Embed Size (px)
Citation preview

Bones and joints InfectionsBones and joints Infections
44thth year Medical Student year Medical StudentWeerachai KosuwonWeerachai Kosuwon

ว�ตถ�ประสงค�ว�ตถ�ประสงค�
ให�น�กศ�กษาร��จ�กภาวะต�ดเช��อท!"พบได�บ&อยในภาคตะว�นออกเฉ!ยงเหน�อให�น�กศ�กษาร��จ�กภาวะต�ดเช��อท!"พบได�บ&อยในภาคตะว�นออกเฉ!ยงเหน�อ ให�น�กศ�กษาเข�าใจพยาธ�ก+าเน�ด อาการ อาการแสดงของโรคต�ดเช��อให�น�กศ�กษาเข�าใจพยาธ�ก+าเน�ด อาการ อาการแสดงของโรคต�ดเช��อ สามารถตรวจร&างกายทางออร�โธป0ด�กส�ท!"เก!"ยวข�องก�บการต�ดเช��อและทราบสามารถตรวจร&างกายทางออร�โธป0ด�กส�ท!"เก!"ยวข�องก�บการต�ดเช��อและทราบ
ถ�งการท+าห�ตถการ การเจาะข�อและกระด�กได�อย&างถ�กต�องและเหมาะสมถ�งการท+าห�ตถการ การเจาะข�อและกระด�กได�อย&างถ�กต�องและเหมาะสม สามารถส�งการตรวจเพ�"มเต�มทางห�องปฏ�บ�ต�การได�อย&างเหมาะสมสามารถส�งการตรวจเพ�"มเต�มทางห�องปฏ�บ�ต�การได�อย&างเหมาะสม สามารถให�ค+าอธ�บายแก& ผ��ป4วยและญาต�ผ��ป4วยท!"เป6นโรคได�อย&างถ�กต�องสามารถให�ค+าอธ�บายแก& ผ��ป4วยและญาต�ผ��ป4วยท!"เป6นโรคได�อย&างถ�กต�อง

ชน�ดของการต�ดเช��อท!"กระด�กชน�ดของการต�ดเช��อท!"กระด�ก
กระด�กต�ดเช��อจากทางกระแสเล�อด กระด�กต�ดเช��อจากทางกระแสเล�อด (Haematogenous (Haematogenous osteomyelitis)osteomyelitis)
กระด�กต�ดเช��อจากกระด�กห�กม!แผลเป0ด กระด�กต�ดเช��อจากกระด�กห�กม!แผลเป0ด (infected open (infected open fracture)fracture)
กระด�กต�ดเช��อจากการล�กลามมาจากเน��อเย��อรอบข�างกระด�กต�ดเช��อจากการล�กลามมาจากเน��อเย��อรอบข�าง

Types of Hematogenous Types of Hematogenous osteomyelitisosteomyelitis
1.1. Acute hematogenous osteomyelitisAcute hematogenous osteomyelitis2.2. Chronic hematogenous osteomyelitisChronic hematogenous osteomyelitis3.3. Subacute hematogenous osteomyelitisSubacute hematogenous osteomyelitis

Acute haematogenous osteomyelitisAcute haematogenous osteomyelitis
ม�กเป6นในเด8กม�กเป6นในเด8ก พบมากท!"กระด�กรอบเข&า พบมากท!"กระด�กรอบเข&า (distal femoral and proximal (distal femoral and proximal
tibial metaphyses)tibial metaphyses) ม!ประว�ต�ได�ร�บบาดเจ8บในบร�เวณด�งกล&าวมาก&อนม!ประว�ต�ได�ร�บบาดเจ8บในบร�เวณด�งกล&าวมาก&อน ม!ไข�ส�ง ม!ไข�ส�ง irritability lethargyirritability lethargy ผ�วหน�งบร�เวณท!"เป6นม!การอ�กเสบ บวม เด8กจะเด�นลงน�+าหน�กขาด�านท!"เป6นผ�วหน�งบร�เวณท!"เป6นม!การอ�กเสบ บวม เด8กจะเด�นลงน�+าหน�กขาด�านท!"เป6น
ไม&ได� ไม&ยอมใช�แขน ขาด�านท!"เป6นโรคไม&ได� ไม&ยอมใช�แขน ขาด�านท!"เป6นโรค อาจจะตรวจพบ ฝ;หนองท!"ผ�วหน�ง หร�อม!การต�ดเช��อท!"อว�ยวะอ�"นๆอาจจะตรวจพบ ฝ;หนองท!"ผ�วหน�ง หร�อม!การต�ดเช��อท!"อว�ยวะอ�"นๆ

Acute hematogenous osteomyelitisAcute hematogenous osteomyelitis

Pathophysiology and Clinical Pathophysiology and Clinical findings findings
Acute inflammation Acute inflammation and abscess increase and abscess increase intraosseous pressureintraosseous pressure
Pus drainage to Pus drainage to subperiostium viasubperiostium via Volkmann’s canal Volkmann’s canal
Ischemia and necrosis Ischemia and necrosis of cortexof cortex
sinus drainage at skinsinus drainage at skin
Pain , swelling and Pain , swelling and fever limitation of fever limitation of motionmotion
localized swelling at localized swelling at metaphyseal region metaphyseal region and Periostium and Periostium reaction by x-rayreaction by x-ray
Involucrum and Involucrum and sequestrum sequestrum

involucrum
pus
sequestrum
Pathophysiology of acute hematogenous


RadiographyRadiography
In acute stage, there is no any bone change In acute stage, there is no any bone change however, there may present soft tissue however, there may present soft tissue swelling. After 10 days periosteum reaction swelling. After 10 days periosteum reaction will be presented.will be presented.
In sub-acute and chronic stages will present In sub-acute and chronic stages will present sequestrum or osseous localized abscess sequestrum or osseous localized abscess (Brodies’ abscess) (Brodies’ abscess)

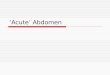
X-ray of proximal tibia shows sclerotic change and some areas of osteolytic lesions. Periostial reaction

Heamatogenous Osteomyelitis of proximal tibia. Maximum point of tenderness

Needle aspiration at the maximum point of tendernessNeedle aspiration at the maximum point of tendernessNeedle aspiration at the maximum point of tenderness


DiagnosisDiagnosis
Bone pain plus fever in a child constitutes Bone pain plus fever in a child constitutes osteomyelitis until proved otherwise.osteomyelitis until proved otherwise.
Definitive diagnosis: isolated pathogen from the Definitive diagnosis: isolated pathogen from the bone lesion and blood culturebone lesion and blood culture
Bone aspiration, using 18 gauge spinal needle at Bone aspiration, using 18 gauge spinal needle at the point of maximal tenderness.the point of maximal tenderness.
Aspirate sub-periosteal abscess and insert Aspirate sub-periosteal abscess and insert through the cortex and into the cancellous bone.through the cortex and into the cancellous bone.
Sent fluid or blood for culture( positive 50-87%) Sent fluid or blood for culture( positive 50-87%)

Sinugraphy of the chronic osteomyelitis

Treatment of acute osteomyelitisTreatment of acute osteomyelitis
Rest or immobilizationRest or immobilization Hydration and start iv anti-staphylococcusHydration and start iv anti-staphylococcusIf clinical conditions do not response within 48 If clinical conditions do not response within 48
hours , surgical drainage is indicated.hours , surgical drainage is indicated.The IV antibiotics (cloxacillin 5 gm/d or The IV antibiotics (cloxacillin 5 gm/d or
nafcillin or vancomycin) should be nafcillin or vancomycin) should be continually used for 4 weeks and orally for continually used for 4 weeks and orally for 4-6 weeks or until ESR or C-reactive protein 4-6 weeks or until ESR or C-reactive protein level is normal. level is normal.

Indications for surgeryIndications for surgery
1.1. Soft tissue abscessSoft tissue abscess2.2. Clinical not response within 48 hrs after Clinical not response within 48 hrs after
specific antibioticspecific antibiotic3.3. Joint abscessJoint abscess

RemarkRemark
If all culture results are negative, bone If all culture results are negative, bone biopsy is indicated unless clinical biopsy is indicated unless clinical improvement with empirical therapyimprovement with empirical therapy

Chronic and sub-acute osteomyelitis Chronic and sub-acute osteomyelitis
It is a complication of acute osteomyelitis It is a complication of acute osteomyelitis consisted withconsisted with
1.1. Sequestrum formationSequestrum formation2.2. InvolucrumInvolucrum3.3. Sinus tractsSinus tracts4.4. Acute on top chronic osteomyelitisAcute on top chronic osteomyelitis5.5. ESR and CRP are increasedESR and CRP are increased

Treatment chronic osteomyelitisTreatment chronic osteomyelitis
Identify organism by gram stain and cultureIdentify organism by gram stain and culture Antibiotics iv 4 wks. and/or local gentamycin Antibiotics iv 4 wks. and/or local gentamycin
bead.bead. Well develop involucrum and sequestrum Well develop involucrum and sequestrum
are indicated for sequestrectomyare indicated for sequestrectomy Soft tissue reconstruction if neededSoft tissue reconstruction if needed


Local antibiotic (gentamycin bead)Local antibiotic (gentamycin bead)

Differential diagnosisDifferential diagnosisof Acute hematogenous of Acute hematogenous
osteomyelitisosteomyelitis Ewing sarcomaEwing sarcoma OsteosarcomaOsteosarcoma Sickle cell anemiaSickle cell anemia Soft tissue infectionSoft tissue infection FractureFracture

ภาวะแทรกซ�อนของ ภาวะแทรกซ�อนของ acute osteomyelitisacute osteomyelitis
Growth arrestGrowth arrest septic arthritisseptic arthritis pathologic fracturepathologic fracture septicemiasepticemia chronic osteomyelitischronic osteomyelitis

Infected fractureInfected fracture
หมายข��นการต�ดเช��อท!"เก�ดข��นหล�งจากม!การห�กของกระด�กหมายข��นการต�ดเช��อท!"เก�ดข��นหล�งจากม!การห�กของกระด�ก ม�กเก�ดข��นใน ม�กเก�ดข��นใน open fracture open fracture หร�อได�ร�บการผ&าต�ด หร�อได�ร�บการผ&าต�ด open reductionopen reduction ม�กจะต�ดเช��อหลายชน�ดท��ง ม�กจะต�ดเช��อหลายชน�ดท��ง S. aureus S. aureus และ และ Gram negative Gram negative
bacteriabacteria ส&วนใหญ&ร&วมก�บการม! ส&วนใหญ&ร&วมก�บการม! implant implant อย�&ท!"กระด�กเช&น อย�&ท!"กระด�กเช&น plate screws, IM plate screws, IM
nail nail เป6นต�นเป6นต�น ม!ประว�ตได�ร�บการผ&าต�ดหลายคร��ง หร�อหล�งผ&าต�ดม!ไข� แผลม!หนองไหลออกมา แผลม!ประว�ตได�ร�บการผ&าต�ดหลายคร��ง หร�อหล�งผ&าต�ดม!ไข� แผลม!หนองไหลออกมา แผล
ต�ดเช��ออาจจะเก�ดข��นภายใน ต�ดเช��ออาจจะเก�ดข��นภายใน 1 1 ส�ปดาห� หร�ออาจเก�ดข��นหลายเด�อนหล�งผ&าต�ดส�ปดาห� หร�ออาจเก�ดข��นหลายเด�อนหล�งผ&าต�ด

Pathophysiology of infected open Pathophysiology of infected open fracturefracture
Once the organism reach the bone and soft Once the organism reach the bone and soft tissue, suppurative formation (edema, tissue, suppurative formation (edema, vascular congestion and small vessel vascular congestion and small vessel thrombosis. thrombosis. Acute osteomyelitisAcute osteomyelitis
Blood supplies to the bone reduce and dead Blood supplies to the bone reduce and dead bone is developed: If acute stage is unable bone is developed: If acute stage is unable to control: fibrous tissue and chronic to control: fibrous tissue and chronic inflammation occur around the granulations inflammation occur around the granulations and dead boneand dead bone

Pathophysiology of infected open Pathophysiology of infected open fracturefracture
Dead bone is absorbed by granulation Dead bone is absorbed by granulation tissue at its surface and junction of living tissue at its surface and junction of living and necrotic boneand necrotic bone
Dead Cortical bone
Lysis of Cancellous bone
Granulation tissue

Pathophysiology of infected open Pathophysiology of infected open fracturefracture
Cancellous boneCancellous bone is absorbed rapidly and is absorbed rapidly and sequestrated or lyses in 2-3 wkssequestrated or lyses in 2-3 wks
Cortical boneCortical bone requires 2 wks-6 months for requires 2 wks-6 months for sequestration and is slowly eroded and sequestration and is slowly eroded and absorbed by granulation tissueabsorbed by granulation tissue

Involucrum
sequestrum
Pathophysiology of infected open fracture

Pus and sinus tract
External fixator

Open fracture tibia and fibula, This was one week after debridement and internal fixation with plate and screws
Swelling and draining discharge from the wound

Infected non-union

Conditioning film
Biomaterial
Host tissue
Bacteria
BiomaterialConditioning film
Bacteria
Host cell and PMN
Glycocalyx
The race for the surface

การต�ดเช��อท!"กระด�กการต�ดเช��อท!"กระด�ก Hematogenous Hematogenous
OsteomyelitisOsteomyelitis ม�กเป6นในเด8กม�กเป6นในเด8ก เป6นท!" เป6นท!" MetaphysisMetaphysis ความร�นแรงข��นก�บอาย�ความร�นแรงข��นก�บอาย�, , ได�ร�บการได�ร�บการ
ร�กษาช�าร�กษาช�า เช��อม�กจะเป6น เช��อม�กจะเป6น
Staphylococcus Staphylococcus aureusaureus
Infected Open Infected Open FractureFracture
เป6นได�ท�กกล�&มอาย� เป6นได�ท�กกล�&มอาย� เป6นได�ท�กต+าแหน&งของกระด�กข��นก�บเป6นได�ท�กต+าแหน&งของกระด�กข��นก�บ
ว&ากระด�กช��นไหนห�กว&ากระด�กช��นไหนห�ก ความร�นแรงข��นก�บขนาดของการได�ความร�นแรงข��นก�บขนาดของการได�
ร�บบาดเจ8บร�บบาดเจ8บ Multiple organismMultiple organism

หล�กการร�กษากระด�กอ�กเสบต�ดเช��อหล�กการร�กษากระด�กอ�กเสบต�ดเช��อ ให�การว�น�จฉ�ยให�ได� ให�การว�น�จฉ�ยให�ได� aspiration, plain X-ray, ESR,aspiration, plain X-ray, ESR,
CRP, bone scanCRP, bone scan ตรวจหาเช��อ ตรวจหาเช��อ Heamoculture, gram staining Heamoculture, gram staining ให�ยาปฏ�ช!วนะท!"เหมาะสม ให�ยาปฏ�ช!วนะท!"เหมาะสม (cloxacillin 5 mg/d or (cloxacillin 5 mg/d or
vancomycin vancomycin IVIV + aminoglycoside + aminoglycoside 4-64-6 wks wks and Oral and Oral 88 Wks Wks
ก+าจ�ดเน��อเย�"อท!"ตายท��งก+าจ�ดเน��อเย�"อท!"ตายท��ง ตกแต&งเน��อเย�"อท!"ด!ทดแทนเพ�"อเพ�"มการไหลเว!ยนของเล�อดด!ข��นตกแต&งเน��อเย�"อท!"ด!ทดแทนเพ�"อเพ�"มการไหลเว!ยนของเล�อดด!ข��น ส&งเสร�มความม�"นคงและการต�ดของกระด�กท!"ห�กส&งเสร�มความม�"นคงและการต�ดของกระด�กท!"ห�ก ฟ\]นฟ�สภาพของผ��ป4วยท��งอาหารและความแข8งแรงของร&างกายฟ\]นฟ�สภาพของผ��ป4วยท��งอาหารและความแข8งแรงของร&างกาย


Complications of infected open Complications of infected open fracturefracture
1. infected non union1. infected non union 2. delayed union2. delayed union 3. acute on top chronic osteomyelitis3. acute on top chronic osteomyelitis 4. amputation4. amputation 5. chronic sinus drainage caused squamous 5. chronic sinus drainage caused squamous
cell CA of the skincell CA of the skin

Septic arthritisSeptic arthritis
Staphylococcus aureusStaphylococcus aureus
Knee joint Knee joint 38%,38%, Hip joint Hip joint 32%32% Fever, painful joint swelling, limit motionFever, painful joint swelling, limit motion Underlying diseases DM, Renal failureUnderlying diseases DM, Renal failure Intra-articular injection, Intra-articular injuries Intra-articular injection, Intra-articular injuries
or surgeryor surgery

Pathogenesis of Pathogenesis of septic arthritisseptic arthritis
Haematogenous infection Haematogenous infection (synovial tissue is (synovial tissue is very vascular and does not have a very vascular and does not have a basement membrane).basement membrane).
Extension from adjacent tissue or structures Extension from adjacent tissue or structures e.g. osteomyelitis, myositis.e.g. osteomyelitis, myositis.
Contamination from open joint injuries, Contamination from open joint injuries, intraarticular injection or intraoperative intraarticular injection or intraoperative procedureprocedure

Clinical feature of septic arthritisClinical feature of septic arthritis
Painful swelling and limitation of the Painful swelling and limitation of the affected jointaffected joint
FeverFever Generalized tenderness of periarticular area Generalized tenderness of periarticular area
(in contrast to the point tenderness as found (in contrast to the point tenderness as found in acute osteomyelitis)in acute osteomyelitis)
Palpable joint effusion (90%)Palpable joint effusion (90%) Regional lymph nodes positiveRegional lymph nodes positive

Swelling at the knee joint

Needle aspiration

Joints AspirationJoints Aspiration



Clinical feature of septic arthritisClinical feature of septic arthritis
Misleading symptoms in septic arthritisMisleading symptoms in septic arthritis1. Septic hip :patient compliant pain at anterior 1. Septic hip :patient compliant pain at anterior knee or just above knee jointknee or just above knee jointใใ2. Septic sacroiliac joint: refer pain to abdomen2. Septic sacroiliac joint: refer pain to abdomen3. OA joint: pain is common persistent symptom, 3. OA joint: pain is common persistent symptom, therefore,therefore, a definitive diagnosis may be delayeda definitive diagnosis may be delayed4. Neonate: FUO and psuedoparalysis is 4. Neonate: FUO and psuedoparalysis is commonly found.commonly found.

DiagnosisDiagnosis
Joint fluid aspiration and examination for: Joint fluid aspiration and examination for: gram stain, culture, WBC, Crystals, glucose gram stain, culture, WBC, Crystals, glucose levellevel
Blood cultureBlood culture Blood test: CBC, ESR, CRPBlood test: CBC, ESR, CRP RadiographRadiograph

Septic arthritis of the Knee jointSeptic arthritis of the Knee joint

Early radiographic bone destruction in both sides of the joint

Synovial analysesSynovial analyses
00.8-1Mononuclear3,000-10,000Reactive
<0.5>0.570% PMN3,000-30,000Fungus
<200.5-150%-70% PMN10,000-20,000TB
>90<0.5>90% PMN10,000-100,000Septic
00.8-1Mononuclear200-600Normal
% positive smear
Glu ratioSyn:bld
Cell typeWBC cell/mmCondition

Management of Management of Septic arthritisSeptic arthritis
Diagnosis: Aspiration, and Bacterial diagnosis e.g. Diagnosis: Aspiration, and Bacterial diagnosis e.g. gram staining, culture gram staining, culture (50%)(50%) Staphylococcus Staphylococcus ((80%80%))
Appropriate antibiotics CloxacillinAppropriate antibiotics Cloxacillin 5 gm/d 5 gm/d IVIV for 3 for 3 wks and oral wks and oral 44 wks wks (vancomycin or 1(vancomycin or 1stst Gen Ceph) Gen Ceph)
Reduce intraarticular pressure e.g. repeated Reduce intraarticular pressure e.g. repeated aspiration, arthroscopic drainage, or arthrotomyaspiration, arthroscopic drainage, or arthrotomy
Rest : traction (skin or skeletal traction), Rest : traction (skin or skeletal traction), immobilizationimmobilization
Continuous passive motionContinuous passive motion

IndicationIndicationss for arthrotomy or for arthrotomy or arthroscopic drainage arthroscopic drainage
Very turbid pusVery turbid pus Deep joint e.g. hip and shoulder jointsDeep joint e.g. hip and shoulder joints Patient’s cooperationPatient’s cooperation increasing amount of pus from every day increasing amount of pus from every day
aspirationaspiration no clinical responses after 48 hr. conservative no clinical responses after 48 hr. conservative
treatmenttreatment and /or persistently high neutrophil and /or persistently high neutrophil count >25,000 per ml.count >25,000 per ml.
Osteomyelitis is a complicationOsteomyelitis is a complication Present of loculationPresent of loculation

Comparison of drainage proceduresComparison of drainage procedures
expensivemodestinexpensivecost
prolongshortshortRecovery time
significantmoderateminimalMorbidity
nonoyesNeed patient’s cooperation
yesyesNoAdhesion lysis
ExcellentExcellentpoorDrainage capability of turbid pus
All jointsLimited to large joint
Limited to large superficial joint
eg. knee
Joint
Regional/genRegional/genlocalAnesthesia
ORORbedsideLocation
ArthrotomyArthroscopyAspiration

Complications of septic arthritisComplications of septic arthritis
eearly degenerative arthritisarly degenerative arthritis oosteomyelitissteomyelitis septicemicsepticemic cchronic septic arthritishronic septic arthritis ppathological dislocationathological dislocation

Complication of septic arthritis; osteomyelitisOf the tarsal bones

Differential DiagnosisDifferential Diagnosisseptic arthritis of the hip jointseptic arthritis of the hip joint
Soft tissue infection eg. Psoas abscess Soft tissue infection eg. Psoas abscess Trochanteric and Iliopectineal bursitisTrochanteric and Iliopectineal bursitis Perthes’diseasePerthes’disease Slip capital epiphysisSlip capital epiphysis ChondroblastomaChondroblastoma Matastatic tumorMatastatic tumor

Psoas abscess clinical Psoas abscess clinical presentationspresentations
ผ��ป4วยสามรถเด�นลงน�+าหน�กได�ในขณะผ��ป4วยสามรถเด�นลงน�+าหน�กได�ในขณะท!" ท!" septic hip septic hip ไม&สามารถลงน�+าไม&สามารถลงน�+าหน�กท!"ขาด�านท!"เป6นได�หน�กท!"ขาด�านท!"เป6นได�
ผ��ป4วยม! ผ��ป4วยม! flexion flexion contracture contracture ในภาพท&าย�นในภาพท&าย�นตะโพกด�านขวางอ และ ตะโพกด�านขวางอ และ Thomas’stest positiveThomas’stest positive

Differential diagnosis Differential diagnosis of the septic knee of the septic knee
Gouty or pseudogouty arthritisGouty or pseudogouty arthritis Transient synovitisTransient synovitis Rieter’s disease Rieter’s disease Rheumatoid arthritisRheumatoid arthritis Prepatellar bursitisPrepatellar bursitis Osteochondritis dissecansOsteochondritis dissecans Pigmented villonodular synovitisPigmented villonodular synovitis

Spinal tuberculosisSpinal tuberculosis
It is a granulomatous infection caused by It is a granulomatous infection caused by Mycobacterium tuberculosisMycobacterium tuberculosis
Percival Pott described 1779 Percival Pott described 1779 ““Pott’s disease”Pott’s disease”In HIV neg patients, spinal TB occurs in 1% of In HIV neg patients, spinal TB occurs in 1% of
all tuberculosis, in contrast, 60% found in all tuberculosis, in contrast, 60% found in HIV pos.HIV pos.

TB spineTB spine
Spinal TB represents 50-60% of Spinal TB represents 50-60% of musculoskeletal TBmusculoskeletal TB
Hematogenous spread from primary foci in Hematogenous spread from primary foci in the lung or genitourinary tractthe lung or genitourinary tract
Thoracolumbar region is the most commonly Thoracolumbar region is the most commonly foundfound

Pathogenesis of TB spinePathogenesis of TB spine The infection starts at metaphysis of The infection starts at metaphysis of
vertebra, pathologic changes occur more vertebra, pathologic changes occur more slowly, allowing greater deformity to develop slowly, allowing greater deformity to develop before symptoms appear.The abscess occubefore symptoms appear.The abscess occurs and extend to other vertebra.rs and extend to other vertebra.
The disk intact initially after the infection The disk intact initially after the infection extend to another adjacent vertebra then the extend to another adjacent vertebra then the disk will destroy.disk will destroy.
Neurologic involvement results from Neurologic involvement results from compression by epidural granuloma or compression by epidural granuloma or sequestrum or disk protrusion into the spinal sequestrum or disk protrusion into the spinal canal.canal.
Risk factors: age, cephalad level, lack of Risk factors: age, cephalad level, lack of paraspinal abcessparaspinal abcess

PathophysiologyPathophysiology
12
3 4

Neurological complication in TB Neurological complication in TB spinesspines
Dural sacGranulomatous materialor disc or sequestrum

Clinical findings in TB spineClinical findings in TB spine Back pain and gibbus, Back pain and gibbus, CChronic illness, hronic illness, wweight loss, fever eight loss, fever more than more than
one month (contrast, pyogenic spondylitis)one month (contrast, pyogenic spondylitis) Spasm of the muscle at the affected spineSpasm of the muscle at the affected spine Limit motions of the affected spineLimit motions of the affected spine Point of tenderness at the affected spinePoint of tenderness at the affected spine Kyphosis at the affected siteKyphosis at the affected site Neurological involvement can be detectedNeurological involvement can be detected Cold abscess may be detected at lumbar Cold abscess may be detected at lumbar
triangle or intraabdomen (Psoas abscess)triangle or intraabdomen (Psoas abscess)


Investigations for TB spineInvestigations for TB spine
Plain X-ray at the spine AP/Lat alwaysPlain X-ray at the spine AP/Lat always CBC not specific, ESR increase CBC not specific, ESR increase 25%25% Biopsy:Open or needle biopsy, AFB Biopsy:Open or needle biopsy, AFB
positive, culture takes time 10 wk., PCRpositive, culture takes time 10 wk., PCR sensitivity 97% accuracy 92% sensitivity 97% accuracy 92%
CT and MRI may be requestedCT and MRI may be requested Clinical diagnosis and therapeutic diagnosisClinical diagnosis and therapeutic diagnosis

TB spineTB spine
Intervertebral disk involvement 46%-72%Intervertebral disk involvement 46%-72% Para vertebral abscess found 55%-96%Para vertebral abscess found 55%-96% Paraplegia or paraparesis encountered at Paraplegia or paraparesis encountered at
T4-T5 level, due to this area has the poorest T4-T5 level, due to this area has the poorest vascular supply of spinal cord.vascular supply of spinal cord.

Para vertebral abscess
Narrowing disk spaces

TB spine: narrowing of disc space and paravertebral soft tissue shadow

Bony destruction
Disk spacenarrowing
Spinal compression
MRI

Para vertebral abscess
MRI

Anti-TB drugsAnti-TB drugsTriple drugs of I,R,P or ETriple drugs of I,R,P or E
300mg/d for 12 months600-900mg/d for 12 months1.5-2 mg/d for 2-3 months15mg/kg/d for 2-4 months
IsoniazidRifampin
PyrazinamideEthambutol
DosageDrug

Differential Diagnosis of TB spineDifferential Diagnosis of TB spine
Metastatic tumorMetastatic tumor Osteoporotic fracture Osteoporotic fracture Pyogenic spondylitisPyogenic spondylitis Pyogenic discitisPyogenic discitis Epidural AbscessEpidural Abscess

Differential diagnosis betweenTB spine and CA metastasis
Para-vertebral abscess
Narrowing disk space
Lysis of pedicleCollapse of the body

Management of TB spineManagement of TB spineGoals of treatment Goals of treatment 1. Eradication of the infection: Anti TB drugs INH, 1. Eradication of the infection: Anti TB drugs INH,
Rifampicin, Pyrazinamide, Ethambutol, Rifampicin, Pyrazinamide, Ethambutol, Streptomycin; Surgical debridementStreptomycin; Surgical debridement
2. Prevention of further neurologic deterioration 2. Prevention of further neurologic deterioration by early decompression or debridement by early decompression or debridement (vertebral resection)(vertebral resection)
3. Prevention or correction of spinal deformity by 3. Prevention or correction of spinal deformity by immobilization the spine e.g.. Body plaster of immobilization the spine e.g.. Body plaster of Paris jacket, internal fixation with rods or pediclParis jacket, internal fixation with rods or pedicle screwse screws

Prognosis of TB spinePrognosis of TB spine Surgical treatment Vs Conservative Surgical treatment Vs Conservative
treatment in neurological outcomes : 94% Vs treatment in neurological outcomes : 94% Vs 79% improvement79% improvement
Complication from surgical treatment Complication from surgical treatment Mortality rate 3%; early diagnosis+ anti TB Mortality rate 3%; early diagnosis+ anti TB drugs mortality rate 5%drugs mortality rate 5%
Healing (fusion) rates Surgical Vs Healing (fusion) rates Surgical Vs Conservative treatment : 70% vs 23% at 12 Conservative treatment : 70% vs 23% at 12 months; 85% Vs 52% at 18 monthsmonths; 85% Vs 52% at 18 months;;
92% Vs 84% at 5 yr.92% Vs 84% at 5 yr.