Embed Size (px)
Citation preview

CASE REPORT
Chinese Herbs and Bone DiseaseJunichi HOSHINO, Yoshifumi UBARA, Tetsuo TAGAMI, Naoki SAWA, Masafumi YOKOTA,
Hideyuki KATORI, Fumi TAKEMOTO,Yoshihisa MlKAMI*,Shigeo HARA**and Shigeko Hara
Abstract
Wetreated a patient with an unusual bone disease atleast partly associated with Chinese herbs. Seven yearsafter 65-year-old man had begun to consume Chineseherbs, multifocal osteoarthralgias were noted, and thepatient was hospitalized for renal dysfunction (serumcreatinine, 2.8 mg/dl; urea nitrogen, 19 mg/dl). Fanconisyndromealso was apparent. Arenal biopsy specimenshowed tubulo-interstitial fibrosis. Chinese herbs werediscontinued and prednisolone was started, but bone andjoint pain as well as renal function gradually worsened.Four years later, creatinine was 9.0 mg/dl and alkalinephosphatase was 571 IU//. As bone scintigraphy revealedlocalized asymmetric lesions, Paget's disease of bone wassuspected at first. However, neither osteosclerosis nor hy-pertrophy was seen in radiographs. Based on a bonespecimen histology we diagnosed as mixed-type renalosteodystrophy including osteomalacia and osteitisfibrosa. Mosaic pattern of cement lines was not present.This case was not compatible with either Paget's diseaseor typical renal osteodystrophy as seen in dialysis pa-tients. Etidronate disodium was effective in alleviatingbone symptoms. The patient's bone disorder may be anew disease at least partly related to Chinese herbs inde-pendently of nephropathy.(Internal Medicine 42: 345-350, 2003)
Key words: osteitis fibrosa, osteomalacia, renal osteodystro-phy, Paget's disease, osteopathy
IntroductionChinese herbs, long regarded as a relatively safe tradi-
tional remedy, rarely have caused adverse reactions despitetheir wide use. However, since the initial report in 1993 byVanherweghem and colleagues (1), nephropathy induced by
Chinese herbs has drawn increasing attention. Extra renal le-sions associated with Chinese herbs involving the lung, liver,heart, and lower urinary tract also have been reported.However,we knowof no reported occurrences of bonedisease caused by Chinese herbs. Weencountered an unusualcase with radiologically localized, asymmetric bone lesions,and a histologically mixed pattern including both osteitisfibrosa and osteomalacia, which became evident 7 years afterthe patient began to consume Chinese herbs.Paget's disease of bone and renal osteodystrophy might beconsidered as the differential diagnosis.
Case ReportA 65-year-old Japanese man was admitted to our hospitalbecause of generalized fatigue and multiple bone and jointpains including low back pain.Since 1989 the patient had taken Chinese herbs (Table 1)imported from Taiwan, intending to promote his generalhealth. On July 4, 1989, serum urea nitrogen (s-UN), serumcreatinine (s-Cr), and serum uric acid (s-UA) concentrationswere 16, 1.1, and 5.4 mg/dl, respectively. Multiple asymmet-ric osteoarthralgia in the right lumbar lesion, both knees, andfeet first appeared in January 1996. In November, renal dys-function was noted.The patient was admitted to our hospital on December 19,1996 for further evaluation. Laboratory findings at that timewere: s-UN, 20 mg/dl; s-Cr, 2.5 mg/dl; and s-UA, 2.5 mg/dl.Sodium was 140 mmol//, potassium 4.1 mEq//, chloride 113mmol//, calcium 4.1 mEq//, and phosphate 1.6 mg/dl. Alka-line phosphatase (Al-P) was 804 IU/Z (normal range; 120 to350); the elevated Al-P isoenzyme was the bone-derivedtype. Fasting blood glucose was 104 mg/dl, and HbAlc
5.4%. By arterial blood gas analysis, pH was 7.32; HCO3" 17mmol//; and anion gap 10. On endocrinologic examination,intact parathyroid hormone (i-PTH) was 104 pg/ml (normalrange; 20.0 to 53.0), 1,25(OH)2 Vitamin D3 concentrationwas below 7.9 ng// (normal range; 20 to 60) and bone glaprotein(BGP) was ll.2 ng/ml (normal range; 3.1 to 12.7). On
From Kidney Center, ^Department of Orthopedics and **Department of Pathology, Toranomon Hospital, TokyoReceived for publication August 15, 2002; Accepted for publication January 16, 2003Reprint requests should be addressed to Dr. Junichi Hoshino, Kidney Center, ToranomonHospital, 2-2-2 Toranomon, Minato-ku, Tokyo 105-8470
Internal Medicine Vol. 42, No. 4 (April 2003)345

Hoshino et al
Table 1. Components of the Chinese HerbsAdministered in This Case
1. Alisma rhizome2. Ginseng
3. Japanese angelica root4. Poria sclerotium
5. Atractylodes lancea rhizome6. Atractylodes rhizome7. Astragalus root8. Achyranthes root9. Phellodendron bark10. Rehmannia root1 1. Eucommiaecortex
12. Ophiopogon tuber13. Moutan bark14. Asini corii collas15. Schisandra fruit
16. Panax notoginseng burk17. Japanese angelica root
18. Cervus Nippon temminck19. Dipsacus asper wal20. Chinemys reevesii21. Salva miltiorrhiza22. Lycii fructus23. Cibotinm barometz24. Cornus fruit25. Dendrobium officinale K26. Paeonia lactiflora27. Dioscorea batatas decne
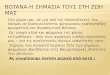
Figure 1. Light microscopic examination of renal bi-opsy specimen showed extensive tubulo-interstitial fi-brosis with scant cell filtration (Periodic acid Schiff(PAS) reagent staining; x20).
Figure 2. Light microscopic examination of rightiliac bone biopsy showed evidence of increased boneresorption such as increased number and size ofosteoclasts, and evidence of increased percentage offibrous tissue (HE stain, xlOO).
urinalysis, pH was 6.5. Dipstick reagent readings were glu-cose, 3+; protein, 1+; and occult blood, 3+. Amino acid
analysis of urine revealed accelerated excretion of 19 kindsof amino acids, and Fanconi syndrome was diagnosed. Withhis mouth dryness and fibrous salivary gland was also diag-nosed by lip biopsy. The Chinese herbs formula was ana-lyzed by high performance liquid chromatography (HPLC)and aristolochic acid (AA) was detected.
A renal biopsy was performed on January 13, 1997; thespecimen showed extensive tubulo-interstitial fibrosis withscant cell infiltration (Fig. 1), compatible with Chinese herbnephropathy. Although bone scintigraphy with 99nTc-labeledmethylene diphosphonate revealed asymmetric areas of in-tense uptake (a characteristic of Paget's disease) in the rightiliac bone, both knees (right dominant), and joints of the feet,only localized changes were shown by radiography and com-puted tomography;no areas of bone enlargement or thicken-ing were seen. Right iliac bone biopsy showed evidence ofincreased bone resorption such as increased numberand sizeof osteoclasts, and evidence of increased percentage of fi-brous tissue (Fig. 2). Osteitis fibrosa was diagnosed at thattime. Neither any bone tumors nor metastasis was shown.Wecould not analyze further because it was a decalcifiedsection.Chinese herbs were discontinued, and prednisolone (20mg p.o. on alternate days), and calcitriol (0.25 |jg p.o. daily)
were initiated.In 1998, Fanconi syndrome showed improvement, and theelevated serum Al-P concentration decreased (Fig. 3). Boneand joint pains also decreased. [Laboratory findings at thattime were: s-UN, 35 mg/dl; s-Cr, 4.6 mg/dl; and s-UA, 7.3mg/dl. Sodium was 140 mmol//, potassium 4.0 mEq//, chlo-ride 109 mmol//, calcium 4.0 mEq//, phosphate 2.4 mg/dl,and Al-P 334 IU//. By arterial blood gas analysis, pH was7.39; HCO3 20 mmol//; and anion gap ll. On urinalysis,neither aminoaciduria nor glycosuria nor proteinuria was de-tected].In December 1999, the pain increased, as did Al-P. Thepatient was admitted to our hospital for further evaluation ofbone metabolism on February 24, 2000. On admission, s-UNwas 42 mg/dl; s-Cr, 9.0 mg/dl; s-UA, 6.8 mg/dl; calcium, 4.3mEq/ /; phosphate, 4.6 mg/dl; intact PTH, 248.1 pg/ml; Al-P,571 IU/Z; BGP, 54.7 ng/ml; and cross-linked C-terminal
346 Internal Medicine Vol. 42, No. 4 (April 2003)

Chinese Herbs and Bone Disease
Chinese herbsP77777777I Etidronate disodium å å å å
Calcitriol fQM gg/foy.^Ss^Sft^^^Prednisolone '(alternate days) 20 mg 15 mg 10 mg [
iPTH(pg/ml) 104 98 141 197 421 248 228 228BGP (ng/ml) ll.2 18.4 26.8 54.7 91.2 45.1
12 [ ^ Biopsy ^ Biopsy 1 900(mg/dl) r (IU/ /)(mEq/l) rV\ /
/ \ r^sy - 6oo , ,I \ / Cr (mg/dl)
' \ ^^ /"^ /\ k Ca(mEq/l)
6- V/ V'V yV y\ /J Vv P(mg/dl)N/ As--J- r' x^ A \ ALP(IU//)
0I i i i i 1 1 1 1 1 « å 1 à"0
Jul. Nov. Mar. Jul. Nov. Mar. Jul. Nov. Mar. Jul. Nov. Mar. Jul.
96 96 97 97 97 98 98 98 99 99 99 00 00
Figure 3. Clinical course.
telopeptide of type I collagen (ICTP), 26.3 ng/ml (normalrange; 0.6 to 4.9). Results of repeat bone scintigraphy (Fig.
4A), radiography, and computed tomography (Fig. 4B) ap-
peared as previously.On February 24, 2000, right iliac bone biopsy was per-
formed again, 14 days after administration of tetracycline fordouble labeling studies. Undecalcified thin sections 5|um inthickness were prepared from the bone specimenand were
stained by the Villanueva methods. Histomorphometric
analysis is shown in Table 2. Light microscopic examinationshowed evidence of increased bone resorption such as in-creased numberand size of osteoclasts and an increased per-centage of lacunar bone surface. This osteolysis wasaccompanied by evidence of bone formation, and fibrous tis-sue was increased adjacent to the trabecular bone. Excessiveunmineralized lamellar osteoid also was present (Fig. 5A).Osteoclasts with more than 50 nuclei were observed (Fig.5B). Deposition of aluminumwas not found within the
Table 2. Histomorphometric Analysis of the Bone
Bone volume (BV/TV) 28.0% (normal, 14.9±2.6%)Osteoid volume (OV/TV) 6.0% (0. 1 - 1.0)Osteoid volume (OV/BV) 21.5% (1.6±0.4)Osteoid surface (OS/BS) 79.5% (23. 1+9.8)Osteoid thickness (O.Th) 19.8 jum (9.8+2. 1)
Eroded surface (ES/BS) 1 8.2% (4.0±1.2)Osteoblast surface (Ob.S/BS) 2 1.0%Osteoclast number (N.Oc/B S) 0.3/mm2Fibrous tissue volume (Fb.V/TV) 5.6% ( 0 )Mineral apposition rate (MAR) 0.67 jum/day (0.66±0. 1 3)Doubly labeled surface (dLS/BS) 1 1.6%Single labeled surface (SLS/BS) 32.8%
Bone formation rate (BFR/BS) 0.0689 mmVmmVyearBone formation rate (BFR7BV) 73. 1 %/year
Internal Medicine Vol. 42, No. 4 (April 2003) 347

Hoshino et al
A
B
Figure 4. (A) Bone scintigraphy revealed localizedasymmetric bone lesions. (B) Computed tomographyshowed no areas of bone enlargement or thickening.
mineralization in the surface of the bone. Polarizing micro-scopic examination showed normal lamellar bone, but also
wovenbone (a sign of high bone turnover). No mosaic pat-tern of cement lines (a characteristic of Paget's disease) wasseen (Fig. 5C). Fluorescence microscopy showed a singly la-beled surface as well as a doubly labeled surface (Fig. 5D),indicating osteomalacia (unmineralized, low-turnover bone)
and osteitis fibrosa (high-turnover bone) admixed in a single
specimen.Histomorphometric analysis according to Coburn' s classi-fication yielded a diagnosis of mixed-type renal osteodystro-phy, with excessive total osteoid volume (>15%) andexcessive fibrous tissue volume (>0.5%) (2, 3).The patient was given etidronate disodium (200 mg dailyfor 14 days every 12 weeks). Osteoarthralgia gradually re-solved, and Al-P decreased to 220 mg/dl and BGP to 24.0ng/ml. However, s-Cr had increased further to 12.6 mg/dl, byJuly 2002.
Discussion
Vanherweghemet al first reported Chinese herb nephro-pathy occurring in Belgium in 1993 (1). One year later,Vanhaelen et al reported that in Belgium, the number of
known cases of Chinese herb nephropathy had risen to 70(4). Subsequently, renal damage from Chinese herbs hasbeen recognized in manycountries. Renal biopsy specimensin these cases showed extensive tubulo-interstitial fibrosiswithout glomerular lesions.
In 1993, Izumotani (5) first reported a similar case in
Japan, followed by manyother Japanese reports of Chineseherb nephropathy. Characteristically many Japanese caseshave been complicated by Fanconi syndrome.Extra-renal disease caused by Chinese herbs has includedpneumonitis associated with Ougon and Ouren-gedoku-to(6); hepatitis with Jin Bu Huan (7); meningoencephalocelewith Tripterygium wilfordii (8); cardiotoxicity with Aconi-tum rootstocks (9); valvular heart disease with Stephaniatetrandra and others (10); aplastic anemia (ll); pulmonaryembolism; thromboembolism (12); and urothelial cancer(13). Although Chinese herbs have been linked to disease inmanyorgans, no report has suggested a relationship betweenChinese herbs and bone disease.Renal disease is well knownto cause bone disease, and arelationship has been reported between Fanconi syndrome
and osteomalacia (14). Renal osteodystrophy, which occursin chronic renal failure, is encountered frequently. Lesions
are classified into osteitis fibrosa, representing high-turnoverbone disease; and osteomalacia and aplastic bone disease,representing low-turnover bone disease. Osteitis fibrosa re-sults from excess in secretion of parathyroid hormone(PTH); characteristics include increased surface resorption
caused by hyperactivity of both osteoblasts and osteoclasts,as well as endosteal fibrosis. Osteomalacia, in which alumi-num toxicity is the most commoncause, is a condition show-ing excessive unmineralized lamellar osteoid. In mixed-typerenal osteodystrophy the characteristics of both osteitisfibrosa and osteomalacia coexist symmetrically in the samepatient. Asymmetric mixed-type renal osteodystrophy hasnot been reported.Paget's disease of bone, well known as a localized bonedisease showing osteitis fibrosa, is descriptively termedosteitis deformans (15) and affects approximately 3% ofCaucasians over the age of 40 years old in Western countries
348 Internal Medicine Vol. 42, No. 4 (April 2003)

Chinese Herbs and Bone Disease
A B
c D
Figure 5. (A) Light microscopic examination showed increased bone resorption and fibrous tissue adjacent tothe trabecular bone, and excessive unmineralized lamellar osteoid (Villanueva reagent staining; xlOO). (B)
Osteoclasts with more than 50 nuclei were seen (Villanueva reagent staining; x200). (C) Polarizing microscopicexamination showed normal lamellar bone and woven bone without mosaic pattern of cement lines (xlOO). (D)Fluorescence microscopic examination showed singly labeled surface as well as doubly labeled surface (xlOO).
(16). In Japan, Paget's disease is rare. Although the cause ofthis disease is unknown,somereports have suggested thatvarious paramyxoviruses including the measles virus mighthave roles in initiation (17). However, Paget's disease has
not been reported as an adverse reaction to drugs. Nonehavesuggested a relationship to Chinese herbs. Histologically, thecharacteristic feature is increased resorption of bone accom-panied by an increase in bone formation, followed by re-placement of marrow by fibrous tissue. In the sclerotic
phase, an increase in the numberof irregular cement lines isobserved as a "mosaic" pattern. Radiologically, the bone en-larges to show an irregularly widenedcortex in a coarse, stri-ated pattern, with lesions occurring in a focal distribution.The present case showeddistinctive characteristics com-pared with osteitis fibrosa in renal osteodystrophy and withPaget's disease. Bone scintigraphy revealed asymmetrical
bone disease. Neither radiography nor computed tomographyshowed osteosclerosis with hypertrophy. Histologically, thiscase showed mixed findings including both osteomalacia andosteitis fibrosa. A mosaic pattern of cement lines, character-istic of Paget's disease, was not seen. This case, then, was
incompatible with Paget' s disease, while its asymmetry dif-fered from classic mixed-type renal osteodystrophy as seenin uremia. Other asymmetric bone disease, for exampleprostatic carcinoma and bone fracture due to prednisolonewere excluded radiographically and histologically. At least
in part, this case is likely to be a new bone disease distinctfrom presently established categories.
Aristolochic acid (AA), a constituent of Chinese herbs,
has been considered one possible cause (18-21). This suspi-cion was strengthened by the discovery of AA-DNAadductsin the kidney tissue of affected patients (22, 23). The recentdemonstration that, in rabbits, AAalone causes similar renallesions removes any doubt on the causal role of AA(24).Here, in the clinical course, the serum Al-P concentrationbecame elevated twice, irrespective of prednisolone orcalcitriol. The first elevation may relate to osteomalacia
caused by Fanconi syndrome, because it was decreased afterthe treatment of Fanconi syndrome. But the cause of the sec-ond elevation can't be explained only by chronic renal fail-ure because of the asymmetric radiological findings. On theother hand, Chinese herb-induced nephropathy can result in
Internal Medicine Vol. 42, No. 4 (April 2003) 349

HOSHINOet al
gradual clinical deterioration even after discontinuation ofherbs. For these reasons, the Chinese herbs may conceivablyhave caused osteopathy either directly, indirectly throughrenal disease, or both. Accumulation of more cases and fur-ther clinical investigation of Chinese herb users should bepursued.
Steroids and other immunosuppressant therapy have beenreported to have a slight beneficial effect in this nephropathy(25). In the present case, steroid administration was not con-sistently effective against either bone disease ornephropathy. In contrast, etidronate disodium showed a cleareffect against bone disease; Al-P decreased and bone painabated. This modality may be an important therapeutic op-tion in this kind of bone disease.
Acknowledgement:Histomorphometricanalysis of bone tissue wasper-formed by Dr. Hideaki Takahashi and Mrs. Akemi Itou at the Niigata BoneScience Institute, Niigata, Japan.
References
1) Vanherweghem JL, Depierreux M, Tielemans C, et al. Rapidly progres-sive interstitial renal fibrosis in young women:association with slim-
ming regimen including Chinese herbs. Lancet 341: 387-391, 1993(see comments).
2) Coburn JW. Renal osteodystrophy. Kidney Int. 17: 677-693, 1980.3) Sherrard DJ, Hercz G, Pei Y, et al. The spectrum of bone disease inend-stage renal failure-An evolving disorder. Kidney Int 43: 436-442,
1993.
4) Vanhaelen M, Vanhaelen-Fastre R, But P, Vanherweghem JL.
Identification of aristolochic acid in Chinese herbs. Lancet 343: 174,1994 (letter).
5) Izumotani T, Ishimura E, Tsumura K, Goto K, Nishizawa Y, Morii H.An adult case of Fanconi syndrome due to a mixture of Chinese crudedrugs. Nephron 65: 137-140, 1993.
6) Nishimori F, Yamazaki K, Jin Y, et al. Pneumonitis induced by thedrug Ougon. Nihon-Kokyuki-Gakkai-Zasshi 37: 396-400, 1999.
7) Picciotto A, Campo N, Brizzolara R, et al. Chronic hepatitis induced byJin Bu Huan. J Hepatol 28: 165-167, 1998.
8) Takei A, Nagashima G, Suzuki R, et al. Meningoencephalocele associ-ated with Tripterygium wilfordii treatment. Pediatr Neurosurg Jul 27:
45-48, 1997.
9) Tai YT, But PP, Young K, Lau CP. Cardiotoxicity after accidentalherb-induced aconite poisoning. Lancet 340: 1254-1256, 1992 (see
comments).
10) Vanherweghem JL. Association of valvular heart disease with chinese-herb nephropathy. Lancet 350: 1858, 1997.
ll) Nelson L, Shih R, Hoffman R. Aplastic anemia induced by anadulterted herbal medication. J Toxicol Clin Toxicol 33: 467-470,1995.
12) Gorey JD, Wahlqvist /ML, Boyce NW.Adverse reaction to a Chineseherbal remedy. Med J Aust 157: 484-486, 1992.
13) Cosyns JP, Jadoul M, Squifflet JP, Van Cangh PJ, van Ypersele deStrihou C. Urothelial malignancy in nephropathy due to Chinese herbs.
Lancet 344: 188, 1994 (letter).
14) Clarke BL, Wynne AG, Wilson DM. Osteomalacia associated withadult Fanconi's syndrome: clinical and diagnostic features. ClinEndocrinol (Oxf) Oct 43: 479-490, 1995.
15) Paget J. On a form of chronic inflammation of bones (osteitis de-formans). Med Chir Trans 60: 37-63, 1877.
16) Barker DJP. Paget's disease of bone: the Lancashire focus. Br Med J280: 1105-1107, 1980.
17) Kurihara N, Reddy SV, Menaa C, Anderson D, Roodman GD.
Osteoclasts expressing the measles virus nucleocapsid gene display apagetic phenotype. J Clin Invest 105: 607-614, 2000.18) But PPH. Need for correct identification of herbs in herbal poisoning.
Lancet 341: 637, 1993 (letter; see comments).19) Depierreux M, Van Damme B, Nanden HK, Vanherweghem JL.
Pathologic aspects of a newly described nephropathy related to the pro-longed use of Chinese herbs. Am J Kidney Dis 24: 172-180, 1994.
20) Jadoul M, de Plaen JF, Cosyns JP, van Ypersele de Strihou C. Adverseeffects from traditional Chinese medicine. Lancet 341: 892-893, 1993
(letter; comment).21) Cosyns JP, Jadoul M, Squifflet JP, Plaen JF, Ferluga D, van Yperselede Strihou C. Chinese herbs nephropathy: A clue to Balkan endemicnephropathy? Kidney Int 45: 1680-1688, 1994.
22) Schmeiser HH, Bieler CA, Wiessler M, van Ypersele de Strihou C,Cosyns JP. Detection of DNAadducts formed by aristolochic acid inrenal tissue from patients with Chinese herbs nephropathy. Cancer Res
56: 2025-2028, 1996.
23) Bieler CA, Stiborova M, Wiessler M, Cosyns JP, van Ypersele deStrihou C, Schmeiser HH. 32P-post labelling analysis of DNAadductsformed by aristolochic acid in tissues from patients with Chinese herbs
nephropathy. Carcinogenesis 18: 1063-1067, 1997.
24) Cosyns JP, Dehoux JP, Guiot Y, et al. Chronic aristolochic acid toxic-ity in rabbits: A model of Chinese herbs nephropathy? Kidney Int 59:2164-2173, 2001.
25) Vanherweghem JL, Abramowicz D, Tielemans C, Depierreux M.
Effects of steroids on the progression of renal failure in chronic intersti-tial renal fibrosis: a pilot study in Chinese herbs nephropathy. AmJKidney Dis 27: 209-215, 1996.
350 Internal Medicine Vol. 42, No. 4 (April 2003)