Embed Size (px)
Citation preview

病例讨论及习题Chapter(1) Drug-Receptor InteractionsObjectives
Understand the molecular bas is for drug-receptor interact ions and the ir
subsequent ce l lu lar ef fects.
Case 1In tent on enjoy ing h is newly found ret i rement, Mr. B. has made a point of p lay ing
tennis as of ten as possible dur ing the past year . For the past 3 months, however , he
has noted increasing fat igue. Moreover, he is now unable to f in ish a meal despi te
be ing an av id l i fe long eater. Worr ied and wonder ing what these nonspeci f ic
symptoms mean, Mr. B. schedules an appointment wi th h is doctor . On phys ical
examinat ion, the physic ian notes that Mr. B. has an enlarged sp leen, extending
approximate ly 10 cm below the le f t costal margin; the phys ical examinat ion is
otherwise within normal l imi ts . Blood tests show an increased to ta l whi te b lood cel l
count (70,000 ce l ls/mm 3 ) , w i th an absolute increase in neutrophi ls , band forms,
metamyelocytes, and myelocytes, but no blast ce l ls (undi f ferent iated precursor
ce l ls) . Cytogenet ic analys is o f metaphase cel ls demonstrates that 90% of Mr. B. 's
myeloid cel ls possess the Phi ladelph ia chromosome ( ind icat ing a t rans locat ion
between chromosomes 9 and 22) , conf i rming the diagnosis o f chronic myelo id
leukemia. The physic ian in i t ia tes therapy with imat in ib .
Questions1. How does the BCR-Abl receptor tyrosine kinase affect intracellular s ignal ing
pathways?
A. This k inase phosphory la tes steroid hormones, caus ing them to upregulate growth
t ranscr ip t ional regulators of ce l l growth.
1
B. This k inase phosphory la tes the tyros ine residue on the cytop lasmic tai l of the
receptor and opens p lasma membrane channels to a l low the entry of growth
regulators.
C. This k inase removes phosphate groups f rom G prote in receptors, a l lowing the
adenyly l cyclase signal ing pathway to become act ivated.
D. This k inase removes phosphate groups f rom DNA, a l lowing t ranscr ip t ional
regulators access to speci f ic genes.
E. This k inase phosphory la tes cytosol ic prote ins, leading to dysregulated cel l
growth.
Hide Answer
Normally, the receptor tyrosine kinases phosphorylate tyrosine
residues on the cytoplasmic tai l of the receptor, as well as on cytosolic
signal ing molecules. The mutant Phi ladelphia chromosome codes for a
consti tutively active receptor tyrosine kinase protein, BCR-Abl . and
chronic myeloid leukemia. This mutat ion is an example of a “gain-of-
function” mutation, which al lows l igand-independent activi ty and, in this
case, uncontrol led cell growth.
2. How does imatinib interrupt the activi ty of the BCR-Abl protein?
A. Imat in ib reverses the Phi ladelphia chromosomal mutat ion.
B. Imat in ib prevents t ranscr ip t ion of the Phi ladelph ia chromosome.
C. Imat in ib b inds to the ATP-binding s i te o f the BCR-Abl tyrosine kinase, denatures
the prote in , and destroys the kinase receptor.
D. Imat in ib b inds to the p lasma membrane and prevents the BCR-Abl access to i ts
target bind ing si te .
E. Imat in ib inh ib i ts the abi l i ty o f BCR-Abl to phosphorylate subst rates.
Hide Answer
. I t b inds to the ATP-binding site of the BCR-Abl tyrosine kinase and
causes the protein to assume an enzymatical ly inact ive conformation,
which inhibi ts i ts kinase activi ty . This l imits the intracellular s ignals for
myeloid cel l growth.
2
Over the next month, the cel ls conta in ing the Phi ladelph ia chromosome d isappear
completely f rom Mr. B. 's blood, and he begins to fee l wel l enough to compete in a
seniors ' tennis tournament . Mr . B. cont inues to take imat inib every day, and he has
a completely normal b lood count and no fee l ings of fat igue. He is not sure what the
fu ture wi l l br ing, but he is g lad to have been g iven the chance to en joy a heal thy
re t i rement.
3. Unl ike imatinib, most of the older therapies for chronic myeloid leukemia
(e.g. , interferon-α) had signif icant “f lu- l ike” adverse effects. Why did these
older therapies cause signif icant adverse effects in most patients, whereas (as
in this case) imatinib causes adverse effects in very few patients?
A. Older therapies target al l myeloid ce l ls .
B. Older therapies target the BCR-Abl prote in k inase in normal ly funct ion ing ce l ls.
C. Older therapies target BCR-Abl product ion in a l l hematopoiet ic ce l ls .
D. Older therapies target the Phi ladelphia chromosome throughout the body.
E. Older therapies target al l fu ture product ion of BCR-Abl prote in k inase.
Hide Answer
and have effects on diverse cel l processes. This leads to signif icant
toxic adverse effects in many cel ls or t issues, which are affected by the
chemotherapeutic drug's mechanism of action.
4. Why is imatinib a specif ic therapy for chronic myeloid leukemia?
A. Imat in ib select ive ly b inds the BCR-Abl prote in of the tyrosine kinase receptor in
abnormal ly growing hematopoiet ic ce l ls.
B. Imat in ib select ive ly degrades the Phi ladelph ia chromosome in leukemic ce l ls.
C. Imat in ib select ive ly targets the tyrosine k inase–associated receptors.
D. Imat in ib select ive ly b inds to phosphatases, which phosphory la te tyrosine.
E. Imat in ib select ive ly targets BCR-Abl synthesis in hematopoiet ic precursor cel ls .
Hide Answer
I t is a chemotherapeutic agent, whose act ion is restricted to a specif ic
cell -type distr ibut ion of a receptor. This accounts for i ts specif ici ty and
the low incidence of adverse effects in pat ients treated with imatinib. In
contrast to receptor tyrosine kinases, tyrosine kinase=nassociated
3
receptors do not have innate enzymatic activi ty , but rather, induce other
cytosol ic proteins to phosphorylate tyrosine residues.
5. When a drug interacts with i ts receptor, the magnitude of the cellular
response may be greater than the magnitude of the immediate effect of the
molecular drug-receptor interact ion. This is referred to as:
A. tachyphylaxis
B. receptor recru i tment
C. s ignal ampl i f icat ion
D. second messenger act ivat ion
E. hetero logous desensi t izat ion
Hide Answer
refers to the abil i ty of a cell to ampl ify the effects of receptor binding.
For example, when a l igand binds to a G protein=ncoupled receptor, the
G protein molecule can bind to and act ivate many effector molecules,
ampl ifying the cellular second messenger response to the l igand
binding. Tachyphylaxis occurs when drugs have diminishing effects over
t ime. The desensit ization of the receptor and the cel l can be
homologous (only one type of receptor shows a diminished response to
the agonist) , or heterologous ( two or more types of receptors show a
coordinately diminished response).
Case 2A 62-year-o ld man is rushed to the hospi tal a f ter ingest ing a conta iner o f an
organophosphate insect ic ide in a su ic ide at tempt . On arr iva l in the emergency
depar tment, care providers note a s trange odor emanat ing f rom the pat ient . The
pat ient is unresponsive, and h is phys ical examinat ion is remarkable for profuse
sweat ing, miot ic pupi ls , and copious oral and bronchia l secret ions. He is noted to
have di f fuse muscle fasc iculat ions, but is f laccid and paralyzed. When the pat ient is
in tubated, the physic ian notes copious amounts of st range-smel l ing watery
secret ions. The doctor subsequent ly develops tear ing and bronchospasm. The
4
pat ient 's soaking clothes are removed and safe ly d isposed of . The nurses a lso
subsequent ly develop tear ing and runny noses.
Questions1. This patient 's signs are consistent with excessive acetylcholine activi ty at
both muscarinic and nicot inic receptors. Organophosphate insect icides cause
toxici ty by prevent ing the normal metabolism of acetylcholine. The most l ikely
binding si te of the organophosphate resides on:
A. a cel l sur face adhesion receptor
B. an ext racel lu lar enzyme
C. a tyros ine k inase receptor
D. a t ranscr ipt ion regulator
E. an in t racel lu lar s ignal t ransduct ion enzyme
Hide Answer
The binding site of organophosphate insecticides is an ,
acetylcholinesterase. These chemicals bind to the active site of
acetylcholinesterase and form an oxygen=nphosphorus bond in the
enzyme complex, which prevents the degradat ion of acetylcholine within
the synaptic clef t . Because organophosphates nonselect ively bind to
acetylcholinesterase at both nicot inic and muscarinic sites, they can
cause enhanced cholinergic neurotransmission at both of these
chol inergic synapses. This results in a depolar iz ing neuromuscular
blockade, as well as muscarinic symptoms of profuse sweating, miot ic
pupi ls , and copious oral and bronchial secretions. Cel l surface adhesion
receptors mediate cell to cell interactions and communication.
2. Based on their effect at chol inergic synapses, organophosphate insect icides
would be considered:
A. noncompet i t ive, reversible antagonis ts
B. compet i t ive, reversible antagonis ts
C. inverse agonis ts
5
D. d i rect agonists
E. ind irect agonists
Hide Answer
Organophosphate insect icides would be considered at chol inergic
synapses. They do not bind directly to the acetylchol ine receptor as
direct agonists, but increase the concentration of acetylchol ine within
the synapse. In this way, they facil i tate the agonist effect of
acetylcholine at i ts receptor, where acetylchol ine binds and induces a
conformational change in the receptor-associated ion channel to
increase membrane permeabi l i ty for cat ions. Inverse agonists cause
consti tutively active receptor targets to adopt an inactive receptor
conformation. Antagonists inhibit the abi l i ty of receptor targets to be
activated by endogenous agonists.
3. The oxygen–phosphorus bond formed between organophosphate insect icides
and acetylcholinesterase is subject to a process of “aging,” in which the bond
results in permanent destruction of acetylchol inesterase funct ion. The “aged”
oxygen–phosphorus bond is:
A. an ion ic bond
B. a hydrophobic in teract ion
C. a group of van der Waals in teract ion
D. covalent bond
E. hydrogen bond
Hide Answer
The “aged” oxygen=nphosphorus bond is a that is essent ial ly
irreversible. The affected enzyme is destroyed, and subsequent
acetylcholinesterase funct ion is dependent on the regeneration of new
enzyme. The ant idote to organophosphate poisoning, pral idoxime,
reverses the oxygen=nphosphorus bond but must be administered
before aging occurs and the bond becomes covalent . An ionic bond
occurs between atoms with opposite charges. Van der Waals forces
6
result f rom the induced polar ity on molecules as a result of shif t ing
electron density, and create a weak attract ive force between chemicals
and their receptors. Hydrogen bonding is mediated by the interact ion
between posit ively and negat ively polarized atoms.
4. Normally, acetylchol ine acts at i ts nicot inic receptor at the neuromuscular
junction to effect muscle cell depolar izat ion and contraction. The nicotinic
acetylcholine receptor is an example of:
A. a l igand-gated ion channel
B. a vol tage-gated ion channel
C. a l igand-gated G protein–coupled receptor
D. a l igand-gated tyrosine k inase receptor
E. a vol tage-gated ext racel lu lar enzyme
Hide Answer
The nicot inic acetylchol ine receptor is an example of When two
acetylcholine molecules bind to the postsynaptic receptor, a
conformational change in the transmembrane channel occurs, al lowing
ion conductance through the channel. Voltage-gated ion channels
change their state and conformation based on changes in the cel l
membrane potent ial .
5. G protein–coupled receptors are composed of extracel lular domains,
transmembrane regions, and intracellular regions. Which of the fol lowing
statements regarding G protein–coupled receptors is correct?
A. The extracel lu lar domain consis ts o f enzyme si tes, which hydrolyze guanosine
tr iphosphate to guanosine d iphosphate af ter binding of the l igand.
B. The in tracel lu lar reg ion is l inked to a G protein, which af fects s ignal ing molecules
af ter b inding of the l igand.
C. The t ransmembrane reg ion consists of f ive subunits, which release the G protein
af ter b inding of the l igand.
D. When the t ransmembrane region opens, i t a l lows ions to pass through i t .
E. The G protein–coupled receptors are speci f ic to acety lchol ine receptors.
7
Hide Answer
to the extracellular domain of the receptor. The G protein di ffuses away
from the intracel lular domain of the receptor to act on a number of
ef fector molecules, including adenylyl cyclase, phospholipase C, and
ion channels. Signals mediated by G proteins are usually terminated by
the hydrolysis of GTP to GDP. The transmembrane region consists of a
single polypeptide chain, which traverses the membrane seven t imes,
connect ing the extracellular l igand-binding si te with the intracellular G
protein l inkage. I t is not an ion channel. The G protein=ncoupled
receptors are the most abundant class of receptors in the human body.
Chapter(2)Pharmacodynamics
Objectives Understand the molecular bas is for drug-receptor b inding and i ts impact on
drug dose–response relat ionships, and the therapeut ic index of a drug.
Understand the act ions of agonists and var ious antagonist c lasses, and the ir
re la t ionships to drug potency and ef f icacy.
Case 1Admira l X. is a 66-year-o ld re t i red submarine capta in wi th a 70 pack-year smoking
history ( two packs a day for 35 years) and a fami ly h is tory of coronary ar tery
disease. Al though he usual ly ignores the adv ice of h is phys ic ians, he does take the
pravastat in prescr ibed to reduce his cholestero l level and aspi r in to reduce h is r isk
of coronary artery occlusion.
One day, whi le work ing in his woodshop, Admiral X. begins to fee l t ightness in his
chest. The feel ing becomes rap id ly pa infu l , and the pain begins to rad iate down h is
le f t arm. He ca l ls 911, and an ambulance transports him to the loca l emergency
depar tment. Af ter evaluat ion, i t is determined that Admira l X. is having an anter ior
8
myocard ia l in farc t ion. Because the hospi tal has no cardiac catheter izat ion
laboratory and Adm. X has no speci f ic contraind icat ions to thrombolyt ic therapy
(e.g. , uncontro l led hypertension, h is tory of st roke, or recent surgery) , the phys ic ian
in i t ia tes therapy with both a thromboly t ic agent, t issue-type plasminogen act ivator
( t -PA) , and an ant icoagulant , hepar in . Improper dosing of both of these drugs can
have di re consequences (hemorrhage and death) because of the ir low therapeut ic
indices, so Admiral X. is c losely moni tored, and the pharmacologic e f fect o f the
hepar in is measured per iod ica l ly by test ing the part ia l thromboplast in t ime (PTT).
Admira l X. 's symptoms resolve over the next several hours, a l though he remains in
the hospi ta l for monitor ing. He is d ischarged af ter 4 days in the hospi ta l ; h is
discharge medicat ions include pravastat in , aspir in , atenolo l , l is inopr i l , and
clop idogrel for secondary prevent ion of myocardial infarct ion.
Questions1. Which of the fol lowing statements is correct regarding the relat ionship
between the molecular interact ion of a drug with i ts receptor and the potency
of the drug?
A. The greater the number of receptors occupied by a drug, the greater i ts potency.
B. Drugs with h igh potency have a h igh EC 5 0 .
C. Drugs with h igh potency have a drug dose–response curve that l ies to the r ight of
less potent , but s imi lar drugs.
D. The presence of a compet i t ive antagonist shi f ts the agonist dose–response curve
to the r ight and decreases i ts potency.
E. The greater a drug's potency, the higher i ts drug-receptor d issociat ion constant,
K d .
2. Which of the fol lowing statements regarding drug eff icacy is correct?
A. The ef f icacy of a drug is d irect ly proport ional to i ts drug-receptor b inding
dissoc iat ion constant.
B. The maximal ef f icacy of an agonis t is the condi t ion at which receptor-mediated
signal ing by the drug is maximal .
C. H ighly e f f icac ious drugs have h igh ED 5 0 s and low LD 5 0 s.
9
D. H ighly e f f icac ious drugs mediate the ir e f fect at a lower f ract ion of receptor
bind ing.
E. The presence of a compet i t ive antagonist reduces the maximal possible response
to drug-receptor b inding, and hence reduces drug ef f icacy.
3. What properties of certain drugs, such as aspir in, al low them to be taken
without monitoring of plasma drug levels, whereas other drugs, such as
heparin, require such monitor ing?
A. Whereas aspi r in is an ora l agent, hepar in is administered parenteral ly .
B. Aspir in is avai lab le without prescr ip t ion and can be taken safe ly wi thout
moni tor ing.
C. Whereas aspi r in exer ts an i r reversible pharmacologic ef fect , which does not need
moni tor ing, the revers ib le ef fect of hepar in must be monitored.
D. Whereas aspi r in causes a graded dose–response relat ionship, hepar in causes a
quantal dose–response re lat ionship that must be monitored per iod ical ly .
E. Whereas aspi r in has a larger therapeut ic index, hepar in has a smal l therapeut ic
index.
4. Why does the fact that a drug has a low therapeutic index mean that the
physician must use greater care in i ts administration?
A. Drugs with a low therapeut ic index can cause tox ic i ty a t a high ED 5 0 .
B. Drugs with a low therapeut ic index can only cause tox ic i ty over a smal l range of
drug doses.
C. Drugs with a low therapeut ic index can cause i r revers ib le ef fects af ter they are
admin is tered.
D. Drugs with a low therapeut ic index do not have therapeut ic e f fects unt i l the
admin is tered dose approaches the toxic dose.
E. Drugs with a low therapeut ic index have a greater degree of safety when
admin is tered at therapeut ic doses.
5The concept of “spare receptors” refers to:
A. the up-regulat ion of receptors , enhancing the ef fect o f a drug (agonist )
B. the fact that the EC 5 0 is greater than the K d
10
C. a maximal agonis t response occurr ing with less than 100% receptor occupancy
D. the fact that receptors are res is tant to the presence of receptor antagonis ts
E. the f ind ing of enhanced potency despi te the presence of receptor antagonis ts
Case 2Pi t tsburgh, PA; November 1988: A 34-year-old man is dropped of f by a pr ivate car a t
the ambulance entry of an emergency department . He is disheveled and
unresponsive and is rushed by secur i ty guards in to the department . He is quick ly
placed on a card iac moni tor, and in travenous access is estab l ished. His v i ta l s igns
reveal a hear t ra te of 26 bpm and he is apneic . He has no palpable b lood pressure
but has a palpable s low pulse at his femora l artery. Fresh needle t rack marks,
cons is tent wi th recent in ject ions, are present in h is le f t antecubi ta l fossa.
Phys ic ians suspect he is a v ic t im of the current ep idemic of “superpotent ” hero in ,
“China White, ” which is sweeping Al legheny County. Despi te ora l in tubat ion,
mechanica l vent i lat ion, advanced card iac l i fe suppor t measures, and large
in travenous doses of an ant idote, the pat ient dies.
Questions1. In 1988, the Pit tsburgh, PA area experienced an epidemic of heroin abusers
dying from accidental overdoses of a short-acting synthet ic opioid agonist , 3-
methyl fentanyl , known on the street as China White. These synthetic
analogues of fentanyl were est imated to have 6000 t imes the potency of
morphine. Pharmaceutical fentanyl has 75 to 100 t imes the potency of
morphine. I f a semilogari thmic dose–response curve of these three opioid
agonists were plotted, which agent would have the smallest EC 5 0 and the left -
most drug dose–response curve?
A. morphine
B. fentanyl
C. 3-methyl fentany l
D. naloxone
E. nal t rexone
11
. Heroin abusers sought out the “superpotent” China White in 1988 for the
experience of the intense rush and the thr i l l of taking a potent drug with l i fe-
threatening effects. Many unsuspecting abusers injected 3-methyl fentanyl
once and suffered cardiorespiratory arrest within minutes. Those who survived
to receive medical care required large doses of naloxone. In many cases,
patients experienced reversal of their opioid agonist effects within minutes of
an ini t ial administration of naloxone but then experienced resedation, requir ing
mult iple repeated doses of naloxone. This effect of naloxone is a characterist ic
of:
A. a revers ib le agonis t drug ef fect
B. a revers ib le compet i t ive antagonis t drug ef fect
C. a noncompet i t ive antagonist drug ef fect
D. a part ia l agonis t drug ef fect
E. an inverse agonis t drug ef fect
. Heroin is usually measured in doses of 25-mg bags. Unsuspect ing users of
China White, who might have achieved a desired “high” with three bags of
heroin, died after in ject ing one bag of 3-methyl fentanyl. I f 50% of China White
users died after in ject ing one bag of 3-methyl fentanyl , which of the fol lowing
statements is correct?
A. Heroin is more potent than 3-methy l fentanyl .
B. The therapeut ic index for 3-methyl fentany l is larger than that for hero in .
C. The ED 5 0 for 3-methyl fentany l is 25 mg.
D. The TD 5 0 for 3-methyl fentany l is 75 mg.
E. The LD 5 0 for 3-methyl fentany l is 25 mg.
4. Based on the above case, which of the fol lowing statements is correct?
A. The therapeut ic index of 3-methy l fentanyl is high.
B. The EC 5 0 o f 3-methy l fentanyl is h igh.
C. The LD 5 0 o f 3-methy l fentanyl is h igh.
D. The af f in i ty o f 3-methyl fentanyl for the µ opio id receptor is high.
E. The K d o f 3-methy l fentanyl is h igh.
12
r
5. Which of the fol lowing is an example of the act ion of a chemical antagonist?
A. Naloxone b inds to the µ opioid receptor and prevents op io id agonis t e f fects .
B. D igox in-speci f ic ant ibodies b ind to digoxin and prevent i ts act ion at the cardiac
sodium-potass ium pump.
C. Fentanyl b inds to the µ opioid receptor and prevents the act ion of morphine.
D. β-Adrenergic receptor antagonis ts b ind to the β1-adrenerg ic receptor and
decrease tachycard ia in the set t ing of hyperthyroidism.
E. Mannitol osmot ical ly draws water in to the renal tubule and prevents i ts
reabsorpt ion.
Chapter(3)Local Anesthetic PharmacologyObjectives
Understand the mechanism of act ion by which loca l anesthet ics d imin ish
sensory, motor, and autonomic impulse t ransmiss ion.
Understand the physiology of pa in t ransmiss ion and how var ious loca l
anesthet ics are administered to reduce pain percept ion.
Recognize categor ies of loca l anesthet ics , thei r pharmacology, therapeut ic
uses, and potent ia l toxic i t ies .
Case 1E.M. is a 24-year-o ld graduate s tudent in organic chemistry. Whi le working in the
lab one evening, he sp i l ls a beaker o f hydrof luor ic ac id (HF) in the fume hood.
Al though he ref lex ively jerks his hand away, some of the l iquid fa l ls on the f ingert ips
of h is le f t hand. Some minutes later , E.M. feels a st inging pain, which increases in
in tensi ty and is fo l lowed by a burn ing, throbbing ache. Real iz ing the corros iveness
of the ac id , E.M. begins r insing h is hand with water and a magnesium sul fate
so lut ion ( the magnesium chelates the toxic f luor ide ions). He also te lephones 911
and is t ranspor ted to the emergency department .
13
The res ident notes that the ac id has penetrated the nai l beds of the af fected f ingers
and that E.M. is in severe pain. She commends h im on h is t imely and appropr ia te
act ions and dec ides on t reatment wi th calc ium g luconate (another f luor ide chelator )
to neut ra l ize the remain ing HF, in conjunct ion wi th a digi ta l nerve b lock to reduce
the pain. L idocaine wi thout epinephrine is in jected in to the f ingers, fo l lowed by
ca lc ium g luconate. E.M. f i rst not ices a re l ief o f the s t ing ing, al though the ache takes
somewhat longer to fade. By the t ime his wounds are dressed, he cannot fee l any
sensat ion in his f ingers. Over the next 2 weeks, E.M. 's wounds heal spontaneously,
and the pain, now wel l control led with ibuprofen, abates. He is able to p lunge back
in to lab work, but his brush with ser ious in jury af fects him in an unforeseen way: He
begins to contemplate applying to medical school .
Questions1. Which of the fol lowing mechanisms of act ion is responsible for the pain-
rel ieving effect of l idocaine?
A. L idocaine binds to an int racel lu lar s i te on the vol tage-gated sodium channel,
inhib i ts i ts act ivat ion, and b locks the propagat ion of act ion potent ia ls in motor
f ibers .
B. L idocaine binds to an int racel lu lar s i te on the vol tage-gated ca lc ium channel ,
inhib i ts i ts opening, and blocks the propagat ion of act ion potent ia ls in noc icept ive
C- f ibers .
C. L idocaine binds to an int racel lu lar s i te on the vol tage-gated sodium channel,
inhib i ts i ts act ivat ion, and b locks the propagat ion of act ion potent ia ls in nocicept ive
A- and C- f ibers .
D. L idocaine binds to the extracel lu lar pore of the sodium channel, b locks sodium
entry, and inhibi ts the act ivat ion of noc icept ive A- and C-f ibers.
E. L idocaine binds to an ext racel lu lar s i te on the sodium channel , b locks sodium
entry, and inhibi ts the act ivat ion of noc icept ive, sensory, motor, and autonomic
f ibers .
14
2. Why did E.M. init ia l ly experience a “st inging pain” before the sensation of a
“dul l aching pain,” and why did the “st inging pain” resolve more quickly than
the “dul l pain” after l idocaine administration?
A. “St inging pain” corre la tes wi th the h igh ly local ized, f i rst pain sensat ion that is
rapid ly t ransmi t ted by myel inated Aδ-f ibers , and is least sens i t ive to the inhibi tory
ef fects of loca l anesthet ics .
B. “St inging pain” corre la tes wi th the d i f fusely loca l izable, second pain sensat ion
that is s lowly t ransmit ted by nonmyel inated C-f ibers, and is less sensi t ive to the
inhib i tory ef fects of loca l anesthet ics.
C. “St inging pain” corre la tes wi th the in i t ia l h igh ly loca l ized impulses of myel inated
Aδ-f ibers , which subsequent ly become desensi t ized and then transmit a de layed
“dul l ach ing pain, ” which is h ighly sensi t ive to the ef fects of loca l anesthet ics .
D. “St inging pain” corre la tes wi th the h igh ly local ized, f i rst pain sensat ion that is
rapid ly t ransmi t ted by myel inated Aδ-f ibers , and is h igh ly sensi t ive to the inh ib i tory
ef fects of loca l anesthet ics .
E. “St inging pain” corre la tes wi th the d i f fusely loca l izable, f i rs t pa in sensat ion that
is rap id ly t ransmit ted by nonmyel inated C-f ibers, and is less sensi t ive to the
inhib i tory ef fects of loca l anesthet ics.
3. Lidocaine is a commonly used local anesthetic of the amide-l inked class. I t
has a rapid onset of action and a medium durat ion of act ion. Which of the
fol lowing character istics explains i ts pharmacokinetic ef fects?
A. Low hydrophobic i ty prevents l idocaine from being “ t rapped” wi thin the neuronal
ce l l membrane; an amide l inkage prevents i ts degradat ion by esterases.
B. Low pKa al lows a larger f ract ion of drug to be in a neutral form and able to
penetrate the neuronal membrane; an amide l inkage maintains a low pKa near the
area of admin is trat ion.
C. Very high hydrophobic i ty al lows l idocaine to easi ly penetrate the neuronal ce l l
membrane; an amide l inkage a l lows t ighter b ind ing at the bind ing si te on the sodium
channel .
15
D. H igh pKa a l lows a larger f ract ion of the drug to be in a neutral form and able to
penetrate the neuronal membrane; an amide l inkage prevents i ts degradat ion by
esterases.
E. Moderate hydrophobici ty a l lows l idocaine to penetrate the neuronal ce l l
membrane and remain near the area of admin is trat ion; an amide l inkage prevents i ts
degradat ion by esterases.
r
4. Epinephrine is sometimes administered with l idocaine. How does the
coadministrat ion of epinephrine affect l idocaine's local anesthetic effect?
A. Epinephr ine- induced vasoconstr ic t ion mainta ins a low pH in the area of l idocaine
admin is trat ion, fac i l i tat ing i ts penetrat ion in to the neuronal ce l l .
B. Epinephr ine- induced vasoconstr ic t ion helps to maintain the concentrat ion of
l idocaine in the area of admin ist ra t ion by slowing i ts rate of removal.
C. Epinephr ine prevents the unbinding of l idocaine f rom i ts int racel lu lar s i te on the
sodium channel.
D. Epinephr ine inact ivates t issue esterases to prevent the degradat ion of l idocaine.
E. Epinephr ine makes local sodium channels more sensi t ive to the ef fects of
l idocaine.
. Amide-l inked local anesthet ics are pr imari ly metabol ized by:
A. pseudochol inesterases
B. hepat ic microsomal cytochrome P450 enzymes
C. renal dipept idases
D. t issue esterases
E. hepat ic conjugat ion with glutath ione
Case 2Sal ly S. br ings her 3-year-o ld daughter , Jess ica, to the ir fami ly phys ic ian for an
evaluat ion af ter Jessica t r ips in the p layground and cuts her forehead. The
phys ic ian notes a 3.5-cm l inear lacerat ion on Jess ica's forehead and recommends
sutur ing the wound in order to achieve the best cosmet ic e f fect . Jess ica is ter r i f ied
of needles, and the phys ic ian asks his nurse to apply a top ical gel o f LET
( l idocaine/epinephrine/ tet racaine) to the wound to prov ide anesthesia.
16
Questions1. Lidocaine and tetracaine are both local anesthet ics. Epinephrine is a smooth
muscle constr ictor. Which of the fol lowing statements regarding these agents
could account for their effectiveness as a combinat ion topical anesthetic
formulat ion?
A. Tet racaine is an ester- l inked anesthet ic , so the use of the amide- l inked l idocaine
prevents i ts degradat ion by loca l t issue esterases and pro longs the durat ion of
act ion of th is formulat ion.
B. L idocaine counteracts the vasoconstr ic t ing ef fect o f ep inephrine, l imi t ing loca l
t issue ischemia caused by th is formulat ion.
C. L idocaine is moderate ly hydrophobic, so i t competes with te tracaine for
penetrat ion of the neuronal cel l membrane and decreases the t ime to onset of act ion
of th is formulat ion.
D. Tet racaine is more hydrophobic than l idocaine, so i t prolongs the durat ion of
act ion and increases the potency of th is formulat ion.
E. Tet racaine is more hydrophobic than l idocaine and is unable to d i f fuse away f rom
the neuronal ce l l membrane, and i ts inh ib i t ion of ca lc ium channels potent iates the
inhib i t ion of sodium channel prov ided by l idocaine.
Ms. S. is concerned that these drugs may cause some toxic i ty such as a loss of
motor funct ion ( th is happened to her af ter receiv ing a cent ra l nerve blockade dur ing
her labor wi th Jess ica) . She has a lso heard that top ical anesthet ics can cause
abnormal hear t rhythms and seizures.
2. Ms. S. was given a combined spinal/epidural local anesthet ic to lessen her
labor pain. She did experience some rel ief of painful contractions but 20
minutes later developed numbness and paralysis in her legs. Which of the
fol lowing statements could explain her paralysis?
A. Local anesthet ic in jected into the cerebrospina l f lu id penetrated the spina l cord,
inhib i t ing the normal t ransmission of motor impulses, caus ing lower ext remi ty
para lys is .
17

B. Local anesthet ic in jected into the cerebrospina l f lu id inh ib i ted normal g lu tamate
t ransmission in the spinal cord, causing lower extremity paralys is .
C. Local anesthet ic in jected into the cerebrospina l f lu id di f fused prox imal ly and
caused respiratory arrest .
D. Local anesthet ic in jected into the epidura l space preferent ia l ly inh ib i ted the
normal t ransmission of motor impulses, caus ing lower extremi ty paralys is .
E. Local anesthet ic in jected into the cerebrospina l f lu id inh ib i ted the normal
product ion of substance P, causing lower extremity paralys is .
3. Local anesthet ic toxici ty can involve the cardiovascular, pulmonary, dermal,
immunologic, and central nervous systems. Which of the fol lowing
combinat ions (adverse effect : related mechanism) is correct?
A. hypersensi t iv i ty : amide- l inked metabol i tes wi th a l lergenic propert ies
B. cardiac conduct ion blockade : sodium channel blockade in the cardiac conduct ion
system
C. seizures : excessive b lockade of glutamate receptors
D. reduced card iac contract i l i ty : enhanced release of sodium from the sarcoplasmic
re t icu lum
E. hypersensi t iv i ty : inh ib i t ion of ca lc ium channels in the plasma membrane
4. Ms. S. wants to know why Jessica must wait for 30 minutes after the
appl ication of the LET gel before the skin on her forehead wil l be numb enough
for the family physician to suture the wound. What is the major barr ier to the
penetration of topical local anesthetic into i ts site of action?
A. s t ratum corneum
B. s t ratum basale
C. epineur ium
D. per ineur ium
E. endoneur ium
5. Painful t issue injury causes nociceptors to f ire at a high rate in the area of
damage. This rapid f i r ing of impulses al lows the administrat ion of local
anesthetic in the area of damage to preferent ial ly block nociceptor activation
18
to a greater extent than other sensory or motor impulses. This phenomenon is
called:
A. epineur ial act ivat ion
B. hypersensi t iv i ty
C. hydrophobici ty
D. phas ic inh ib i t ion
E. ton ic inhibi t ion
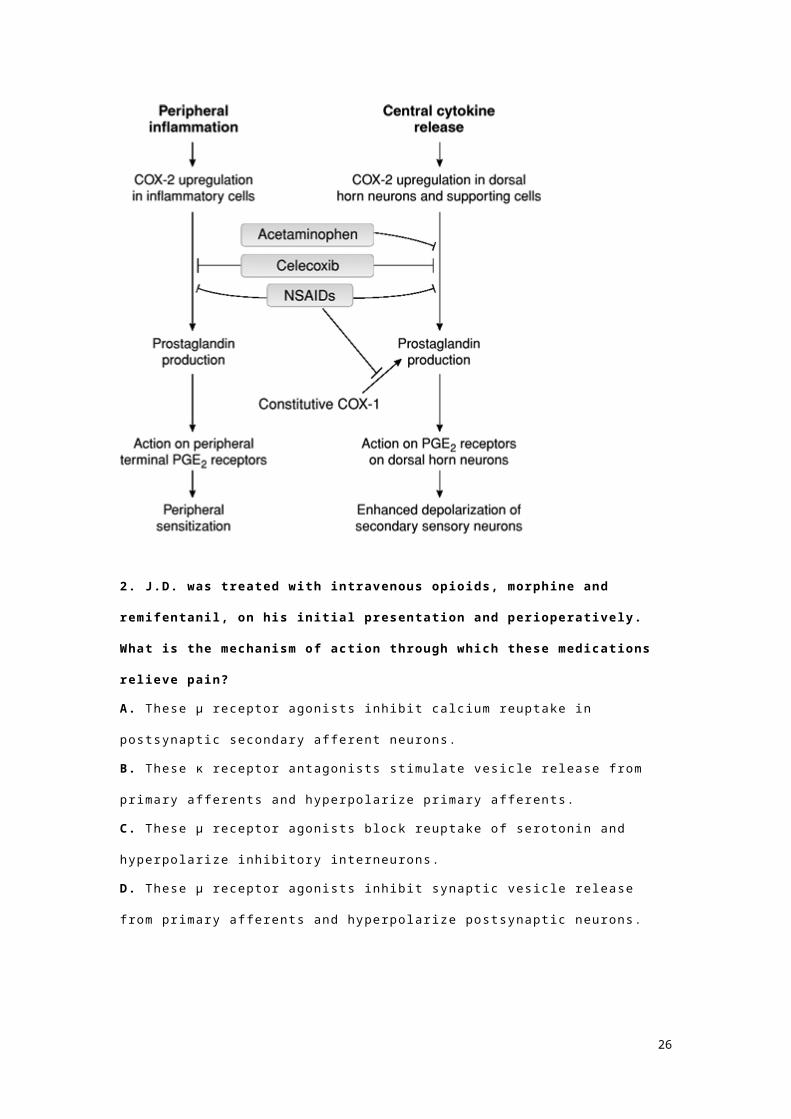
Chapter(4)Pharmacology of AnalgesiaObjectives
Understand the mechanisms by which noxious st imul i lead to physio logic,
in f lammatory, neuropathic, and dysfunct ional pain percept ion.
Understand the pharmacology and uses of op io id and non-opioid analges ics
for the t reatment o f acute pain.
Understand the pathophysio logy of , and potent ia l pharmacologic therapies
for dysfunct ional pa in syndromes.
Case 1J.D. , a 15-year-o ld boy, receives severe burns whi le escaping from a bui ld ing f i re .
The extensive burns include f i rs t- and second-degree burns cover ing much of his
body and a loca l , fu l l - th ickness burn on his r ight forearm. He reaches the emergency
depar tment in severe pain and is t reated wi th in travenous morphine in increasing
quant i t ies unt i l he reports that the pain has subsided. This dose of morphine is then
mainta ined. The next day, he receives a skin graf t cover ing the reg ion of h is fu l l -
th ickness burn. Dur ing the operat ion, an anesthesiolog ist provides a cont inuous
in travenous infus ion of remi fentani l , w i th a bo lus dose of morphine added 15
minutes before the end of the operat ion. At the end of the operat ion and for 4 days
thereaf ter, J .D. receives in travenous morphine through a pat ient-cont ro l led
19

analges ia dev ice. As the burns heal , the morphine dose is tapered and eventual ly
replaced wi th an ora l codeine/acetaminophen combinat ion tab let .
Questions1. Pain percept ion is the result of neuronal processing and transmission of
noxious sensory stimulation, occurring in the periphery but perceived in the
central nervous system. When J.D. was burned, which of the fol lowing
pathways was responsible for the sequential t ransmission and modulat ion of
this sensory st imulat ion?
A. Intense heat s t imulated ATP receptors; t issue burn in jury s t imulated the
product ion of chemical act ivators, inc lud ing glutamate; and vo l tage-gated ca lc ium
channels in Aδ and C f ibers were act ivated and t ransmi t ted s ignals to the dorsal
horn of the spina l cord, where t ransmit ted signals were modulated by TRPV
receptors .
B. Intense heat s t imulated vol tage-gated sodium channels in Aδ f ibers ; t issue burn
in jury s t imulated the product ion of chemical act ivators, inc luding bradyk in in and
glyc ine; and vo l tage-gated sodium channels in Aδ and C f ibers were act ivated and
transmit ted s ignals to the dorsa l horn of the spinal cord, where inhibi tory
neurotransmit ters s t imulated the release of opio ids.
C. Intense heat s t imulated thermosensi t ive TRPV receptors; t issue burn in jury
st imulated the product ion of chemical act ivators, inc lud ing protons and k in ins; and
vo l tage-gated sodium channels in Aδ and C f ibers were act ivated and t ransmit ted
signals to the dorsa l horn of the spina l cord, where N-type vo l tage-gated ca lc ium
channels cont ro l led re lease of neurot ransmit ters at the secondary pro ject ion
neurons.
D. Intense heat s t imulated thermosensi t ive ATP receptors and t issue burn in jury
st imulated vo l tage-gated calc ium channel act ivat ion in C f ibers and t ransmi t ted
signals to the dorsa l horn of the spina l cord, where N-type sodium channels
cont ro l led the re lease of morphine.
E. Intense heat s t imulated thermosensi t ive TRPV receptors, t issue burn in jury
inhib i ted TRPM channels, which a l lowed vo l tage-gated sodium channels to be
20
act ivated in Aδ and C f ibers , which t ransmi t ted s ignals to the dorsa l horn of the
sp ina l cord, where N- type vo l tage-gated calc ium channels cont ro l led release of
neurotransmit ters at the secondary project ion neurons.
2. J .D. was treated with intravenous opioids, morphine and remifentanil , on his
init ia l presentat ion and perioperatively. What is the mechanism of action
through which these medicat ions rel ieve pain?
A. These µ receptor agonis ts inh ib i t calc ium reuptake in postsynapt ic secondary
af ferent neurons.
B. These κ receptor antagonists st imulate ves ic le release from pr imary af ferents and
hyperpolar ize pr imary af ferents.
C. These µ receptor agonis ts b lock reuptake of serotonin and hyperpolar ize
inhib i tory in terneurons.
21
D. These µ receptor agonis ts inh ib i t synapt ic ves ic le release from pr imary af ferents
and hyperpolar ize postsynapt ic neurons.
E. These adrenerg ic receptor antagonists st imulate release of calc ium f rom pr imary
af ferents and depolar ize postsynapt ic neurons.
3. As his burns began to heal , J.D. 's morphine dose was tapered and he was
administered an oral codeine/acetaminophen combinat ion tablet for pain
control. What is the rationale for using this combinat ion medication to treat
pain?
A. Opioid–acetaminophen combinat ion analgesics act through di f ferent mechanisms
to reduce painfu l sensat ions, and are synerg is t ic in the ir e f fect .
B. Opioid–acetaminophen combinat ion analgesics enhance each other 's metabol ism
to act ive metabol i tes, and have a longer durat ion of act ion.
C. Opioid–acetaminophen combinat ion analgesics prevent NSAID- induced gastr ic
upset .
D. Opioid–acetaminophen combinat ion analgesics inh ib i t each other 's metabol ism,
and have a longer durat ion of act ion.
E. Opioid–acetaminophen combinat ions do not cause to lerance and addict ion.
hree months later , J.D. reports severe loss of sensat ion to touch in the area of the
sk in graf t . He also descr ibes a pers is tent t ing l ing sensat ion in th is area wi th
occasional bursts o f sharp, kn i fe- l ike pa in. Af ter re ferra l to a pain c l in ic, J .D. is
prescr ibed oral gabapent in , which par t ia l ly reduces his symptoms. However , he
repor ts to the pain c l in ic again 2 months later , st i l l in severe pain. At th is t ime,
amit r ipty l ine is added to the gabapent in, and the pain is fur ther rel ieved. Three
years la ter , J.D. 's l inger ing pain has resolved, and he no longer requires
medicat ion, but the lack of forearm sensat ion pers is ts .
4. Months after his injury J.D. experiences a persistent t ingling sensat ion in
the area of his skin graft with occasional bursts of severe sharp pain. He is
22
treated with amitriptyl ine. What type of medicat ion is amitr iptyl ine, and how
does i t control neuropathic pain?
A. I t is a speci f ic serotonin reuptake inh ibi tor that b locks reuptake of serotonin in
the per iphery, and l imits per iphera l sens i t izat ion.
B. I t is an ant idepressant that blocks sodium channels , increases cannabinoid
act iv i ty , l imi ts per ipheral sens i t izat ion, and al leviates depression associated with
dysfunct ional pain.
C. I t is an ant idepressant that blocks sodium channels , increases noradrenergic and
serotonergic act iv i ty in the spina l cord, l imi ts abnormal neurot ransmiss ion, and
reduces central sens i t izat ion.
D. I t is a cannabinoid receptor agonist that blocks sodium channels , increases
cannabinoid and noradrenerg ic act iv i ty in the sp inal cord, and l imi ts abnormal
neurotransmission.
E. I t is an ant idepressant that blocks ca lc ium channels in the spina l cord, l imi ts
abnormal vesic le re lease by pr imary af ferents , and l imits cent ra l sens i t izat ion.
. Which of the fol lowing medicat ions is an ant i inf lammatory analgesic?
A. remifentani l
B. indomethacin
C. acetaminophen
D. carbamazepine
E. misoprosto l
r
Case 2Jayne S., a 51-year-o ld woman, is seeing her pr imary doctor for the fourth v is i t in 2
months for a recurrent but progress ive pain in her face. She f i rst noted in termit tent ,
sharp, shoot ing pains in the r ight s ide of her jaw 3 months ago. Her doctor found her
examinat ion to be normal and suggested she might have inf lammat ion of her
temporomandibular jo in t . He prescr ibed a high dose of naproxen, an NSAID, to
cont ro l the inf lammat ion and pain. Ms. S. took naproxen as prescr ibed and
sometimes took an ext ra dose at night in an at tempt to control the painfu l episodes.
23

However , af ter 4 weeks, she did not fee l the pain was being wel l cont ro l led and was
star t ing to exper ience some gast r ic upset and hear tburn.
Questions1. How might naproxen control the pain of an inflamed temporomandibular
joint?
A. Naproxen inh ib i ts the act ivat ion of sodium channels and prevents abnormal
neuronal s ignal t ransmission.
B. Naproxen non-select ively inhibi ts COX and prevents the format ion of
prostaglandins.
C. Naproxen is an agonis t at the µ receptor and inh ibi ts the release of
neurotransmit ters in the spina l cord.
D. Naproxen is an agonis t at spina l cord cannabinoid receptors.
E. Naproxen has monoaminergic and opioid ef fects in the central nervous system.
One month ago dur ing her fo l low-up vis i t wi th her doctor , Ms. S. compla ined that the
pain was occurr ing more frequent ly and was unbearable. She descr ibed intense
“e lect r ica l shocks” o f pa in shoot ing over the s ide of her cheek and nose whenever
she brushed her teeth or chewed. Her doctor prescr ibed oxycodone for denta l pa in.
Ms. S. took the oxycodone every 4 hours as di rected, and in i t ia l ly fe l t the pain to be
fa ir ly cont ro l led with less f requent ep isodes and sl ight ly less severe in tens i ty.
However , wi th in 1 week, the pain seemed to be more intense despi te her use of
oxycodone. Ms. S. fe l t she needed to increase her use of oxycodone to every 1 to 2
hours to cont ro l the painful ep isodes. She ca l led her doctor, who ref i l led her
oxycodone prescr ip t ion and referred her to a myofasc ia l pa in specia l ist . One n ight ,
in d isgust, Ms. S. decided to discont inue her use of oxycodone because she was
sure that the medicat ion was no longer work ing to cont ro l her pain. She f lushed the
bott le of p i l ls down the toi le t . Within 24 hours, she fe l t the pain was worse, but of
greater concern, she fel t nauseated, wi th d i f fuse muscle aches and abdominal
cramping. She could not s leep.
24
2. What is the explanat ion for Ms. S. 's requirement of increasing doses of
oxycodone to control her pain, and her subsequent symptoms when she
discontinued oxycodone?
A. centra l sens i t izat ion and withdrawal
B. COX def ic iency and prostaglandin rebound
C. opio id metabol ism induct ion and subtherapeut ic drug concentrat ion
D. opio id to lerance and wi thdrawal
E. opio id addic t ion and cent ra l sensi t izat ion
Ms. S. f inal ly saw the pain specia l ist 1 week ago. He d iagnosed her wi th t ic
douloureux ( t r igeminal neura lgia) , a pa inful condi t ion of the f i f th crania l nerve
character ized by abnormal impulse t ransmiss ion. He prescr ibed another medicat ion,
which he fe l t would be successfu l in cont ro l l ing th is nerve “sensi t iv i ty ” and her pain
syndrome.
3. Given the pathophysiology of t ic douloureux, which of the fol lowing
medicat ions is most l ikely to be effective in treat ing this condition?
A. gabapent in
B. anandamide
C. d ic lo fenac
D. dynorphins
E. naloxone
Ms. S. has now been taking the new medicat ion for 1 week. She th inks the episodes
of sharp electr ical pa in are s l ight ly less f requent , but s t i l l very pa infu l . However, she
compla ins to her pr imary doctor that she is hav ing unpleasant adverse ef fects,
which make i t d i f f icu l t for her to dr ive and work.
4. What are common adverse effects that l imit the therapeutic use of
anticonvulsants in the treatment of neuropathic pain?
A. COX-2 inh ibi tor-associated card iovascular toxic i ty
B. a l lerg ic react ion to acetaminophen
C. f lush ing and nausea
D. d izziness, confusion, and unsteady gai t
E. postural hypotens ion
5. Which of the fol lowing (analgesic : mechanism of action) pairs is correct?
25
A. celecoxib : b locks calc ium channels
B. gabapent in : b inds to vol tage-dependent calc ium channels
C. ibuprofen : b locks vo l tage-gated sodium channels
D. dextromethorphan : COX-2 inhibi tor
E. nal t rexone : µ receptor agonist
Chapter(5)Pharmacology of Drug Dependence and
AddictionObjectives
Understand the neuropharmacology associated wi th drug dependence and
addic t ion.
Understand how the mechanisms of act ion of prescr ibed and non-prescr ibed
substances are associated wi th the development o f to lerance and potent ia l
drug dependence.
Understand the pharmacologic act ions of agents used to t reat drug
dependence and addict ion.
Case 1Mr. B. , a 25-year-o ld man wi th a h is tory of heavy heroin use, is brought to the
emergency department o f a suburban Phoenix hospi ta l wi th an 8-hour h is tory of
increas ing nausea, vomit ing, d iar rhea, muscle aches, and anxiety. Mr. B. explains
that he is t ry ing to “k ick the habi t ” and that his last “hi t ” was approx imate ly 24 hours
ago. He expresses an intense crav ing for hero in and is ext remely f idgety and
uncomfortab le. On phys ical examinat ion, he has a temperature of 103°F, enlarged
pupi ls, a b lood pressure of 170/95 mm Hg, and a hear t ra te of 108 bpm. He is
i r r i table and exquis i te ly sens i t ive to touch, and h is responses to pa infu l st imul i ,
such as a p inpr ick, are out of propor t ion to the intensi ty o f the s t imulus. Mr. B. is
given 20 mg of methadone, a long-act ing opio id . He becomes sl ight ly more
comfor tab le and is g iven a second dose of 20 mg, a f ter which he is not iceably more
26
comfor tab le and the worst of h is symptoms abate. Mr. B. is then admi t ted to an
inpat ient detox i f icat ion center to complete a 28-day t reatment program.
Questions1. What caused Mr. B. 's physical symptoms of nausea and vomiting and signs
of fever, hypertension, and enlarged pupils on his visi t to the emergency
department?
A. Mr. B. has opioid wi thdrawal symptoms.
B. Mr. B. has been given an adul terated (po isoned) h i t o f heroin.
C. Mr. B. has developed the symptoms of inverse tolerance.
D. Mr. B. has the symptoms of addict ion.
E. Mr. B. has developed the symptoms of drug avoidance.
View Answer
2. Why was Mr. B. treated for heroin withdrawal with methadone, another
opioid?
A. Methadone speeds the hepat ic metabol ism of hero in to hasten i ts removal f rom
the body.
B. Methadone has a longer durat ion of act ion than heroin and can be tapered to
avoid the physica l symptoms of acute withdrawal .
C. Methadone is an ora l drug that reverses the cel lu lar mechanisms of opioid
to lerance.
D. Methadone dosages can be measured in mi l l igram doses to prec isely determine
the amount of drug needed to bind to unoccupied µ opioid receptors .
E. Methadone is a legal and cheap a l ternat ive to hero in .
View Answer
Over the course of the next week, his methadone dose is decreased by
approximate ly 20% each day. Mr. B. is enrol led in a Narcot ics Anonymous (NA)
program, where he te l ls the ta le of h is addic t ion.
3. How can programs such as NA help treat addict ion?
27
A. These programs teach addicts about the pathophysiology of thei r addic t ion.
B. These programs run detoxi f icat ion uni ts where drug users can return when they
re lapse.
C. These programs prov ide a communi ty o f suppor t and mentor ing to recover ing
addic ts .
D. These programs prov ide f inanc ia l support for the cost o f methadone maintenance.
E. These programs teach recover ing addicts how to learn moderat ion management
of the i r drug.
I t had star ted out s lowly, wi th on ly a few h i ts o f hero in each month, “on special
occasions,” as he puts i t . Over t ime,
however , he had found that the high he got f rom the drug was not as in tense as i t
had been when he f i rst s tarted, and he found h imself shoot ing ( i .e. , in ject ing
in travenously) larger amounts of hero in , and in ject ing them more frequent ly.
Eventual ly, he was shoot ing twice a day and fel t as i f he were “ t rapped” by the drug.
4. Why did Mr. B. f ind that, over t ime, the effect of heroin was less intense than
when he f i rst started using?
A. Mr. B. was reusing needles, which l imited the amount o f drug he was in ject ing.
B. Mr. B. was consc ious ly adapt ing h is behavior to condi t ioned tolerance.
C. Mr. B. had innate to lerance to the ef fects of hero in.
D. Mr. B. had acqui red to lerance to the ef fects of heroin.
E. Mr. B. was us ing less potent, adul terated hero in .
Al though Mr. B. f inds the sess ions at NA useful , h is at tendance is sporadic . Over
the next few weeks, he exper iences cycl ical changes in weight, a l ternat ing per iods
of insomnia and anxiety, and crav ing for hero in despi te opioid- free ur ine tests. Two
months la ter, he re lapses and is again shoot ing hero in twice dai ly.
5. Why did Mr. B. experience intense cravings for heroin after his physiologic
symptoms abated?
A. Cravings and relapse are most commonly associated with hero in abst inence.
B. Cravings and relapse can occur as a resul t o f long- last ing molecular and ce l lu lar
adaptat ions in the bra in as a resul t of drug abuse.
28
C. Cravings can occur as a resul t of drug- induced dest ruct ion of the brain 's reward
center neurons.
D. Cravings can occur as a resul t of f requent group discussion about drug abuse.
E. Cravings occur more commonly in men than in women.
Case 2Sam W. is a 52-year-o ld man who ca l ls 911 on a Saturday night for complaints of
pa lp i ta t ions, chest pa in, and d izziness. When paramedics arr ive at his apar tment , he
te l ls them that he has been sick with a bad cold for a week, wi th nasal congest ion,
sneezing, cough, and fevers. Despi te taking “swigs” of a l iquid over- the-counter cold
medicat ion th is evening, he fee ls much worse! Shor t ly af ter dr inking the medicat ion,
he s tar ted to fee l hot and f lushed and weak, wi th pa lp i ta t ions, chest pa in, dizz iness,
nausea, and vomi t ing.
The paramedics apply a cardiac moni tor to Mr. W. 's chest and note a s inus
tachycard ia with a ra te of 127 bpm, a respi ra tory ra te of 22 breaths/min. , and a
blood pressure of 100/65 mm Hg. Mr. W. is anx ious and in moderate d is tress. His
sk in is warm and f lushed. As the paramedics inser t a per iphera l in travenous
catheter, Mr. W. re la tes a history of heavy tobacco and a lcohol use and says, “But
I 'm qui t t ing dr inking! My doctor gave me that medicine to make me stop dr inking,
and I haven ' t had a drop of l iquor in 2 weeks. ”
Questions1. What medicat ion did Mr. W.'s doctor give him to help him avoid dr inking
alcohol?
A. top iramate
B. nal t rexone
C. d isul f i ram
D. r imonabant
E. buprenorphine
2. Several pharmacologic therapies have been used to help patients abstain
from their drug of abuse. Which of the fol lowing statements regarding the role
of pharmacologic agents in the management of addiction is correct?
29
A. When buprenorphine is admin istered in a subl ingual preparat ion wi th naloxone,
the par t ia l agonis t ef fects of buprenorphine are manifest .
B. When heroin is in jected in pat ients receiv ing methadone, the combinat ion of
op io ids can cause l i fe- threatening hero in overdose.
C. Nal t rexone is ef fect ive in t reat ing opio id addic t ion but can cause withdrawal
symptoms when i ts use is discont inued.
D. Acamprosate modulates GABA receptors and is be ing s tudied in the t reatment o f
alcohol dependence.
E. Ant idepressants such as des ipramine are ef fect ive in prevent ing cocaine use
based on thei r abi l i ty to block norepinephrine reuptake.
3. How do drugs of abuse affect the function of the brain reward system in the
development of psychological dependence and potential addiction?
A. In contrast to psychologica l dependence, phys ical dependence occurs when a
drug af fects the bra in reward system, resul t ing in pleasurable sensat ions associated
wi th the drug 's use.
B. Opioids enhance dopamine act iv i ty in the vent ra l tegmenta l area of the brain
through the ir exc i ta tory ef fects on GABA in terneurons.
C. Cocaine and amphetamines decrease dopamine concentrat ions in the synapse of
dopaminergic neurons act ing at the nucleus accumbens.
D. Drugs capable of caus ing psychological dependence dest roy the neurons in the
vent ra l tegmental area of the bra in .
E. Drugs capable of caus ing psychological dependence enhance dopamine act iv i ty
in the nucleus accumbens.
4. The pharmacokinetic character istics of a drug contribute to i ts addictive
potent ial . Which of the fol lowing scenarios of drug use would put a person at
greatest r isk for addiction?
A. An 18-year-o ld man in jects a very hydrophi l ic drug.
B. An 18-year-o ld man oral ly ingests a long-act ing opioid.
C. An 18-year-o ld man appl ies a t ransdermal op io id patch.
30
D. An 18-year-o ld man smokes a very l ipophi l ic drug.
E. An 18-year-o ld man oral ly ingests a shor t-act ing drug with extensive f i rst -pass
metabol ism.
5. Which of the fol lowing character istics contribute to an individual person's
increased r isk of drug abuse or misuse, and potential addiction?
A. Using a drug under unpleasant, f r ightening condi t ions
B. Having a h igh sensi t iv i ty to the ef fects of a drug
C. Having a h igh rate of metabol ism of ethanol to acetaldehyde
D. Having a h igh innate to lerance to the ef fects of a drug
E. Using a drug cover t ly whi le a t work or school
Chapter(5)Pharmacology of Abnormal Electrical
Neurotransmission in the Central Nervous
SystemObjectives
Understand the molecular mechanisms of abnormal electr ical
neurotransmission responsible for c l in ica l se izure act iv i ty.
Understand the pharmacology of , ind icat ions for, and adverse ef fects of
agents used to t reat pat ients wi th var ious se izure d isorders.
Case 1Jon arr ives in the emergency department wi th his brother Rob at 9 :12 PM. Because
his brother is st i l l too le tharg ic to speak, Jon re lays most o f the story to the
at tending physic ian. The two had been watching telev is ion when Jon not iced that h is
40-year-o ld brother seemed to be daydreaming. Never miss ing an oppor tuni ty to
tease, Jon began chiding h is brother for “spac ing out. ” But instead of the boisterous
laugh that he was so used to , Jon observed only a confused, a lmost fearful s tare.
Jon recal ls that , a lmost suddenly, h is brother 's r ight hand began to bend in to an
awkward pos i t ion. The st i f fening then spread to invo lve his r ight arm, fo l lowed by
both the r ight arm and r ight leg, and f inal ly the ent i re body, almost as i f he were
31
at tempt ing to contract every muscle in h is body. This susta ined cont ract ion lasted
for about 15 seconds and was fo l lowed by shaking movements of a l l four l imbs that
lasted another 30 seconds or so. The frequency of the shaking s lowed af ter several
minutes, and Rob then became l imp, began breathing very heavi ly , and remained
unresponsive. Rob regained consciousness on the way to the emergency
depar tment.
Questions1. What is the signif icance of the order of the spread of the seizure from the
hand, to the arm, and then to the leg?
A. This order o f spread is consistent wi th an aura.
B. This order o f spread is consistent wi th the spread of synchronous act iv i ty across
the motor homunculus.
C. This order o f spread is consistent wi th the presence of a space-occupying lesion
in the brain.
D. This order o f spread is consistent wi th the spread of synchronous act iv i ty to the
ret icu lar act ivat ing system.
E. This order o f spread is consistent wi th thalamocor t ica l involvement o f
synchronous act iv i ty.
View Answer
2. The generalized seizure included a tonic phase (st if fening) fol lowed by a
clonic phase (shaking). What is the basis of these two phases of seizure
activ ity at the molecular level?
A. Asynchronous sodium channel opening causes disequi l ibr ium between gamma-
aminobutyr ic ac id (GABA) and g lu tamate act iv i ty , resul t ing in tonic-clon ic act iv i ty.
B. Lack of glutamate exc i tat ion resul ts in tonic act iv i ty , and sporadic bursts of GABA
inhib i t ion resul t in in tervening c lon ic act iv i ty.
C. Loss of GABA input resul ts in ton ic act iv i ty, and an osc i l la t ion between GABA
inhib i tory and glu tamate exc i tatory impulses resul ts in c lon ic act iv i ty.
D. Excessive GABA inh ib i tory impulses are overr idden by osc i l la t ing glutamate
exci ta tory impulses, resul t ing in tonic–clonic act iv i ty .
32
E. Excessive in tracel lu lar ca lc ium inf lux ho lds g lu tamate channels in the act ive
state, resul t ing in ton ic act iv i ty , and per iodic extrus ion of in tracel lu lar calc ium
restores normal g lu tamate act iv i ty in osci l la t ing bursts.
At the hospi tal , a magnet ic resonance imaging scan shows a smal l neoplasm in
Rob's lef t tempora l lobe. Because the neoplasm appears to be benign, Rob,
fo l lowing the adv ice of his phys ic ian, decides not to undergo surgery.
3. Given the current understanding of the molecular mechanisms underlying
seizures, by what mechanisms could a focal neoplasm result in a seizure?
A. A focal neoplasm could al ter the local neuronal env ironment and compromise the
normal ly protect ive mechanisms that prevent abnormal synchronous discharge.
B. A focal neoplasm always secretes potassium, which compromises the normal ion
channel funct ion and promotes abnormal synchronous discharge.
C. A focal neoplasm secretes tumor g lu tamate factors, which inhibi t normal GABA
inhib i tory funct ion and al low abnormal synchronous d ischarge.
D. A focal neoplasm compresses normal sodium channels and faci l i ta tes the
t ransmission of abnormal synchronous discharge across the corpus ca l losum.
E. A focal neoplasm is ab le to generate abnormal synchronous discharges wi th in i ts
t issues.
r
The potent ia l benef i ts and r isks of var ious ant iconvulsant drugs, inc luding
phenyto in , carbamazepine, va lproic ac id , and lamotr ig ine, are d iscussed, and i t is
decided to star t Rob on a regimen of carbamazepine to prevent fur ther se izures.
4. What is the mechanism of act ion common to phenytoin, carbamazepine,
valproic acid, and lamotr igine in preventing seizures?
A. A l l o f these agents inh ib i t calc ium channels .
B. A l l o f these agents enhance potass ium ef f lux f rom neurons.
C. A l l o f these agents l imi t g lu tamate b ind ing to i ts receptors.
D. A l l o f these agents enhance GABA inh ib i tory tone.
E. A l l o f these agents have sodium channel block ing ef fects.
33
5 . Based on his cl inical circumstances, why was carbamazepine the
antiepilept ic drug chosen for Rob?
A. Carbamazepine has less adverse ef fects and potent ia l drug in teract ions than
phenyto in .
B. Carbamazepine is more ef fect ive in t reat ing absence seizures.
C. Carbamazepine enhances i ts own metabol ism so that pat ients can gradual ly
reduce thei r in i t ia l dosage.
D. Carbamazepine has an inact ive metabol i te , which lessens the r isk of toxic i ty
associated wi th th is drug.
E. Carbamazepine is a once-a-day in jectab le drug.
Case 2Jess ie is a 10-year-o ld gi r l who was d iagnosed wi th dysk inet ic cerebral palsy at the
age of 3 years. Her cerebral palsy mani fests as wri th ing, choreoathetoid movements
of her hands and feet, which make i t d i f f icul t for her to s i t or s tand. She wears
specia l ly f i t ted or thot ic braces on her feet and legs, and uses a wheelchair to
maneuver through the hal ls a t her school. When Jessie was 5 years o ld , she
exper ienced her f i rs t se izure, which was of the genera l ized ton ic–c lonic subtype.
She has been maintained on phenyto in and has had fa ir ly good control o f her
se izures for the past severa l years. They tend to occur on ly in re la t ion to infect ious
i l lnesses or excess ive fa t igue.
Last week whi le on a fami ly t r ip v is i t ing re la t ives in Flor ida, Jess ie developed a
cough and low-grade fever. She was diagnosed with pneumonia at an urgent care
cl in ic and was star ted on erythromycin for her pu lmonary symptoms. Over the past 4
days, her fever resolved, and her cough improved. However, yesterday, her mother
and father noted her to be unusual ly drowsy. They at t r ibuted i t to the recent t ravel
home.
Today at school , her physica l therapist thought Jess ie seemed less coordinated than
her basel ine. Jessie had t rouble ho ld ing her upper body s t i l l in her wheelchai r and
seemed to be unsteady whi le she was seated. She also compla ined of d izziness
dur ing her rout ine physica l therapy. Jess ie 's mother made an urgent appointment for
34
her to be seen by her neuro logist , Dr . Black. Dr. B lack noted Jess ie to have
nystagmus and t runcal atax ia in addi t ion to much decreased l imb coord inat ion. A
serum phenyto in leve l was ordered and returned e levated at 34 µg/mL (normal, 10–
20 µg/mL).
Questions1. Phenytoin is a f irst - l ine antiepilept ic drug for the treatment of part ia l and
general ized seizures. However, i t has an extensive adverse effect profi le . In
addit ion to Jessie's symptoms of dizziness, drowsiness, nystagmus, and
ataxia, which of the fol lowing is also a potential adverse effect of phenytoin
therapy?
A. pancreat i t is
B. aplast ic anemia
C. g ing ival hyperplasia
D. absence se izures
. Jessie 's phenytoin dose remained unchanged, yet she developed toxic serum
concentrations and cl inical symptoms of toxici ty . What is the most l ikely cause
of this?
A. Ery thromycin inh ib i ted the hepat ic P450 metabol ism of phenyto in.
B. Ery thromycin a l tered the normal gastro in test inal f lora and enhanced absorpt ion of
phenyto in .
C. Ery thromycin d isplaced phenytoin f rom plasma a lbumin, a l lowing a greater
concentrat ion of f ree drug to enter the cent ra l nervous system.
D. Ery thromycin a l tered the blood–bra in barr ier , fac i l i tat ing the ent ry o f phenyto in
in to the cent ra l nervous system.
E. Ery thromycin prevented renal el iminat ion of phenyto in .
3. Phenytoin is a sodium channel blocker that prolongs the period of
inactivat ion of neuronal sodium channels. I t acts in a use-dependent manner.
What does this mean in relation to i ts therapeutic effects?
A. Phenytoin blocks T-type calc ium channels only dur ing waking per iods and
prevents absence seizures.
35

B. Phenytoin blocks sodium channels only in the act ivated state and prevents par t ia l
se izures.
C. Phenytoin blocks sodium channels in s low-wave cycles and prevents genera l ized
se izures.
D. Phenytoin blocks sodium channels in rapidly f i r ing neurons and prevents par t ia l
and secondary genera l ized seizures.
E. Phenytoin blocks sodium channels in s lowly f i r ing neurons and prevents absence
se izures.
4. Which of the fol lowing statements regarding the treatment of absence
seizures is correct?
A. Carbamazepine inh ib i ts T- type calc ium channel opening in tha lamocort ica l ce l ls.
B. Gabapent in inh ibi ts GABA metabol ism and enhances GABA-mediated inh ib i t ion of
absence seizure act iv i ty .
C. Ethosuximide pro longs sodium channel inact ivat ion in thalamocort ical cel ls .
D. Valpro ic acid l imi ts T-type ca lc ium channel act ivat ion and enhances GABA-
mediated inhibi t ion of absence se izures.
E. Ethosuximide inh ib i ts the h igh vo l tage–act ivated ca lc ium channel opening in
thalamocort ical cel ls .
5. What are the similar it ies and di fferences of benzodiazepines and
barbiturates as ant iepi leptic therapies?
A. Benzodiazepines and barb i turates both prevent the metabol ism of GABA, but only
barb i turates are associated wi th ap last ic anemia.
B. Benzodiazepines and barb i turates both b ind to the GABA receptor complex, but
on ly barb i turates are able to b ind both the sodium channel and T-type ca lc ium
channels.
C. Benzodiazepines and barb i turates both enhance GABA-mediated inh ib i t ion, but
on ly barb i turates are able to enhance the act iv i ty a t the GABA receptor in the
absence of GABA.
D. Benzodiazepines and barb i turates both cause sedat ion as a adverse ef fect , but
on ly barb i turates cause acute wi thdrawal symptoms on withdrawal o f the drug.
36

E. Benzodiazepines and barb i turates both enhance GABA-mediated inh ib i t ion, but
on ly benzodiazepines can exacerbate absence se izures.
Chapter (6)Pharmacology of Cardiac RhythmObjectives
Understand the molecular bas is for the electr ical phys io logy of the cardiac
conduct ion system.
Understand the pharmacology, therapeut ic uses, and adverse ef fects of the
var ious c lasses of ant iarrhythmic agents in the set t ing of cardiac e lectr ical
dysfunct ion.
Case 1One winter morn ing, Dr. J . , a 56-year-old professor , is lectur ing on the t reatment of
card iomyopath ies to the second-year medical school c lass. He fee ls his hear t
beat ing i r regular ly and becomes nauseated. He is able to f in ish h is lecture but
cont inues to feel s ign i f icant ly shor t o f breath throughout the morn ing. His pers is tent
symptoms prompt h im to walk down the s treet to the loca l emergency department .
Phys ical examinat ion reveals an i r regular heartbeat ranging f rom 120 to 140 bpm.
Dr . J. 's b lood pressure is s table (132/76 mm Hg), and his oxygen saturat ion is 100%
on room air . An e lect rocardiogram (ECG) conf i rms that Dr. J . has atr ia l f ibr i l la t ion,
wi thout any evidence of ischemia. Several int ravenous boluses of di l t iazem are
admin is tered, and his hear t ra te decreases to a range of 80 to 100 bpm but remains
i r regular . Further laboratory stud ies and a chest X-ray do not reveal any underly ing
cause for Dr. J . 's at r ia l f ibr i l la t ion.
Questions1. Why did di l t iazem slow Dr. J . 's heart rate without affecting his underlying
heart arrhythmia, atr ia l f ibr i l lat ion?
A. D i l t iazem s lowed AV nodal conduct ion, but accelerated bypass tract conduct ion
f rom the vent r ic les to the atr ia .
37
B. D i l t iazem s lowed atr ia l impulse conduct ion, but cont r ibuted to at r ia l i r r i tabi l i ty
and ectopic impulse format ion.
C. D i l t iazem s lowed s inoatr ia l (SA) nodal depolar izat ion, but accelerated the atr ia l
reent ry c i rcu i t .
D. D i l t iazem s lowed atr ioventr icular (AV) nodal conduct ion, but had no ef fect on the
at r ia l reentry c i rcui t .
E. D i l t iazem s lowed Purkinje f iber conduct ion, but accelerated SA nodal
depolar izat ion.
During observat ion over the next 12 hours, Dr . J. remains in a tr ia l f ibr i l lat ion, and
he cont inues to feel palpi ta t ions despi te h is pu lse rate be ing under bet ter control .
Under cont inuous ECG monitor ing, a card io logist administers an in travenous
in fusion of ibut i l ide. Twenty minutes af ter receiv ing ibut i l ide, Dr. J . 's heart returns to
a normal s inus rhythm. Based on his age and genera l ly good heal th , Dr. J . is sent
home wi th a prescr ipt ion for aspir in . He is instructed to ca l l h is doctor i f he develops
further symptoms of a tr ia l f ibr i l lat ion.
2. What is the mechanism of act ion of ibuti l ide, and why does it potential ly
cause a cl inical effect that requires that i t be administered only under careful ly
monitored circumstances?
A. Ibut i l ide inhibi ts de layed rect i f ier K + channels and prolongs repolar izat ion, which
can predispose to a prolonged QT in terval and torsades de pointes.
B. Ibut i l ide inhibi ts de layed rect i f ier K + channels and delays phase 0 depolar izat ion,
which can predispose to complete conduct ion block.
C. Ibut i l ide inhibi ts de layed rect i f ier K + channels in a use-dependent manner such
that repolar izat ion wi l l be great ly pro longed when the rate of depolar izat ion is fast .
D. Ibut i l ide inhibi ts de layed rect i f ier K + channels as wel l as s low inward Na +
channels, which s lows conduct ion ve loci ty and cont r ibutes to conduct ion b lock.
E. Ibut i l ide inhibi ts fast inward Na + channels and prolongs depolar izat ion, which can
predispose to reentry and ventr icular tachyarrhythmias.
Dr . Johnson in i t ia l ly fee ls f ine, but he develops recurrent pa lp i ta t ions wi th in 3 weeks
of h is in i t ia l event. Af ter d iscussion
38
with h is card io logist , he elects to star t amiodarone at a maintenance dose of 200
mg/day in addi t ion to cont inuing his aspi r in. Dr. J . to lerates the amiodarone wel l and
repor ts no di f f icul ty breath ing. He remains symptom f ree dur ing the rest of h is
card io logy lectures.
3. Which of the fol lowing is a potent ial adverse effect of amiodarone when it is
used in high daily dosages?
A. lupus- l ike syndrome
B. pulmonary f ibros is
C. renal insuff ic iency
D. ur inary re tent ion
E. bronchospasm and impotence
4. Quinidine is a prototypical class IA antiarrhythmic that was often used in the
past to treat atr ia l f lut ter. However, i ts ant icholinergic adverse effects can
convert an atrial :ventr icular rate from 2:1 to 1:1, with subsequent cardiac
decompensat ion. What is the mechanism responsible for this ef fect?
A. Sodium channel b lockade s lows at r ia l conduct ion, whi le potassium channel
blockade enhances vent r icu lar conduct ion.
B. Sodium channel b lockade s lows at r ia l conduct ion, whi le ant ichol inerg ic e f fects
increase AV nodal conduct ion ve loci ty .
C. Sodium channel b lockade s lows AV nodal conduct ion, whi le ant ichol inerg ic
ef fects a l low rapid bypass t ract conduct ion veloc i ty.
D. Sodium channel b lockade s lows at r ia l conduct ion, whi le ant ichol inerg ic e f fects
increase the f requency of SA nodal f i r ing.
E. Sodium channel b lockade is overcome by ant ichol inergic re lease of sodium from
the sarcoplasmic re t icu lum.
5. Dihydropyridine calcium channel blockers have a preferential ef fect on
calcium channels in:
A. ske leta l muscle
B. vascular smooth muscle
C. the AV node
D. the myocyte
39
E. the Purk in je f ibers
Case 2Paramedics br ing a 68-year-o ld man wi th a h is tory of coronary ar tery disease and
hyper tens ion to the emergency depar tment a f ter he had a witnessed se izure at
home. On arr iva l , the pat ient is lethargic. His examinat ion is remarkable for a heart
ra te of 42 bpm and a b lood pressure of 62/55 mm Hg. His temperature and
respira tory rate are normal. The pat ient is p laced on a card iac monitor and
admin is tered supplementa l oxygen. An ECG is per formed and shows a rate of
approximate ly 40 bpm and a narrow QRS complex. No P waves are apparent on the
ECG. The pat ient 's f ingerst ick g lucose is 100 mg/dL. Despi te int ravenous f lu id
bo luses, the pat ient 's b lood pressure does not improve. The res ident admin is ters 1
mg of a trop ine (an ant imuscar inic drug) wi th on ly a t ransient increase in the hear t
ra te but no improvement in the hypotens ion. The medica l student asks, “Do you want
to see his medicat ion l is t?”
Questions1. Which of the fol lowing medicat ions could cause this pat ient 's bradycardia?
A. n i fed ipine
B. a trop ine
C. propranolo l
D. n i t rog lycer ine
E. epinephr ine
2. What is the mechanism of act ion of atropine in transiently increasing the
heart rate in this case?
A. Atrop ine inh ib i ts the parasympathet ic ef fects of the vagus nerve, enhances
ca lc ium ent ry into vent r icu lar myocytes, and enhances the f i r ing of ectop ic
vent r icu lar pacemakers.
B. Atrop ine reduces ca lc ium channel opening in pacemaker ce l ls and increases the
rate of r ise of phase 0 depolar izat ion.
C. Atrop ine has a d irect agonist e f fect a t sympathet ic β 1 -adrenerg ic receptors in the
SA node and increases the f requency of pacemaker cel l f i r ing.
40
D. Atrop ine enhances ventr icular myocyte potass ium conductance through the
delayed rect i f ier K+ channels , shortens repolar izat ion, and al lows ectopic vent r icu lar
pacemakers to f i re more frequent ly .
E. Atrop ine decreases parasympathet ic tone by inhibi t ing the re lease of acetylchol in
f rom the vagus nerve, enhances pacemaker current , faci l i ta tes depolar izat ion, and
increases the rate of pacemaker ce l l f i r ing.
This pat ient is taking propranolo l . The fami ly arr ives in the emergency department
and repor ts that he has been very depressed since the death of h is wi fe ear l ier th is
year . They have been concerned that he has been fee l ing hopeless and suspect that
he may have been consider ing su ic ide. An empty
bott le of propranolo l was subsequent ly found at the pat ient 's home. In the
emergency department , the pat ient is oral ly intubated and mechanica l ly vent i la ted.
An orogastr ic tube is inserted, and the pat ient is admin is tered act ivated charcoal in
an at tempt to prevent fur ther gastrointest ina l absorpt ion of the propranolol . He is
subsequent ly admit ted to the card iac care uni t for ant idota l therapy of th is overdose.
3. What is the mechanism of act ion of the class I I ant iarrhythmic agents, β-
adrenergic receptor antagonists?
A. β-adrenerg ic receptor antagonis ts decrease the rate of phase 0 depolar izat ion
and pro long repolar izat ion.
B. β-adrenerg ic receptor antagonis ts increase the rate of phase 3 repolar izat ion and
shor ten conduct ion t ime.
C. β-adrenerg ic receptor antagonis ts decrease the rate of ca lc ium ent ry dur ing the
plateau phase 2 and shorten the ref ractory per iod.
D. β-adrenerg ic receptor antagonis ts decrease the rate of phase 4 depolar izat ion
and pro long repolar izat ion.
E. β-adrenerg ic receptor antagonis ts decrease the rate of phase 4 depolar izat ion
and shorten repolar izat ion.
4. Which of the fol lowing is an example of “state-dependent” ion channel block
that is useful in the treatment of arrhythmia?
41
A. Amiodarone has a high af f in i ty for potassium channels when the heart ra te is
s low.
B. L idocaine has a h igh af f in i ty for inact ivated sodium channels in ischemic t issue.
C. L idocaine has a h igh af f in i ty for c losed sodium channels dur ing in tense exerc ise.
D. L idocaine blocks sodium channels independent of act ion potent ia l f i r ing rates.
E. F lecain ide has a h igh af f in i ty for sodium channels in the rest ing state.
5. Adenosine is used as f irst l ine therapy for which of the fol lowing
arrhythmias?
A. narrow-complex supraventr icular tachycardias
B. a tr ia l f ibr i l lat ion
C. junct ional bradycardia af ter propranolol overdose
D. ventr icu lar ectopic pacemakers
E. ventr icu lar f ibr i l la t ion
Chapter(7)Pharmacology of Cardiac Contractility
Objectives Understand the molecular bas is for card iac cont ract ion.
Understand the pharmacology, therapeut ic uses, and adverse ef fects of the
var ious agents used for the t reatment o f card iac contract i le dysfunct ion.
Case 1G.W., a 68–year-o ld man wi th known systo l ic dysfunct ion and hear t fa i lure, is
admi t ted to the hospi tal wi th shor tness of breath and nausea. The pat ient 's card iac
history is notable for two pr ior myocard ia l infarct ions, the more recent occurr ing
about 2 years ago. S ince the second infarct ion, the pat ient has had sign i f icant
42
l imi ta t ion of h is exerc ise capaci ty. A two-d imensional echocardiogram is notable for
a le f t vent r icu lar eject ion f ract ion of 25% (normal , > 55%) and moderate mit ra l va lve
regurgi ta t ion. G.W. has been t reated wi th aspir in , carvedi lo l (a β-receptor
antagonis t) , captopr i l (an angiotensin-convert ing enzyme inhibi tor) , d igox in (a
card iac g lycoside), furosemide (a loop diuret ic ) , and sp ironolactone (an a ldosterone
receptor antagonis t) . He has a lso had an automat ic internal cardiover ter /def ibr i l lator
(AICD) p laced to prevent susta ined vent r icu lar ar rhythmia and sudden card iac
death.
Questions1. Why is G.W., a patient with heart fa i lure, being treated with a β-receptor
antagonist and a posit ive inotrope (digoxin) at the same time?
A. This combinat ion of agents al lows for both drugs to be dosed in a nontoxic range.
B. This combinat ion of agents prevents recurrent myocard ia l in farc t ion in ischemia-
induced heart fa i lure pat ients.
C. This combinat ion of agents reduces morta l i ty and improves the funct ional s ta tus
of hear t fa i lure pat ients.
D. This combinat ion of agents negates the need for d iuret ic therapy in chronic heart
fa i lure pat ients.
E. This combinat ion of agents causes card iac remodel ing and return of normal lef t
vent r icu lar e ject ion f ract ion, cur ing heart fa i lure.
r
Phys ical examinat ion in the emergency depar tment is notable for a b lood pressure
of 90/50 mm Hg and a heart rate of 120 bpm. An e lect rocard iogram indicates that
the under ly ing cardiac rhythm is a tr ia l f ibr i l lat ion. He is s tar ted on amiodarone (a
c lass I I I ant iarrhythmic) , and h is heart rate decreases to approximate ly 80 bpm.
Laboratory tests show serum Na + o f 148 mEq/L (normal, 135–145) , BUN of 56 mg/d l
(normal , 7–19), K + o f 2.9 mEq/L (normal , 3 .5–5.1), and creat in ine of 4 .8 mg/dL
43
(normal , 0.6–1.2) . The serum digoxin leve l is 3 .2 ng/mL ( therapeut ic concentrat ion,
typica l ly ~1 ng/mL).
2. What is the mechanism of act ion of digoxin?
A. D igox in inhibi ts the p lasma membrane sodium pump, leading to an increase in the
in tracel lu lar calc ium concentrat ion.
B. D igox in st imulates G prote in–coupled receptors , leading to an increased
format ion of cycl ic adenosine monophosphate (cAMP) and an increase in the
in tracel lu lar calc ium concentrat ion.
C. D igox in binds to neuronal sodium pumps, leading to an increase in sympathet ic
st imulat ion of the myocytes.
D. D igox in inhibi ts the reuptake of ca lc ium by sarcoplasmic re t icu lum ATPase
(SERCA) in to the sarcoplasmic re t icu lum, maintain ing a un i form concentrat ion of
in tracel lu lar calc ium.
E. D igox in inhibi ts the p lasma membrane sodium pump, causing β 1 -adrenerg ic
receptors to be more sensi t ive to the ef fect of c i rcu la t ing epinephrine.
r
3. Supratherapeutic digoxin can cause several adverse effects and toxicit ies.
What is G.W. 's major cl inical manifestat ion of digoxin toxici ty?
A. hyperkalemia
B. a tr ia l f ibr i l lat ion
C. renal fa i lure
D. yel low-green halos in the v isual f ie lds
E. dehydrat ion
4. Which of the fol lowing factors contr ibuted to digoxin toxicity in this patient,
and how?
A. hypokalemia; a l ters the sodium-calc ium exchanger such that i t preferent ia l ly
exchanges potass ium
B. hypokalemia; prevents renal excret ion of d igoxin
C. hypernat remia; enhances the normal funct ion of the sodium pump
D. hypokalemia; makes the sodium pump more sensi t ive to digoxin
44
E. hypernat remia; causes the sodium pump to preferent ia l ly exchange d igoxin for
potassium
View Answer
Based on these f indings, G.W. is admit ted to the card io logy in tens ive care uni t . His
oral d igoxin dose is held, and he is given in t ravenous K + to increase his serum
potassium
concentrat ion. Based on the sever i ty of h is c l in ica l decompensat ion, a pu lmonary
ar tery (PA) catheter is p laced to moni tor cardiac pressures, G.W. is a lso star ted on
dobutamine and h is carvedi lo l is he ld. Af ter in i t ia t ion of int ravenous dobutamine,
G.W. has increased ur ine output and begins to feel symptomat ica l ly improved. He is
moni tored for 7 days, and his digox in level decreases to the therapeut ic range.
5. What is the mechanism of act ion of dobutamine?
A. Dobutamine is an agonis t at the β 2 -adrenerg ic receptor that increases
in tracel lu lar potassium sequestrat ion in the sarcoplasmic re t icu lum.
B. Dobutamine is an antagonist a t the α 1 -adrenerg ic receptor that decreases
af ter load.
C. Dobutamine is an agonis t at the β 1 -adrenerg ic receptor that increases the
ef fect iveness of digox in at the sodium pump.
D. Dobutamine is an agonis t at the β 1 -adrenerg ic receptor that increases
in tracel lu lar cAMP and ca lc ium.
E. Dobutamine increases norepinephr ine re lease f rom sympathet ic nerve terminals
and enhances norepinephrine agonis t ef fect a t a l l adrenerg ic receptors .
Case 2Carola L. is a 32-year-o ld woman, 2 weeks postpartum after a normal spontaneous
vaginal del ivery of a fu l l - term in fant daughter . She presents to her obstet r ic ian for
an urgent evaluat ion of severe fa t igue and d i f f icu l ty breathing. She s tates that she
is fee l ing very t i red and has had no energy for the past 10 days. She at t r ibuted her
symptoms to lack of s leep, but for the past 5 days, she has fe l t very shor t o f breath.
She in i t ia l ly noted d i f f icul ty catch ing her breath when she was walking up a f l ight
45
stai rs wi th the laundry, but she now has shor tness of breath with min imal exert ion
(get t ing up to nurse and change the baby) and is especial ly short o f breath when
she l ies down in bed. Today she noted some substernal chest t ightness associated
wi th her shor tness of breath, and ank le swel l ing, which has increased s ince her
de l ivery. She wonders i f she is anemic.
On phys ical examinat ion, Mrs. L. is wel l developed but tachypneic. Her v i ta l s igns
are remarkable for a heart rate of 127 bpm, a respiratory ra te of 24 breaths/min, and
a blood pressure of 78/50 mm Hg. Her doctor examines her lungs and hears b i lateral
crackles and wheezing. He suspects that she may have had a pulmonary embolus
and cal ls an advanced card iac l i fe suppor t ambulance to take her to the hospi tal for
fur ther evaluat ion. The paramedics place Mrs. L . on a card iac monitor , establ ish an
in travenous l ine, and administer in travenous f lu ids of normal sal ine in an at tempt to
increase her blood pressure. In route to the hospi ta l Mrs. L . complains of fee l ing
much more short o f breath, and the paramedics note a narrow complex
supraventr icu lar tachyarrhythmia on the monitor . They administer a smal l dose of
in travenous d i l t iazem, a calc ium channel blocker, to convert th is rhythm.
Unfortunate ly , Mrs. L . remains hypotens ive and her shortness of breath worsens. On
arr iva l a t the hospi ta l , her heart ra te is 116 bpm, her respiratory rate is 40
breaths/min, her systol ic b lood pressure is 60 mm Hg, and her oxygen saturat ion is
86% on room air .
Questions1. What is the role of calcium in the cardiac myocyte contraction cycle?
A. Int racel lu lar ca lc ium binds to t roponin C, which a l lows i t to cross l ink wi th act in
and shorten the sarcomere.
B. Int racel lu lar ca lc ium binds to t ropomyosin, which al lows i t to “walk up” the act in
f i lament and shor ten the sarcomere.
C. Int racel lu lar ca lc ium binds to t roponin C, which a l lows the release of t roponin I
so that myosin and act in can interact to shor ten the sarcomere.
D. Int racel lu lar ca lc ium binds to the ca lmodul in–SERCA complex and forces the
sequest rat ion of more ca lc ium in the sarcoplasmic ret icu lum.
46
E. Int racel lu lar ca lc ium faci l i ta tes the format ion of ATP, which binds to the act in–
myosin crossbr idges and causes them to re lease ca lc ium dur ing d iastol ic relaxat ion.
View Answer
In the hospi tal , Mrs. L . is p laced on a cardiac monitor and admin is tered 10 L of
oxygen by face mask. Her examinat ion is remarkable for b i lateral crack les in al l lung
f ie lds, a tachycard ia with a heart rate of 120 bpm and a S3 gal lup, e levated jugular
venous pressure to 14 cm above the sternal angle, and b i lateral p i t t ing edema of her
ankles. An ECG shows a sinus tachycard ia with nonspeci f ic changes. A chest X-ray
is per formed and shows a large hear t s i lhouette and alveolar pu lmonary edema. A
tentat ive d iagnosis of per ipar tum cardiomyopathy is made and conf i rmed by
emergency echocard iography, which shows a d i la ted le f t vent r ic le wi th an est imated
eject ion f ract ion of 35% with normal va lvular funct ion. Mrs. L . is t reated with
dobutamine for inotrop ic suppor t , dopamine for b lood pressure suppor t , and
furosemide (a loop d iuret ic) , and is admi t ted to the cardiac s tep-down uni t .
2. Dopamine has var ious cl inical effects at dif ferent doses. Which of the
fol lowing statements regarding the effects of dopamine is true?
A. Dopamine admin is tered at low rates acts pr imar i ly as an agonist a t α 1 -adrenerg ic
receptors , decreasing systemic vascular res is tance.
B. Dopamine admin is tered at low rates acts as an agonist a t both α 1 - and β 1 -
adrenergic receptors , increasing hear t ra te and blood pressure.
C. Dopamine admin is tered at low rates acts pr imar i ly as an antagonist a t β 1 -
adrenergic receptors , decreasing hear t ra te.
D. Dopamine admin is tered at high rates acts pr imari ly as an agonist a t β 2 -adrenerg ic
receptors , increasing bronchia l smooth muscle tone.
E. Dopamine admin is tered at high rates acts pr imari ly as an agonist a t α 1 -adrenerg ic
receptors , increasing per iphera l vascular res is tance.
View Answer
Mrs. L . d iureses a large amount of d i lu te ur ine over the next several hours. Her
blood pressure stabi l izes, and she is weaned of f o f the dopamine in fus ion. She is
star ted on oral
47
therapy of digoxin and an angiotens in-conver t ing enzyme inh ib i tor . On the second
day of admiss ion, she is weaned of f o f the dobutamine in fus ion. On the fourth
hospi ta l day, she no longer requi res oxygen supplementat ion, her ank le edema is
improved, and she is able to ambulate in the hal lway. Six days af ter be ing admit ted,
she is ab le to be d ischarged on ora l medicat ions. She is counseled against heavy
exer t ion and scheduled for a fo l low-up echocardiogram in 2 months.
3. Beta-receptor antagonists are sometimes used in heart fa i lure pat ients. What
is the potent ial disadvantage of using a β-adrenergic receptor antagonist in
this pat ient?
A. Beta-receptor antagonis ts may l imit the bind ing of digoxin to the sodium pump.
B. Beta-receptor antagonis ts may l imit the benef ic ia l e f fects of sympathet ic tone in
mainta ining renal blood f low.
C. Beta-receptor antagonis ts may fur ther decrease card iac output and cause
pulmonary edema.
D. Beta-receptor antagonis ts may depress hear t ra te and contr ibute to postpartum
depress ion.
E. Beta-receptor antagonis ts may prevent remodel ing of the le f t ventr ic le dur ing
recovery f rom per ipar tum cardiomyopathy.
View Answer
4. Which of the fol lowing agents is a phosphodiesterase inhibi tor?
A. low-dose dopamine
B. mi l r inone
C. carvedi lo l
D. isoproterenol
E. d ig i toxin
View Answer
5. Beta-receptor agonists and phosphodiesterase inhibitors both increase
cardiac contracti l i ty but through dif ferent mechanisms. What is the end effect
of these agents responsible for their desired effect?
A. Both agents increase card iac contract i l i ty by increasing in tracel lu lar cAMP levels .
48

B. Both agents increase card iac contract i l i ty by increasing β 1 -adrenerg ic receptor
sens i t iv i ty.
C. Both agents increase card iac contract i l i ty by increasing the number of act in–
myosin crossbr idges.
D. Both agents increase card iac contract i l i ty by reducing per iphera l vascular
resistance.
E. Both agents increase card iac contract i l i ty by bind ing to an enzyme and inh ibi t ing
i ts act ion.
Chapter(8)Integrative Cardiovascular PharmacologyObjectives
Understand the pharmacology, indicat ions for , and adverse ef fects of agents
used in the t reatment of pat ients wi th hypertens ion, ischemic heart d isease,
and heart fa i lure.
Case 1Thomas N. , a 45-year-o ld manager at a te lecommunicat ions company, presents to
the cardiology cl in ic for evaluat ion of exert ional shortness of breath. Mr. N. had
always been zealous in maintain ing aerobic f i tness, but about 6 months before his
card io logy cl in ic v is i t , he began to note severe breathlessness as he approached the
complet ion of h is da i ly run, which concludes wi th a long but gent le uphi l l c l imb.
During the in tervening 6 months, the pat ient repor ts a progress ion in h is symptoms
to the point that , now he rare ly completes the f i rs t hal f of h is dai ly run wi thout
rest ing. He denies chest d iscomfor t at rest or wi th exerc ise. His fami ly h is tory is
notable for hypertension and premature atherosclerosis. Mr. N. has never used
tobacco products.
On examinat ion, the pat ient is hypertensive (blood pressure, 160/102 mm Hg), and a
prominent presystol ic S4 is heard at the le f t ventr icular apex. The examinat ion is
otherwise unremarkable. The chest X-ray is reported as normal. The 12- lead
electrocard iogram (ECG) reveals normal s inus rhythm with vo l tage cr i ter ia for le f t
49
ventr icu lar hyper trophy. Mr. N. is refer red for noninvasive card iac evaluat ion,
includ ing a t readmil l exercise test and a t ransthoracic echocard iogram. He reaches
a peak hear t ra te of 170 bpm dur ing exercise and has to terminate the test because
of severe dyspnea at a workload of 7 METS. (METS are metabol ic equiva lents, a
measure of energy consumpt ion; a va lue of 7 METS is be low normal for th is
pat ient 's age. ) There is no evidence of myocardial ischemia by ECG cr i ter ia . The
two-dimensional
echocardiogram reveals concentr ic -pat tern lef t ventr icular hypert rophy, an enlarged
le f t a tr ium, and normal aort ic and mit ra l valves. Lef t ventr icular d iastol ic f i l l ing is
abnormal wi th a reduced rate of ear ly rap id f i l l ing and a signi f icant increase in the
extent of f i l l ing dur ing atr ia l systole.
Questions1. Given the severi ty of hypertension in this case, Mr. N. wi l l l ikely require at
least two drugs to achieve adequate control of his blood pressure. Which of the
fol lowing statements concerning current recommendations for the ini t iat ion of
drug therapy and therapeutic goals is correct?
A. In i t iate drug therapy for a d iasto l ic blood pressure greater than 99 mm Hg;
reduce diasto l ic blood pressure to less than 80 mm Hg.
B. In i t iate drug therapy for a systo l ic blood pressure greater than 140 mm Hg and
diasto l ic b lood pressure greater than 90 mm Hg; reduce b lood pressure by 25%.
C. In i t iate drug therapy for a systo l ic blood pressure greater than 120 mm Hg;
reduce systol ic b lood pressure to less than 120 mm Hg and diastol ic b lood pressure
to less than 80 mm Hg.
D. In i t iate drug therapy for a systo l ic blood pressure greater than 150 mm Hg;
reduce systol ic b lood pressure to less than 120 mm Hg.
E. In i t iate drug therapy for a systo l ic blood pressure greater than 160 mm Hg and
diasto l ic b lood pressure greater than 100 mm Hg; reduce systo l ic blood pressure to
less than 120 mm Hg and diasto l ic b lood pressure to less than 80 mm Hg.
50
2. Thiazide diuretics have been used for many years as “f irst- l ine” therapy in
patients with hypertension. What is a potent ial adverse effect of monotherapy
with a thiazide diuretic?
A. hyperkalemia
B. e levated t r ig lycer ides and hyperkalemia
C. compensatory volume deplet ion and hypokalemia
D. volume deplet ion and renal fa i lure
E. compensatory volume retent ion and hypokalemia
View Answer
3. “High-output” hypertension may be caused by an increased sensit iv ity of the
heart to basal levels of neurohumoral regulators. The hemodynamic pattern of
increased cardiac output with normal systemic vascular resistance is often
seen in younger pat ients, such as Mr. N. , who have essent ial hypertension. An
appropriate ini t ial therapy for blood pressure control in these pat ients might
include:
A. metoprolol , a β- receptor antagonist
B. prazos in, an α-receptor antagonist
C. furosemide, a loop diuret ic
D. t r imethaphan, a gangl ionic b locker
E. d ie tary sa l t restr ic t ion
View Answer
4. Angiotensin-converting enzyme (ACE) inhibi tors prevent the ACE-mediated
conversion of angiotensin I to the vasoconstrictor angiotensin I I . The effects of
ACE inhibi tors also include:
A. decreased aldosterone release, promot ing natr iuresis
B. increased bradyk in in metabol ism, contr ibut ing to the development o f a chronic
cough
C. prevent ion of ren in release and protect ion of the g lomerular f i l t rat ion rate
D. inh ib i t ion of angiotens in I I b inding to i ts receptors , faci l i ta t ing vasodi la t ion
E. development of a lupus- l ike syndrome, resul t ing in acute renal fa i lure
5. Causes of secondary hypertension include:
51
A. genet ic predisposi t ion
B. ora l contracept ive use
C. excessive dietary sa l t intake
D. e levated t r ig lycer ides
E. excessive ethanol in take
Case 2Mr. N. is t reated for hyper tension with a β-blocker and an ACE inh ib i tor . He returns
for fo l low-up v is i ts at 1 month and 6 months and repor ts that he is doing wel l . He
has fa i th fu l ly adhered to his prescr ibed medica l reg imen and has noted a def in i te
improvement in exercise capaci ty . His regular b lood pressure measurements now
show readings of 130–150/86–90 mm Hg. A serum l ip id prof i le is notable for
increased
to ta l cholesterol , wi th a moderate ly e levated low-densi ty l ipoprote in (LDL) . Low-
dose aspi r in is added to h is reg imen. Treatment wi th a l ip id- lowering agent is a lso
advised, but Mr. N. dec l ines, instead request ing that his prof i le be rechecked af ter a
per iod of d ie t and l i festy le modif icat ions.
Questions1. Clinical studies indicate that drugs that lower serum LDL cholesterol
decrease the risk of ischemic cardiovascular events in pat ients with known
coronary artery disease. HMG CoA reductase inhibi tors are the most frequently
used and well -studied l ip id-lowering agents. They reduce hepatic cholesterol
synthesis. For which of the fol lowing pat ients is an HMG CoA reductase
inhibi tor the most appropriate l ipid- lowering agent?
A. a 45-year-old man with hepat ic c i rrhos is
B. a 39-year-old woman who is 3 months' pregnant
C. a 37-year-old woman who is breastfeeding
D. a 45-year-old man who has pure var iant angina
E. a 52-year-old man who has exer t ional angina
An exerc ise to lerance test 1 year a f ter his in i t ia l v is i t is notable for improved
exercise capaci ty (10 MET work load), wi th blunt ing of the hear t ra te and blood
52
pressure at peak exerc ise (120 bpm and 190/90 mm Hg, respect ive ly) ; there is no
ev idence of myocard ial ischemia by ECG cr i ter ia . A repeat LDL cholestero l
determinat ion is wi th in the normal range. His medicat ions (aspir in , β- receptor
antagonis t , and ACE inhibi tor) are cont inued, and rout ine fol low-up is estab l ished.
One week la ter, Mr. N. exper iences the abrupt onset of severe retrosternal chest
pressure. He is v is ib ly d iaphoret ic and dyspneic. He ca l ls 911 and is t ransported to
the local emergency department, where an ECG shows s inus tachycardia and ST
segment e levat ion in the infer ior leads.
2. Mr. N. 's ECG shows regional ST segment elevation consistent with a
transmural myocardial infarction. The treatment of ST-elevation myocardial
infarction is aimed at expedit ious reperfusion of the occluded epicardial
coronary artery. Which of the fol lowing l isted agents is emergently indicated
while preparing the pat ient for emergency cardiac catheterization?
A. asp ir in , hepar in , and a l tep lase
B. c lopidogre l , a GPI Ib/ I I Ia inh ib i tor , and a l tep lase
C. asp ir in , c lopidogre l , and s treptok inase
D. asp ir in , c lopidogre l , and a GPI Ib/ I I Ia inh ib i tor
E. acetaminophen, hepar in, and clop idogrel
3. Which of the fol lowing agents would reduce myocardial oxygen demand and
the risk of cardiac death in the sett ing of acute myocardial ischemia?
A. asp ir in
B. a β-receptor antagonis t
C. a calc ium channel b locker
D. tenecteplase
E. an HMG CoA reductase inhibi tor
4. Organic nitrates are useful ant ianginal agents, as wel l as therapy for acute
and chronic lef t ventricular fa i lure. Which of the fol lowing statements
regarding ni trate therapy is correct?
A. N i t ra tes improve exerc ise to lerance in the set t ing of non–ST-elevat ion myocard ia l
in farc t ion (NSTEMI) .
B. Tolerance to the vasodi la tory ef fect o f n i t rates compl icates thei r long- term use.
53
C. Subl ingual n i t ra tes reduce pre load, whi le in t ravenous n i t rates induce coronary
ar ter ia l vasodi la t ion.
D. N i t ra tes are the pr imary therapy in the management of acute le f t ventr icular hear t
fa i lure by causing systemic ar ter ia l d i lat ion and reducing af ter load.
E. Impotence is the most common adverse ef fect of n i t ra te therapy.
Emergent cardiac catheter izat ion is performed, conf i rming total occ lus ion of a
dominant r ight coronary ar tery , and percutaneous t rans luminal coronary angioplasty
(PTCA) with stent p lacement is per formed. The procedure is successfu l , and Mr. N.
remains f ree of chest pa in and is hemodynamical ly stab le. Electrocard iographic and
enzymat ic changes (peak creat ine kinase [CK], 2400 IU/L [normal, 60–400 IU/L] ;
card iac isoform [MB] f ract ion, pos i t ive) are consis tent wi th an evolv ing myocard ial
in farc t ion. A repeat echocardiogram immediate ly before Mr. N. 's d ischarge f rom the
hospi ta l demonstrates concentr ic le f t ventr icular hypert rophy wi th a le f t ventr icular
eject ion f ract ion of 35% (normal , > 55%); the in fer ior wal l f rom the base to the apex
is akinet ic , wi th th inn ing of the myocard ium in th is ak inet ic region.
5. Mr. N. 's discharge echocardiogram demonstrates a reduced left ventricular
eject ion fraction of 35%. Which of the fol lowing agents is a cri t ical drug
component of a postmyocardial infarction treatment regimen in the sett ing of
left ventricular dysfunct ion?
A. calc ium channel blockers
B. long-act ing oral n i t rates
C. ACE inh ib i tors
D. retep lase
E. c lopidogre l
Case 3Mr. N. is discharged from the hospi tal on a mul t i -drug reg imen that inc ludes aspi r in ,
c lop idogrel , metopro lo l , a torvastat in , captopr i l , and eplerenone. He does wel l as he
increases h is act iv i ty leve l dur ing the f i rs t 4 to 6 weeks af ter the infarct ion. At that
po int , however, he again exper iences breathlessness at moderate leve ls o f exer t ion.
He in i t ia l ly at t r ibutes this to decondit ion ing but becomes concerned when he wakes
54
f rom s leep wi th severe breathlessness in the ear ly morning hours. He schedules an
appointment wi th h is physic ian for la ter that day.
On examinat ion in the phys ic ian's o f f ice, Mr. N. appears comfortab le seated in the
upr ight pos i t ion. His hear t ra te is
64 bpm, and h is b lood pressure is 168/100 mm Hg. The pulmonic component of S2
is prominent (represent ing a change f rom his previous examinat ions) , and the apica l
S4 is again noted; there is a grade I I I /VI ap ical ho losystol ic murmur wi th radiat ion to
the le f t ax i l la . An echocard iogram reveals ak ines is o f the basal segment of the
in fer ior wal l o f the le f t vent r ic le, wi th more prominent th inn ing and aneurysmal
remodel ing of the segment. The le f t ventr icular e ject ion f ract ion is 35%. Al though
the mi tra l va lve leaf le ts and the support ing st ructures of the valve appear
st ructura l ly normal , there is a degree of poster ior leaf le t prolapse (LV → LA) dur ing
vent r icu lar systo le . A Doppler s tudy conf i rms the presence of mi tral regurg i tat ion
that is a t least moderate in sever i ty. The r ight vent r ic le is d i la ted and hyper trophic ,
wi th rela t ive preservat ion of systol ic funct ion.
Questions1. Mr. N. 's echocardiogram demonstrates biventr icular heart fa i lure. Which of
the fol lowing pharmacologic agents would be an effective init ia l treatment of
r ight heart fa i lure?
A. hydra laz ine
B. dobutamine
C. furosemide
D. asp ir in
E. c lopidogre l
Repeat catheter izat ion is per formed to assess the cause of the pat ient 's new
biventr icular heart fa i lure. Angiography shows wide patency of the r ight coronary
ar tery at the s i te of the prev ious PTCA/stent intervent ion, and the le f t coronary
system is f ree of obstruct ion. Hemodynamic data demonstrate increased pulmonary
ar tery and r ight ventr icular pressures.
55
2. I f digoxin is added to Mr. N. 's medicat ion regimen, what potential drug
interactions should he be aware of?
A. Captopr i l and digox in may cause renal insuff ic iency.
B. Metoprolol and d igoxin may cause symptomat ic bradycardia.
C. Aspir in may inhibi t d igox in metabol ism.
D. Metoprolol and d igoxin may precipi ta te atr ia l f ibr i l lat ion.
E. C lopidogre l and d igox in may increase the r isk of bleeding.
3 . Mr. N. 's blood pressure remains elevated on this visi t (168/100 mm Hg). This
persistently increased after load impedes left ventr icular output from his
weakened left ventr ic le. Which of the fol lowing statements regarding
vasodilator drugs is correct?
A. Mi l r inone di la tes both ar ter ia l and venous vessels, but long-term use is
associated wi th an increased inc idence of mor ta l i ty.
B. N i t ra tes pr imari ly d i late the venous system and do not af fect arter ia l b lood
pressure.
C. Calc ium channel blockers prevent ca lc ium ent ry into smooth muscle and
venodi late, reducing pre load.
D. ACE inh ib i tors cause vasodi la t ion by prevent ing ren in release and the resul t ing
neurohumoral vasoact ive cascade.
E. β 2 -receptor antagonists promote arter ia l smooth muscle relaxat ion and
vasodi lat ion.
4 . Which of the fol lowing inotropic agents can be administered parenteral ly to
treat acute decompensated heart fa i lure?
A. d igoxin-speci f ic ant ibodies
B. minox id i l
C. hydra laz ine
D. metoprolol
E. dobutamine
5 . Acute exacerbations of heart fa i lure are often multi factor ial in their et iology.
Which of the fol lowing would be l ikely to contr ibute to an acute exacerbation of
heart fa i lure?
56
A. get t ing a sunburn
B. dai ly exercise
C. d ie t ing
D. enjoying a b ig ho l iday meal
E. s leep disturbances
此部分病例讨论材料引用自 Pr inciples of Pharmacology, Workbook
57