-
DEMOGRAFI & KELUARGA BERENCANADr. Alfaina Wahyuni,
M.Kes,SpOG
-
Latar Belakang Masalah
BANYAK NEGARA YANG MENGALAMI MASALAH YANG SANGAT KOMPLEK
:POPULASI EXPLOTION (LEDAKAN PENDUDUK) INDONESIA : negara
berkembang dengan jumlah penduduk terbesar ke-4 didunia setelah
CINA, INDIA, USASENSUS PENDUDUK TH.2010 MENYATAKAN jumlah penduduk
Indonesia 237,6 juta (th 2000 = 205,1jt)Laju pertumbuhan penduduk:
1,41%Jumlah laki-laki lebih bnyak 1,6 juta dibandingkan dengan
wanita: Ledakan jumlah lansia60,1% di Jawa
-
Kependudukan
PENDUDUKORANG YANG MENDIAMI WILAYAH DALAM WAKTU
TERTENTUDEMOGRAFI / ILMU KEPENDUDUKANPEROBAHAN KOMPOSISI
PENDUDUKDISTRIBUSI PENDUDUK
-
FAKTOR DEMOGRAFI dan EVALUASI DATA DEMOGRAFI
FERTILITAS/KESUBURAN - Angka Kelahiran kasar (jumlah kelahiran
hidup per 1000 populasi)Angka kelahiran umum (jumlah kelahiran
hidup per 1000 perempuan usia 15-49 tahun)MORTALITAS /
KEMATIAN:Angka kematian kasar (jumlah kematian per 1000
populasi)Angka kematian maternal (jumlah kematian perempuan karena
hamil, persalinan atau nifas per 100.000 kelahiran hidup)Tahun 2008
di Indonesia: AKM: 225/100.000 persalinan AKM th 2008 di DIY:
93/100.000 persalinanMillenium Development Goals (MDGs)2015: AKM
103/ 100.000 persalinan) PERKAWINANMIGRASIMOBILITAS SOSIAL
-
MASALAH KEPENDUDUKAN INDONESIA
JUMLAH PENDUDUK BESARPERTUMBUHAN PENDUDUK TINGGIPENYEBARAN TIDAK
MERATA (th 2010, 60,1% di Jawa)KUALITAS KURANG / RENDAHANGKA
KELAHIRAN TINGGIAngka kematian tingiAngka kematian ibu tinggi (2008
= 225/100.000 persalinan)Angka kematian bayi tinggi (2008= 35/1000
kelahiran hidup)
-
KEBIJAKAN KEPENDUDUKAN DI INDONESIA:
Penurunan angka kelahiran Keluarga BerencanaPenurunan angka
kematianPerpanjangan angka harapan hidupPenyebaran penduduk yang
lebih serasi dan seimbangPola urbanisasi yang lebih berimbang dan
merataPerkembangan dan penyebaran angkatan kerja
-
KELUARGA BERENCANAKELUARGA BERENCANAMEMBANTU MENYELESAIKAN
MASALAH KEPENDUDUKAN MEMBANTU TERCAPAINYA KELUARGA BAHAGIA DAN
SEJAHTERAPROGRAMMENGATUR KEHAMILANMENGOBATI KEMANDULANNASEHAT
PERKAWINAN
KB merupakan pilar dalam program Safe Motherhood (1994) dan
Making Pregnancy Safer (2000)
-
Safe motherhood (1994):
Suatu usaha untuk menyelamatkan kehamilan yang mengancam jiwa
ibu/janin sebagai akibat langsung kehamilan/persalinannya5 Pilar
safe motherhood:Keluarga BerencanaAsuhan antenatal penilaian risiko
tinggiPersalinan bersih dan amanAsuhan pasca
keguguranPenatalaksanaan kegawatdaruratan obstetri
-
Making Pregnancy Safer (2000)
Strategi sektor kesehatan yang berfokus pada perencanaan
sistematis & terpadu dalam melakukan intervensi klinsTarget:
tahun 2010 AKI 125/100.000 & AKP 35/1000Strategi : Rencana
Strategis Nasional MPS 2001-20103 Pesan Kunci:1. Setiap persalinan
ditolong oleh tenaga kesehatan terlatih/terampil;2. Setiap
komplikasi obstetri dan neonatal memperoleh pelayanan rujukan yang
adekuat.3. Setiap wanita usia subur mempunyai akses terhadap
pencegahan kehamilan yang tidak diinginkan dan penanganan
komplikasi keguguran
-
TUJUAN DARI DUKUNGAN PELAYANAN KB UNTUK MEMECAHKAN MASALAH
DEMOGRAFI
Konseling dan konsultasiKomunikasiInformasiEdukasiPelayanan
kontrasepsiIUCD (Intra Uterine Contraception Device) / AKDR (Alat
Kontrasepsi Dalam Rahim).InjeksiPil oralSterilisasi wanita secara
medisEfek samping manajemenKegagalan kontrasepsiPerdarahan
spot/bercak pervaginamInfeksiNyeri panggul.Konseling
pernikahanKonsultasi remaja dan menopause
-
Contraceptive
OptionsEstrogen/progestinoraltransdermaltransvaginalinjectableProgestin
onlyoralinjectableimplantsIntrauterineSterilizationtubal
ligationtranscervical (Essure)vasectomy
Non-hormonal IUDBarrier methodsmale condomfemale
condomdiaphragm, cervical cap
Periodic abstinence or fertility awareness Emergency
contraception
-
Contraceptive ConsiderationsEffectivenessFrequency of
intercourseSexual behaviorDesire for future fertilityCost of
methodSide effectsContraindicationsNoncontraceptive
benefitsPatients perceptions and misconceptionsPatients health
status and medical conditions
-
PERIODIK ABSTINENCE / PANTANG BERKALAMASA SUBUR: dicatat 3
siklus menstruasiSIKLUS TERPANJANG - 11SIKLUS TERPENDEK -
18SELISIHNYA MASA SUBURContoh: terpanjang 35 hari, terpendek 28
hari. Masa subur (28-18) sd (35-11),atau hari ke 10-24KONDOM /
SARUNG KBOBAT SPERMATISID:TABLET, BUSA, KRIM, GEL / AGAR
-
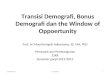
Barrier Methods
-
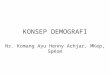
AKDR / IUDMEKANISME KERJA:LOCAL STERILE
INFLAMATIONSPERMICIDALTIPE: CU T, NOVA T, CU 7, + PROGESTERON,
MLKONTRA INDIKASI:KEHAMILAN, RADANG PANGGUL, PERDARAHANRISIKO /
EFEK SAMPINGNYERI PANGGUL, PERDARAHAN, PERFORASI, INFEKSI
PANGGUL
-
COPPER BEARING IUDsTCU-200COPPER-7+ progesteronLippes Loop
-
Hormonal Contraceptives (Estrogen & Progestin)
-
Combination Contraceptives (Estrogen &
Progestin)Ingredients:Estrogen (ethinyl estradiol) 20-50
mcgProgestin (varying forms, doses, potency)
Mechanisms of action:Suppression of ovulationThickening of
cervical mucusThinning of endometriumSlowing of tubal and
endometrial motility
-
Progestin-Only ContraceptivesMechanisms of action: Inhibition of
ovulation Prevention of sperm penetration by thickening and
decreasing the quantity of cervical mucus Endometrial atrophy
-
JENIS PROGESTAGEN PADA KONTRASEPSI HORMONAL
LOW ANDROGEN EFFECT Nor Ethindron0,5Desogestrel 0,15Cyproteron
AcetatDrospirenon MEDIUM ANDROGEN EFFECT Nor Ethindron
1,0Ethynordiol Diacetat 1,0HIGH ANDROGEN EFFECTNorgestrel 0,5 /
0,3Nor Ethindron 1,5 / 2,5Levonorgestrel 0,15
-
PROFIL FARMAKOLOGI PROGESTAGEN
JENISAKTIFITASPROGESTOGENAKTIFITAS ANTI ANDROGENIKAKTIFITAS ANTI
M. CORTICOIDAKTIFITASG.
CORTICOIDPROGESTERONE+(+)+_DROSPIRENONE+++_CYPROTERONE
ACETATE++_(+)DESOGESTREL+___LEVO NORGESTREL+___GESTODENE+_(+)_
-
KONTRASEPSI ORAL YANG BEREDAR DI INDONESIA
N0NAMA DAGANGPRODUKSIOESTROGENPROGESTAGEN123456789101213Gracial
28GyneraMicrogynonLyndiolMarvelon 28Mercilon 28Nordette 28Ovostat
28Trinordiol 28TriquilarDiane 35YasminOrganonSchering AGSchering
AGOrganonOrganonOrganonWyethOrganonWyethSchering AGSchering
AGSchering AGEthinil Estradiol7 hr : 0,04 mg15 hr : 0,03 mgEE 30
mcgEE 30 mcgEE 30 mcgEE 30 mcgEE 20 mcgEE 30 mcgEE 50 mcg6 hr : EE
30 mcg5 hr : EE 40 mcg10 hr : EE 30 mcg6 hr : EE 30 mcg5 hr : EE 40
mcg10 hr : EE 30 mcgEE 35 mcgEE 30 mcgDesogestrel0,025 mg0,125
mgGestodene 75 mcgLevonorgestrel150 mcgLynestrenol 2,5
mgDesogestrel 150 mcgDesogestrel 150 mcgLevonorgestrel150
mcgLynestrenol 1 mgLevonorgestrel 50 mcgLevonorgestrel 75
mcgLevonorgestrel125 mcgLevonorgestrel 50 mcgLevonorgestrel 75
mcgLevonorgestrel125 mcgCyproteron Acetat 2mgDrospirenon 3 mg
-
Kontrasepsi oralMonofasik berisi estrogen atau progesterone atau
kombinasi keduanya dengan dosis tetap sepanjang siklus
haid.Trifasik obat yang berisi kombinasi estrogen dan progesterone
dengan dosis bervariasi 3 macam sepanjang siklus haid.Sekuensial
14-15 hari pertama hanya diberikan estrogen, selanjutnya diberi
kombinasi estrogen dan progesterone sampai siklus haid selesai.Mini
pil pil mini mengandung progesterone saja, tanpa estrogen. Dosis
progesteron dalam pil ini 0,5 mg atau kurang. After-morning pil
disebut juga postcoital contraception. Pil ini berupa estrogen yag
diberikan dalam dosis tinggi segera setelah coitus yang tidak
dilindungi.
-
Kontrasepsi hormonal injeksi
Kontrasepsi suntikan Long acting progesterone: 1 bulan, 3 bulan
Kombinasi
-
KONTRASEPSI DARURAT
MENCEGAH KEHAMILAN YG TAK DIKEHENDAKI:SEXUAL INTERCOURS TANPA
PERLINDUNGAN KONTRASEPSIPERKOSAANKESALAHAN PEMAKAIAN
KONTRASEPSI:KONDOM BOCORTERLAMBAT SUNTIK KBSALAH HITUNG MASA
SUBURLUPA MINUM PIL KB
-
JENIS KONTRASEPSI DARURAT
MEKANIK : AKDR / IUCDMENCEGAH FERTILISASIMENCEGAH
IMPLANTASIMEDIK : OBAT HORMONALMENCEGAH OVULASIMENCEGAH
FERTILISASIMERUBAH ENDOMETRIUM / MENCEGAH NIDASIMENGGANGGU TUBA
-
Kontrasepsi Darurat
OBAT YANG SERING DIGUNAKAN: ESTROGEN (LYNORAL, PREMARIN),
PROGESTIN (POSTINOR-2, LEVONORGESTREL), PIL KB KOMBINASI / METODE
YUZPE (MYCROGYNON, NEOGYNON)DIMINUM SEBELUM 72 JAM SESUDAH SEKSUAL
INTERCOURSE DAN DIULANG 12 JAM KEMUDIAN
-
Tubal LigationMechanism of action: the fallopian tubes are cut
or mechanically blocked to prevent the sperm and ovum from
unitingCan be performed laparo-scopically or through a suprapubic
mini-laparotomy incision (or at C-section)Failure rate: 0.5%
-
VasectomyMechanism of action: each vas deferens is cut to
prevent the passage of sperm into the ejaculated seminal fluid
FAILURE RATE: perfect use0.10%typical use0.15%
-
ANGKA KEGAGALAN KONTRASEPSI
JENIS KONTRASEPSIKEGAGALANPANTANG BERKALA20 %SPERMICIDE20
%SERVICAL CAP20 %SERVICAL SPONGE20 %KONDOM20 %DIAPHRAGMA20 %ORAL
PIL3 %IUD1 %DEPO PROVERA0,3 %NORPLANT0,1 %MOW0,4 %MOP0,1 %
-
Biologi Reproduksi
Biologi Reproduksi
-
KB dalam perseptif IslamBerbuatlah baik kepada kedua ibu
bapakmu, ibu telah mengandung dalam keadaan lemah dan bertambah
lemah, menyapih dalam dua tahun (Luqman 14)Berbuat baiklah kepada
ibu bapakmu, ibu mengandung dalam keadaan susah payah dan
melahirkan dalam keadaan susah payah. Mengandung sampai menyapih
adalah tigapuluh bulan (Al Ahqaf 15)Berkawinlah kamu dengan wanita
yang berbakat punya anak banyak dan penyayang, rosululloh bangga
dengan jumlah umatnya dihari kiyamatLebih baik tinggalkan ahli
warismu dalam keadaan kaya dari pada menjadi beban yang minta-minta
orang banyakOrang mumin yang kuat itu lebih baik dan lebih disayang
oleh alloh daripada orang mumin yang lemah (Hadist)
-
PRINSIP DASAR KELUARGA BERENCANA DALAM ISLAM
Menyelamatkan ibu.Pendidikan anak dan jaminan dan prospek masa
depanMoralnya baik dan selamat agamanya
*What are the contraceptive options? They include:
A combination of estrogen and a progestin, which can be
delivered:orally (combined OCPs)transdermally (Ortho Evra
patch)transvaginally (Nuva Ring)as an injection (Lunelle; currently
unavailable in the U.S.)
Progestin-only methods:oral (progestin-only or mini
pills)injectable (Depo Provera)implants (Norplant) intrauterine
(Mirena)
Non-hormonal IUD: Paragard copper TBarrier methods:male
condomfemale condomdiaphragm, cervical cap
Periodic abstinence or fertility awareness methods
Sterilizationfemale: tubal ligation or Essure transcervical
sterilizationmale: vasectomy
Emergency contraception: post-coital contraception*These are the
clinicians considerations in helping a woman to choose a
contraceptive method:effectivenessfrequency of intercoursesexual
behaviordesire for future fertilitywhether the method is
affordablepotential side effectscontraindicationsnoncontraceptive
health benefitsthe patients perceptions and misconceptionsthe
patients general health and any medical conditions*Barrier methods
are some of the oldest forms of contraception. They include male
and female condoms, diaphragms and cervical caps, and
spermicides.*Combination contraceptives contain a combination of
estrogen and a progestin.
They are available in several forms.
All of the most common oral contraceptives are a combination of
estrogen and progestin. Birth control pills were first introduced
in 1960.
The Ortho Evra patch came out in 2002 and delivers the same
hormones through a transdermal system.
Also in 2002, the Nuva Ring was introduced which delivers
estrogen and progestin by means of a flexible plastic ring inserted
in the vagina.
This combination was also available in an injectable form in the
U.S. under the brand name Lunelle. Lunelle was introduced into the
U.S. market in 2000 and withdrawn by the manufacturer in 2002
because of concerns that some lots of the drug were not
sufficiently potent to prevent pregnancy. There is currently no
injectable combination contraceptive available in the U.S.*All of
the combination contraceptives contain estrogen as ethinyl
estradiol in dosages ranging from 20 to 50 micrograms plus one of
seven different progestins.
Combination contraceptives work by:(1) suppression of ovulation
(90-95% of the time)(2) thickening of the cervical mucus, blocking
sperm penetration and entry into the upper reproductive tract(3)
thinning of the endometrial lining, thus inhibiting implantation(4)
slowing tubal and endometrial motility, thus inhibiting
implantation*Progestin-only contraceptives work by:
Inhibiting ovulation by inhibiting positive feedback of
estradiol on LH and FSH (suppressing midcycle peaks of LH and
FSH)
Thickening cervical mucus to prevent sperm penetration
Changing the endometrium so that the atrophic lining is not
receptive to the blastocyst*Tubal ligation can be performed
laparoscopically or through a suprapubic mini-laparotomy incision.
It can also be performed at the time of C-section.
Tubal ligation works by cutting or blocking the fallopian
tubes.
It has a failure rate of 0.5%. NOTHING IS PERFECT!*Vasectomy is
permanent male sterilization. The vas deferens on each side is
severed so that sperm cannot pass into the ejaculated seminal
fluid.
Vasectomy is highly effective, with a typical use failure rate
of only 0.15%. Failures are believed to be due to sperm exposure
before all of the sperm have been cleared from the reproductive
tract. This takes about 20 ejaculations.