Embed Size (px)
Citation preview

Clinical Approach on Syphilis: Diagnosis & Treatment
นายแพทย์อนพุงศ์ ชิตวรากรสมาคมแพทย์โรคตดิตอ่ทางเพศสมัพนัธ์แห่งประเทศไทยท่ีปรึกษาส านกัโรคเอดส์และโรคติดตอ่ทางเพศสมัพนัธ์
SCC@TropMed





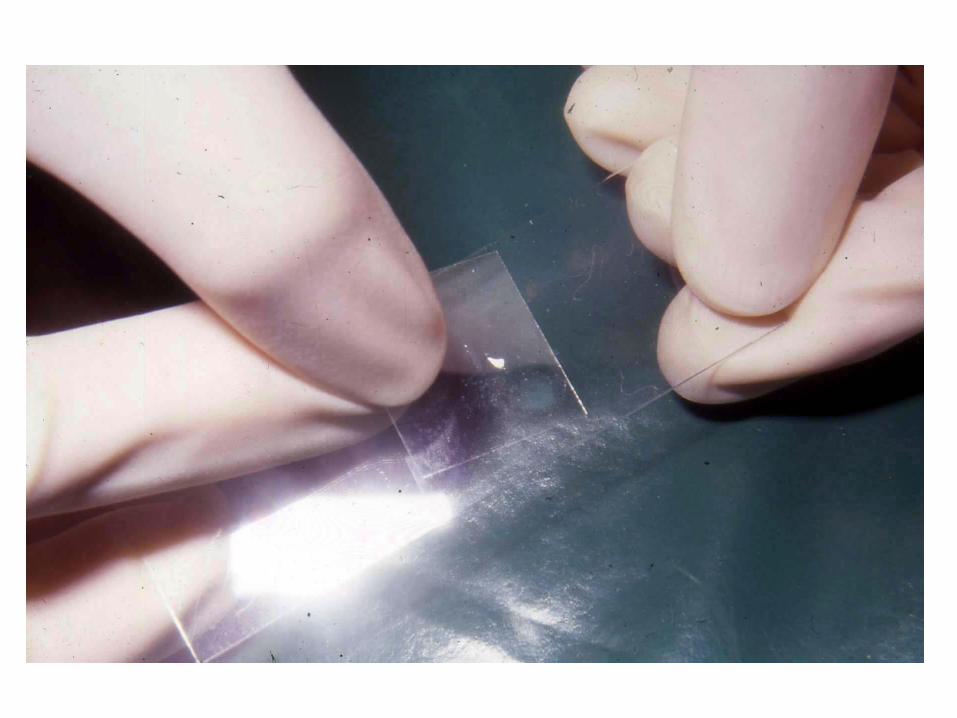
Primary syphilis: diagnosis
1. clinical characteristic of chancre: indurated,
well defined, painless, clean base ulcer
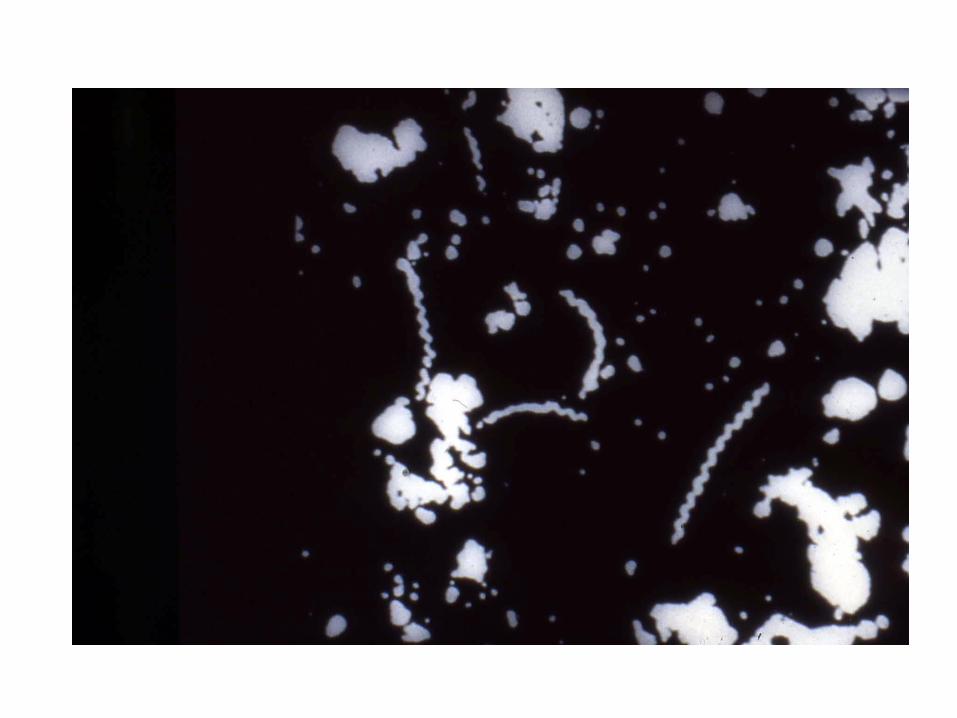
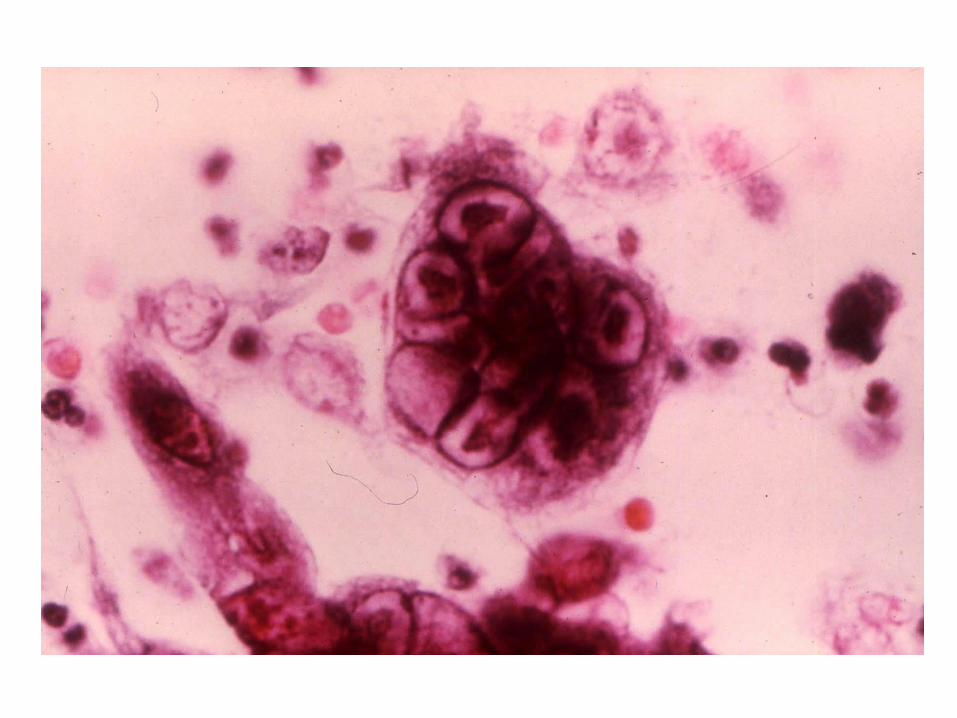
2. Dark field examination positive
3. VDRL or RPR positive in 50-70%
4. FTA-Abs positive in 70-90%
Secondary Syphilis: general clinical manifestation
• Constitutional symptom: malaise, fever, headache, anorexia, nausea, vomiting
• Generalized lymphadenopathy: painless, discrete, rubbery on palpation




Condyloma lata, Dark ground: POSITIVE
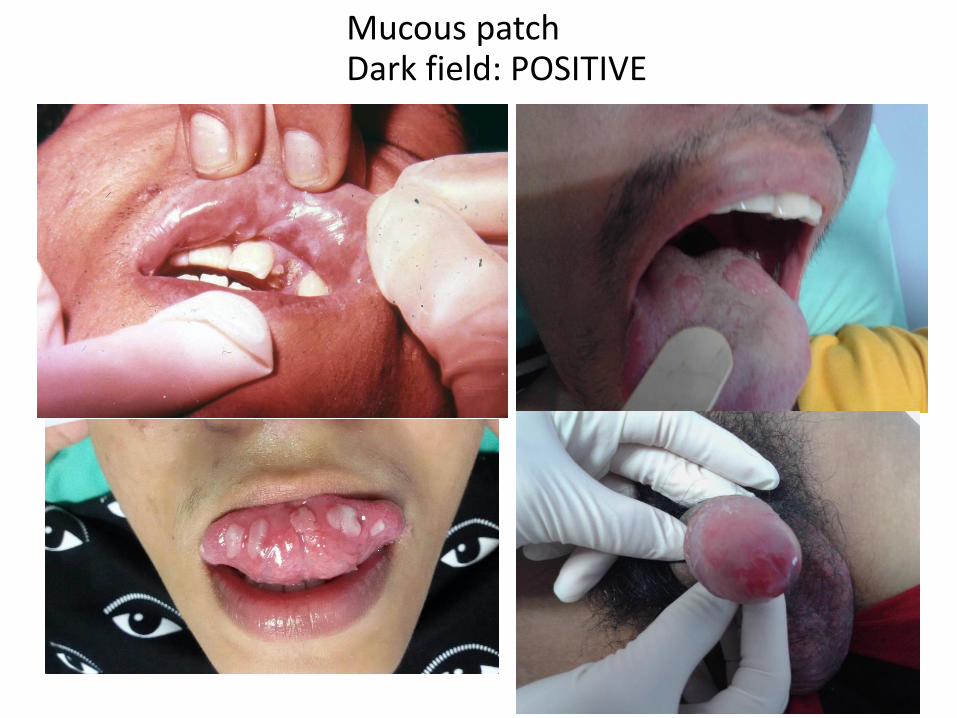
Mucous patchDark field: POSITIVE

Moth eaten alopeciaRPR, VDRL, TP: POSITIVE
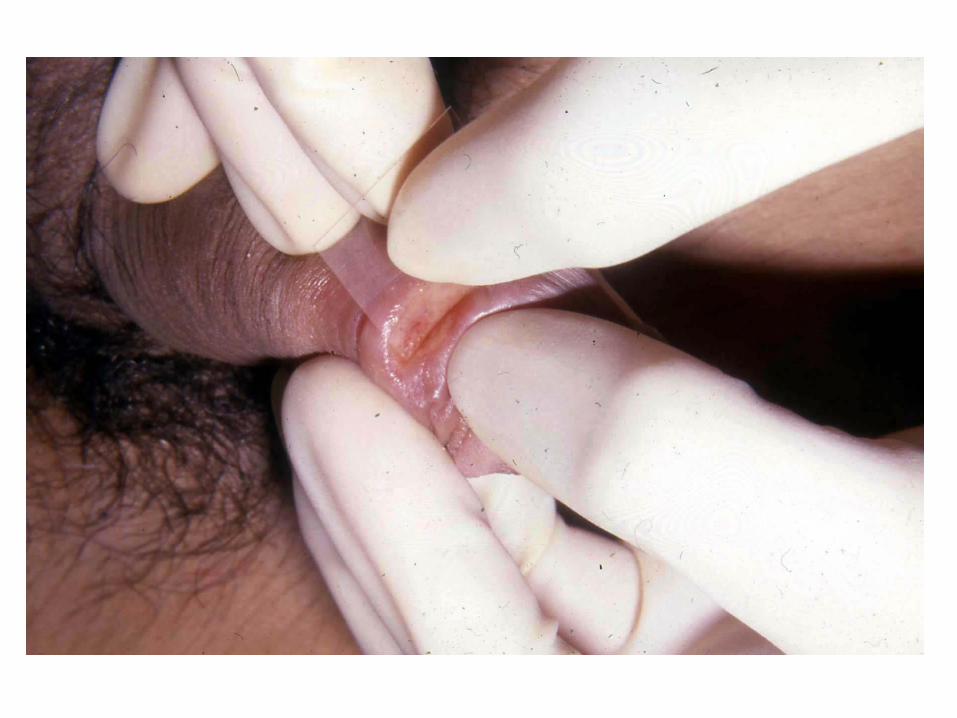
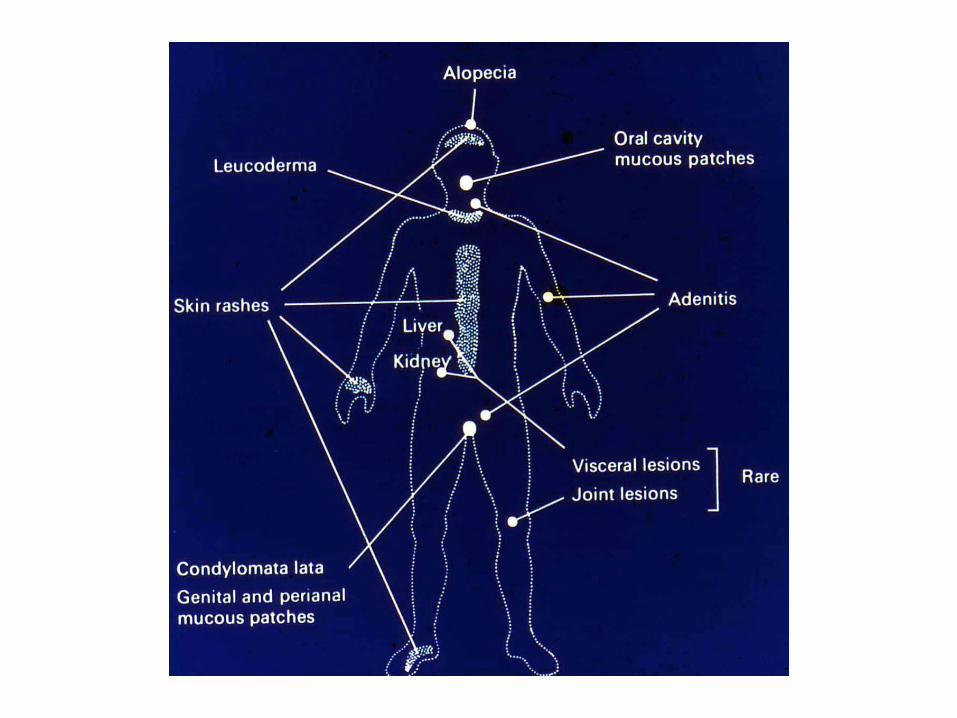
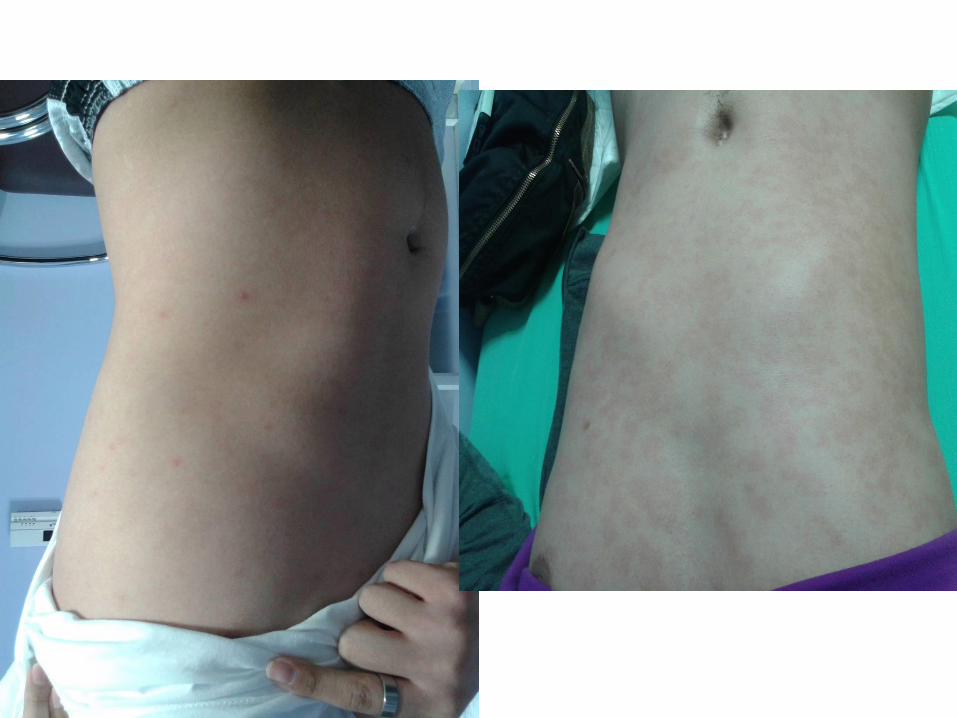
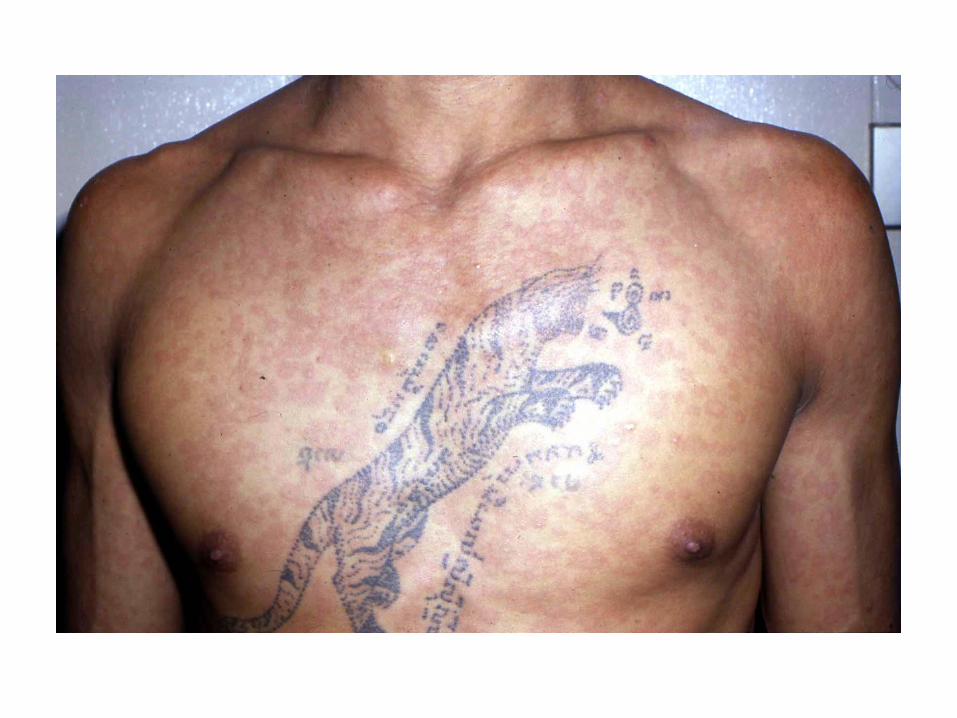
Secondary syphilis:
Specific clinical manifestation
1. Skin rash: macular, maculopapular, papular,
papulosquamous, pustualar, (non-itching,
symmetrical)
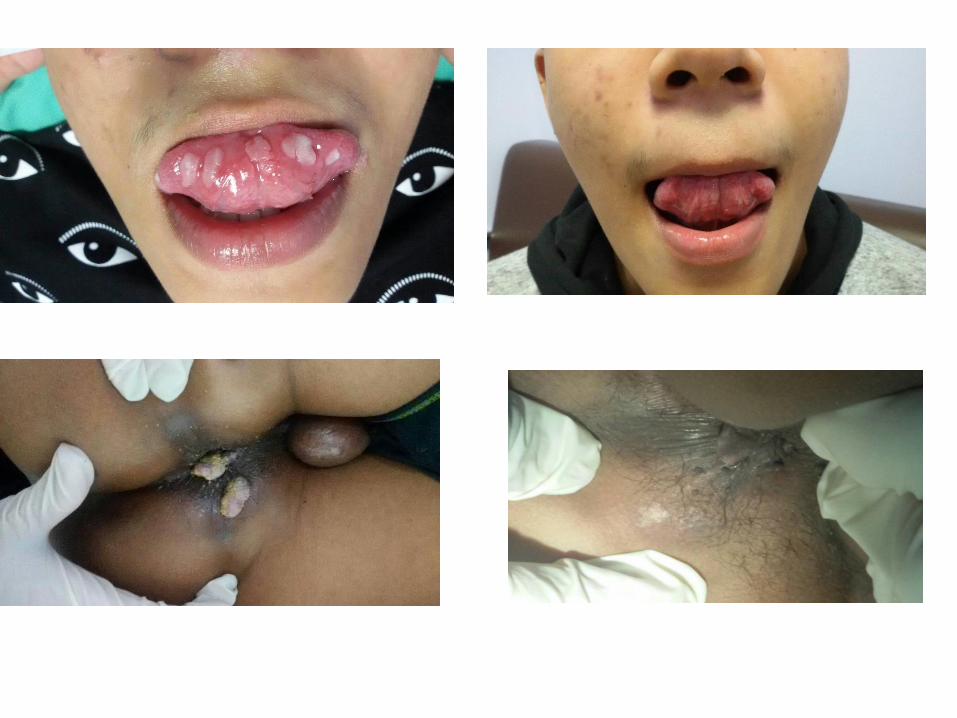
2. Condyloma lata: papular lesions in intertrigineous
area which erode
3. Mucous patch at genital or oral cavity
4. Moth eaten alopecia
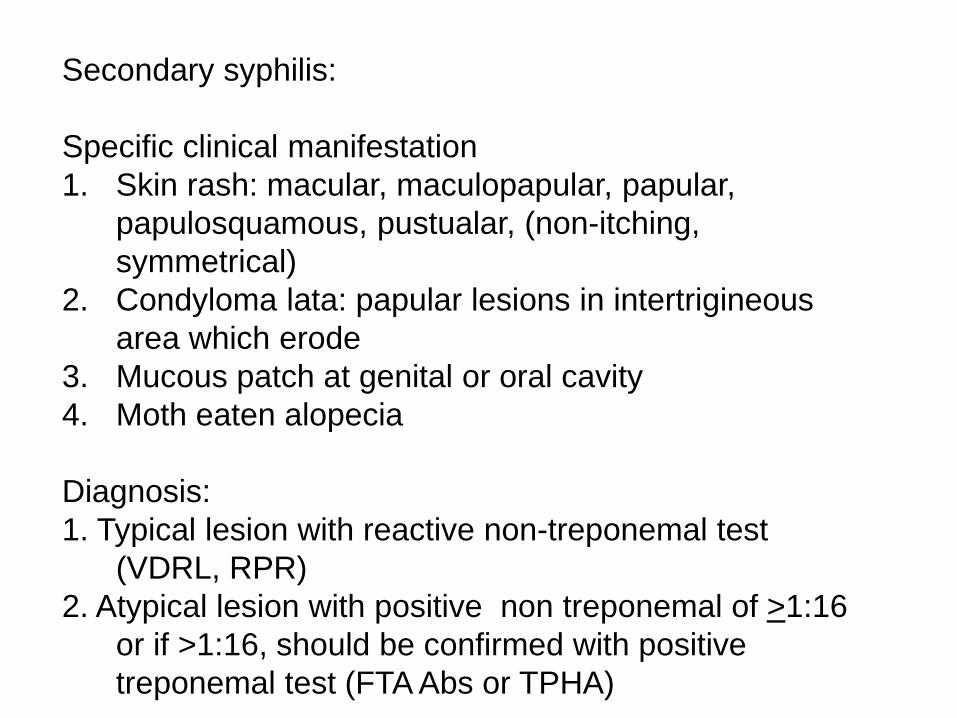
Diagnosis:
1. Typical lesion with reactive non-treponemal test
(VDRL, RPR)
2. Atypical lesion with positive non treponemal of >1:16
or if >1:16, should be confirmed with positive
treponemal test (FTA Abs or TPHA)
Latent syphilis:
1. Early latent : less than 1
year duration
2. Late latent: > 1 year or
unknown duration
Diagnosis:
1. Non treponamal test
and treponemal test
reactive
2. No abnormal finding
from physical
examination and other
investigations
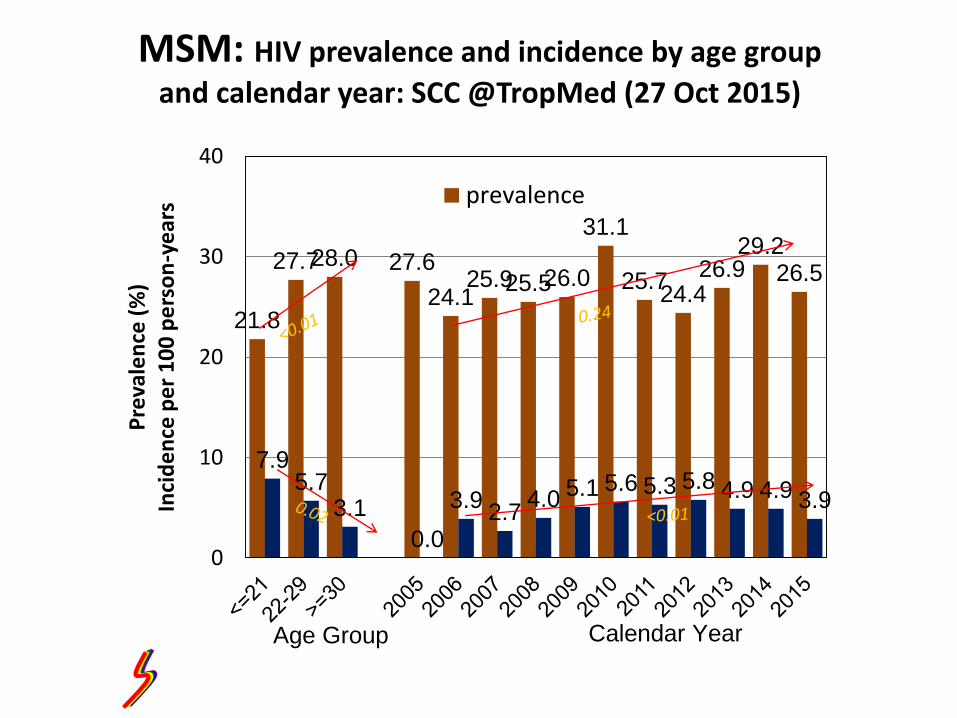
MSM: HIV prevalence and incidence by age group
and calendar year: SCC @TropMed (27 Oct 2015)
21.8
27.728.0 27.6
24.125.925.526.0
31.1
25.724.4
26.929.2
26.5
7.95.7
3.1
0.0
3.92.7
4.0 5.1 5.6 5.3 5.8 4.9 4.9 3.9
0
10
20
30
40P
reva
len
ce (
%)
Inci
de
nce
pe
r 1
00
pe
rso
n-y
ear
s prevalence
Age Group Calendar Year
10.110.7
12.9
6
3.2
6.2
4.4
8
11.710.7
12.7
15.416.3
3.9 43
0 01
0.3
4 3.9 4.23.7 4.1 4.4
0
5
10
15
20
<=21 22-29 >=30 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014
Pre
vale
nce
(%
)In
cid
en
ce p
er
100
pe
rso
n-y
ea
rs
prevalence incidence
Age Group Calendar Year
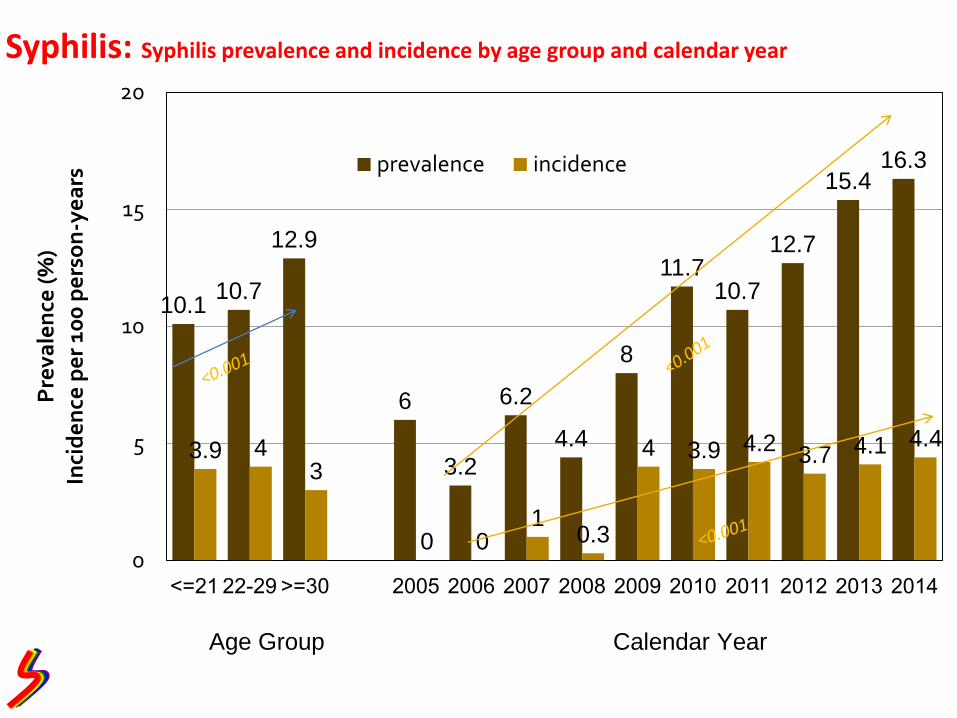
Syphilis: Syphilis prevalence and incidence by age group and calendar year
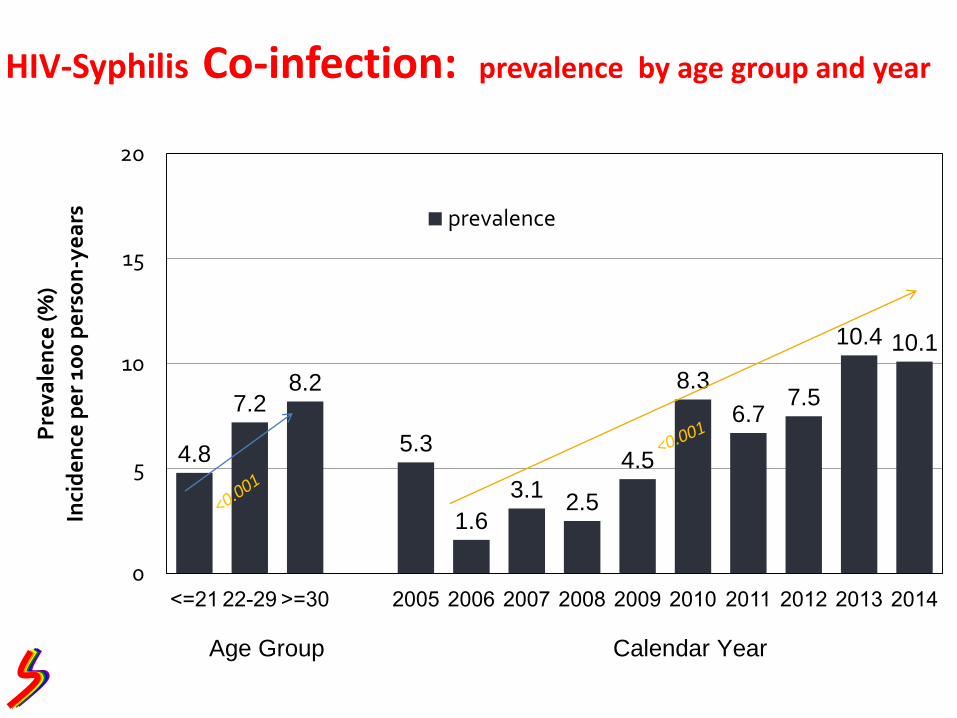
4.8
7.28.2
5.3
1.6
3.12.5
4.5
8.3
6.77.5
10.4 10.1
0
5
10
15
20
<=21 22-29 >=30 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014
Pre
vale
nce
(%
)In
cid
en
ce p
er
100
pe
rso
n-y
ea
rs prevalence
Age Group Calendar Year
HIV-Syphilis Co-infection: prevalence by age group and year
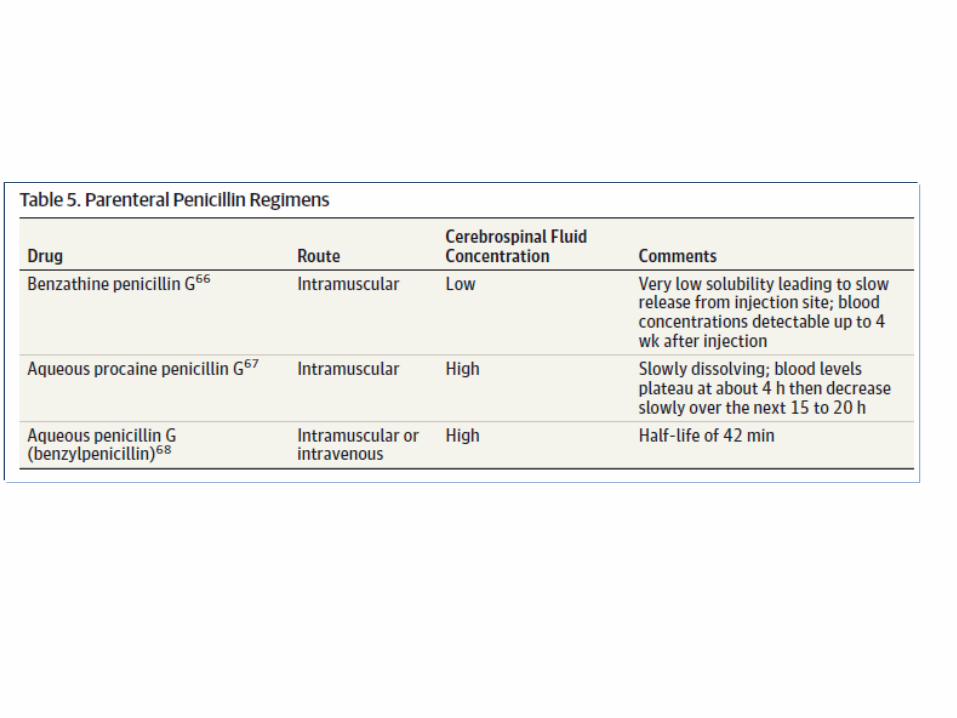
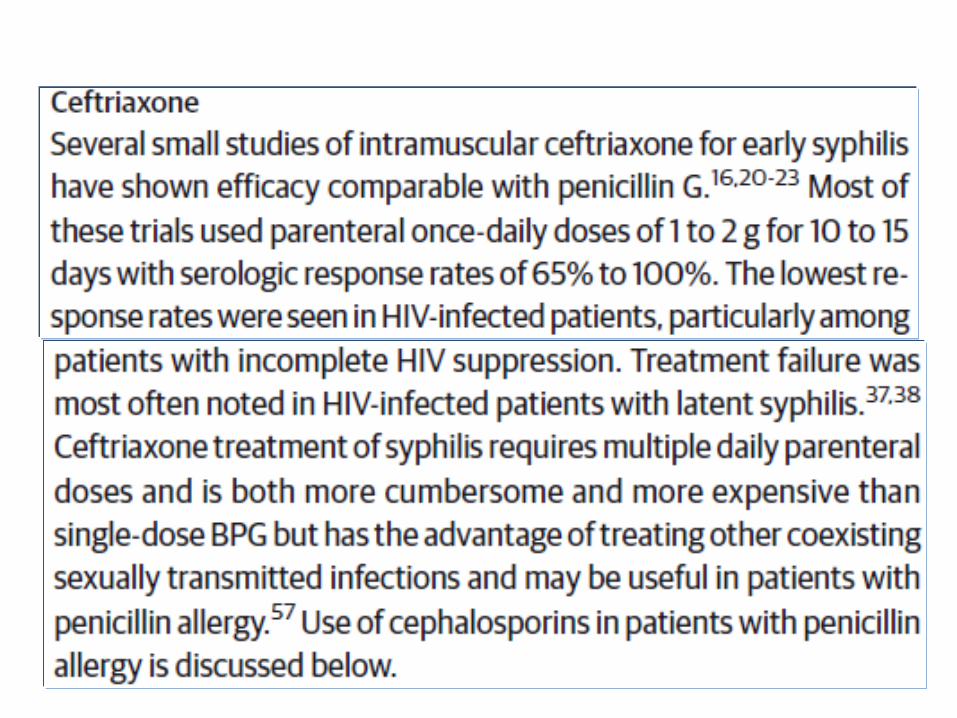
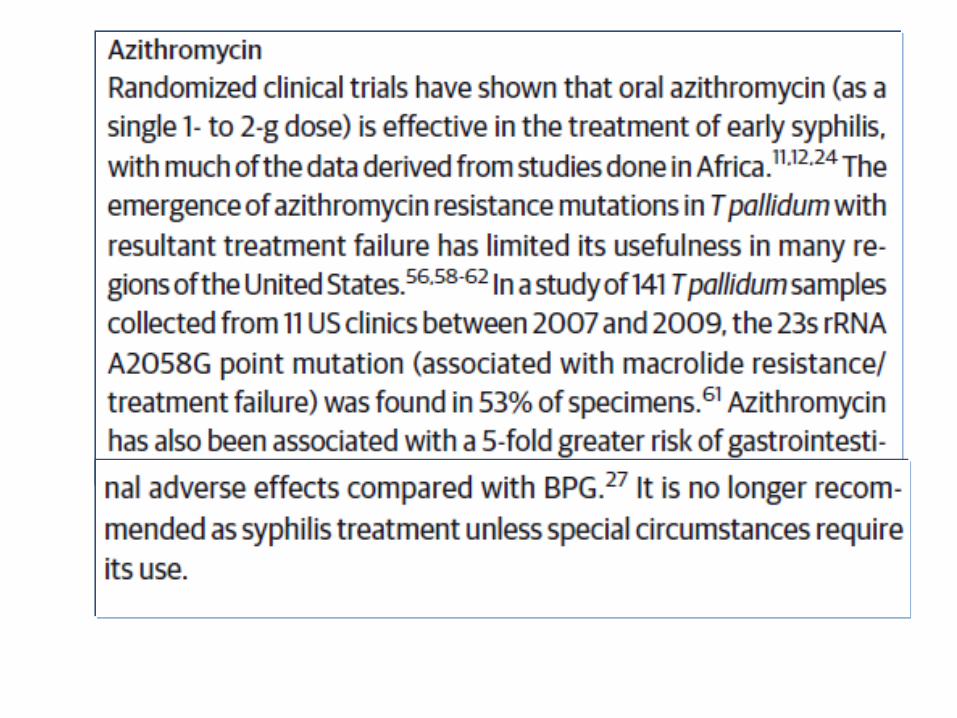
Syphilis: treatment
• Early syphilis: primary, secondary and early latent syphilis
• Benzathine penicillin 2.4 M unit IM, single dose
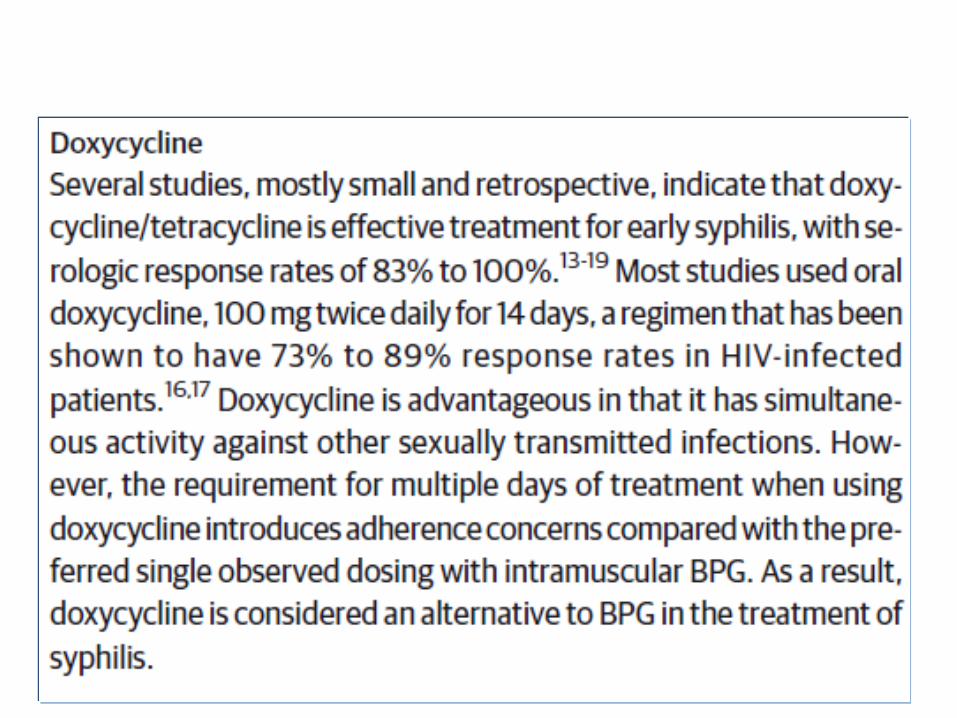
• Alternative: tetracycline 500mg. qid. 14 days or doxycycline 100mg. bid. 14 days or erythromycin 500mg. qid. 14 days
Syphilis: treatment
• Late syphilis: latent syphilis
• Benzathine penicillin 2.4 M unit IM, weekly for 3 consecutive weeks
• Alternative: tetracycline 500mg. qid. 28 days or doxycycline 100mg. bid. 28 days or erythromycin 500mg. qid. 28 days
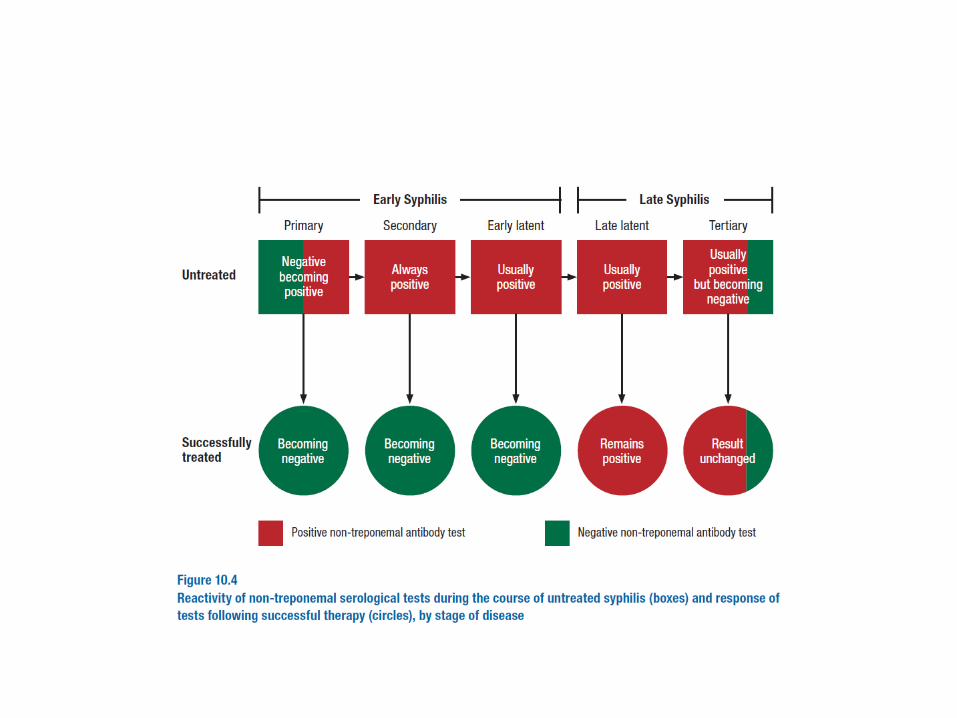
Syphilis: follow up
• Quantitative non-treponemal test (VDRL or RPR) for every 3 months in year 1, every 6 months in year 2 after treatment.
• Additional once a year in case of reactive test.
Indication for retreatment: syphilis
• Clinically persist or relapse
• Increase in VDRL, RPR titer of > 4 folds
• 1 year after treatment, RPR or VDRL titer of >1:8 failed to show 4 folds decrease
• Retreatment as late syphilis
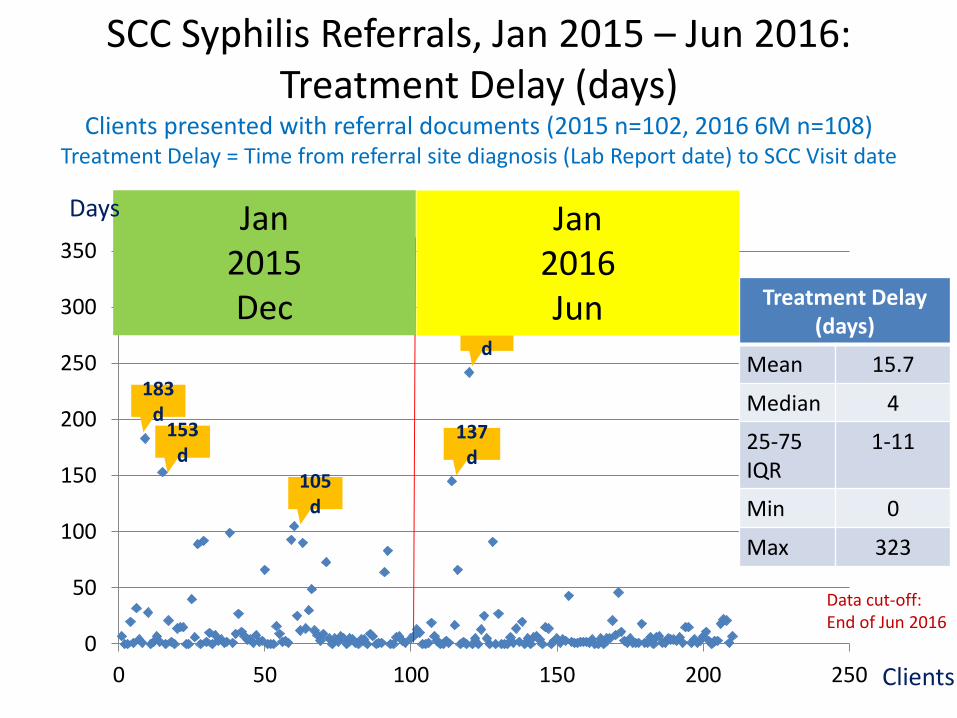
0
50
100
150
200
250
300
350
0 50 100 150 200 250
183 d
105 d
137 d
242 d
323 d
153 d
Data cut-off:End of Jun 2016
SCC Syphilis Referrals, Jan 2015 – Jun 2016: Treatment Delay (days)
Clients presented with referral documents (2015 n=102, 2016 6M n=108)Treatment Delay = Time from referral site diagnosis (Lab Report date) to SCC Visit date
Clients
Jan 2015 Dec
Jan 2016 Jun
Days
Treatment Delay (days)
Mean 15.7
Median 4
25-75 IQR
1-11
Min 0
Max 323
790 menavailable both HIV and TP result
Prozone phenomenon
• Occurred in 1-2 % of secondary SY
• Typical lesion of secondary sy but non reactive non-treponemal test (VDRL, RPR)
• Because of excess amount of anticardiolipin antibody
• Diluting serum should be performed to overcome the phenomenon
Jarisch- Herxheimer Reaction
• Following the treatment of primary or secondary sy
• Occure within few hours after treatment and subsides within 24 hours
• Triggered by endotoxin or allergy phenomenon
Jarisch- Herxheimer ReactionClinical manifestation
• Fever, chill, malaise, arthralgia, myalgia, headache, nausea
• Intensification of skin and mucous membrane lesion
• Increase in metabolic and heart rate
Biological false positive
• Reactive non-treponemal test (VDRL, RPR), but treponemal test (FTA-Abs, TPHA) non reactive
Acute BFPDuration of < 6 monthsAssociated with: 1. Acute infection (bacteria,viral, protozoa)2. Immunization, vaccination
Chronic BFP
Duration of > 6 months
Associated with:
1. Chronic infection:
Leprosy, malaria,
Autoimmune diseases
2. Intravenous drug users
3. normal, old age











![Sezione 9 gb - Moto-Abruzzo · 2019. 9. 22. · ETV mille Rally SUMMARY 9.1. ... [1000 km (625 miles)] Every 7500 km (4687 miles) or 12 months Every 15000 km ... (as per the instructions](https://img.pdfslide.tips/doc/110x75/60cfab357d413727970f4204/sezione-9-gb-moto-abruzzo-2019-9-22-etv-mille-rally-summary-91-1000.jpg)


















