Embed Size (px)
Citation preview

1320
TABLE I-PREVIOUS ADVERSE REACTIONS TO SEMISYNTHETIC
_ PENICILLINS AND CEPHALOSPORINS
*Carbenicillin, azlocillin, and piperacillin; tcefsulodin, ceftazidime, and cefotaxime.
TABLE II-LUNG FUNCTION* AT START AND END OF A TWO-WEEK
COURSE OF AZTREONAM PLUS TOBRAMYCIN
*Mean and range, values expressed as percentage of normal value for the same height, sex,and age.t Mann- wrutney test for non-parametnc paired data.
noted in all patients. Aztreonam seems to be a safe drug to use inpatients with hypersensitivity to other beta-lactams, and we are nowdoing a clinical trial comparing the clinical efficacy of aztreonamwith that of conventional treatment to identify the place of this drugin the management of patients with CF.
Department of Paediatrics,Rigshospitalet,DK-2100 Copenhagen, Denmark
T. JENSENC. KOCH
Department of Clinical Microbiology,State Seruminstitute,Rigshospitalet, Copenhagen
S. S. PEDERSENN. HØIBY
1. Moss RB, Babin S, Hsu YP, Blessing-Moore J, Lewiston NJ. Allergy to semisyntheticpenicillins in cystic fibrosis. J Pediatr 1984; 104: 460-66.
2. Stead RJ, Kennedy HG, Hodson ME, Batten JC. Adverse reactions to piperacillin incystic fibrosis. Lancet 1984; i: 857-58.
3. Wise R, Andrews JM, Hancox J. SQ26,776, a novel beta-lactam: an in-vitrocomparison with other antimicrobial agents. J Antimicrob Chemother 1981; 8 (supplE): 39-47.
4. Adkinson NF, Saxon A, Spence MR, Swabb EA. Cross-allergenicity andimmunogenicity of aztreonam. Rev Infect Dis 1985; 7 (suppl 4): 613-21.
CAPD PERITONITIS
SIR,-During 1985, when we used cefotaxime as first-line
therapy for CAPD peritonitis, the incidence of methicillinresistance in coagulase-negative staphylococci isolated frominfected peritoneal dialysis fluid rose from 46 % to 75 %. This led toan unacceptable failure rate. We now use netilmicin and
vancomycin as first-line therapy since currently 48% of strains ofcoagulase-negative staphylococci from infected peritoneal dialysisfluid are methicillin resistant, precluding the reintroduction of acephalosporin to our treatment regimen. We share the concern ofDr Muscat and colleagues (May 16, p1142) over the potential forototoxicity of aminoglycoside/vancomycin combinations and forthis reason have considered potentially less toxic agents.We have just completed a pilot study in 11 patients with twelve
episodes of proven gram-positive peritonitis, using teicoplanin, aglycopeptide with little or no ototoxicity or nephrotoxicity.1 On thebasis of our pharmacokinetic data/ we add 20 mg to each litre of
dialysis fluid, with a single dose of 400 mg intravenously if thepatient is febrile. Serum levels are predictable, and the dosingregimen is easily modified in the second and third week oftreatment, to maintaih serum levels below 10 mg/1.Cure was achieved in 10 patients. The single failure was in a
patient with recurrent Staphylococcus aureus peritonitis who wastreated twice with teicoplanin before unsuccessful therapy withvancomycin. Teicoplanin was well tolerated and there was noevidence of ototoxicity (as determined by serial audiometry) or offurther decline in residual renal function. All 10 patients haveremained well at follow-up (4 weeks to 11 months). Although theemergence of teicoplanin-resistant strains of coagulase-negativestaphylococci-"-’ has been noted in other centres, this has not
happened in our hospital. 6
Clearly additional cover is needed in case the patient is found tohave a gram-negative infection, as happens in about 30% of cases.We are planning to use aztreonam, a monobactam believed to benon-toxic in patients in renal failure,7 to provide this cover in acomparative study of teicoplanin vs vancomycin in CAPD
peritonitis.Unlike Dr Maskell (May 16, p 1142) we find microscopy useful; a
differential white cell count is invaluable in distinguishing betweenbacterial peritonitis and other causes of cloudy dialysis bags such aseosinophilic peritonitis and excessive fibrin production. We agree,however, that routine cultures of any but cloudy bags is a waste oflaboratory time, and that inoculation of blood culture bottles withdialysis fluid should be done in the clinical area by a trained dialysisnurse. This procedure has proved successful in our dialysis unit.
Departments of Medical Microbiologyand Nephrology and Transplantation,
Royal Free Hospital,London NW3 2QG
LOUISE O. NEVILLEROSEMARIE BAILLOD
J. M. T. HAMILTON-MILLERW. BRUMFITT
1. Williams AH, Gruneberg RN. Teicoiplanin. J Antimicrob Chemother 1984; 14:441-48.
2. Neville LO, Baillod R, Grady D, Brumfitt W, Hamilton-Miller JMT. Teicoplanin inpatients with chronic renal failure on dialysis: microbiological and pharmacokineticaspects. Future Trends Chemother (in press).
3. Wilson AP, O’Hare MD, Felmingham D, Gruneberg RN. Teicoplanin resistantcoagulase-negative staphylococci. Lancet 1986; ii: 973.
4. Grant AC, Lacey RW, Brownjohn AM, Turney JH. Teicoplanin-resistant coagulase-negative staphylococci. Lancet 1986; ii: 1166-67.
5. Arioli V, Pallanza R. Teicoplanin-resistant coagulase-negative staphylococci. Lancet1987; i: 38.
6. Brumfitt W, Hamilton-Miller JMT, Neville LO. Teicoplanin-resistant coagulase-negative staphylococci. Lancet 1987; i: 328.
7. Sattler FR, Schramm M, Swabb EA. Safety of aztreonam and SQ26,992 in elderlypatients with renal insuficiency. Rev Infect Dis 1987; 7 (suppl 4): S622-27.
SiR,—The report of the British Society of Antimicrobial
Chemotherapy working party (April 11, p 845) on the treatment ofperitonitis in chronic ambulatory peritoneal dialysis (CAPD) doesnot discuss the effect of peritoneal dialysate in decreasing theactivity of some antibiotics.
For Staphylococcus epidermidis and Pseudornonas aeruginosa, theminimum inhibitory concentrations of aminoglycosides can beeight to sixteen times higher in sterile used dialysate than inconventional laboratory mediae which may explain the poorcorrelation between sensitivity patterns obtained in conventionallaboratory media and the observed clinical course, despiteapparently appropriate doses of intraperitoneal antibiotics. Themechanism for the reduction in antibiotic activity is not clear.
Aminoglycoside activity is known to be influenced by extracellularcalcium and magnesium concentrations and it is postulated thatthere is inhibition of aminoglycoside entry into bacteria byincreased concentrations of extracellular divalent cations.s Theconcentrations of calcium and magnesium in sterile used dialysateare six to eight times higher than those in conventional laboratorymedia, which may partly explain the observed reduction in
aminoglycoside activity. Similar but smaller decreases in antibioticactivity have been reported for other antibiotics such as ceftazidime.
In uncomplicated cases of CAPD peritonitis the influence of thedialysate on antibiotic activity may not be clinically relevant.
However, in difficult cases the assumption that the antibioticsusceptibility of the organisms is the same in the presence of
peritoneal dialysate as in conventional laboratory media may result

1321
in inappropriate antibiotic therapy. The reduction of antibioticactivity in the presence of peritoneal dialysate may be an importantand unrecognised cause of treatment failure.
Osler Chest Unit,Churchill Hospital,Headington, Oxford OX3 7LJ C. F. CRADDOCK
1.Wilcox MH, Edwards R, Finch RG. Laboratory studies on coagulase-negativestaphylococci from CAPD-associated peritonitis. J Antimicrob Chemother 1985; 15:297-303.
2. Shalit I, Welch DF, San Joaquin VH, Marks MI. In vitro antibacterial activities ofantibiotics against Pseudomonas aeruginosa in peritoneal dialysis fluid. AntimicrobAg Chemother 1985; 27: 908-11.
3. Verbrugh HA, Keane WF, Conroy WE, Paterson PK. Bacterial growth and killing inchronic ambulatory peritoneal dialysis fluids. J Clin Microbiol 1984; 20: 199-203.
4. Craddock CF, Edwards R, Finch RG. Pseudomonas CAPD peritonitis: Laboratorypredictors of clinical failure. J Hosp Infect (in press).
5. Washington JA, Snyder RJ, Kohner PC, Wiltse CG, Ilstrup DM, McCall JT. Effectof cation content of agar on the activity of gentamicin, tobramycin and amikacinagainst Pseudomonas aeruginosa. J Infect Dis 1978; 137: 103-11.
WHEN SHOULD AT-RISK PATIENTS WITHTHALASSAEMIA BE BOOSTED WITH HEPATITIS B
VACCINE?
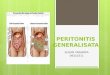
SiR,—Goursaget et aP have reported hepatitis B virus infection inSenegalese children 4-6 years after vaccination and concluded thatchildren in endemic areas should be given a booster dose of hepatitisB vaccine five years after initial vaccination. Viladomin et al on thebasis of antibody titre, suggest a booster every two years, especiallyfor children vaccinated at birth. A similar question arises in patientswith thalassaemia, who are frequently given blood transfusions. Wehave closely followed up, measuring anti-HBs titres for more thanfive years after vaccination, two groups of patients withthalassaemia. Group A (26 patients) had been immunised with fourdoses and group B (74 patients) had been given three doses ofhepatitis B vaccine.3 All patients were seen regularly since they werehaving transfusions every 2-3 weeks.The table summarises anti-HBs titres (’Ausria’; Abbott) one
month and six months after initial vaccination and before thebooster dose five to six years after vaccination.
All patients except 1 seroconverted one month after vaccination;96 % of group A and 84 % of group B had very high titres (more than100 radioimmunoassay units [RU]). During follow-up there was asteady fall in titres. Five to six years after initial vaccination 1 patientin group A and 4 in group B had no detectable antibodies (less than21 RU) and a further 1 in group A and 18 in group B had very low,presumably non-protective titres (2-1-10 RU); high titres (above100 RU) were found in only 33% of group A and 14% of group B.During follow-up 3 patients acquired anti-HBc antibodies
without any clinical or biochemical findings of hepatitis B infection.Alanine aminotransferase was regularly measured and was normalin these 3 patients throughout follow-up. These 3 patients had hadlow titres after the initial vaccination, and before detection ofanti-HBc they had no detectable anti-HBs.
Booster doses, containing only 5 ng/ml HBsAg, were given to96 % of the patients and two weeks later a rise in anti-HBs titre wasfound. All patients had detectable antibodies. Only 1 had a very lowtitre (2-1-10 RU) while titres above 100 RU were found in 67% ofgroup A and in 60 % of group B.Our data suggest that vaccinated patients with thalassaemia, who
are at high risk of hepatitis B infection because of their frequenttransfusions, should be given booster immunisation as indicated bytheir anti-HBs titres at follow-up. A booster dose is recommended
for patients with low, non-protective titres. The time after primaryvaccination when a booster may be required varies from two to morethan five years and seems to be closely related to the primaryantibody response.
Supported in part by the Ministry of Health and Social Services.
Thalassaemia Unit,First Department of Paediatrics,University of Athens,St Sophie’s Children’s Hospital,Athens 115 27 Greece,
NICHOLAS MATSANIOTISCHRISTOS KATTAMISSOPHIA LASKARIMARIA TZETIDESPINA MARKOSOGLOU
1. Coursaget P, Yvonnet B, Chotard J, et al. Seven year study of hepatitis B vaccineefficacy in infants from an endemic area (Senegal). Lancet 1986; ii: 1143-45.
2. Viladomin J, Genesca J, Esteban J, et al. When should at-risk-infants be boosted withhepatitis B vaccine. Lancet 1987; i: 49.
3. Matsaniotis N, Kattamis C, Laskari S, et al Immune responses to hepatitis B vaccine.Lancet 1981, i: 210.
NOCTURNAL ADRENAL SUPPRESSION INCHILDREN INHALING BECLOMETHASONE
DIPROPIONATE
SIR,-Last year1 we reported nocturnal cortisol profiles innineteen asthmatic children; twelve were receiving inhaledbeclomethasone dipropionate (BDP). We observed a dose-
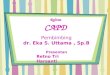
dependent adrenal suppression produced by inhaled BDP. Afterinconsistencies between figs 1 and 2 in our paper were pointed outwe reanalysed the data and found an error in the calculated areaunder the curve (CAUC). Fig 2 has been redrawn, with the revisedunits for CAUC, as follows: The regression equation becomesCAUC =49 172 (±4284) - 40’5( ± 9-5) dose (p< 0001).
Dose of inhaled BOP (fJ9/dalf)Plasma cortisol area-under-the-curve from midnight to 0600 h(CAUC) and dose of inhaled BDP.
This revision (figure) makes no difference to our conclusion.
Department of Growth and Development,Institute of Child Health,London WC1;
and Department of Paediatrics,Cardiothoracic Institute,
London SW3 6HP
C. M. LAWM. A. PREECE
J. O. WARNER
1. Law CM, Marchant JL, Honour JW, Preece MA, Warner JO. Nocturnal adrenalsuppression in children inhaling beclomethasone dipropionate. Lancet 1986; i942-44.
ANTI-HBS TITRES AFTER PRIMARY VACCINATION AND AFTER BOOSTER DOSE