Embed Size (px)
Citation preview
Dèficit de vitamina D i risc cardio-vascular
Dr. Jaume Almirall
Servei de Nefrologia. Corporació Parc Taulí.
Sabadell
Manresa, gener de 2015
aspectes a tractar: (proposta 30 minuts)
• VD: breu resumen del metabolisme, nivells sèrics a la població general
• associació del dèficit de VD amb múltiples patologies, estudis epidemiològics i observacionals –focus sobre els risc CV-
• mecanismes fisiopatològics que pretenen explicar aquesta associació
• resultats d’estudis d’intervenció amb suplementació de VD
• conclusions (o millor: reflexions)
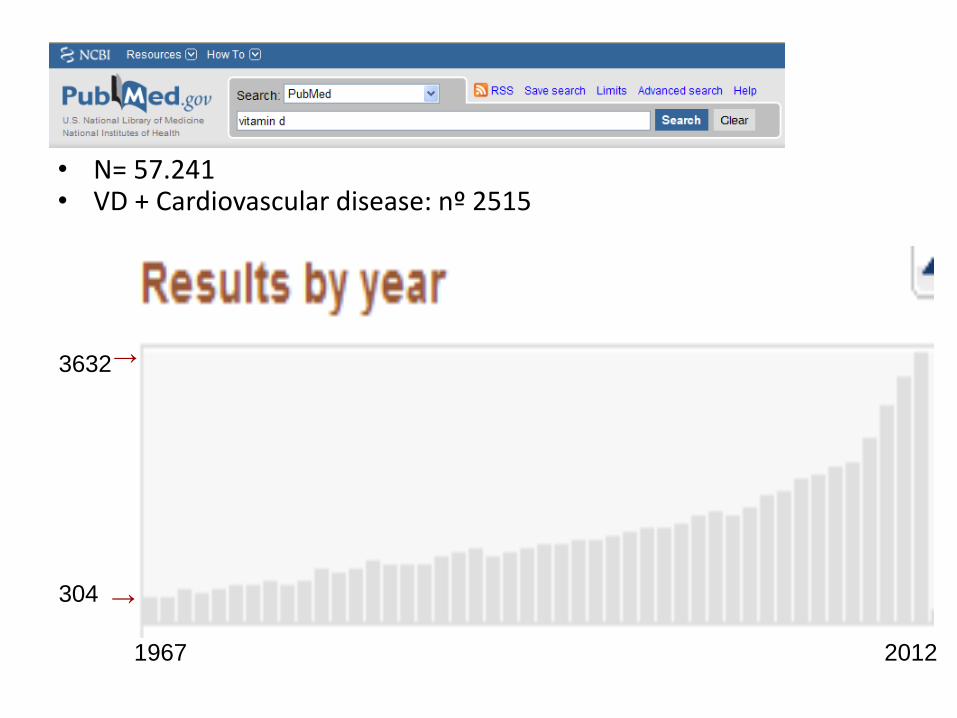
• N= 57.241 • VD + Cardiovascular disease: nº 2515
→
1967 2012
3632
304
→
El coneixement sobre el metabolisme i les funcions de la VD ha experimentat un avanç extraordinari en els darrers anys
Que ha canviat?
• Les accions de la VD no es limiten al manteniment del sistema
esquelètic i del metabolisme Ca-P
• El sistema hormonal de la VD es complexa, distingint unes accions “endocrines” i unes accions “paracrines o autocrines”
aspectes a tractar: (proposta 30 minuts)
• VD: breu resumen del metabolisme, nivells sèrics a la població general
• associació del dèficit de VD amb múltiples patologies, estudis epidemiològics i observacionals
• mecanismes fisiopatològics que pretenen explicar aquesta associació
• resultats d’estudis d’intervenció
• conclusions (o millor: reflexions)
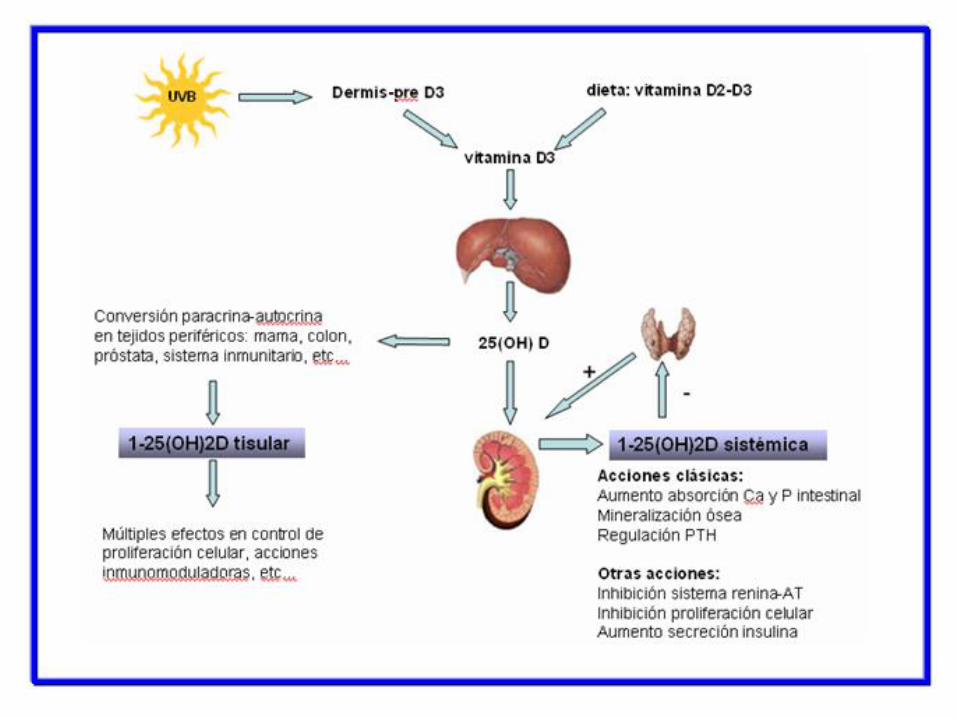

un mecanismo endocrino (hormona calciotrópica) a través del calcitriol
circulante sintetizado en el riñón y que está regulado por la PTH y el FGF23. un mecanismo autocrino (no calciotrópico) que sintetiza, utiliza y degrada el calcitriol intracelularmente. Acción dependiente de sustrato.
sistema responsable de muchas de las funciones “no clásicas” de la VD
Resumen: La VD actúa en el organismo a través de la activación
del VDR (factor de transcripción) mediante :
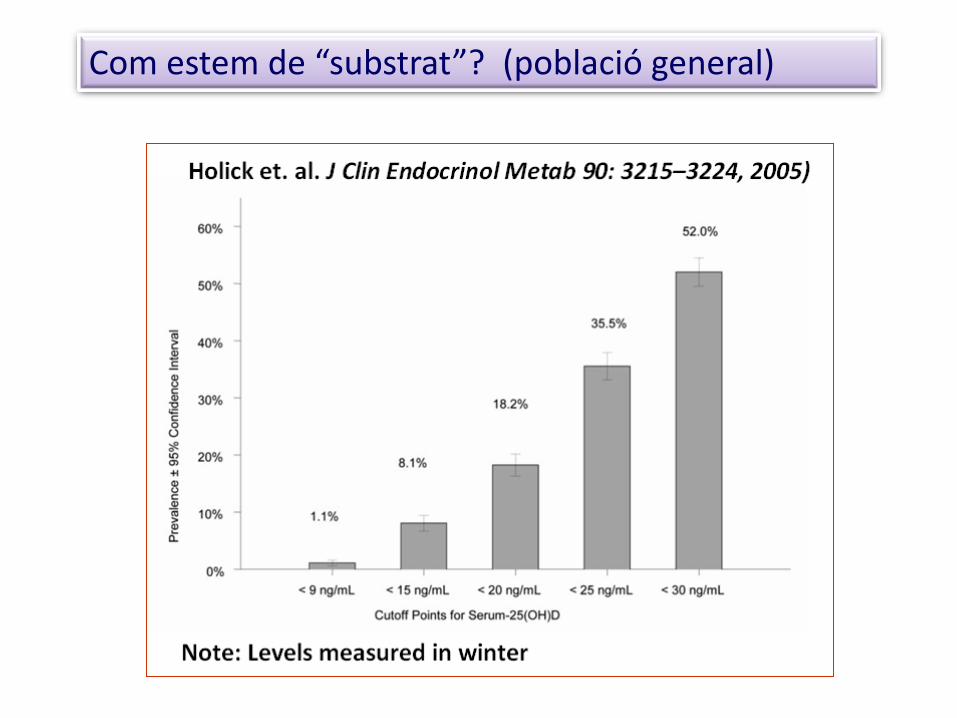
Com estem de “substrat”? (població general)

Demographic differences and trends of VD insufficiency is US population, 1988-2004 Ginde AA, et al. Arch Intern Med, 2009; 23;169(6):626-32
• The prevalence of VD insufficiency may be rising, but population-based trends are uncertain.
• Compared 25[OH]D from NHANES III (1988-94: n=18.883), with data collected from 2001-4:n=13.369
• RESULTS:
• 1988-94 mean 25(OH)D was 30 ng/mL
• 2001-04 mean 25(OH)D decreased to 24 ng/mL
• prevalence of levels < 10 ng/mL increased from 2% to 6%
• prevalence of levels > 30 ng/mL decreased from 45% to 23%.
• National data demonstrate a marked decrease in serum 25(OH)D levels from
the 1988-94 to the 2001-04.
• Current recommendations for VD supplementation are inadequate to address
the growing epidemic of VD insufficiency
I sembla que seguim empitjorant…

aspectes a tractar: (proposta 30 minuts)
• VD: breu resumen del metabolisme, nivells sèrics a la població general
• associació del dèficit de VD amb múltiples patologies, estudis epidemiològics i observacionals
• mecanismes fisiopatològics que pretenen explicar aquesta associació
• resultats d’estudis d’intervenció
• conclusions (o millor: reflexions)
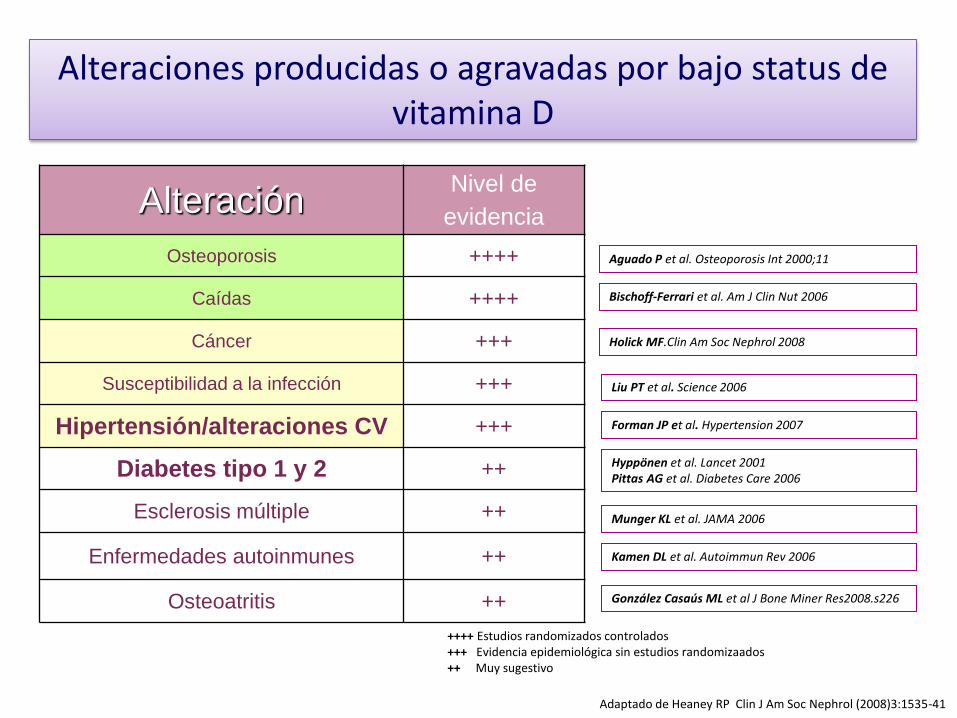
Alteraciones producidas o agravadas por bajo status de vitamina D
Alteración Nivel de
evidencia
Osteoporosis ++++
Caídas ++++
Cáncer +++
Susceptibilidad a la infección +++
Hipertensión/alteraciones CV +++
Diabetes tipo 1 y 2 ++
Esclerosis múltiple ++
Enfermedades autoinmunes ++
Osteoatritis ++
Adaptado de Heaney RP Clin J Am Soc Nephrol (2008)3:1535-41
Bischoff-Ferrari et al. Am J Clin Nut 2006
Kamen DL et al. Autoimmun Rev 2006
Munger KL et al. JAMA 2006
Hyppönen et al. Lancet 2001 Pittas AG et al. Diabetes Care 2006
González Casaús ML et al J Bone Miner Res2008.s226
Holick MF.Clin Am Soc Nephrol 2008
Liu PT et al. Science 2006
Forman JP et al. Hypertension 2007
Aguado P et al. Osteoporosis Int 2000;11
++++ Estudios randomizados controlados +++ Evidencia epidemiológica sin estudios randomizaados ++ Muy sugestivo
Melamed ML et al: Serum 25(OH)D levels and the prevalence of peripheral arterial
disease: results from NHANES 2001-4. Arteroscler Thromb Vasc Biol, 2008; 28: 1179-85
Kim DH et al: Prevalence of hypovitaminosis D in cardiovascular diseases (NAHNES
2001-4); AmJ Cardiol 2008: 102: 1540-44
Giovannucci E, et al: 25-Hydroxyitamin D and risk of miocardial infarction in men. Arch
Intern Med 2008; 168: 1174-80
Wang TJ et al; VD deficiency and risk of CV Disease. Circulation 2008; 117: 503-11
Forman JP et al: plasma 25-(OH)D levels and risk of incidence hypertension.
Hypertension 2007; 49:1063-69
Pilz S, et al: low Vitamin D levels predict stroke in patients referred to coronary
angiography. Stroke 2008; 39; 2611-13
Anderson JL, et al: relation of vitamin D deficiency to cardiovascular risk factors,
disease status, and incident events in a general healthcare population. Am J
Cardiol; 2010;106: 963-068
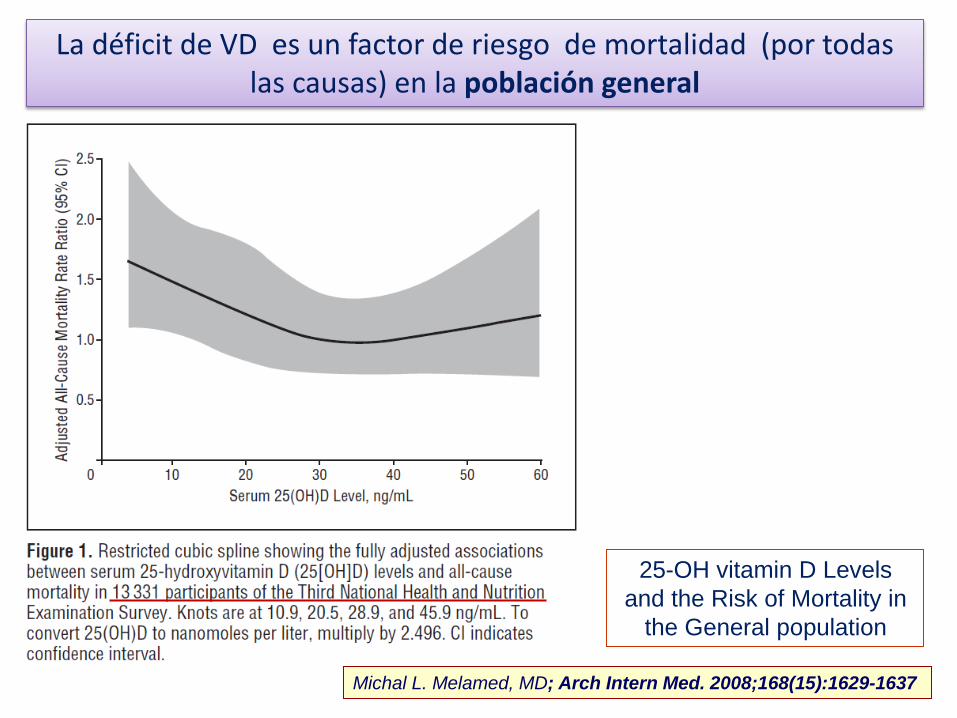
Michal L. Melamed, MD; Arch Intern Med. 2008;168(15):1629-1637
25-OH vitamin D Levels
and the Risk of Mortality in
the General population
La déficit de VD es un factor de riesgo de mortalidad (por todas las causas) en la población general

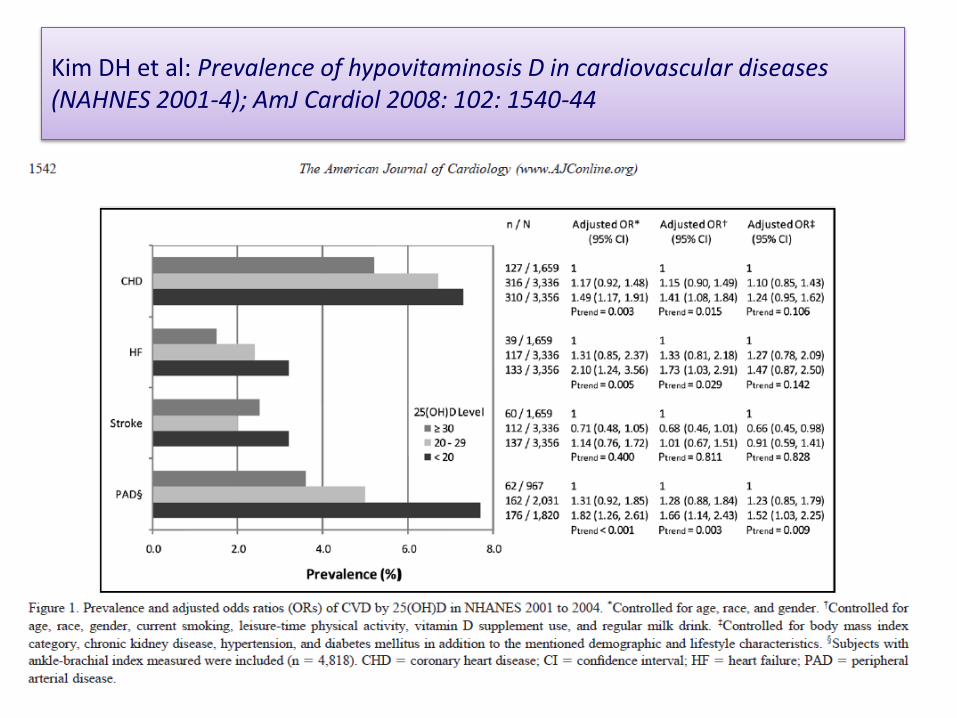
Kim DH et al: Prevalence of hypovitaminosis D in cardiovascular diseases (NAHNES 2001-4); AmJ Cardiol 2008: 102: 1540-44
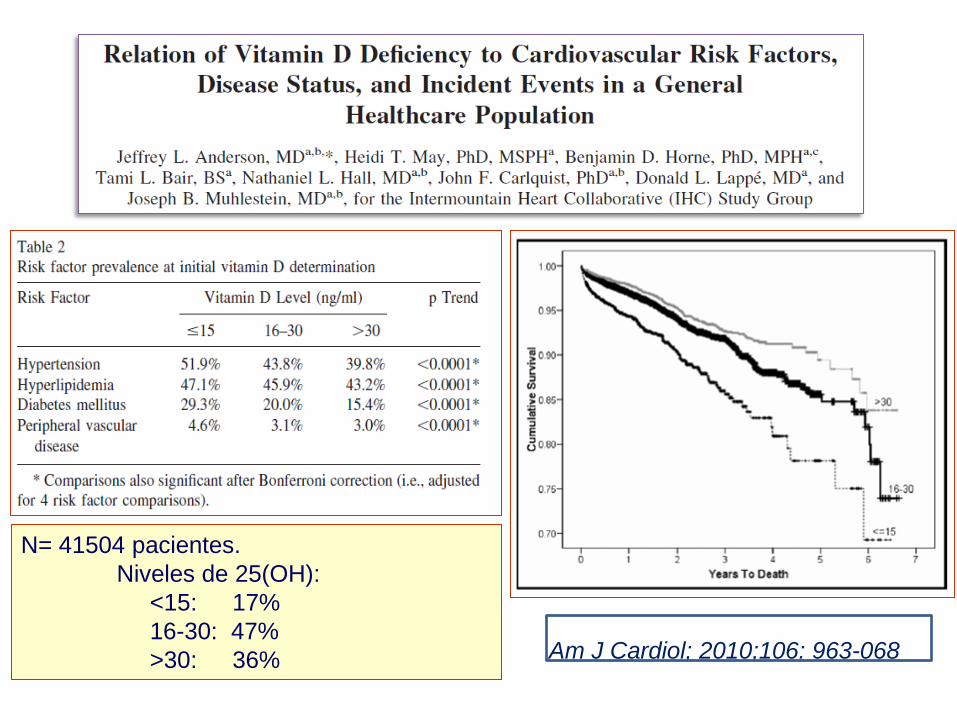
N= 41504 pacientes.
Niveles de 25(OH):
<15: 17%
16-30: 47%
>30: 36% Am J Cardiol; 2010;106: 963-068
• Background: – VD deficiency is common among the elderly and may contribute to cerebrovascular diseases.
We aimed to elucidate whether low VD levels are predictive for fatal stroke.
• Methods: – The LURIC study includes 3316 patients who were referred to coronary angiography at
baseline between 1997 and 2000. 25(OH)D and 1,25(OH)2D were measured in 3299 and 3315 study participants
• Results: – During a median follow-up time of 7.75 years, 769 patients died, including 42 fatal (ischemic
and hemorrhagic) strokes.
• Conclusions: – Low levels of 25(OH)D and 1,25(OH)2D are independently predictive for fatal strokes,
suggesting that VD supplementation is a promising approach in the prevention of strokes
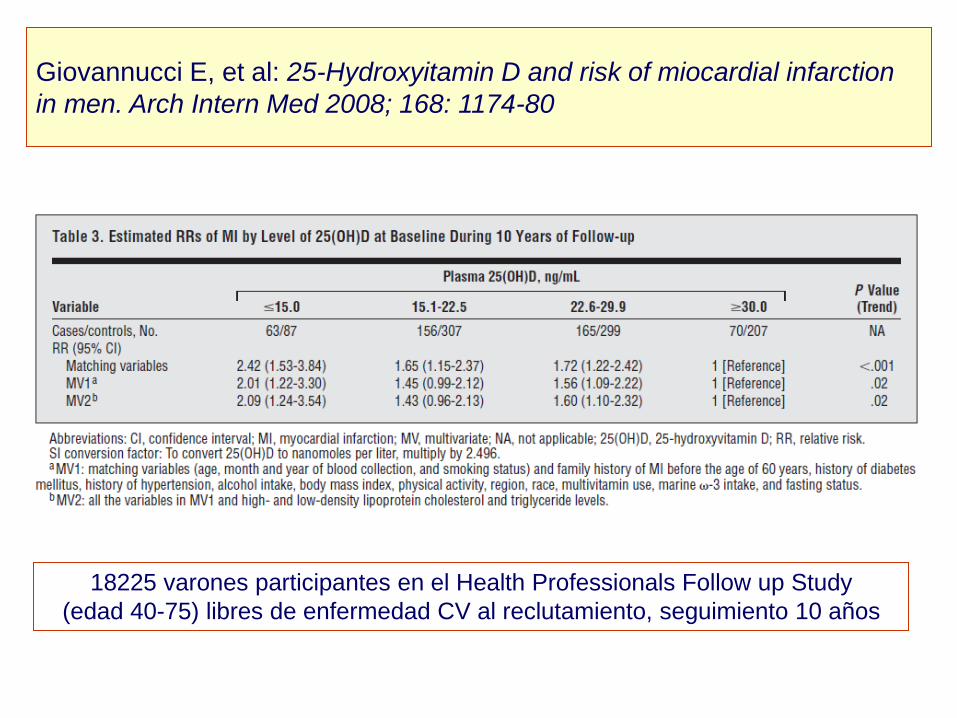
Giovannucci E, et al: 25-Hydroxyitamin D and risk of miocardial infarction
in men. Arch Intern Med 2008; 168: 1174-80
18225 varones participantes en el Health Professionals Follow up Study
(edad 40-75) libres de enfermedad CV al reclutamiento, seguimiento 10 años
• 1739 Framingham Offspring Study participants without prior CV disease. • 28% had levels <15 ng/mL (9% <10 ng/mL).
• mean follow-up: 5.4 years, 120 individuals developed a first CV event.
• Individuals with 25-OH D <15 had a multivariable-adjusted hazard ratio of 1.62 for
incident CV events compared with those with >15 ng/mL.
• effect was evident in participants with HTA but not in those without HTA
Conclusions: - VD deficiency is associated with incident CV disease. - Further studies may be warranted to determine whether correction of
VD deficiency could contribute to the prevention of CV disease
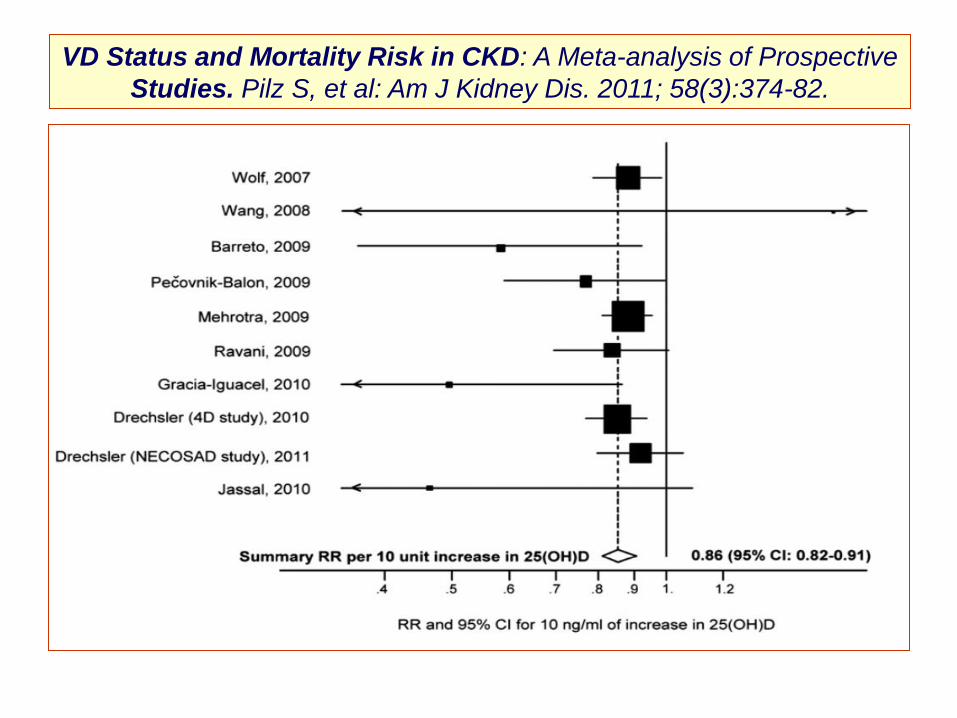
VD Status and Mortality Risk in CKD: A Meta-analysis of Prospective
Studies. Pilz S, et al: Am J Kidney Dis. 2011; 58(3):374-82.
METHODS:
10,170 participants (18 years of age) using National Health and Nutrition Examination Survey data
(2001-2004) combined with National Death Index for vital status information through December 2006.
Cox proportional hazard models with spline (single knot at population median of 25[OH]D) were fit to
estimate hazard ratios (HRs) for all-cause and cardiovascular disease mortality for each 10-unit
increase in serum 25(OH)D.
Models were adjusted for demographic and conventional cardiovascular disease risk factors
The American Journal of Medicine (2013) 126, 509-514
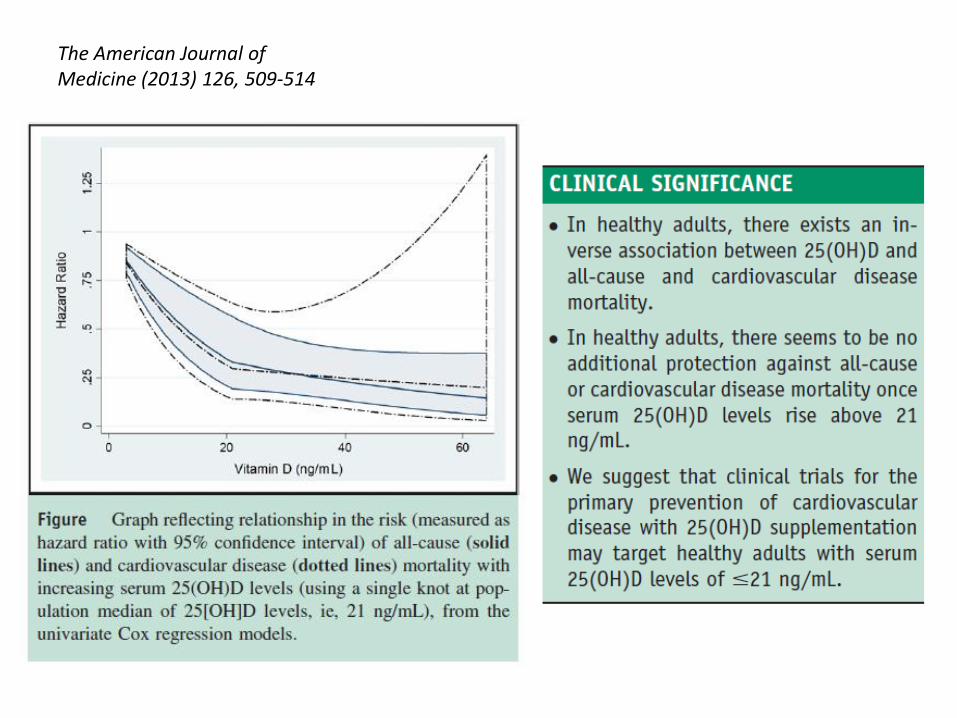
The American Journal of Medicine (2013) 126, 509-514
aspectes a tractar: (proposta 30 minuts)
• VD: breu resumen del metabolisme, nivells sèrics a la població general
• associació del dèficit de VD amb múltiples patologies, estudis epidemiològics i observacionals
• mecanismes fisiopatològics que pretenen explicar aquesta associació
• resultats d’estudis d’intervenció
• conclusions (o millor: reflexions)
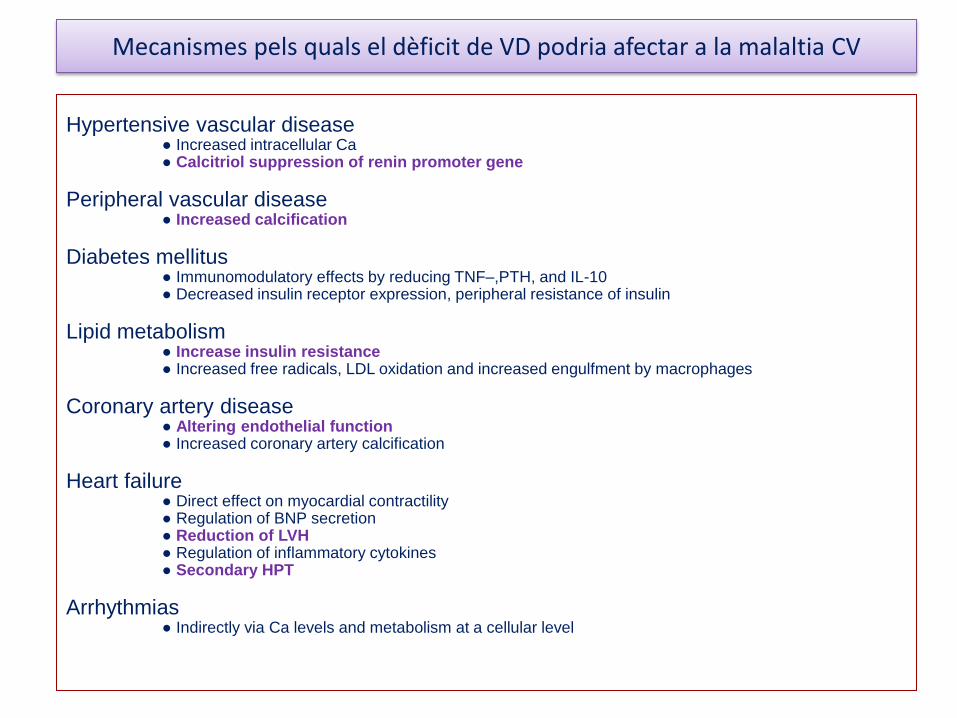
Mecanismes pels quals el dèficit de VD podria afectar a la malaltia CV
Hypertensive vascular disease ● Increased intracellular Ca ● Calcitriol suppression of renin promoter gene
Peripheral vascular disease ● Increased calcification
Diabetes mellitus ● Immunomodulatory effects by reducing TNF–,PTH, and IL-10 ● Decreased insulin receptor expression, peripheral resistance of insulin
Lipid metabolism ● Increase insulin resistance ● Increased free radicals, LDL oxidation and increased engulfment by macrophages
Coronary artery disease ● Altering endothelial function ● Increased coronary artery calcification
Heart failure ● Direct effect on myocardial contractility ● Regulation of BNP secretion ● Reduction of LVH ● Regulation of inflammatory cytokines ● Secondary HPT
Arrhythmias ● Indirectly via Ca levels and metabolism at a cellular level
aspectes a tractar: (proposta 30 minuts)
• VD: breu resumen del metabolisme, nivells sèrics a la població general
• associació del dèficit de VD amb múltiples patologies, estudis epidemiològics i observacionals
• mecanismes fisiopatològics que pretenen explicar aquesta associació
• resultats d’estudis d’intervenció
• conclusions (o millor: reflexions)
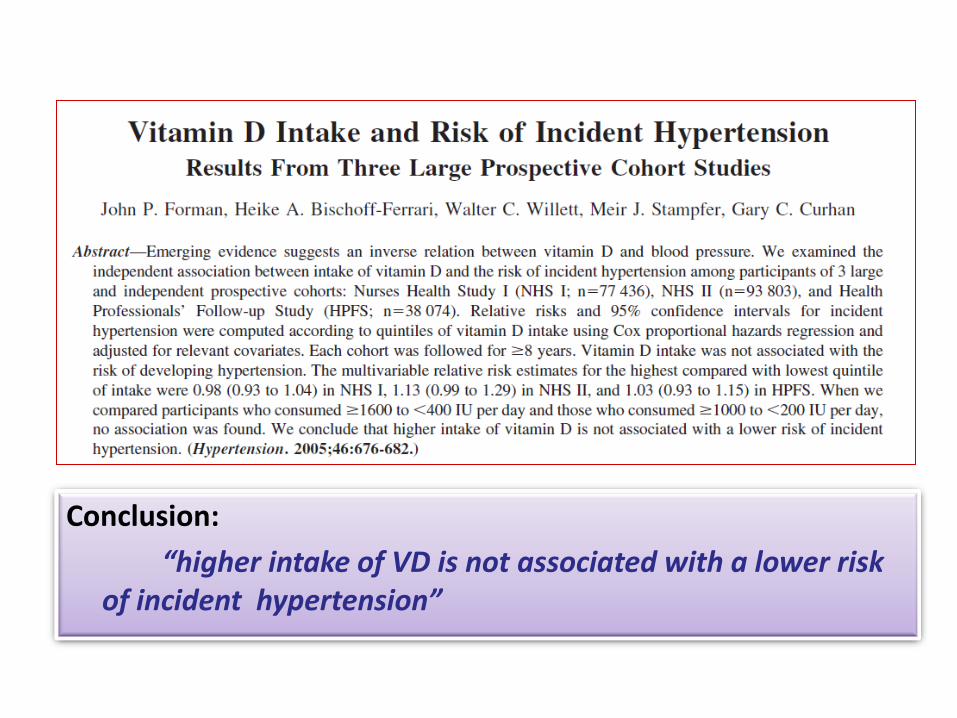
Conclusion:
“higher intake of VD is not associated with a lower risk of incident hypertension”
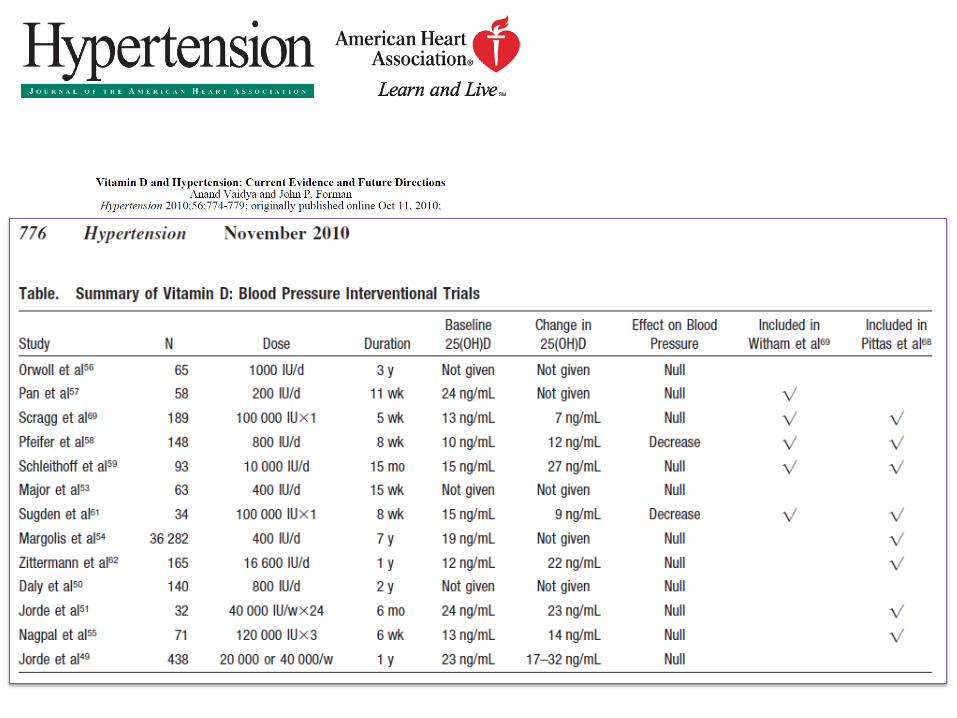

Conclusions: • observational data suggest that lower levels of VD may be associated with
a higher BP and a higher risk of developing HTA.
• Experimental studies in animals, as well as some data in humans, suggest that VD and its metabolites are integrally related to BP and the RAS.
• Nevertheless, randomized, controlled trials have thus far failed to confirm that VD supplementation lowers BP.
• Additional evidence is required before recommending widespread VD supplementation to treat BP or prevent HTA.
• Trials showed no clinically significant effect of VD supplementation at the dosages given on cardiometabolic oucome • VD remains a promising, although unproven, new element in the prevention and management of cardiometabolic disease.
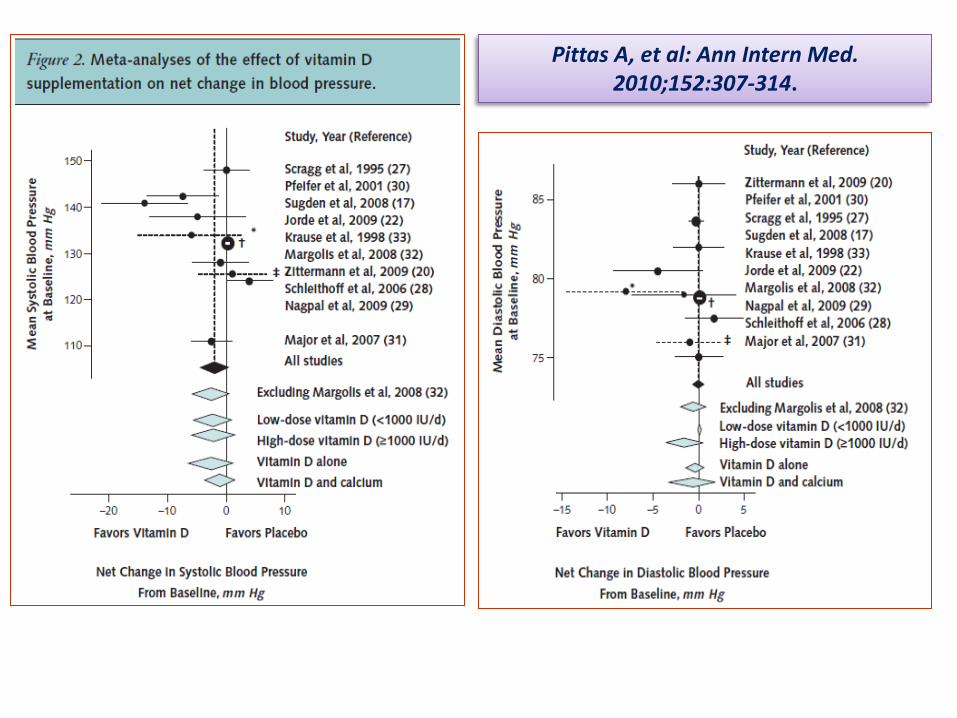
Pittas A, et al: Ann Intern Med. 2010;152:307-314.
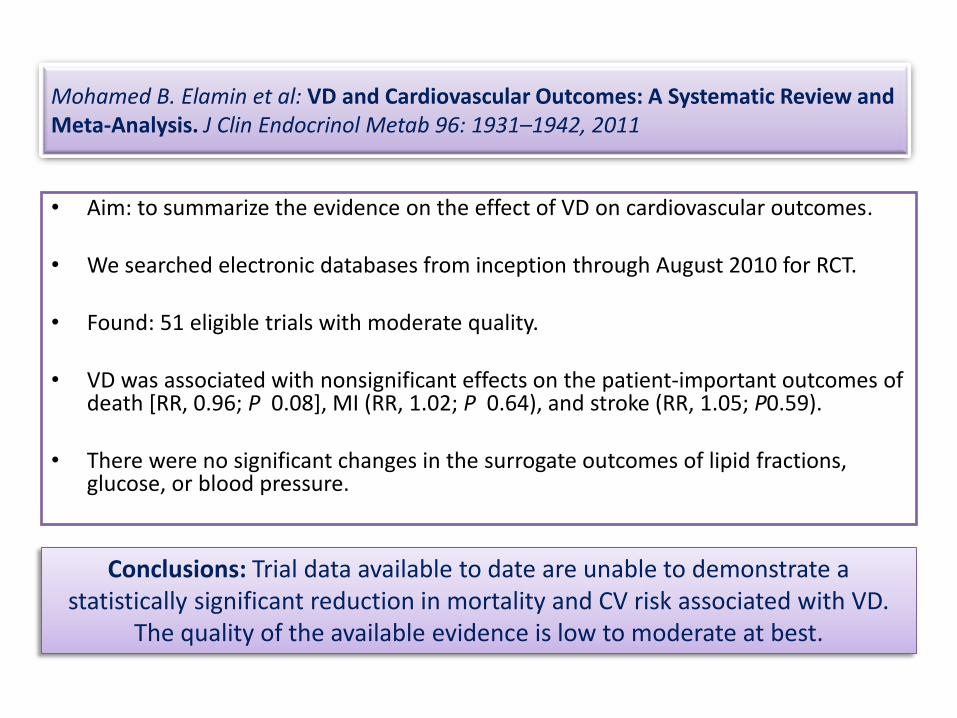
Mohamed B. Elamin et al: VD and Cardiovascular Outcomes: A Systematic Review and Meta-Analysis. J Clin Endocrinol Metab 96: 1931–1942, 2011
• Aim: to summarize the evidence on the effect of VD on cardiovascular outcomes.
• We searched electronic databases from inception through August 2010 for RCT.
• Found: 51 eligible trials with moderate quality.
• VD was associated with nonsignificant effects on the patient-important outcomes of death [RR, 0.96; P 0.08], MI (RR, 1.02; P 0.64), and stroke (RR, 1.05; P0.59).
• There were no significant changes in the surrogate outcomes of lipid fractions, glucose, or blood pressure.
Conclusions: Trial data available to date are unable to demonstrate a statistically significant reduction in mortality and CV risk associated with VD.
The quality of the available evidence is low to moderate at best.

Cholecalciferol Treatment to Reduce BP in Older Patients With Isolated Systolic HTA. The VitDISH Randomized Controlled Trial. JAMA Intern Med. online August 12, 2013.
OBJECTIVE To test whether high-dose, intermittent cholecalciferol supplementation lowers BP in older patients with isolated systolic HTA. DESIGN Parallel group, double-blind, placebo-controlled randomized trial. PARTICIPANTS: 159 patients, 70 years and older with isolated systolic HTA and baseline 25-OH-D <30 ng/mL. Randomized 100 000 U of oral cholecalciferol or matching placebo every 3 months for 1 year. MAIN OUTCOMES AND MEASURES Difference in office BP, 24-hour BP, arterial stiffness, endothelial function, cholesterol level, insulin resistance, and b-type natriuretic peptide level RESULTS: No significant treatment effect was seen for mean office BP or for any of the secondary outcomes (24-hour BP, arterial stiffness, endothelial function, cholesterol, glucose, and walking distance). There was no excess of adverse events in the treatment group, and the total number of falls was non significantly lower in the group receiving vitamin D (36 vs 46, P = .24).
CONCLUSIONS AND RELEVANCE: VD supplementation did not improve BP or markers of vascular health in older patients with isolated systolic HTA
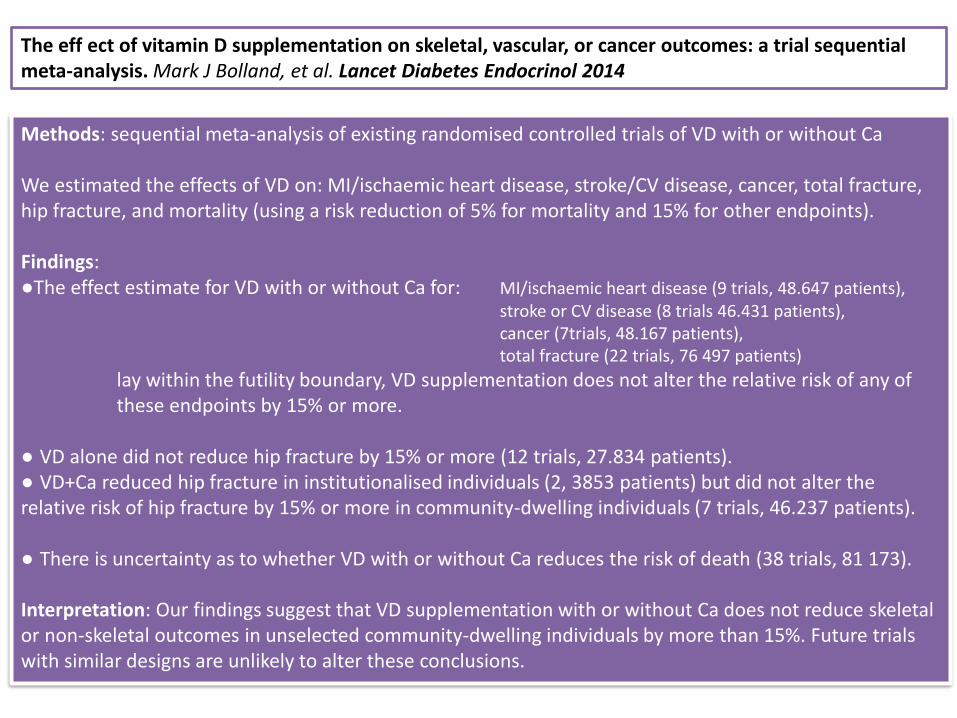
The eff ect of vitamin D supplementation on skeletal, vascular, or cancer outcomes: a trial sequential meta-analysis. Mark J Bolland, et al. Lancet Diabetes Endocrinol 2014
Methods: sequential meta-analysis of existing randomised controlled trials of VD with or without Ca We estimated the effects of VD on: MI/ischaemic heart disease, stroke/CV disease, cancer, total fracture, hip fracture, and mortality (using a risk reduction of 5% for mortality and 15% for other endpoints). Findings: ●The effect estimate for VD with or without Ca for: MI/ischaemic heart disease (9 trials, 48.647 patients), stroke or CV disease (8 trials 46.431 patients), cancer (7trials, 48.167 patients), total fracture (22 trials, 76 497 patients)
lay within the futility boundary, VD supplementation does not alter the relative risk of any of these endpoints by 15% or more. ● VD alone did not reduce hip fracture by 15% or more (12 trials, 27.834 patients). ● VD+Ca reduced hip fracture in institutionalised individuals (2, 3853 patients) but did not alter the relative risk of hip fracture by 15% or more in community-dwelling individuals (7 trials, 46.237 patients). ● There is uncertainty as to whether VD with or without Ca reduces the risk of death (38 trials, 81 173). Interpretation: Our findings suggest that VD supplementation with or without Ca does not reduce skeletal or non-skeletal outcomes in unselected community-dwelling individuals by more than 15%. Future trials with similar designs are unlikely to alter these conclusions.
Conclusion:
“Hypovitaminosis D seems to be associated with a worse prognosis in some cancers, but the currently available evidence is insufficient to recommend VD supplementation in cancer patients in clinical practice”
Prognostic role of VD status and efficacy of VD supplementation in cancer patients: a systematic review. Buttigliero C et al; Oncologist. 2011;16:1215-27.
Whether or not hypovitaminosis D can influence the prognosis of cancer patients and whether or not vitamin D (vitD) supplementation improves outcome remain controversial. DESIGN: Studies evaluating the prognostic role of vitD and vitD receptor (VDR) in cancer patients and trials evaluating the efficacy of vitD administration on patient outcome were identified by a search of MEDLINE, EMBASE, ISI Web of Knowledge, and the Cochrane Library through June 2010. RESULTS: Twenty-five studies were included. A negative prognostic role for low serum vitD level was observed in five cohort studies including patients with breast cancer (one study), colon cancer (two studies), prostate cancer (one study), and melanoma (one study), but not in two studies on non-small cell lung cancer and one study on breast cancer. Three of four studies showed that VDR(+) tumors carry a better prognosis than VDR(-) tumors, whereas VDR polymorphisms were significantly associated with prognosis in five of 10 studies. A significant interaction between serum vitD level and VDR polymorphism was observed in one study. Three randomized trials involving advanced prostate cancer patients explored the prognostic role of vitD supplementation. A meta-analysis of these trials showed no effect on survival (pooled risk ratio, 1.07; 95% confidence interval, CI, 0.93-1.23), with strong heterogeneity among studies.
Conclusion: monthly administration of 100 000 IU of VD did not reduce the incidence or severity of URTIs in healthy
adults
David R. Murdoch et al, Effect of Vitamin D3 Supplementation on Upper Respiratory Tract Infections in Healthy Adults. The VIDARIS Randomized Controlled Trial. JAMA. 2012;308(13):1333-1339

aspectes a tractar: (proposta 30 minuts)
• VD: breu resumen del metabolisme, nivells sèrics a la població general
• associació del dèficit de VD amb múltiples patologies, estudis epidemiològics i observacionals
• mecanismes fisiopatològics que pretenen explicar aquesta associació
• resultats d’estudis d’intervenció
• conclusions (o millor: reflexions)
conclusions (reflexions):
• En conjunt, els estudis clínics no han pogut demostrar efectes
estadísticament significatius en quant a la suplementació amb VD en la evolució cardio-metabólica.
• Les dades disponibles son inadequades per mantenir la hipòtesis de que es podria millorar la evolució cardio-metabolica mitjançant l’augment de l’administració de VD.
• Es necessari la realització d’estudis adequats, prospectius, aleatoritzats, en poblacions ben seleccionades per comprovar el paper de la VD com a tractament en prevenció primària
• L’ administració de VD sembla ser un element prometedor (?), encara que de moment sense evidencia comprovada, en la prevenció i maneig de la malaltia cardio-metabólica
The IOM report suggests that a
serum level of 20 ng per milliliter of 25-(OH)D would protect 97.5% of the
population against adverse skeletal outcomes such as fractures and falls.
Scientific evidence indicates that Ca
and VD play key roles in bone health.
The current evidence, however, does not support other benefits for VD or
Ca intake.
IOM report on calcium and vitamin D. Washington, DC: Institute of Medicine, 2010. (http://www.iom.edu/vitaminD.)
Osteoporosis, heart disease, cancer,
autoimmune disease,
stroke,depression, insomnia, arthritis,
diabetes, dementia, hypertension,
chronic pain, psoriasis, infections….
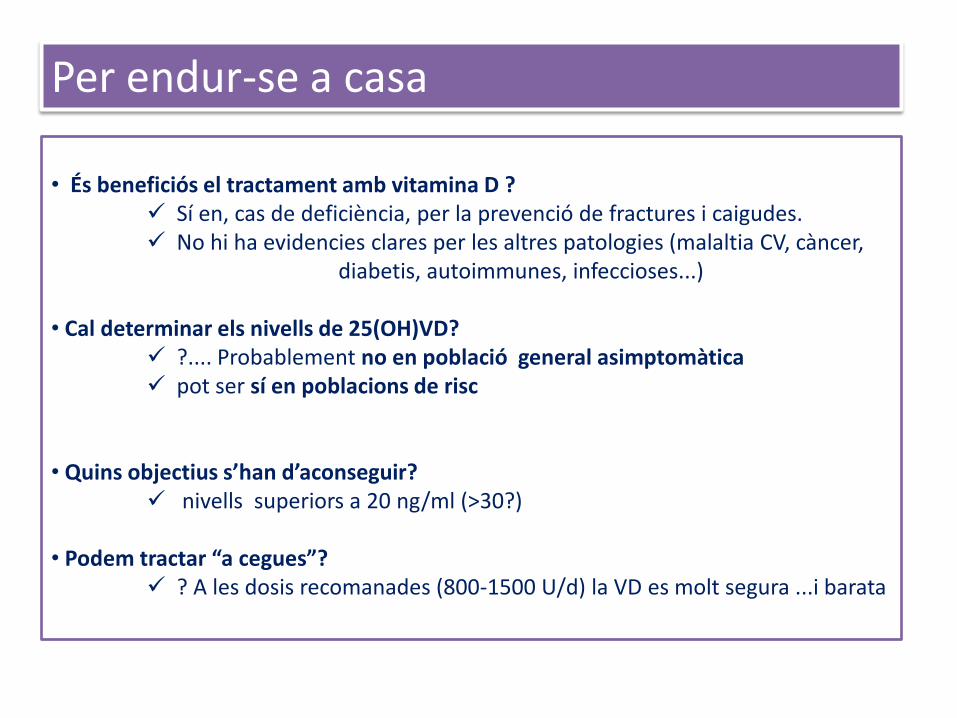
• És beneficiós el tractament amb vitamina D ?
Sí en, cas de deficiència, per la prevenció de fractures i caigudes. No hi ha evidencies clares per les altres patologies (malaltia CV, càncer, diabetis, autoimmunes, infeccioses...)
• Cal determinar els nivells de 25(OH)VD?
?.... Probablement no en població general asimptomàtica pot ser sí en poblacions de risc
• Quins objectius s’han d’aconseguir?
nivells superiors a 20 ng/ml (>30?) • Podem tractar “a cegues”?
? A les dosis recomanades (800-1500 U/d) la VD es molt segura ...i barata
Per endur-se a casa