Embed Size (px)
Citation preview
Cervical Degenerative Disease
- Surgical Approaches to CSM
KNS Main Topic Session
Spine Surgery :
Case-Based Lecture of Spinal Disease
가톨릭의대 인천성모병원 척추센터
김 종 태
Cervical Spondylotic Myelopathy
( CSM ) (1984, Brain )
Impaired function of the spinal cord caused by
advanced degenerative changes of the discs and
facet joints acquired in adult life
Pathophysiology
Direct compression of spinal cord
Ischemia
Repeated microtrauma to cord by neck motion
( Dynamic factor )
Surgery for CSM
Decompression of the spinal cord
-- resolve direct compression & Ischemia
Maintain the spinal stability
-- elimination of dynamic factor ( microtrauma )
Correction of instabililty, deformity
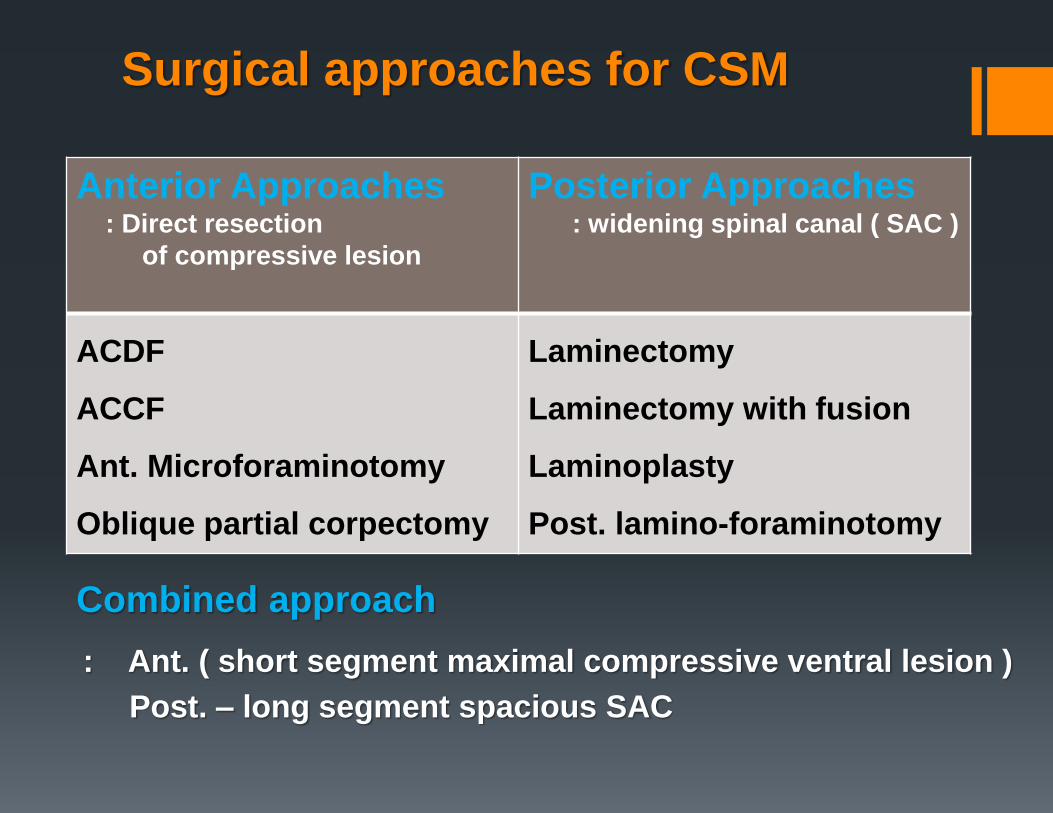
Surgical approaches for CSM
Anterior Approaches : Direct resection
of compressive lesion
Posterior Approaches : widening spinal canal ( SAC )
ACDF
ACCF
Ant. Microforaminotomy
Oblique partial corpectomy
Laminectomy
Laminectomy with fusion
Laminoplasty
Post. lamino-foraminotomy
Combined approach
: Ant. ( short segment maximal compressive ventral lesion )
Post. – long segment spacious SAC
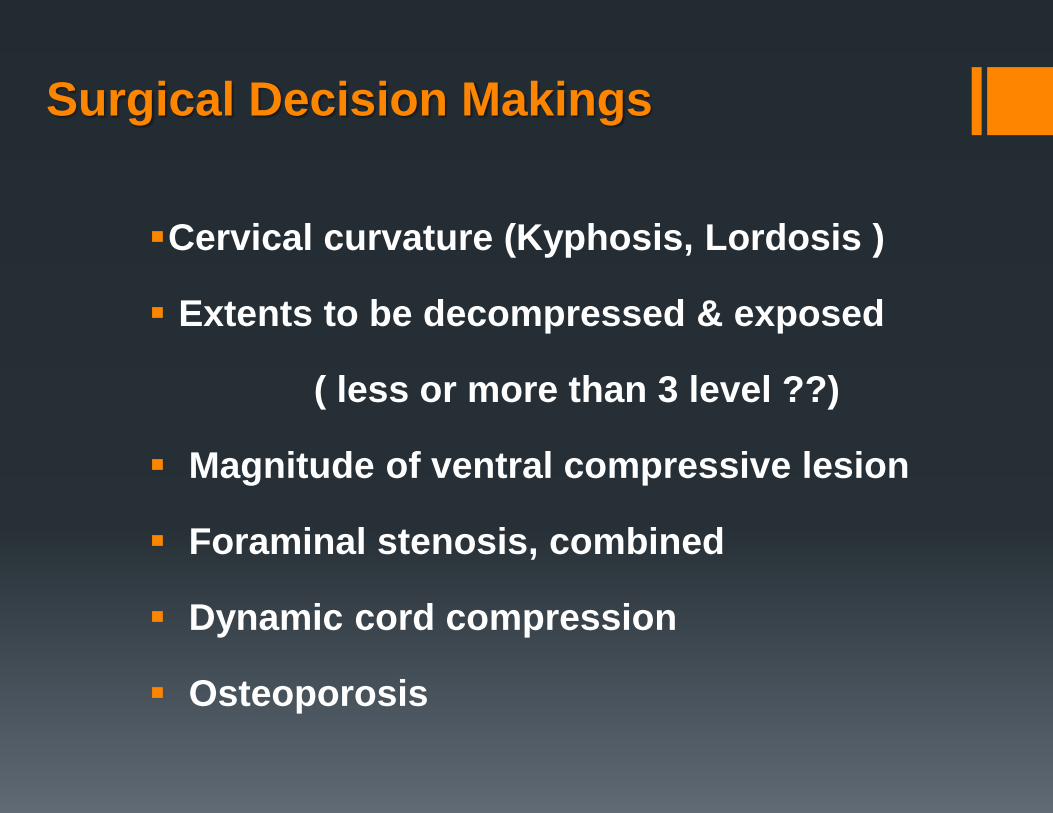
Surgical Decision Makings
Cervical curvature (Kyphosis, Lordosis )
Extents to be decompressed & exposed
( less or more than 3 level ??)
Magnitude of ventral compressive lesion
Foraminal stenosis, combined
Dynamic cord compression
Osteoporosis
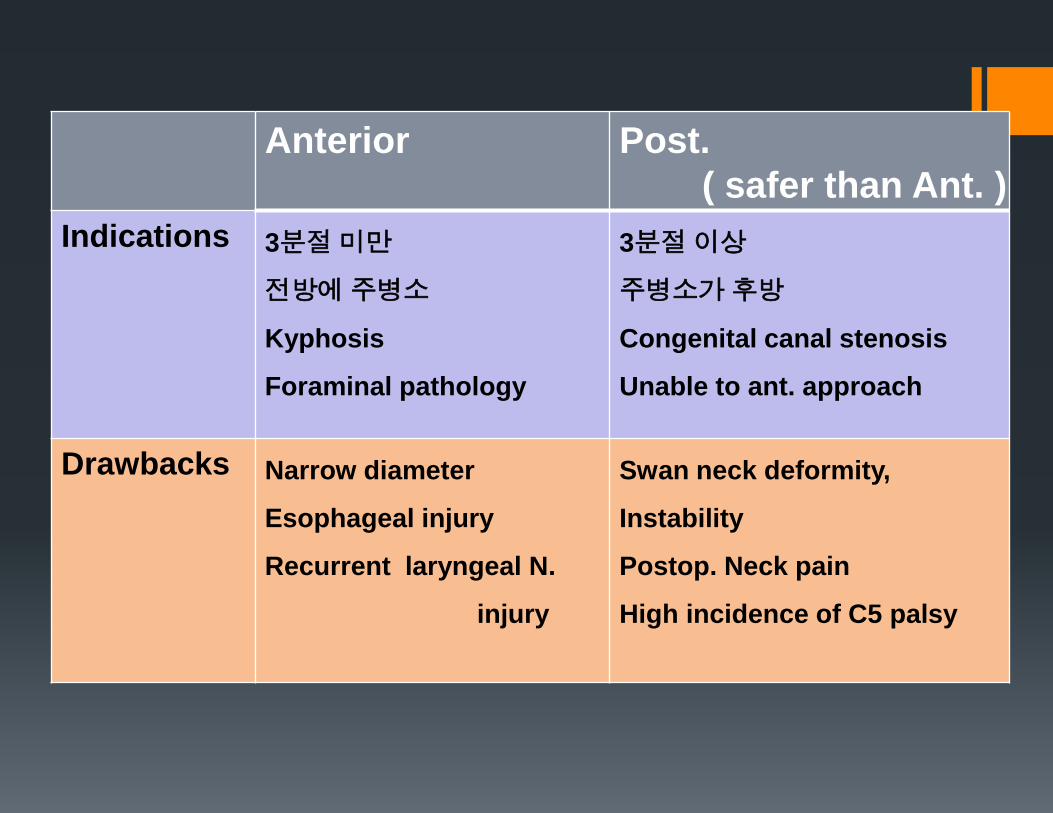
Anterior Post.
( safer than Ant. )
Indications 3분절 미만
전방에 주병소
Kyphosis
Foraminal pathology
3분절 이상
주병소가 후방
Congenital canal stenosis
Unable to ant. approach
Drawbacks Narrow diameter
Esophageal injury
Recurrent laryngeal N.
injury
Swan neck deformity,
Instability
Postop. Neck pain
High incidence of C5 palsy
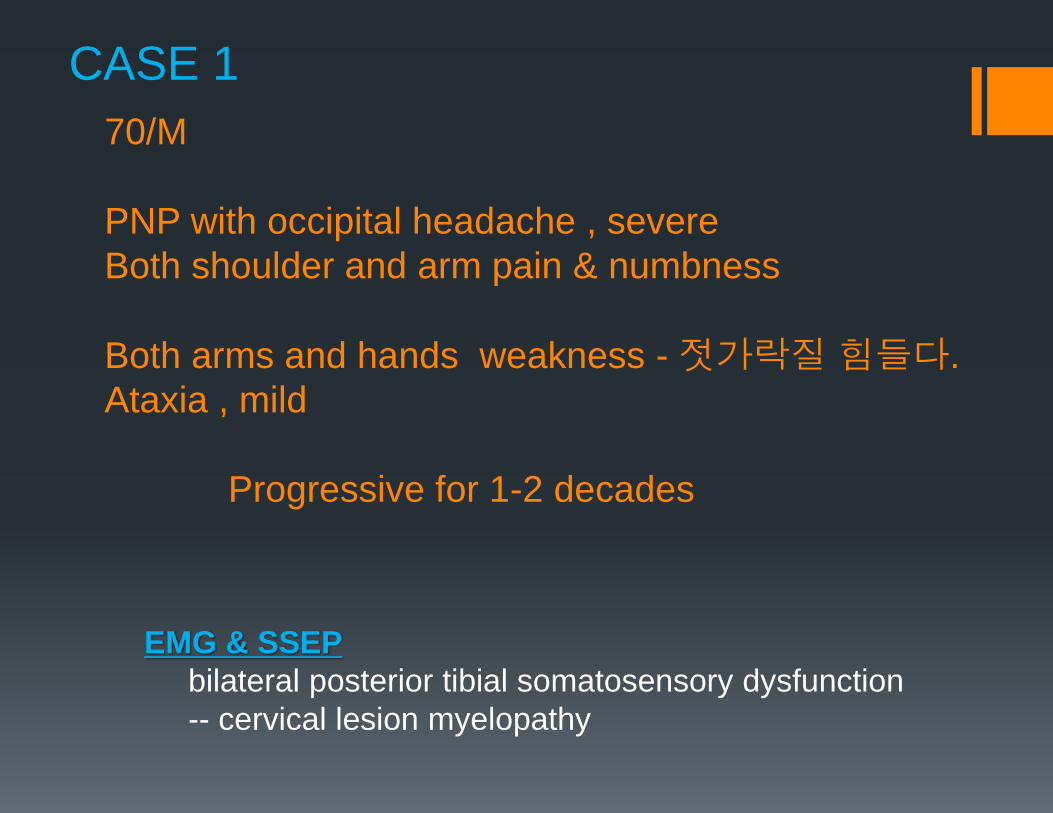
70/M
PNP with occipital headache , severe
Both shoulder and arm pain & numbness
Both arms and hands weakness - 젓가락질 힘들다.
Ataxia , mild
Progressive for 1-2 decades
EMG & SSEP
bilateral posterior tibial somatosensory dysfunction
-- cervical lesion myelopathy
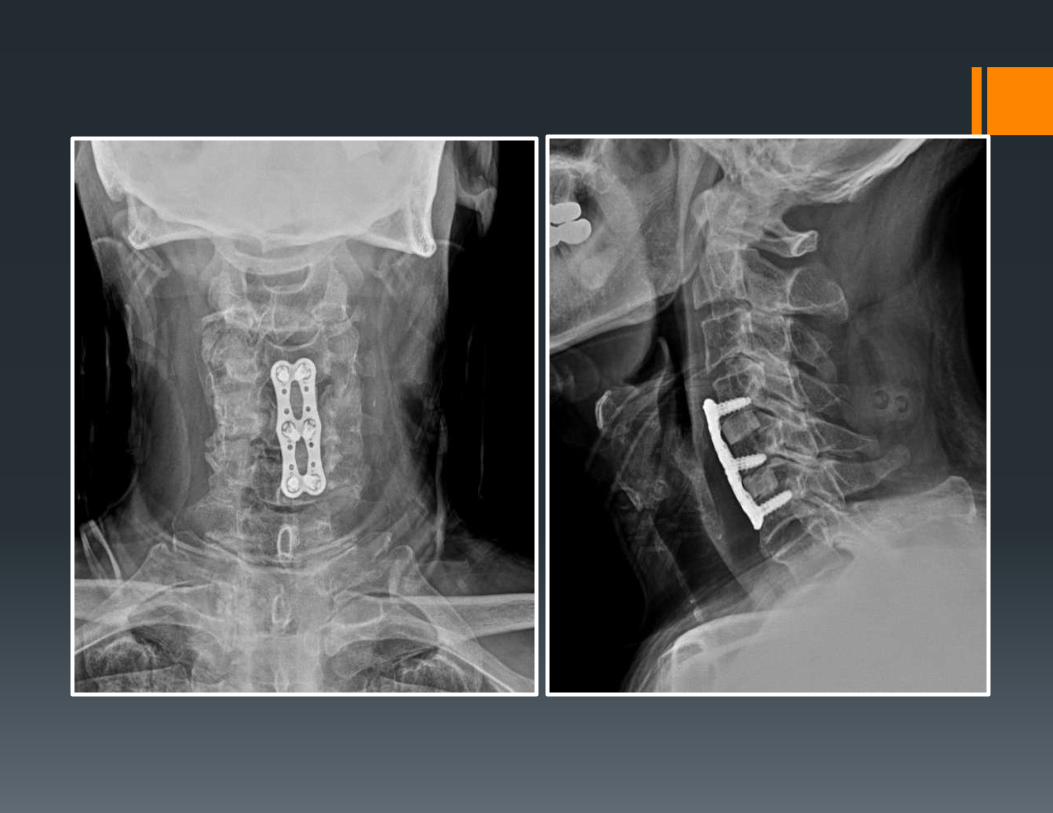
CASE 1
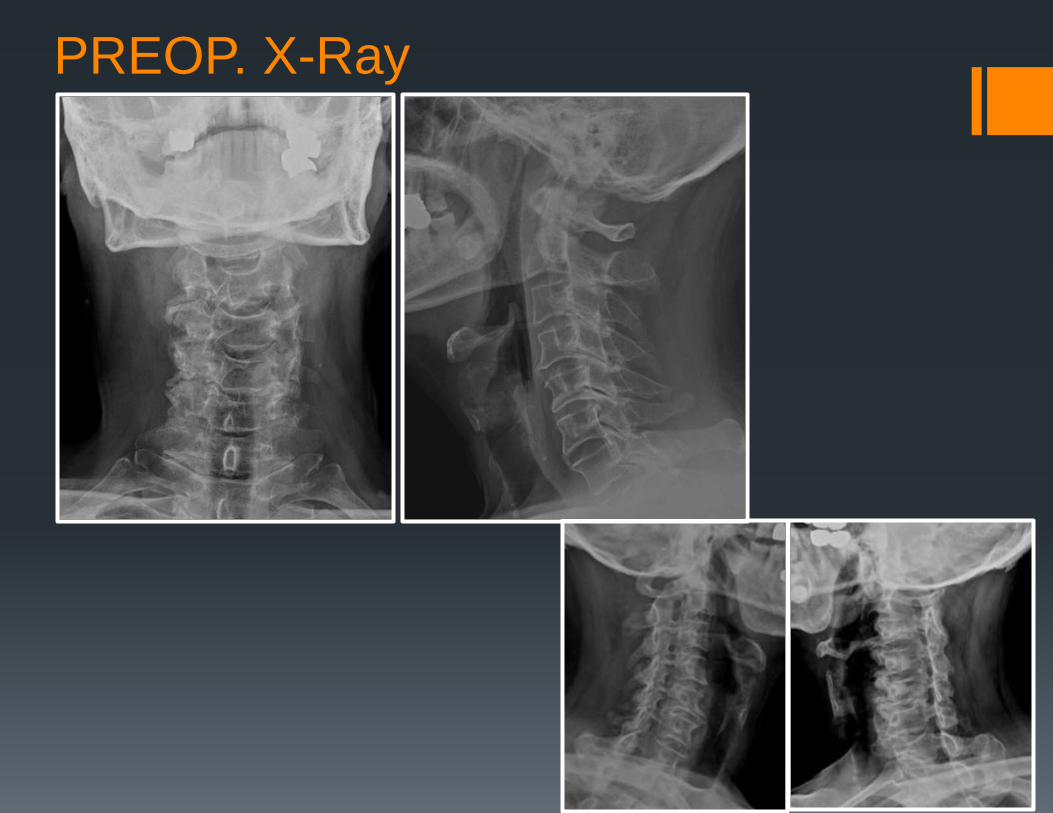
PREOP. X-Ray
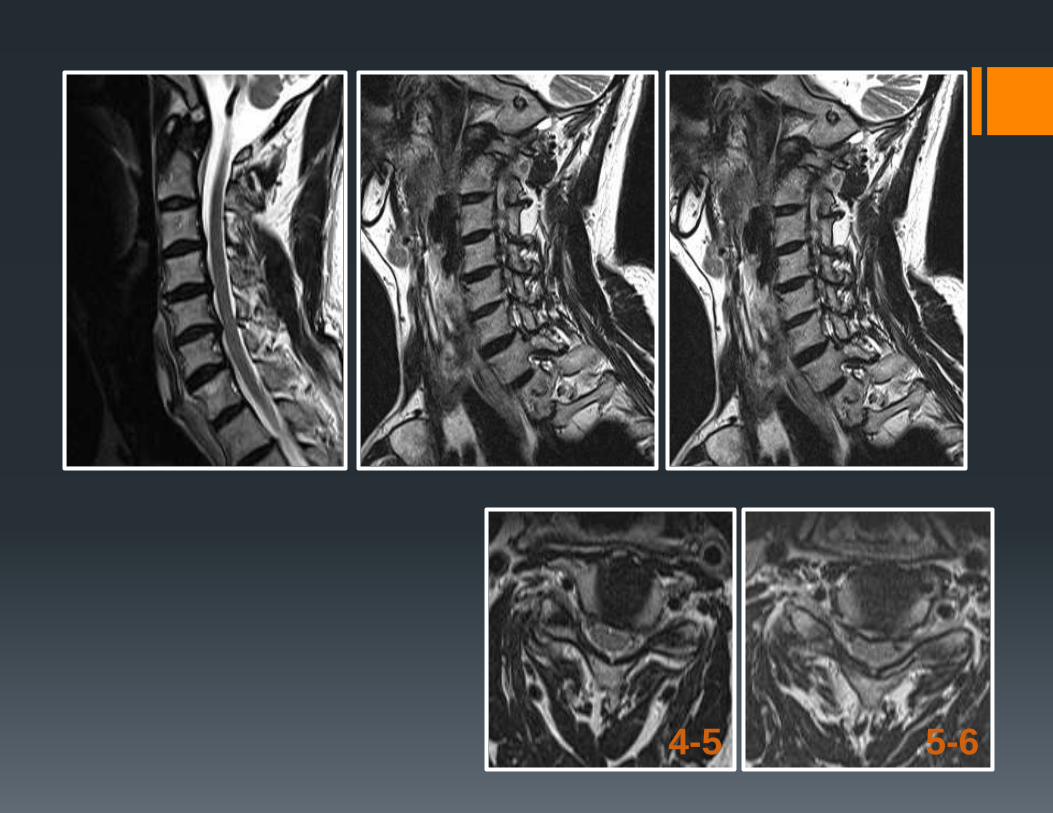
4-5 5-6
1) Ant. cervical discectomy with fusion (ACDF)
2) Ant. cervical corpectomy with fusion (ACCF)
3) Post. lamino-foraminotomy
4) Post. laminectomy with fusion
5) Laminoplasty
CASE 1
가장 적절한 수술법은 ?
47/M
Quadriparesis
Both extremities tingling sensation
after head trauma
DTR : increased
Hoffman , Babiski sign : positive
EMG/SSEP
: Both median somatosensory pathway
abnormality maybe due to CSM
CASE 2
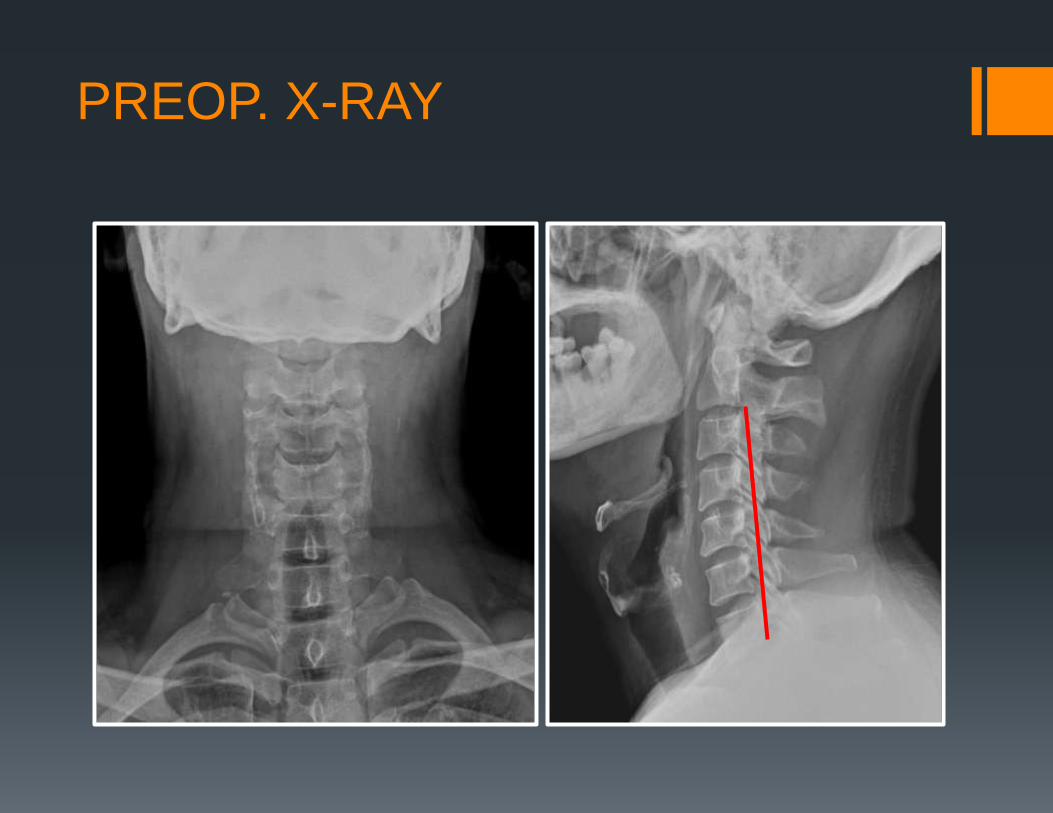
PREOP. X-RAY
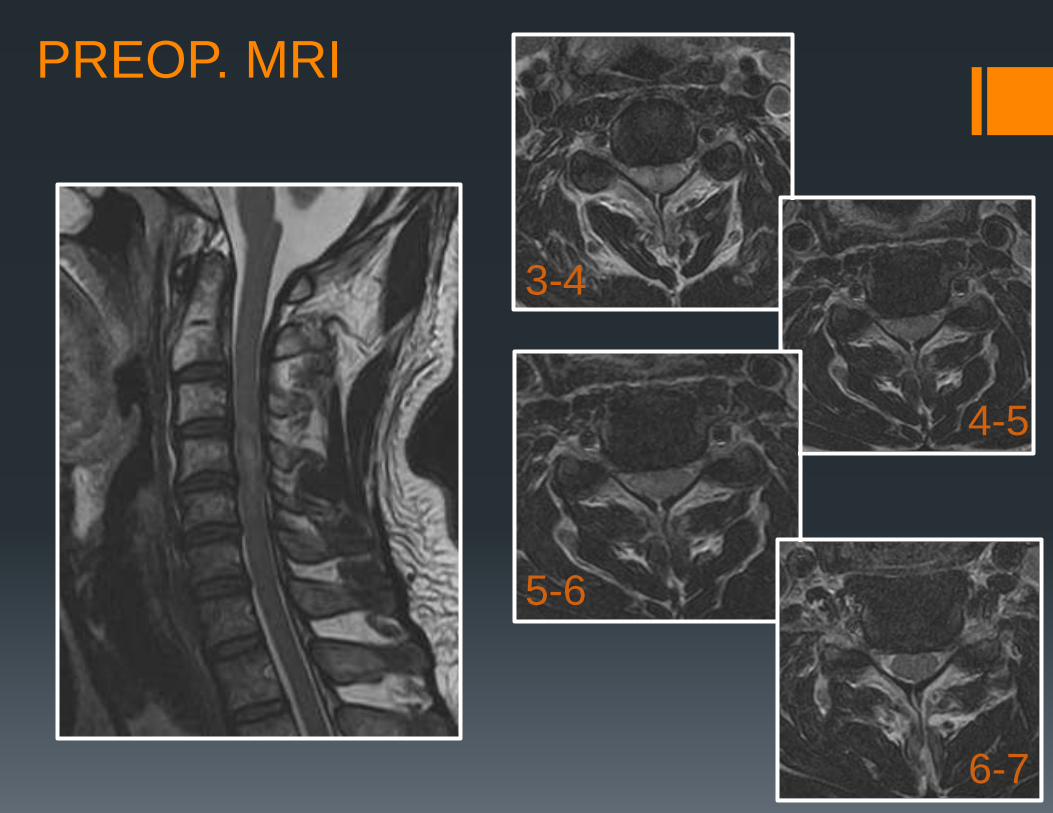
PREOP. MRI
3-4
5-6
4-5
6-7
1) Ant. cervical discectomy with fusion (ACDF)
2) Ant. cervical corpectomy with fusion (ACCF)
3) Post. laminoforaminotomy
4) Post. laminectomy with fusion
5) Laminoplasty
CASE 2 가장 적절한 수술법으로 고려될 방법은 ?
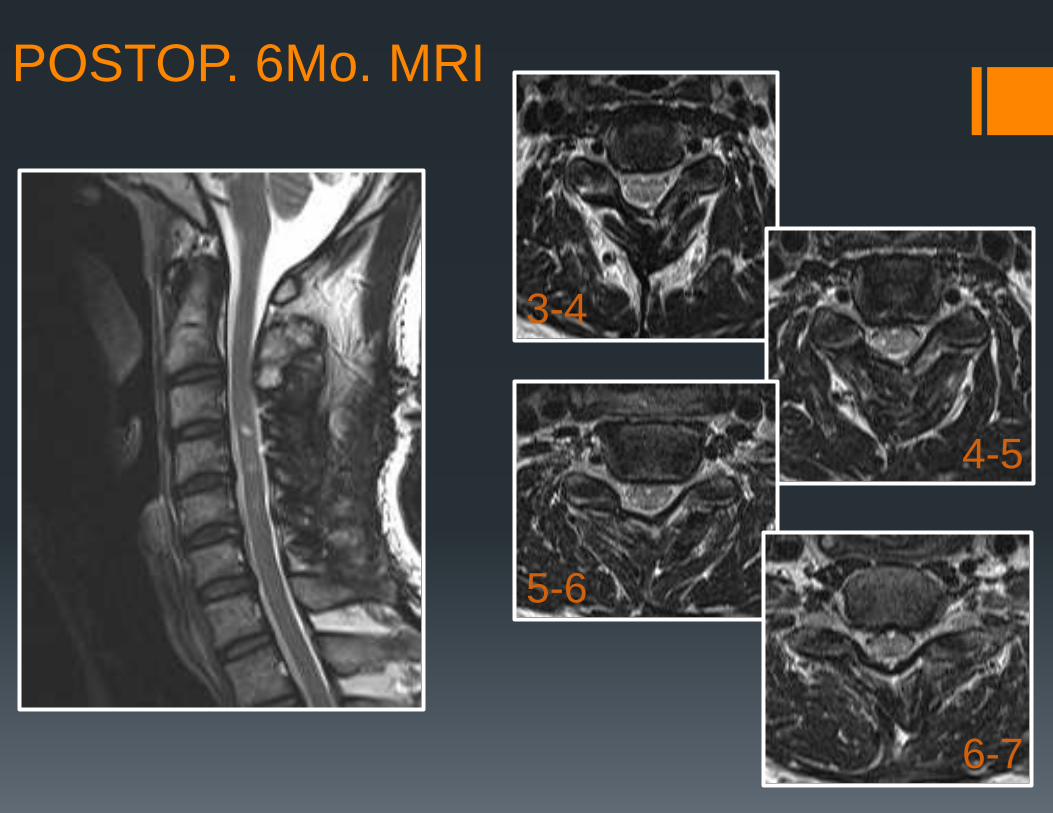
POSTOP. 6Mo. MRI
3-4
6-7
5-6
4-5
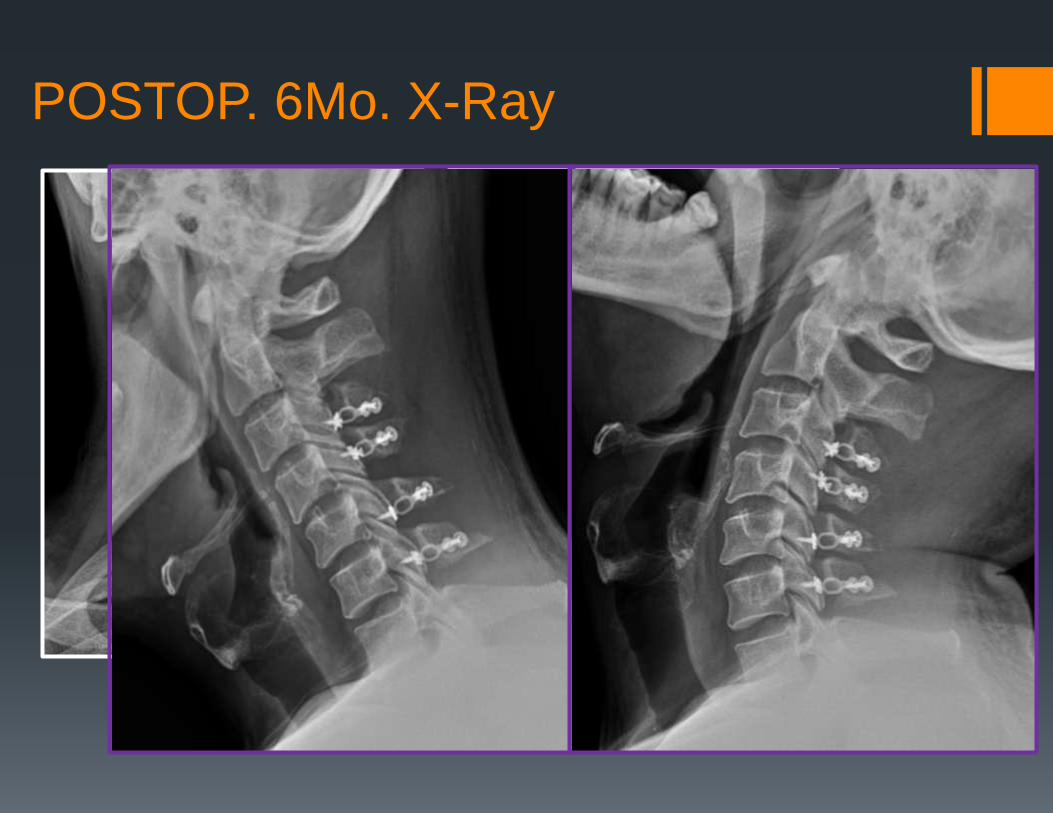
POSTOP. 6Mo. X-Ray
66/M
Both legs weakness, grade 3
Ataxia, severe
after slip down ( slowly progression )
LBP , BOTH LEGS PAIN , NUMBNESS
FOR 6-7 YRS
CASE 3
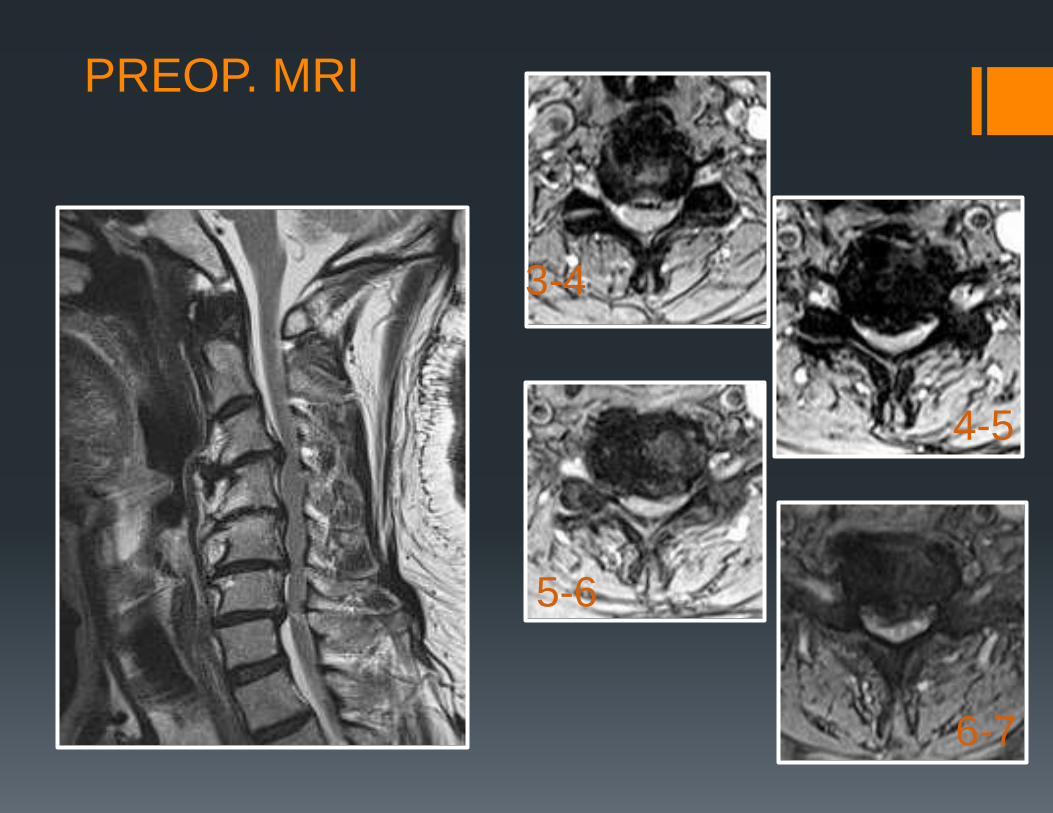
PREOP. MRI
3-4
5-6
4-5
6-7
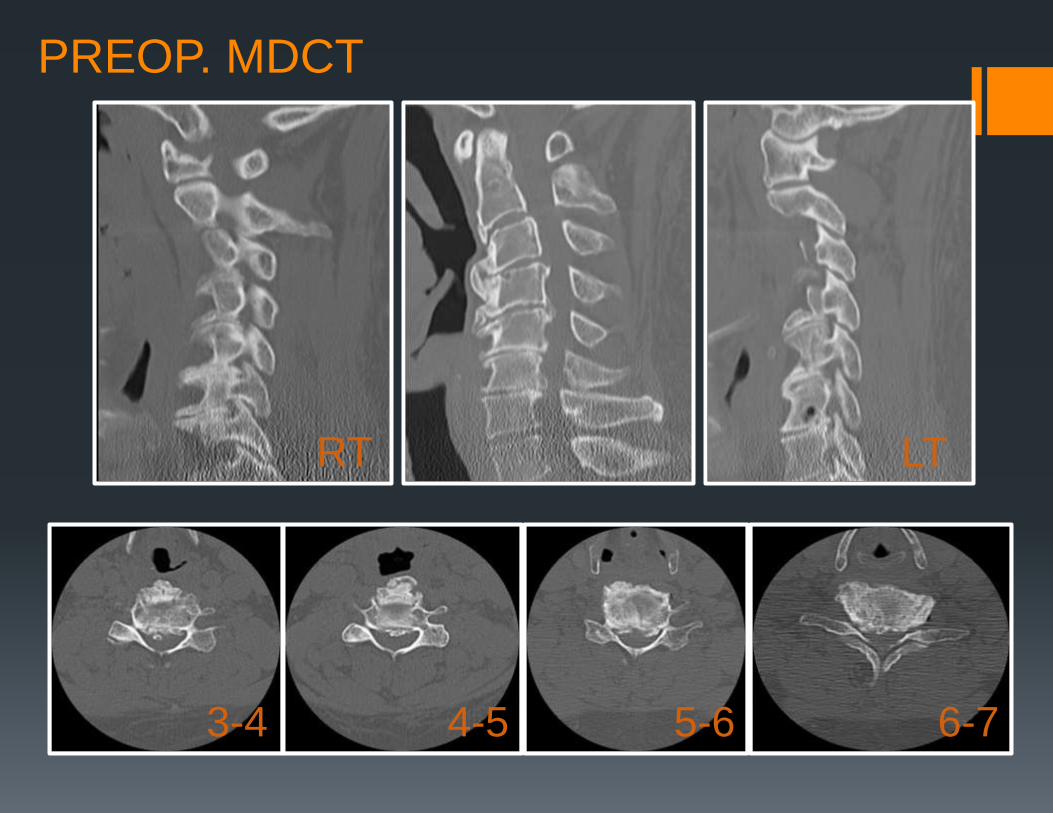
PREOP. MDCT
3-4 4-5 5-6 6-7
RT LT


L-MRI
1) Ant. Discectomy with Fusion , multilevel (ACDF)
2) Ant. Corpectomy with Fusion (ACCF)
3) Post. Laminectomy with Fusion
4) Expansive Laminoplasty
5) Lumbar decompression with Fusion
Case 3 이 환자에 있어 가장 적절한 수술적 접근법은 무엇이라고 생각하십니까?
68/M
Unsteady gait & Left hemiparesis grade 3,
progressive for several yrs Bilateral arms and hands numbness and paresthesia
P/Hx : HBP ,
Both ICA wall arteriosclerosis – ASA, CLOPD
EMG/SSEP :
Rt cerviacal radiculopathy C5 -- chronic
bilateral posterior tibial SEP dysfunction -- cervical myelopathy
CASE 4
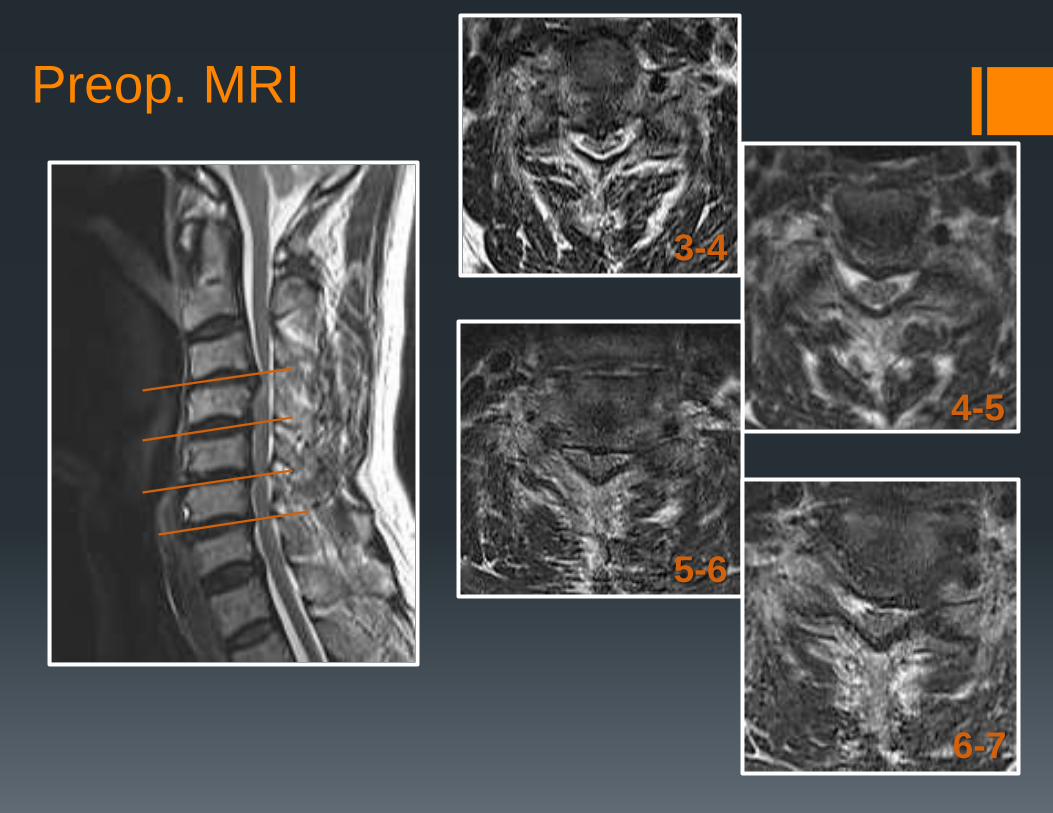
Preop. MRI
3-4
5-6
4-5
6-7
1) Ant. Discectomy with fusion (ACDF)
2) Ant. Corpectomy with fusion (ACCF)
3) Post. Laminectomy with fusion
4) Laminoplasty
5) Post. Laminoforaminotomy
CASE 4-1
환자의 임상 증상 및 증후, 방사선 소견 으로 보아 적절한 수술법은 ?

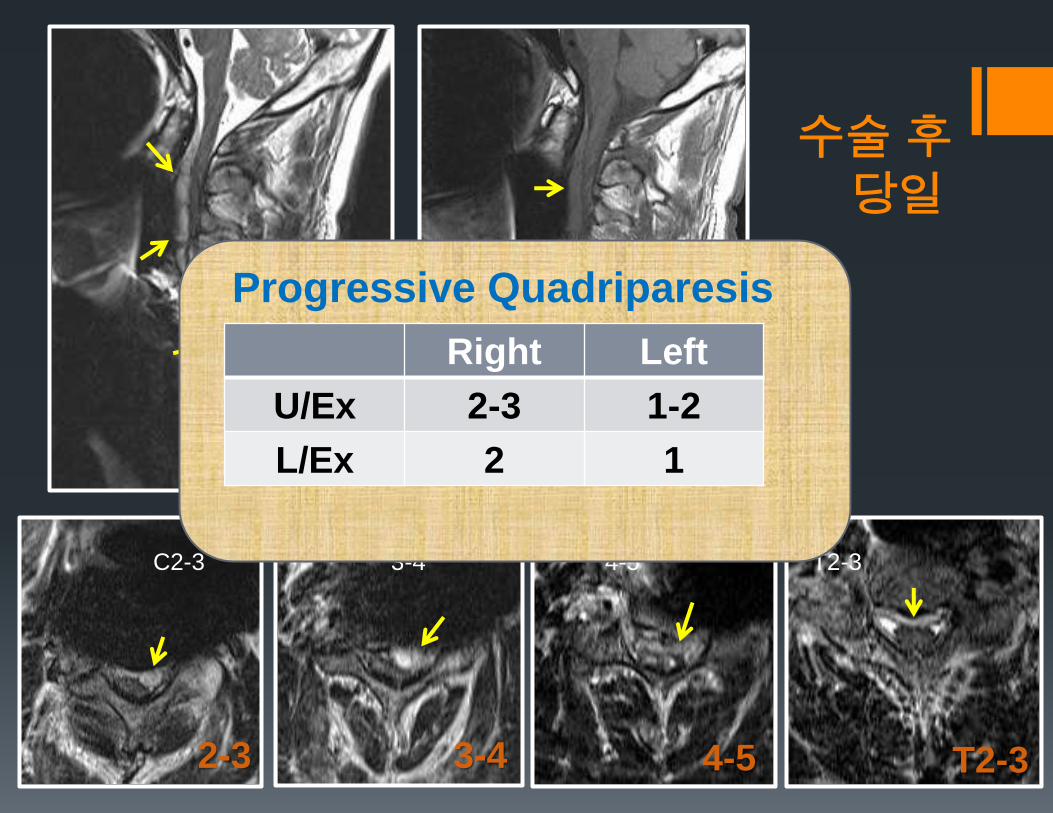
수술 후
당일
C2-3 3-4 4-5 T2-3
T2-3 4-5 3-4 2-3
Progressive Quadriparesis
within 1-2hous postop.
Right Left
U/Ex 2-3 1-2
L/Ex 2 1
1) Ant. Revision with hematoma removal
2) Extended ant. Decompression with hematoma removal
3) Laminectomy with fusion, limited to upper cervical
4) Laminectomy with fusion from upper cervical to upper
thoracic
5) Combined Ant. and Post. approach with hematoma removal
CASE 4-2
상부 경추부터 상부 흉추까지 광범위하고
상부 경추강 전방애 심한 혈종 및 경수 압박이 있는
이러한 경우 수술적 접근법은 ?
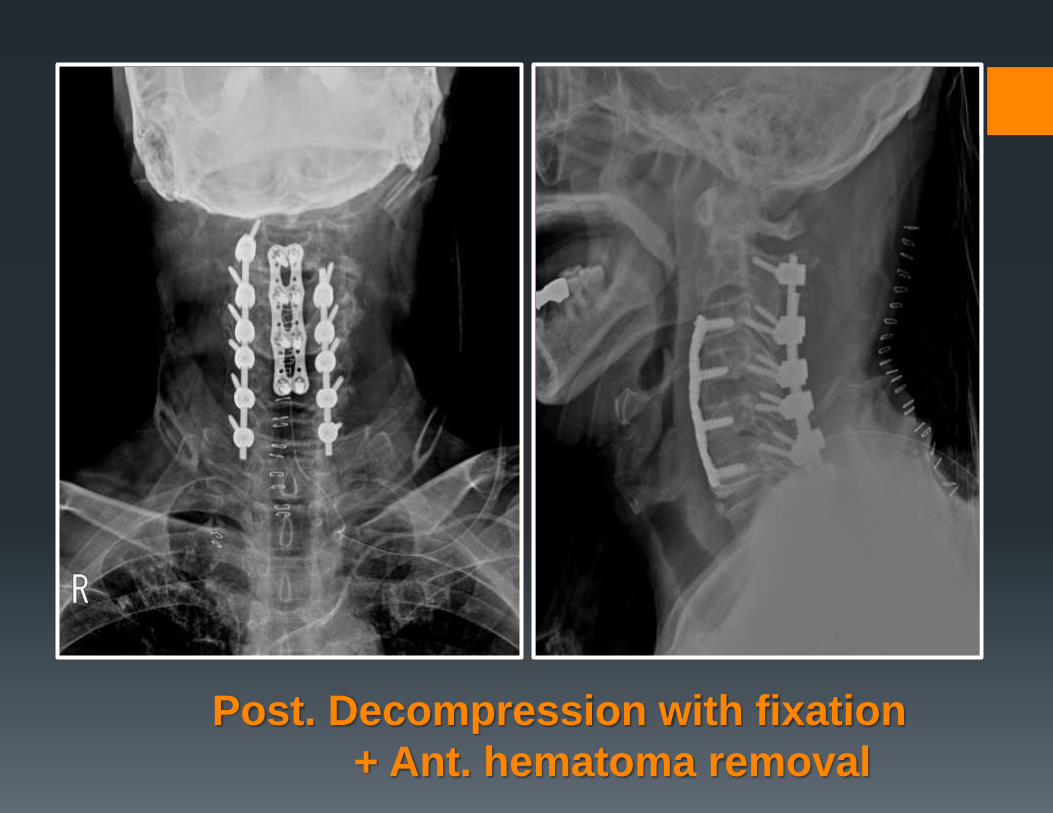
Post. Decompression with fixation
+ Ant. hematoma removal
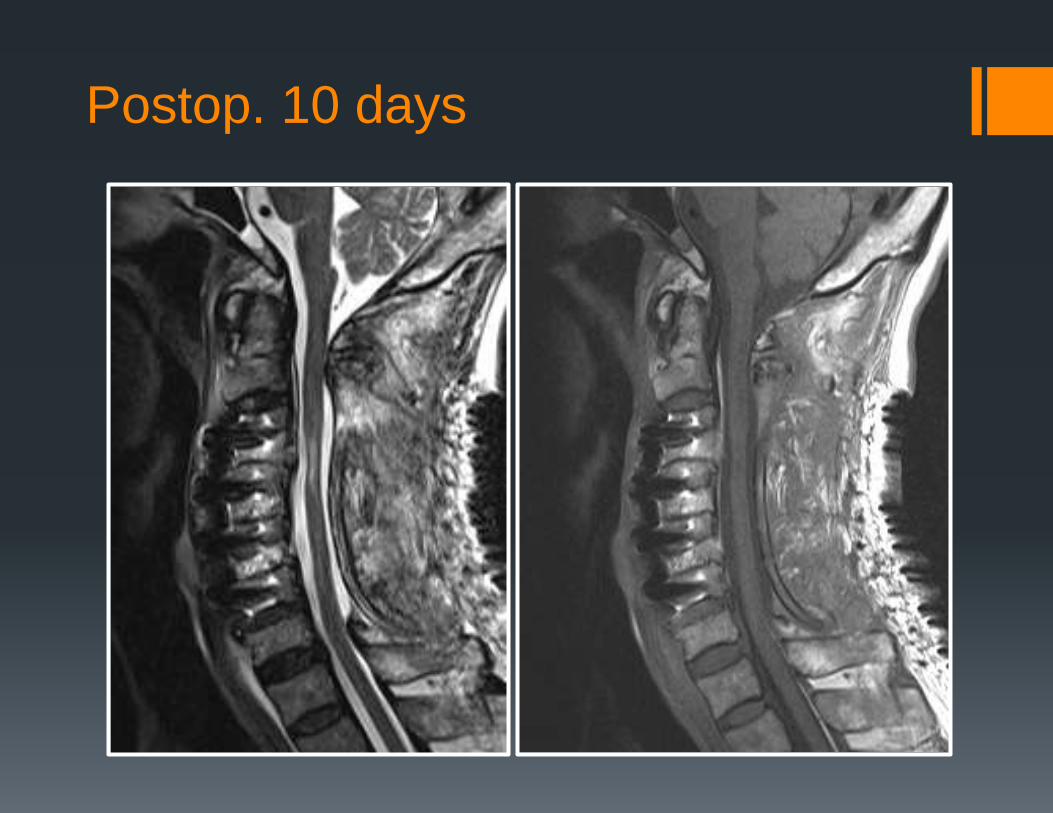
Postop. 10 days
Surgical Decision Makings For CSM
Cervical Alignment (Kyphosis, Lordosis )
Extents to be decompressed & exposed
Magnitude of ventral compressive lesion
CASE BY CASE !!!