Embed Size (px)
Citation preview

Chronic Kidney Disease
and
Its Complications
ภญ.อษณย วนรรฆมณ
คณะเภสชศาสตร มหาวทยาลยสงขลานครนทร
Outline
• Introduction • Staging of CKD and clinical plan• Complications from renal impairment
and managements• Renal replacement therapy (RRT)• Case study• Rx role • Conclusion
Chronic Renal Failure (CRF)
Chronic Kidney Disease CKD
4
Definition of CKD
National Kidney Foundation 2001:
• Evidence of kidney damage (structural
damage) for at least 3 months
- pathologic abnormalities
- markers of damage, e.g. abnormalities
in blood or urine tests or imaging studiesor
• GFR < 60 ml/min/1.73m2 for at least 3 months

Persistent albuminuria categories A1 A2 A3 Normal to
mildly increased
Moderately increased
Severely increased
< 30 มก./กรม < 3 มก./มลลโมล
30-300 มก./กรม 3-30 มก./มลลโมล
> 300 มก./กรม > 30 มก./มลลโมล
GFR
cate
gorie
s (ม
ล./
นาท/
1.73
ตรม.
)
G1 Normal or high > 90 G2 Mildly decreased 60-89 G3a Mildly to moderate decreased 45-59 G3b Moderately to severely decreased 30-44 G4 Severely decreased 15-29 G5 Kidney failure < 15
หนาท� 202
การแบงระยะโรคไตเรGอรงตามระดบ GFR และแผนการจดการ
ระยะของ CKD
GFR (มล./
นาท/1.73 ตรม.)
แผนการจดการ
G1* > 90
• วนจฉยและรกษาท<สาเหตของการเกด CKD • ประเมนปจจยเส<ยงของ CKD • ควบคมปจจยเส<ยงของ CKD เพ<อชะลอการ
ดาเนนโรค • ควบคมปจจยเส<ยงตอการเกดโรคหวใจและ
หลอดเลอด • รกษาโรครวมท<ม
G2* 60-89เพVมเตมจากระยะ G1*
• ประมาณการอตราการเส<อมของไต
G3a 45-59เพVมเตมจากระยะ G2* • ปรบขนาดยาตามหนาท<การทางานของไต
การแบงระยะโรคไตเรGอรงตามระดบ GFR และแผนการจดการ
ระยะของ CKD
GFR (มล./นาท/1.73
ตรม.) แผนการจดการ
G3b 30-44
เพVมเตมจากระยะ G3a ประเมนและรกษาภาวะแทรกซอนจากภาวะไตบกพรอง
G4 15-29
เพVมเตมจากระยะ G3bเตรยมการบาบดเพ<อทดแทนหนาท<การทางานของไต
G5 < 15
• เร<มการบาบดเพ<อทดแทนหนาท<การทางานของไต
• ปรบขนาดยาตามหนาท<การทางานของไต• ประเมนและรกษาภาวะแทรกซอนจากภาวะ
ไตบกพรอง• รกษาโรครวมท<ม

ลกษณะอาการและอาการแสดงทางคลนก
• อาจไมมอาการจนกระท<งเขาสโรคไตเรLอรงระยะทายๆ• ความผดปกตสามารถเกดขLนไดกบหลายระบบ
: สมดลนLา สมดลกรด-ดาง สมดลเกลอแร ระบบตอม ไรทอ ระบบประสาท ระบบหวใจและหลอดเลอด ระบบผวหนง ระบบเลอด ระบบทางเดนอาหาร รวมท Lงระบบภมคมกน • อาจไมจาเพาะเจาะจง: อาการปวดศรษะ นอนไมหลบ
อาการชก ไมมประจาเดอน มตะครว สะอก • ตารางท< 3 หนา 207
การวนจฉย หนา 208-209
1. การสมภาษณประวตและผลการตรวจรางกาย
2. การตรวจทางหองปฏบตการ
3. ภาพถายทางรงส
4. Renal biopsy
การชะลอการเสVอมของไต หนา 209-211
1. การลดการร<วของโปรตนในปสสาวะโดยการใช ยาท<มฤทธ_ยบย Lง RAAS
2. ควบคมระดบนLาตาลในผปวยโรคเบาหวาน
3. ปองกนไมใหเกดภาวะไตวายเฉยบพลนรวมดวย
4. การควบคมอาหารโปรตน
5. การปรบเปล<ยนพฤตกรรม (Lifestyle modification)
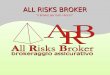
Confusion, Insomnia, Depression
CVD
AnemiaHyperpigment, Pruritus
Bone disease
Infertile, loss of libido
N/V, Anorexia
Polyneuropathy
Acid/base, E’lyte, Fluid-imbalance

Complications from renal impairment
CKD stage 1
CKD stage 2
CKD stage 3
CKD stage 4
CKD stage 5
Cardiovascular disease (CVD)
CVD, Bone Dz, Anemia
CVD, Bone Dz, Anemia
Acid/base,
E’lyte, Fluid-imbalance
ภาวะแทรกซอนจากโรคไตเรGอรง และการรกษา หนา 211
1. ความผดปกตของระบบเลอด 2. ความผดปกตของสมดลแคลเซยม ฟอสเฟต
และกระดก 3. ความผดปกตของระบบหวใจและหลอดเลอด 4. Metabolic acidosis
15
� The primary cause: insufficient production of
erythropoietin (EPO)
� Generally, normochromic, normocytic anemia
� Other causes, Iron def, chronic inflammation ,
malnutrition, severe hyperparathyroidism
Anemia ���� fatigue, dyspnea, difficulty concentrating, decreased cognition, dizziness, cold intolerance, left ventricular hypertrophy
(LVH)
Anemia in CKD
16
Pathophysiology of LVH in CKD
Hypertension Concentric LVH
CKD ↑↑↑↑ Plasma volume
Eccentric LVH
Anemia↓↓↓↓ Erythropoietin
production
LVH

17
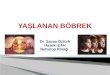
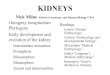
Baseline prevalence of LVH versus
renal function
Levin et al AJKD 1999
Morbidity/mortality
LVH
50
40
30
20
10
0
p<0.001,CrCl <25 ml/minvs all others
CrCl ml/min >50 35–49 25–34 <25Hb, g/dL 14.1 13.2 12.5 11.4
*
% of patients with LVH
18
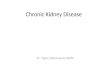
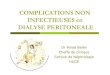
Cumulative Survival in Patients with Normal and Abnormal LV at Start of
Dialysis
Parfrey et al.Nephrol Dial Transplant 1996; 11: 1277–1285.
Normal
ConcentricLVH
0000 6666 12121212 18181818 24242424 30303030 36363636 42424242 48484848 54545454 60606060 66666666 72727272
1111
0.90.90.90.9
0.80.80.80.8
0.70.70.70.7
0.60.60.60.6
0.50.50.50.5
0.40.40.40.4
0.30.30.30.3
0.20.20.20.2
0.10.10.10.1
0000
LVdilatation
Systolic dysfunction
19
� Erythropoiesis stimulating agent (ESA)
� Iron therapy
� Correct other causes: ตารางทV 211 � Blood loss
� Malnutrition
� Inflammation
� Deficiencies of folate, vitamin B12
Management of Anemia in CKD:

21
Prim Care Clin Office Pract 2008;35:329 – 44. Semin Nephrol 2006; 26:313-8.
Continuous Erythropoietin Receptor Activator
Erythropoiesis stimulating agents: ESAs
22
• เร<มใหในผปวยท<มระดบ Hgb นอยกวา 10
กรม/ดล.
• มกเร<มใชในขนาด 20-50 IU ตอนLาหนก 1
กก. ให 2-3 คร Lงตอสปดาห (EPO-alfa
หรอ EPO-beta)
• IV หรอ SC
การบรหารยา erythropoietin
23
K/DOQI (2007)
HD and ND pts., on ESA:
11 – 12
�Not more than 13
ERBP (2008)11 – 12
�Not more than 13
CSN (2008)
Target = 11, Range 10 – 12
�Not more than 12, esp. in the pts who
have higher risks for CVD
UK Renal Assoc. (2007) 10.5 – 12.5
K/DOQI (2012) 10.0-11.5
Target Hemoglobin (g/dL):
ESA dose > 500 IU/กก./สปดาห
แตยงไมสามารถทาใหระดบ Hgb
มากกวา 11.0 กรม/ดล.หรอเขาส
คาเปาหมายได บงบอกวามการ
ตอบสนองตอ ESA ต<า

25
Adverse Effects of ESAs:
� Flu like symptom (first use)
� higher blood pressure
� Increased risk of cardiovascular events;
heart attack, HF, blood clots, stroke and
death.
� Pure red cell aplasia (PRCA)
� Seizure
Kidney International 2008;74(Suppl 110):S12–S18.26
ประเดนทVตองคานงถงในการใชยา ESAs:
� การเกบยา
� การควบคมความดนโลหตเพ<อใหไดรบ
การฉดยาสม<าเสมอ
27
K/DOQI
(2006)
ND-CKD & PD:
� Serum ferritin 100-500 ng/mL
� TSAT (SI/TIBC) > 20%
HD-CKD:
� Serum ferrition 200-500 ng/mL
� TSAT > 20%
KDIGO
(2012)
สามารถให IV iron หากม ferritin นอยกวา 500 นาโนกรม/มล. และ TSAT นอยกวา 25 % เพVอใหสามารถลดขนาด ESA ลงได
Iron target:
AJKD; 47(Suppl 3):S1-S146Kidney Int 2012; 2(4): 279-335 28
IV iron-Different properties
Composition
Molecular size
Degradation Kinetics (rate of iron dissociation from
the complex)
Side effect profiles
anaphylaxis, anaphylactoid (iron dextran)
���� Test dose (25 mg IV infusion)

29 30
Comparison of intravenous iron products
Products
Properties
Iron Dextran SFGC
Iron Sucrose
Molecular size(Kilodaltons)
Low MW ~ 96High MW ~ 267
~ 38 ~ 43
rate of iron dissociation from the complex
slow rapid intermediate
Bloodstream t 1/2
(hr)40-60 1 6
Modified from Yee and Besarb AJKD 2002; vol 40 (6): 1111-1121
and P&T News September/October 2001 Virtual Hospital
31
ระดบ Hgb• ทกเดอน: ในระหวางเร<มตนการรกษาดวย ESA
(CKD ทกระยะ)• ทกเดอน: ในระยะ maintenance phase ของการใช
ESA (CKD ระยะท< 5 ท<ไดรบการฟอกเลอด)• ทก 3 เดอน: ในระยะ maintenance phase ของการใช
ESA (โรคไตเรLอรงท<ยงไมไดรบการฟอกเลอด)Iron status
• ตดตามทก 3 เดอน • ตดตามบอยขLนหากมการเพ<มขนาด ESA มการสญเสย
เลอดเกดขLน หรอสงสยวาอาจมภาวะเหลกท<เกนคาเปาหมายท<แนะนาไว
การตดตามผลการรกษา
32
Bone metabolism (calcium, phosphate, PTH)
• พบไดต Lงแต CKD ระยะท< 3 (G3a และ G3b) เปนตนไป
• ไตทางานลดลงจนมการค<งของฟอสเฟตในรางกาย และ
calcitriol มระดบลดลง
• ภาวะ hyperphosphatemia และ hypocalcemia �
secondary hyperparathyroidism � เพ<ม bone
turnover � กระดกมลกษณะ osteitis fibrosa cystica

33
-Calcification-CVD / PVD-nervous system-immunologic-cutaneous
osteitis fibrosa cystica
35
Calcification
36
Mitral Valve Calcification in a Dialysis Patient
Scan courtesy of P. Raggi.

37
Arterial calcification increases mortality risk
Hypertension 2001;38:938–42.
การปองกน
• ไมสามารถแกไขปญหา calcification ท<
เกดขLนแลว
• ปองกนทาไดโดยการจากดอาหารท<ม
ฟอสเฟตสงรวมกบการใชยาจบฟอสเฟตใน
ทางเดนอาหาร
39
Dietary phosphorus 800 - 1,000 mg/day
� อาหารประเภทถ �วทกชนด ท �งชนดแปรรป และ ไมแปรรป เชน ถ �วลสง ถ �ว เขยว ถ �วแดง ถ �วเหลอง เมลดอลมอนด เมลดมะมวงหมพานต เมลดฟกทอง เมลดแตงโม เมลดทานตะวน เปนตน
� สตวท �รบประทานท �งเปลอก หรอกระดก เชน ปลา ซารดนกระปอง กงแหง ปลากรอบ กะป เปนตน
� อาหารท �มสวนผสมของนม และผลตภณฑจากนม เชน นมผง ขนมเคก ขนมปงบสกท ขนมปงกรอบ
� ขนมและเคร �องด �มตางๆ เชน ขนมท�ผสมไขแดง ธญพชท�ไมไดขดส ชอกโกแลต โกโก กาแฟ เปนตน
สารโพลฟอสเฟต: โซเดยมไตรฟอสเฟต ไตรโซเดยมฟอสเฟตลดการสญเสยนLาหนกจากขณะท<เปนนLาแขง นLาจะถกเปล<ยนโครงสรางเกดผลกซ<งมความคม และเนLอเย<อมการหดตว

ยาจบฟอสเฟตในอดมคต
• จบกบฟอสเฟตไดอยางรวดเรว • ดดซมเขากระแสโลหตไดนอยหรอไมดดซม • ไมเปนพษตอรางกาย • มหลกฐานทางคลนกรบรองวาม
ประสทธภาพในการลดระดบฟอสเฟตในเลอด
• ลดระดบฮอรโมนพาราไทรอยด (PTH) • รบประทานงาย
กลมยา ขอด ขอดอย
Aluminium-based phosphate binderAluminiumhydroxide
• จบกบฟอสเฟตไดสง (ใน pH ทกระดบ) • ราคาไมแพง
• มรายงานการเกดพษจากการทVมการเกบสะสมในอวยวะตางๆ ของรางกายเชน กระดก สมอง เปนตน
Calcium-based phosphate binderCalcium acetate • จบกบฟอสเฟตไดด
ใน pH ทกระดบ • ทาใหเกดอาการคลVนไส
อาเจยนไดสง • เกดภาวะ
hypercalcemia
Calciumcarbonate
• ราคาไมแพง • จบกบฟอสเฟตไดดท VpH ตVา ๆ
• เกดภาวะ hypercalcemia
กลมยา ขอด ขอดอย
Aluminium- and calcium-free phosphate binders
Sevelamerhydrochloride
Sevelamercarbonate
• สามารถลดไขมน total cholesterol และ LDL cholesterolได
• ราคาแพง• ความสามารถในการจบ
ฟอสเฟตไมสงทาใหตองรบประทานยาในขนาดทVสง
• มรายงานการเกด metabolic acidosis จาก sevelamerhydrochloride
Lanthanum carbonate
• มความสามารถในการจบกบฟอสเฟตไดสง
• จบกบฟอสเฟตไดดใน pH ทกระดบ
• ราคาแพง
Sevelamer HCL � Sevelamer carbonate

ภาวะผปวย ยาจบฟอสเฟต
CKD ระยะ 3 หรอ 4 Calcium-based phosphate binderCKD ระยะ 5
• ระดบแคลเซยมในเลอดนอยกวา 10.2 มก./ดล.
Calcium-based phosphate binderหรอ non-calcium, non-aluminiumbased phosphate binderหรอใช รวมกน
• ระดบแคลเซยมในเลอด มากกวา 10.2 มก./ดล. และ PTH นอยกวา 150 พโค กรม./มล. 2 คร Lง ตดตอกน
หลกเล<ยงการใช calcium-based phosphate binder
ภาวะผปวย ยาจบฟอสเฟต
• ม severe vascular calcification และ/หรอ soft tissue calcification
หลกเล<ยงการใช calcium-based phosphate binder
• ระดบฟอสเฟตในเลอดมากกวา 7.0 มก./ดล.
Aluminium-based phosphate binder ใชในระยะส Lน (ไมเกน 4 สปดาห)
noncalcium, nonaluminium based phosphate binder
วธการรบประทานวธการรบประทานวธการรบประทานวธการรบประทาน
- เคยวพรอมอาหาร ยกเวน sevelamer, capsule
ชนดและขนาดยาทใชชนดและขนาดยาทใชชนดและขนาดยาทใชชนดและขนาดยาทใช ปรบตามขนาด และชนดของ
อาหาร
ขอควรระวงขอควรระวงขอควรระวงขอควรระวง
drug interaction, Mg-containing antacid
Adverse effectAdverse effectAdverse effectAdverse effect
constipation, hypercalcemia, hypophosphatemia
Hyperparathyroidism (iPTH > 300 pg/mL)
1. Correct calcium and phosphate levelCorrect calcium and phosphate levelCorrect calcium and phosphate levelCorrect calcium and phosphate level2. Vitamin D or vitamin D analogue Vitamin D or vitamin D analogue Vitamin D or vitamin D analogue Vitamin D or vitamin D analogue
- 1,25-α-dihydroxyvitamin D3 (Calcitriol) - vitamin D analogue: 1-α-hydroxyvitamin D3
(alfacalcidol)- direct and indirect effect - PulsePulsePulsePulse or daily - ขนาดยาปรบขนกบระดบ iPTH- Adverse effect: hypercalcemia, hyperphosphatemia

49
Bone Metabolism Disorder
Managements
2003 2009
ระยะของ โรคไตเรGอรง
คาเปาหมายของระดบ
ฟอสเฟตในเลอด
(มก./ดล.)
คาเปาหมายของระดบแคลเซยมในเลอด*(มก./ดล.)
คาเปาหมายของผลคณระหวางระดบแคลเซยมและฟอสเฟต(มก.2/ดล.2)
คาเปาหมายของระดบฮอรโมนพาราไทรอยด
(พโคกรม/มล.)
K/DOQI
CKD ระยะท< 3 2.7 – 4.6 8.4–10.2 - 35 - 70
CKD ระยะท< 4 - 70 – 110
CKD ระยะท< 5/dialysis
3.5 – 5.5 8.4 – 9.5 < 55 150 – 300
KDIGO
CKD G5/G5D Normal range Normal range
- 150 – 600
51American Journal of Kidney Diseases 2003;42(4):S12-S28.
Management of hyperparathyroidism:

53
Conclusion: Alfacalcidol can be used to control
secondary hyperparathyroidism at doses of 1.5–
2.0 times that of calcitriol.
The two drugs are equally efficacious and lead to
similar changes in calcium and phosphorus.Nephrology 16 (2011) 277–284
Treatment of severe hyperparathyroidism
• Percutaneous Ethanol Injection (PEI)
• Parathyroidectomy
in patients with severe hyperparathyroidism
(persistent serum levels of intact PTH >800 pg/mL
with hypercalcemia and/or hyperphosphatemia that
are refractory to medical therapy
Parathyroidectomy
• HUNGRY bone disease
(bone absorption � hypocalcemia, hypophosphatemia
and hypomagnesemia)
Monitor calcium level every 4 to 6 hrs for the first 48 to 72 hrs after surgery, and then twice daily until stable.
IV calcium if severe hypocalcemia
Calcimimetics:
� Cinacalcet (Regpara®) บรษทเคยววะ ฮคโค ครน
• Increase sensitivity of calcium sensing receptors
(CaSR) on the surface of parathyroid gland to
calcium.
• decrease PTH, Calcium and Phosphate.
• US-FDA approved for the treatment of 2º hyperparathyroidism in HD patients.
Management of hyperparathyroidism:

57
Morbidity and Mortality Along the Renal
Continuum
DiabetesWith
normoalbuminuria
EndothelialDysfunction
Micro-albuminuria
Macro-proteinuria
NephroticProteinuria
End-Stage Renal Disease
CVD
Death
ความผดปกตของระบบหวใจและหลอดเลอด
Circulation 2007; 116;85-97
ตารางทV 10 Traditional risk factors และ CKD-related risk factors หนาท< 220
CKD-related risk factors “Nontraditional” CVD risk factors • ไตมอตราการกรองลดลง• มโปรตนร Vวในปสสาวะ• มการกระตนระบบ rennin-angiotensin
aldosterone system มากขGน• มภาวะน Gาเกนในรางกาย• การเสยสมดลของแคลเซยมและฟอสเฟตในรางกาย• ภาวะโลหตจาง• ภาวะทพโภชนาการ• Uremic toxins 60

Modifiable risk factor
61
Hypertension
• “nondipping phenomenon” – need long acting Anti-HTN at night
• Target BP: < 140/90 mmHg (age < 60 yrs)• Prefer ACEI, ARB (avoid combined use of
ACEI and ARB)– Requires potassium and Scr monitoring
• Need BP home monitoring
JAMA Published online December 18, 2013, p E1-14.AJKD 2005; 45 (SUPPL 3): S1-128.
Lipid abnormalities found in CKD
Semin Nephrol. 2009 ;29(6):610-20.
Dyslipdemia
• CKD exhibit a unique CVD pathology,
characterized by vascular stiffness and calcification,
structural heart disease, and sympathetic nervous
system overactivity
• pathophysiology of CV events in this patient group
is not always related to atherothrombotic plaque
rupture

Ann Intern Med 2012; 157(4): 263-275
Metabolic acidosis
66Pediatr Nephrol (2011) 26:19–28
67
Exacerbation or Development
of Cardiac Disease:
Clinical Consequences of Metabolic Acidosis:
A retrospective analysis of laboratory
data obtained from more than 12,000
HD pts showed an increased risk for
death when plasma bicarbonate
concentration was less than 15 to 17
mEq/L (mmol/L).
Am J Kidney Dis 2005;45:978-993.68
Am J Kidney Dis 2004;44:661-671.
Association of midweek predialysis serum
bicarbonate level and mortality

ประเภทของ RRT
• Hemodialysis
• Peritoneal dialysis
• Kidney transplantation
69 70
Renal replacement therapy (RRT)
HD PD
KT
การเตรยมความพรอมของผปวยและญาตกอน
RRT โดยแพทยหรอพยาบาลผประสานงาน
• KDOQI แนะนาใหเตรยมต Lงแต CKD stage IV
• แนะนาขอด ขอดอยของ RRT แตละวธ
• เตรยม vascular access สาหรบการฟอกเลอด
• ใหความร ความเขาใจและทศนคตท<ถกตองตอ
RRT 71
การเตรยมความพรอมของผปวยและญาตกอน RRT (ตอ)
• การประเมนความพรอมทางดานครอบครว
เศรษฐานะ และการเบกจายคารกษา
• การรกษาโรครวม
72

ปจจยทVเกVยวของกบการตดสนใจเลอก RRT
• Residual renal function
• Dialysis access: vascular access, สภาพผนง
หนาทอง
• ระยะทางในการเดนทางไป dialysis center
• Comorbidity/underlying disease: CVD, DM
• คณภาพชวต
73
ปจจยทVเกVยวของกบการตดสนใจเลอก RRT
• คาใชจาย
• ความสามารถของ Patient/caregiver: PD ผปวย
และญาตตองมความสามารถในการเรยนรท<ด ม
ความสะอาด ละเอยด
• ระบบบรการสาธารณสขในภมลาเนา
• Preference ของผปวยหรอผดแล
74
Hemodialysis
• ขอด
• ผปวยและญาตไมตองทาเอง
• การฟอกเลอดแตละคร Lงใชเวลาไมมาก
• สามารถแกไขภาวะแทรกซอนท<เกดจากการท<ของ
เสยค<ง ภาวะเกลอแรผดปกต หรอ pulmonary
edema ไดอยางรวดเรว75
ขอเสย• ตองมารพ.หรอศนยไตเทยมบอยๆ อาทตยละ 2-3 คร Lง ไม
เหมาะสาหรบผปวยท<มท<อยหางไกลหรอไมสะดวก
• ไมไดมการขจดของเสยอยตลอดเวลาอยางการรกษาทางชองทอง
• ในผสงอาย หรอในโรคเบาหวานท<มปญหาเร<องของหลอดเลอด ไมสามารถทาหลอดเลอดสาหรบการฟอกเลอดได
• ผปวยท<มปญหาเร<องโรคหวใจ และหลอดเลอดท<รนแรง การฟอกเลอดดวยเคร<องไตเทยมอาจจะทาใหสญญาณชพไมคงท< (hemodynamic instability) และ มความดนโลหตต<าขณะฟอกเลอดได
76

77
Peritoneal dialysisขอด
• มการขจดของเสยตลอดเวลา
• ไมมการเปล<ยนแปลงของสญญาณชพท<รนแรงและรวดเรว
• ชวยชะลอการสญเสย residual renal function ได ดกวา
• ผปวยและญาตสามารถทาเองไดท<บาน และไมตองมาโรงพยาบาลบอย ผปวยสามารถทางานไดตามปกต
• ในกรณเกดภยพบต มความคลองตวมากกวา 78
PD
ขอเสย
• หากไมระมดระวงความสะอาดใหดจะเกดการตดเชLอ
ไดงาย
• ผปวยท<มความผดปกตของผนงหนาทองท<ไม
สามารถแกไขได จะไมสามารถลางไตทางชองทอง
ได
79
PDAnatomy of Renal Transplantation

Contraindications• Recent or metastatic malignancy
• Active infection, AIDS
• Severe extrarenal disease (cardiac, pulmonary, hepatic)
• Active vasculitis or glomeulonephritis
• Uncorrectable lower urinary tract disease.
• Noncompliance
• Psychiatric illness including alcoholism and drug addiction
• Morbid obesity
• Age > 70 years
• Persistent coagulation disorder
กรณศกษา• ผปวยหญงไทยคอาย 34 ป (สวนสง 160 ซม. นLาหนก 48
กก.) อาชพแมบาน • PMH: • Chronic kidney disease x 10 ป คาดวาสาเหตมาจาก
glomerular disease และการตดเชLอในทางเดนปสสาวะแบบซLา ๆ
• ไดรบการฟอกเลอดดวยเคร<องไตเทยม 2 คร Lงตอสปดาห x 10 ป
• มกราคม 2556: aortic regurgitation with infective endocarditis
• ตลาคม 2556: parathyroidectomy with autotransplant ท<ตนขาดานขวา
• ไมรบประทานยาตามท<แพทยแนะนา มกหยดใชยาเองบอย ๆ • FH: ไมมคนในครอบครวเปนโรคไต• SH: ปฏเสธการสบบหร<หรอด<มแอลกอฮอล
ผลการตรวจ (คาปกต)
เดอนม.ค. ก.พ. ม.ค. เม.ย. พ.ค. ม.ย. ก.ค. ส.ค. ก.ย. ต.ค. พ.ย. ธ.
ค.Hgb (10-12 g/dL)
7.4 8.8 8.9 8.8 7.9 7.5 6.9 8.4 8.6 9.6 10.4 11.1
Ferritin (200-500 ng/mL)
424 450
% TSAT (20-50%)
22.6 25.4
Potassium (3.5-5.0 mEq/L)
5.73 6.58 5.41 5.75 4.34 4.59 4.61 5.02 4.88 5.57 4.17 4.14
HCO3
(22-29 mEq/L)21 23 24 21 24 23 21 21.5 22.2 22.4 21.5 22
.5Calcium (8.5-10.5 mg/dL)
8.2 8.6 8.1 9.1 8.9 8.9 9.5 7.8 8.3 6.2 7.5 9.3
Phosphate (2.5-4.5 mg/dL)
6.2 9 6.5 6.2 4.3 4.4 5.6 10.1 12.5 2.5 4.4 4.6
Albumin (3.5-5.5 g/dL)
3.9 4.1 4.1 4.1 3.9 4.1 3.8 3.9 4.0 3.8 4.2 4.1
PTH(< 300 pg/mL)
1278 1574 1529 2140 256 (หลงผาตด)
Q1. ผปวยรายนGจดเปนผปวยโรคไตเรGอรงระยะใด มเปาหมายใน การรกษาอยางไร
• CKD G5D คอ kidney failure ท<ไดรบการฟอกเลอดแลว
• เปาหมายในการรกษา: ใหผปวยไดรบการรกษาบาบดเพ<อทดแทนหนาท<การทางานของไตดวยการฟอกเลอดดวยเคร<องไตเทยมไดอยางเพยงพอ และแกไขภาวะแทรกซอนท<เกดขLนจากหนาท<การทางานของไตบกพรอง และสรางความเขาใจและทศนคตท<ดถงการใชยาและปฏบตตวตามท<บคลากรทางการแพทยให คาแนะนา

Q2. ภาวะแทรกซอนทVเกดขGนในผปวยรายนGม อะไรบาง และจะกระทบตอรางกายของผปวยอยางไร
• 2 /3 hyperparathyroidism• Anemia
Q3. ภาวะแทรกซอนทVเกดข Gนควรไดรบการแกไขดวยยาอยางไร
• 3 hyperparathyroidism“Hungry bone syndrome” หลงการผาตด parathyroid gland
• Anemia Hgb เพ<มขLนและอยในคาเปาหมายหลงการผาตด parathyroid gland
87
Bone marrow
fibrosis
บทบาทของเภสชกรในการดแลผปวยโรคไตเรGอรง • ทางานเช<อมประสานกบบคลากรทางแพทยอ<น ๆ ท<รวมดแล
ผปวยไดอยางไรรอยตอ
• การดแลผปวยแตละรายเภสชกรควรทราบวาผปวยเปนโรคไตเรLอรงอยในระยะใด และมเปาหมายในการรกษาอยางไร
• ใหคาแนะนาถงขอบงใชของยา ความสาคญของการรบประทานยา เปาหมายของการใชยาแตละชนด อาการไมพงประสงคท<พบไดบอย และการจดการเบLองตนกบอาการดงกลาว การปองการอนตรกรยาระหวางยากบยา หรอยากบอาหาร
• หลกเล<ยงการใชยาท<สงผลทาใหไตเส<อม และการออกแบบขนาดยาใหเหมาะสมตามหนาท<การทางานของไต

บทสรป
• CKD เปนโรคเรLอรงซ<งมการเส<อมถอยชนดหน<งหากไมไดรบการรกษาอยางเหมาะสม
• เปาหมายของการรกษาท<สาคญคอชะลอไมใหโรคดาเนนเขาสโรคไตเรLอรงระยะสดทายอยางรวดเรว
• ผปวยควรไดรบการแนะนาใหมความตระหนกเก<ยวกบความจาเปนของการตดตามการรกษาท<สถานพยาบาลอยางสม<าเสมอ เพ<อปองกนไมใหโรคไตเรLอรงดาเนนไปอยางรวดเรว
บทสรป
• ผปวยและญาตควรมความเขาใจและมสวนรวมในการวางแผนการรกษาดวย– ผปวยควรทราบวาเปนโรคไตเรLอรงอยในระยะใด โรค
ดาเนนเรวชาอยางไร มเปาหมายในการรกษาอยางไร ตองรกษาอยางไรบาง
– ส<งใดท<ผปวยควรระวงหรอหลกเล<ยง เชน ยาท<มพษตอไต – หากผปวยจาเปนตองไปรกษาท<สถานพยาบาลอ<น ๆ หรอ
รานยาท<ไมทราบประวตวาผปวยเปนโรคไต ตองแนะนาให ผปวยแจงสถานพยาบาลนLนดวยเพ<อปองกนอนตรายจากการไดรบยาไมเหมาะสมในแงชนดและขนาดยา
Thank you