Embed Size (px)
Citation preview

R E V I S T A P O R T U G U E S A D E P N E U M O L O G I A
Vol XII N.º 5 Setembro/Outubro 2006
615
Pneumonia aguda fibrinosa e organizante
Acute fibrinous and organizing pneumonia
Recebido para publicação/received for publication: 06.03.28Aceite para publicação/accepted for publication: 06.05.26
C Damas1
A Morais2
C S Moura3
J A Marques4
ResumoA designação acute fibrinous and organizing pneumonia(AFOP) foi proposta por Beasley et al para os casosem que as características histopatológicas das lesõesnão se enquadravam em outras situações clínicas (agu-das ou subagudas) conhecidas. A presença de fibrinaintra alveolar e de pneumonia organizativa, com dis-tribuição difusa, é a principal alteração histológicaassociada a esta entidade.Os autores descrevem o caso de um doente do sexomasculino, com o diagnóstico de AFOP, por bióp-sia pulmonar cirúrgica. O doente teve uma apre-sentação subaguda, apresentando por queixas prin-cipais tosse, dor torácica e febre. TAC torácicamostrou infiltrados bilaterais, difusos. Após início
Caso ClínicoClinical Case
AbstractThe term Acute Fibrinous and Organizing Pneumo-nia (AFOP) has been proposed by Beasley et al forcases that not fit into the histopathologic criteria ofthe recognized entities described as acute or subacu-te clinical presentations. The presence of intra-alveo-lar fibrin in the form of fibrin ‘balls’ and organizingpneumonia with patchy distribution are the main his-tological features of this entity. We describe the caseof a male patient with the diagnostic of AFOP madeby surgical lung biopsy. He had a subacute presen-tation of symptoms consisting of productive cough,chest pain and fever. Bilateral infiltrates with patchyand diffuse distribution were the predominant fea-tures in his chest HRCT scan. The patient had a good
1 Interna Complementar de Pneumologia2 Assistente Hospitalar de Pneumologia3 Assistente Hospitalar de Anatomia Patológica4 Chefe de Serviço de Pneumologia, Professor Catedrático de Pneumologia da FMUP, Director do Serviço de Pneumologia
Serviço de Pneumologia, Hospital de São João, EPE, PortoFaculdade de Medicina da Universidade do Porto (FMUP)
Correspondência/Correspondence to: Carla DamasTravessa Fernando Namora, 48 5.º Esq.4425 Pedrouços – MaiaPortugal

R E V I S T A P O R T U G U E S A D E P N E U M O L O G I A
Vol XII N.º 5 Setembro/Outubro 2006
616
Pneumonia aguda fibrinosa e organizanteC Damas, A Morais, C S Moura, J A Marques
de corticoterapia sistémica e ciclofosfamida, o do-ente apresentou melhoria clínica significativa. Aoelaborar este caso, os autores esperam acrescentarmais alguns dados sobre esta nova entidade.
Rev Port Pneumol 2006; XII (5): 615-620
Palavras-chave: AFOP, pneumonia organizativa.
clinical course after a treatment with prednisone andcyclophosphamide. Our hope in reporting this casestudy is to add some more data to the discussion ofthis new entity.
Rev Port Pneumol 2006; XII (5): 615-620
Key-words: AFOP, organizing pneumonia.
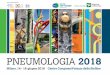
Case reportIn September of 2003 a 66 year old Cauca-sian man, with abnormal lung radiologicalfindings and two month history of produc-tive cough and diffuse thoracic pain was ad-mitted to our hospital. He was a retired judge,smoker (20 packs a year) and had no relevantclinical history previous to the present epi-sode. One month earlier he had visited hisprimary care physician who requested a chestradiograph which showed bilateral reticulon-odular opacifications with basal predominance(Fig. 1). The CT scan confirmed bilateral lungconsolidations with basal and peripheral pre-valence (Fig. 2). Treatment with antibiotic wasprescribed and his clinical condition improved.However radiological worsening with enlarge-ment and spread of lung opacifications (Fig.3) was seen in re-evaluation after antibiotictreatment. After this he was admitted to ourward where he did not present any othersymptoms besides those initially described.On admission he was alert, temperature was36.4º, pulse 92 beats per minute, respiratoryrate 19 breaths per minute and blood pres-sure 133/73 mmHg. No signs of respiratorydiscomfort were seen. Heart sounds and ab-
Table I
domen were normal and there were no pe-ripheral edemas. Reduced respiratorysounds and diffuse crackles were heard in lunglower zones and heart sounds were normal.The WBC count, sedimentation rate, serumelectrolytes, liver tests, creatinine level and uri-nalyses were in the normal range. Sputumspecimens contained few neutrophils, with nomicroorganisms. A serious restrictive ventila-tory pattern and lung diffusion impairmentwere observed in lung function testing (TableI). Arterial blood gas measurements indica-ted a partial pressure of oxygen of 68 mmHg,a partial pressure of carbon dioxide of 39mmHg and the ph 7.37. Cardiac doppler ul-trasonography revealed no marked changes.

R E V I S T A P O R T U G U E S A D E P N E U M O L O G I A
Vol XII N.º 5 Setembro/Outubro 2006
617
Pneumonia aguda fibrinosa e organizanteC Damas, A Morais, C S Moura, J A Marques
Fig. 3
Fig. 2Fig. 1

R E V I S T A P O R T U G U E S A D E P N E U M O L O G I A
Vol XII N.º 5 Setembro/Outubro 2006
618
No visible endobronchial secretions were seenin bronchoscopy examination. Examinationof bronchoalveolar lavage (BAL) specimendid not show any microorganisms. There wereno malignant cells either. The bronchoalveo-lar fluid contained high levels of neutrophils(16.6%), lymphocytes (16%) and eosinophils
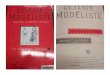
(2.8%). The lymphocytes were predominant-ly CD8+ (CD4-18.8%, CD8-71.1%).During the clinical investigation the patienthad a clinical deterioration, namely with dys-pnoea and fever. Since we could not reach adefinitive diagnosis an open lung biopsy wereperformed. Lung tissue without preservationof alveolar arquitecture was obtained causedby destruction due to an inflammatory pro-cess. There were some granulomas, with areasof necrosis and other with fibrin and con-nective tissue in organization in the alveolarspaces, assuming characteristics of acute fi-brinous pneumonia in resolution.The treatment consisted initially of pred-nisone (1 mg/Kg/day) with clinical, func-tional and radiological improvement. Someweeks later, because of some lateral effectsrelated to prednisone, cyclophosphamide(150 mg/day, po) was added to prednisoneand a good clinical course was observed.Currently, nearly eighteen months after thefirst symptoms the patient is asymptomaticbut still under treatment (prednisone and cy-clophosphamide in tapering doses).
Pneumonia aguda fibrinosa e organizanteC Damas, A Morais, C S Moura, J A Marques
Fig. 4
Fig. 5

R E V I S T A P O R T U G U E S A D E P N E U M O L O G I A
Vol XII N.º 5 Setembro/Outubro 2006
619
Pneumonia aguda fibrinosa e organizanteC Damas, A Morais, C S Moura, J A Marques
DiscussionIn 2002 Beasley MB et al. described a newhistological pattern named Acute FibrinousOrganizing Pneumonia (AFOP) 1 after a re-evaluation of lung specimens obtained inpatients with acute or subacute clinical pres-entations. This histologic pattern is mainlycomposed of the presence of intra-alveo-lar fibrin in the form of fibrin ‘balls’ andorganizing pneumonia with a patchy distri-bution2. These histological characteristicsare separate from those associated with thewell recognized entities described in patientswith acute or subacute clinical presentationssuch as Diffuse Alveolar Damage (DAD),Bronchiolitis Obliterans with OrganizingPneumonia (BOOP) and EosinophilicPneumonia (EP). No hyaline membraneswere seen as in DAD and despite the presen-ce of eosinophils in some specimens, theywere never predominant as in EP. Insteadof organized fibrin balls, Organizing Pneu-monia (OP) has fibroblastic Masson bodieswithin alveolar spaces, ducts and bronchio-les as dominant feature. The authors alsohypothesis that this histological patternmight be a fibrinous variant of DAD1 sincethe mortality rates are similar and the AFOPpattern was observed focally in DAD spec-imens, suggesting inadequate samples insome of the related cases. However, the lackof hyaline membranes, the presence of in-tra-alveolar fibrin in the form of fibrin‘balls’ and the patchy distribution adding toa better clinical course than seen in DADsuggests that the AFOP findings probablyrepresent a singular histologic pattern thatwas never previously identified3.The first aim of describing this case studywas to contribute with more data to dis-cussing the consistency of this new his-
tological pattern. All 17 patients classi-fied as having AFOP by Beasley et al pre-sented constitutional and/or respiratorysymptoms no more than two months be-fore biopsy. Gradually increasing dyspneaand dry cough were the most commonpresenting symptoms. Our patient’s clin-ical features had similarities with most ofthose patients. He had a subacute pre-sentation consisting of productive cough,chest pain and fever, 2 months prior tothe admission in our hospital. ChestHRCT scan demonstrated bilateral infil-trates, initially with basal and peripheralpredominance progressing to other areasand becoming patchy and diffuse. Theseradiological features agree with Beasley etal who observed diffuse parenchymalabnormalities mostly with patchy areas ofinfiltrates predominantly in the lower lungzones. Pulmonary function test ingshowed a moderate to severe restrictiveimpairment (TLC-53%) in our patient. Hehad also a severe decrease in the diffu-sion capacity of the lung for carbon mo-noxide and hypoxia at rest (paO2- 68mmHg). As there is no data about lungfunction in Beasley’s study these resultscannot be compared. However they aresimilar to those described in a case studyby Bawa AS. et al, except for the lower res-trictive impairment observed in this case.In bronchoalveolar lavage fluid (BALF) ahigh neutrophil count (16%) was the pre-dominant finding. There also a lack ofdata about this procedure in other publi-cations. Several medications were used inBeasley’s series, namely steroids and anti-biotics. However no treatment was iden-tified as the most advantageous. The goodclinical course observed in our patient

R E V I S T A P O R T U G U E S A D E P N E U M O L O G I A
Vol XII N.º 5 Setembro/Outubro 2006
620
Pneumonia aguda fibrinosa e organizanteC Damas, A Morais, C S Moura, J A Marques
demonstrates that the addition of cyclo-phosphamide to corticosteroids might bea useful treatment for patients withAFOP.Two different outcomes have been obser-ved by Beasley with nine patients having arapid progression to death (average of 29days). On the contrary, the rest recoveredand are alive and healthy. As in other histo-logical patterns of acute and subacute lunginjury, AFOP can occur as an idiopathicform or be associated with known causesor underlying diseases (infectious causes,connective tissue disorders, occupationaland drug exposures). There were no signi-ficant occupational and drug exposures orevidence of an underlying disease so far.Additionally the examination of sputumand BAL did not reveal any microorganismsbesides normal respiratory flora specimens.These features suggest an idiopathic natureto this clinical case.
In conclusion AFOP seems to define a dis-tinct histological pattern associated with adiffuse lung disease with a better outcomethan others with an acute or subacute pre-sentation. However further presentationof new clinical cases and patient series arenecessary to support the validity of thisnew histological pattern and understand itsclinical picture.
Bibliography1. Beasley, MB, Franks, TJ, Galvin, JR, Gochuico, B,Travis, WD. Acute Fibrinous and Organizing Pneu-monia: a histologic pattern of lung injury and possi-ble variant of difuse alveolar damage. Archives ofPathology and Laboratory Medicine 2002; 126(9):1064-70.2. Cordier, JF. Organizing Pneumonia. Thorax 2002;55:318-28.3. Ryu, JH, Myers, JL, Swensen, SJ. BronchiolarDisorders. Am J Resp and Crit Care Med 2003;168:1277-129.