-
8/8/2019 Anesthesia & Gestosis 2004
1/30
-
8/8/2019 Anesthesia & Gestosis 2004
2/30
-
8/8/2019 Anesthesia & Gestosis 2004
3/30
The Study Of DexmedetomidineThe Study Of Dexmedetomidine
Versus Morphine For Pain AndVersus Morphine For Pain And
Blood Pressure Control AfterBlood Pressure Control AfterCesarean
Section ForCesarean Section For
E.P.H. Gestotic PatientsE.P.H. Gestotic Patients
-
8/8/2019 Anesthesia & Gestosis 2004
4/30
Reem H. El-Kabarity, MDDepartment of Anesthesia.
Abdelmegeed I. Abdelmegeed, MD
Department of Ob/Gyn.
Ain Shams University,
Cairo, Egypt.
-
8/8/2019 Anesthesia & Gestosis 2004
5/30
Introduction:Introduction:
EPHEPH--Gestosis is a high riskGestosis is a high riskpregnancy
condition. It is characterisedpregnancy condition. It is
characterised
by Edema (abnormal body gain ofby Edema (abnormal body gain
ofweight water retention), and/orweight water retention),
and/orProteinuria (excretion of pathologicalProteinuria (excretion
of pathologicalamounts of urinary proteins) and/oramounts of
urinary proteins) and/orHypertension (elevated systolic
andHypertension (elevated systolic anddiastolic blood
pressure).diastolic blood pressure).
-
8/8/2019 Anesthesia & Gestosis 2004
6/30
3210
>180160-179140-159Less
than 140Systolic BP
(mmHg)
>110100-10990-99Less
than 90
Diastolic BP
(mmHg)
GeneralizedLegs
abdomen
Legs
edema
Occult
or legEdema
> 1 gm/litre
+++
> 0.5-1 gm/L
++
0.5 gm/L
+
Nil or
traceProteinuria
EL-Kabarity Modified Gestosis Index
-
8/8/2019 Anesthesia & Gestosis 2004
7/30
The current protocol of management of EPH-
Gestosis has the following principles:
11-- Team approachTeam approach..
22-- Obstetric intensive care management.Obstetric intensive
care management.
33-- MgSoMgSo44 administration.administration.
44-- Control of hypertension.Control of hypertension.
55-- Termination of pregnancy after stabilizationTermination of
pregnancy after stabilization
sof general condition.sof general condition.
66-- Control of pain to avoid emergence ofControl of pain to
avoid emergence of
patient into convulsive fits.patient into convulsive fits.
-
8/8/2019 Anesthesia & Gestosis 2004
8/30
SelectiveSelective 2 adrenoreceptor agonist.2 adrenoreceptor
agonist.
Half life 2.3hours.Half life 2.3hours.
DMED isDMED is Central and peripheral sympatholyticCentral and
peripheral sympatholyticeffecteffect inhibit N.E. release.inhibit
N.E. release.
Stimulates 2 adrenoceptorStimulates 2 adrenoceptor
spinal cordspinal cord in locus ceruleusin locus ceruleus
analgesia.analgesia. sedation.sedation.
-
8/8/2019 Anesthesia & Gestosis 2004
9/30
ObjectivesObjectives
Comparison betweenComparison between
dexmedetomidine anddexmedetomidine and
morphine for pain control andmorphine for pain control and
decrease of blood pressuredecrease of blood pressure
for EPHfor EPH--Gestotic patientsGestotic patientsafter
C.S.after C.S.
-
8/8/2019 Anesthesia & Gestosis 2004
10/30
Patients and MethodsPatients and Methods
42 parturient ladies with severe EPH42 parturient ladies with
severe EPH
Gestosis, antepartum and intrapartumGestosis, antepartum and
intrapartumeclampsia delivered by C.S.eclampsia delivered by
C.S.
MgSo4 (4 gm slowly iv as a loadingMgSo4 (4 gm slowly iv as a
loading
dose then I gm/2hrs for24 hrs).dose then I gm/2hrs for24 hrs).
They were randomized equally into twoThey were randomized equally
into two
groups.groups.
-
8/8/2019 Anesthesia & Gestosis 2004
11/30
Group (I):Group (I): ReceivedReceived
dexmedetomidinedexmedetomidine 11 g/kgg/kgoverover1010 minutes
(loading) followed byminutes (loading) followed by 00..44
g/kg/hr forg/kg/hr for22 hours (maintenance) in the posthours
(maintenance) in the post--anesthesia care unit (PACU).anesthesia
care unit (PACU).
Group (II):Group (II): Received single bolus ofReceived single
bolus ofmorphinemorphine
sulphatesulphate 00..0808 mg/kg.mg/kg. Both drugs were started
intravenouslyBoth drugs were started intravenously 1010minutes
before endof surgery.minutes before endof surgery.
Over two hours postoperatively in the PACU,Over two hours
postoperatively in the PACU,the followingdata were
registeredeverythe followingdata were registeredevery 1010minutes:
HR,MAP,RR,Level of sedation andminutes: HR,MAP,RR,Level of sedation
andanalgesia using the Visual Analogue Scoreanalgesia using the
Visual Analogue Score
(VAS).(VAS).
-
8/8/2019 Anesthesia & Gestosis 2004
12/30
Exclusion CriteriaExclusion Criteria
History of psychiatric disorder on psychotropic
medication.History of psychiatric disorder on psychotropic
medication.
Organ failure Renal FailureOrgan failure Renal Failure
Hepatic FailureHepatic Failure
Respiratory FailureRespiratory Failure
Patients receiving Dexmedetomidine itself or other alpha
2Patients receiving Dexmedetomidine itself or other alpha 2
agonists as clonidine.agonists as clonidine.
Severe degrees of heart block as it causes bradycardia.Severe
degrees of heart block as it causes bradycardia.
-
8/8/2019 Anesthesia & Gestosis 2004
13/30
Technique of AnaesthesiaTechnique of Anaesthesia
Calcuim channel blockers (10mg sublinguial).Calcuim channel
blockers (10mg sublinguial).
MgSo4.MgSo4.
Continuous monitoring (ECG, NIBP,O2Continuous monitoring (ECG,
NIBP,O
2saturation).saturation).
11--2mg/kg lidocaine before intubation.2mg/kg lidocaine before
intubation.
5mg/kg soduim thiopental then succinyl choline5mg/kg soduim
thiopental then succinyl choline
1mg/kg for intubation.1mg/kg for intubation.
-
8/8/2019 Anesthesia & Gestosis 2004
14/30
Post Anaesthetic Care Unit (PACU)Post Anaesthetic Care Unit
(PACU)
OverOver22 hours postoperatively everyhours postoperatively
every 1010 mins.mins.
The followingdata were registered:The followingdata were
registered: HR, MAP,RRHR, MAP,RR
Addition of morphine doses.Addition of morphine doses.
Assessment of level of sedation andAssessment of level of
sedation andanalgesia using Visual Analog Score (VAS).analgesia
using Visual Analog Score (VAS).
-
8/8/2019 Anesthesia & Gestosis 2004
15/30
Demographicdata showedno statistically
significantDemographicdata showedno statistically
significantdifferencedifference (P>(P>00..0505).).
Group (I):
DMED
Group (II):
MorphineP Significance
Age (years)24.4
1.2 2
6.10
.8 > 0
.05 NS
Parity 0.91.3 0.81.1 > 0.05 NS
Gestational age at time
of T.O.P. (weeks) 35.32.3 34.21.8 > 0.05 NS
Body Mass Index
(kg/m2)28.01.3 27.41.9 > 0.05 NS
-
8/8/2019 Anesthesia & Gestosis 2004
16/30
Comparing bothgroupsComparing bothgroups as regards theas
regards theintraoperative dataandthe
hemodynamicvaluesintraoperative dataandthe hemodynamicvaluesbefore
givingthe drug shows no statisticallybefore givingthe drug shows no
statistically
significantdifferencesignificantdifferenceGroup (I)
DMED
Group (II)
MorphineP Significance
Operative time (min) 43.36.7 49.25.9 > 0.05 NS
End-tidal halothane (%) 0.60.3 0.70.2 > 0.05 NS
Crystalloids (ml) 1023257 1131303 > 0.05 NS
Estimated blood loss
(ml) 62690 709
104 > 0.05 NS
Heart rate (bpm) 8014 8518 > 0.05 NS
MAP (mmHg) 1018 1057 > 0.05 NS
-
8/8/2019 Anesthesia & Gestosis 2004
17/30
Heart rate (beats/min) values overHeart rate (beats/min) values
over 1010 min aftermin afterinjection of the study drugs showed
statisticalinjection of the study drugs showed
statisticalsignificant difference(P
-
8/8/2019 Anesthesia & Gestosis 2004
18/30
MAP (mmHg) values overMAP (mmHg) values over 1010 min after
injection showedmin after injection showedstatistical significant
difference showed statisticalstatistical significant difference
showed statistical
significant difference( P
-
8/8/2019 Anesthesia & Gestosis 2004
19/30
Heart rate (beats/min) value of the studied drugs inHeart rate
(beats/min) value of the studied drugs inthe PACU showed
statistical significant differencethe PACU showed statistical
significant difference
( P
-
8/8/2019 Anesthesia & Gestosis 2004
20/30
MAP (mmHg) values of the studied drugsMAP (mmHg) values of the
studied drugs showedshowedstatistical significant
differencestatistical significant difference in the PACUin the
PACU
( P
-
8/8/2019 Anesthesia & Gestosis 2004
21/30
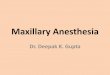
Respiratory rate (breath/min) values of theRespiratory rate
(breath/min) values of thestudied drugs in PACU showed no
statisticalstudied drugs in PACU showed no statistical
difference ( P >difference ( P > 00..0505) .) .
0
5
10
15
20
0 30 60 90 120
DMED
Mor i
-
8/8/2019 Anesthesia & Gestosis 2004
22/30
Oxygen saturation (%) values of the studiedOxygen saturation (%)
values of the studieddrugs in PACU showed no statistical
differencedrugs in PACU showed no statistical difference
(P >(P > 00..0505):):
94
95
96
97
98
99
100
030
60
90
120
Ti ( i )
2
t
r
tion
(
)
DM ED
M or ine
-
8/8/2019 Anesthesia & Gestosis 2004
23/30
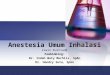
Cumulative added doses of morphine (mg) forCumulative added
doses of morphine (mg) forcontrol of pain in the PACU was
statisticallycontrol of pain in the PACU was statistically
significant in the morphine group.significant in the morphine
group.
0
2
4
6
8
10
0 30 60 90 120
Time (min)
Dose
DMED
Morphine
-
8/8/2019 Anesthesia & Gestosis 2004
24/30
The mean total dose/patient of morphine (mg)The mean total
dose/patient of morphine (mg)overover 22 hours period in the PACU
washours period in the PACU was
statistically significant in the morphine group.statistically
significant in the morphine group.
0
2
4
6
8
10
DMED Group Morphine Group
Dose
-
8/8/2019 Anesthesia & Gestosis 2004
25/30
The mean total dose/patient of morphine additions (mg)The mean
total dose/patient of morphine additions (mg)in ward throughin ward
through 22--1212 hours postoperatively washours postoperatively
was
statistically significant in the morphine group.statistically
significant in the morphine group.
-
8/8/2019 Anesthesia & Gestosis 2004
26/30
Discussion:Discussion:
EE22--receptors regulate the autonomic andreceptors regulate the
autonomic andcardiovascular system.cardiovascular system.
They are located in locus ceruleus and dorsal hornThey are
located in locus ceruleus and dorsal horn
of spinal cord leading to sedation and analgesia.of spinal cord
leading to sedation and analgesia. Lawerence andDe Lange (Lawerence
andDe Lange (19971997)) reported areported a
biphasic effect on hemodynamic after IV DMED.biphasic effect on
hemodynamic after IV DMED.
Venn andGround(Venn andGround(20012001)) found that DMED is
safefound that DMED is safe
and acceptable sedative agent in ICU patient forand acceptable
sedative agent in ICU patient forsedation.sedation.
Aho andhis collegues(Aho andhis collegues(19911991)) concluded
thatconcluded thatDMED relieves pain and opioid drug request
afterDMED relieves pain and opioid drug request afterlaparoscopic
tubal ligation.laparoscopic tubal ligation.
-
8/8/2019 Anesthesia & Gestosis 2004
27/30
Bhana andhis collegues (2000)Bhana andhis collegues (2000)
showedshowed
sedative, analgesic and anxiolytic effectssedative, analgesic
and anxiolytic effects
after IV DMED in post surgical patients inafter IV DMED in post
surgical patients inICU.ICU.
Coursin andhis collegues (2001)Coursin andhis collegues (2001)
foundfound
DMED stimulatesDMED stimulates EE22 receptors in locusreceptors
in locuscerulus in spinal cord to provide sedationcerulus in spinal
cord to provide sedation
and enhance analgesia.and enhance analgesia.
Arain and
Ebert (2002)Arain and
Ebert (2002) found also thatfound also thatadministration of
DMED versus propofoladministration of DMED versus propofol
showed more sedation, lower MAP,showed more sedation, lower
MAP,
improved analgesia in the recovery room.improved analgesia in
the recovery room.
-
8/8/2019 Anesthesia & Gestosis 2004
28/30
In our study, we found that parturients receivingIn our study,
we found that parturients receivingdexmedetomidine for
postoperative Cesarean Sectiondexmedetomidine for postoperative
Cesarean Section
pain and blood pressure control for EPHpain and blood pressure
control for EPH--Gestosis hadGestosis had
significantly slower postoperative HR, decrease insignificantly
slower postoperative HR, decrease in
MAP without intial increase.MAP without intial increase.
This may be due to small dose infused,This may be due to small
dose infused,
increased duration of infusion and the ability of
volatileincreased duration of infusion and the ability of
volatile
anesthetics directly to relax vascular smooth
muscles.anesthetics directly to relax vascular smooth muscles.Hence
they required less morphine in the PACUHence they required less
morphine in the PACU
compared with the control group who received onlycompared with
the control group who received only
morphine.morphine.
SummarySummary
-
8/8/2019 Anesthesia & Gestosis 2004
29/30
ConclusionConclusion
The use of dexmedetomidine as a postoperativeC.S. analgesic
resulted in significantly lessaddition of pain-relief medications,
slower HR as
well as lower MAP than the other group thatreceived only
morphine. These results may provethat dexmedetomidine is more
advantageous andbeneficial for gestotic patients; who might be
jeopardized by the higher risk of postoperativepain,
hypertension, tachycardia, respiratorydepression as well as the
need of using larger doses of morphine.
-
8/8/2019 Anesthesia & Gestosis 2004
30/30