetson D, Dougherty B, et al.Acquired EGFR C797S mutation mediates resistance to AZD9291 in non–small cell lung cancer harboring EGFR T790M. Nat Med 2015;21:560–2.
32. Chabon JJ, Simmons AD, Lovejoy AF, Esfahani MS, Newman AM, Har-ingsmaHJ, et al. Circulating tumourDNAprofiling reveals heterogeneity ofEGFR inhibitor resistance mechanisms in lung cancer patients. Nat Com-mun 2016;7:11815.
33. EberleinCA, StetsonD,Markovets AA, Al-Kadhimi KJ, Lai Z, Fisher PR, et al.Acquired Resistance to the Mutant-Selective EGFR Inhibitor AZD9291 IsAssociated with Increased Dependence on RAS Signaling in PreclinicalModels. Cancer Res 2015;75:2489–500.
34. Planchard D, Loriot Y, Andre F, Gobert A, Auger N, Lacroix L, et al. EGFR-independent mechanisms of acquired resistance to AZD9291 in EGFRT790M-positive NSCLC patients. Ann Oncol 2015;26:2073–8.
35. Ortiz-Cuaran S, Scheffler M, Plenker D, Dahmen I, Scheel A, Fernandez-Cuesta L, et al. Heterogeneous mechanisms of primary and acquiredresistance to third-generation EGFR inhibitors. Clin Cancer Res 2016;22:4837–47
36. Mizuuchi H, Suda K, Murakami I, Sakai K, Sato K, Kobayashi Y, et al.Oncogene swap as a novel mechanism of acquired resistance to epidermalgrowth factor receptor-tyrosine kinase inhibitor in lung cancer. Cancer Sci2016;107:461–8.
37. Tanizaki J, Okamoto I, Okabe T, Sakai K, Tanaka K, Hayashi H, et al.Activation of HER family signaling as a mechanism of acquired resistanceto ALK inhibitors in EML4-ALK-positive non–small cell lung cancer. ClinCancer Res 2012;18:6219–26.
38. Sathirapongsasuti JF, Lee H, Horst BA, Brunner G, Cochran AJ, Binder S,et al. Exome sequencing-based copy-number variation and loss of hetero-zygosity detection: ExomeCNV. Bioinformatics 2011;27:2648–54.
39. Burke JE, Perisic O, Masson GR, Vadas O, Williams RL. Oncogenic muta-tions mimic and enhance dynamic events in the natural activation ofphosphoinositide 3-kinase p110alpha (PIK3CA). Proc Natl Acad Sci U S A2012;109:15259–64.
40. Samuels Y, Wang Z, Bardelli A, Silliman N, Ptak J, Szabo S, et al. Highfrequency of mutations of the PIK3CA gene in human cancers. Science2004;304:554.
EGFR Wild-Type Allele Amplification Induces Resistance
www.aacrjournals.org Cancer Res; 77(8) April 15, 2017 OF11

41. Araya CL, Cenik C, Reuter JA, Kiss G, Pande VS, Snyder MP, et al. Iden-tification of significantly mutated regions across cancer types highlights arich landscape of functional molecular alterations. Nat Genet 2016;48:117–25.
42. Sequist LV,Waltman BA,Dias-SantagataD,Digumarthy S, Turke AB, FidiasP, et al. Genotypic and histological evolution of lung cancers acquiringresistance to EGFR inhibitors. Sci Transl Med 2011;3:75ra26.
43. Kanda R, Kawahara A, Watari K, Murakami Y, Sonoda K, MaedaM, et al. Erlotinib resistance in lung cancer cells mediated byintegrin beta1/Src/Akt-driven bypass signaling. Cancer Res2013;73:6243–53.
44. Sos ML, Koker M, Weir BA, Heynck S, Rabinovsky R, Zander T, et al. PTENloss contributes to erlotinib resistance in EGFR-mutant lung cancer byactivation of Akt and EGFR. Cancer Res 2009;69:3256–61.
45. Roskoski R Jr. The ErbB/HER family of protein-tyrosine kinases and cancer.Pharmacol Res 2014;79:34–74.
46. Sequist LV, Soria JC, Camidge DR. Update to rociletinib data with theRECIST confirmed response rate. N Engl J Med 2016;374:2296–7.
47. Kim TM, Song A, Kim DW, Kim S, Ahn YO, Keam B, et al. Mechanisms ofacquired resistance to AZD9291: a mutation-selective, irreversible EGFRinhibitor. J Thorac Oncol 2015;10:1736–44.
48. Ercan D, Zejnullahu K, Yonesaka K, Xiao Y, Capelletti M, Rogers A, et al.Amplification of EGFR T790M causes resistance to an irreversible EGFRinhibitor. Oncogene 2010;29:2346–56.
49. Piotrowska Z, Niederst MJ, Karlovich CA, Wakelee HA, Neal JW, Mino-Kenudson M, et al. Heterogeneity underlies the emergence of EGFRT790wild-type clones following treatment of T790M-positive cancers with athird-generation EGFR inhibitor. Cancer Discov 2015;5:713–22.
Cancer Res; 77(8) April 15, 2017 Cancer ResearchOF12
Nukaga et al.