Embed Size (px)
Citation preview

Approach in Glomerular DiseasesApproach in Glomerular Diseases
์ผศ.นพ. เถลิงศักดิ์ กาญจนบุษย
สาขาวิชาโรคไต ภาควิชาอายุรศาสตร
ั ั โ ไ ป ึหัวหนาศูนยวิจัยโรคไตและความผิดปกติทางเมตาบอลิซึม
จุฬาลงกรณมหาวิทยาลัย
JCMS 2009



HematuriaHematuriaDysmorphic
AcanthocyteProteinuriaProteinuriaP i i /dAcanthocyte
RBC castProteinuria > 2 gm/day
GFR ↓GFR ↓iAzotemia
Oliguria
GLOMERULARGLOMERULARSaltSalt--water retentionwater retention
EdemaGLOMERULAR GLOMERULAR DISEASEDISEASE
Edema
HT

Helen Liapis, 2002


Afferent arterioleEfferent arteriole
Bowman’s capsule
Endothelium
Podocyte
Pedicle
PCT

GFR = snGFR x Nephron
snGFR = (PGC-PT) x KUF
AzotemiaOliguria
PPGCGC
KKUFUF
PPTT

MechanismMechanismGFR
Reabsorption
ManifestationsEdemaHTHT

Glomerular hematuria
Acute self-limited inflammation
Proteinuria usually < 3 gm/day
Salt retentionAGN DPGNOliguria, Azotemia
Abrupt, usually self‐ limiting
DPGN
Glomerular hematuria
GBM ruptureGlomerular hematuria
Proteinuria usually < 3 gm/day
Less salt retentionRPGNIC mediatedAnti-GBMPauci-immune
RF over days/week; progessivePauci-immune

HT
Progressive disease: ongoing, sclerosis
Proteinuria > 2 gm/day
Renal insufficiencyCGNIC mediatedNon-IC mediatedN iFit in CRF criteria Non-immune
Podocyte injury GBM charge lossProteinuria ≥ 3.5 gm/day/1.73 m2 ; UPCR > 3
gm/day + Lipiduria
Podocyte injury, GBM charge loss
g y p
Edema
HyperlipidemiaNSMCDFSGS IgM nephropathy
Hypercoagulationg p p yMPGNMN

H t i /HPIgATBM/Al t’
Less severe injuryHematuria > 2/HP
Asymptomatic
TBM/Alport’sPostinfectiousPost-GN
Proteinuria 0.15‐3.0
gm/day ±
y pFSGS IgM
Hematuria > 2/HP MPGNMNIgA Alport’sIgA, Alport s IC mediated
Gross hematuriaMacroscopic hematuria
IgAStoneAIN&CTIN
GBM gaps
hematuria AIN&CTINLoin painhematuria


Case 1
A 43 year old female presented with 1 weeks of progressive facial edema, orthopnea, and PND . A day before admit she developed sudden gross hematuria PE revealsadmit, she developed sudden gross hematuria. PE reveals afebrile, BP 140/92 mm.Hg, and generalized edema. Laboratory evaluation reveals BUN 49 mg/dL, Cr 1.5 mg/dL, hypoalbuminemia hyperkalemic wide-gap MAhypoalbuminemia, hyperkalemic wide-gap MAUrinalysis revealed sp.gr. 1.020, 2+ urinary protein, RBC 80-100/HP, WBC 5-7/HP.
1) Which glomerular syndrome is fit for the patient? 2) What additional laboratory tests should be performed in
this patient ? p

1. Acute GN
2. Rapidly progressive GN Nephritis
3. Chronic GNNephrosis
A i i i / h i
4. Nephrotic syndromep
5. Asymptomatic proteinuria / hematuria

Etiologies of Acute Glomerulonephritis
Low Complement Normal ComplementPrimary
Acute PSGN (>90%)MPGN
PrimaryIgA nephropathyIdiopathic CGN
Type I (50‐80%)Type II (80‐90%)
Secondary
pAnti‐GBMPauci‐immune
SecondaryySLE
Focal (75%)Diffuse (90%)
yHypersensitivity vasculitisWGHSP9
Acute‐subacute IE (90%)Visceral abscess“Shunt” nephritis
HSPGoodpasture syndrome
pCryoglobulinemia (85%)

Pathway Complement Glomerular diseasePathway affected
Complement changes
Glomerular disease
Classical ‐C3, C4, CH50 MPGN I
LN III, IV
Alternative ‐C3, CH50 PSAGN, HUS
Infection related+ C3 nephritic factor MPGN II

Disease C’ levels Comment
Atheroembolism ↓C3, ± ↓C4 Usually transient, mainly during acute t e oe bo s ↓C3, ↓C4 Usua y t a s e t, a y du g acuteembolism
Severe sepsis ↓C3, ↓C4 Esp. with shock
HUS/TTP ↓C3, ± ↓C4 ~50% of cases
Acute pancreatitis ↓C3 ↓C4 Subsides in a few daysAcute pancreatitis ↓C3, ↓C4 Subsides in a few days
Severe malnutrition ↓C3, ± N C4 C1q is also low
Severe liver disease ↓C3, ↓C4 C1q levels are normal
Inherited C4 deficiency N C3, ±↓C4 20‐40% of normals have one or two C4 null genes; higher incidence found in SLE

Case 1
A 43 year old female presented with 1 weeks of progressive facial edema, orthopnea, and PND . A day before admit she developed sudden gross hematuria PE revealsadmit, she developed sudden gross hematuria. PE reveals afebrile, BP 140/92 mm.Hg, and generalized edema. Laboratory evaluation reveals BUN 49 mg/dL, Cr 1.5 mg/dL, hypoalbuminemia hyperkalemic wide-gap MAhypoalbuminemia, hyperkalemic wide-gap MAUrinalysis revealed sp.gr. 1.020, 2+ urinary protein, RBC 80-100/HP, WBC 5-7/HP.Further investigations found low C3 but normal C4, negativeFurther investigations found low C3 but normal C4, negative viral serologies, and UPCI 2.2
1) What is your final conclusion?2) How to confirm the diagnosis?3) How to manage the patient?

Nephrotic Features Nephritic Features
MCD ++++ ‐MN ++++ +FSGS +++ ++Fibrillary GN +++ ++Mesangioproliferative GN ++ ++g p ++ ++MPGN ++ +++Diffuse proliferative GN ++ +++Diffuse proliferative GN ++ +++Acute PSGN + ++++
iCrescentic GN + ++++

Children (%) Elderly (%)
Hematuria 100 100
Proteinuria 80 92
Edema 90 75
Hypertension 60-80 83
Oliguria 10-50 58
Dyspnea/heart failure <5 43
Nephrotic proteinuria 4 20
Azotemia 25-40 83
Early mortality <1 25

Case 1
A 43 year old female presented with 1 weeks of progressive facial edema, orthopnea, and PND . A day before admit she developed sudden gross hematuria PE revealsadmit, she developed sudden gross hematuria. PE reveals afebrile, BP 140/92 mm.Hg, and generalized edema. Laboratory evaluation reveals BUN 49 mg/dL, Cr 1.5 mg/dL, hypoalbuminemia hyperkalemic wide-gap MAhypoalbuminemia, hyperkalemic wide-gap MAUrinalysis revealed sp.gr. 1.020, 2+ urinary protein, RBC 80-100/HP, WBC 5-7/HP.Further investigations found low C3 but normal C4, negativeFurther investigations found low C3 but normal C4, negative viral serologies, and UPCI 2.2
1) What is your final conclusion?2) How to confirm the diagnosis?3) How to manage the patient?

ASO ~ ASO ~ 7575% % AntiAnti--DNase B DNase B 9090%%AHA more sensitive for pyodermaAHA more sensitive for pyodermaAntiAnti--GAPDH (NPlr)GAPDH (NPlr)AntiAnti--SpeB/ ZymogenSpeB/ ZymogenDemonstrates streptococcal infection, but Demonstrates streptococcal infection, but does not predict development or severity does not predict development or severity
f GNf GNof GNof GN

Case 1
A 43 year old female presented with 1 weeks of progressive facial edema, orthopnea, and PND . A day before admit she developed sudden gross hematuria PE revealsadmit, she developed sudden gross hematuria. PE reveals afebrile, BP 140/92 mm.Hg, and generalized edema. Laboratory evaluation reveals BUN 49 mg/dL, Cr 1.5 mg/dL, hypoalbuminemia hyperkalemic wide-gap MAhypoalbuminemia, hyperkalemic wide-gap MAUrinalysis revealed sp.gr. 1.020, 2+ urinary protein, RBC 80-100/HP, WBC 5-7/HP.Further investigations found low C3 but normal C4, negativeFurther investigations found low C3 but normal C4, negative viral serologies, and UPCI 2.2
1) What is your final conclusion?2) How to confirm the diagnosis?3) How to manage the patient?

Atypical presentationCli i l Short latent period Clinical Short latent period
Nephrotic syndrome or RPGN Anuria Multiorgan involvement
Lab Low antistreptococcal titerNormal C3Low C1q, C2 or C4
Delayed resolution
Short term Renal failure: 2 weeksH i h t i kHypertension or gross hematuria: 3 weeksLow C3: 6 weeks
Long term Proteinuria: 6 monthsHematuria: 12 monthsHematuria: 12 months

Get rid source
Corticosteroid & immunosuppressive agentpp g
Some organisms still progress in spite of effective treatmentStaphylococcus aureus
ll iBrucellosisQuartan malariaSchistosomiasis


Case 2
A 43 year old year is found to have Scr of 1.6 mg/dland BUN of 32 mg/dl on her annual check up. Her urinalysis shows 3 4+ protein a few rbc’s with some dysmorphic but noshows 3-4+ protein, a few rbc’s with some dysmorphic but no rbc casts. She is found to have 3.8 g proteinuria daily. PE reveals a BP 160/92 mm.Hg, and no edema. Further laboratory evaluation reveals WBC 50 000 /mm3 a reducedlaboratory evaluation reveals WBC 50,000 /mm3, a reduced CH50, a borderline C3 level, and a reduced C4 level.
1) What is the differential diagnosis for renal diseases with1) What is the differential diagnosis for renal diseases with nephrito-NS?
2) What additional laboratory tests should be performed in this patient ?this patient ?

Classification of Glomerular Diseases
1o Glomerular Disease(idiopathic; renal‐limited)
MCD
2oGlomerular Disease(associated with multi‐system
disease)MCDFSGSMesangial GN (IgA, IgM)
disease)Systemic diseasesSystemic Infections
MN MPGNCrescentic GN
Vascular diseasesMetabolic & Deposition diseasesHereditary nephropathiesCrescentic GN
Sclerosing GNUnclassified GN
Hereditary nephropathiesMiscellaneous

Mesangiocapillary GNDeposition diseases
Amyloidosis
Light‐chain deposition diseaseFibrillary GN and Immunotactoid GNFibrillary GN and Immunotactoid GN
Hereditary disease: Alport’s syndromeSome cases of mesangial focal and diffused Some cases of mesangial, focal and diffused proliferative GN
IgA nephropathyg p p y
Post‐infectious GNLupus nephritis
Diabetic nephropathy

Case 2
A 43 year old year is found to have Scr of 1.6 mg/dland BUN of 32 mg/dl on her annual check up. Her urinalysis shows 3 4+ protein a few rbc’s with some dysmorphic but noshows 3-4+ protein, a few rbc’s with some dysmorphic but no rbc casts. She is found to have 3.8 g proteinuria daily. PE reveals a BP 160/92 mm.Hg, and no edema. Further laboratory evaluation reveals WBC 50 000 /mm3 a reducedlaboratory evaluation reveals WBC 50,000 /mm3, a reduced CH50, a borderline C3 level, and a reduced C4 level.
1) What is the differential diagnosis for renal diseases with1) What is the differential diagnosis for renal diseases with nephrito-NS?
2) What additional laboratory tests should be performed in this patient ?this patient ?


Classification of Cryoglobulinemia
Type I Type II Type III
Ig content Single mIg (IgMk, IgGk, pIgG pIgG
IgAk ) mIgM
(IgMk – IgG)
pIgM
(IgM – IgG)
RF Negative Positive Occ. positive
Associated
disease
Multiple myeloma
Dysproteinmias
HCV
HBV
Collagen vascular
Chronic infections
SBELymphoma Lymphoma •SBE
•Leprosy
•HBV
•HCV

Unknown genetic and environmental factor
HCV
Unknown genetic and environmental factor
HCV
E 2t (14,18 )t Bcl 2*
o ere pression
B B B
overexpressionCD 81
B cell NHLPolyclonal RF Oligoclonal RF
MC type III MC type II-III Cli E Rh t l 2003 21 (S l 31)MC type IIIOther autoimmune
disorder
MC type II-IIIMC type II
Clin Exp Rheumatol 2003; 21 (Suppl. 31)S78-S84.

Evidence for HCV Virus in EMC
Anti-HCV antibidies (by RIBA) pressent in 91% of 45 pts with EMC(Ferri et al. Infection 1991; 19:417)
HCV RNA detected in 86% of 45 patients with EMC (Ferri et al. Clin Exp Rheumatol 1991; 9:621)
HCV RNA and anti-HCV Ab are concentrated in the cryoglobulins (Agnello et al. NEJM 1992; 327:1490)
(Misiani et al. Ann Int Med 1992; 117:573)

Spectrum of HCV-Associated IC Disease
EMC EMC ĉ
MPGN
MPGN ĉ
Cryoglobulins
MPGN ŝ
Cryoglobulins
MN
IC Size


Case 3
A 66 year old, an accountant, develops cough, arthralgias, malaise, and weight loss. He is normotensive, and has no arthritis or edema. He is found to have a hazy LLLinfiltrate on his chest X-ray, a urinalysis with 3+ proteinuriaand 4+ heme, with many rbc’s and many dysmorphic acanthocytes, a BUN of 25 mg/dl and serum creatinine of 1.8
/dl d 24 h i h 5 6 lb i i d ilmg/dl, and 24 hour urine shows 5.6 grams albuminuria daily. ANA is positive 1:80, and complement is WNL.
1) What is the differential diagnosis of “renal pulmonary1) What is the differential diagnosis of renal-pulmonary syndromes” ? Which serologic tests are helpful in this case ?
2) A renal biopsy is performed but there is only a small piece2) A renal biopsy is performed, but there is only a small piece of tissue. Although there will be adequate amount for light microscopy, the pathologist asks you whether to put the remaining tissue for, IF, or EM. You advise ?g , ,

With pulmonary edemaARF with hypervolemiaSevere cardiac failureSevere cardiac failure
InfectiveSevere bacterial pneumonia (e.g. Legionella) with RFHantavirus infectionHantavirus infectionOpportunistic infections in the immunocompromised
OthersARDS with RF in multi‐organ failureARDS with RF in multi organ failureParaquat poisoningRenal vein/IVC thrombosis with pulmonary emboliDisease associated with Anti‐GBM (20‐40% of cases) ( 4 )Goodpasture’s disease (spontaneous anti‐GBM disease)

Anti-GBM Ab (20-40%)Goodpasture’s disease (spontaneous anti-GBM dis.)
Systemic vasculitis (60-80%)Wegener’s granulomatosis
Commong g
Microscopic polyangiitisSystemic lupus erythematosusChurg Strauss syndromeg yHenoch‐SchÖnlein purpuraBehçet’s diseaseEssential mixed cryoglobulinemiaEssential mixed cryoglobulinemiaRheumatoid vasculitisDrugs: penicillamine, hydralazine, propylthiouracil

Case 2
A 66 year old, an accountant, develops cough, arthralgias, malaise, and weight loss. He is normotensive, and has no arthritis or edema. He is found to have a hazy LLLinfiltrate on his chest X-ray, a urinalysis with 3+ proteinuriaand 4+ heme, with many rbc’s and many dysmorphic acanthocytes, a BUN of 25 mg/dl and serum creatinine of 1.8
/dl d 24 h i h 5 6 lb i i d ilmg/dl, and 24 hour urine shows 5.6 grams albuminuria daily. ANA is positive 1:80, and complement is WNL.
1) What is the differential diagnosis of “renal pulmonary1) What is the differential diagnosis of renal-pulmonary syndromes” ? Which serologic tests are helpful in this case ?
2) A renal biopsy is performed but there is only a small piece2) A renal biopsy is performed, but there is only a small piece of tissue. Although there will be adequate amount for light microscopy, the pathologist asks you whether to put the remaining tissue for, IF, or EM. You advise ?g , ,



DiagnosisFollow upp
Remission: 80% ANCA ‐Relapse: 75% ANCA +p 75No symptom: 1/4 ‐ 1/3 increasing titerLimitation:ANCA testing represents several testsANCA‐vasculitis represents several diseasesVary in criteria dx of relapseVary in criteria dx of relapse
Predict outcome

Age > 50 yrAge > 50 yr
Clinical presentationPrevalence of
PI‐CGNPPV for PI‐
CGNNPV for PI‐
CGNClinical presentation PI‐CGN CGN CGN
RPGN 66% (82/124) 99% 65%
Hematuria, proteinuria, and Cr > 3 mg/dl
30% (147/497) 95% 89%Cr > 3 mg/dl
Hematuria, proteinuria, and Cr 1 5‐3 mg/dl
11% (36/311) 85% 97%Cr 1.5‐3 mg/dl
Hematuria, proteinuria, and Cr < 1 5 mg/dl
4% (7/195) 66% 99%Cr < 1.5 mg/dl

Case 3
A 66 year old, an accountant, develops cough, arthralgias, malaise, and weight loss. He is normotensive, and has no arthritis or edema. He is found to have a hazy LLLinfiltrate on his chest X-ray, a urinalysis with 3+ proteinuriaand 4+ heme, with many rbc’s and many dysmorphic acanthocytes, a BUN of 25 mg/dl and serum creatinine of 1.8
/dl d 24 h i h 5 6 lb i i d ilmg/dl, and 24 hour urine shows 5.6 grams albuminuria daily. ANA is positive 1:80, and complement is WNL.
1) What is the differential diagnosis of “renal pulmonary1) What is the differential diagnosis of renal-pulmonary syndromes” ? Which serologic tests are helpful in this case ?
2) A renal biopsy is performed but there is only a small piece2) A renal biopsy is performed, but there is only a small piece of tissue. Although there will be adequate amount for light microscopy, the pathologist asks you whether to put the remaining tissue for, IF, or EM. You advise ?g , ,


Case 4
A 48 year old female pharmacist has a history of DVT 4 yrs ago, and a PE 2 years ago. She is found to have an elevated Scr of 1.8 mg/dl, urinalysis 3+ protein 5-10 rbc’s 0 g , y pcasts. Physical exam shows BP 150/92 mm.Hg, 1+ pedal edema, prominent P2, and livedo reticularis of the legs. 24 hr urinary protein excretion is 1.9 g/day, ANA+ 1:160, anti DNA antibody negative, serum complement WNL; wbc 6,200, HCT 36%, platelets 100,000.
1) Wh t l i t t i ht fi th di i h ?1) What serologic tests might confirm the diagnosis here ?
2) What features in the history might help in the diagnosis ?
3) What other routine laboratory features are useful3) What other routine laboratory features are useful diagnostically while the definitive serologic tests are pending ?



Case 5A 29 year old. Female computer processor presents
with fever, lymphadenopathy, and diffuse arthritis of the small hand joints. She is found to have a WBC of 2,800, HCT 22%,platelets 168 000 Urinalysis shows 4+ protein 20 30 rbc andplatelets 168,000. Urinalysis shows 4+ protein, 20-30 rbc, and rbc casts; ANA 1:1280. A renal biopsy shows DPLN, WHO Class IV.
1) Which tests predict the best prognosis of this patient over the next decade ?
2) What serologic tests are the best guide to immediate therapy of this patient ?
3) If the patient had been taking minocycline for acne what3) If the patient had been taking minocycline for acne, what serologic tests might help in determining whether this is drug related disease ?
4) What medications can produce drug related SLE ? How is4) What medications can produce drug related SLE ? How is the diagnosis established ?

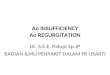
C4(mg/dL)(mg/dL)
C3 (mg/dL)

Case 5A 29 year old. Female computer processor presents
with fever, lymphadenopathy, and diffuse arthritis of the small hand joints. She is found to have a WBC of 2,800, HCT 22%,platelets 168 000 Urinalysis shows 4+ protein 20 30 rbc andplatelets 168,000. Urinalysis shows 4+ protein, 20-30 rbc, and rbc casts; ANA 1:1280. A renal biopsy shows DPLN, WHO Class IV.
1) Which tests predict the best prognosis of this patient over the next decade ?
2) What serologic tests are the best guide to immediate therapy of this patient ?
3) If the patient had been taking minocycline for acne what3) If the patient had been taking minocycline for acne, what serologic tests might help in determining whether this is drug related disease ?
4) What medications can produce drug related SLE ? How is4) What medications can produce drug related SLE ? How is the diagnosis established ?

Ag Specificity Clinical Association
dsDNA Marker for active disease; titers fluctuate with disease activityy
ssDNA Non-specific
Ro/SSA Cutaneous lupus (75%), photosensitivity, neonatal lupus
La/SSB With La, low prevalence of renal disease, neonatal lupus (75%)
Sm Marker for disease; 15-30 % sensitivity, may be asso. with CNS disease
RNP (U1-RNP) MCTD, required for diagnosis; in SLE-mild, non-renal
Phospholipids Hypercoaqulable state in some, no significance in others; thrombocytopenia, latertrimester abortionslatertrimester abortions
Histones >95% in drug-related lupus; present in RA> SLE, systemic sclerosis with pulmonary fibrosis
KU SLE, MCTD (Europeans/Americans): scleroderma/myositis overlap (Japanese)

Homogenous Peripheral
Speckle Nucleolar

D fi it P iblDefiniteProcainamideHydralazine
PossibleAnticonvulsants - phenytoinQuinidineHydralazine
DiltiazemMinocyclinePenicillamine
QuinidineAnti-thyroid drugsSulfonamidesLithiumPenicillamine
INHMethyldopaChlorpromazine
LithiumBeta-blockersNitofurantoinPASChlorpromazine
PractololPASCaptoprilInterferon alphaHCTZHCTZGlyburideCarbamazepineSulfasalazineSulfasalazineHydralazine

Fever, myalgias, rash, arthralgiasFever, myalgias, rash, arthralgias--arthritis, arthritis, serositis hemotologic abnomalitiesserositis hemotologic abnomalitiesserositis, hemotologic abnomalitiesserositis, hemotologic abnomalitiesKidney disease and CNS uncommonKidney disease and CNS uncommonAntiAnti DNA Ab and low C` uncommonDNA Ab and low C` uncommonAntiAnti--DNA Ab and low C uncommonDNA Ab and low C uncommonSome with renal disease are ANCA + (antiSome with renal disease are ANCA + (anti--MPO + lactoferin)MPO + lactoferin)MPO + lactoferin)MPO + lactoferin)

Clinical feature Spontaneous lupus Drug‐induced lupusUsual age 20‐40 50
Female to male ratio 9:1 1:1Female to male ratio 9:1 1:1
Race All “No blacks”
Acetylation type Slow = Fast Slow
O t f t G d l Ab tOnset of symptoms Gradual Abrupt
Constitutional symptoms 83 50
Arthralgia and arthritis 90 95
Pleuropericarditis (procainamide)
50 50
Hepatomegaly 25 25
Rash (all types) 74 10‐20
Discoid lesions 20 0
Malar erythema 42 2y 4
Renal diseases 53 5
CNS disease Common Unusual

Immunologic abnormalitiesANA 95 95
LE cells 90 90
Anti RNP 40 50 20Anti‐RNP 40‐50 20
Anti‐Sm 20‐30 Rare
Anti‐DNA 80 Rare
Antihistone 80 90
Complement Reduced Normal
Immune complexes Elevated NormalImmune complexes Elevated Normal

Present in > 95% drugPresent in > 95% drug--induced lupusinduced lupusPresent in > 95% drugPresent in > 95% drug induced lupusinduced lupusCommon with procainamide, hydralazine, Common with procainamide, hydralazine, chlorpromazine, quinidinechlorpromazine, quinidinep , qp , qCommon in native SLE ( but with AntiCommon in native SLE ( but with Anti--DNA DNA Abs, AntiAbs, Anti--Sm Ab, etc.)Sm Ab, etc.),, , ), )

Etiologies:Etiologies:H d l iH d l iHydralazine Hydralazine
High dose (>High dose (>200 200 mg/day mg/day ±± cumulative > cumulative > 100 100 gmgmFemaleFemaleFemaleFemaleSlow hepatic acetylationSlow hepatic acetylationHLAHLA--DR DR 44CC4 4 def.def.
MinocyclineMinocyclineANA ANA 9292%%pp--ANCA ANCA 8383%% Should not be used in SLE

ManifestationManifestationfrequent present with renalfrequent present with renalAntiAnti--dsDNA+dsDNA+AntiAnti histone: may negativehistone: may negativeAntiAnti--histone: may negativehistone: may negativeHigh titer MPOHigh titer MPOlupuslupus--like RPGN PANlike RPGN PANlupuslupus like, RPGN, PANlike, RPGN, PANMay need aggressive PX +drug withdrawalMay need aggressive PX +drug withdrawal


Case 6A 62 year old white female housewife develops y p
periorbital edema in the AM followed by pedal and ankle edema later in the day, and a 6 kg weight gain. PE shows BP 142/84 mm.Hg, CTS, and edema only. Lab shows Urinalysis 4+ protein, 2-3 rbc, few oval fat bodies, BUN 18 mg/dl, creatinine 0.9 mg/dl, glucose 118 mg/dl, plasma albumin 2.4g/dl, cholesterol 236 mg/dl, and 24 hour urinary protein 10
/dg/day.
1) What serologic tests are helpful in the nephrotic syndrome before biopsy ?p y
2) If the patient was 32 years old rather than 62 years old would the testing be different ?
3) Is biopsy useful here ?

Histopathologic diagnosis Age 15‐35 yrsN = 175 (%)
Age 36-60 yrsN = 180 (%)
Age > 60 yrsN = 46(%)
MCD 8MCD 22.4 7.8 13
FSGS 20 26.7 23.9
MN 12.1 17.8 10.9
MPGN 4.2 3.3 4.4
IgAN 23 11.7 4.4
Non‐IgA MesPGN 8.5 8.3 6.5
LNLN 1.2 1.1 4.4
DN 1 9.4 4.4
Post‐infectious GN 3 7.8 8.7
D iti di 8Deposition diseases 0 1.1 8.7
Congenital glomerulopathies 1.2 0 0
Miscellaneous 5.1 4.4 2.1
U k 6 6Unknown 0.6 0.6 11

Clinical and lab. Features in AL amyloidosis 474 pts
Initial symptoms Laboratory findings
Fatigue 62%
Weight loss 52%
P i %
Increase plasma cell( BM> 6%) 56%
Anemia (Hb< 10 g/dL) 11%
Pain 5%
Purpura 15%
Gross bleeding 3%
Serum creatinine> 1.3 mg/dL 45%
Elevated alkaline phosphatase 26%
Physical finding
Palpable liver 24%
Hypercalcemia(>11 mg/dL) 2%
Proteinuria( > 1 g/24 hr) 55%
i li h h i %Palpable spleen 5%
Lymphadenopathy 3%
Macroglossia 9%
Urine light chain 73%
Ќ chain 23%
ג chain 50%Macroglossia 9%
Kyle, RA, Semin Hematol 1995; 32: 45.

Syndrome at diagnosis in 229 pts with AL l id iamyloidosis
Syndromes Without myeloma
(182 pts)
With myeloma
(47 pts)Nephrotic syndrome % %Nephrotic syndrome 37% 13%
Carpal tunnel syndrome 21% 38%
h f lCongestive heart failure 23% 23%
Peripheral neuropathy 20% 6%
Orthostatic hypotension 16% 4%
Kyle, RA, Mayo Clin Proc 1983, 58:665


Echocardiography
LVH & RVH ith ki LVH & RVH with sparking appearance, no restrictionEF 6 %EF 60%Mild TR & MR

Cardiac amyloidosisCardiac amyloidosis
ECG Decreased amplitude of the QRS complex in the limb lead,
Pseudoinfarct pattern across the anterior lead

Bone SurveyBone Survey

Case 6A 62 year old white female housewife develops y p
periorbital edema in the AM followed by pedal and ankle edema later in the day, and a 6 kg weight gain. PE shows BP 142/84 mm.Hg, CTS, and edema only. Lab shows Urinalysis 4+ protein, 2-3 rbc, few oval fat bodies, BUN 18 mg/dl, creatinine 0.9 mg/dl, glucose 118 mg/dl, plasma albumin 2.4g/dl, cholesterol 236 mg/dl, and 24 hour urinary protein 10
/dg/day.
1) What serologic tests are helpful in the nephrotic syndrome before biopsy ?p y
2) If the patient was 32 years old rather than 62 years old would the testing be different ?
3) Is biopsy useful here ?

Familial AmyloidosisFamilial Amyloidosis
ADADATTR : most commonRenal disease : less common than ALRenal disease : less common than ALNeuropathy ( Sensori‐motor, ANS )GI : diarrhea, wt. lossNo macroglossiaCardiac involvement : Heart failure uncommon


Case 7A 38 year old. male drug addict is found to have 6g
proteinuria daily and a Scr of 1.4 mg/dl. He is found to be HIV+HIV+.
1) Is this likely to be HIV associated nephropathy (HIV AN) ? If this were HIV AN what laboratory tests would be? If this were HIV AN what laboratory tests would be useful to establish a diagnosis ?
2) What other possibilities could this patient have? What l i i h b h l f l i hi i iserologic tests might be helpful in this patient in
establishing a diagnosis ?

Renal cause
ATN
Nephrotoxic
Glomerular disease
IgA nephropathyATIN
IschemicPigment-relates
Immune complex GNOther glomerulopathy
Drug induced
Vascular disease
HUSCrystal asso. Nephropathy
TTPATIN
Drug-induceInfection
Uric acidSulfadiazine
AcyclovirIndinavirInfection
Plasmacytic interstitial nephritisIndinavirfoscanet

HIV asso. ATN
NephrotoxicIschemic
Pigmented induce
Rhabdomyolysis
Amphotericin BAminoglycoside
Pentamidine
Ischemic
ShockVasopresser Rx hemolysis
PentamidineRadiocontrast
NSAIDSRitonavir
Vasopresser Rxcocaine
Foscanetcidofovir
Am J Med Sci 2000:319;385-91

Glomerular Syndromes in HIVGlomerular Syndromes in HIV
1) HIV‐associated TMA
2) HIV‐associated IC renal disease
3) Classic HIV associated nephropathy3) Classic HIV‐associated nephropathy

Glomerular disease diag. by renal biopsy in 136 consecutive HIV pt.
Type of glomerular disease N=127 Type of tubulointerstitial disease N=9
FSGS 88
MPGN 13
MCD 6
Interstitial nephritis 5
ATN 3
Malignant lymphoma 1MCD 6
MN 5
Lupus like nephritis 4
Malignant lymphoma 1
Amyloidosis 4
Acute postinfectious GN 2
F l t l ti i GN Focal segmental necrotizing GN 1
HUS 1
IgA nephropathy 1
Immunolactoid glomerulopathy 1
End stage kidney disease 1Semin nephro;18;406-421:1998

AIDS-Associationed ESRD Incident in US
ESRD from AIDS Deaths in American
American with AIDS/Yr
1000
1200
25500
600
800
15500
20500
s/yr
s/yr
400 10500Cas
esC
ases
0
200
500
5500
(Bruggeman et al. JASN, 2001)
90 91 92 93 94 95 96 97 98 99 '00 '01 '02